
Abstract
Background:
The death of a loved one is considered as one of the most stressful life events. During the COVID-19 pandemic, grief processes are potentially affected by measures such as social distancing and self-quarantine.
Aim:
The aim of this study was to give insight in the impact of the COVID-19 pandemic on quality of life, social support, and self-care of bereaved relatives of people with advanced cancer in order to evaluate whether care for bereaved relatives during the COVID-19 pandemic should be improved.
Design:
A cross-sectional analysis using data from bereaved relatives of a prospective, longitudinal, multicenter, observational study on quality of care and quality of life of people with advanced cancer and their (bereaved) relatives (eQuiPe).
Setting/participants:
Quality of life, social support, and self-care of bereaved relatives who completed a questionnaire within 3–6 months after their relative died during COVID-19 (April-November 2020) were compared with bereaved relatives who completed this questionnaire pre-COVID-19 (April-November 2019).
Results:
Ninety-one bereaved relatives were included in the analysis, 44 bereaved relatives completed the questionnaire pre-COVID-19 and 47 during COVID-19. The median age of the participants was 65 (IQR = 14) years and 58% were female. There were no significant differences between the pre-COVID-19 and during COVID-19 bereaved relatives in quality of life (68 vs 69), social support (17 vs 18), and self-care (20 vs 19).
Conclusions:
On the short-term, the COVID-19 pandemic did not have significant impact on bereaved relatives’ wellbeing. However, long-term impact of the pandemic on their wellbeing should be assessed.
Self-care and social support are positively related with better grief outcomes.
Grief processes may be influenced due to safeguards during the COVID-19 pandemic.
This study demonstrates that on the short term, the COVID-19 pandemic does not appear to have an impact on the quality of life, social support, and self-care of bereaved relatives.
Future study is recommended to investigate the long-term impact of the COVID-19 pandemic on bereaved relatives of people with advanced cancer.
Palliative care professionals, grief counselors, and policy makers should pay attention to the support of bereaved relatives, since there are still improvements to make in the support of bereaved relatives, regardless of the pandemic.
Introduction
The death of a loved one is considered as the most stressful of all life events. 1 Grief is the normal reaction to loss, particularly to the loss of a loved one. The coronavirus disease 2019 (COVID-19) pandemic affects most aspects of life, including experiences of end-of-life care and bereavement. 2 Due to COVID-19, restrictive measures are in place in the Netherlands, such as social distancing, self-quarantine, and restricting the number of visitors. These may have influenced grief processes. 3 For instance, social distancing and self-quarantine can result in a lack of practical and emotional support for bereaved relatives and can intensify the feeling of loneliness, which is part of any bereavement experience.4,5 Lower levels of social support may result in worse grief outcomes, with signs of complicated grief, depression, and PTSD.6–8 Self-care can also be hindered by COVID-19 since social activities are restricted. Self-care can be defined as a process of purposeful engagement in practices that promote overall health and well-being of the self. 9 Low scores in self-care can lead to anxiety, depression, and mental health. 10
The aim of this study was to give insight in the impact of the COVID-19 pandemic on the experienced quality of life, social support, and self-care of bereaved relatives in order to evaluate whether care for bereaved relatives during the COVID-19 pandemic should be altered. This is important to know since a worse quality of life of bereaved relatives due to the pandemic, can result in more people suffering from depression or complicated grief, which can increase the societal impact including health care use.
Methods
Study design
A cross-sectional analysis was conducted, using data of bereaved relatives participating in a prospective, longitudinal, multicenter study on quality of care and quality of life of people with advanced cancer and their relatives (eQuiPe). 11
Population
People with advanced cancer were recruited in 40 Dutch hospitals between November 2017 and January 2020. 11 Advanced cancer was defined as a diagnosis of a solid metastasized tumor (stage IV).
Sampling
Health care professionals of participating hospitals identified patients who met the inclusion and exclusion criteria. Health care professionals handed out a patient information leaflet and asked eligible patients if they could be approached by the research team. The patients were asked whether his/her relative may be approached. There was also the possibility of self-referral.
