
Abstract
Background:
Palliative care has been widely implemented in clinical practice for patients with cancer but is not routinely provided to people with chronic obstructive pulmonary disease.
Aim:
The study aims were to compare palliative care services, medications, life-sustaining interventions, place of death, symptom burden and health-related quality of life among chronic obstructive pulmonary disease and lung cancer populations.
Design:
Systematic review with meta-analysis (PROSPERO: CRD42019139425).
Data sources:
MEDLINE, EMBASE, PubMed, CINAHL and PsycINFO were searched for studies comparing palliative care, symptom burden or health-related quality of life among chronic obstructive pulmonary disease, lung cancer or populations with both conditions. Quality scores were assigned using the QualSyst tool.
Results:
Nineteen studies were included. There was significant heterogeneity in study design and sample size. A random effects meta-analysis (n = 3–7) determined that people with lung cancer had higher odds of receiving hospital (odds ratio: 9.95, 95% confidence interval: 6.37–15.55, p < 0.001) or home-based palliative care (8.79, 6.76–11.43, p < 0.001), opioids (4.76, 1.87–12.11, p = 0.001), sedatives (2.03, 1.78–2.32, p < 0.001) and dying at home (1.47, 1.14–1.89, p = 0.003) compared to people with chronic obstructive pulmonary disease. People with lung cancer had lower odds of receiving invasive ventilation (0.26, 0.22–0.32, p < 0.001), non-invasive ventilation (0.63, 0.44–0.89, p = 0.009), cardiopulmonary resuscitation (0.29, 0.18–0.47, p < 0.001) or dying at a nursing home/long-term care facility (0.32, 0.16–0.64, p < 0.001) than people with chronic obstructive pulmonary disease. Symptom burden and health-related quality of life were relatively similar between the two populations.
Conclusion:
People with chronic obstructive pulmonary disease receive less palliative measures at the end of life compared to people with lung cancer, despite a relatively similar symptom profile.
Palliative care is widely implemented into the treatment of cancer patients; however, it is less commonly used for people with chronic lung disease.
The disparity in palliative care among people with chronic obstructive pulmonary disease and those with lung cancer has not been previously compared in a comprehensive review.
People with chronic obstructive pulmonary disease and lung cancer both have poor health-related quality of life at the end of life and relatively similar symptom burden.
People with chronic obstructive pulmonary disease receive less palliative care services, medications for symptom management, but more life-sustaining interventions at the end of life compared to people with lung cancer
There is an unmet need for palliative care in the treatment of people with chronic obstructive pulmonary disease that needs to be addressed to relieve suffering at the end of life.
Introduction
Chronic obstructive pulmonary disease (COPD) and lung cancer are two of the leading causes of death, with approximately 3.04 and 1.71 million deaths worldwide in 2016, respectively. 1 Both COPD and lung cancer are associated with significant symptom burden and poor health-related quality of life at the end of life.2,3 People with either condition experience similar distressing symptoms near the end of life, notably dyspnea and pain.3–5 Due to the high mortality rates and significant symptom burden, it is important to consider palliative care in these populations.
Palliative care focuses on improving the quality of life for patients with advanced disease through the treatment of physical or psychological symptoms to reduce symptom burden at the end of life. 6 Palliative care is often provided to patients with end-stage lung cancer7,8 but services are lacking for patients with advanced COPD.9,10 Although the use of palliative care among those with advanced COPD remains low, evidence suggests it is increasing over time. 11 Yet notable barriers to the provision of palliative care in COPD still exist. Lack of clarity on when to initiate palliative care is largely due to the inability to predict COPD disease progression and unclear prognosis. 12 Although numerous prognostic models do exist, only a small number of models have been externally validated and their clinical utility remains to be established.13,14 People with advanced COPD can remain stable for extended periods of time or experience frequent exacerbations 12 and cause of death is not limited to respiratory failure or pneumonia but is often the result of common, related comorbidities including cancer or consequence of the disease such as heart failure. 15 As a result of the difficulty in determining prognosis, COPD patients are more likely to receive life-sustaining measures prior to death, such as cardiopulmonary resuscitation (CPR) or mechanical ventilation, than they are to receive palliative care. 16 As patients with advanced stage lung cancer follow a more predictable timeline of disease progression compared to people with COPD, it is recommended that palliative care be initiated early in the treatment of people with lung cancer, accompanying curative measures. 8
Due to the symptom overlap, high prevalence and mortality rates, it is important to evaluate end-of-life care in patients with COPD using lung cancer as a reference standard. To date, no comprehensive review has been performed to evaluate this comparison. Thus, the primary objective of this review was to compare the receipt of formal palliative care and provision of medications for symptom management, between populations of advanced COPD patients, end-stage lung cancer patients or those with end-stage lung cancer and co-existing COPD. Secondary objectives included comparisons of life-sustaining measures, place of death, symptom burden and health-related quality of life.
Methods
Databases
Searches of electronic databases (MEDLINE, EMBASE, PubMed, CINAHL and PsycINFO) were performed on 23–24 April 2019 using terminology related to ‘chronic obstructive pulmonary disease’ AND ‘lung cancer’ AND ‘palliative care’. Common synonyms for palliative care included; terminal, hospice, supportive, end of life, advance care planning, pain or symptom management. The detailed search strategy for MEDLINE is included in the Supplementary Material. The combined terminology was specifically adjusted for each database searched. References from related reviews were hand-searched for any missed data sources along with the removal of duplicates prior to the screening process. The search was updated on 24 October 2019 and the protocol was registered on PROSPERO (ID: CRD42019139425).
Inclusion and exclusion criteria
Two researchers (S.J.B. and L.E.) individually reviewed abstracts and full-text articles for inclusion. Primary studies (retrospective or prospective cohort studies or cross-sectional studies), which compared measures of palliative care services (including medications), place of death, life-sustaining measures, symptom burden or Health-related quality of life between at least two of the following populations with a diagnosis of COPD, lung cancer, or lung cancer with co-existing COPD, were included. Intervention or qualitative studies were excluded. Studies that did not separate lung cancer from other cancer types were also excluded. Studies, which included individuals with lung metastases as a result of another primary cancer (e.g. breast cancer) were excluded. If studies examined a population with chronic lung disease, at least 80% of participants needed to have COPD in order to be included. Only English language studies were included in this review due to feasibility reasons.
Quality assessment
The QualSyst tool (Standard Quality Assessment Criteria for Evaluating Primary Research Papers), developed by the Alberta Heritage Foundation for Medical Research, 17 was used by two researchers (S.J.B and L.E.) to independently assess the quality of each study. For each study, this tool assesses the population, sample size, diagnostic methods, study design, data collection and the statistical analyses used and whether each is appropriate. For each question, studies are scored on the degree to which they met the criteria, with yes (2 points), partial (1 point), no (0 points) or not applicable. Studies were scored as partial for question two regarding comparison groups if it was unclear whether the COPD and lung cancer groups were mutually exclusive. Studies were also scored as partial for question three regarding subject characteristics if insufficient information was reported to characterize the population. Studies that reported spirometry and/or GOLD staging for COPD and also reported staging of lung cancer were given two points for question two. The total score was used to categorize risk of bias as high (<79%), moderate (80%–89%) or low (>90%). Any discrepancies between the researchers were resolved by a third author (D.B.) to reach a consensus.
