
Abstract
Background:
Dry mouth is a disruptive symptom in patients with life-limiting illnesses. It has one of the highest symptom burdens in palliative care and a significant impact on quality of life. Nonetheless, dry mouth remains an underacknowledged and undertreated symptom with limited evidence-based interventions.
Aim:
To examine the quality and content of guidelines for the treatment of dry mouth in patients with life-limiting illnesses.
Design:
A systematic review of clinical practice guidelines was conducted (preregistered in PROSPERO in 2023). PRISMA reporting guidelines were followed. The search strategy involved 4 scientific databases and 9 guideline databases, targeted searches and stakeholder outreach for 183 countries/regions. Quality and content were analysed using the AGREE II instrument and directed content analysis, respectively.
Data sources:
Seventy-two clinical practice guidelines from 42 countries across 6 continents were included.
Results:
Only two guidelines were recommended for use based on the AGREE II quality appraisal. Four main themes emerged from the content analysis: (1) Assessment of dry mouth by medical history, oral examination and measuring instruments (n = 32, n = 36 and n = 19 guidelines respectively); (2) Oral care (n = 68); (3) Management by treating causes (n = 40), saliva substitutes (n = 66) and stimulants (n = 62), diet (n = 45), and medication (n = 40); and (4) Patient and family involvement (n = 43).
Conclusion:
Despite differences in quality and comprehensiveness of guidelines for treatment of dry mouth in palliative care, many care practices are shared worldwide. This review highlights the need for methodologically robust guidelines with a strong evidence base that specifically focus on dry mouth.
Dry mouth is a prevalent and severely distressing symptom in patients with life-limiting illnesses.
Dry mouth is underacknowledged by patients, health care professionals, and in scientific research, leading to inadequate treatment.
Clinical practice guidelines in palliative care are a key facilitator for improving both knowledge and care practices, including symptom management of dry mouth.
Quality of guidelines for dry mouth is limited, and most recommendations are based on expert opinion rather than (graded) scientific evidence.
Few guidelines fully focus on oral problems (including dry mouth) in palliative care, and most recommendations are non-specific in nature.
While the methodological quality and comprehensiveness vary widely across guidelines, there is a high level of consistency among recommendations for the assessment of dry mouth, the role of oral care, the management of dry mouth, and the patient and family involvement in dry mouth care.
This study highlights the necessity of developing methodologically robust, easy-to-use guidelines that specifically focus on dry mouth in palliative care.
Guidelines for dry mouth should include detailed, practical recommendations for the assessment and management of dry mouth, adapted to local context, and with an increased focus on the psychosocial dimension of dry mouth.
Future research should focus on evaluating current dry mouth care practices in high quality clinical trials in the palliative care setting, and on identifying new dry mouth treatment options.
Introduction
Dry mouth is a common and disruptive symptom in people in all phases of palliative care, and with different underlying life-limiting conditions, such as advanced cancer, severe systemic diseases, and geriatric frailty. 1 Dry mouth may result from reduced salivary flow due to salivary gland hypofunction (hyposalivation) or occur as a subjective sensation of oral dryness (xerostomia) that is not always explained by decreased saliva production. 2 It is present in 40%–83.5% of patients with advanced cancer,3–6 and up to 91% in terminally ill cancer patients. 7 Similarly, 40%–70% of frail older people suffer from dry mouth,8–10 around 60% of patients with advanced COPD or heart failure,11,12 28%–74% of patients with end-stage renal disease 13 and 59% of hospitalised HIV/AIDS patients. 14
Dry mouth is a highly disruptive symptom in daily life.1,15,16 It can have a severe functional impact on swallowing, eating, sleeping, and speaking, and may lead to pain, infection, halitosis and other oral symptoms.15,17–20 Dry mouth is also known to have a significant psychosocial impact and has one of the highest symptom burdens for patients with advanced diseases.6,16,21 It affects patients’ social interaction and intimacy,17–19 leads to feelings of shame and loneliness,18,22 and is associated with anxiety and depression.21,22
Dry mouth is an underacknowledged and undertreated symptom by patients, family caregivers, and healthcare professionals. Few patients report their dry mouth, perceiving their symptoms as an inevitable consequence of their disease or treatment, and being unaware of available treatment options.19,23 Healthcare professionals do not systematically or appropriately assess oral health and dry mouth in patients with life-limiting illnesses.19,24–26 They report a lack of knowledge and confidence in conducting oral health consultations and in providing oral care.25,26 Furthermore, healthcare professionals have reported to consider dry mouth to be someone else’s responsibility and a low priority condition.23,26,27 Suggested reasons for this include limited formal training and a lack of uniform guidelines.23,24,26,27 In addition, scientific evidence for the effect of dry mouth interventions is limited and of low quality, both in general28–30 and for patients with life-limiting illnesses.31,32 Therefore, an overview of current best practice is needed to provide a foundation for clinical practice and future research. Based on the best available evidence, best practices can be found in clinical practice guidelines.
