
Abstract
Background:
The WHO definition of palliative care includes bereavement support as integral to palliative care, yet a previous survey of bereavement support in palliative care in Europe has shown a range of service responses to loss. A rigorous approach to agreeing and implementing a palliative care bereavement framework was required.
Aim:
The aim of this study was to develop consensus on best-practice recommendations for bereavement care principles, structures, processes and delivery based on current practice and evidence.
Design:
In accordance with Guidance on Conducting and Reporting Delphi Studies, a consensus-building five-round Delphi technique was performed. A scoping review of research literature informed drafting of 54 statements by the EAPC Bereavement Task Force. Evaluation of the statements was performed by an expert panel using a 5-point Likert scale. ⩾80% agreement were defined as essential items and 75%–79% agreement were defined as desirable items. Items with a consensus rating <75% were revised during the process.
Setting/participants:
The Delphi study was carried out by an expert panel among membership organisations of the European Association for Palliative Care.
Results:
In total, 376 email requests to complete Delphi questionnaire were distributed with a response rate of 23% (n = 87) and a follow-up response-rate of 79% (n = 69). Of the initial 54 statements in six dimensions, 52 statements were endorsed with 26 essential statements and 26 desirable statements.
Conclusions:
The six dimensions and 52 statements agreed through this Delphi study clarify a coherent direction for development of bereavement services in palliative care in Europe.
Previous studies show a lack of consensus about appropriate bereavement support in palliative care, hence, a rigorous approach to agreeing and implementing a bereavement framework was required.
A Delphi study achieved consensus on a set of best-practice recommendations for bereavement principles, structures, processes and delivery based on current practice and evidence.
Services can now develop their bereavement care principles, structures, delivery and governance by addressing the core recommendations across six dimensions.
Background
The WHO definition of palliative care includes bereavement support as integral to palliative care, yet little is known about bereavement support in palliative care. Grief is a natural response to loss, a dynamic and situated process, experienced within a family, social and cultural context.1–3 A small proportion experience severe difficulties and develop health problems.4–6 To identify this group, a syndrome called ‘Prolonged Grief Disorder’ has been included in the International Classification of Disease – 11. 7 Tiered models describe grief as a process of adaptation and while distress is common, extended disruption and functional impairment occur in a minority of people. Responses should be linked to the relevant tier. These models come from the public health approach based on reviews of bereavement research in the US, Europe and Australia8–11 and the UK National Institute for Clinical Excellence 12 guidelines for palliative and supportive care derived from a systematic review conducted in 2004. These models offer a structure within which bereavement support can be considered, designed and operationalised in palliative care. They emphasise the importance of targeted support and explicitly value the support of social networks and communities. Standards developed for general bereavement care in the UK acknowledge these models 13 as do palliative care bereavement standards from Australia.14,15 Neither define bereavement nor the scope of bereavement care in palliative care.
While support for bereaved people is a core part of palliative care, services have largely developed in response to demand for support rather than from an evidence base. 16 A European Association for Palliative Care (EAPC) survey of bereavement support in palliative care identified that while 18% of respondents representing palliative care organisations and services reported having no formal service, the majority (82%) described a range of service responses to loss. 17 Where these supports were available, it was less clear how they were offered, and what, if any, guiding principles such as those suggested in the tiered approach were applied. The survey results also showed that few services had national or local policy informing the provision of bereavement care, with limited reference to research and clinical literature. Few bereavement-specific roles were noted, with variation in the provision of bereavement education. 17 Hence, a rigorous approach to agreeing and implementing a palliative care bereavement framework is required. An EAPC Bereavement Taskforce undertook the study (see author list). The aim of this study was to develop best-practice recommendations by performing a Delphi study among EAPC organisations to formulate recommendations for bereavement care principles, structures, processes and delivery based on current practice and evidence and to establish a consensus on these recommendations.
Methods
A Delphi technique was chosen to identify shared priorities and integrate routine clinical practice and expert knowledge. 18 Consensus-building is important if recommendations are to be appropriate and relevant to a range of different service types at various stages of development. In accordance with Guidance on Conducting and Reporting Delphi Studies (CREDES), it acknowledges the value of expert knowledge and supplements evidence, given the lack of clinical trials in bereavement care. 18 To be successfully implemented recommendations need to address the issues and experiences of clinicians. Finally, we aimed for the recommendations to be relevant to all of the constituents of the EAPC and a Delphi allows for this to be demonstrated through establishing consensus.
Planning and design
To initiate the Delphi study, a five-member expert advisory group (EAG) was convened by the bereavement Task Force to advise on definitions, the study approach and to minimise bias. The EAG members represented international (Canada, the Netherlands, UK, Australia) clinical and academic expertise and advised on research, service and policy aspects of bereavement care broadly and specifically, for palliative care.
Procedure
The Delphi study comprised five rounds of drafting statements, survey and feedback to comply with the CREDES recommendations. 18 A flow chart of the Delphi rounds is presented in Figure 1.