Data extraction and analysis
Data was extracted independently by two reviewers (S.J.B. and L.E.) and included information on study details, demographics and outcome measures for each study. Study details included the study design, study period, inclusion and exclusion criteria and diagnostic methods. For each population group, the sample size was recorded along with demographics, including: mean age, number of males and females. Additional data were extracted on palliative care services, medications, place of death, life-sustaining measures, symptoms and health-related quality of life for each population group.
Data were analysed using Review Manager 5 and MetaXL. Odds ratios and pooled prevalence were calculated using a random effects meta-analysis and the Mantel–Haenszel method. For all analyses, alpha was set at 0.05.
Results
Search results
As outlined in Figure 1, a total of 1954 records were identified using the search criteria. Abstracts were excluded (n = 978), if it was clear they did not compare a COPD and lung cancer population; were case studies or qualitative studies; or articles on palliation of lung cancer via surgery or radiation. A total of 82 full-text articles were screened and 19 studies met the inclusion criteria. Two studies10,18 utilized the same data sets but reported on different outcomes. All studies either reported measures within the last year of life, during a final hospitalization, or were conducted in a population with advanced COPD and end-stage lung cancer.
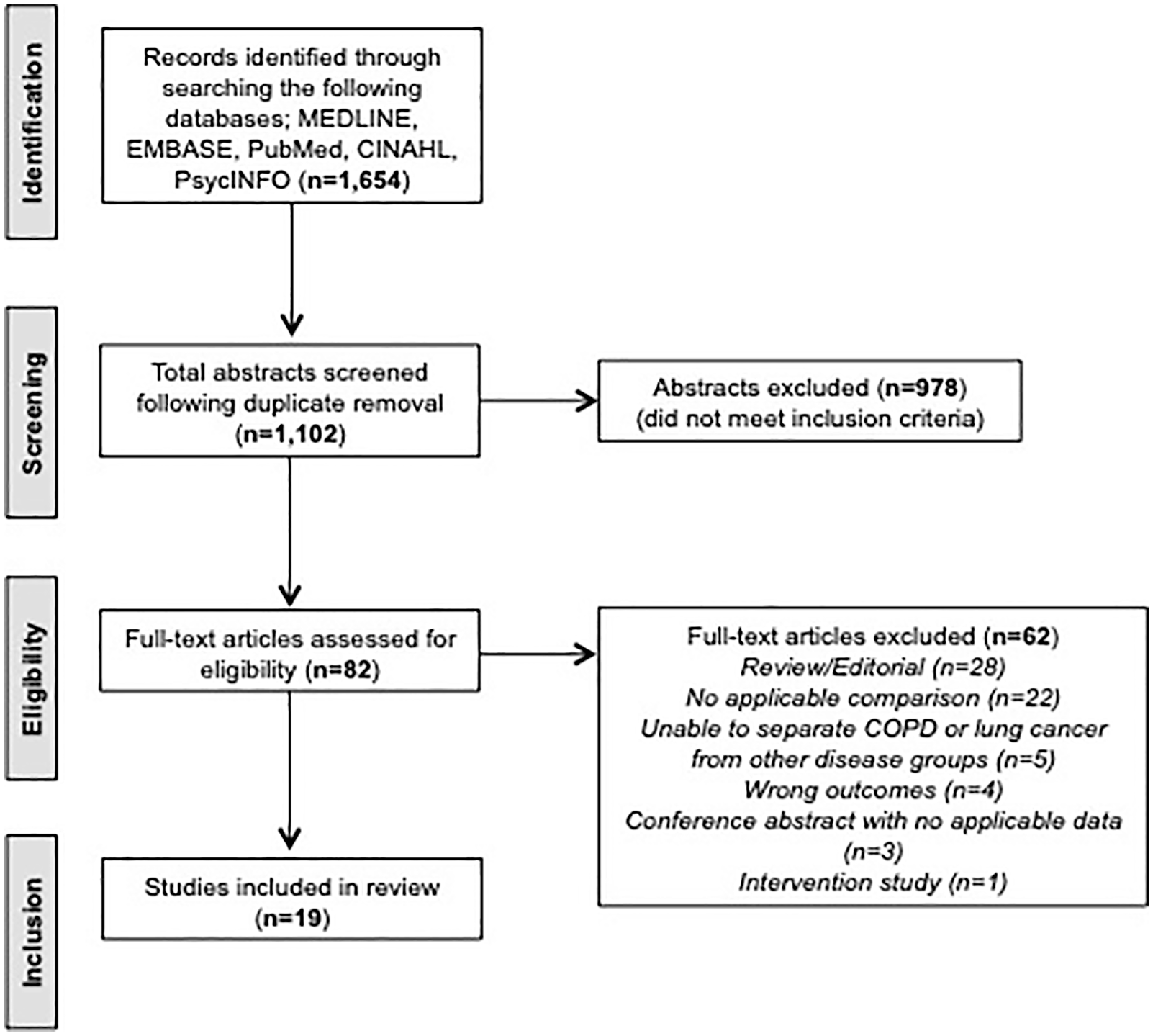
PRISMA flow diagram of study selection.
Eleven studies2,3,5,18–25 compared a population with lung cancer to a population with COPD and consisted of retrospective studies of deceased populations (n = 5), cross-sectional studies (n = 3), prospective cohort studies (n = 2) and post-bereavement interviews with caregivers (n = 1). Three retrospective studies compared a population with COPD to a population with lung cancer of which a proportion (17%–42%) also had co-existing COPD.26–28 Two studies compared a population with COPD to a population with both lung cancer and co-existing COPD with one retrospective 29 and one prospective design. 30 Three studies10,31,32 compared across three disease groups: COPD, lung cancer, both COPD and lung cancer. All three studies were retrospective and utilized health administrative data. Study characteristics are summarized in Table 1. The majority of studies reported data collected in the past 15–20 years, with eight studies reporting on data exclusively collected in the past 10 years. The majority of studies were conducted in Europe (n = 8) or North America (n = 5). Few studies were conducted in Asia (n = 3) and only one study was conducted in Australia. All studies were conducted in one country, with the exception of the study by Cohen et al. 21 which compared place of death among 14 countries.
Overview of included studies.
