
Abstract
Background:
Cancer-related fatigue is a complex multidimensional concept. However, little is known about the experience of cancer-related fatigue in people with advanced lung cancer. How they emotionally react to and cope with the experience of cancer-related fatigue according to cultural influences has not been extensively explored.
Aim:
To explore the experience of cancer-related fatigue, its impacts and emotional reactions to and coping strategies for cancer-related fatigue amongst people with advanced lung cancer in China.
Design:
This was a cross-sectional, descriptive qualitative study with face-to-face semi-structured interviews. Data were analysed using content analysis.
Setting/participants:
Twenty-one people with advanced lung cancer who experienced cancer-related fatigue were recruited in a hospital setting.
Results:
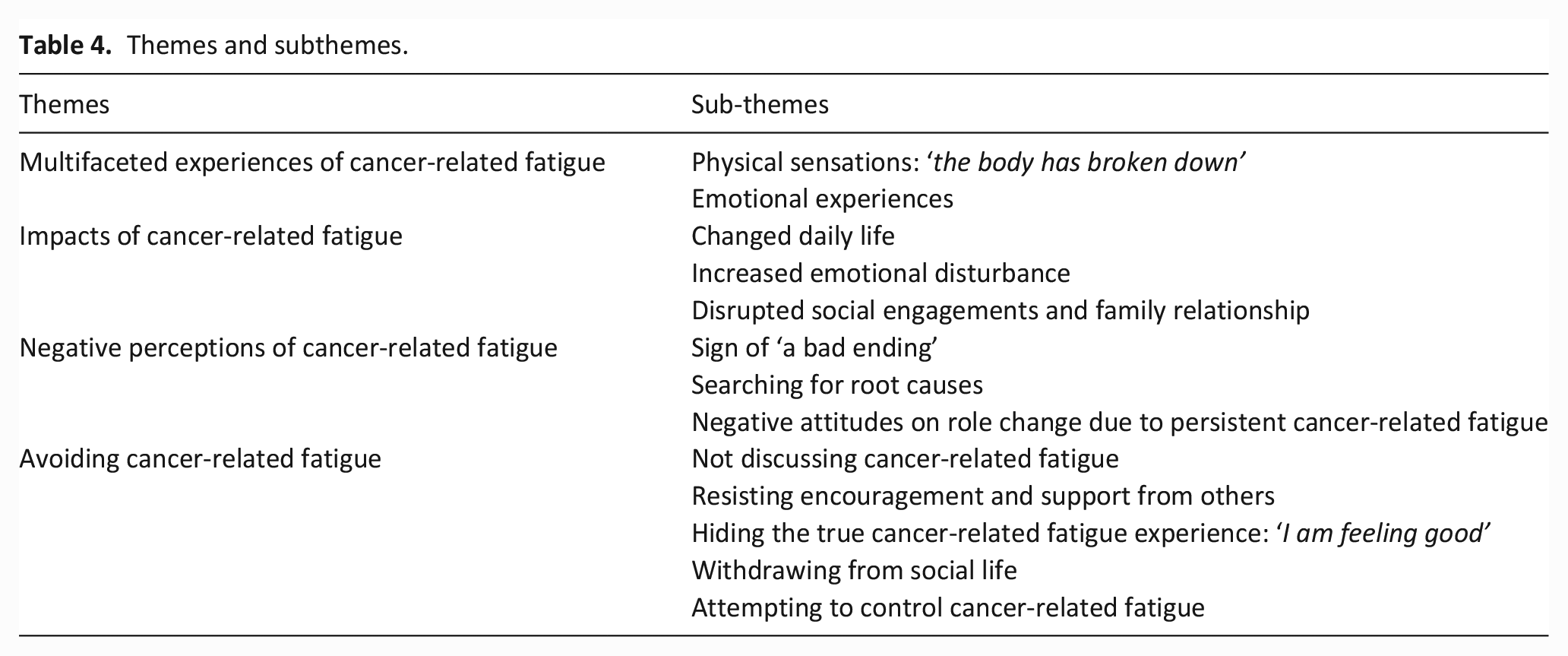
Four themes were identified: multifaceted experiences of cancer-related fatigue, impacts of cancer-related fatigue, negative perceptions of cancer-related fatigue and avoiding cancer-related fatigue. The multifaceted experience of cancer-related fatigue had physical, psychological and social impacts along the cancer trajectory. Informants regarded it as a sign of a ‘bad ending’, searched for root causes and had negative attitudes towards role changes. Avoiding coping strategies included not discussing cancer-related fatigue, refusing encouragement and support, hiding feelings, withdrawing from social life and attempting to control cancer-related fatigue.
Conclusion:
The findings provide insights into the lack of flexibility of people with advanced lung cancer to adapt to the multidimensional experience of cancer-related fatigue. The reactions and coping towards cancer-related fatigue are profoundly influenced by Chinese culture. Developing psychological interventions based on the cultural background are highly recommended to cultivate the ability to cope flexibly with stressful events and live a meaningful cancer life.
Cancer-related fatigue is common in people with advanced lung cancer and has a lasting effect on daily life.
People with advanced cancer differ in their emotional reactions, which further influence their coping strategies.
Cultural issues play a pivotal role in determining the emotional reactions to and coping strategies for the symptoms experienced by people with advanced cancer.
There are a limited number of qualitative studies about the experience of, emotional reactions to and coping strategies for cancer-related fatigue amongst Chinese people with advanced lung cancer.
Chinese people with advanced lung cancer avoid disclosure of their cancer-related fatigue, attempt to control it and experience pessimistic beliefs and negative attitudes associated with cancer-related fatigue.
Chinese culture profoundly influences individuals’ descriptions of their experience of cancer-related fatigue. It also influences their emotional reactions and behavioural responses to cancer-related fatigue.
Culturally relevant acceptance-based interventions are recommended to be developed and offered to people with advanced lung cancer to foster the acceptance of cancer-related fatigue and its impacts.
Facilitating being in the present moment and paying attention to important aspects of life will contribute to these individuals’ ability to live a meaningful life with cancer.