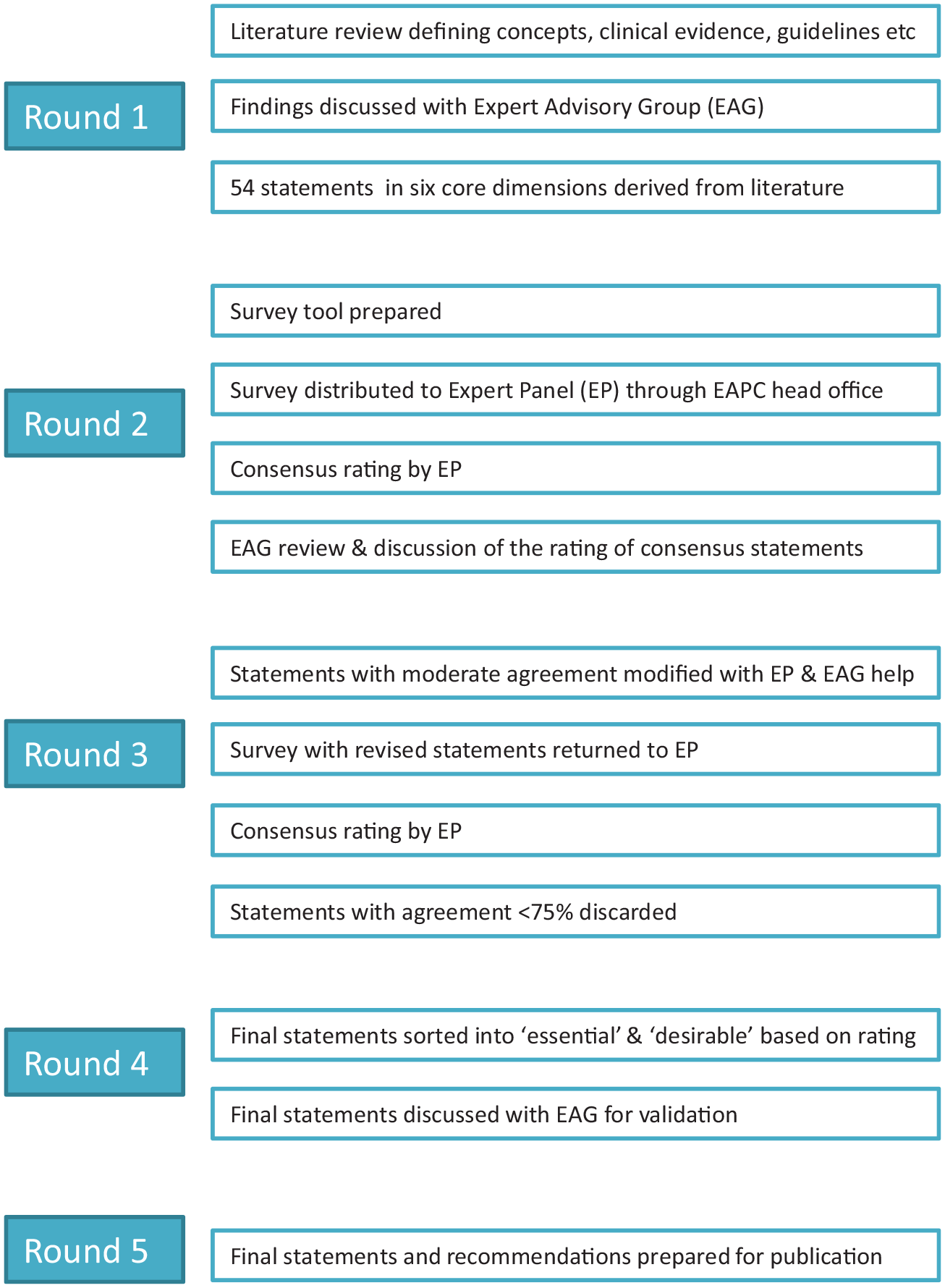
Flow chart of Delphi study approach.
Delphi Round 1
We performed a narrative literature review incorporating research sources and results of our 2015 survey of EAPC palliative care services.17,19 The narrative incorporated models for bereavement care and studies on palliative care-specific bereavement support as well as systematic reviews on interventions and predictors of complicated grief up to 2016. This review discussed at an open meeting of EAPC Congress in 2015 and endorsed by the EAG, constituted the knowledge-base for the structure and drafting of the Delphi consensus statements.
