
Abstract
Background:
Infection control measures during infectious disease outbreaks can have significant impacts on seriously ill and dying patients, their family, the patient-family connection, coping, grief and bereavement.
Aim:
To explore how family members of patients who are seriously ill or who die during infectious disease outbreaks are supported and cared for during serious illness, before and after patient death and the factors that influence family presence around the time of death.
Design:
Systematic review and narrative synthesis.
Data sources:
CINAHL, Medline, APA PsycInfo and Embase were searched from inception to June 2020. Forward and backward searching of included papers were also undertaken. Records were independently assessed against inclusion criteria. Included papers were assessed for quality, but none were excluded.
Findings:
Key findings from 14 papers include the importance of communication and information sharing, as well as new ways of using virtual communication. Restrictive visiting practices were understood, but the impact of these restrictions on family experience cannot be underestimated, causing distress and suffering. Consistent advice and information were critical, such as explaining personal protective equipment, which family found constraining and staff experienced as affecting interpersonal communication. Cultural expectations of family caregiving were challenged during infectious disease outbreaks.
Conclusion:
Learning from previous infectious disease outbreaks about how family are supported can be translated to the current COVID-19 pandemic and future infectious disease outbreaks. Consistent, culturally sensitive and tailored plans should be clearly communicated to family members, including when any restrictions may be amended or additional supports provided when someone is dying.
Keywords
COVID-19 has caused widespread changes in visiting patterns and practices in hospitals, care homes and other health and social care facilities.
The effect of these changes on family caregivers, and the extent to which family members are supported when their family member is seriously ill or dying are not known, but may be similar to experiences in previous epidemics and pandemics.
Family caregivers mostly understand and acknowledge the reasons for restrictions in visiting and caring for family members and use of personal protective equipment during epidemics and pandemics, but this does not eliminate the suffering and distress these cause.
Virtual modes of communication via telephone or other means is consistently highlighted as fundamentally important to maintaining the patient-family connection and family perceptions of support during infectious disease outbreaks.
Clear plans should address the needs for Frequent and personal communication with family caregivers both from health and social care professionals, and with the person who is unwell, if their condition allows should be planned during the current COVID-19 pandemic, and included in policies addressing any future epidemics.
Current restrictions are likely to mean a higher likelihood of adverse grief and bereavement reactions from family caregivers, and attention needs to be paid to setting up appropriate support services as a priority.
Introduction
The COVID-19 pandemic has had many personal, societal, economic and other costs. 1 One of the greatest costs and challenges is in terms of how it has affected our means and ability to provide human support offered to patients and their family. In times of disaster, basic human needs of humans to feel safe, connected, useful and helpful are intensified. 2 Thus, human and social connections are important to health and wellbeing,3 –5 being alongside others is a fundamental coping response to threat, and tending to others can sustain psychological health. 6 Person or family-centred approaches to care are fundamentally important to the conceptualisation of modern healthcare because health and illness is also not only experienced individually, but often via connections with family or significant others. Serious illness impacts the functioning of family units, and influences the health and wellbeing of those within the unit. This has long been recognised within palliative care practice, with family care seen as integral to its provision, and an understanding of family systems important to effective care. 7
A key feature of the COVID-19 pandemic has been the rapid initiation of policies that restrict family contact. Whether this be a public health response to reducing virus transmission (e.g. restrictions on household visits), or more clinically mediated strategies to protect vulnerable patients and health care providers (e.g. through severe hospital visiting restrictions) the impact on the family unit, family-centred care 8 and the support provided to family members is significant. Impacts are felt not only by those who are sick, but also others who are well but isolated such as older adults, or those in long-term care facilities, who rely on family to navigate healthcare, act as advocates and surrogate decision makers, 9 as well as those who may be subject to visiting restrictions because they are unwell. It is argued that such policy decisions need to consider issues of equity, publicity, transparency and the appeal process, 10 with a particular appeal to taking facts from a scientific perspective into consideration. This can be perceived as a challenge in the rapidly changing context of a global pandemic, where policies must be made in advance of scientific knowledge, or based on knowledge from previous similar, but not identical situations.
There is a body of knowledge that addresses some issues of both family involvement in the care of those with serious illness or dying, and also attitudes towards the policies that may restrict such involvement. In general, families of critically ill patients want to be regularly informed, involved in patient care and decision-making,8,11,12 to be present at the bedside 8 and to observe, protect and comfort the dying person. 13 When access is restricted, not being able to say ‘goodbye’ can be deeply distressing and associated with psychological trauma in bereavement. 14 In the early days of COVID-19, rapidly developed systems such as use of telephone and video calls were used to aid families in preparing for death and to assist their grief and mourning process, 15 but whether this is enough in terms of support, is not fully understood. What is known is that as many as one-third of family members of patients in critical care settings experience significant negative psychological symptoms that can be long-lasting,16,17 with particular risk factors associated with being female or a spouse. 18 The response in pandemic situations appears similar, with family members of those hospitalised for influenza A/H1N1 showing elevated levels of stress and depression. 19
It is important therefore that there is an understanding of how best to support and care for families of those who are seriously ill or die during infectious disease outbreaks that may occur locally, but also on a larger scale, such as epidemics and pandemics both in the past and related to the current COVID-19 pandemic.
Methods
Aim
The aim of this review was to explore how family members of patients who are seriously ill or who die during infectious disease outbreaks were supported and cared for during serious illness, before and after patient death and the factors that influence family presence around the time of death.
Design
A systematic review with narrative synthesis. A narrative synthesis approach was considered most appropriate due to the exploratory nature of the research question and heterogeneity of the data in included studies. 20 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was used to guide reporting of this systematic review. 21 The protocol was registered with Prospero (CRD42020192577).
