
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) is a life-limiting condition with palliative care needs. Despite increasing awareness about the role palliative care can play in care provision for patients with advanced COPD, integration in standard care remains underdeveloped. The unpredictability of the disease progression and misconceptions about palliative care being equivalent to end-of-life care often prevent a timely integrated approach in advanced COPD.
Aim:
To identify practices designed to increase integration of palliative care in the management of patients with advanced COPD in a respiratory service in Southern Switzerland.
Design:
A participatory action research approach was chosen and key stakeholders were involved to develop new knowledge and practices, supported by a Theory of Change framework. Data from each cycle and retrospective analysis at the end of the whole research were analysed using thematic analysis.
Setting/participants:
Five action research cycles with seven healthcare professionals working in palliative or respiratory care settings were conducted.
Results:
Three elements of integrated palliative care in advanced COPD were identified: multidimensional assessment, healthcare professionals’ education and interdisciplinary team meetings, which are the pillars of a new integrated palliative care model for patients with advanced COPD.
Conclusions:
The new integrated palliative care model in advanced COPD includes essential elements with a focus on patients, healthcare professionals and care delivery. Further research on testing this model in clinical practice, service development, implementation processes and possible outcomes, including evaluation of the financial impact of integrated palliative care is necessary to foster this care approach across all possible settings.
Although the recognition of COPD as a life-limiting condition with palliative care needs is increasing, palliative care provision in COPD remains underdeveloped.
Integrated palliative care aims to create continuity of care within a patient’s care network, thus avoiding care fragmentation with all individuals involved.
Development of a new integrated palliative care model through a participatory action research with key stakeholders who care for patients with advanced COPD.
Identification of essential elements to foster care integration, as these key features are often overlooked in clinical practice.
The use of a Theory of Change (ToC) framework as a theory to support reflections about the need to change care delivery for patients with advanced COPD and foster palliative care integration.
Institutions that are supporting change of care delivery for these patients are challenged to develop educational programmes for healthcare professionals caring for patients with advanced COPD and their families.
Multidimensional assessment, healthcare professionals’ education and interdisciplinary team meetings are the pillars of this new integrated palliative care model for patients with advanced COPD.
Raising awareness among healthcare professionals working for palliative and respiratory care services about the role palliative care might play in advanced COPD.
Availability of a theory to guide implementation that can be tested in both local evaluation processes and in further research.
Future research on service development, implementation processes and outcomes, including evaluation of the financial impact of integrated palliative care provision is deemed necessary to foster this care approach across all patients’ settings.
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of worldwide morbidity and mortality in adults. 1 Advanced disease is characterised by a decline in overall function, a progressive loss of independence and an important multidimensional symptom burden. 2 Although the recognition of COPD as a life-limiting condition with palliative care needs is increasing, palliative care provision in COPD remains underdeveloped. 3 The disease unpredictability, the misconceptions about palliative care being restricted to cancer and perceived to be only relevant in the last days of life often prevent a timely integrated care plan for patients with advanced COPD. 4 Several national and international guidelines on care provision for patients with COPD include the role of palliative care in advanced disease, suggesting a palliative care approach and involvement of a palliative care team.5–8 However, they seldom advise how to provide palliative care in advanced COPD services, thus fostering debates on key components of palliative care delivery in this population.
Integrated palliative care aims to create continuity of care within a patient’s care network, thus avoiding care fragmentation with all individuals involved. 9 A definition of palliative care integration was proposed through expert consensus. 10 This definition of care integration was developed linking aspects identified in the literature and agreed through consensus by palliative care experts.11,12 Palliative care integration is described as ‘bringing together administrative, organisational, clinical and service aspects in order to realise continuity of care between all individuals involved in the care network of patients receiving palliative care. It aims to achieve quality of life and a well-supported dying process for the patient and the family in collaboration with all the care givers (paid and unpaid)’ (p. 2).