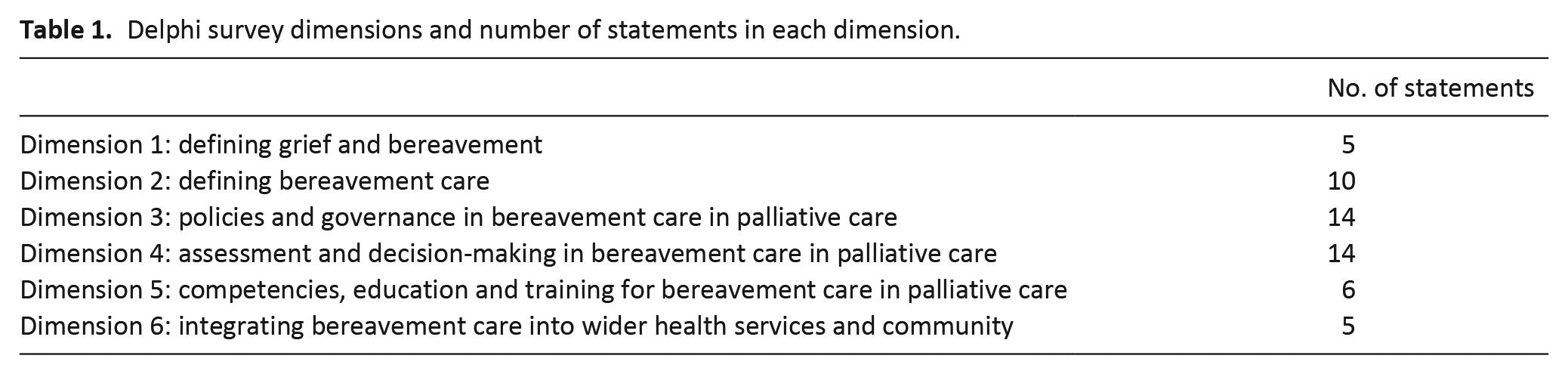
Six core dimensions were devised and for each dimension recommendation statements were drafted in accordance with the literature review and subsequent discussions (Table 1). The draft dimensions and statements were piloted among a small group of EAPC stakeholders for comprehension and distribution methods.
Delphi survey dimensions and number of statements in each dimension.
Delphi Round 2
In 2017, the online Delphi survey was distributed through EAPC head office. 19 Respondents to the 2014 baseline survey of palliative care services across Europe were chosen as an Expert Panel for the study. Attempts were made to identify contacts in countries not represented in the panel. Round 2 of the survey was opened for 51 days, during which time two reminders were sent to the panel and to national organisations. Panellists rated their agreement/disagreement on each recommendation statement of the survey. Evaluation was performed using a 5-point Likert scale: ‘strongly disagree’ (1), ‘disagree’ (2), ‘neither agree nor disagree’ (3), ‘agree’ (4) and ‘strongly agree’ (5). Very strong consensus was defined as ⩾80% strongly agree/agree. Strong consensus was defined as 75%–79% strongly agree/agree. Items with a consensus rating below 75% were subject to revision. In addition, the Expert Panel provided qualitative comments on the dimensions and statements of the survey. These comments were used in the revision of statements with low consensus rating. Further, information was gathered on service type (Inpatient/hospice/homecare service/hospital service/daycare service/other); country; and email address to receive the survey in Delphi Round 3.
Delphi Round 3
Delphi Round 2 statements with Expert Panel agreement of less than 75% were modified based on the qualitative comments. The revised statements were reviewed by the EAG before returning them to Delphi Round 3. The revised statements were distributed to the Expert Panel using the same procedure as Round 2. Statements that did not reach consensus agreement, based on the previously defined criteria, were discarded. Round 3 was open for 31 days beginning June 2017 and three reminders sent.