Inclusion and exclusion criteria
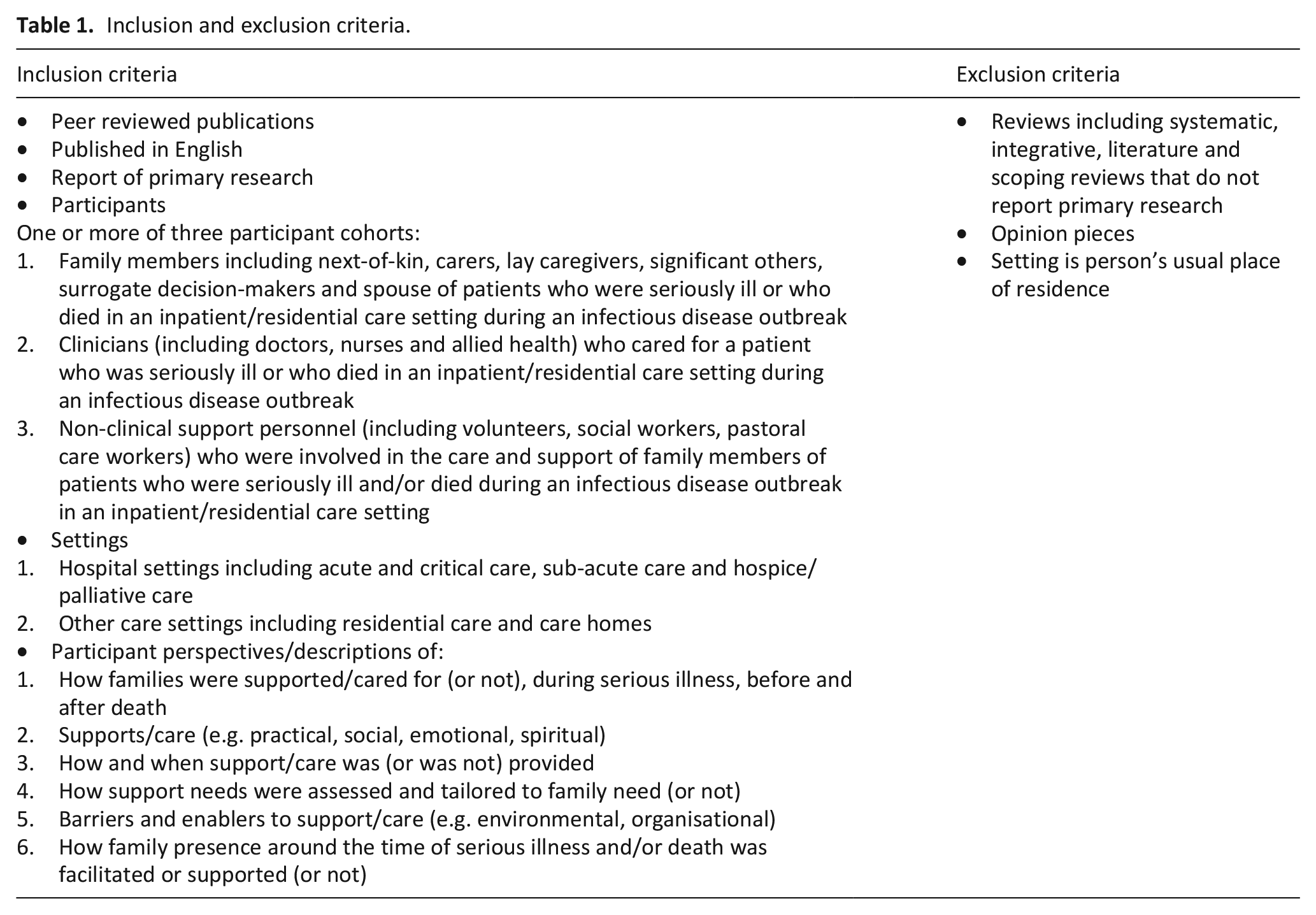
The focus of this review was family members, clinicians and/or non-clinical support personnel involved in the care of seriously ill or dying patients during an infectious disease outbreak. The concept and context guided the development of the inclusion and exclusion criteria detailed in Table 1.
Inclusion and exclusion criteria.
Search terms
Data-base specific search terms, MeSH headings and synonyms that described the concepts of ‘family’ and ‘infectious disease’ were used with Boolean operators in the search for literature (Table 2).
Search terms.
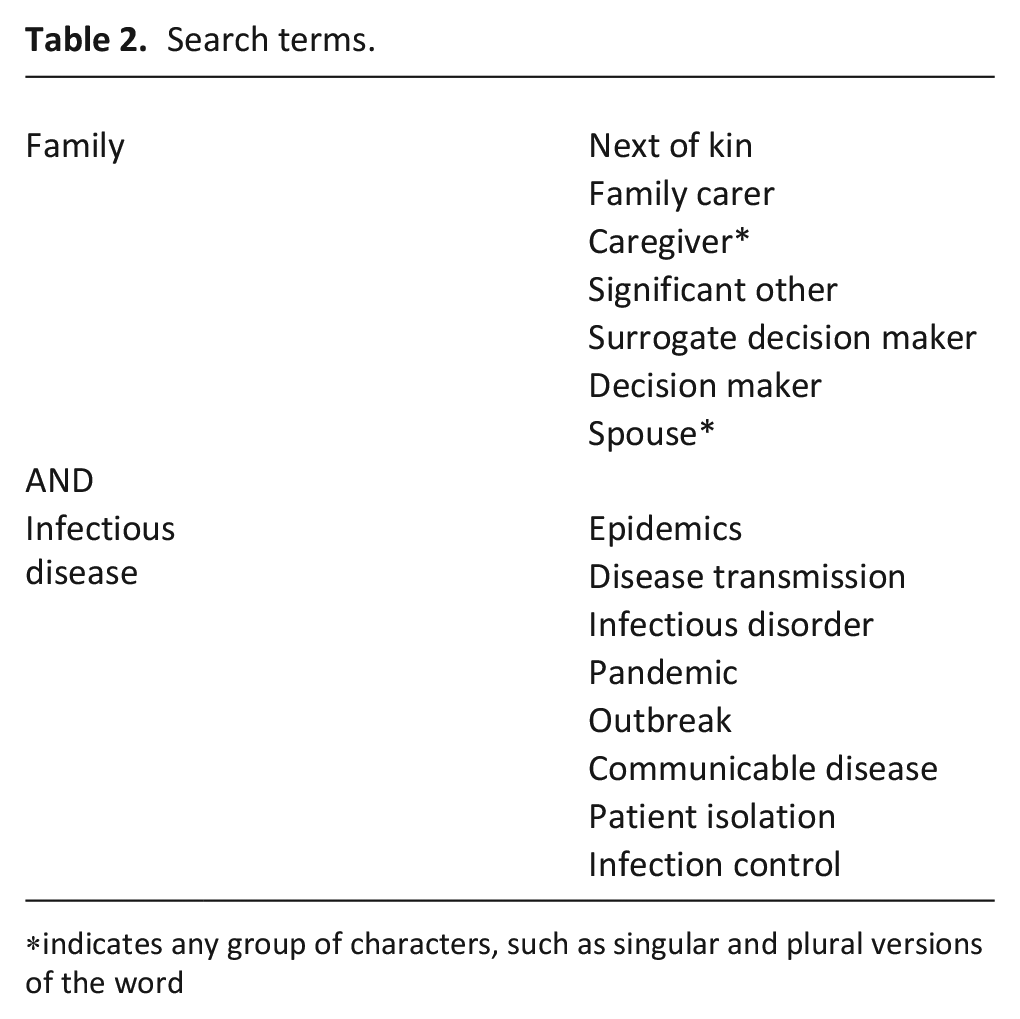
indicates any group of characters, such as singular and plural versions of the word
Search strategy
A search of Cumulative Index of Nursing and Allied Health Literature (CINAHL) Complete, Medline, APA Psycinfo and Embase databases was undertaken in June, 2020, with no date limit applied to the searches. The full search strategy for each database is provided as Supplemental File 1. A backward search of the reference list of all included papers and a forward search of papers which cited included papers was undertaken.