Prior to this research, the institution delivered specialised palliative care through inpatient consultations for every hospitalised COPD patient presenting with advanced disease; however outpatients in the respiratory service did not benefit from a systematic palliative care provision. Consequently, further strategies were judged to be needed to promote greater utilisation of palliative care for patients with advanced COPD. The development and implementation of new healthcare initiatives maybe theory-driven, with a focus on understanding whether, how and why these initiatives work in a specific context. 13 Theory of Change is a ‘theory of how and why an initiative works which can be empirically tested by measuring indicators for every expected step on the hypothesised causal pathway to impact’ 14 (p. 2). Furthermore, it helps to map all the steps that are required during the developmental process in order to identify short- and medium-term goals that foster and promote long-term goals in healthcare interventions. 15
A systematic review of the literature on palliative care integration in advanced COPD performed prior to this study, underlined the importance of organisational changes that are necessary to develop integrated care. 16 This helped to focus the research aim on how to identify practices designed to increase palliative care integration for patients with advanced COPD in a respiratory service in Southern Switzerland through a participatory action research approach, supported by a ToC framework.
Methods
Study design
A participatory action research design was chosen for this study. Participatory action research can generate new knowledge from practice through a collaborative partnership between researchers and participants. 17 This approach considers key stakeholders as decision-makers in research (collaborative inquiry group, CIG) and aims to change a pre-specified healthcare intervention. The involvement of key stakeholders within the research group may lead to a ‘bottom-up’ modification of current practices in palliative care integration into standard care. 18
Action research involves a continuum of action planning, action performing, observing and reflecting on what happened in this process, as depicted in Figure 1. 19 Crucial in this cyclic process is critical reflexivity, which supports changes in practices. Unlike quality improvement, action research aims to draw on multiple forms of knowledge and generate knowledge generalisable to situations beyond the context of the initial study. 20
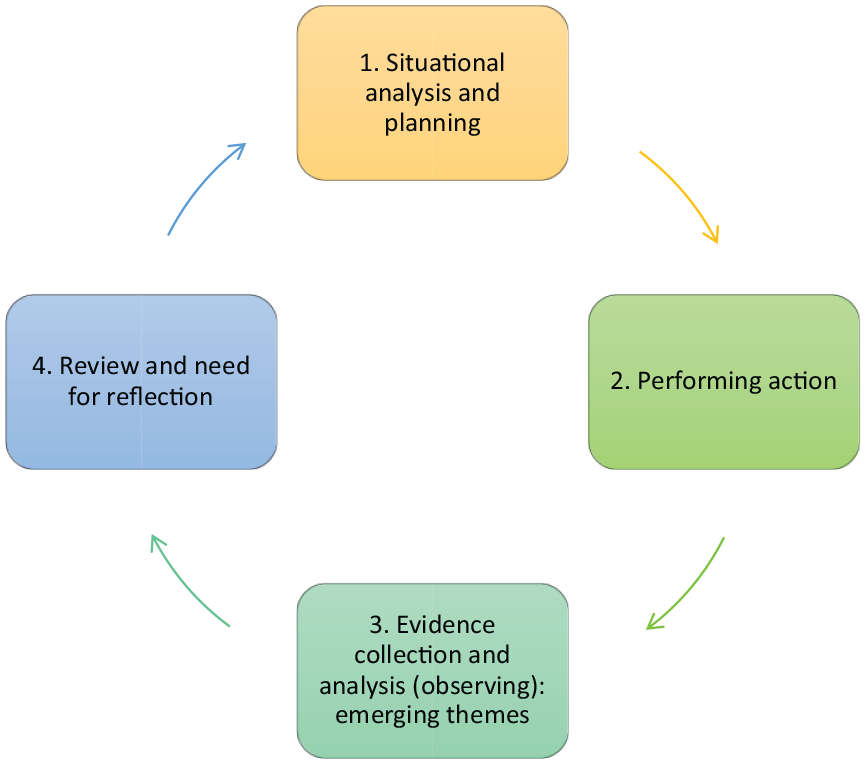
Model of each small cycle with a four-step process description.
The study was undertaken over five action research cycles. The situational analysis of the first cycle reviewed the results from a previous study that explored patients and carers’ experiences in living with COPD and their awareness about palliative care provision in advanced COPD. 21 Guilt, sense of discrimination by healthcare professionals with regard to their smoking habits and caring for a loved-one with a self-inflicted disease were among the identified themes. 21 The fourth step of each small cycle led to the situational analysis and planning of the next cycle and this process ended within the fifth action research cycle.