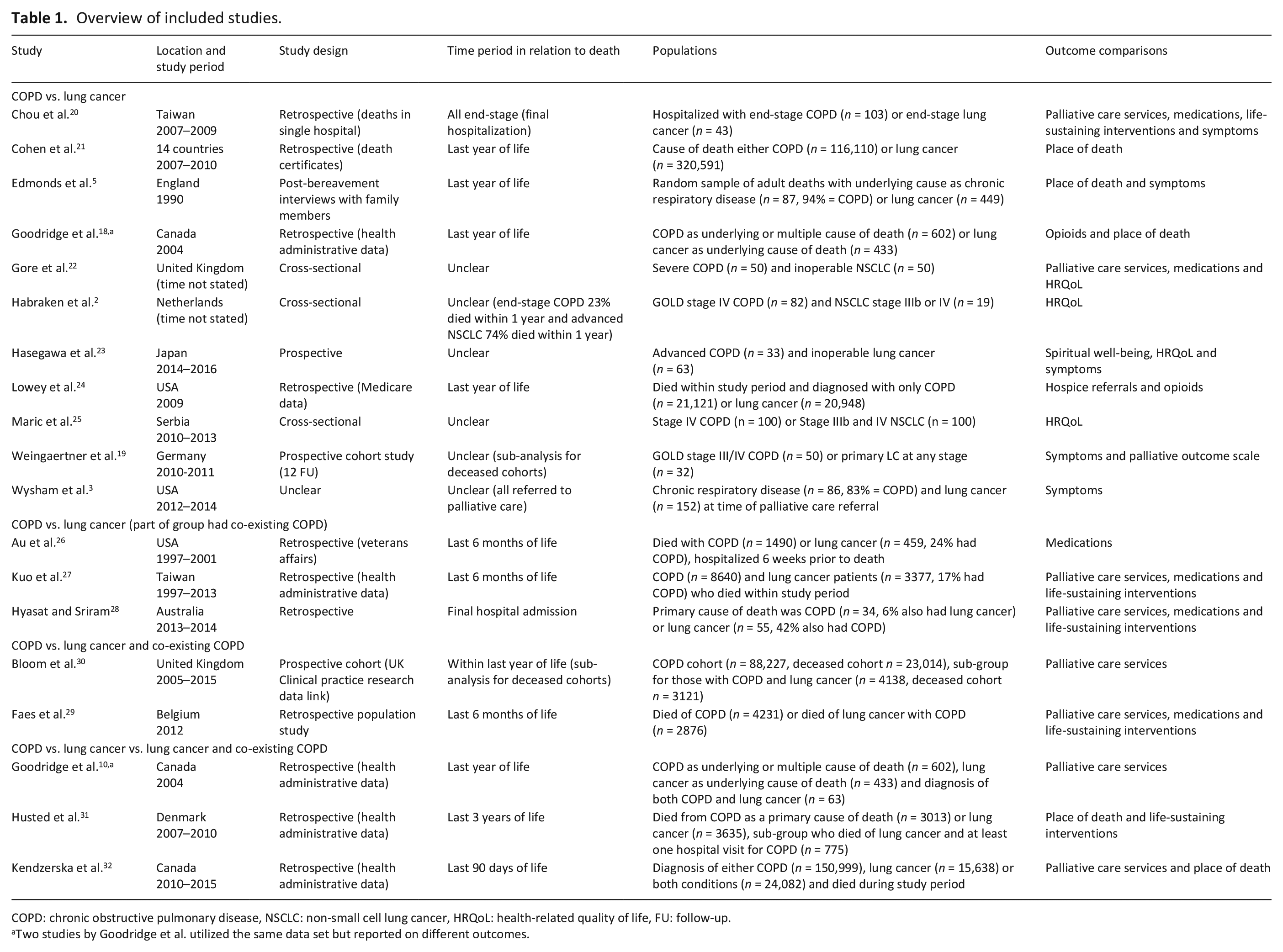
COPD: chronic obstructive pulmonary disease, NSCLC: non-small cell lung cancer, HRQoL: health-related quality of life, FU: follow-up.
Two studies by Goodridge et al. utilized the same data set but reported on different outcomes.
Results of the quality assessments are provided in Table 2. There were insufficient number of studies (n < 3) for all outcomes with the exception of palliative home care to compare populations of co-existing COPD and lung cancer to either disease alone. Retrospective and prospective cohort studies and cross-sectional studies were included. Five studies had low risk of bias, while the majority of studies were of moderate quality as there were some concerns, often due to insufficient detail regarding participant characteristics, results or small sample size. A number of studies were unclear as to whether the lung cancer group also had co-existing COPD (Table 1).
Quality assessment.
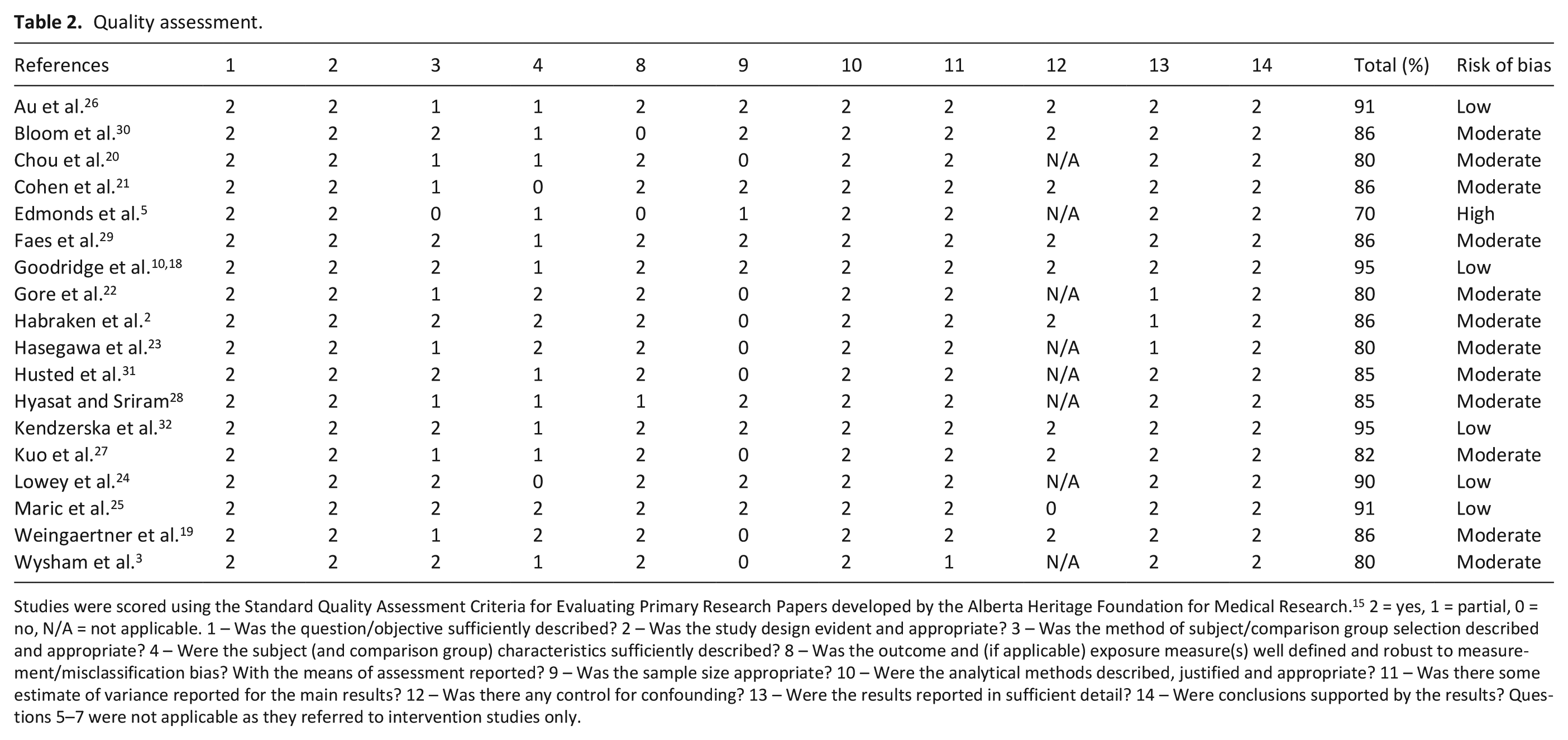
Studies were scored using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers developed by the Alberta Heritage Foundation for Medical Research. 15 2 = yes, 1 = partial, 0 = no, N/A = not applicable. 1 – Was the question/objective sufficiently described? 2 – Was the study design evident and appropriate? 3 – Was the method of subject/comparison group selection described and appropriate? 4 – Were the subject (and comparison group) characteristics sufficiently described? 8 – Was the outcome and (if applicable) exposure measure(s) well defined and robust to measurement/misclassification bias? With the means of assessment reported? 9 – Was the sample size appropriate? 10 – Were the analytical methods described, justified and appropriate? 11 – Was there some estimate of variance reported for the main results? 12 – Was there any control for confounding? 13 – Were the results reported in sufficient detail? 14 – Were conclusions supported by the results? Questions 5–7 were not applicable as they referred to intervention studies only.
