
Abstract
Background:
Palliative care has been identified as an area of low outpatient referral from our emergency department, yet palliative care has been shown to improve the quality of patient’s lives.
Aim:
This study investigates both provider and patient perspectives on palliative care for the purpose of identifying barriers to increased palliative care utilization within our healthcare system.
Design:
Two surveys were developed, one for patients/caregivers and one for healthcare providers.
Setting/participants:
This was a single-center study completed at a quaternary academic emergency department. A survey was sent to emergency medicine providers with 47% response rate. Research staff approached Emergency Department patients who had been identified to be high risk to fill out paper surveys with 76% response rate.
Results:
Only 28% of patients had already undergone palliative care, with an additional 25% interested in palliative care. Nearly half of the patients felt that they needed more resources to prevent hospital visits. Patients identified low understanding of palliative care and difficulty accessing appointments as barriers to consultation. Among providers, 98% indicated that they had patients who would benefit from palliative care. A majority of providers highlighted patient understanding of palliative care and access to appointments as barriers to palliative care. Notably, 52% of providers reported that emergency medicine provider knowledge was a barrier to palliative care consultation.
Conclusions:
Despite emergency department patients’ self-identified need for resources and emergency medicine providers’ recognition of patients who would benefit from palliative care, few patients receive palliative care consultation.
Many patients with life-limiting illness will be seen in the emergency department during the last months of their lives.
Palliative care is not well-incorporated into emergency medicine training or practice.
Randomized studies demonstrate that integrating palliative care into the emergency department increases frequency of palliative care consultations for patients and improves quality of life.
Emergency department patients report lack of understanding of palliative care and lack of access to appointments as barriers to palliative care consultation.
Emergency medicine providers report that patient understanding of palliative care, ability to get to appointments, and access to appointments as the greatest barriers to palliative care consultation.
A majority of emergency medicine providers reported that provider understanding of palliative care was a barrier to palliative care consultation.
Patient education regarding palliative care and increased access to appointments would improve palliative care utilization among emergency department patients.
There continues to be a knowledge gap among emergency medicine providers regarding palliative care.
Background/introduction
A recent survey showed that adults in the United States have little knowledge of palliative care. Misconceptions persist even among patients that consider themselves “knowledgeable.” 1 One international study found that patients had limited understanding of diseases, unmet information needs, poor communication with their health teams, and a limited understanding of the palliative care role. 2 Limited knowledge of palliative care exists among non-palliative physicians. 3
Many patients will be seen during the last month of life in the emergency department (ED).4,5 Prior studies show palliative medicine has not been a central part of emergency medicine (EM) training and has associated perceived barriers and misconceptions.6,7 This restricts palliative medicine consultation. 8 Even when emergency physicians have palliative medicine skills, they may not understand which patients would benefit from palliative care. 9
This study investigates patients’ and providers’ understanding of palliative care in an ED and identifies gaps in utilization of palliative care within a particular quaternary care hospital.
Methods
This survey study followed standardized reporting guidelines.10–12
Research question
What is the understanding of palliative care in the ED by providers and patients? What are the associated limitations to outpatient palliative referral for high-risk patients?
Design
The survey was designed with the Mayo Clinic Survey Research Center. Survey methodology was selected to obtain qualitative perspectives of patients and providers and obtain a larger sample size. Separate surveys were developed for patients and providers.
Setting and population
This study was conducted at Mayo Clinic in Minnesota, a quaternary care center.
Sample
The ED provider survey was distributed through email and was open for 3 months. This was sent to a distribution list that included attending physicians, advanced practice providers (physician assistants and nurse practitioners), and EM resident physicians.