Participants and setting
The study was conducted in a major public teaching hospital in Italian-speaking Southern Switzerland, where both respiratory and palliative care services are available. Study participants were selected through purposive sampling among 38 healthcare professionals from different professional background (physicians, nurses and physiotherapists) and from both services who expressed an initial interest to participate.
Inclusion and exclusion criteria, as listed in Table 1 below, were applied during the process.
Inclusion and exclusion criteria for healthcare professionals.

Potential participants were approached via email. Recruitment was supported by a detailed information letter, which explained who was undertaking the research, what the aims were and what the research involved (including time requirements, potential risks and data handling in terms of confidentiality). Face-to-face appointments between the researcher and potential participants were offered to give them a chance to ask questions about the study: two people took up this opportunity. Healthcare professionals who declared an interest in participating, received a postage paid envelope, together with the participant information sheet and the consent form. Participants were given two weeks to consider whether to join the study. The researcher met with participants at the first CIG meeting and gained informed, written consent before the meeting began.
Data collection
Data collection followed a series of five action research cycles over a period of 16 months, from May 31st 2017 to September 27th 2018. The CIG meetings were conducted in a conference room on clinic premises during working hours, digitally recorded, anonymised and transferred to a password-protected computer. Data was retrieved among different data sources and in different formats. Audio recordings, observations (field notes) and notes from a personal reflective journal represented data sources from the CIG meetings. Demographic data, CIG meetings’ attendees for each session and all the results from an interview study with patients and carers exploring their perceptions in living with advanced COPD were also considered as data that informed the results of this research. The data format was heterogeneous, such as audio material transcribed verbatim, written notes, visual material such as power point presentations, diagrams, sketches, drawings and flowcharts.
The data collected had different functions in the research process: it informed the CIG, it informed decisions about subsequent other data collection in all research cycles, guaranteeing the process flow among cycles and it supported the process evaluation and outcomes for the entire research. 22
Data analysis
Two different data analysis approaches were used. 23 Firstly, concurrent analysis during each small cycle (cycle one to five) was adopted to develop themes within the individual cycle. This supported the research process and helped to further develop the next action research cycle. After every action performance, data collected was analysed using a thematic analysis approach. 24 Field notes taken during all CIG meetings helped to triangulate data. Engagement with raw data, identification of initial codes and development of main themes were the steps in data analysis. A summary of preliminary themes and subthemes from the previous cycle was discussed at the beginning of the next CIG meeting, thus enabling participants to: (1) Discuss the possible themes from the previous cycle, (2) Generate new data during discussion on the themes, while shaping the new action to perform in the upcoming cycle.
Furthermore, a retrospective analysis was performed at the end of the whole research process. All data collected in the five action research cycles were analysed through thematic analysis to generate understanding about the whole research process, to inform the discussion and to answer the research question. A ToC framework supported the analysis and synthesis of themes identified during the CIG meetings. Moreover, Theory of Change embedded in this action research encouraged reflections about the need to recognise different levels of an institution where changes may be facilitated or prevented. 25 To support a fundamental change in care delivery for patients with advanced COPD and foster palliative care integration, it was essential either to rethink the system where care is delivered or to adopt different models for care provision compared to the current situation. 26 Key elements of a Theory of Change approach (the ‘how and why’) were applied to understand how to further shape and develop the new integrated care model and to provide a framework for monitoring and promoting future evaluations.
Ethical considerations
Ethical approval was granted from both the Swiss and the Lancaster University Research Ethics Committee (CE 3044 BASEC 2016-00361, FHMREC15099).
Results
Five females and two males participated in the study. The median age of participants was 49 years (range 32–66 years). Five participants were physicians, one was a nurse and one a physiotherapist. All healthcare professionals had more than 10 years of clinical experience in their specific field (palliative or respiratory care). A higher level of detail could not be provided due to anonymity concerns. All meetings lasted about an hour and all participants attended the five meetings.
Through concurrent analysis of the five action research cycles and retrospective analysis of the whole process, three themes were identified as being essential for the development of integrated palliative care in advanced COPD and they are listed in Table 2.