Receipt of formal palliative care
Very few patients with COPD received formal palliative care, as either inpatients in hospital, home-based or hospice care (Figure 2). People with lung cancer had higher odds of receiving palliative care as inpatients in hospital compared to those with COPD (odds ratio (OR) = 9.95, 95% confidence interval (CI): 6.37–15.55, p < 0.001, n = 4) (Figure 2(a)). A sensitivity analysis excluding the single study reporting palliative care unit admissions during a final hospitalization revealed a similar result in favour of lung cancer (OR = 9.65, 95% CI: 6.10–15.26, p < 0.001, n = 3). Rates of palliative home care were also low in COPD populations (Figure 2(b)). People with lung cancer had higher odds of receiving palliative home care than people with COPD within the last year of life (OR = 8.79, 95% CI: 6.76–11.43, p < 0.001, n = 4) (Figure 2(b)). Four studies reported higher palliative home care rates among people with co-existing lung cancer and COPD when compared to people with COPD alone (OR = 8.79, 95% CI: 6.76–11.43, p < 0.001, n = 4). Heterogeneity in the meta-analyses was high (I2 = 87%–90%) due to the variability in sample size. Two studies specifically reported on hospice use.20,24 Lowey et al. 24 reported 40.8% of people with COPD and 67.7% of people with lung cancer using this service (p value not provided). In the study by Chou et al., 20 people with lung cancer were more likely to be referred to hospice during their final hospitalization compared to people with COPD (69.8% vs. 21.4%, p < 0.001). The duration of days in hospice was similar (p = 0.553) for people with COPD (average length of stay (LOS) 9.5 days (interquartile range (IQR): 4.0, 15.0)) and people with lung cancer (average LOS 8.0 days (IQR: 4.0, 14.0)).
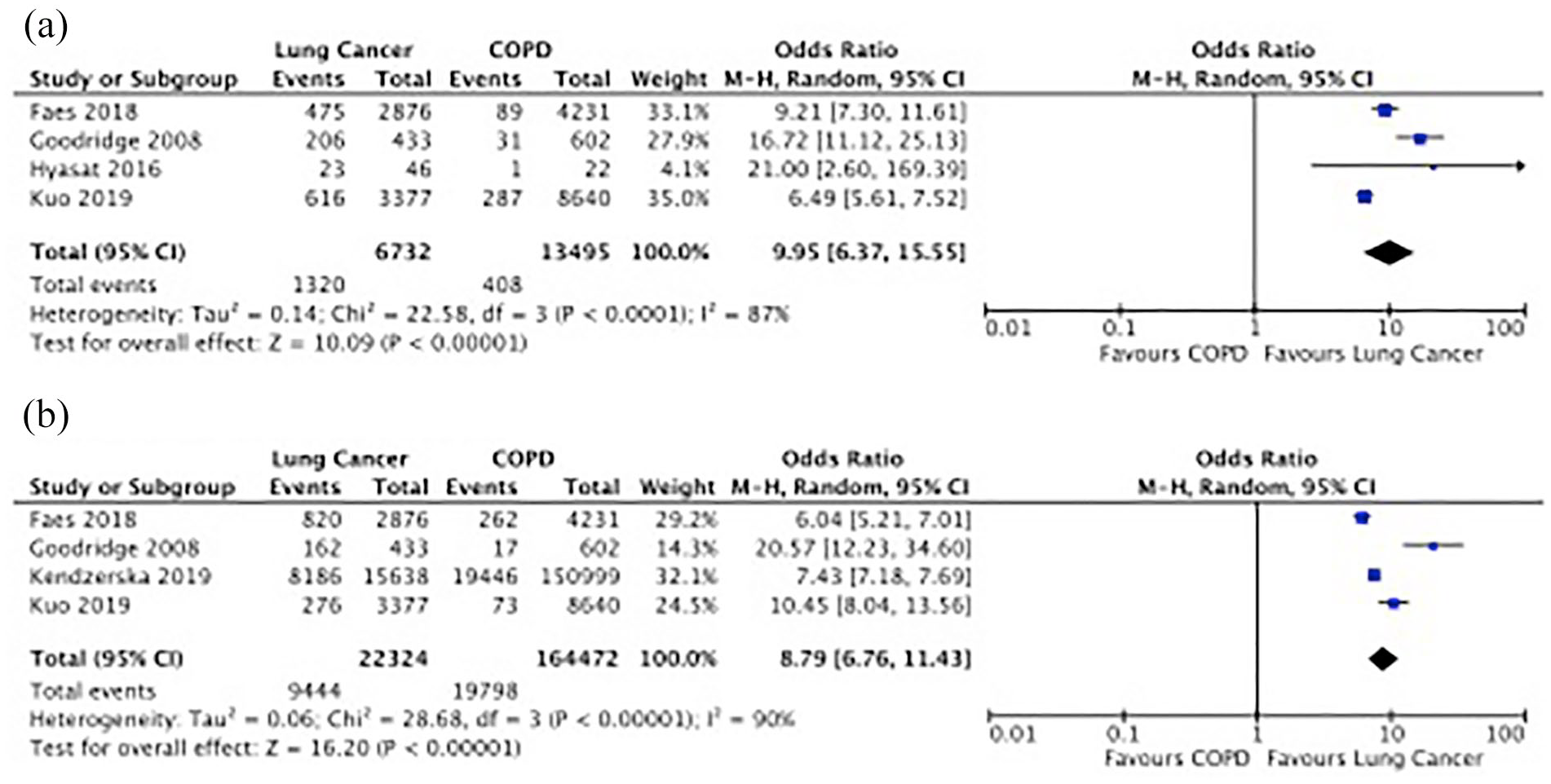
Meta-analysis of palliative care services: (a) hospital-based palliative care and (b) home-based palliative care.
Two studies22,30 did not specify the type of palliative care provided and thus were unable to be included in the meta-analyses. Gore et al. 22 reported that 30% of patients with non-small cell lung cancer (NSCLC) received assistance from a hospice centre or specialist nurse, while no patients with COPD received these services. A population study based out of the United Kingdom by Bloom et al. 30 reported only 5.8% of people with COPD received palliative care support compared to 50% for people with both lung cancer and COPD. When the authors restricted the analysis to only the deceased cohort, there was an uptake of palliative care for people with COPD (16.7%) but this still fell below the rates for people with both lung cancer and COPD (56.5%).