Clinical practice guidelines are used to formalise and standardise clinical practice with the aim of improving quality of care.33,34 They assist health care professionals’ decision-making, as well as highlight areas of (in)effective treatment.34,35 While there is no evidence yet for dry mouth guidelines specifically, both the World Health Organisation and previous research have suggested that palliative care guidelines and oral health guidelines can improve awareness, knowledge and effectiveness of care practices.33,36–39
To our knowledge, no formal evaluation has been conducted to analyse the quality and content of clinical practice guidelines for dry mouth in palliative care. This review therefore aims to provide insight into current standards for care practices for dry mouth in patients with life-limiting illnesses.
Specifically, the aim of this review is to:
Analyse the quality of clinical practice guidelines for dry mouth in patients with life-limiting illnesses.
Analyse the content and consistency of clinical practice guideline recommendations for the assessment and treatment of the symptom dry mouth in patients with life-limiting illnesses.
Methods
Design
This systematic review was conducted based on the recommendations for reviews of clinical practice guidelines from Johnston et al. (2019) 40 and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol. 41 The review was pre-registered using the International Prospective Register of Systematic Reviews (PROSPERO, CRD42023415285). 42
Search strategy
Multiple search processes were employed to ensure a wide international coverage of clinical practice guidelines. The search strategy combined two search strings related to (1) dry mouth and (2) clinical practice guidelines. In addition, search strings related to (3) oral care were included in all search processes except the scientific database searches (see Supplemental File 1).
First, a systematic literature search in four scientific databases (PubMed, CINAHL, Cochrane Library and EMBASE) was conducted with an information specialist (first search November 2023, updated August 2025).
Second, nine guideline databases were searched (Trip Pro, BIGG International Database of GRADE guidelines, ECRI Guidelines Trust, GIN International Guidelines Library, Scottish Intercollegiate Guidelines Network (SIGN), U.S. Preventive Services Task Force (USPSTF) Database, Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) Leitlinien Register, WHO Guidelines, GRADEpro GDT database).
Third, targeted searches were performed for 183 countries and other territories across six continents (Europe, Asia, North America, South America, Africa, Oceania). These countries were selected based on the list of EAPC members, the directory of the International Association for Hospice and Palliative Care (IAHPC), 43 the APCA Atlas of Palliative Care in Africa, 44 the EAPC Atlas of Palliative Care in Europe, 45 the Atlas of Palliative Care in Latin America 46 and the Atlas of Palliative Care in the Eastern Mediterranean region. 47 Searches were conducted in the language of origin for each country and in English.
Fourth, at least one key stakeholder per country (if available) was approached via email to request any clinical practice guidelines, and/or to confirm the use of a clinical practice guideline found in one of the other search steps. This stakeholder was preferably a national representative for palliative care, identified from the IAHPC directory, 43 the Palliative Care Atlases44–47 or a key scientific publication (see Supplemental File 2 for more information on the targeted searches & stakeholder outreach).
Fifth, additional clinical practice guidelines were searched by screening the reference lists in the included guidelines.
Eligibility criteria & screening
The PICAR framework (Population, Intervention(s), Comparator(s), Attributes of eligible clinical guidelines and Recommendation characteristics) 40 was used to define the criteria for eligibility (Table 1).
PICAR framework 40 for systematic reviews.