Identified themes for integrated palliative care in COPD.
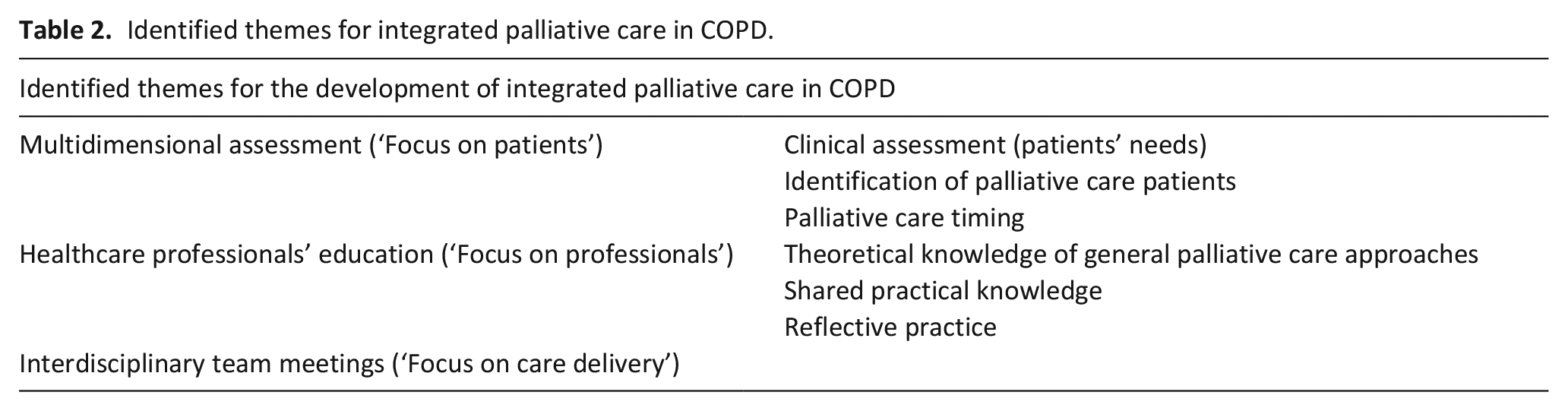
Some of these themes had been previously described as integrated care criteria for palliative care initiatives.11,27 These themes were considered as key elements which helped to develop a new integrated palliative care model for patients with advanced COPD. The starting point of this new integrated palliative care model was the assessment of needs. The identification of advanced COPD patients as palliative care recipients, the timing of palliative care provision in standard respiratory care and a holistic evaluation of patients’ needs, were key features of this first component of the new model of care provision.
The second key component of the model of service delivery was healthcare professionals’ education. Acquiring theoretical knowledge on palliative care approaches, developing skills and competences through shared consultations and fostering reflective practice among all professionals involved with care management of patients with advanced COPD, were considered to be required elements of basic education.
The third key component of this model of care integration focused on how care is delivered to patients with advanced COPD. The main element that was identified from this action research study as being fundamental for integrated care provision was the implementation of interdisciplinary team meetings. Interdisciplinary team working was understood as integrating knowledge and competences from all healthcare professionals towards a common, patient-centred approach of care delivery. 28 This is different to multidisciplinarity, where collaborative work approaches among healthcare professionals with different competencies and skills are practiced within discipline borders. 29 Further elements of interdisciplinary team meetings were not explored by participants during the CIG meetings.
In summary, the study results provide information on essential elements that foster palliative care integration in ‘real clinical life’ for patients with advanced COPD, as these elements are often overlooked in the overall management of this particular population.
Discussion
This research reiterates already known essential elements for palliative care integration in advanced COPD, such as holistic needs’ assessment, educational initiatives and modalities of service delivery.30–32 However, this study addresses the identification of key features each essential element should include to allow and foster the process of palliative care integration in patients with advanced COPD, while being supported by a Theory of Change framework. Firstly, multidimensional needs’ assessment should consider three aspects, such as patients’ needs (the ‘what’), palliative care timing (‘the when’) and identification of palliative care recipients (the ‘who’). Secondly, educational initiatives should promote different core components, such as theoretical knowledge (‘to know’), practical knowledge (‘to know how’) and experiential knowledge (‘to know how to be’). 33 Educational interventions such as the development of communication skills and knowledge about palliative care delivery in different care settings have been debated.30,34 Nonetheless, the evidence identified in this study about different levels of healthcare professionals’ knowledge which are required to provide integrated palliative care for patients with advanced COPD is new and represents a pillar of the proposed integrated care model. Lastly, interdisciplinary team meetings should be a fundamental component of service provision in the integrated palliative care model for patients with advanced COPD.