Two studies27,29 reported on the length of stay in inpatient palliative care units. Kuo et al. 27 found no significant difference in LOS for people with COPD (15.9 ± 16.1 days) compared to people with lung cancer in Taiwan (15.3 ± 15.9 days). Faes et al. 29 compared inpatient palliative care unit Length of stay in Belgium among those dying of COPD alone (mean LOS 6.5 days, 95% CI: 5.3–7.7), dying of COPD with lung cancer (mean LOS 8.5 days, 95% CI: 7.8–9.1) or dying of COPD with cardiovascular disease (mean Length of stay 5.4 days, 95% CI: 4.4–6.4). There was a significant difference among the three disease groups (p < 0.001).
Medications
Medications at the end of life were compared in seven studies, with two studies reporting medications in the last year of life,18,24 three in the last 6 months of life26,27,33 and two during a final hospitalization.20,28 All seven studies compared opioids, with four studies also specifying morphine as the type of opioid.18,20,24,29 The pooled rate of opioid prescriptions in COPD was 36.5% (95% CI: 28.4–45.0) and in lung cancer, regardless of co-existing COPD, was 83.6% (95% CI: 73.3–91.9). People with lung cancer had 4.76 times higher odds of receiving opioids compared to people with COPD (95% CI: 1.873–12.11, p < 0.001, n = 7) (Figure 4(a)). The lowest ORs were observed in two studies conducted in the United States using Veterans Affairs 26 or Medicare data. 24 The largest difference in opioid prescriptions among those with lung cancer and COPD were observed in Taiwan,20,27 highlighting the variability by country contributing to significant heterogeneity in the meta-analyses (I2 = 100%). There were an insufficient number of studies with mutually exclusive groups to comment on the role of co-existing COPD on opioid prescriptions in people with lung cancer. As rates of medications could be higher during a final hospitalization, we performed a sensitivity analysis, which only included studies within the last year of life. Excluding studies reporting opioid prescriptions during the final hospital admission revealed an OR 3.60 (95% CI: 1.22–10.64, p = 0.02, n = 4) in favour of lung cancer. People with lung cancer were also had higher odds of receiving morphine compared to people with COPD (OR = 4.61, 95% CI: 1.36–1.57, p = 0.002, n = 4) (Figure 3(b)) with 7.3% (95% CI: 2.1–14.9) of people with COPD and 14.3% (95% CI: 0–62.7) of people with lung cancer receiving morphine. Excluding the single study reporting morphine prescription during final hospitalization revealed an OR of 3.38 (95% CI: 1.15–9.90, p = 0.03, n = 3) in favour of lung cancer. These results are also confounded by significant heterogeneity (I2 = 99%). Four studies compared prescriptions of sedatives20,26,27,29 with two studies specifically comparing benzodiazepines.26,27 People with lung cancer had higher odds of receiving sedatives than people with COPD (OR = 2.03, 95% CI: 1.78–2.32, p < 0.001, n = 4) (Figure 3(c)). Sedatives were prescribed to 48.2% (95% CI: 26.5–70.3) of people with COPD and 63.8% (95% CI: 47.2–78.9) of people with lung cancer. Excluding the single study during final hospitalization had minimal change on the meta-analysis results (OR = 2.01, 95% CI: 1.75–2.31, p < 0.001, n = 3). There was less heterogeneity in sedatives prescriptions among the included studies reflecting similar rates in USA, Belgium and Taiwan. Only one study compared the use of anti-depressants in the last 6 months of life in a population study using data collected at Veterans Affairs medical centres. 26 There was no reported difference in outpatient selective serotonin reuptake inhibitors (SSRIs) between those with COPD (18%) and a population of lung cancer where 24% had co-existing COPD (18%) (p = 0.89).
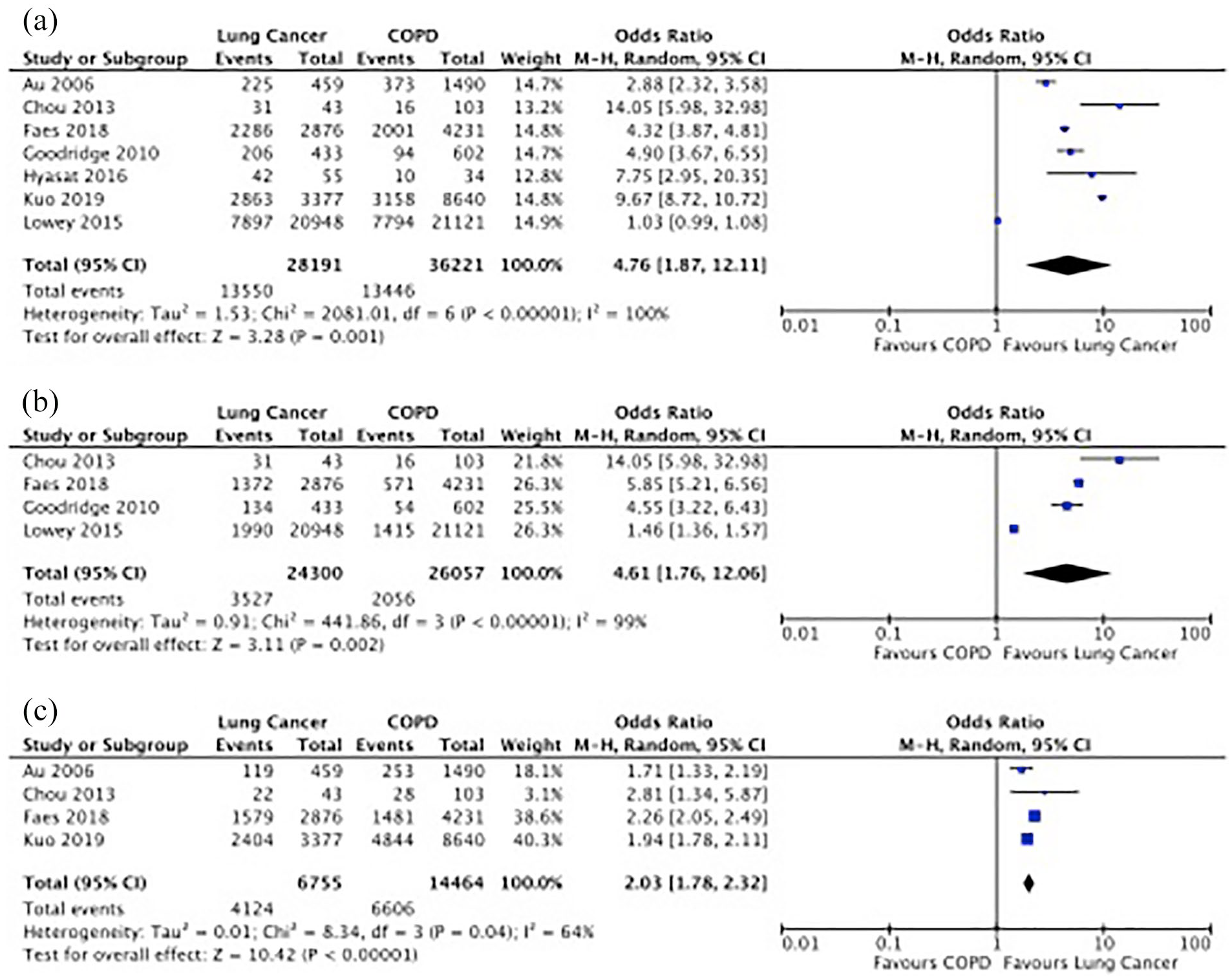
Meta-analysis of medications at the end of life: (a) opioids, (b) morphine and (c) sedatives.