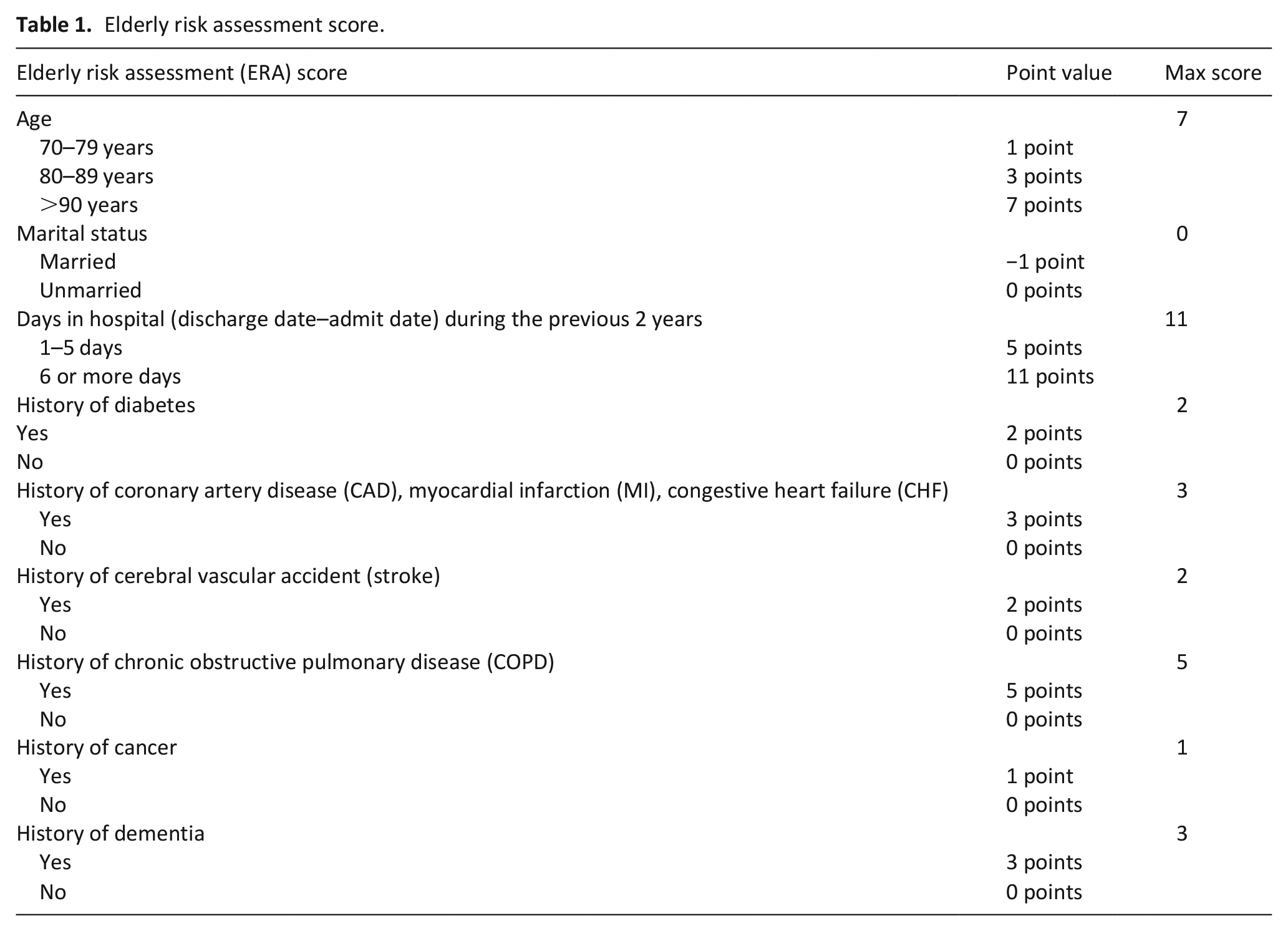
A convenience sample of patients identified by clinician gestalt or with an Elderly Risk Assessment (ERA) score of 16 or greater, as automatically calculated within the electronic health record (EHR; Epic, Verona, WI). The ERA is a validated index that predicts hospitalizations, mortality, and ED visits.13,14 Scores range from −1 to 34 points and incorporates multiple factors (Table 1).
Elderly risk assessment score.
Recruitment
Provider enrollment was voluntary and based off return of survey responses. Patients verbally consented to enrollment. Patients were approached by research coordinators based on physician request of involvement in study or calculated ERA score.
Data collection
Survey data were collected on paper and the study coordinator entered the data into a secured, encrypted database (REDCap, Vanderbilt, TN). Enrollment was from February to August 2019. The provider survey was sent to ED physicians, residents, and advanced practice providers from October to December 2018.