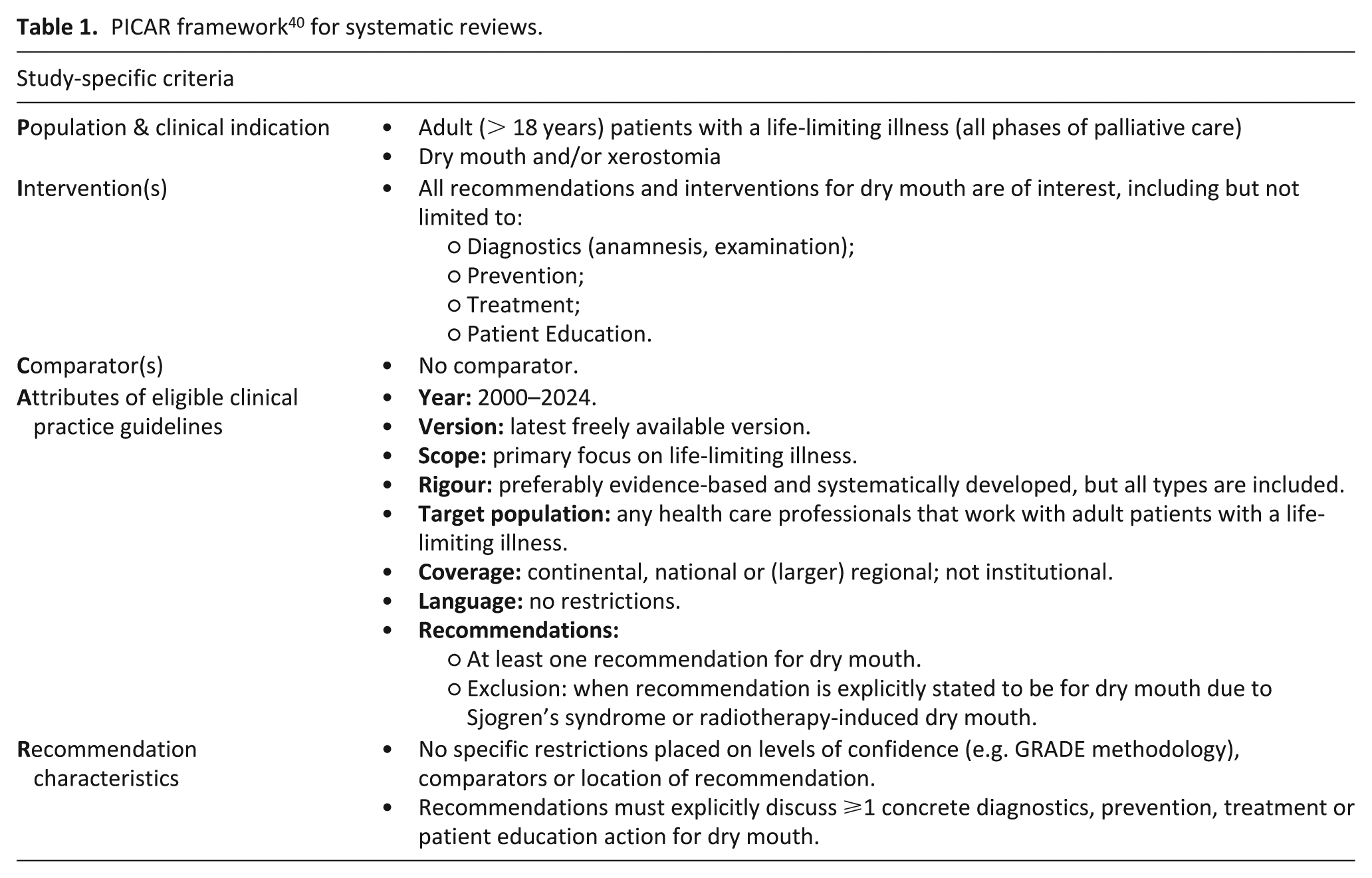
Five main criteria were used during screening:
Document is a clinical practice guideline. The frequently used clinical practice guideline definition by Lohr et al. 1999 was considered as a starting point: ‘systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances’. 48 To allow for guidelines with varying levels of quality and comprehensiveness, our interpretation of a clinical practice guideline was expanded to include guidelines that may not have a systematic review underpinning the recommendations but have been developed and endorsed by a (national) professional organisation, or group of experts.
Document provides recommendation(s) for dry mouth. Clinical practice guidelines with recommendations explicitly targeted at dry mouth caused by Sjogren’s syndrome or radiotherapy for head and neck cancer were excluded. If guidelines also addressed dry mouth in broader populations, they were included, but any recommendations specific to radiotherapy-induced or Sjogren’s-related dry mouth were not extracted or coded (unless mentioned otherwise).
Document is related to adult patients (over 18 years) in palliative care (as defined by the WHO definition). 49 This included patients in all phases of palliative care and with varying life-limiting illnesses, with no restrictions on type of disease, prognosis or life stage. Eligible guidelines encompassed palliative care, end-of-life and terminal care in general, but also advanced diseases (including but not limited to cancer) and geriatric frailty.
Document has a regional, national or international coverage. There were no restrictions based on language of the clinical practice guideline.