Life-sustaining interventions
Overall, people with COPD had higher odds of receiving life-sustaining interventions compared to people with lung cancer (Figure 4). People with lung cancer had lower odds of receiving invasive ventilation while hospitalized within the last 6 months of life or during their final hospitalization, compared to people with COPD (OR = 0.26, 95% CI: 0.22–0.32, p < 0.001, n = 3) (Figure 4(a)). People with lung cancer also had lower odds of receiving non-invasive ventilation (OR = 0.63, 95% CI: 0.44–0.89, p = 0.009, n = 3) (Figure 4(b)) and CPR compared to people with COPD (OR: 0.29, 95% CI: 0.18–0.47, p < 0.001, n = 3) (Figure 4(c)). The small sample sizes in the studies by Hyasat and Sriram 28 and Chou et al. 20 contributed to heterogeneity in these meta-analyses (I2 = 65%–91%). Information on do not resuscitate (DNR) orders were only available for two studies. Chou et al. 34 reported 61.2% of COPD patients and 97.7% of lung cancer patients had DNR consent during their final hospitalization, with CPR performed on 40.8% of COPD and 9.3% of lung cancer patients. At the time of initial palliative care consultation, Wysham et al. 3 found more patients with chronic respiratory disease had DNR orders compared to lung cancer (62% vs. 32%).
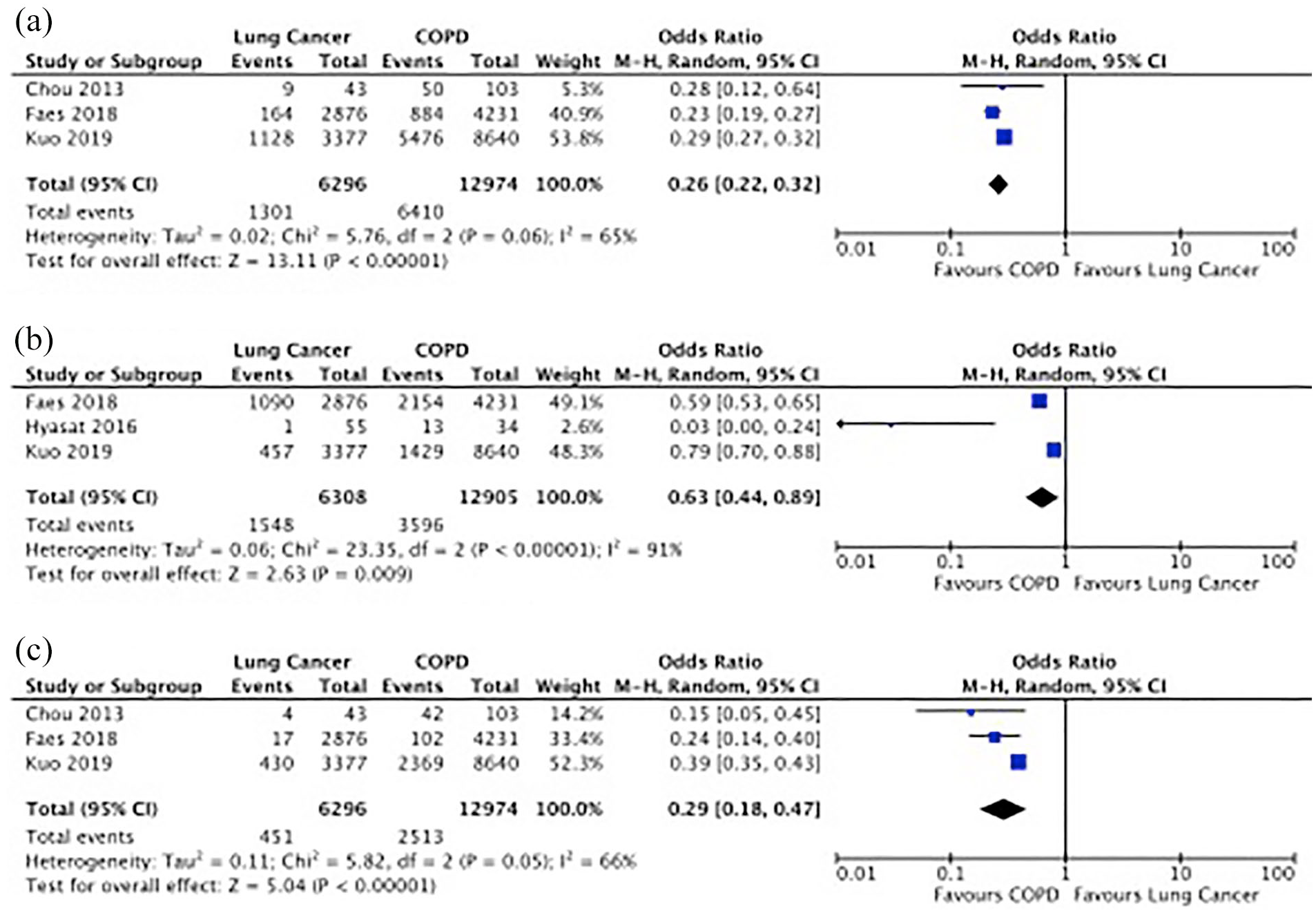
Meta-analysis of life-sustaining measures: (a) invasive ventilation, (b) non-invasive ventilation and (c) cardiopulmonary resuscitation (CPR).
Place of death
There was no significant difference between COPD and lung cancer in hospital deaths (OR = 0.93, 95% CI: 0.83–1.03, p = 0.16, n = 5) (Figure 5(a)). People with lung cancer had higher odds of dying at home (OR: 1.47, 95% CI: 1.14–1.89, p = 0.003, n = 5) compared to people with COPD (Figure 5(b)). People with lung cancer had lower odds of dying in a nursing home or long-term care facility compared to people with COPD (OR: 0.32, 95% CI: 0.16–0.64, p < 0.001, n = 4) (Figure 5(b) and (c)). Heterogeneity was high due to variability in sample size and location (I2 = 95%–100%). The highest reported OR for home death was in the United Kingdom; however, these data are dated (1990) compared to the rest of the studies included in the meta-analyses (data collection dates ranged from 2004 to 2015). Two studies5,21 compared deaths in hospice settings, with a higher percentage of lung cancer deaths occurring in hospice (10.8% and 14%, compared to 1.5% and 0% for COPD). Husted et al. 31 reported deaths at a known address (hospice or relatives home) as 4.9% for COPD, 8.8% for lung cancer and 9.8% for people with lung cancer and COPD.