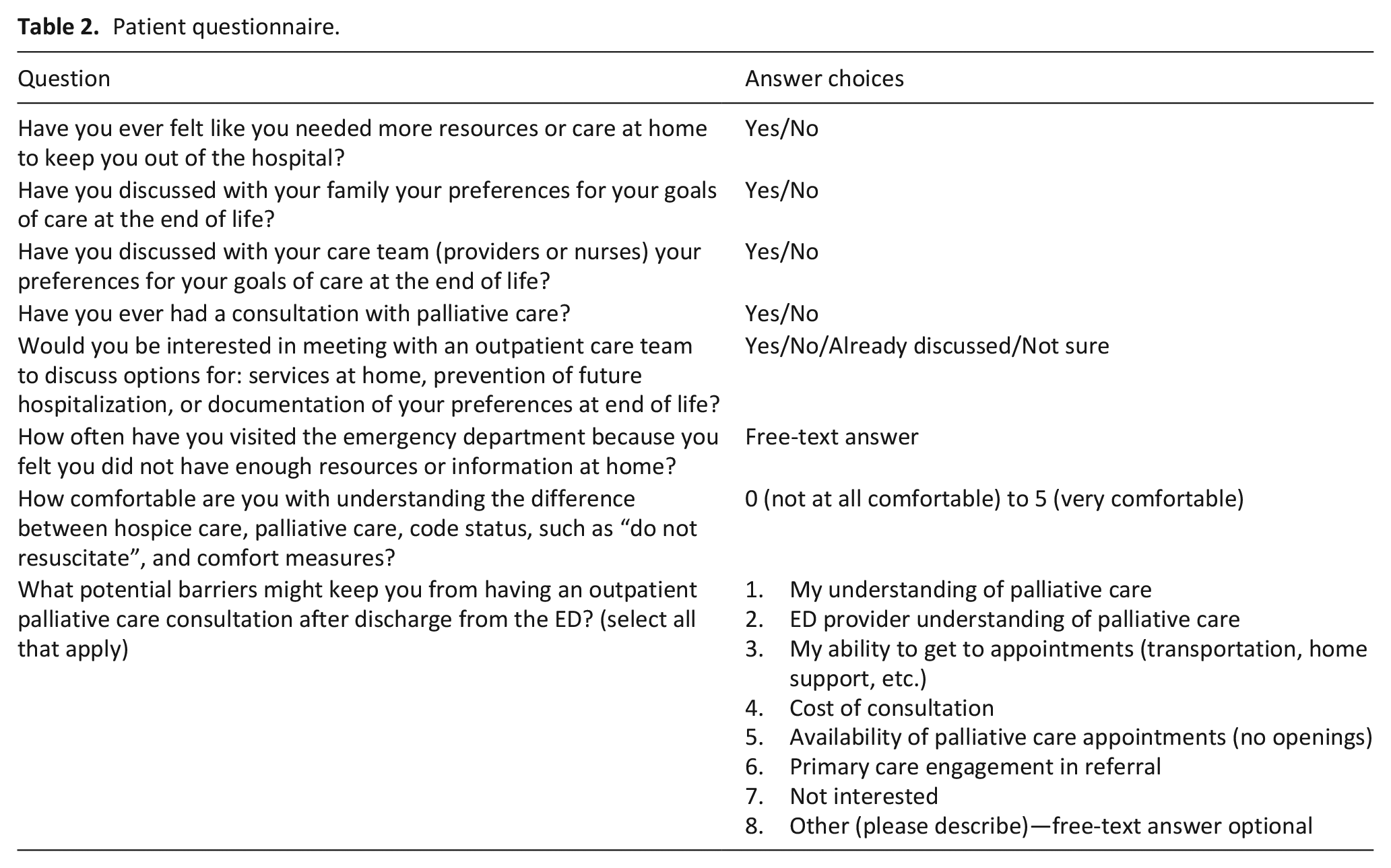
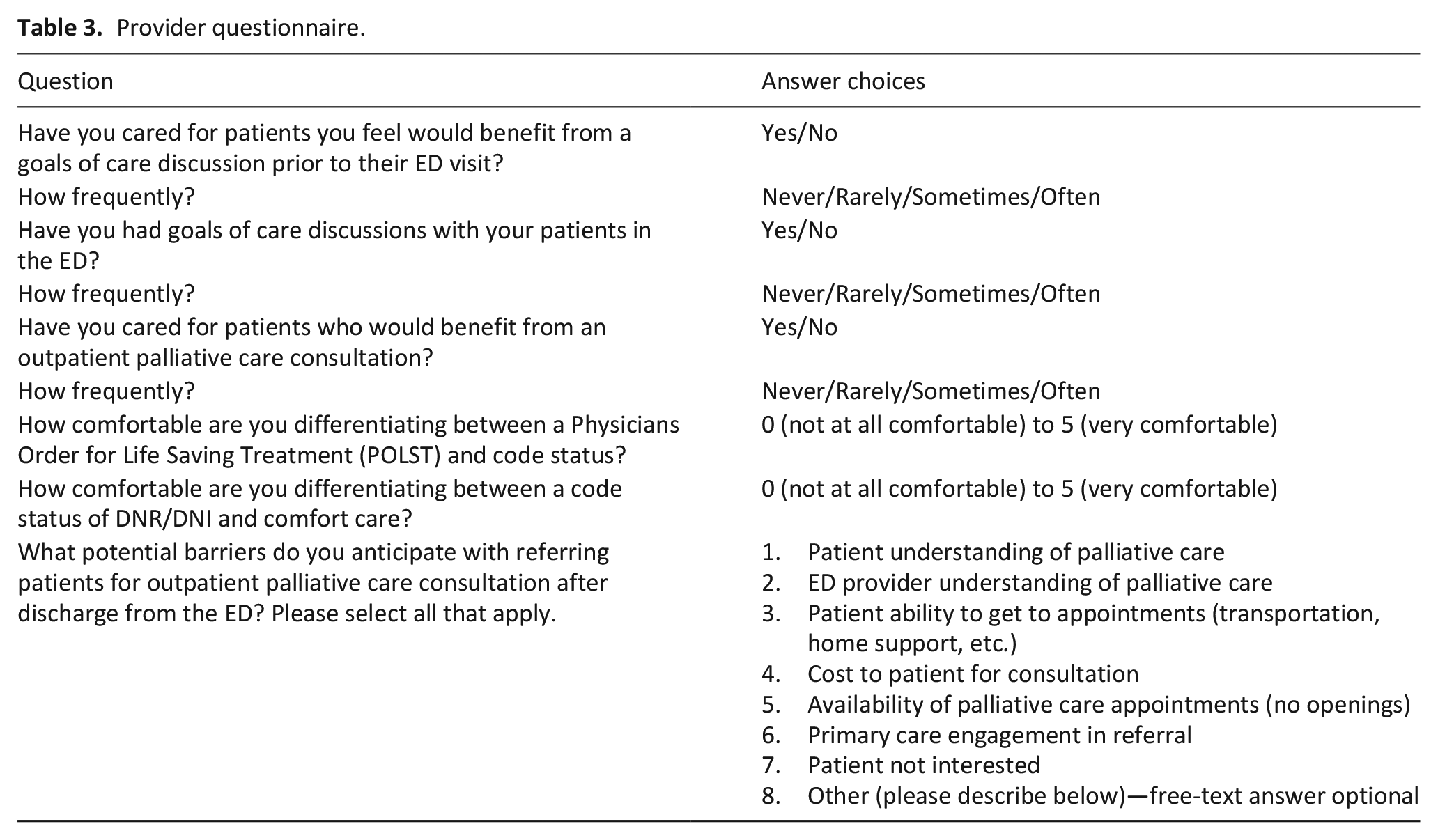
Surveys were designed based on prior literature including yes/no, multiple choice, and Likert-type scale questions. A free-text question was included on barriers to palliative care consultation. A pilot group provided feedback. Surveys are in Tables 2 and 3.
Patient questionnaire.
Provider questionnaire.
Data analysis
Incomplete questionnaires were included, but unanswered questions were not incorporated. Questions underwent descriptive analysis and were reported with percentages. Two authors (E.J.W. and A.D.G.) reviewed free-text answers and assigned responses into categorical groups. Disagreements were mediated by discussion.
Ethics
This study was deemed exempt by the Mayo Clinic IRB (#18-005902) and written informed consent was not required, as personal identifiers were not recorded.
Results
Patient survey
A total of 67 patients were approached by research staff but only 51 patients participated (67% response rate). We found that 57% (n = 29) of respondents discussed their end-of-life goals of care with family and 49% (n = 25) discussed their preferences with their care team. Patient interest in outpatient palliative consultation was mixed (Figure 1).
