
Abstract
Background:
Infections are common occurrences at end of life that are associated with high rates of morbidity and mortality among frail elderly individuals. The problem of infections in nursing homes has led to a subsequent overuse and misuse of antibiotics in this already-frail population. Improving palliative care in nursing homes has been proposed as a key strategy to reduce the use of antibiotics.
Aim:
The aim of this study was to describe the current status of how nursing homes integrates palliative care and infection management at end of life across the nation.
Design:
This is a cross-sectional survey of nationally representative US nursing homes.
Setting/participants:
Between November 2017 and October 2018, a survey was conducted with a nationally representative random sample of nursing homes and 892 surveys were completed (49% response rate). The weighted study sample represented 15,381 nursing homes across the nation.
Results:
Most nursing homes engaged in care plan documentation on what is important to residents (90.43%) and discussed spiritual needs of terminally ill residents (89.50%). In the event of aspiration pneumonia in terminally ill residents, 59.43% of nursing homes responded that resident would be transferred to the hospital. In suspected urinary tract infection among terminally ill residents, 66.62% of nursing homes responded that the resident will be treated with antibiotics.
Conclusion:
The study found wide variations in nursing home palliative care practices, particularly for timing of end-of-life care discussions, and suboptimal care reported for antibiotic usage. Further education for nursing home staff on appropriate antibiotic usage and best practices to integrate infection management in palliative care at the end of life is needed.
Keywords
Approximately 2 million infections occur in nursing home settings annually, and these infections have been associated with high rates of morbidity, mortality, and higher healthcare-related costs.
Infection management at end of life is a complex process, which requires an individualized approach.
Integration of palliative care and infection management can help reduce burdensome treatments and improve quality of care for nursing home residents at the end of life.
In a representative sample of US nursing homes, we found suboptimal palliative care and infection management practices at end of life with preferences for infection management to be more often elicited after an event then on admission.
In the event of aspiration pneumonia, about two-third of nursing homes would be somewhat to very likely to send the terminally ill nursing home resident to the hospital.
In suspected urinary tract infection at the end of life, about two-third of nursing homes would catheterize the resident to obtain a urine specimen and begin treating with antibiotics.
A system where nursing home residents’ preferences for infection management are routinely elicited and frequently revisited by nursing home care providers is urgently needed.
Nursing home residents’ preferences for end-of-life care interventions to be delivered, as well as withheld, is an important part of advance care planning at end of life.
Adequate training and educational opportunities to empower nursing home staff in appropriate use of antibiotics at end of life can cultivate positive changes in how we deliver care to frail nursing home residents.
Introduction
Nursing homes are becoming an important healthcare sector for the provision of skilled nursing and end-of-life care across several countries. The population of those 65 years and older constitutes nearly 80% of the total 1.5 million nursing home users in the United States, and more than half of these individuals are in the oldest age group (i.e. 85 years and older). 1 In Australia, about 80% of those who died in 2010–2011 aged 65 years or above had used aged care services in the 8 years prior to their death. 2 In the United Kingdom, nursing homes (known as care homes) are an increasingly common part of clinical practice for end-of-life care. 3 Furthermore in the United States, it is projected that the demand for nursing homes will continue to rise over the next few decades in conjunction with the aging baby boomer generation; by 2050, the number of older people in the United States is expected to reach approximately 84 million, nearly double the 43 million reported in the 2012 census report. 4