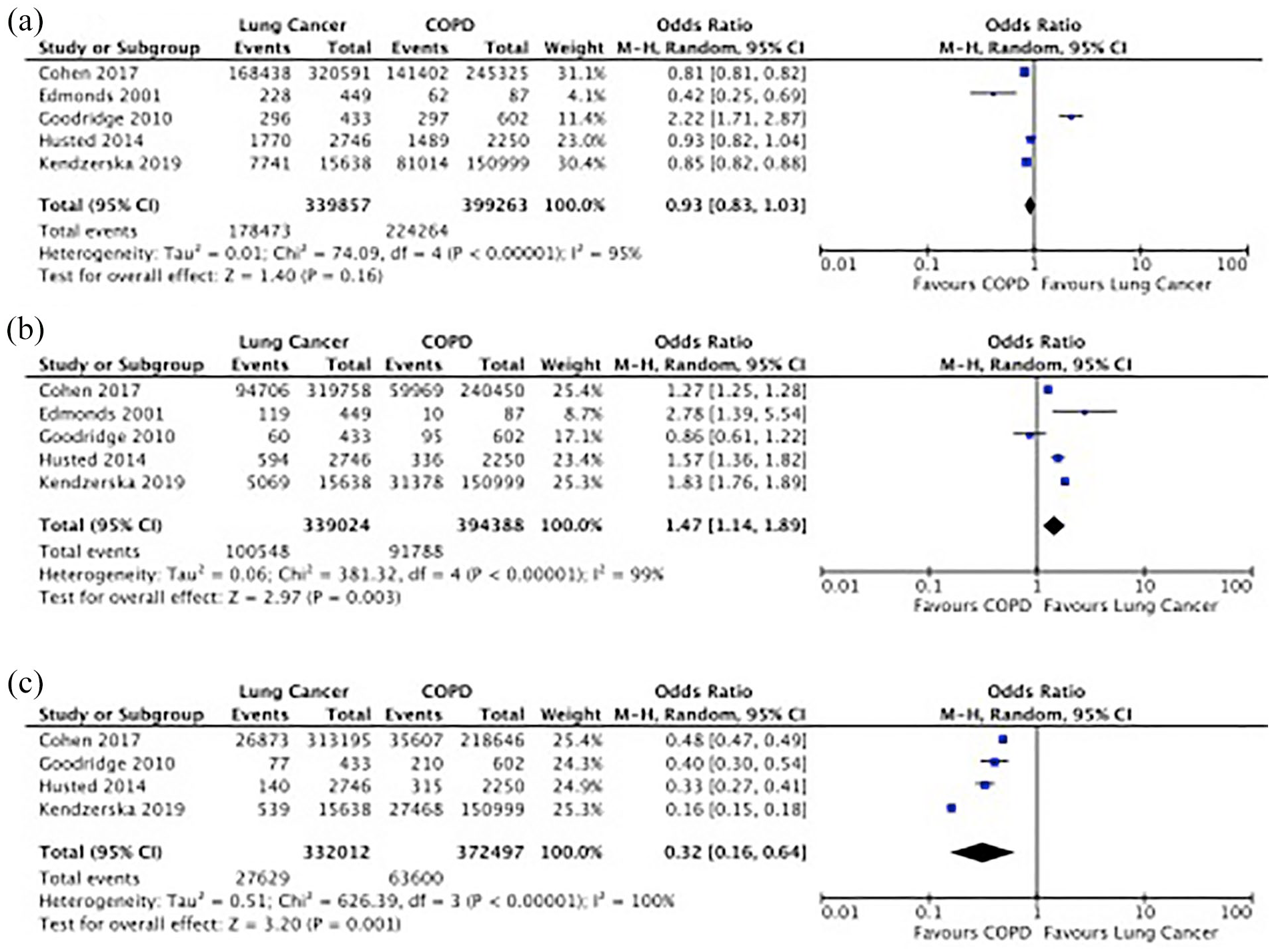
Meta-analysis of place of death: (a) hospital death, (b) home death and (c) nursing home or long-term care facility death.
Symptom burden and HRQoL
Few studies compared symptom burden or health-related quality of life at the end of life between COPD and lung cancer populations. Due to variability in study design, inconsistencies of time of measurement in relation to death and whether participants received palliative care, we were unable to combine results in a meta-analysis.
Only two studies5,20 compared the total number of symptoms experienced at the end of life in deceased populations with COPD or lung cancer. People with COPD (median 10.0, IQR: 8–13) or lung cancer (median 10.0, IQR: 8–12) in hospice reported a similar number of symptoms (p = 0.666). In post-bereavement interviews, caregivers reported an average of 7.1 ± 2.9 symptoms for people with chronic lung disease (94% of whom had COPD) and 6.9 ± 2.9 symptoms on average for people with lung cancer in the final year of life (p = 0.5). 5
The most common symptoms to be compared among those with advanced COPD or lung cancer were pain and dyspnea. The lowest prevalence of pain (6.1% and 20.6%) and dyspnea (57.6% and 11.1%) in stage III/IV COPD and inoperable lung cancer patients, respectively, provided no information on the time of measurement in relation to death. 23 Wysham et al. 3 reported no significant difference in the number of patients reporting pain (COPD = 38.0%, lung cancer = 50.7%) and dyspnea (COPD = 53.5%, lung cancer = 40.8%) in a sample of patients who were receiving palliative care. Edmonds et al. 5 compared pain and dyspnea in the final year and final week of life through post-bereavement interviews with caregivers and found no significant difference (p > 0.05) in the prevalence of pain between those with lung cancer and those with chronic lung disease (94% of whom had COPD). People with chronic lung disease were more likely to report breathlessness in the final year (COPD = 94%, lung cancer = 78%, p < 0.0001) and final week of life (COPD = 91%, lung cancer = 69%, p < 0.001). 5
Three studies3,5,23 reported on several symptoms beyond pain or dyspnea, including pain, weakness, fatigue, cough, insomnia and gastrointestinal symptoms among others. There was no significant difference in prevalence or severity between those with COPD or lung cancer for majority of symptoms. Wysham et al. 3 found a higher percentage of lung cancer patients reported insomnia and nausea compared to those with COPD (p < 0.005). In post-bereavement interviews, Edmonds et al. 5 found a higher percentage of lung cancer patients experienced anorexia or constipation during the final year of life compared to those with chronic lung disease. During the final week of life, more lung cancer patients experienced constipation, and cough was more prevalent in chronic lung disease patients. 5 The majority of studies reporting symptoms were limited by small sample size and few commented on symptom severity. There was significant variation in symptom prevalence among the included studies, which is likely a result of the variable study designs and inconsistency in time of data collection to the end of life.
Four studies compared health-related quality of life with three studies using the 36-item Short Form Health Survey (SF-36)2,22,25 and one study using the McGill Quality of Life Questionnaire. 23 Gore et al. 22 reported significantly lower scores for patients with severe COPD, reflecting worse health-related quality of life, in all domains except physical and emotional functioning. Habraken et al. 2 reported similar health-related quality of life between those with COPD or lung cancer, with the COPD group reporting significantly lower scores in physical functioning and general health perceptions. Maric et al. 25 found COPD patients scored significantly lower in all SF-36 domains except for pain. Hasegawa et al. 23 reported similar scores in the McGill Quality of Life questionnaire but those with COPD had a better psychological state and lung cancer patients had a better support state.
Discussion
Main findings
This review highlights the significant disparity in end-of-life care for people with COPD or lung cancer. People with lung cancer receive substantially more formal palliative care services, medications for symptom management and less life-sustaining measures compared to people with COPD. Both populations experience distressing symptoms, with a similar prevalence of pain. There is limited evidence suggesting more people with COPD experience dyspnea and more people with lung cancer experience gastrointestinal symptoms. Regardless, there is an unmet need for palliative care among people with COPD that should be addressed in order to ease suffering at the end of life.