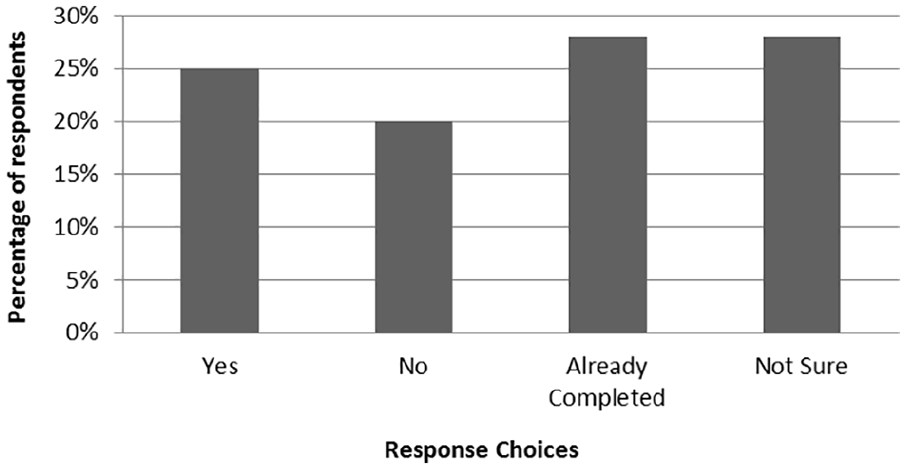
Interest in outpatient palliative consultation.
Almost half, 44% (n = 22), of the respondents indicated they needed more resources or care at home to help prevent hospitalization. In total, 49% of patient/family respondents replied they had at least one visit to the ED due to lack of resources. Responses indicated use of the ED in these circumstances varied (see Table 4).
Free text “Other” responses from patients/their family.
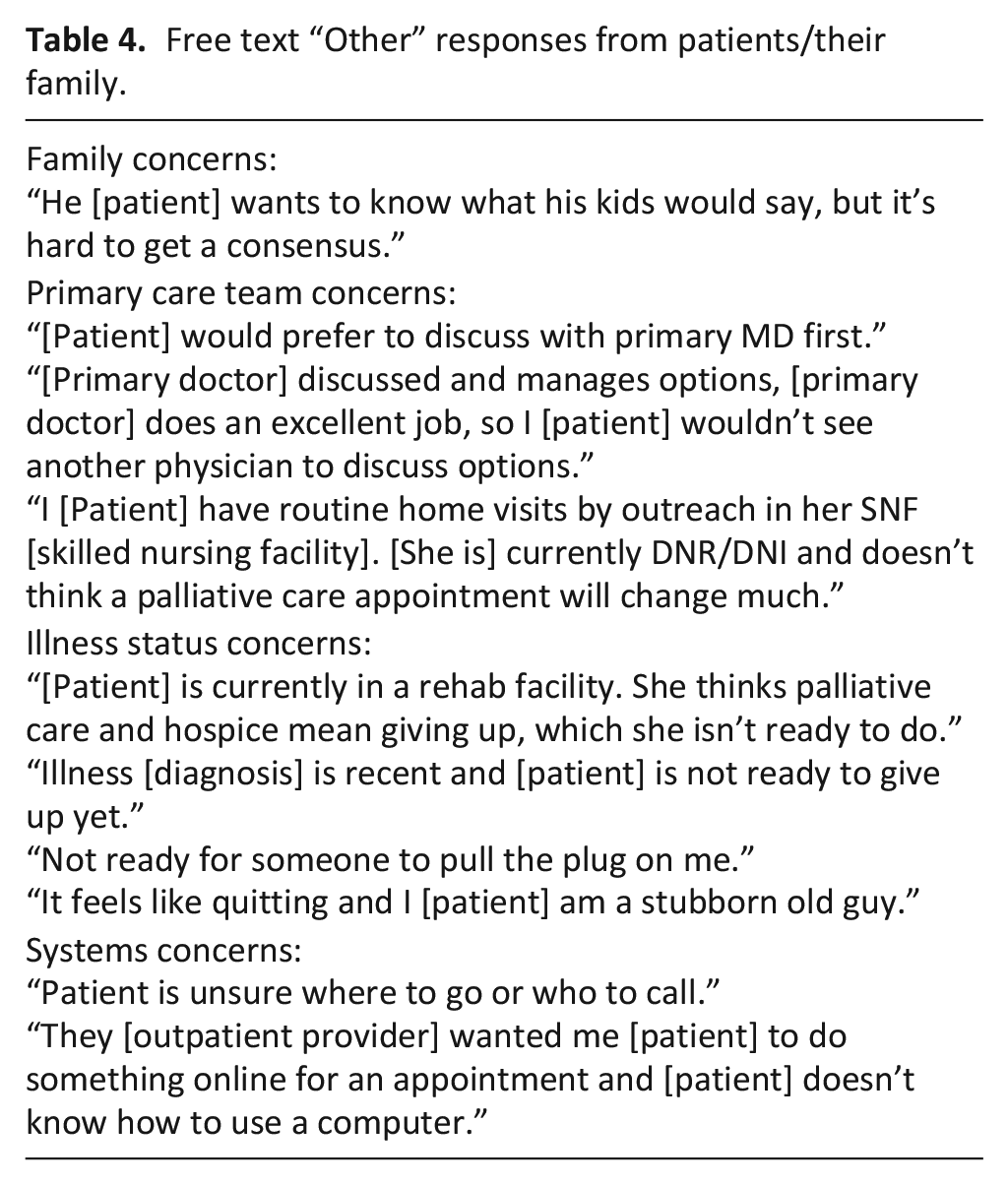
Comfort with understanding the difference between hospice and palliative care was evaluated on a Likert-type scale from 0 (“not at all comfortable”) to 5 (“very comfortable”), mean rating was 2.3. Patients felt the greatest barrier to having outpatient consultation was limited understanding of palliative care (44%, n = 18). Only 10% (n = 4) of patients felt that EM providers’ understanding was a barrier to receiving outpatient palliative care services.
Provider survey
A total of 103 staff were surveyed and 48 responses were received (47% response rate). Almost all (96%, n = 46) felt that they cared for patients who would benefit from goals-of-care discussion prior to their ED visit and 