Long-term nursing home residents have different healthcare needs than that of other healthcare users (e.g. short-term residents receiving rehabilitative care or patients from acute care facilities). These residents are more likely to have two or more chronic conditions,5–7 be living with serious/advanced illnesses,8,9 and be nearing the end of their lives.1,10 Decreased immune function and limited physical mobility among older long-term nursing home residents place them at risk of experiencing negative health outcomes such as healthcare-associated infections,11–14 adverse effects from antibiotics use,15–18 and increased physical suffering.19–22 Furthermore, infections are common at end of life and are associated with high rates of morbidity and mortality.14,23 Infections are also recognized as one of the main risk factors for burdensome care transitions (defined as nursing home resident transfer to acute care facilities at end of life),24–26 which can lead to increased financial burden17,27 as well as receipt of unwanted and often invasive procedures that may contradict a dying patient’s wishes. 28 Moreover, the problem of infections in nursing homes has led to a subsequent overuse and misuse of antibiotics, which has increased risk for multiple drug-resistant organisms and other adverse outcomes (e.g. Clostridioides difficile).29–31
Systematic efforts have been undertaken to promote appropriate antibiotic use (i.e. antibiotic stewardship) and to reduce adverse effects of antibiotics. Although such programs were shown to be highly effective in the reduction of antibiotic-related adverse effects and care-related costs,32–37 data were largely limited to hospital settings. It has been argued that implementation of antibiotic stewardship in nursing homes presents unique challenges due to the high volume of frail individuals with complex medical conditions and lack of resources (e.g. diagnostic testing equipment and/or local antibiotic resistance data).13,38–40 Consequently, up to 80% of terminally ill nursing home residents receive antibiotics.41–44 Strategies to prevent overutilization or inappropriate use of antibiotics is critical in the nursing home setting, in order to enhance quality of care while minimizing potential harms.
The Centers for Medicare and Medicaid Services has a network of contractors called Quality Innovation Network–Quality Improvement Organizations (QIN-QIOs) that seek to prevent infections in nursing home residents and improve antibiotic stewardship in these settings.45,46 One of the ways the QIN-QIOs do this is through supporting nursing homes to enroll and participate in the Centers for Disease Control and Prevention’s the National Healthcare Safety Network (NHSN), an Internet-based infection surveillance tool designed to aid in the tracking and reporting of infections.47,48
Rather than providing aggressive treatments, which heavily focus on the life-prolongation and can inadvertently cause more suffering, a timely introduction of palliative care should be a high priority for nursing home residents at end of life. Palliative care is an interdisciplinary specialty that focuses on symptom management and quality of life for individuals living with serious illnesses.49–51 Palliative care is associated with fewer burdensome care transfers,52,53 enhanced symptom management,54–56 higher care satisfaction,54,57 and lower use of aggressive medical treatments (e.g. intravenous antibiotics).55,57,58 Compared to hospice care, which requires care recipients to have a life expectancy of 6 months or less,49,59 palliative care should occur earlier along the continuum of care and may be more appropriate for long-term nursing home residents who have less predictable illness trajectories.60,61
Improving palliative care in nursing homes has been proposed as one key strategy to improve infection management and reduce the use of antibiotics at the end of life. 62 Previous researchers have found that palliative care is a highly effective approach to meet three important aims in end-of-life care: (1) improved care experiences,63,64 (2) improved health, 65 and (3) reduced use of unnecessary medical interventions. 66 It is the latter that explains how palliative care may help reduce inappropriate use of antibiotics in the nursing home population. With advance care planning discussions, patient preferences for level of care and types of medical interventions (i.e. antibiotics and/or hospital transfer for future infection) are elicited.67–69 Documented care preferences can later serve as an important guide in determining whether the use of these potentially burdensome treatments at end of life aligns with a dying patient’s care wishes. Our objective is to describe the integration of palliative care and infection management practices at end of life in US nursing homes.