Recruitment
Patients and relatives were contacted by phone by the research team to discuss study participation.
Setting
Bereaved relatives completed a questionnaire 3–6 months after their relative with advanced cancer died, regarding quality of life, post-bereavement needs and support, experiences with care in the last months of life of the patient, and the patient’s quality of death. The pre-COVID-19 group consisted of bereaved relatives who completed the questionnaire between 1 April 2019 and 30 November 2019. The during COVID-19 group completed the questionnaire during the COVID-19 pandemic, between 1 April 2020 and 30 November 2020. April 1st was used as cut-off to ensure that responses referred to during the COVID-19 pandemic, since the questionnaire referred to experiences of the “past week” and the COVID-19 pandemic restrictions started on 15 March 2020 in the Netherlands.
Ethical considerations
The ethics committee of the Antoni van Leeuwenhoek hospital (METC17.1491) has reviewed the study and exempted it from medical ethical review, according to the Dutch Medical Research Involving Human Subjects Act (WMO). All participants signed written informed consent before completing the paper or online questionnaires via PROFILES. 12
Measures
The three outcome measures used in this study were quality of life, self-care, and social support. Characteristics of the bereaved relatives were collected by self-developed questions (Supplemental Material 1). Quality of life was measured with the emotional functioning- (4 items), social functioning- (2 items), and global quality of life scale (2 items) of the European Organization for Research and Treatment of Cancer quality of life questionnaire C30 (EORTC QLQ-C30). 13 Self-care was measured with the Personal Self-care subscale (9 items) of the short version of the Self-care Practices Scale (SCPS), including participation in physical and spiritual activities and spending quality time with others.14,15 Social support was measured with the social subscale (6 items) of the Functional Assessment of Cancer Therapy Scale General. 16
Statistical analysis
Descriptive statistics were used to analyze the characteristics of bereaved relatives, using mean (SD) or median (IQR) for continuous variables and percentages for categorical variables. Statistical differences were tested with Pearson’s χ2 (categorical variables), independent t-test and Mann-Whitney U test (continuous variables). Statistical significance was set at p < 0.05.
In a sensitivity analysis the effect of becoming bereaved during the COVID-19 pandemic was compared with becoming bereaved before the COVID-19 pandemic. The sensitivity analysis was performed within the during COVID-19 group, based on date of death, while the main analysis was based on the completion date of the questionnaire. The participants within the during COVID-19 group were divided into participants who became bereaved before 15 March 2020 and after 15 March 2020. All statistical analyses were performed with Stata 16 (StataCorp LLC, College Station, Texas) statistical software.
Results
Characteristics of bereaved relatives
Ninety-one bereaved relatives were included in the analysis. The median age of the participants was 65 (IQR = 14) years and 58% of the participants was female. About 81% of the bereaved relatives lost their partner, 12% lost a parent, 2% was other family, 2% lost a friend, and 2% had another relationship with the patient. Forty-four bereaved relatives completed the questionnaire pre-COVID-19 and 47 during the COVID-19 pandemic (Figure 1). The groups did not differ significantly in age, gender, relationship with patient, and circumstances of the patients’ death (Table 1).