47% (n = 22) reported frequency of caring for these patients as “often.” Nearly all (98%, n = 47) had cared for patients who would benefit from outpatient palliative consultation. In fact, 91% (n = 44) of those surveyed reported having goals-of-care discussions in the ED.
Providers were questioned on comfort differentiating between POLST and code status using a Likert-type scale of 0 (“not at all comfortable”) to 5 (“very comfortable”), with a mean of 3.5. Comfort differentiating between DNR/DNI and comfort care were rated using the same scale with a mean of 3.7.
Providers identified barriers to palliative care and were able to submit multiple answers and free-text responses (Table 5). A majority of providers (85%, n = 41) indicated patient understanding was a barrier, 73% (n = 35) responded that patient ability to get to appointments was a barrier, and 71% (n = 34) felt that access to outpatient palliative care appointments as was a barrier. Interestingly, 52% (n = 25) felt that EM provider understanding of palliative care was a barrier.
Free text “Other” responses from physicians and NP/PA providers.
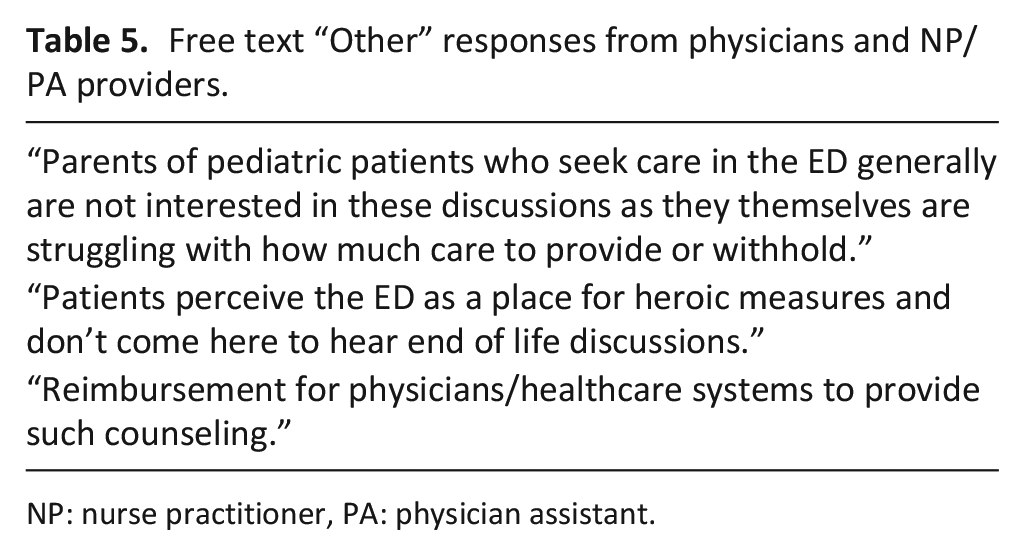
NP: nurse practitioner, PA: physician assistant.