Methods
From a nationally representative stratified random sample of nursing homes, we collected systematic information. The cross-sectional facility-level survey included questions regarding the nursing palliative care processes as well as the integration of infection management and palliative care at the end of life. Our reporting of the methods and results follows the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). 70
Sample
We identified nursing homes from the 2016 Certification and Survey Provider Enhanced Reporting (CASPER) data. Nursing homes were eligible if they were non-specialized, free-standing nursing homes with at least 30 beds, and a CASPER assessment date of 2014 or later. Smaller nursing homes (i.e. those with fewer than 30 beds) were excluded because they are different than the vast majority of facilities that care for the majority of residents across the nation. Random sampling was stratified by QIN-QIO region (an equal number of nursing homes across each of the 14 regions) and NHSN enrollment (30% of all sampled nursing homes were enrolled in NHSN) to increase the probability that the sample is representative of the nation. In addition, because this analysis is part of a larger study investigating how infection prevention in nursing homes has changed over time, a subset of our sample participated in a prior survey conducted by the research team of the larger study (988 nursing homes that completed surveys in 2013–2014). 71
Recruitment
Using previously successful methods, recruitment occurred in waves of 200–300 nursing homes each. The Director of Nursing at each nursing home was mailed an invitation letter with instructions for survey completion. Respondents were given the option to respond through Web or mail. Incentives included US$25 gift cards for completed surveys and inclusion in US$250 lotteries for those who returned the survey within 1 month. Paper-based surveys were entered into an electronic database, and data quality was checked through double data entry of a random sample of 10% of the surveys.
Data collection
We administered our cross-sectional facility-level survey to 1820 nursing home Directors of Nursing between November 2017 and October 2018. Data from paper-based surveys were entered into an online database, and double data entry was done on 10% of the sample to check for data entry accuracy. Web and paper-based survey data were combined into a single analytical dataset. Further details of the survey development, sampling strategy, and recruitment methods are published elsewhere. 72 All procedures were approved by Columbia University Institutional Review Board (protocol no. IRB-AAAR1564). Approval was granted on 10 January 2017.
Measures
Integration of infection management and palliative care was operationalized using two sets of measures. The first set of measures included eight items with four items on eliciting preferences for infection management practices among terminally ill residents and four items on facility-level practices for infection management at end of life. These questions used a four-point Likert-type scale ranging from “rarely” to “almost always.” The second set of measures was in the form of a vignette describing an advanced stage Alzheimer’s patient near the end of life as follows: Ms. Davis has been in your facility for 4 months. On admission, she was ambulatory and needed total assistance with feeding. She was admitted with advanced heart disease, osteoporosis, a right hip fracture, and Alzheimer’s disease. She takes oxycodone 10 mg every 6 hours for pain. In the past month, you notice she is eating less, has lost 10 pounds, and coughs when drinking. Ms. Davis no longer recognizes her family.
The vignette then presented two scenarios. Scenario 1 suggested Ms Davis may have an aspiration pneumonia (seven items). Scenario 2 suggested Ms Davis may have a urinary tract infection (UTI; three items). Under each scenario, the care practices or orders that would be in place in the case were listed and respondents were instructed to select how likely it would occur. Responses for the vignette were scored on a three-point Likert-type scale ranging from “not at all likely” to “very likely.”
Data analysis
Weights to adjust for differential probabilities of inclusion and response in the study were constructed and weighted frequencies were computed. 72 A normalized mean response (µ) was computed for each question by dividing the question response by the highest possible value and multiplying by 100 (i.e. if the response was a 3 on the four-point Likert-type scale, the calculation was 3/4 × 100 = 60) and averaged across nursing homes. The mean response represents the fraction of the total possible score on average and is presented in a scale from 0 to 100 for ease of interpretation as well as to compare scores across the differing Likert-type scales in the two sets of measures. All calculations were done using SAS version 9.4.
Results
We received 892 completed surveys for a 49% response rate. 72 With the weighted sample, the results represent 15,381 nursing homes across the United States.