Background
Lung cancer is the most common and the leading cause of cancer-related deaths globally.1,2 Most people with lung cancer are initially diagnosed at an advanced stage. They are constantly reminded of impending death 3 and experience distressing symptoms and burdens resulting from the advanced disease and its associated treatments.4–7
Cancer-related fatigue is the greatest concern for people with advanced lung cancer. 8 It is a distressing, persistent and subjective sense of physical, emotional and cognitive tiredness or exhaustion related to cancer or its treatment. It is not proportional to recent activity and interferes with normal daily functions. 9 Cancer-related fatigue can impair psychological status, interferes with the abilities to perform self-care and participate in life’s activities,10,11 and affects their compliance with treatment regimen.12,13 The persistence of cancer-related fatigue after treatment prevents individuals from resuming daily routines, severely reducing their quality of life. 14
Numerous quantitative studies have indicated strong links between cancer-related fatigue and psychosomatic symptoms in people with advanced cancer.15–18 Psychological factors are regarded amongst the crucial predictors of cancer-related fatigue.9,19 Negative feelings and attitudes, including depression and anxiety and psychological responses and coping strategies are believed to be associated with alterations in neural, neuroendocrine, psychological, behavioural and immune processes relevant to cancer-related fatigue. 20 Research has indicated that avoidance is the most common psychological response to cancer diagnosis and treatment.21,22 Lack of acceptance on fatigue-related experiences was indicated to be positively related to cancer-related fatigue, which may lead to narrower ranges of behaviour and a reduced focus on a value-based life.23–30
Qualitative studies have been conducted to explore the experience of cancer-related fatigue; however, several research limitations exist. Scott et al. 31 conducted a qualitative systematic review, in which most included studies involving women with breast cancer in mixed stages limited the generalisability of the results on other cancer types, stages (e.g. advanced stage) and males. Moreover, participants mainly described the physical sensations of cancer-related fatigue, few have focused on its psychological adaptation process (i.e. reactions and coping strategies). Bootsma et al. 32 carried out a meta-ethnographic analysis of qualitative research. Six studies primarily reported cancer population had negative beliefs or misrecognition on cancer-related fatigue. However, there is a paucity of further exploration of individuals’ subjective experiences of cancer-related fatigue for those in advanced stages. Evidence suggests that people with advanced cancer differ in emotional reactions, which influence their coping strategies and symptom management. 33 Furthermore, these studies were all conducted in Western countries. Studies have pointed that the Chinese cultural values of Confucian thought, family responsibility and self-esteem influence cancer population’s emotional reactions to their symptoms, which further affect their coping strategies with cancer and their beliefs about the meaning of life. 34 For example, people tend to avoid negative emotions towards distressing symptoms and continue to fulfil their family roles as required according to Chinese cultural values. 35 Despite various coping strategies for cancer-related fatigue reported,22,31 few considered how cultural issues may influence emotional reactions to and coping strategies for cancer-related fatigue in people with advanced cancer.
This qualitative study was conducted to explore the experiences and impacts of cancer-related fatigue, and emotional reactions to and coping strategies for cancer-related fatigue in people with advanced lung cancer in China. The findings of this study will inform the development of culturally sensitive cancer-related fatigue management interventions for this population.
Methods
Design
A descriptive qualitative study was used to explore the experiences of cancer-related fatigue in people with advanced lung cancer. This study was reported following the Consolidated Criteria for Reporting Qualitative Research guideline. 36
Setting
The informants were recruited by purposive sampling from the respiratory department of a university-affiliated hospital in Changsha, China from October to December 2020. The maximum variation strategy was applied to select information-rich cases and identify informants based on their age, sex, educational background, time since diagnosis and stage of advanced cancer. 37
Population
Informants were eligible for inclusion if they (a) were aged at least 18 years, (b) had been diagnosed with advanced lung cancer (stage III or IV) by pathological section or cytology and informed of their cancer diagnosis, (c) experienced cancer-related fatigue (i.e., scored 3 or more on the Fatigue Symptom Inventory (FSI), 38 and (d) were able to comprehend Chinese and provide written informed consent. Informants were excluded if they had (a) severe cognitive impairment or (b) a severe mental disorder.
Sample
The sample size was determined by data saturation, defined as the point when few new insights into the research questions emerged in recent interviews. 39 In the present study, 20 informants were estimated to be necessary before data collection. Data became repetitive after 19 interviews, and two more informants were interviewed thereafter to ensure data saturation.
Recruitment
A clinical nurse at the study site identified potential informants by screening medical records and approached them during their hospitalisation. Each informant was given a research information sheet, which included the study aims, potential benefits and risks and data collection procedures. The principal investigator contacted those who expressed interest, answered their questions and discussed their participation. Upon agreement, the informants provided written consent to participate. A follow-up interview was then scheduled at their convenience.
Data collection
Face-to-face semi-structured interviews were conducted by the principal investigator (HL, female), who was a PhD candidate in nursing at the time of data collection and has extensive experience in lung cancer care. Interviews were conducted in an independent office of the respiratory department. Each interview lasted an average of 46 min (range: 32–75 min).
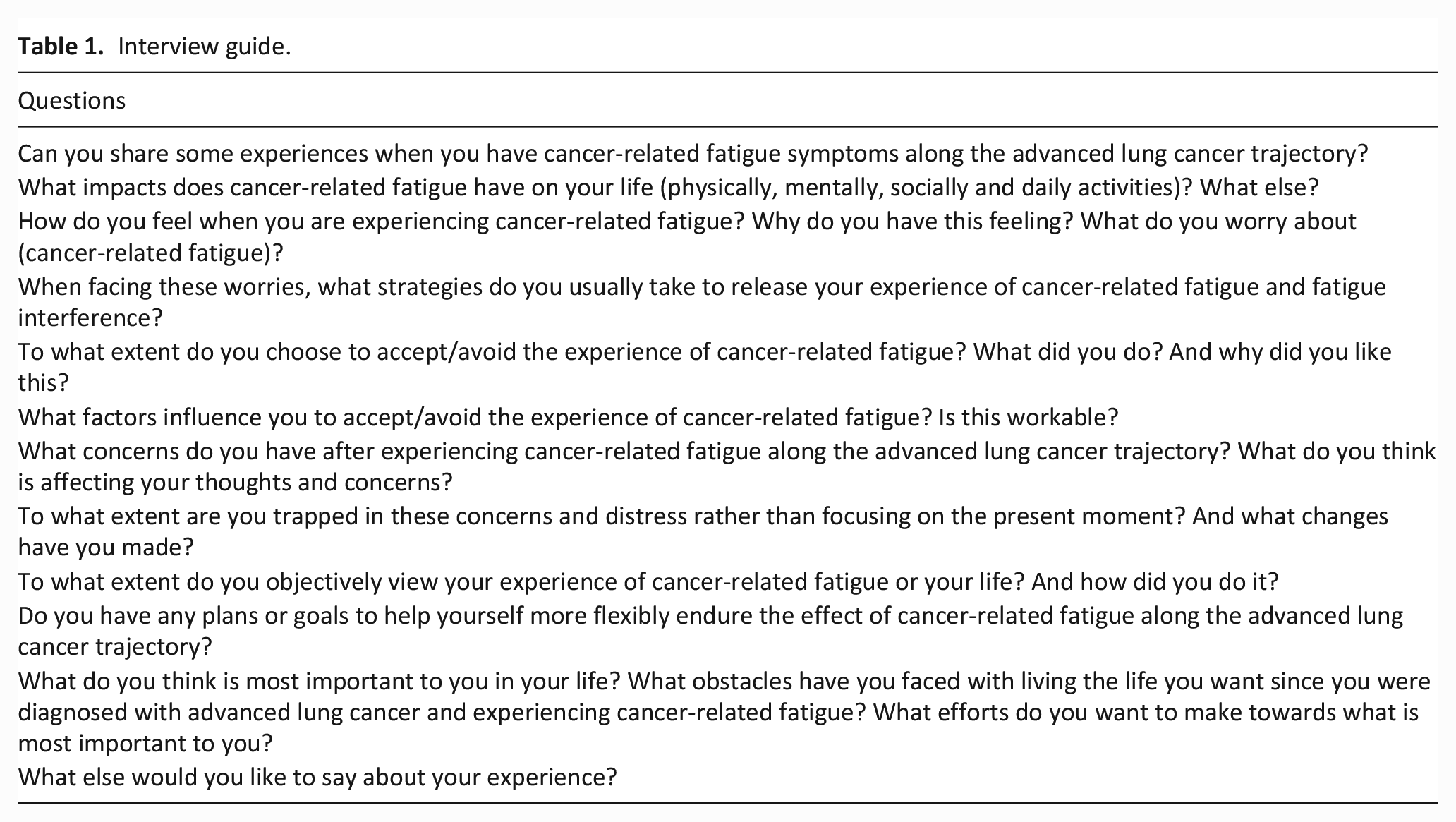
The interview guide was developed with reference to previous qualitative studies of cancer-related fatigue symptoms in cancer population (Table 1). The interview guide consisted of 12 questions and follow-up probes to seek elaboration. 40 These questions covered issues related to cancer-related fatigue along the advanced lung cancer trajectory, its impacts on different aspects of life and the informants’ emotional reactions and coping behaviours. The interview guide was pilot tested on three informants to ensure clarity in the wording of the questions. The interviews began with broad questions, such as ‘Can you share some of your experiences of cancer-related fatigue along the advanced lung cancer trajectory?’ Follow-up probes and prompts were used to evoke information about the informants’ real-life experiences when they did not fully address the research questions. 41 Detailed field notes and the researcher’s reflective notes were also documented.