Discussion
Main findings of the study
In our survey of patients qualifying for outpatient palliative care seen in the ED, only 20% had palliative consultation despite high ERA scores indicating chronic illness or frailty. Almost half of the surveyed patients felt they did not have adequate resources at home. We demonstrate that severely ill patients have unmet needs related to symptom management, home health resources, and alignment treatment with goals of care.
We recognize these patients would benefit from palliative care consultation, yet our referral rate from ED is exceedingly low, in fact during the time of data collection, only a total of 3 outpatient palliative care referrals were made and 13 inpatient consultations of palliative care were placed from the ED, out of a total of more than 60,000 ED visits. The dissonance between self-reported understanding and objective utilization may be manifestation of low provider comfort level with goals of care discussions. Demonstrated discomfort reveals an opportunity to improve conversations by teaching skills necessary for appropriate goals-of-care conversations. Fortunately, there are interventions underway that provide education and skill development to EM physicians. 15 We believe that having emergency providers who are trained in palliative care or goals of care discussions could lead to increased outpatient and inpatient referrals.
There is not currently a system to facilitate outpatient palliative care appointments directly from our ED. Our department does not have a physician, nurse, or social workers at all times with expertise in palliative care who could help facilitate outpatient appointments. This calls for evaluation of our internal and external resources to ensure matching of capacity with demand. A visit to the ED is an underutilized opportunity to engage with palliative care.
Strengths and limitations of the study
Strengths of this study include the following: (1) Patients who may benefit from palliative consultation were identified using a validated tool (ERA score). We identified patients who may derive the most benefit from palliative care. (2) Surveying providers in different roles is a more representative sample of the medical community as a whole. Other studies focused on emergency physicians only to identify barriers.6,8 (3) Identification of barriers by both patients and providers will inform subsequent steps to fill the gap.
Limitations include the following: (1) This was a small convenience sample of patients at a single ED (2) Patients and providers self-reported their understanding of the terminology and there was no objective measure for comparison. (3) It was not recorded whether the patient or surrogate filled out the survey. (4) Providers self-reported their frequency of goals-of-care discussions and level of comfort, without objective analysis for confirmation. (5) It is possible that those providers that felt uncomfortable or less knowledgeable with the terms were less likely to participate in the survey.
What this study adds
A self-reported gap in knowledge surrounding end-of-life care appears greater for patients than providers. Patients identified understanding, appointment access, and primary care engagement as substantiated barriers.
Patients seen in the ED benefit from receiving care that is in concordance with their values. With insights from this study, future efforts and interventions can target identified barriers, including access to outpatient palliative care when high-risk patients are identified.
Conclusion
Patients discuss their goals for end-of-life care with family and their care team, but many do not receive outpatient palliative consultation. Patients recognize that their understanding may be the greatest barrier to referral, but trust their provider’s knowledge.
Emergency medicine providers’ care for patients they believe would benefit from palliative care, but rarely refer in our practice. Providers attributed the largest barrier to outpatient palliative consultation as patient understanding. Future directions include the following: objective assessments of goals-of-care knowledge and development of ED specific educational tools to improve knowledge.
Many providers in our practice do not endorse high levels of comfort with goals-of-care discussions, despite reporting adequate knowledge. This reinforces need for further training. EM providers identified availability and patient attendance of palliative appointments as a barrier. Evaluation of outpatient access will inform the validity of this perception. This must be addressed at a systems level in collaboration with outpatient providers.
Footnotes
Author contributions
E.J.W. contributed to concept and design of work; data acquisition, analysis, and interpretation; and drafting and revision of manuscript. A.D.G. contributed to data analysis and interpretation; drafting and revision of manuscript. F.B. contributed to concept and design of work; drafting and revision of manuscript. L.E.W. contributed to concept and design of work; data acquisition, analysis, and interpretation; drafting and revision of manuscript.
Data Management and Sharing
Contact senior author, Laura E Walker, regarding data accessibility.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH; CTSA Grant Number UL1 TR000135). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH.
Research Ethics and Patient Content
This study was approved by Mayo Clinic Institutional Review Board (IRB # 18-005902, Exempt).
Prior Presentations
This study was presented at the American College for Emergency Physicians (ACEP) National meeting on 28 October 2019 in Denver, CO, as an oral presentation.