The uncertain disease trajectory of COPD is often cited as a barrier to initiating palliative care. In addition, people with COPD may not fully understand the progressive nature of their disease and thus not be aware of the need for discussions regarding palliative care. 35 The high prevalence of comorbidities, particularly underlying cardiovascular disease36,37 also contribute to an unclear prognosis as COPD itself is not always the underlying cause of death. In fact, cardiovascular disease, pulmonary infection, pulmonary embolism and lung cancer account for two-thirds of deaths in COPD populations compared to one-third caused by respiratory failure. 15 The inability to predict prognosis coincides with low rates of formal palliative care services for people with COPD reported in this review. A recent systematic review by Smith et al. 13 identified a number of variables associated with all-cause mortality in COPD, such as measures of disease severity, breathlessness, exacerbation frequency, frailty, comorbidities and long-term oxygen therapy but found insufficient evidence to recommend a prognostic scoring system. It is also important to note that prognostic factors may differ for patients with frequent hospitalizations and those with stable disease. For community-dwelling older adults with COPD, consideration of the severity of dyspnea, health status and exercise capacity are also recommended in addition to clinical tests such as arterial blood gases and spirometry. 38 A reliable model to predict mortality would assist with improving proper initiation of palliative care for people with COPD; however, a palliative care approach to symptom management could still be integrated early along with active treatment. Across all types of disease, when comparing all deaths, regardless of disease type, a Canadian population-based study found early integration of palliative care improves outcomes, lowers emergency department visits and ICU admissions in the final month of life. 39 Early integration of palliative care in lung cancer has been shown to reduce psychological and physical symptom severity, and improve quality of life. 40 Based on the comparable symptom burden, a similar approach could be beneficial for COPD patients.
People with COPD have significant healthcare utilization at the end of life, 41 with one study reporting $4000 (US dollars) higher costs for patients with COPD compared to lung cancer, largely due to invasive measures and ICU admissions. 26 In the three studies identified in this review, all reported higher rates of invasive and non-invasive ventilation and lower rates of palliative care unit admissions in people with COPD. It is important to note that non-invasive ventilation was recently recommended for the long-term management of chronic hypercapnic COPD patients. 42 Higher rates of non-invasive ventilation in people with COPD noted in this review may be reflective of this practice, although data collection preceded 2015 in all cases. It has been proposed that implementing a palliative approach in the treatment of COPD could reduce the use of intensive-care resources and subsequently reduce costs to the healthcare system. A review of the cost-effectiveness of palliative care found an overall trend of lower costs in the palliative group compared to controls, regardless of disease. 43 The limited availability of palliative care resources varies by country and is a critical factor affecting the quality of end-of-life care and rates of palliative care across all types of disease. We found people with COPD were more likely to die in long-term care facilities and people with lung cancer were more likely to die at home. This is consistent with higher rates of palliative care in people with lung cancer as it has been shown patients receiving palliative care are more likely to die at home. 39
Medications for pain and sedation are hallmarks of a palliative approach to symptom management. Despite several studies reporting a similar symptom burden, people with lung cancer still receive more opioids and sedatives within the last year of life than people with COPD. We did not identify any studies that measured medications and symptoms within the same population. The interpretation of opioid use is limited without knowledge of the indication for opioids as they can be used to treat dyspnea as well as pain. 44 It would be expected that opioids would be provided at similar rates to patients with advanced lung cancer and end-stage COPD based on comparable levels of dyspnea and pain.3,5,20 We found people with lung cancer were still over four times more likely to be treated with opioids. Large-scale studies that combine patient level data on symptoms, causes of pain, location or type of pain as well as medication usage and palliative care services would offer more insight into these findings.
A previous systematic review by our group reported people with COPD are over six times more likely to develop lung cancer than those without COPD. 45 The two conditions often co-exist, yet there is little information on end-of-life care for people suffering from both conditions. We only identified four studies10,29–31 which compared end-of-life care among mutually exclusive populations of those with both conditions and those with COPD only. An additional three studies26–28 included people with co-existing COPD (ranging from 17% to 42%) as part of the lung cancer cohort. In all cases, people with lung cancer and co-existing COPD received more palliative care services, medications for symptom management and less life-sustaining interventions than people with COPD alone; however, variability in available data prevented a meta-analysis for people with co-existing disease. Only Goodridge et al. 10 compared palliative care services among all three disease groups (lung cancer, COPD, lung cancer and COPD) and found rates were significantly higher for those with lung cancer and COPD compared to those with COPD alone, but were not significantly different compared to those with lung cancer alone. Further exploration into the role of co-existing COPD on end-of-life care in lung cancer patients is warranted.
Limitations
We acknowledge possible publication bias as only studies published in English were included in this review. The majority of the included studies were conducted in North America, Asia or Europe, limiting the generalizability of the results. The comparison across different regions contributes to the high level of heterogeneity as palliative care guidelines and availability of formal palliative care services vary by country. We included all studies that either specified the timing of data collection in relation to death (i.e. last year of life) or included people with advanced COPD or end-stage lung cancer, who would benefit from palliative care. The variability in time period in relation to death among included studies also contributes to the high level of heterogeneity. In addition, only a small number of studies reported similar measures that could be included in the meta-analysis (n = 3–7). The small number of events in the COPD group also introduces directional bias in the meta-analysis using the Mantel–Haenszel method to combine ORs. Thus, the meta-analysis results should be interpreted with caution and require further exploration. An additional limitation is the focus on formal palliative care services offered through hospital, home or hospice care. We are unable to comment on advanced-care planning directives or interventions related to the psychological needs of patients, which are also integral to quality palliative care. Finally, the quality assessment tool we utilized lacks a consensus on presentation of results. We chose to present both percentage of total score and categorization of scores (high quality, moderate quality and low quality) with very conservative cut-off values. This allowed the comprehensive assessment using one single tool for all included studies, despite difference in study methodology.
What this study adds
This review highlights the disparity in the palliative treatment of patients with lung cancer and those with COPD at the end of life. With a similar symptom burden, it is expected that people with COPD would also benefit from a palliative approach. Future studies should explore the impact of palliative care on patient-oriented outcome measures such as symptom severity and health-related quality of life in people with COPD. Comparing healthcare resource utilization and an economic analysis among people with COPD receiving palliative care to those who did not would also offer valuable insight into the implications on the healthcare system.
Conclusion
Despite a similar symptom burden and poor health-related quality of life, people with COPD receive less palliative care services, medications for symptom management and more life-sustaining interventions than people with lung cancer. People with COPD have an unmet need for end-of-life care that needs to be addressed and should better reflect the rates seen in lung cancer populations.
Supplemental Material
Supplemental_material_search_strategy_MEDLINE – Supplemental material for Comparison of end-of-life care in people with chronic obstructive pulmonary disease or lung cancer: A systematic review
Supplemental material, Supplemental_material_search_strategy_MEDLINE for Comparison of end-of-life care in people with chronic obstructive pulmonary disease or lung cancer: A systematic review by Stacey J Butler, Lauren Ellerton, Andrea S Gershon, Roger S Goldstein and Dina Brooks in Palliative Medicine
Footnotes
Author contributions
The review was primarily written by S.J.B. All authors contributed to the study design, interpretation of the data and manuscript revisions. Authors S.J.B. and L.E. primarily performed the review of articles for inclusion, data extraction and quality assessment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Author D.B. holds a National Sanatorium Chair, West Park Healthcare Centre. Author A.S.G. holds a CIHR New Investigator Award.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.