Delphi Round 4
Based on feedback from Delphi Round 3, all statements reaching consensus were discussed and each dimension’s statements were ordered according to strength of agreement as determined by median scores. Further, statements were labelled by strength of agreement; ‘essential’ based on a median score of 5 and ‘desirable’ based on a median score of 4. The EAG reviewed results for external validation and agreed the process.
Delphi Round 5
The full set of EAPC bereavement recommendations were finalised and forwarded to the EAG and the Board of Directors of EAPC for review and agreement.
Results
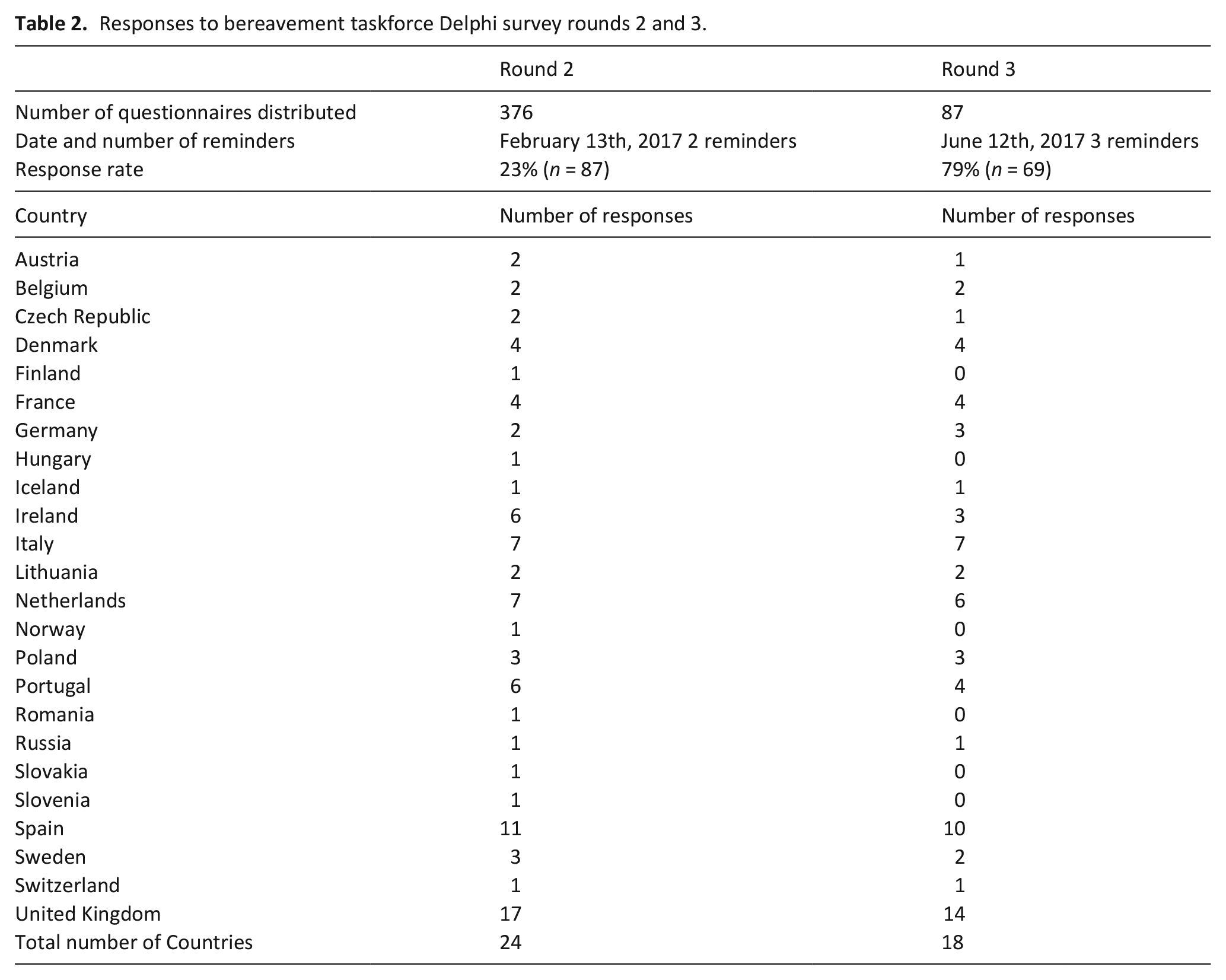
In total, 376 email requests to complete Delphi questionnaire were distributed by EAPC head office to the EP. Response rates in Delphi Round 2 were 23% (n = 87) and Delphi Round 3 were 79% (n = 69) across 24 and 18 countries, respectively (Table 2). In both rounds most respondents (56%–64%) worked in inpatient units/hospices; over a third worked in home care (35%–66%) and approximately one-fifth in hospitals services, (21%–22%) with smaller proportions mentioning day care or ‘other’ settings.
Responses to bereavement taskforce Delphi survey rounds 2 and 3.
Round 2
The majority of statements received strong endorsement from respondents, 49 statements had ‘very strong’ agreement (⩾80%), and two had ‘strong’ agreement (75%–79%). For three dimensions, all statements were fully endorsed: ‘Definitions about grief/bereavement’; ‘Competencies, education and training for bereavement care in palliative care’ and ‘Integrating bereavement care into wider health services and community’ (Table 3).
Delphi round 2 results; number and percentage agreeing/disagreeing; median score and combined strongly agree/agree percentage.
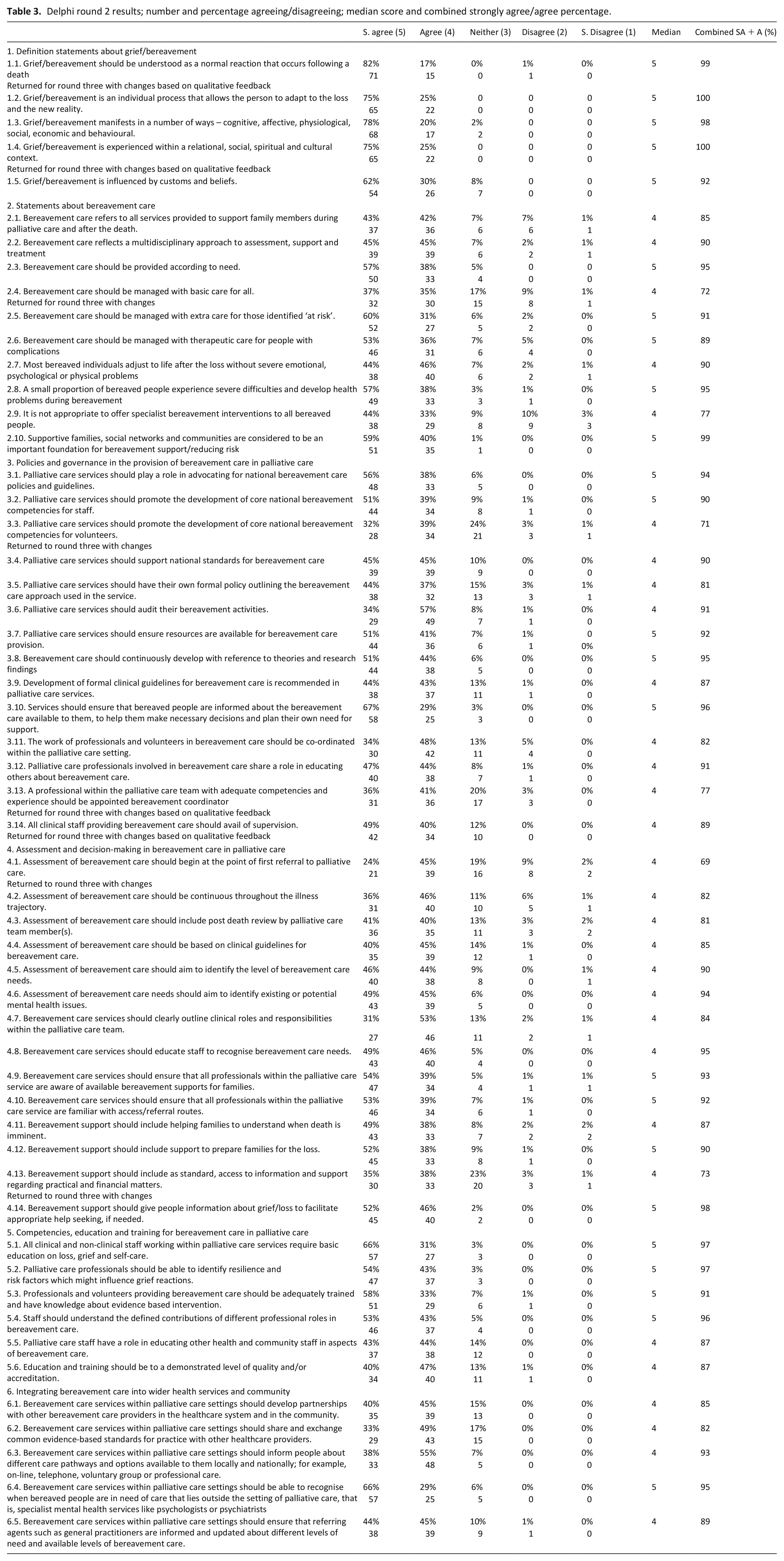