Document is published after the year of 2000, and is the latest version available and accessible.
Potential clinical practice guidelines were screened by two independent researchers (AM and AS), both with a background in palliative care (as a medical doctor and researcher, and as former nurse and post-doctoral researcher, respectively). Clinical practice guidelines were screened independently using Rayyan.ai. After screening, any disagreements were discussed until consensus was reached. When necessary, the wider research group was involved to reach consensus, which consisted of two palliative care specialists (radiation oncologist (YL) and internal medicine specialist (MB), and one post-doctoral palliative care researcher (MT)).
Data extraction
All relevant supporting documents were retrieved before data extraction and analysis. Data extraction was completed by one researcher (AM) and verified by an independent reviewer for accuracy and completion (AS). General characteristics of each included clinical practice guideline were recorded, such as title, author information, year of publication, and target population.
Quality appraisal
The Appraisal of Guidelines for Research and Evaluation Instrument version 2 (AGREE II, online portal: AGREE Plus) was used to assess the quality of the clinical practice guidelines. 35
The 23-item AGREE II tool considers the quality of the clinical practice guideline in terms of scope and purpose, stakeholder involvement, rigour of development, clarity of presentation, applicability and editorial independence. Reviewers score each item from strongly disagree to strongly agree (seven-point Likert scale), after which scaled domain scores are calculated. In addition, a ‘global judgement’ about the clinical practice guideline is made by reviewers to assess the perceived overall quality and recommendation of the clinical practice guideline. 35 Two reviewers (AM, AS) independently applied the AGREE II tool to all clinical practice guidelines. Rater reliability was measured by a two-way mixed effects intraclass correlation coefficient (ICC) for consistency of agreement, using IBM SPSS Statistics v25.
Directed content analysis