We examined the elicitation of infection management preferences at the end of life. Table 1 describes the results regarding the elicitation of infection management preferences at the end of life. On average, for those who are terminally ill, residents’ or families’ preferences for infection management were more likely to be elicited following a change in condition such as developing a fever (µ = 84.93, SE = 0.82) or an event such as aspiration (µ = 82.29, SE = 0.88), and less likely during care plan meetings (µ = 7 5.83, SE = 0.98), or upon admission (µ = 72.56, SE = 1.11). Just over half (55%–60%) of nursing home facilities almost always elicited these preferences during a change in condition versus eliciting preferences upon admission or care plan meetings (about 45% of all nursing homes). On average, nursing homes frequently included residents and resident proxies in treatment decisions for suspected infections near the end of life (µ = 91.77, SE = 0.62), considered residents’ goals in managing care (µ = 90.16, SE = 0.65), and adhered to standard infection control policies such as isolation precautions during end-of-life care (µ = 90.02, SE = 0.73). Just over half of all nursing homes (52.80%) gave antibiotics near the end of life.
Weighted distribution of eliciting preferences for infection management practices in terminally ill residents of US nursing homes (n = 892, weighted n = 15,381).
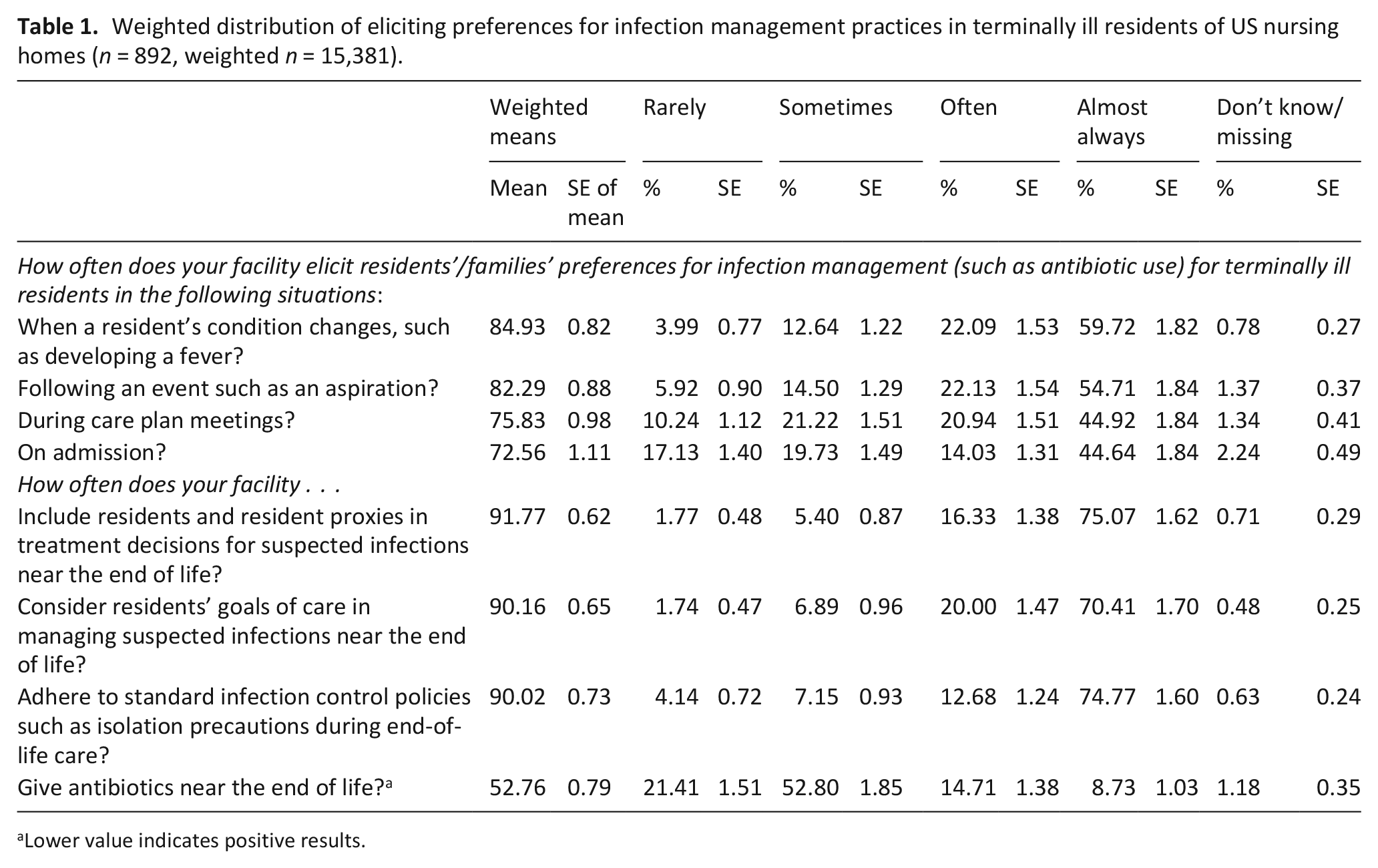
Lower value indicates positive results.