Interview guide.
The interview data were audio-recorded after obtaining permission from the informants (from October to December 2020). Demographic information, such as age, sex, education, employment, level of cancer-related fatigue, diagnosis (stage and subtype) and time since diagnosis, were collected before the interview.
Data analysis
The characteristics of the informants were presented as means and percentages. According to the method proposed by Creswell, 42 content analysis was used to detect the manifest 43 and latent content 44 of the data, following transcribing, coding, categorising and extracting themes.
The principal investigator (HL) transcribed the audio-recorded interviews verbatim in Chinese. The transcripts were compared with and checked against the audio-recorded interviews for accuracy. Revisions were made if necessary. Two independent researchers (HL and XJ) repeatedly listened to the audio recordings and read the transcripts line by line to obtain a general understanding. They then identified meaningful data units to generate initial codes using NVivo 11 (QSR International, Melbourne, Australia). The codes dealing with the same content were grouped into categories, categorised into subthemes using the inductive approach, and then collated into themes. The researchers reviewed the themes and subthemes independently for coherence with the coded extracts. The finalised themes and subthemes, with their corresponding representative quotes, were translated into English. Two bilingual supervisors with extensive experience in conducting qualitative studies (CLW and MSNN) reviewed the themes and subthemes. Any disagreements were resolved through discussion until a consensus was achieved.
Rigour
The rigour of the study was ensured following credibility, dependability, confirmability and transferability. 45 Maximum sampling and audiotaped interviews established credibility by minimising the failure to note important data. 46 Peer debriefing to supervisors with extensive experience in qualitative studies was then performed to ensure the accuracy of the codes and categories. Dependability was established through audio recordings and an audit trail of the transcripts, reflective comments and data analysis notes to demonstrate deviations from the data. 47 For confirmability, 48 the findings were reviewed by all authors to ensure the objectivity and neutrality of the data. Moreover, sufficient contextual information, such as the research setting, recruitment criteria, sample size, data collection process and data analysis, was provided to facilitate transferability.49,50
Ethical considerations
The study was approved by the Survey and Behavioural Research Ethics Committee (Ref. No.: SBRE-20-040, 15 September 2020) of the Chinese University of Hong Kong and the institutional research board of the study site. Written consent was obtained from the informants before the interviews. The informants were informed about the audio recordings, confidentiality and their right to withdraw from the study without penalty. The interview was stopped or paused if the informants felt any physical discomfort or psychological distress during the interview, and in such cases, the details of available resources for further support and treatment were provided. No adverse events occurred during this study. All digital data and transcripts were kept confidential, stored in encrypted devices and accessed only by research team members.
Results
Of the 24 eligible people with advanced lung cancer, 21 consented to participate. Three of the eligible individuals declined because of not feeling well (n = 1), a lack of interest in talking about their personal feelings (n = 1) or their family members’ disagreement with their participation because of fears that it would burden them (n = 1). Tables 2 and 3 present the sociodemographic and clinical characteristics of the informants. The mean age of the informants was 58 years (range: 37–81 years). The average duration since cancer diagnosis was 16 months (range: 1–120 months). All of the informants were married, and most of them were male (n = 15, 71.4%), were living in rural areas (n = 14, 66.7%), were farmers (n = 8, 38.1%), had been diagnosed with non-small cell lung cancer (n = 16, 76.2%), had stage IV cancer (n = 17, 81.0%) and had received chemotherapy (n = 17, 81.0%). The average total FSI score was 46.6 (range: 4–89).
Summary of characteristics of informants.