Search outcome
All records retrieved from the database searches were downloaded into EndNote (Version X9) and de-duplicated. Remaining Records were uploaded to Covidence, a web-based software platform designed to support the systematic review process by allowing both authors to independently screen and assess records, undertake text review and resolve reviewer conflicts. 22
Quality assessment
The quality of each included paper was assessed by the authors independently using an evaluative framework suitable for qualitative and quantitative research. 23 Given the small number of papers meeting the inclusion criteria, an a priori decision was made not to exclude papers based on quality scores, but rather to use the quality assessments to describe the quality of the research evidence.
Data extraction
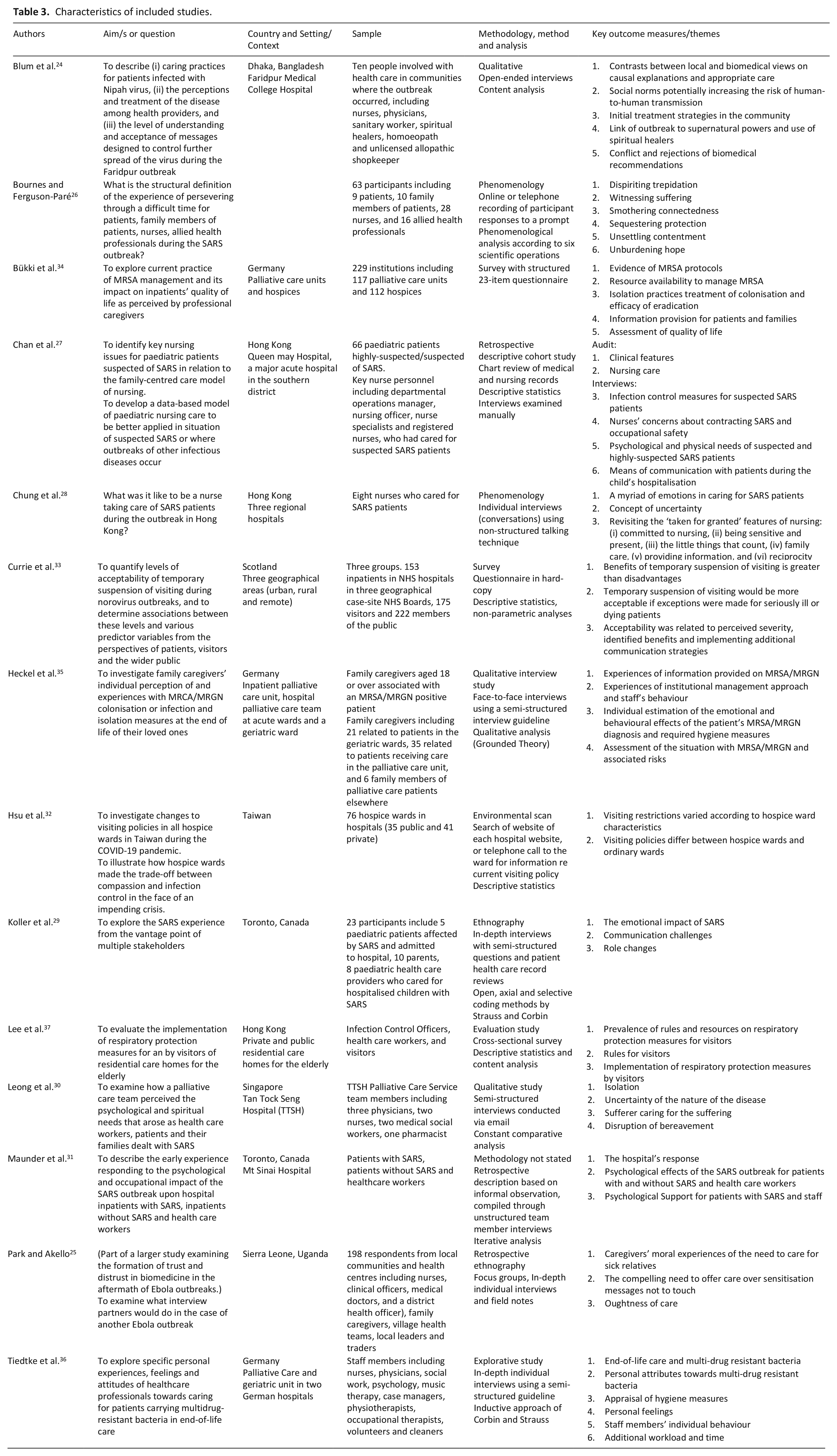
Data were extracted and charted into an evidence table detailing author names, year of publication, country, purpose/aim, design, setting/s and context/s, sample, data collection method/s and key outcome measures/themes (Table 3). Where a study include data related to other samples, settings, only the relevant data were extracted.
Characteristics of included studies.
Data analysis and synthesis
A narrative synthesis approach was used to synthesise data and report study findings. Narrative synthesis is an approach that relies primarily on the use of words to explain and summarise findings. 20 Given the heterogeneity of data between included studies, and that in some cases, only a small portion of the study’s data were relevant to this review, narrative synthesis was considered the most appropriate approach for synthesising findings. Findings were initially grouped according to newly-derived themes by one author and reviewed by the second author. Findings were discussed and revised until both authors agreed in the final findings.
Results
The outcome of the database search is presented in Figure 1.