Table 2 presents the results from the vignette. On average, in the event of symptoms consistent with an aspiration pneumonia, nursing home residents were likely to have a “do not resuscitate” (µ = 83.71, SE = 0.76) and nursing home staff were likely to ask the proxy how to manage the suspected infection (µ = 80.83, SE = 0.89). Having “palliative/comfort measures” order and a “do not hospitalize” order was less frequent on average (µ = 67.33, SE = 0.90; µ = 64.02, SE = 0.92, respectively). On average, about two-third of nursing homes would send a terminally ill resident suspected of an aspiration pneumonia to the hospital (µ = 59.43, SE = 0.83). Half of all nursing home facilities (50.23% of all nursing homes) were somewhat likely to send the patient to the hospital in the event of aspiration pneumonia. Medical providers deciding how to manage care without asking the patient proxy and having a “do not administer antibiotics” order occurred in about half of the nursing homes (µ = 51.77, SE = 0.97; µ = 47.80, SE = 0.75, respectively).
Weighted distribution of vignette-based palliative care and infection management processes among US nursing homes (n = 892, weighted n = 15,381). a
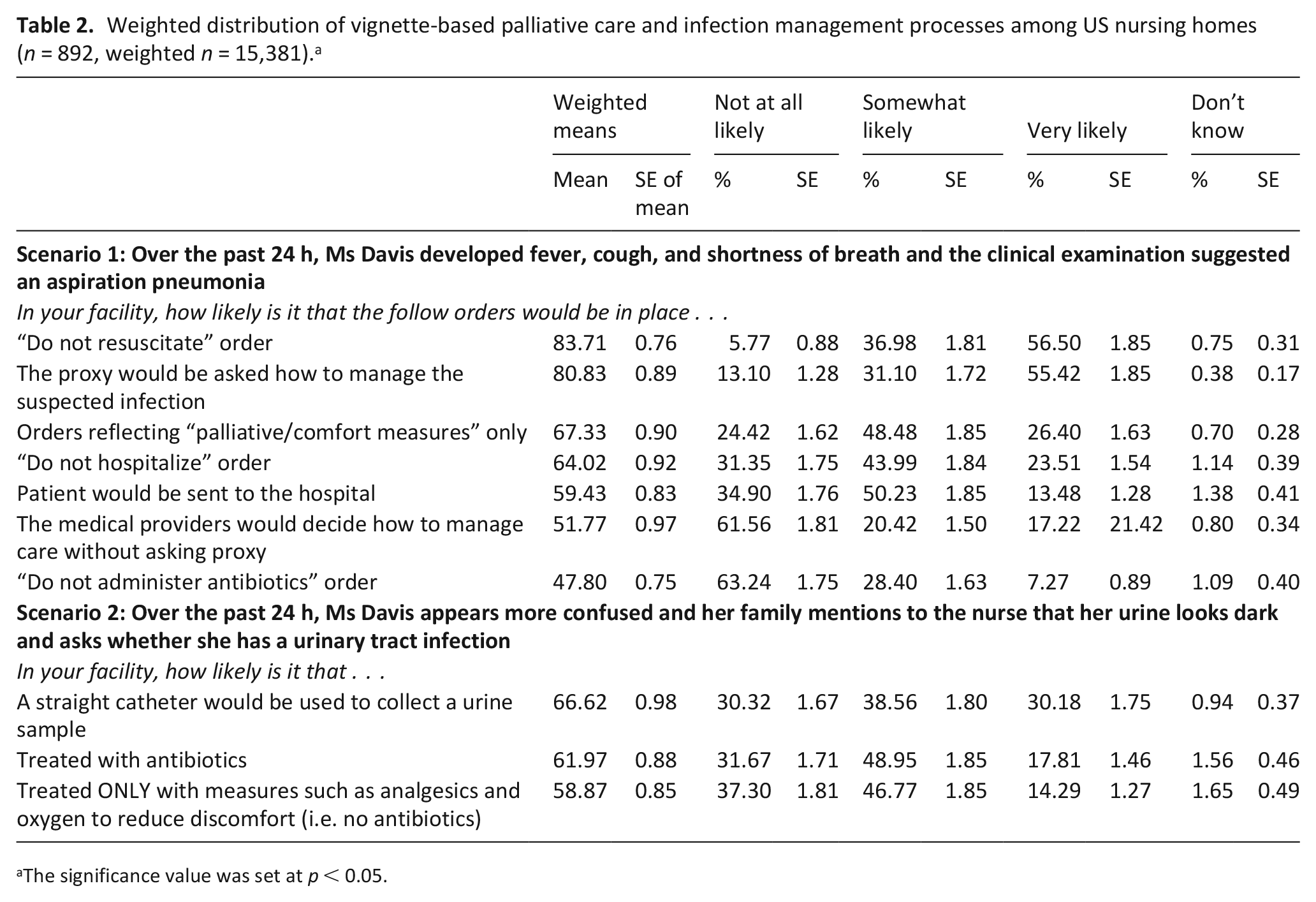
The significance value was set at p < 0.05.
In nursing homes across the country, if a UTI was suspected at the end of life, a straight catheter would be used to collect a urine sample and the patient would be treated with antibiotics over two-third of the time (µ = 66.62, SE = 0.98; µ = 61.97, SE = 0.88, respectively). Treating only with comfort measures and no antibiotics was less likely to occur.
Discussion
Main findings
Using a representative sample of US nursing homes, we described how nursing homes integrate infection management practices. To our knowledge, this is the first survey of infection management practices at end of life in US nursing home settings. We noted a majority of nursing homes almost always document care planning, including the religious or cultural practices that are deemed important for residents. Care discussions for infection treatment decisions most frequently occurred at the time of medical crisis or after the medical events (e.g. aspiration). Preferences were less frequently discussed during the advance care plan meetings, and least likely elicited upon nursing home admission.