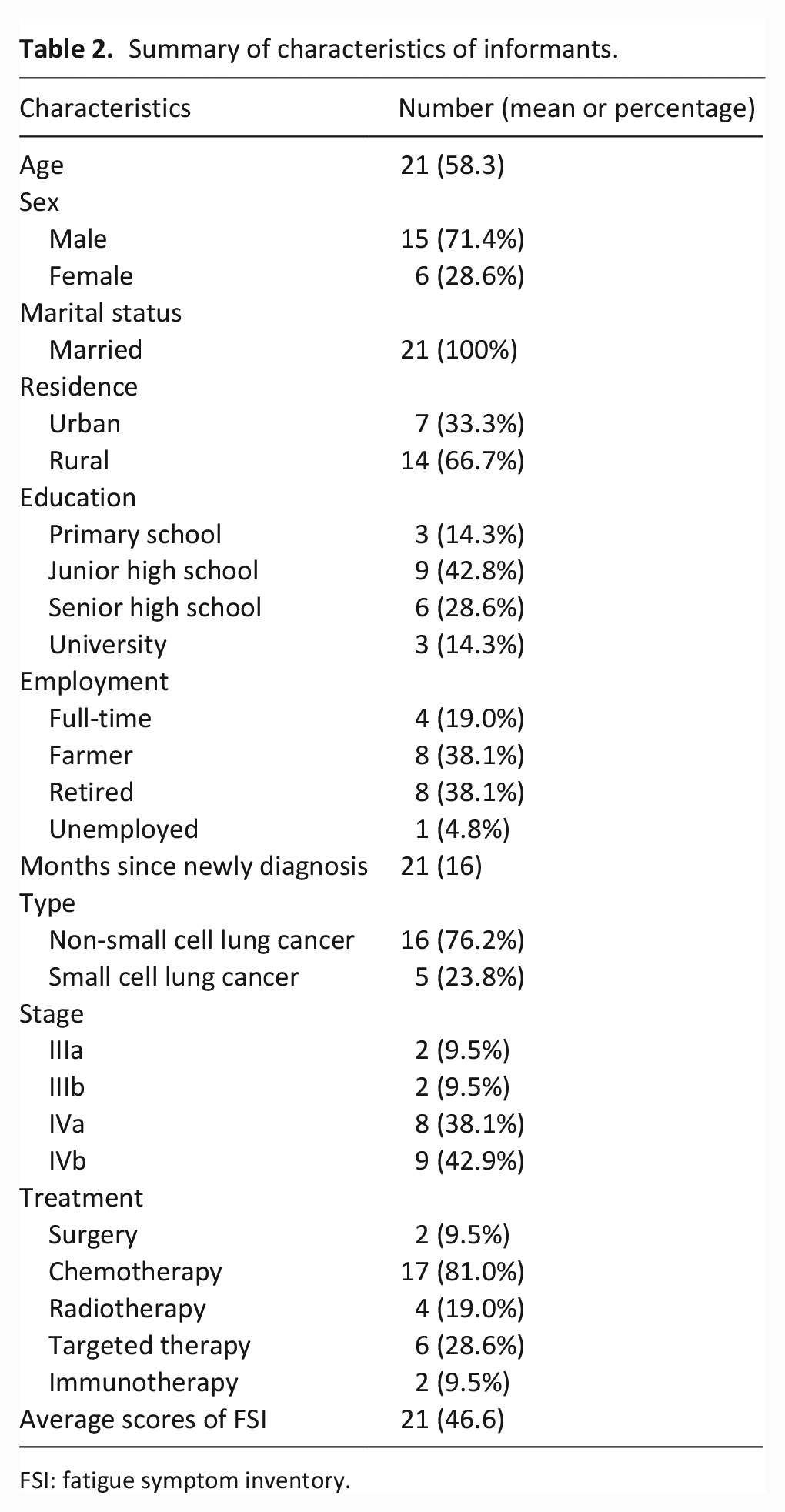
FSI: fatigue symptom inventory.
Detailed characteristics of each informant.
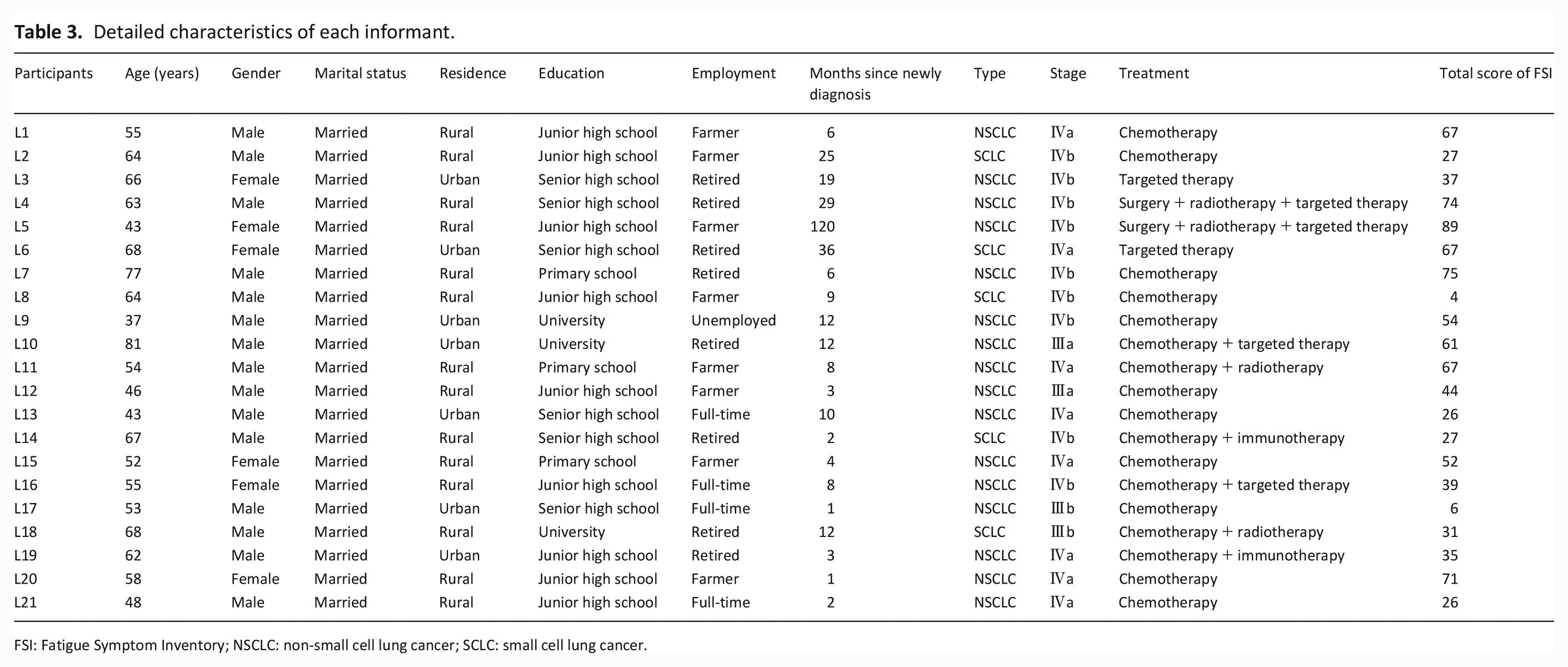
FSI: Fatigue Symptom Inventory; NSCLC: non-small cell lung cancer; SCLC: small cell lung cancer.
Thirteen subthemes in four themes emerged from the data (Table 4).
Themes and subthemes.
Theme 1: Multifaceted experiences of cancer-related fatigue
This theme comprised descriptions of multidimensional cancer-related fatigue experiences. The subthemes included (1) physical sensations: ‘the body has broken down’ and (2) emotional experiences.
Subtheme 1: Physical sensations: ‘the body has broken down’
Informants’ descriptions of their cancer-related fatigue experiences were often concretised. They described their physical experiences as ‘wobbly legs’, ‘a stuffy body’, ‘a lack of energy or a kind of weakness’, ‘drowsy’, ‘no appetite’ or ‘the body has broken down’. With time (range: 7–15 days), the informants reported some degree of relief from cancer-related fatigue.
I didn’t want to move around, and I didn’t have much energy to walk. I didn’t want to talk and I just wanted to lie down. After resting for 8 to 10 days, my whole person seemed to return to life gradually (Informant [I]1).