This study was supported by a systematic review of the literature performed prior to the current research. The review identified a taxonomy involving different levels of care provision, where integrated care is the last step of a dynamic process of care delivery. 16 These results helped to raise awareness within the CIG about organisational changes that are necessary to develop integrated care.
As previously mentioned, a theory-driven approach was chosen to support data analysis and synthesis. A ToC framework helped to clearly define all steps which are essential to support the implementation of this new integrated care model towards a pre-defined long-term outcome. 14 These essential steps were identified through a Theory of Change supported process of rethinking the elements that were defined in the CIG meetings as components of a pathway of change. Therefore, all the elements were linked with long-term and intermediate outcomes, interventions and indicators to evaluate the new integrated care model. This shift from elements identified in the CIG meetings towards a pathway of change helped to understand what is needed to further develop the implementation and broader dissemination of the integrated care model in advanced COPD.
The elements of the pathway of change in relationship to the proposed integrated palliative care model are listed as follows:
(1) Long-term outcome: cantonal integrated palliative care model for advanced COPD.
(2) Interventions: educational training, choice and implementation of patient identification and needs’ assessment tools, development of interdisciplinarity within caring teams.
(3) Intermediate outcomes:
• Education: personnel is trained in palliative and respiratory care (acquiring theoretical, practical and experiential knowledge).
• Needs’ assessment: tools are used in daily clinical practice.
• Service delivery: interdisciplinary team meetings are regularly held.
4) Indicators: they need to be discussed with key stakeholders in order to evaluate the integrated initiative (e.g. number of healthcare professionals who are trained, patients’ and carers’ satisfaction with care delivery, healthcare professionals’ experiences with care model, economic impact).
This pathway of change may provide stakeholders in other settings a process to follow for their implementation of a similar model, adapted to their healthcare service setting. 13
The emerging COVID-19 pandemic prevented the full implementation of the integrated care model in our respiratory outpatients’ service. Nevertheless, a patients’ palliative care identification tool was implemented, fostering shared consultations with pulmonologists, palliative care physicians and physiotherapists. 35 Furthermore, the definition of milestones on the disease trajectory of all patients, such as the introduction of long-term oxygen therapy or loss of recreational activities triggered palliative care referral. Shared consultations addressed patients’ needs assessment through a specific validated tool that helped to tailor care provision according to patients’ needs. 36 Virtual educational conferences for healthcare professionals within the respiratory service were conducted to foster general palliative care knowledge, albeit focussing on issues concerning respiratory diseases. Furthermore, discussions between partner institutions are currently underway to develop a project for a network social worker, who may provide care for patients in every possible setting (homecare, in-hospital consultations and outpatient care).
Collaborative inquiry group meetings were held during working hours of participating members, in accordance with the institution. Additional costs of the development process were allocated to the palliative care service, as a 0.1 full time equivalent of a senior consultant for 1 month. Some preliminary information about potential outcomes from the model testing revealed an increase in early palliative care referral for both in-hospital and outpatients and justified the development of regular palliative care consultations for outpatients within the respiratory care service. Advance care planning discussions and continuity of care between different care settings were also fostered.
Strengths and limitations
The strengths of this study need to be highlighted. To our knowledge, this is the first study involving healthcare professionals developing knowledge through a participatory action research approach to understand how to integrate palliative care for patients with advanced COPD. Furthermore, this study identifies elements of a pathway of change that are needed to implement the new intervention in standard care. These elements may be monitored and evaluated during the implementation process. The limitations of this study need to be acknowledged. Model testing was prevented by the COVID-19 pandemic, as the institution was forced to revise priorities towards the management of this global healthcare crisis. Nonetheless, as previously stated, the developed learning process helped to foster shared consultations and to implement validated patients’ assessment tools.