However, eight statements from four dimensions were selected for Round 3 assessments; four did not reach the 75% pre-defined threshold, and four statements were rephrased based on qualitative survey comments (Table 3). A total of nine (10%) respondents disagreed that ‘Bereavement care should be managed with basic care for all’ and 15 (17%) neither agreed nor disagreed. Almost a quarter of respondents neither agreed nor disagreed about the development of core national bereavement competences for volunteers. There was ambiguity about when bereavement assessment should begin: while 69% (60) endorsed the statement ‘Assessment of bereavement care should begin at the point of first referral to palliative care’, almost 19% (16) neither agreed nor disagreed and 10 (11%) disagreed. The statement ‘Bereavement support should include as standard, access to information and support regarding practical and financial matters’ was endorsed by 73% (63), below the agreed cut-off point of 75%. In addition, 23%, (20) neither agreed nor disagreed and 4% (4) disagreed.
Round 3
Of the eight statements sent to Round 3, seven were returned with increased consensus (Table 4). An original statement about basic bereavement care was adjusted to ‘Basic bereavement care recognises that all bereaved people should have access to verbal and written information about the grief experience and about bereavement services’. Consensus for this item increased from 72% to 87%, and median from 4 to 5. A statement concerning national bereavement competencies for volunteers was adjusted to clarify that such competencies apply where volunteering systems existed, ‘In countries where volunteers provide bereavement care, palliative care services should promote the development of core national competencies FOR VOLUNTEERS’; subsequently consensus rose from 71% to 82%, median unchanged at 4.
Delphi survey round 3 results number and percentage agreeing/disagreeing; median score and combined strongly agree/agree percentage compared to results for Round 2.