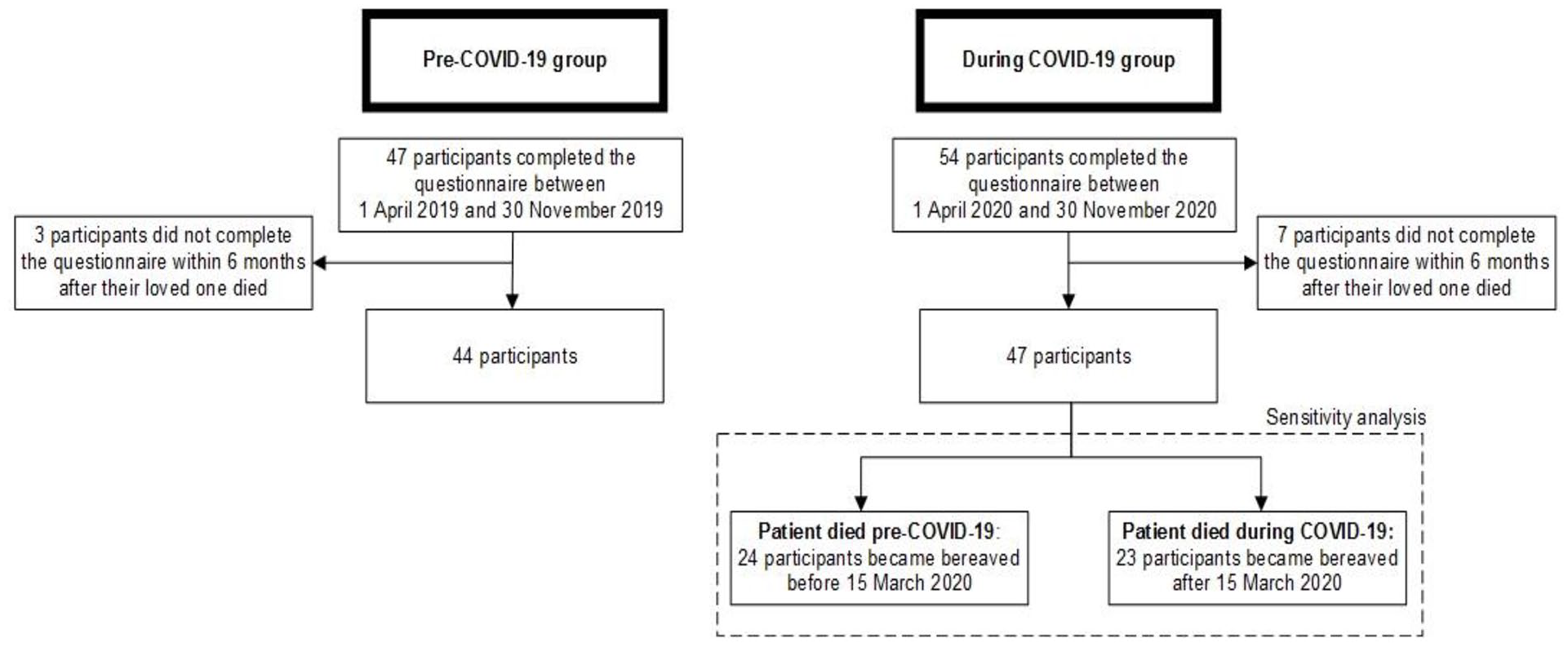
Flowchart.
Characteristics of bereaved relatives and patients death (n = 91).
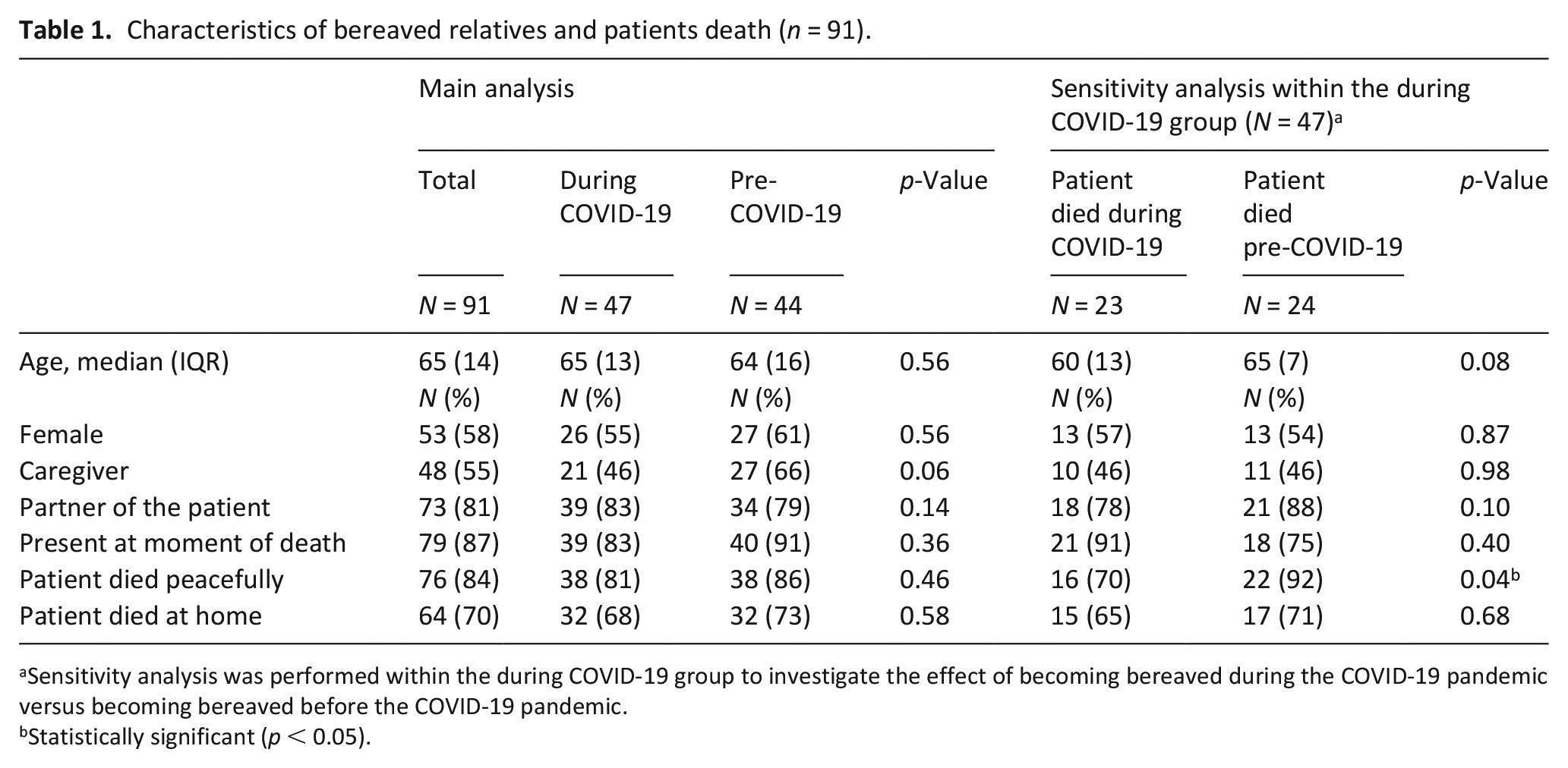
Sensitivity analysis was performed within the during COVID-19 group to investigate the effect of becoming bereaved during the COVID-19 pandemic versus becoming bereaved before the COVID-19 pandemic.
Statistically significant (p < 0.05).
In the during COVID-19 group, 24 participants became bereaved before COVID-19 and 23 during COVID-19. Fewer participants (70%) who became bereaved during COVID-19 experienced the patients’ death as peaceful compared to participants who became bereaved before the pandemic (92%; p < 0.05).
Quality of life of bereaved relatives
The during COVID-19 group and the pre-COVID-19 group did not differ in global quality of life, emotional functioning, social functioning, experienced social support, and self-care (Table 2). The sensitivity analysis confirmed that participants who became bereaved during COVID-19 did not differ from those who became bereaved pre-COVID-19, except for self-care. Self-care was higher in respondents who became bereaved during COVID-19 compared to those who became bereaved before the pandemic (p < 0.05), indicating that the latter participated less in self-care activities.
Quality of life of bereaved relatives (n = 91).