There was no strength in my legs (I6).
Subtheme 2: Emotional experiences
Half of the informants reported how they felt about cancer-related fatigue. Their feelings about cancer-related fatigue were described as ‘frustrating’, that it ‘cannot be mitigated’ and ‘the whole day was dull’, and they felt ‘downhearted’ or ‘overwhelmed’. ‘Frowning’ was the most common facial expression observed when informants were asked and talked about cancer-related fatigue directly or indirectly.
It (cancer-related fatigue) upsets me. . .because I really cannot do anything. . .I do not have the energy. . .It’s too hard (I13).
My mood rises and falls with it (cancer-related fatigue) every day. I think it will drive me crazy (I2).
When I was tired, sometimes I wanted to cry. . . (choked up) . . . it seemed to have no reason. I don’t like this unhappy feeling (I20).
Theme 2: Impacts of cancer-related fatigue
This theme described the impacts of cancer-related fatigue on diverse aspects of daily life in people with advanced lung cancer. The subthemes included (1) changed daily life, (2) increased emotional disturbances and (3) disrupted social engagements and family relationships.
Subtheme 1: Changed daily life
Suffering from cancer-related fatigue changed the informants’ lifestyles and interfered with their activities of daily living because of the deterioration of their physical condition associated with cancer-related fatigue. They had to reduce the intensity and duration of physical exercise, lie on their bed, sit and move slowly (e.g. when chewing food, dressing and grooming). All informants reported that they needed varying degrees of assistance with homemaking, transportation and even simple self-care activities, such as preparing food and bathing.
I used to be keen on travelling everywhere and climbing mountains. Now it’s hard to walk from the hospital gate to the bus stop (around 300 meters) . . . very breathless and tiring. The situation is still the same, and I even slow down (I9).
I need to ask my wife to help twist the towel so I can wipe my face by myself. I have no strength in my arms now. I used to be able to do these things on my own (I8).
Subtheme 2: Increased emotional disturbances
Experiencing cancer-related fatigue brought about consistent emotional disturbances. First, a sense of hopelessness emerged about unresolved cancer-related fatigue and life. As cancer-related fatigue is induced by cancer and is also one of the side effects of treatment, it can make people with advanced lung cancer lose vitality. This discomfort makes them unable to do what they could normally do, leading to worries about being a burden to their family. Due to the unmitigable nature of cancer-related fatigue, combined with misconceptions about cancer-related fatigue, the informants began to worry about and doubt the effectiveness of their current treatment regime and further worry about the possibility of the exacerbation of their condition, causing a sense of hopelessness. This sense of hopelessness formed a vicious circle, such that the informants were shrouded in fear of the future, were depressed about their fate and feared their forthcoming death. This interfered with their ability to calm down and pay attention to what they were doing and wanted to do. The sense of ‘I cannot’ further exaggerated the cancer-related fatigue experience.
. . . (The weakness) was just like a time bomb, making me feel very helpless. I wait for time to pass. It seems that it has become worse. (I9)
I don’t want to dress myself up. I am just wearing pyjamas. I have lost interest in beautiful clothes. It is meaningless (I20).
In addition, seven informants reported that their long-term cancer-related fatigue experience induced in-advance anxiety. Impressed by the severe cancer-related fatigue experiences after each chemotherapy circle, whenever the informants were reminded to go to the next cycle of treatment, they unconsciously thought about their previous cancer-related fatigue experience. This made them distressed, resulting in resistance to undergo subsequent treatment and a sense of anxiety and vigilance about facing cancer-related fatigue again.
I start to get anxious in advance when I need to be re-hospitalised. That seems to suggest it (cancer-related fatigue) will interfere again. . . (I7).
Subtheme 3: Disrupted social engagements and family relationships
Suffering from cancer-related fatigue also disrupted the informants’ social well-being. On the one hand, a lack of energy made them cut back on their workload, quit their jobs or retire early, thus weakening their social functioning and responsibilities. On the other hand, cancer-related fatigue reduced their interest and energy in participating in social activities, including entertainment activities. Tiring quickly or feeling the hassle of applying make-up, grooming and changing clothes kept some of them housebound.
I used to engage in production on the front line, but now I don’t do much work (I13).
I made many friends from all walks of life. But now, if nobody contacts me, I become lazy and do not want to talk (I9).
I used to have a big dog. However, I could not hold it, and the dog was sent away. I don’t have any energy to do this. I used to like taking photos. Now I cannot walk around with my camera equipment (I9).
The informants experienced a loss of purpose in life because of suffering from cancer-related fatigue. They were immersed in the distress of the cancer-related fatigue experience; they isolated and closed their connections and feelings with the outside world; and they completely ignored the aspects that were truly important to them in real life, such as their families, careers and hobbies and relationships with others. Therefore, the informants held an indifferent attitude towards their personal development and life planning. Several young informants experienced the torment of cancer-related fatigue and then became devoid of any life pursuits. No other expectations in life were left.
Now I am a bit decadent. There has been no pursuit for me. The things I was willing to pay for, I do not deserve to work so hard for them now. I think I have enough to live on (I9).
Furthermore, the cancer-related fatigue experience worsened two informants’ family relationships and caused a failing marriage. Two informants described that they did not gain support and care from their partners during vulnerable moments, and one of them had to take care of her sick partner even though she was experiencing cancer-related fatigue.
I have been fatigued and diagnosed with this disease for more than a year. He (husband) has not cared about me. I still have to take care of him, although he is entirely independent. I am considerate of him, but he always wants to quarrel with me (I3).
Theme 3: Negative perceptions of cancer-related fatigue
This theme described the informants’ negative perceptions of cancer-related fatigue. The subthemes included (1) sign of a ‘bad ending’, (2) searching for root causes and (3) negative attitudes due to persistent cancer-related fatigue.
Subtheme 1: Sign of ‘a bad ending’
Informants often described their experience of cancer-related fatigue as ‘unusual’ or ‘a sign of a bad ending’. They also stated that ‘it reveals that the body is out of control’ and ‘this state is impossible to change’. They recognised the cancer-related fatigue experience as an illness after lung-cancer-related treatments.
I have no energy during chemotherapy. It (cancer-related fatigue) lasts for weeks. It feels like I am going to get worse (I16).
Informants were dominated by their pessimistic beliefs and intrusive thoughts about cancer-related fatigue as they were experiencing the symptoms. They regarded it as bad, stating that ‘it’s all over’. When they experienced fatigue, or when the cancer-related fatigue could not be relieved, ideas arose about abandoning treatment or even ending their lives, such as by taking poison. One informant equated the cancer-related fatigue to chronic torture.
We are sentenced to death once suffering from this disease (advanced lung cancer). Now, chemotherapy is just a reprieve. Having no strength (cancer-related fatigue) is a kind of torture. It is all in vain (I19).