To assess the consistency of recommendations in the clinical practice guidelines and identify overarching themes and potential content gaps a directed content analysis was used. 50 After familiarisation with the included clinical practice guidelines, key components of all clinical practice guidelines were independently identified by AS and AM and used as the foundation of the coding framework. This initial deductive approach was then supplemented by inductively adding and adapting codes during the coding process. ATLAS.ti software (v25) was used to collect and analyse the content of the clinical practice guidelines. Clinical practice guidelines were analysed using the English translation of the original document.
Results
Searches retrieved 1749 records from the scientific databases, 717 from the guideline databases and 74 from targeted searching and stakeholder outreach. After deduplication and screening of records, 72 clinical practice guidelines were included in the systematic review. Figure 1 presents the PRISMA flowchart of the guideline selection.
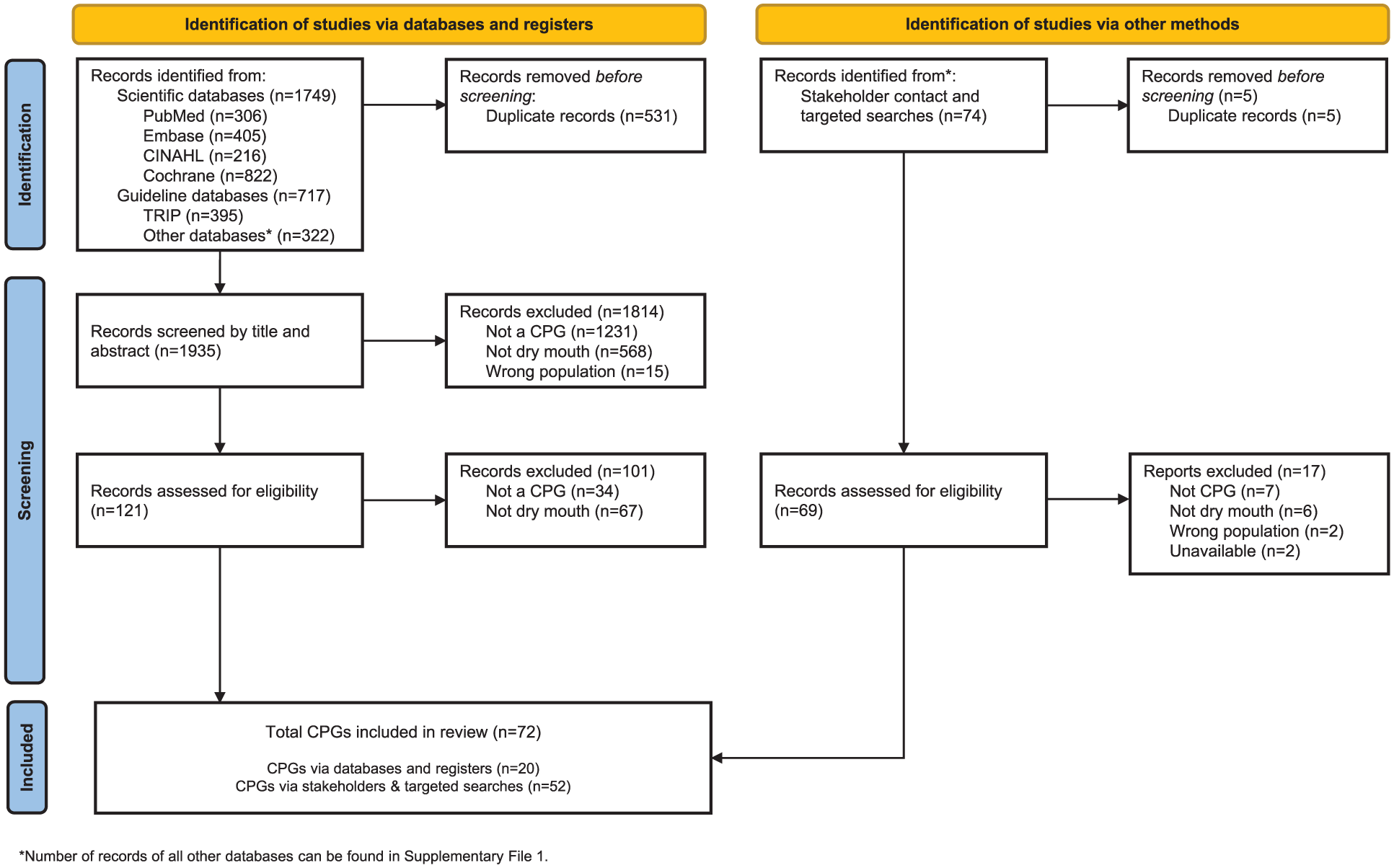
PRISMA flowchart of included clinical practice guidelines (n = 72).
Characteristics of included clinical practice guidelines
General characteristics of the 72 included clinical practice guidelines are shown in Table 2. Guidelines were from 42 different countries across 6 continents. Most included clinical practice guidelines were developed in Europe (n = 26) and Central and South America (n = 13), followed by Africa (n = 8). An additional seven guidelines were not nation-specific but international-based. The comprehensiveness of the dry mouth sections within the clinical practice guidelines varied from limited (n = 35; up to a few recommendations), moderate (n = 25; subsection or multiple recommendations) to extensive (n = 12; guideline, chapter or large subsection). For a detailed overview of each included clinical practice guideline, see Supplemental File 3.
Characteristics of included clinical practice guidelines (n = 72).
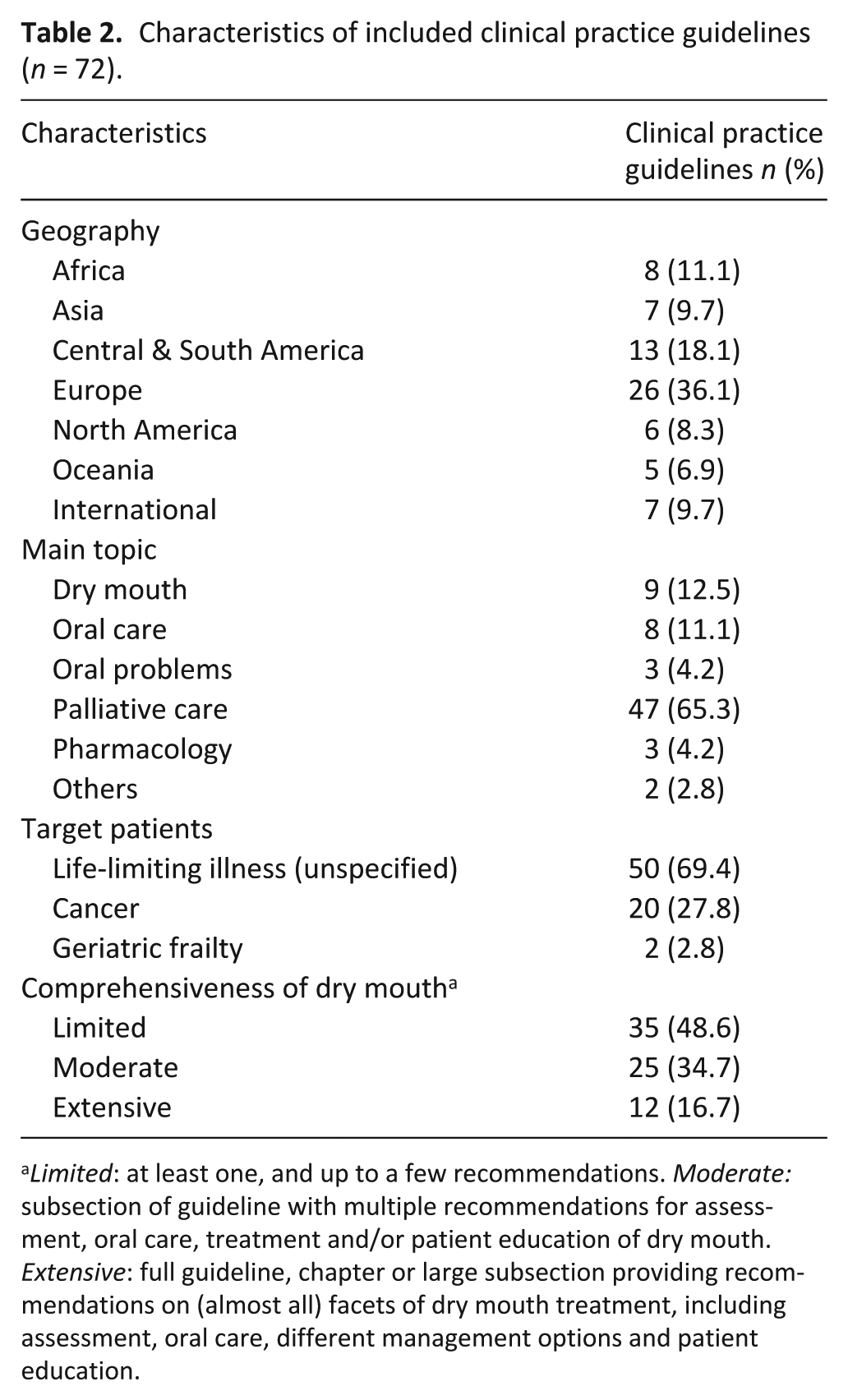