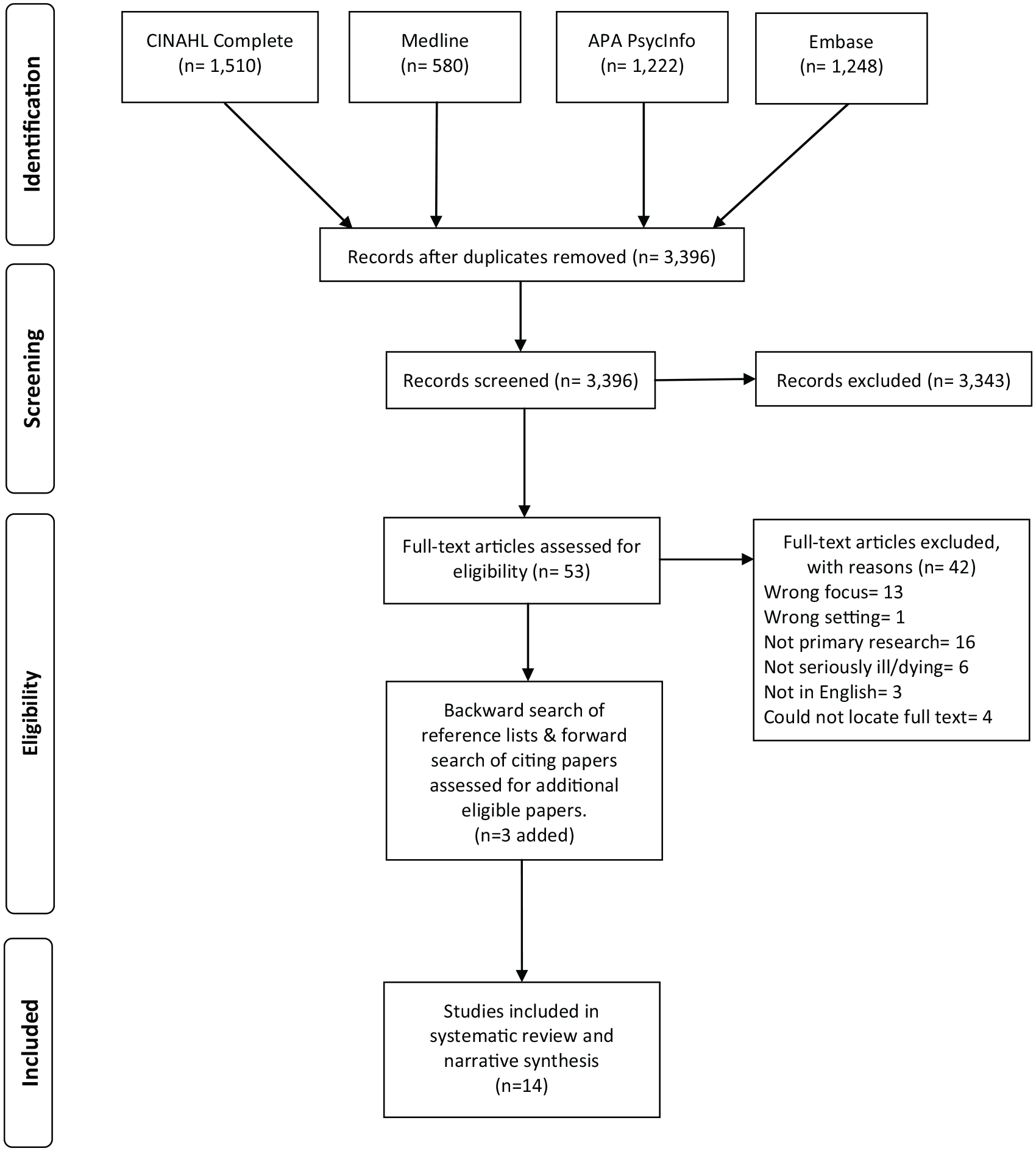
Search outcome.
Characteristics of included studies
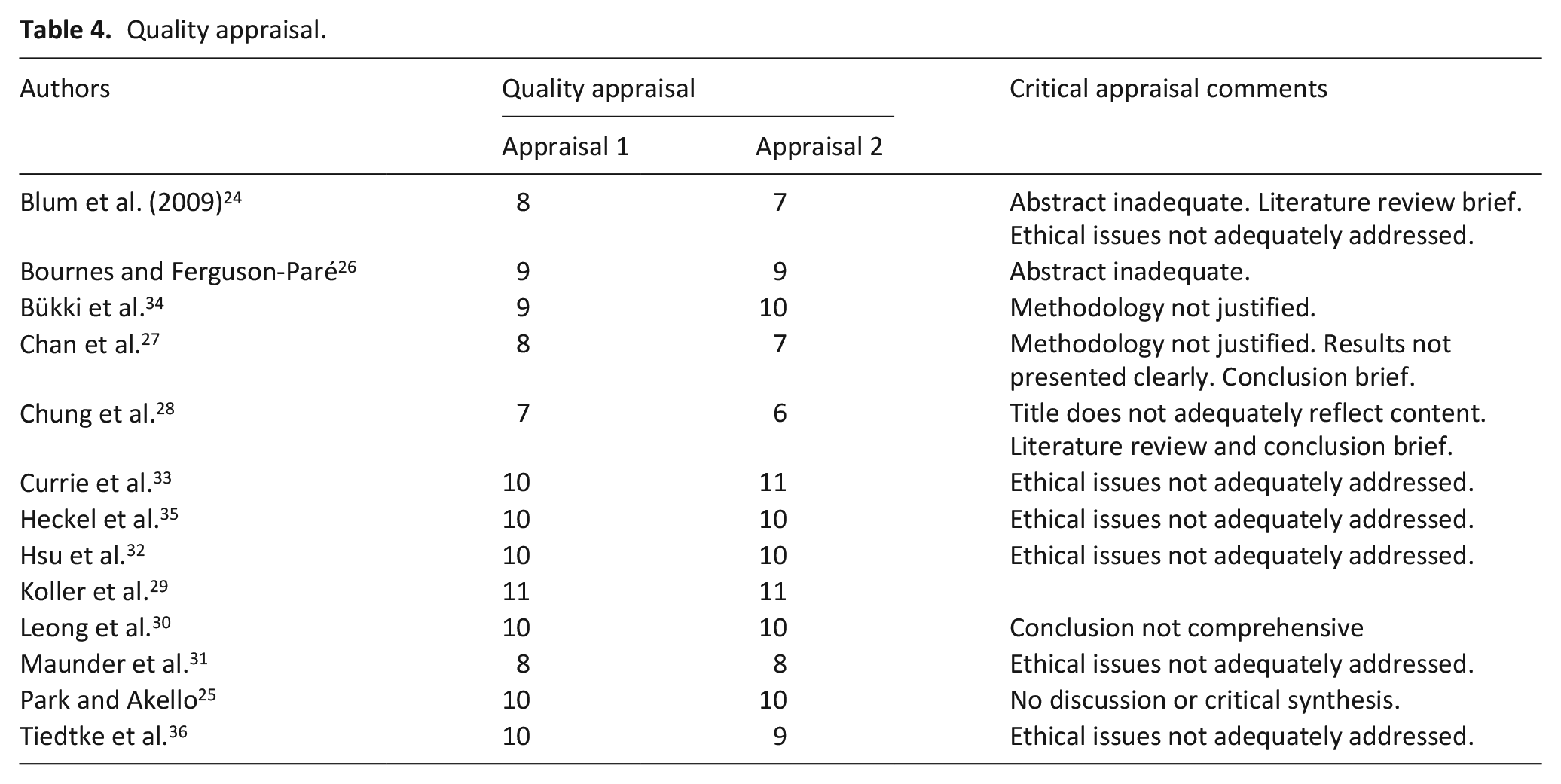
Fourteen papers met the inclusion criteria and were included in this review. Quality assessment scores ranged from 6 to 11 (maximum possible score 11), with both reviewers independently appraising each paper (Table 4). The 14 studies were published between 2003 and 2020. One study related to Nipah Encephalitis, 24 another to Ebola. 25 Six studies related to Severe Acute Respiratory Syndrome (SARS),26 –31 one to coronavirus disease (COVID-19), 32 one to Norovirus, 33 two to Methicillin-Resistant Staphylococcus Aureus (MRSA)34,35 and the final study related to multi-drug resistant bacteria. 35 Three studies were conducted in Canada,26,29,31 three in Germany,34 –36 two in Hong Kong27,28 and single studies were conducted in Uganda, 25 Bangladesh, 24 Singapore 30 and Taiwan. 32 Two studies focused on paediatric patient populations27,29 and three specifically related to palliative care settings and/or patient populations.30,34,36 Nine studies were qualitative in nature, of which eight utilised individual interviews24,26,28 –31,35,36 and one used group and individual interviews 25 to gather data. Three studies were quantitative in nature and used survey34,37 or audit methodology, 32 and the remaining study was a mixed method study utilising interview and audit to gather data. 27
Quality appraisal.
Findings
Studies included in this systematic review provide evidence of family support and care during an infectious disease outbreak, and in particular, where the patients were critically ill or dying. Actions taken to support family members and demonstrate caring include communicating with family members and providing information and supporting family members in spite of restricted or suspended visiting. While personal protective equipment was often necessary for staff, patients, family and visitors, caring was challenged but evident. Family needs and obligations, such as their preferences for involvement and caring, were underpinned by social and cultural norms and belief systems, and were at times, at odds with clinical care requirements and infection control measures. For palliative care and dying patients, exceptions were sometimes made to better meet patient and family needs (Table 5). Each of these key findings are described below.
Study contribution to findings.

Communication and information
The provision of information designed to inform and educate family and visitors about the infectious disease outbreak, and establishing and facilitating communication channels were key features in several studies. This included dissemination of public health messages throughout affected communities.24,25 For example, in an effort to control the spread of Nipah Encephalitis in Bangladesh, one of the public health messages circulated in the community was that that ‘People should avoid direct contact with cases’ (p. 100). 24 In inpatient settings, nurses communicated the importance of hand washing, avoiding direct contact, sleeping and eating with the infected patient to families, 24 as well as requiring families to use personal protective equipment (PPE) including disposable gloves, gowns and face masks 34 as initiatives designed to contain and minimise the spread of infectious disease.