Subtheme 2: Searching for root causes
Immersed with those beliefs and feelings, the informants tried to understand why things unfolded as they did. Repeated thinking about unresolved cancer-related fatigue and its effects along the advanced lung cancer trajectory made informants begin to search for the root causes of the lung cancer diagnosis, such as genetic and lifestyle factors and their working environment. Some speculations were scientific and valid, while some were not. They never stopped looking for potential factors causing their sickness and insisted on entertaining such thoughts.
People shouldn’t work tirelessly once they reach 60 years old. If you are working too hard, the money you earn will be used to cure your illness. I think that my illness is from my hard work. Of course, smoking may also be a reason (I3).
Such thoughts led them to get stuck in the ruminations of asking, ‘Why me?’. One informant stated:
I know genetic factors account for a large proportion. However, I have brothers and sisters. Why did they not get sick, but I got this disease and I’m tortured by cancer-related fatigue here? (I18).
Subtheme 3: Negative attitudes about role changes due to persistent cancer-related fatigue
Most informants felt guilty about their inability to take on family roles and fulfil their obligations in the family and community due to the change from being a helper to being helped and were unable to accept the disparity between their past and current situations. This was constrained by traditional moral and cultural concepts that a man is the family’s breadwinner and should work hard and earn money to support the family. In this case, informants who were husbands or eldest sons expressed more self-blame and guilt than other informants because of their physical condition, as indicated by the statement: ‘My family was dragged down’.
I cannot do anything while seeing others working there. I feel that I am useless (I1).
The informants also became overly sensitive and described themselves as feeling a profound change, as indicated by the following statements: ‘I am incompetent’, ‘I have changed’ and ‘I am a waste now’. The significant changes mainly came from differences in their personality from before to after experiencing cancer-related fatigue (i.e. changing from a positive and active person to a lazy person). These changes caused low self-esteem and further increased the informants’ dissatisfaction with their current illness and weakness. They grieved that they could no longer return to their ‘original’ status. Three informants also misidentified or over-interpreted the behaviour and thoughts of others during this period. Caring and kind help from others led to self-deprecating thoughts, such as ‘they don’t treat me as a normal person’ and ‘they laugh at me’.
I feel that I am different since I became ill. I was reckless and powerful when I was a company’s department manager. Now I am easy-going. You are right about everything. I don’t want to argue with others. I won’t pursue perfection. You’ll find these changes incredible (I9).
Theme 4: Avoiding cancer-related fatigue
This theme explained informants’ psychological and behavioural responses towards cancer-related fatigue and its impacts. The subthemes included (1) not discussing cancer-related fatigue, (2) resisting encouragement and support from others, (3) hiding the true cancer-related fatigue experience: ‘I am feeling good’, (4) withdrawing from social life and (5) attempting to control cancer-related fatigue.
Subtheme 1: Not discussing cancer-related fatigue
The informants consciously or unconsciously protected themselves from ‘uncomfortable occasions’ associated with the cancer-related fatigue experience. They did not discuss the experience of cancer-related fatigue with the people closest to them. Three informants maintained cognitive distance from the experience of cancer-related fatigue.
I couldn’t figure out what was going on. I don’t want to think about that too much, and I don’t have as much energy to think about it (I4).
They tended to avoid being at the centre of conversations with family members or friends and gossip amongst neighbours. One informant reported that he avoided talking about cancer-related fatigue with guests by changing topics.
When they ask me about my current physical condition, I’ll make a perfunctory remark and then remind them to drink tea or eat something (I9).
Subtheme 2: Resisting encouragement and support from others
The informants feared losing face because of their weakness and seeing disappointment, sympathy, disgust or ridicule in others’ eyes. Therefore, they just asked their family members and friends to treat them as ‘healthy people’ when they visited and resisted their encouragement and help. Two informants even described having provocative feelings.
One friend told me I should rest well and not worry. I asked him what his attitude would be if he were to experience severe cancer-related fatigue. I think that is very laughable. I wouldn’t say I like that sympathy (I18).
Subtheme 3: Hiding the true cancer-related fatigue experience: ‘I am feeling good’
Half of the informants described that they tried to hide cancer-related fatigue from their next of kin to varying degrees and concealed the truth about their cancer diagnosis. They always responded with ‘feeling good’ and with a ‘smile’, trying not to make others feel terrible. Informants described their reluctance to confide in their family members to avoid imposing a burden on them. They also tried to show a fighting spirit by enduring cancer-related fatigue as much as possible and repressing their feelings related to cancer-related fatigue, implying they could still do what they used to be able to do. As one male informant described:
I try to get my spirits up when I’m feeling uncomfortable. I try to let myself show less weakness. . . I don’t want to . . . let my family think that my condition is severe (I9).
Subtheme 4: Withdrawing from social life
The cancer-related fatigue experience brought about relational and social fears in the informants, their families and friends, as cancer-related fatigue resulted from cancer. Informants tended to avoid active contact with the outside world. They reduced participation in social activities, including group exercises, and engaged less in meaningful relationships with others. This status of withdrawing from social life and staying at home in solitude enabled them to obtain inner peace and happiness. Some informants were also forced to isolate themselves because of malicious speculation from others. In rural areas of China, people traditionally regard cancer as a sign of bad luck, making others ‘pull away’. People also tend to misrecognise cancer as an infectious disease. These speculations caused informants’ to be unable to attend activities in the community.
Some asked me: ‘What is wrong with you? How did you become so thin?’ I said that I did not know. I dared not speak and face it. I’m so embarrassed to go out now. I always stay at home (I21).
When others in rural areas know you have cancer, they will detour away as soon as you look sick (I5).
Subtheme 5: Attempting to control cancer-related fatigue
Given the persistence of cancer-related fatigue, informants tended to seek methods to take some control over the possible worsening of the cancer-related fatigue and its persistent effects on their daily life. Many informants reflected, ‘It is too much to handle’, and so they never gave up on trying different strategies to alleviate the physical and mental symptoms of cancer-related fatigue. The attempted strategies included modifying their diets, taking naps, lying down and sitting for a while, doing something they liked, practising distraction and even smoking. The most common strategies were sleeping and lying down for a while. One informant regarded smoking as a way to relieve cancer-related fatigue.
If you can eat, you have good spirits (I11).
You know, just curl up or sleep (I19).
I just sat on the couch for a while and watched TV, and this seemed to give me a boost (I6).
Just go around, walk around, and still have no energy (I15).
I now smoke a pack of cigarettes for 3 days, and I would choose to smoke instead of lying down and sleeping (I20).
Discussion
This study highlights the multidimensional experience of cancer-related fatigue along the advanced lung cancer trajectory, bringing about severe effects on daily life. Experiencing cancer-related fatigue trapped people with advanced lung cancer in negative emotional responses, including pessimistic beliefs, searching for root causes and negative attitudes about role changes. These negative responses led to avoidant coping patterns and ignoring what they truly valued. Customised psychological support is recommended to meet the palliative care needs of this population.