Limited: at least one, and up to a few recommendations. Moderate: subsection of guideline with multiple recommendations for assessment, oral care, treatment and/or patient education of dry mouth. Extensive: full guideline, chapter or large subsection providing recommendations on (almost all) facets of dry mouth treatment, including assessment, oral care, different management options and patient education.
Quality appraisal
The quality appraisal per AGREE II for all included clinical practice guidelines and the rater reliability are presented in Supplemental File 4. Domain 4 (clarity and presentation) scored the highest, with 64/72 guidelines scoring ⩾60%. Domain 5 (applicability) scored lowest, with only 7/72 guidelines scoring ⩾60% and 45/72 scoring ⩽10%. Domain 3 (rigour of development) and domain 6 (editorial independence) also received low scores, both with only 15/72 guidelines scoring ⩾60%.
Two guidelines from Germany and the Netherlands were ‘recommended for use’ based on the AGREE II criteria,51,52 with another 14 clinical practice guidelines recommended with modifications. The clinical practice guideline from Germany recorded the highest overall score.
The rater reliability was consistently high for each domain of the AGREE II (ICC = 0.79–0.96, p < 0.001).
Content analysis and synthesis
Four themes emerged from the synthesis: (1) assessment of dry mouth; (2) importance of oral care (3) management of dry mouth; and (4) patient education and family involvement. Full content analysis is presented in Table 3.
Content analysis of dry mouth recommendations in the included clinical practice guidelines (n = 72).

Empty cell means: no recommendation available; NCI-CTCAE: NCI common terminology criteria for adverse events; RTOG/EORTC: radiation therapy oncology group/European organisation for research and treatment of cancer; LENT-SOMA: late effects normal tissue task force-subjective, objective, management, analytic; PRO Palliation: Danish patient-reported outcome form for palliation, CODS: clinical oral dryness score, GOHAI: geriatric oral health assessment index; meds: medication; (n)×/d: n times a day, Medication: RT-only: only indicated for radiotherapy-induced dry mouth; Stimulants: (T)ENS: (transcutaneous) electrical nerve stimulation; end-of-life care: care in the final days or weeks before death.