What this paper adds
In general, preferences for infection management were almost always elicited, indicating a positive shift in nursing home care practices, away from a paternalistic to a more patient-centered and shared decision-making approach. However, there were important variations in terms of timing of when such preferences are elicited. Care discussions for infection treatment decisions most frequently occurred at the time of medical crisis or after the medical events. Preferences were less frequently discussed during the advance care plan meetings, and least likely elicited upon nursing home admission.
The variations in the timing of care discussion showed a gap in palliative care practice for a few important reasons. First, the timing of end-of-life care discussions is closely associated with the level of aggressiveness in the care options one elects. Previous studies show that when the care wishes are elicited in the face of medical crisis, there is an increased chance of electing highly aggressive and burdensome care options.73–75 Research suggests that hurried discussions around urgent medical needs bring added pressure to make prompt decisions, failing to allow dying patients to autonomously reflect on his or her care options and preferences. 76 Consequently, it is difficult to identify whether the elicited treatment decisions truly reflect the patient’s core values and desires for the care journey. Furthermore, those who complete advance directives within just a few weeks from their deaths (as opposed to years before) show higher rates of opting for the most aggressive interventions. 75
Second, as the number of older people grow, so will the occurrence of infections. Lack of US standards that encourage care providers to initiate end-of-life care discussions could be a reason why such conversations do not occur early on. There is an urgent need to implement a system where infection-related care options are routinely elicited and frequently revisited by care providers. A federally mandated repeated assessment of one’s end-of-life care preferences could act as a catalyst for a change.