Other studies reported the use of written information for family and visitors. A German study of MRSA management practices across 179 palliative care units and 181 hospices identified that more than two thirds of institutions provided specific information to visitors (p = 0.001) recommending precautionary measures. 34 Another German study of MRSA however, reported that some, but not all families, received information about the diagnosis, therapy and disease transmission and hygiene measures either via a note pinned to a patient’s door or contract precaution material placed in front of the patient’s room. 35 However, these written materials were not always satisfactory, as one family member wrote ‘I also received a brochure but didn’t really understand it fully. It was German. How do you say. Lots of foreign words. Powerless’ (p. 276). 35
Aside from written information, four studies reported on use of the telephone as a primary mode of communication.27
–29,31 Telephone was also used for patient-family communication
31
and to provide progress reports and reassuring families: ‘Family members could receive information on the patient every day even when they were unable to visit. I showed care by being reassuring. I think that the physical and emotional presence of the nurses over the phone in times of crisis is important to family members because it demonstrates that someone cares about them and their relatives’ (p. 515).
28
Telephone communication was reported in two paediatric studies. In one study, a nurse participant expressed that a nurse’s major responsibility was to maintain communication with parents of paediatric patients to provide updates on the child’s progress or condition via telephone, and doctors also provided a daily telephone call to parents on their child’s disease progress.
27
Telephone contact was also described as a key resource in maintaining open and accurate lines of communication and support: ‘You try to keep them in contact in terms of phone conversations . . . so they could directly speak to their parents . . . So we always try to keep that family-centred care’ (p. 54).
29
A parent also described how telephone was used during her son’s admission: ‘Oh, I was constantly on the phone. I never hung up the phone unless the cordless battery started to die. . . he didn’t even hang up the phone at night. The phone stayed off the hook and eventually some time throughout the night the nurse hung it up’ (pp. 54–55).
29
Telephone contact allowed a form of connection between patients and family despite physical separation and was viewed as playing an important role in ‘attenuating the negative impact of infection control procedures’ (p. 55).
29
In reflecting on the impact of communication with family however, one nurse in a study of SARS commented: ‘I didn’t realize that simply having a chance to talk to family members was so important until I handed the wireless phone to an old patient aged 75 to talk to his wife. . . it was unbelievable how his oxygen saturation improved afterwards’ (p. 515).