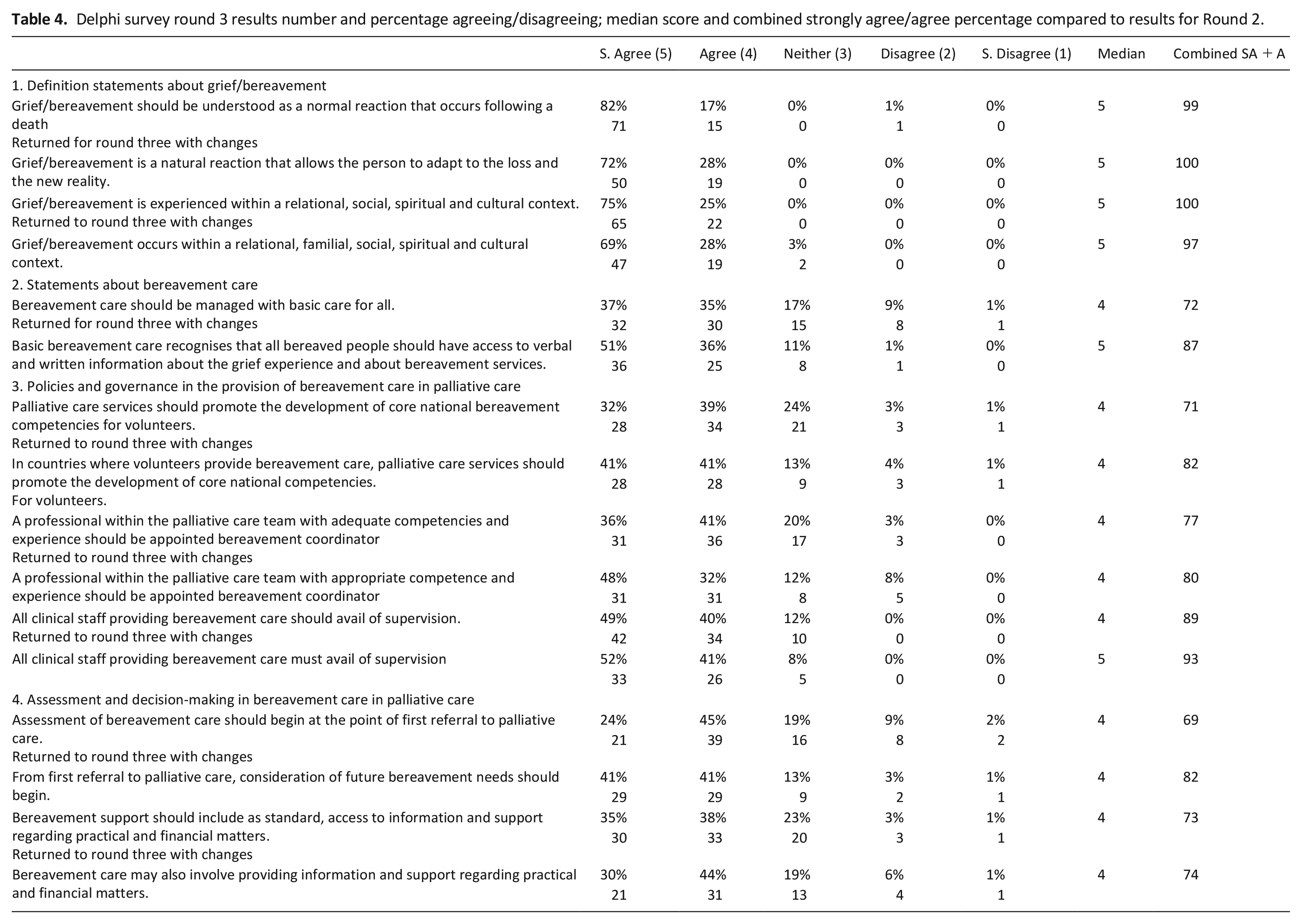
The Round 2 item with least consensus concerned assessment, ‘Assessment of bereavement care should begin at the point of first referral to palliative care’. This statement was agreed by 69% of respondents and was adjusted to read ‘From first referral to palliative care, consideration of future bereavement needs should begin’. Consensus increased to 82% agreement. Emphasis on clinical supervision for staff working in bereavement increased from 89% to 93% and median from 4 to 5. One statement ‘Bereavement care may also involve providing information and support regarding practical and financial matters’ failed to reach strong agreement and was removed (combined agree/strongly agree of 74%, median 4).
Round 4
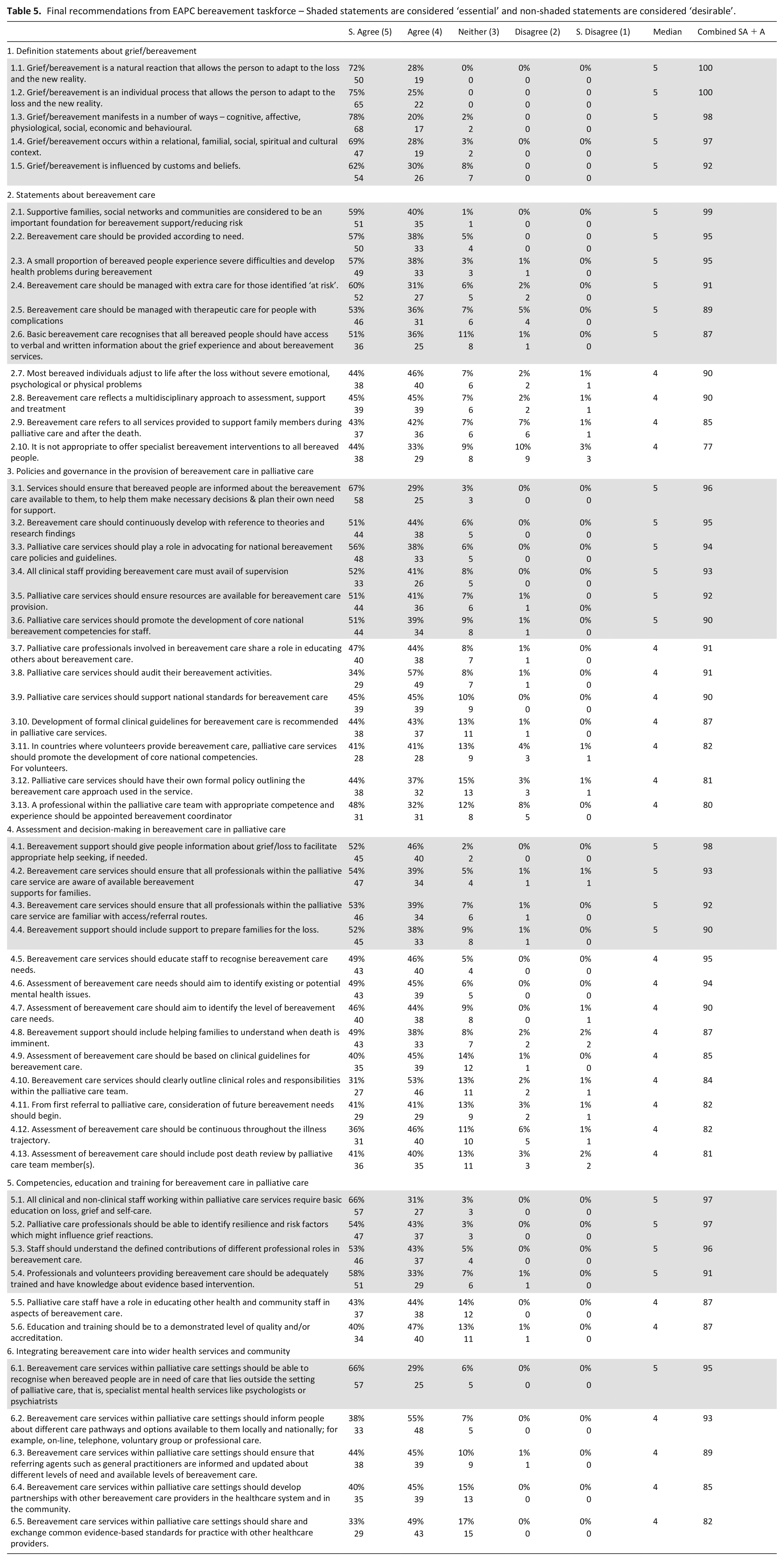
In Round 4, almost all statements were endorsed as ‘strongly agree/agree ⩾ 80%’. One statement ‘It is not appropriate to offer specialist bereavement interventions to all bereaved people’ received moderate agreement (77% strongly agree/agree, median 4). For this round, statements with a median of 5 were classified as ‘essential’ features under the six dimensions of bereavement care, while statements with strong agreement and median of 4 were classified as ‘desirable’ features. Table 5 sets out the completed recommendations for bereavement care in palliative care generated through the Delphi.
Final recommendations from EAPC bereavement taskforce – Shaded statements are considered ‘essential’ and non-shaded statements are considered ‘desirable’.
Discussion
Main findings
A coherent direction for development of palliative care bereavement support across diverse European countries has been outlined, using the Delphi Technique. 18 There was very strong consensus on the definition of bereavement, allowing agreement on the main features of bereavement care; an aspect omitted in previous work.13–15 This consensus can be framed as a ‘call to action’ in the planning and provision of bereavement care in palliative care services. A public health approach was endorsed through 54 statements across six dimensions. The recommendations support the empowerment of bereaved people to understand their experiences and make care choices 3 ; early identification of care needs 35 ; provision of targeted bereavement care36–38; provision of education and training for professionals and integration with local communities and services 16 thus addressing gaps in bereavement care identified in contemporary bereavement research.