In the vignette-based palliative care and infection management processes, more than half of our nursing home samples responded that “do not administer antibiotics” order will not be in place in the care of terminally ill patients. This suggests ample room for further improvement in the types of medical scenarios being discussed during end-of-life care discussions. In advance care planning, it is important to elicit patient preferences for both what to do and what not to do. That is, the care providers must be able to elicit specific treatment preferences to deliver or to withhold treatment interventions based on the patient’s or patient’s proxy expressed wishes. Medical decisions regarding treatment should align with the treatment’s intended goal as expressed by the patient’s preferences and values. 77 This critical, and yet sometimes missing, component of end-of-life care planning can lead to receipt of highly aggressive and burdensome interventions performed by default.
The pattern of antibiotic usage and antibiotic prescribing processes are fundamentally different in nursing homes than that of hospitals or clinics.12,78 That is, the decision to prescribe and forgo treatment with antibiotics in nursing homes are often made off-site,79,80 heavily influenced by nursing staff,81,82 and made with limited laboratory evaluation. 83 While antibiotic stewardship is regarded as a highly effective approach in reducing the misuse of antibiotics,32,35,84 in-depth knowledge on how to facilitate antibiotic stewardship in nursing home continues to remain a high priority. Previous studies show that drivers of nursing home antibiotic usage are the nursing staff and organizational commitment.38,78,81,85,86 Increased efforts to provide adequate trainings and educational opportunities for nursing staff can cultivate positive change in end-of-life care.
Limitations
There are limitations to this study. First, our survey was based on self-reported data from Directors of Nursing, which may have introduced social desirability bias and provided responses different from those of other facility staff. However, previous research has shown that the Director of Nursing is a key informant and the best person to provide an accurate account of a facility’s end-of-life care. 87 Second, there were differences in survey respondents and non-respondents on certain characteristics. 72 To account for these differences and improve generalizability in the United States, we developed population weights. Finally, with limited literature available on the integration of palliative care and infection management at end of life to date, we were unable to compare our findings with other research. However, we do evaluate our findings based on the broader context of palliative care and infection management.
Conclusion
Providing high-quality palliative care to long-term nursing home residents at the end of life is important to improve the quality of life of these residents. We found wide variation in practices and suboptimal care being reported across a study of nursing homes in the United States. Educating nursing home staff as well as the public on the importance of appropriate antibiotic usage and infection management into the provision of palliative care at the end of life is needed.
Footnotes
Author contributions
P.W.S. made a substantial contribution to the concept or design of the work. A.T., M.A., and L.V.E. made a substantial contribution to the acquisition, analysis, or interpretation of the data. A.T., M.A., L.V.E., and P.W.S. drafted the article. M.A., M.E.T., D.D.Q., and P.W.S. revised the drafted article critically for important intellectual content. A.T., M.A., L.V.E., M.E.T., D.D.Q., and P.W.S. approved the version to be published. M.E.T. and D.D.Q. have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Data management and sharing
Per instruction, statistical data files were submitted along with this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Columbia University Institutional Review Board (protocol no. IRB-AAAR1564, original approval date: 10 January 2017).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Study of Infection Management and Palliative Care at the End of Life (SIMP-EL, R01 NR013687), the Comparative and Cost-effectiveness Research Training for Nurse Scientists (CER2, T32 NR014205), and the Center for Improving Palliative Care for Vulnerable Adults with MCC (CIPC, P20 NR018072). A.T. is also funded by Jonas Center for Nursing and Veterans Health care.