28
Visiting practices
Several studies described restriction or suspension of visiting during an infectious disease outbreak. In relation to Norovirus, a UK study was conducted to assess the acceptability of suspension of visiting in the event of a norovirus outbreak. Whilst it was acknowledged that there was a societal expectation to visit a sick relative or friend, almost 90% of respondents (n = 492) agreed that it would be more acceptable to close a ward to visitors so long as communication through mobile phones or skype was permitted. 33
Commonly however, visiting practices or policies were changed to prohibit or restrict visitor entry to the healthcare facility. Three studies related to SARS reported visitor restrictions. In Singapore, visitors were allowed for non-SARS patients, but for those with SARS, visitors were only allowed if the patient was deemed seriously ill, and visitors had to don personal protective equipment (PPE), with no physical contact allowed. 30 One participant described ‘They could not be near their loved ones, (or) touch them, (or) whisper to them. Everything had to be done through the cold glass panel’ (pg. 15). 30 Similarly, in Canada, visitor restrictions were described by a family member of a SARS patient as ‘severe’ (p. 329), including visitor line-ups and screening lasting ‘anywhere from 30-45 minutes depending on the number of visitors’ (p. 329). 26 In the same study, other family members reported not being allowed into the hospital at all, as a family member of a patient with cancer (not SARS) described: ‘When we dropped him off at the emergency we were not allowed . . . to accompany him . . . We were unable to visit him during that week because of SARS’. (p. 329). 26 In Hong Kong, paediatric patients with SARS were isolated from nursing staff and their families, with parents not permitted to visit. 27
Two studies reported specifically on hospice and palliative care settings.32,34 In response to the COVID-19 pandemic in Taiwan, an audit of visiting policies of 76 hospice wards revealed that 86.8% (n = 66) implemented a structured visiting policy, 11.8% (n = 9) stopped visiting completely and only one hospice (1.4%) maintained visiting during the study period. 32 Restrictions included limiting the number of visitors at one time to one or two people in 94.0% (n = 63) of settings, limiting the daily visiting slots to one or two time periods per day (89.6%, n = 60) and/or limiting the duration of visiting (83.6%, n = 56). In 17.9% (n = 12) settings, visitor entry was also contingent on the visitor presenting identification documents and an assessment of travel history. 32 In comparison to ordinary wards in the same health facilities, visiting was allowed in the hospice wards but not in the ordinary wards in 75.0% (n = 15) of cases. 32 A survey was also undertaken of MRSA management in palliative care units and hospices in Germany. 34 Of the 117 palliative care units and 112 hospices involved in the survey, precautionary measures were recommended for visitors in 95.6% (n = 219) of settings, and PPE such as disposable gloves, gowns and face masks were used more commonly in palliative care units than hospices (p = 0.000). 34
A UK study used a survey of patients, visitors and members of the public to assess acceptability of temporary suspension of visiting during a Norovirus outbreak. 33 While the majority of respondents (84.6%, n = 462) agreed the possible benefits for closing a ward during an outbreak were greater than the possible disadvantages, 25.8% (n = 141) believed it was wrong as it ignored peoples’ rights to have contact with family and friends. Acceptability was improved if exceptions were made for seriously ill or dying patients (81.6%, n = 444), and when visitors were the patients’ caregivers (52.4%, n = 282). 33
Restricted visiting practices were challenging. For family members, not being able to visit meant some family felt they were unable to provide support to their sick relative.
31
One family member reflected on being separated from her son ‘Standing outside sobbing while they took our son away’ (p. 330).
26
Another described their frustration like this: ‘What is most frustrating about SARS rules is that all of the children live at least 2 hours away from the hospital and to be there at 5 p.m. for visiting hours we drive through rush hour traffic, wait in line anywhere from 30-45 minutes depending on the number of visitors. It cuts into our visiting time. We see mom for about 1 hour approximately and then we have to leave. Because of my mom’s memory problems she forgets why we cannot be there more often or is upset when we have to leave so soon. My mom has had great care, but our biggest worry is that she would think that we have left her there’ (p. 329).
26
Nursing and allied health participants also described witnessing suffering associated with visitor restrictions: ‘Visiting restrictions were a necessary step to protect the health of our patients, but I know they were very difficult for patients and their support, and even more difficult if a loved one got sicker or died during this time’ (p. 328).
26
‘I can understand how hard it must be to be told “you cannot come into the hospital to visit until the patient has been here for more than 12 days”’ (p. 329).
26
Separation between patient and family was described as smothering the connectedness between a dying patient and their family: ‘Mrs P. died alone in isolation. . . Her family sat by their phones waiting for communication from staff having not seen their loved one for a week nor having been able to say goodbye’ (p. 328).
26
In a paediatric setting, the restricted visitation resulted in feelings of helplessness for parents stemming from lack of parental choice: ‘But being separated from them, you know, you almost felt like you lost them. You feel hopeless. . . it’s a hard feeling to be pulled away from them when you realise that you’re not seeing them in a few days. And it’s not your choice’ (p. 55).
29
Personal protective equipment
Four studies specifically described the use and impact of personal protective equipment (PPE). PPE was described as a source of discomfort and alienation
26
and when healthcare professionals showed different attitudes toward hygiene measures and handled these measures differently, this irritated family members and raised their doubts about management of the disease: ‘One time he had to wear a protective garment, the next he didn’t have to. The next day he didn’t have to and then someone told him he would have to. I . . . didn’t really know what was going on or what is right and wrong’ (p. 279).
35
Responses to the need to wear PPE also varied with one family member suggesting ‘psychologically speaking, the “disguise” is a barrier’ (p. 277).
35
Others commented: ‘I don’t really get the rationale behind it. I wear a mask, a cap, gloves and a garment. But then I would also have to protect my feet because otherwise I will carry MRSA out of the room. . . therefore I can’t walk out of the room without MRSA’ (p. 277).
35
‘I do not feel as close to my father due to the protective clothing. I feel restricted, I feel – I don’t know how best to describe it, trapped in a cage’ (p. 279).
35
Staff also acknowledged the downside of PPE by commenting that ‘I would find it extremely burdensome if my relatives were allowed to visit me only in gowns if I were a patient’ (p. 3119).
36
Face masks were also negatively perceived, and thought to inhibit effective communication
29
and comfort, with a family member expressing ‘Feeling uncomfortable and blocked off by the mask’ (p. 329).
26
Staff perceptions on the impact of face masks were also negative: ‘It has been very hard to wear the mask because it cuts down on so much important nonverbal expression . . . Not only did we lose a lot of nonverbal communication but so did the patients. It is harder to build rapport with someone when you are under all these layers. . . I kept smiling, but could they even tell there was a change in my expression under there? Hopefully they saw my eyes crinkle a bit (I often hoped) and realized it was the effect of an exaggerated smile in an attempt to reach out to them’ (pp. 328–329).