The multidimensional experiences of cancer-related fatigue were consistent with the findings of previous studies in cancer populations.22,51–55 These findings may fill the gap in comprehensively understanding cancer-related fatigue from their perspective, rather than from the investigator’s observations. The multifaceted cancer-related fatigue experience helps healthcare providers to discover the individuals’ physical and emotional boundaries and thus, in turn, suggest timely strategies to break unhelpful habits and negative beliefs about cancer-related fatigue and facilitate new modes of behaviour. 14 In addition, the results provide insights into developing interventions to manage the experience of cancer-related fatigue from a multifaceted perspective.
The physical effects of cancer-related fatigue aligned with those identified in previous studies.30,31,56 The possible reason may be related to the nature of the cancer-related fatigue, which cannot be relieved by rest. Long-term treatments related to advanced lung cancer also bring about persistent side effects, including cancer-related fatigue.
Informants worried about their future being limited by cancer-related fatigue and were concerned about survivorship. These worries and a sense of hopelessness were consistent with the findings of previous studies.56,57 In Confucian thought and Chinese family culture, there are three ways of being unfilial: (1) the inability to support one’s parents, love one’s family and fulfil one’s responsibilities as offspring; (2) the failure to abide by one’s duties and act faithfully; and (3) the inability to conduct self-cultivation and become a virtuous person. The informants’ frustration was related to this cultural attribution 34 : a failure to fulfil these positive duties and obligations. 58 As the cancer-related fatigue experience may lead individuals to be unable to complete their family responsibilities, to impose a burden on their family and to incur a tremendous financial burden, they may suffer from emotional distress. As such, helping them reconnect to the present moment to loosen their bondage to the past or their imagined future is highly recommended.
In addition, cancer-related fatigue influenced the informants’ social well-being. The curtailed social interactions may be related to the influence of Confucian ideas. Chinese strongly prefer interpersonal harmony 59 and consider it one of the critical elements of a meaningful life. They may be afraid of breaking this interpersonal harmony due to the sense of shame arising from cancer-related fatigue; thus, they keep social distancing to avoid possible conflicts and to protect their self-esteem. 60 Considering the increasing number of culturally and linguistically diverse populations living in countries in which they were not born, especially with 466,000 Chinese immigrants living in the countries belonging to the organisation for economic co-operation and development until 2019, 61 healthcare professionals with different backgrounds should consider and address the psychosocial impacts of cancer-related fatigue on people with advanced lung cancer, preparing for providing culturally competent palliative care. 62
Informants held pessimistic beliefs about their cancer-related fatigue experiences, regarding them as a sign of a ‘bad ending’, which is consistent with the findings of previous studies.51,55,63 The experience of cancer-related fatigue perceived after receiving treatment, as well as the misconception of the cancer-related fatigue experience, affected their perception of lung cancer, such that they thought they were dying soon. One possible explanation is that symptom perception is a holistic psychological process of evaluating bodily sensations. 64 Consequences associated with worsening cancer-related fatigue may shape an individual’s attitudes, which then influence the psychological evaluation of their bodily sensations. The other potential explanation may be because that the informants grew up in a culture with severe negative preferences and were encouraged to pay more attention to their pain and problems. 63 Such conventional thinking made it easy for them to catastrophise the cancer-related fatigue experience, further regurgitating their thinking and constantly questioning the injustice of fate by repeatedly asking, ‘why me?’. In China, individuals are also constrained by the traditional thoughts that the man is the breadwinner of the family and should work hard and earn money to support the family. Moral qualities in Chinese culture are rooted in a strong work ethic. Male informants tended to regard themselves as a ‘burden’ to their families. Due to cancer-related fatigue, the unfulfilled family responsibility led to low self-esteem, 65 thus aggravating their sense of guilt and hopelessness. These disparities may be influenced by culturally determined beliefs and behaviours. Different from the ethical principle of respecting patient autonomy in Western countries, collectivist cultures, such as those found in China, tend to viewing family members as a ‘unit’, thus usually considering families’ feelings during the palliative care process. 66 In this case, conducting cultural assessments on hospitalised individuals will assist in developing people-centred approaches to care for culturally and linguistically diverse populations. 62
Consistent with previous studies,53,57 as a consequence of their feelings about cancer-related fatigue, the informants described a sense of loss of self, such as negative self-evaluations due to cancer-related fatigue and negative cognition of others’ attitudes towards themselves. The informants may have become fused with the previously mentioned negative emotional responses to cancer-related fatigue, and immersed in their subjective thoughts, resulting in inflexible self-evaluations. This self-identity change is related to low self-esteem in Chinese culture. 65
The informants tended to avoid discussing their cancer-related fatigue experience. This aligns with those from previous studies.57,67,68 The possible reason is related to their lack of understanding of cancer-related fatigue. They could not rationalise the link between their cancer-related fatigue experience and their advanced lung cancer diagnosis. 69 The Chinese culture may also explain this finding. Most people with advanced lung cancer were from rural areas and born from the 1950s to the 1970s. In China, especially in rural areas, people regard cancer as a form of retribution for their own/ancestors’ misdeeds. 70 People tend to ‘pull away’ once someone is diagnosed with cancer or suspected of having cancer due to a sick appearance. Thus, to respond to the perceived pressure of public opinion, the informants avoided showing themselves as listless in front of others and discussing their disease.
The informants were reluctant to receive care and support from others. This finding may be due to the cultural origins of the Chinese concept of ‘face’ in Confucian society. People strive to earn positive evaluations from others and protect their public image to maintain their psychosocial equilibrium and social self-esteem. 60 The disclosure of private matters, such as the inability to work due to cancer-related fatigue, shows weakness and incompetence to others, resulting in a sense of losing face. 71 By refusing care from others, people protect themselves from further reinforcing the sensation.
The informants also hid their emotional responses associated with cancer-related fatigue and forthcoming death to maintain family harmony. This finding was not surprising. In Chinese culture, ‘forbearing’ internal experiences and avoiding negative emotions are important virtues. In a collectivistic culture, harmony is advocated by avoiding personal feelings and emotions to prevent interpersonal conflict. 35 These cultural factors made them reluctant to express their real feelings about cancer-related fatigue to those closest to them. Due to the differences of emotional disclosure and moral distress related to the conflict between Western models of care and competing values from culturally and linguistically diverse populations, appropriate training is recommended for healthcare providers to address the ethical dilemmas and promote quality care delivery. 72 Considering that people tend to hold on to what is pleasant and push away things that are unpleasant, by cultivating a willingness to be equally near pleasant and unpleasant experiences (i.e. cancer-related fatigue and its impacts), they can learn to accept the facts and relate to that what is present in the moment.73,74 Furthermore, the informants closed themselves off by reducing the times they went out and avoiding group activities, using various strategies to control cancer-related fatigue. Although these strategies were able to diminish the cancer-related fatigue level in the short term, informants noticed the unworkability and even aggravation of cancer-related fatigue, which exacerbated their psychological distress and sense of meaninglessness. This finding indicates a need to provide flexible management of cancer-related fatigue to better adapt to it.