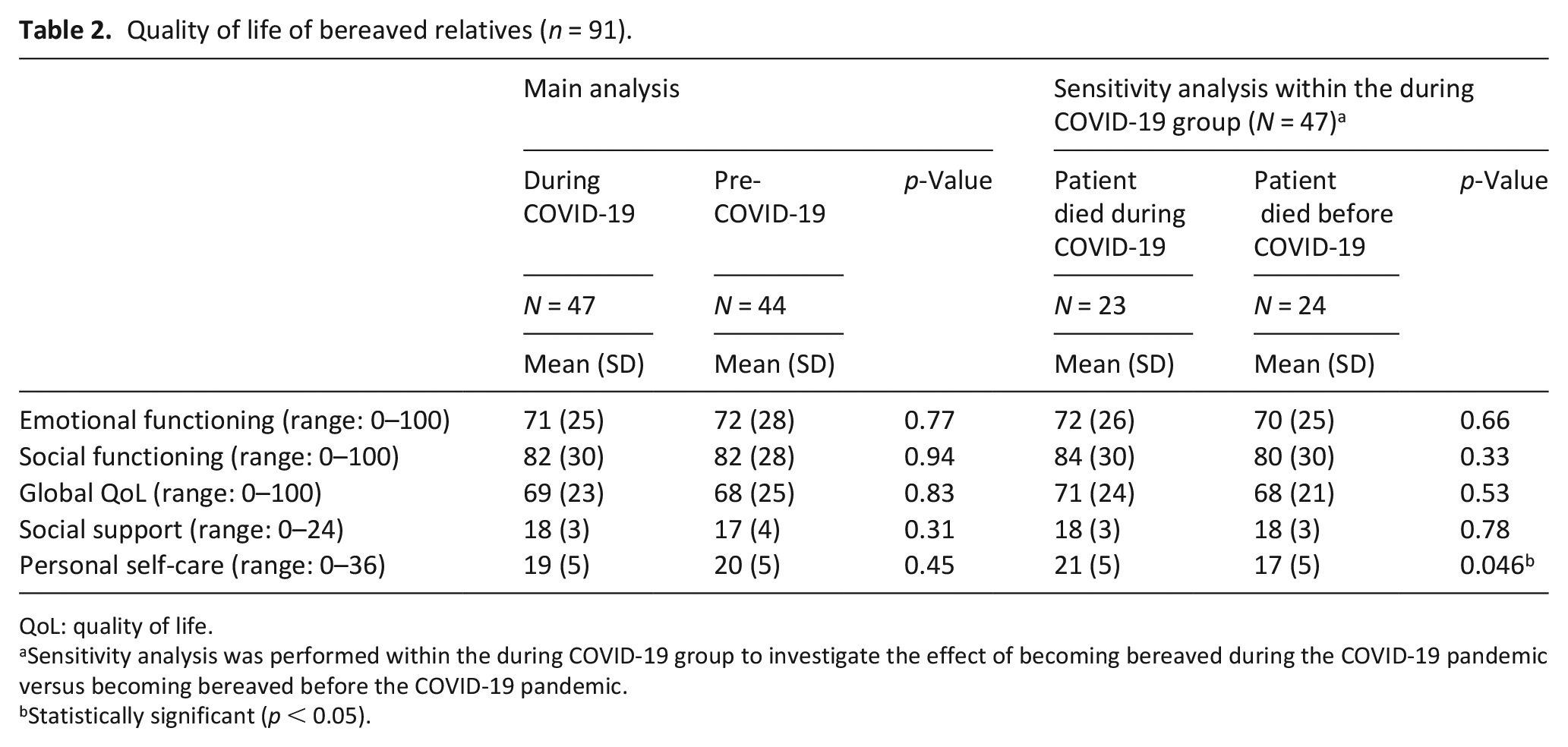
QoL: quality of life.
Sensitivity analysis was performed within the during COVID-19 group to investigate the effect of becoming bereaved during the COVID-19 pandemic versus becoming bereaved before the COVID-19 pandemic.
Statistically significant (p < 0.05).