26
‘We went in looking like aliens to them and sure, they didn’t recognize us and there’s a lot of times when you try and smile from behind the mask and you realize they can’t see your smile. . . That was one of the hardest things in terms of communication’ (p. 54).
29
Family needs and obligations
Data from the studies included in this review demonstrate that care of family members and honouring their preferences for involvement in patient care were impacted by infection control measures and clinical priorities. Family members’ responses to being confronted with infection control measures for the first time ranged from feeling shocked and irritated to not being affected at all. Some described that they got used to the situation ‘after the first shock’ (p. 276). 35 Yet in another study, the impact was more profound: ‘The stress on our family was unbelievable. It was a horrible and traumatic experience. The treatment of family and caregivers has been ridiculous’ (p. 327). 26 Another commented that the family were ‘Living a nightmare with unbelievable stress’ (p. 330). 26
Despite efforts to communicate key information to family members and the greater community, infection control measures cultural norms and belief systems were challenged. In Bangladesh, supernatural belief systems of the local community contributed to misconceptions about the infectious disease and an unwillingness of family members to subscribe to infection control measures, such as those used in the hospitals. 24 Instead, family members believed that those with Nipah Encephalitis deteriorated in hospital, contributing to lost confidence in the care provided: ‘. . . they knew that they couldn’t make them well. . . If they had not been taken to hospital they would have lived. They killed my son in the hospital’ (p. 98). 24 Advice given to family members about the disease also opposed cultural norms and impacted family’s desired caring role because failing to engage in direct contact was considered equivalent to sending a signal that the person was not important. 24
‘They alerted my by saying that I should be more careful while nursing my husband. They said that it is contagious and I should cover my mouth while going to him. I did not want to do this since I am his wife. Would I cover my mouth with my hands or take care of him? . . . he did not smell badly, then why would I put the cloth to my nose and mouth? No matter what, he was my husband. He would get upset if he saw me covering my mouth’ (p. 99).
24
In a Ugandan study of Ebola, family members’ cultural and moral obligations towards the sick person, meant family members provided care in direct violation of the preventive measures prescribed by the official Ebola response: ‘When the healthcare workers in Lacor saw that my brother was now badly off with Ebola, as he was sweating and bleeding everywhere, they started to avoid him. That is when I stepped in and started doing my best. . . all this time not minding about all the messages we had heard’ (p. 63).
25
‘. . . many people with children and close relatives in Lacor Hospital forgot about some of the preventive measures in order to take care of their relatives . . .“If I die with my daughter, then let us die together”’ (p. 63).
25
In some studies however, the care provided for family members, was reported positively. In a study of SARS, despite one nurse participant describing how masks resulted in ‘covering smiles, compassionate expressions, trembling lips, and tears’ (p. 328),
26
family members described ‘experiencing caregivers that are patient despite pressure’ (p. 331) and caregivers who demonstrated ‘welcoming kindness, patience and humour’ (p. 331). Another explained: ‘I feel welcome. I guess it’s because under the plexiglass and above the masks there are crinkles around the eyes, an extension of the smiles that are hidden by the masks. I did expect professional care and concern but did not anticipate the kindness and the sense of humor. I did not realise you can see smiles under masks’ (p 331).
26
These findings match with a nurse’s comments from caring for family members: ‘I think that the physical and emotional presence of the nurses over the phone in times of crisis is important to family members because it demonstrates that someone cares about them and their relatives’ (p. 515).
28
In paediatric settings where the focus was on the provision of family-centred care, identifying families’ needs, offering an opportunity to express feelings and supporting effective coping strategies helped to enhance the families’ sense of competence and control were key,
31
but not universally possible. In a paediatric study conducted in Hong Kong, nurses reported that their care of patients suspected of SARS was in conflict with the usual family-centred nursing practices in the ward.
27
Stringent infection control measures overshadowed family-centred care, with family participation minimised as no visitors were permitted, ‘a policy that clearly exacerbated anxiety in the children as well as the parents’ (p. 24).
27
Nurses also reported that parents worried about the child’s safety, loneliness and fear stemming from their isolation, creating conflict between nurses and parents and aggravated parents’ anxiety.
27
Similarly, concerns were also expressed in a Canadian paediatric study relating to the impact of separation, isolation, loss of choice and how opportunities for supportive relationships and confidence building were prevented: ‘Being separated from them, you know, you almost felt like you lost them. You feel hopeless. . . . It’s a hard feeling to be pulled away from them when you realise that you’re not seeing them in a few days. And it’s not your choice’ (p. 55).
29
Dying and bereavement
Infection control measures also impacted dying and bereavement. Some studies reported staff were willing to find compromises to support patients and families.32,34 For example, in Taiwanese hospice and palliative care settings where almost 90% implemented structured visiting policies to stop visiting completely, limit the number of visitors or limit the duration of visits, 32 visiting was allowed for dying patients. Similarly, in German hospice and palliative care settings, visitors were still allowed so long as visitors wore PPE as a precaution. 34 Alternately, while no detail was provided on how infection control practices might be altered, other studies indicated there was clear support for the notion that exceptions should be made when the patient was seriously or terminally ill.32,33
In other studies however, the negative impact on the family and visitors of dying patients was described. In recounting the impact of restrictions to visitors for a terminal cancer patient at the time of the SARS epidemic, one healthcare professional commented: ‘. . .I saw him walk out and sit in the common area and cry quietly to himself. Nobody was there to be with him’ (p. 15).
30
The impact of infection control for family of dying patients was also exemplified in other studies: ‘You can touch him [the patient], but with gloves it’s something completely different. . . that’s an additional constraint which isn’t nice, especially at the end of life’ (p. 3118).
36
‘Visiting restrictions . . . were very difficult for patients and their support, and even more difficult if a loved one got sicker or died during this time’ (p. 328).
26
One study described that not helping family prepare for death was thought to be cruel, inhibiting satisfactory completion of the process of death.
30
In this way, conflicting principles of isolation and end-of-life care meant that saying goodbye was disturbed, potentially complicating the bereavement, amplifying burden and prolonging grief.
35
Similarly, bereavement was disrupted when family members were not able to support each other in their grief or bid their farewells.
30
Respect at the point of death was also compromised as funeral arrangements were dictated more by law than by choice.
30
For example, mandated requirements for handling of the deceased and for immediate burial or cremation interrupted bereavement: ‘Families could not claim the body for wakes. The lid of the hermetically-sealed coffin could not have a window. Informants perceived this as a disruption of the bereavement process. Families do not get to pay their last respects. This is often seen as an undignified death, a ‘poor’ death. I think the elderly may have more difficulty accepting this practice, as there would be no sense of closure’ (p. 16).