Strengths and limitations
These recommendations were developed in a systematic Delphi technique study conducted with reference to CREDES guidance for Delphi studies providing scientific rigour. 18 A group of international experts on bereavement provided guidance and the recommendations were discussed and feedback received at two EAPC Congresses.
The study was informed by scientific consensus on the efficacy of bereavement care and by recent developments in international clinical diagnostic guidance as well as the public health model.10,20–23 It resonates with the seminal hospice studies by Parkes,24,25 and further develops the tiered approach of the NICE recommendations promoting the importance of targeting services.12,20,25,26
The response rate in round 2 of the Delphi study was low at 23% (n = 87) of the original 376 respondents. A 2009 Delphi study on grieving styles reported 20 of 61 invitees agreed to be on a panel (32%), later rounds were not reported. 39 A review of Delphi studies found a minority (39%) report all round response rates. 40 In our study the large panel size may have influenced the low response rate. 41 Efforts were made through EAPC to identify contacts from missing countries and to encourage participation. Eastern Europe was under-represented, perhaps biasing the results. The Delphi survey was distributed in English, which may have limited the response rate, or biased results in favour of English speakers. However, most countries were represented and reflected a range of service types. Despite these limitations, the representativeness of the study was deemed satisfactory and the majority of those who completed the Round 2 Delphi questionnaire went on to complete Round 3 (79%, 69/87).
What the study adds
The six dimensions and 54 statements clarify a direction for development of bereavement services in palliative care in Europe. Recognising variation in the development and maturation of bereavement services in different countries, statements were analysed and reported in a way that services and national associations can prioritise. The ‘essential’ elements under each dimension are suggested as first-line priorities, with ‘desirable’ statements providing scope for further development.