Discussion
In this study among 91 bereaved relatives who participated before or during the COVID-19 pandemic, we found no differences in the scales of quality of life, self-care, and social support. These findings are in line with a Dutch study that found no differences between grief levels of bereaved relatives who participated before and during the COVID-19 pandemic and whose loved one died a non-COVID-19-related death. 17 However, in a secondary analysis, they found that people who became bereaved during COVID-19 experienced more severe grief than people who became bereaved before COVID-19. In contrast, in our sensitivity analysis no differences were found in quality of life between people who became bereaved before or during COVID-19. These findings can be explained by the differences in outcome measures (grief severity vs quality of life), although it is known that grief reactions are closely related to quality of life dimensions. 18
Some explanation for the absence of differences in quality of life of bereaved relatives pre- and during COVID-19 are present. First, the patients in our study died of cancer, while most studies assess experiences of bereaved relatives of patients who died of COVID-19. The death of the patients in our study was expected, therefore, the bereaved relatives were more prepared to lose their relative, which is associated with lower levels of grief. 19 Second, 70% of the patients died at home, without the strict rules of a hospital or nursing home. Bereaved relatives were able to be present at the time of death and to say goodbye, which is important for relatives according to recent studies investigating the effect of the pandemic on bereaved relatives.2,20–22 In the sensitivity analysis we found that fewer participants who became bereaved during COVID-19 experienced the patients’ death as peaceful compared to participants who became bereaved pre-COVID-19. This can be a risk factor for distress, 23 but the groups did not differ in quality of life. Third, grieving during the pandemic might have benefits, as the forced isolation provided bereaved relatives time and space to grief and recognize their coping skills and personal resilience. 24 Fourth, restricted social contacts and limited freedom of movement might have less impact on bereaved relatives. A recent study showed that patients with cancer reported less loneliness during the COVID-19 pandemic than the general population. 25 This might also hold for bereaved relatives.
In our study, only the short-term effects of the COVID-19 pandemic on bereaved relatives were investigated. We cannot rule out any long-term effect of the COVID-19 pandemic on quality of life of bereaved relatives, as suggested by other researchers, who based their assumptions on expert assessment of prior bereavement research and professional experience.8,19,21–23,26–30 Therefore, we recommend a future study to investigate the long-term impact of the COVID-19 pandemic. Besides, we believe that there are still improvements to make in the support of bereaved relatives, regardless of the pandemic. Therefore, palliative care professionals, grief counselors, and policy makers should pay attention to the support of bereaved relatives.
Strengths and limitations
This is one of the few cross-sectional studies examining quality of life of bereaved relatives after a cancer-related death before and during the COVID-19 pandemic. Therefore, this study can give insight in the impact of the COVID-19 pandemic on quality of life in comparison with pre-COVID-19 bereavement. This in contrast with most other studies, where the information about the quality of life of bereaved relatives who grieved before the pandemic is lacking. It is possible that bereaved relatives with higher quality of life were more likely to complete the questionnaire compared to bereaved relatives with lower quality of life (selection bias). Second, as this was a cross-sectional study, we compared quality of life between subgroups of bereaved relatives and did not gain insight in the course of quality of life before and during COVID-19.
Conclusion
On the short term, the COVID-19 pandemic does not appear to have an impact on the quality of life, social support, and self-care of bereaved relatives. However, improvements can be made in the support of bereaved relatives, regardless of the COVID-19 pandemic.
Footnotes
Authorship
All authors made substantial contributions to this review. The data was collected by LH and JvR. LH analyzed the data and interpreted the data. All authors critically revised the manuscript for important intellectual content and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The eQuiPe study is funded by the Roparun Foundation
Research ethics and patient consent
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Medical Research Ethics Committee of the Antoni van Leeuwenhoek hospital, Amsterdam, the Netherlands (METC17.1491).
ORCID iDs
Data management and sharing
Since 2011, PROFILES registry data is freely available according to the FAIR (Findable, Accessible, Interoperable, Reusable) data principles for non-commercial (international) scientific research, subject only to privacy and confidentiality restrictions. The datasets analyzed during the current study are available through Questacy (DDI 3.x XML) and can be accessed by our website (www.profilesregistry.nl). In order to arrange optimal long-term data warehousing and dissemination, we follow the quality guidelines that are formulated in the “Data Seal of Approval” (![]() ) document, developed by Data Archiving and Networked Services (DANS). The data reported in this manuscript will be made available when the eQuiPe study is completed.
) document, developed by Data Archiving and Networked Services (DANS). The data reported in this manuscript will be made available when the eQuiPe study is completed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.