30
Discussion
The findings of this systematic review highlight several important points about the impact of the response to infectious disease outbreaks for palliative care providers and what can be learnt from this both in relation to COVID-19 and other possible epidemics or pandemics. While there is no doubt that public health and infection control measures are necessary for risk reduction, this review provides clear evidence that these measures are perceived and experienced differently by family members of critically ill and dying patients impacted by the measures, to how they were intended. Infection control measures not only manifested as physical barriers between family members and the patient, but also a psychological barrier disrupting family connection with the patient.
Grounded in recognition of the family as a social unit connected by blood and/or kinship, emotional and legal relationships, 38 extending care to family is more, not less important in times of crisis 39 and essential to maintaining humanity and compassion in care. 40 Under normal circumstances, when a person is critically ill or dying, family members have social and cultural obligations associated with the family connection 41 ; they want to stay close, 42 keenly observe, protect and comfort. 13 Dying is seen as a time of poignancy and intimacy for family, 13 highlighting the importance of bedside vigils, in-person farewells and family involvement in preparing the body. 43 Even when social and familial practices are re-shaped by legal, behavioural and social interventions designed to contain an infectious disease outbreak, 43 family members’ desires to maintain these practices do not cease. Disruptions to rituals before and after death and a lack of social support compounds family members’ grief. 44 Thus, the potential for complicated and protracted grief, and other negative psychological consequences for family members are also significant.1,16,41 When public health and infection control measures remove or limit opportunities for family members to provide support and be comforted by closeness to the patient, and to be supported themselves, the onus is on care providers to find creative and innovative solutions to address family members’ needs. At the very least, acknowledging that family members, who are an extension of the patient receiving care, are suffering and may have unmet needs is fundamental, and a central tenet to palliative care. 45
Given that not all infectious disease outbreaks can be entirely anticipated, such as the COVID-19 pandemic, forward planning so that every concern is anticipated is not feasible. But, rather than taking the purely risk-averse approach to care at the end of life, which is dictated by public health and infection control measures, care providers must also have the courage to be creative in addressing palliative care challenges, 46 which includes acknowledging the significance of individual deaths and ensuring multiple approaches to ensure the bereaved are supported. 47 The findings of this review reinforce, that communication and the provision of information remain as a key source of support for family members. Therefore, establishing alternate methods for communication according to family needs and preferences 48 and protection of the patient-family connection whilst also adhering to public health and infection control measures is a logical way forward. As identified in this review, facilitating telephone communication between patient and family, and for daily updates from care providers was perceived positively by family members as a key source of support, particularly because it assisted to maintain family involvement and connection to the critically ill or dying person. Innovative ways of doing this in fast-paced environments with severe staffing challenges must be shared, and it may be that trained volunteers could have important roles. 49
Cultural perspectives, such as how culture influences family caregiver roles, cultural beliefs and rituals has emerged as an important factor in COVID-19 and the family caregiver response, especially when someone is dying. Culture here is understood as the customs, values, beliefs, knowledge and language of a society or a community, including shared patterns of behaviours, interactions and understandings that are learned by socialization. 50 More broadly, commentators have suggested differences in response to COVID-19 which can be characterised as a (mostly) Western cultural individualistic or independent response, versus a (mostly) Asian cultural collective or interdependent response.51,52 Such societal responses are also intertwined with differences in cultural norms and responses to family caregiving, with differences in filial obligations and beliefs being commonly observed.53 –55 These cultural factors have a number of implications. First, findings from studies conducted in one (dominant) culture may not easily translate to other cultures if there are differences in what may be perceived as acceptable or reasonable in policy or practice terms from an individual, organisational or societal perspective. Second, such findings may not take account of the cultural norms and expectations of minority or marginalised populations, which may lead to disadvantage or inequality. 56 Third, broad cultural characterisations may mask the individual responses and needs of patients and their family caregivers. The challenge is in using research evidence from a range of cultural perspectives to inform policy and practice in a way that respects the context in which the evidence was generated, takes account of the cultural milieu in which the policy will be enacted, and is appropriately and safely responsive to the needs of individual families.
Strengths and limitations
This systematic review is the first to examine how family members of patients who are seriously ill or who die during infectious disease outbreaks are supported and cared for during serious illness, before and after patient death. Limited data was available to describe the factors that influence family presence around the time of death.
The search was comprehensive and broad. Multiple databases were used to identify studies from any year and with any study design, published in English that contributed to addressing the aims of this systematic review. As a result, it is possible that relevant research published on other languages may have been missed.
Given that only 14 papers met the inclusion criteria, none were excluded on the basis of quality scores. As a result, the findings of this review were derived from research papers of diverse quality. Many studies were conducted in single settings, with small samples, such that care will need to be taken in judging whether the experiences described are specific to the context of the study or have a wider applicability. Care has been taken in this synthesis to consider the context of the included studies, such as the setting, infectious disease challenges and resources available (personal, social and institutional) to address these challenges, but then focus the synthesis on what appear as fundamental lessons for improving support of family carers.
Conclusion and recommendations
The studies included in this review are heterogeneous in terms of setting, location, infectious disease and the resources available to address the challenges posed. It is important that these differences are recognised, with a nuanced consideration of the transferability of some findings. Nevertheless, the synthesis presented here reveals what appear to be fundamental or essential considerations when supporting family members when someone is ill enough to die; prioritising communication and human contact as safely as possible. Family members are at high risk of negative psychological impacts from their experiences and interruption of the patient-family connection. Not only are palliative care providers integral to the holistic care of critically ill and dying patients and their family, but also for the expertise in providing grief and bereavement support and advise to care providers in other specialties and settings. Demonstrating support and caring for family members through regular information and facilitating communication with care providers and the patient is fundamentally important. Care providers with innovative solutions to supporting family members and maintaining the patient-family connection during infectious disease outbreaks need to share solutions urgently to allow effective spread of learning.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211029515 – Supplemental material for Smiles behind the masks: A systematic review and narrative synthesis exploring how family members of seriously ill or dying patients are supported during infectious disease outbreaks
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211029515 for Smiles behind the masks: A systematic review and narrative synthesis exploring how family members of seriously ill or dying patients are supported during infectious disease outbreaks by Melissa J Bloomer and Catherine Walshe in Palliative Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.