The strong consensus and shared understanding of definitions and of the experience and context of grief is welcome, as the survey in Phase 1 of the Task Force found considerable diversity of theoretical perspectives across Europe. 17 Other guidances have not explicitly defined grief and bereavement nor have they targeted culturally or linguistically diverse populations.13,14 Given the cultural, linguistic, funding and service model variance across Europe the Task Force considered the achievement of consensus on definitions to be fundamental for future developments.
Dimension 2 statements are consistent with the tiered model of bereavement care 12 and the Public Health Model10,11 and endorse intervention for those most in need of care.9,20 Respondents to the Delphi Survey agreed the importance of mobilising family, community and social networks in supporting the bereaved. 27 The multidisciplinary approach to assessment, support and treatment and the opportunity to assess from point of first referral to the post-death period is endorsed. The item with the lowest consensus was on the inappropriateness of offering specialist interventions to all bereaved people. This was unexpected, echoing concerns about lack of adherence to evidence base.16,20 Nevertheless, there was agreement on the nature of bereavement care and the elements it must contain. This is significant as previous work of the Task Force found few services referencing research and clinical literature. 17 Further, it aligns with concern about adherence to models of care which lack or even contradict evidence, 28 and also the Task Force finding that a range of models underpin bereavement care, not all are evidence-based. 29
There was strong endorsement in dimension 3 that bereavement care should be integral to national policies, guidelines, standards and competence frameworks. The advocacy role defined and agreed for palliative care will give stronger focus in furthering WHO guidance on integrating aspects of palliative care into national policies. 30 Also, this dimension suggests endorsement of a public health approach to bereavement care at national level which should be a European-wide priority. Palliative care services are stakeholders in overall bereavement care and therefore bereavement support planning should situate palliative care bereavement support within a wider network of services. Specific actions were endorsed for local palliative care services including audit, continual review, development of formal clinical guidance and the appointment of a named bereavement co-ordinator. However, the EAPC survey showed that these practices were by no means common among services and the challenge to develop them should not be underestimated. 17
Decision-making and assessment in bereavement is challenging.31,32 However, there is acceptance in dimension 4 for continually assessing bereavement need/risk from first point of contact to post-death. There is acknowledgement of bereaved people’s role in self-assessment of need – a concept which can be supported through public education, 26 consistent with a public health approach and values of empowerment. 23 Professional intervention must be based on assessment of need according to clinical guidance. Developing this capacity might be challenging as ambivalence in the use of standard assessments amongst palliative care providers has been noted. 31 A minority of palliative care services use formal needs assessment; assessment is often based on professional observations rather than direct user participation.17,31,33
The importance of education, training and achievement of competence in grief and loss for all working within palliative care was strongly endorsed in dimension 5 with a recommendation that professionals should be able to identify resilience and risk factors. This dimension is important for building capacity within services – appropriate education and training is critical for the implementation of recommendations.
The recommendations refer to education needs of bereavement volunteers but are not as prescriptive as other standards documents.13,14 Volunteer involvement in bereavement support in palliative care is uncommon in many countries, 17 although there is some evidence that volunteer support is helpful and acceptable to the bereaved. 34 In line with other bereavement support standards respondents accept the proposition that palliative care services can and should have a role in educating health and community staff about bereavement. 14
The connectedness of palliative care services to local health and social services is the focus for dimension 6, continuing an integration theme. Where services are not in a position to support bereaved people with complex needs, it is important that they forge links with other care providers. Therefore, local review must identify external bereavement services and clarify access routes.
Further, bereavement needs and responses leading to appropriate outcomes must be incorporated into national palliative care and general health and social policies. 42
Our original survey of bereavement care in palliative care services in Europe in 2015 showed considerable theoretical diversity. 17 Therefore, the achievement of evidence-based consensus representing countries across Europe is a significant contribution to the planning and developing of a fundamental aspect of palliative care.
Footnotes
Acknowledgements
Members of EAPC taskforce phase one, Dame Barbara Monroe and Mariant Lascasta; Expert Advisory Group John Birrell, Susan Cadell, Linda Machin, Henk Schut; EAPC head office staff who distributed the link to the Delphi questionnaire. All Ireland Institute of Hospice and Palliative Care and the Irish Hospice Foundation who supported the phase one study.
Author contributions
Conception of the project and selection of methodology was led by OK and IM and contributed to by MG, MR, IB, JL. Research Ethics review was arranged by JL. Delphi statements and criterion ranges were developed by OK and IM and MG, IB, MR, JL contributed to design. Data collection was conducted by OK and IM. Data analysis was conducted by MG. Tables were prepared by OK and IM. First drafting of paper was developed by OK IM, and MG. Subsequent drafts were managed by OK and IM; MG wrote abstract and key statements. All provided critical comments on drafts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics
This study was reviewed by Ethics Committee on Animal and Human Research of the Universitat Autònoma de Barcelona which concluded that research ethics approval was not required.