Theme 1: Assessment of dry mouth
Medical history (n = 32)
Structured and detailed questioning about dry mouth symptoms was recommended in 32 clinical practice guidelines. Topics deemed important for assessment included:
Information on the complaint (presence, severity, frequency, duration, fluctuation);
The impact of dry mouth symptoms on daily functioning;
Potential causes, including a review of medical history, medication and recent interventions, dietary habits and intake, history of smoking and alcohol, and oral hygiene
Factors that may influence the choice of intervention (such as comorbidities or the prognosis);
The oral care routine, and the ability to carry out oral care independently.
The most frequent recommendation was the review of medication to identify any drugs with possible xerostomic effects (n = 31). While most guidelines mentioned the functional and physical impact of dry mouth symptoms (such as the impact on nutritional status), only eight guidelines recommended asking about the psychosocial impact of dry mouth and coping ability.69,81,86,89,90,94,99,117
Oral examination (n = 36)
Oral examination to evaluate the severity of dry mouth and oral health status was recommended in 36 guidelines. Specific recommendations focussed on the presence of dry, cracked lips, the amount and texture of saliva, tongue fissures, the presence of halitosis, signs that may indicate concurrent infection (fungal, viral or bacterial), mucositis, gingivitis/periodontitis, and ill-fitting dentures.
Regular monitoring (n = 23)
Specific frequency for monitoring of dry mouth was recommended in 23 guidelines: daily assessment (n = 8),55,56,65,83,84,100,105,120 at least twice a week (n = 1), 92 and at every contact with a health care provider (n = 5),52,68,88,105,116 while other guidelines gave less detailed instructions (n = 9, ‘often’, ‘regularly’).51,66,87,89,94,105,113,116,119
Measurement instruments (n = 19)
Specific measuring instruments were recommended in 19 guidelines. These were recommended for use in assessment and monitoring of dry mouth severity, of frequency and impact, or in the differentiation between xerostomia and salivary gland hypofunction.
Patient-reported outcome measures focussed on severity or impact on quality of life, and included numeric rating scales (NRS) ranging from 0 to 10 (n = 5),52,68,69,90,101 1–4 (n = 2),75,76 and 0–4 (n = 4),51,78,99,122 the shortened Xerostomic Inventory (s-XI, n = 2),52,90 and oral health assessment tools (n = 2; OSAS; EORTC QLQ - OH15). 89 Physician initiated tools included oral assessment guides (n = 7, of which n = 2 for the validated Oral Health Assessment Tool (OHAT)),52,65,81,84,94,105,116 the spatula/mirror test (n = 1), 101 and dry mouth severity grading scales (Xerostomia NCI CTCAE grading scale (n = 3) and other (n = 2)).52,68,90,94,116 Three guidelines recommended sialometry to differentiate between xerostomia and salivary gland hypofunction/hyposalivation.52,101,119 One guideline noted that sialometry might be inappropriate for some patients with a life-limiting disease due to added burden. 52
Theme 2: Oral care
Importance of oral care (n = 68)
68 clinical practice guidelines emphasised the importance of oral care within the prevention and management of dry mouth.
Oral care routine (n = 60)
Specific oral care instructions included: brushing teeth a minimum of twice a day (n = 25), using a mild toothpaste with fluoride (n = 22), or a prescription-strength fluoride toothpaste (5000 ppm; n = 7)52,68,69,81,87,89,115; using a mild, non-alcoholic mouth rinse (n = 50; water, saline, baking soda and/or fluoride); and avoiding alcohol-based oral care products (n = 13).
Moisturising the lips was recommended by 47 clinical practice guidelines, with petroleum jelly (e.g. Vaseline; n = 18), water-soluble lubricants (n = 12) and cocoa butter (n = 7)55,56,70,71,107,120,121 as the most recommended products. Six clinical practice guidelines specifically recommended against using petroleum jelly due its hydrophobic and flammable nature.52,55,61,104,107,116 Glycerine-based toothpaste and moisturising gels were recommended in three75,86,107 but cautioned against in seven guidelines,51,52,69,84,89,98,105 due to reported humectant benefits versus potential dehydrating effects.
Oral care in the weakened or dying person (n = 22)
Recommendations specific to the weakened or dying person were offered in 22 guidelines. These focussed on oral comfort rather than oral hygiene, increasing the frequency of oral care and moistening the mouth with soft materials other than toothbrushes (like swabs, gauzes, sponge sticks) and with sprays.
Role of the dental health care professional (n = 22)
Active involvement of a dental professional was recommended in 22 guidelines, for regular checkups, and for specialist advice for treatment-resistant dry mouth and concurrent oral problems.
Theme 3: Management of dry mouth
Recommendations for the management of dry mouth mostly consisted of treating the underlying cause, (non)-pharmacological saliva substitution, non-pharmacological saliva stimulation, dietary advice and medication.