Strengths and limitations
This study is one of the few qualitative studies to reveal the experiences of cancer-related fatigue, its impacts on daily life, emotional reactions to and strategies of coping with cancer-related fatigue amongst Chinese people with advanced lung cancer. Measures have been taken to realise the researcher’s reflexivity in the study. First, twenty-one interview texts were read through several times to reach immersion and complete familiarity with the data. Second, detailed field notes, including observation notes (i.e. a description of the physical setting, nonverbal expression and emotional status) and reflective notes (the researcher’s speculation, feelings and impressions), were also documented during and after the interview. Third, analysis results were discussed with team members to increase trustworthiness. Fourth, no direct nurse-client relationship existed between the researcher (HL) and informants to influence interviews. The researchers provided an audit trail to determine that the informants’ responses were not based on any potential bias or personal motivations of the researchers.
Several limitations should be noted. First, this study was conducted in south-central China. The findings may not represent the experience of all Chinese population. Second, imbalances still existed despite applying the maximum variation strategy to select participants with different demographic and clinical characteristics. For example, approximately 71.4% (n = 15) of the informants were male due to the epidemiological feature of a higher incidence of lung cancer in men, and 66.7% (n = 14) of them were from rural areas. Third, this study lacked further exploration of subgroups of people with advanced lung cancer. Future studies are recommended to compare the experiences of cancer-related fatigue in different subgroups, such as men versus women, non-small cell lung cancer versus small cell lung cancer, stage III versus stage IV cancer and different age groups, to enrich the findings. Furthermore, the researcher is still necessary for the researcher to make full use of the reflexivity principle throughout the research process and present it in multiple dimensions throughout the report. In future qualitative studies, the researcher’s reflexivity on personal (i.e. reporting how the researcher’s unique perspectives influence the research), interpersonal (i.e. documenting what power dynamics are at play), methodological (i.e. documenting how the researcher makes methodological decisions) and contextual (i.e. summarising how aspects of context affect the research and the people involved) aspects should be included. 75 This will further increase transparency by helping the researcher consciously reflect on their role in the qualitative process.
Implications
The findings increase our understanding of the experience of cancer-related fatigue from a comprehensive perspective. Oncological healthcare professionals should keep abreast of individuals’ experiences of cancer-related fatigue and prioritise their needs during palliative care. Providing psychological support may enable people who are distressed to become aware of the root cause and extent of their issues. 76 People should be informed that cancer-related fatigue is a natural part of the advanced lung cancer trajectory that interferes with different aspects of daily life, but appropriate interventions can decrease its impacts and improve their coping ability.
In light of these findings, an inflexible adaptation to cancer-related fatigue and its impacts exists, and this process includes avoiding the disclosure of cancer-related fatigue and attempting to control cancer-related fatigue and its impacts, being stuck in negative emotions and attitudes towards cancer-related fatigue, self-labelling about the fatigued status and a blurred life direction. This process may correspond to the acceptance and commitment therapy model’s pathological processes, namely psychological inflexibility, 77 including six subprocesses: experiential avoidance, cognitive fusion, dominance of the future or past, attachment to the self-story, lack of clarity or contact with values and lack of action or impulsivity. 78 It is a widely used mindfulness-based cognitive behavioural therapy that targets the psychological flexibility of an individual, and posits that an individual’s psychological flexibility can be fostered by using metaphors, experiential exercises and/or mindfulness exercises, so that he/she can develop acceptance of psychological difficulties on distressing experiences, awareness of life values and commitments to take values-driven action. 78 A previous systematic review by our research team and a latest meta-analysis by Fang et al.–have shown its promising effects in improving cancer-related fatigue and other health outcomes in people with advanced cancer. 79 , 80 Nonetheless, most studies were conducted with small sample sizes in Western countries, thus more rigorous full-scall randomised controlled trials are recommended to further confirm the effects of acceptance and commitment therapy for managing cancer-related fatigue. Based on the findings of the systematic reviews and qualitative study, developing an acceptance and commitment therapy-based intervention adapted to Chinese culture may be far-reaching for people with advanced lung cancer experiencing cancer-related fatigue in China. Acceptance-based interventions can be promising to help promote psychological flexibility, improve functional interference, allow difficult thoughts and feelings about cancer-related fatigue and encourage paying attention to what matters.
In addition, the experience of cancer-related fatigue in people with advanced lung cancer, including their interpretation of their condition, coping style and behavioural pattern, was deeply influenced by traditional Chinese culture. As Chinese immigrants are increasingly growing in different parts of the world. Understanding what matters to Chinese people matters. From our qualitative findings, it is notable that the reactions and copings towards cancer-related fatigue in Chinese people with advanced lung cancer are deeply influenced by face, self-esteem, family responsibility and interpersonal harmony in Chinese Confucian culture. When taking care of the Chinese population, healthcare professionals should carefully consider these cultural issues and actively engage in attempts to accommodate their cultural beliefs. This could help health professionals avoid exacerbating other negative impacts and provide culturally appropriate and equitable care. On the other hand, these findings also provide insights into exploring cancer-related fatigue in palliative care and providing quality care for culturally and linguistically diverse populations. It is known that culturally and linguistically diverse populations are vulnerable to marginalisation and receive inadequate palliative care. 61 Healthcare providers are recommended to actively engage in attempts to accommodate cultural beliefs, including receiving training to address ethical dilemmas, and collaborating with communities to provide tailored education and information for people with diverse cultural backgrounds.61,81 Raising healthcare providers’ awareness will benefit them in providing culturally competent cancer-related fatigue management and integrating culturally sensitive acceptance-and-commitment-therapy-based interventions into routine palliative care.
Conclusion
This qualitative study explored the experience of cancer-related fatigue in Chinese people with advanced lung cancer. The findings revealed the multifaceted experience of cancer-related fatigue, the diverse impacts of cancer-related fatigue, the negative perceptions of cancer-related fatigue and avoiding cancer-related fatigue. An inflexible psychological adaptation process to cancer-related fatigue was found in the Chinese cultural context, following a sense of meaninglessness. Future research should focus on developing and implementing Acceptance-based interventions based on the cultural context to foster accepting the experience of cancer-related fatigue and increase the overall quality of life amongst people with advanced lung cancer.
Footnotes
Acknowledgements
The authors are grateful to Ms Nina Wang for her assistance with identifying participants for the study and people with advanced lung cancer who participated.
Author contributions
HL, CLW and MSNN conceived the study. HL and XJ jointly analysed and interpreted the data. HL drafted the manuscript. All authors revised the manuscript critically and approved the final version.
Data management and sharing
The datasets generated and analysed during the current study are not publicly available due to privacy protection and ethical considerations but are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.