The assessment of quality and rigour in action research remains an open debate. 37 However, this research was supported by already established criteria, such as evaluation of worthwhile practical purposes, participative and democratic inquiry, inclusion of different forms of knowledge and maintaining a continuum of research development over time. 38 Furthermore, it is important to highlight the role of the researcher, as practising action research within a practitioner’s group with hierarchical relationships is challenging. The risk of developing asymmetrical relationships and thus preventing a truthful capture of all opinions and voices needs to be constantly assessed. 39 The CIG presented a dual power imbalance: one between the researcher and the non-medical professionals (nurse, physiotherapist), the second between the researcher, a senior consultant in palliative care and her medical colleagues. Continuous reflexivity and ongoing discussions about power relationships and sources of inequity were helpful to address potential study limitations. 40 In addition, the use of few practicalities, such as participants interacting by first name, creating an informal Smartphone chat-app to schedule all group meetings and attending meetings in plainclothes, thus avoiding white coats within the physician group, helped to overcome potential power imbalance.
Implication for policy and clinical practice
This study evidences how palliative care can be integrated in respiratory care services for patients with advanced COPD and what elements are essential to foster care integration in ‘real clinical life’. Developing shared practices and training healthcare professionals on working together are examples of key elements that are often overlooked in the overall management of patients with advanced COPD. This research would not have been possible without a raised awareness among healthcare professionals working for the palliative and respiratory care service about the role palliative care might play in advanced COPD. 41 This aspect is fundamental for promoting integrated care models into practice. 42 Supporting knowledge dissemination on this topic could mitigate pre-existing misconceptions about palliative care, such as being relevant only in end-of-life and oncological settings, thus increasing interest and initiatives towards palliative care integration in advanced COPD. 43
Healthcare professionals’ education was recognised as a pillar of this integrated care model. Fostering theoretical, practical and experiential knowledge is essential to promote care integration in advanced COPD. Hence, institutions that are supporting change of care delivery for these patients are challenged to develop educational programmes for healthcare professionals working with advanced COPD patients and their families. Collaboration within educational networks may help to develop common programmes and define content and modalities of healthcare professionals’ education in palliative care. 44
The new integrated palliative care model underlines the importance of working in an interdisciplinary manner. Interdisciplinarity requires integrating knowledge and competences from all involved healthcare professionals towards a common and patient-centred approach of care provision. 28 Learning how to work together in an interdisciplinary way needs training and the use of individual and group reflective practice. This is a process that is time consuming and requires guidance from professionals who are used to working in and conducting interdisciplinary teams. 45
Lastly, respiratory care services that are interested in implementing integrated care models should consider the impact of professional resources needed for palliative care delivery. The lack of available specialised healthcare professionals may prevent the implementation of an integrated care model. 41 Therefore, it is paramount to encourage healthcare professionals interested in working for integrated palliative care services to pursue educational programmes and develop competencies in this specific field. Increased training and input from palliative care specialists will foster high-quality palliative care delivery by respiratory care teams.
Future research priorities
In consideration of the implications for practice previously discussed, it is important to highlight areas of future research. The value of studying the care integration process as it was conducted helped to develop a theory to guide implementation in both local evaluation processes and in research contexts. It will be of utmost importance to understand how this model for palliative care provision may fit within existing institutions. Therefore, facilitators and barriers for implementation need to be explored and acknowledged during future service developments. Furthermore, integrated palliative care models for patients with advanced COPD could benefit from future research on quality indicators for practice. These indicators may help to understand the ‘how and the why’ of future care integration, while fostering high-quality care delivery. Lastly, understanding the perspectives of end-users and of professionals working within and across services may foster quality improvement and ongoing model adaptation to changing needs.
Conclusion
This new developed integrated palliative care model in advanced COPD includes essential elements with a focus on patients, healthcare professionals and care delivery. Future research on model testing in clinical practice, service development, implementation processes and outcomes, including evaluation of the financial impact of integrated palliative care provision is deemed necessary to foster this care approach across all patients’ settings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.