Treating underlying cause (n = 40)
Interventions treating the underlying cause included replacing or removing xerogenic medication (n = 26); managing underlying diseases (e.g. diabetes, HIV infection, Sjogren’s syndrome; n = 19); treating oral infections and diseases (n = 11), humidifying patients’ oxygen (n = 6)55,67,86,104,105,117; using a room humidifier in dry or warm environments (n = 16); and reducing or avoiding smoking (n = 12), alcohol use (n = 14) and caffeine consumption (n = 9).52,61,68,69,100,103,105,109,118
Substituting saliva (n = 66)
Frequently sipping fluids, or using sponges/swabs with fluids, was recommended in 55 clinical practice guidelines to substitute saliva and moisten the mouth. Most clinical practice guidelines recommended water or unsweetened, non-acidic drinks to moisten the mouth, while four mentioned to offer any drinks the patient prefers. Saliva substitution products made from natural or household compounds were recommended (n = 24), including cooking oil (n = 11), chamomile (n = 8),70,55,77,96–98,107,108 and sage (n = 2).52,77
Commercial saliva substitutes to alleviate dry mouth were recommended in 53 guidelines. Common substitutes included: Biotene (OralBalance) spray or gel (n = 11), AS Saliva Orthana (n = 6)52,53,98,104,115,118 and BioXtra gel or spray (n = 3).84,98,115 The most common active ingredients in these substitutes were carboxymethylcellulose or hydroxyethyl cellulose, mucin, glycerine, xylitol, and fluoride. Half of the 12 guidelines that recommended a mucin-based product also mentioned its porcine origin, and potential issues with cultural, religious or dietary beliefs. Four clinical practice guidelines mentioned a cost-effective and accessible alternative for commercial saliva substitute: intraoral use of a water-based lubricating gel, primarily used for lubrication during intimacy (K-Y Jelly),62,105 and a recipe to make artificial saliva with methylcellulose, lemon essence and water.77,97
Stimulating saliva (n = 62)
Mechanical and gustative saliva stimulants (n = 62)
Frequently recommended mechanical stimulants were chewing on (sugar-free) gum (n = 44) and sucking on ice cubes, crushed ice or frozen pieces of fruit (n = 42). Other examples of mechanical stimulants were chewing on (sugar-free) hard sweets (n = 11) and sucking on pieces of fruit, lollipops and lozenges (n = 21).
The most mentioned gustative stimulants were acidic products, such as citrous fruits, sour sweets and fruit juices (n = 57). However, 22 clinical practice guidelines recommended avoiding these acidic products, due to their erosive and ulcerative effect on teeth and oral mucosa. Clinical practice guidelines (n = 36) that did recommend the use of (lightly) acidic products to stimulate saliva, specifically mentioned fresh or frozen pineapple (n = 31), sour candies (n = 7),51,74,84,86,88,102,105 vitamin C lozenges or tablets (n = 8),53,77,89,94,97,101,105,120 and sour teas (n = 3).51,96,101 Pineapple was also mentioned to be beneficial for dry mouth due to the soothing effect of its anti-inflammatory enzyme bromelain on oral mucosa (n = 3).51,105,117
Other saliva stimulants (n = 10)
Acupuncture was recommended in nine guidelines in the context of saliva stimulation (n = 7 for all patients with a life-limiting disease or frailty52,68,87,94,109,115,119; n = 3 for patients with radiotherapy-induced xerostomia only69,88,103).
Other saliva stimulants recommended were xylitol-based products (n = 12); sparkling or tonic water (n = 5),57,75,84,104,105 (transcutaneous) electrostimulation (recommended for all patients n = 452,87,91,119; for radiotherapy-induced xerostomia only n = 269,88); massaging the tongue, the oral cavity, the jaw and/or the parotid and submandibular gland (n = 3).84,91,93
Dietary advice (n = 45)
Dietary advice consisted of the amount of fluids, and the type of food and fluids that are appropriate and pleasant for patients with dry mouth.
Adequate fluid intake was recommended in 30 clinical practice guidelines, with four guidelines providing extra instructions for the amount of fluid, ranging from 1.5 to 2.5 l per day.68,94,96,121
Dietary recommendations were provided in 35 clinical practice guidelines. These included eating moist food or moistening food (n = 19), foods with soft consistency (n = 15), and eating frequently with small bites (n = 6).52,60,65,68,69,118 Particular foods were recommended to be avoided including dry and hard food (n = 13), spicy food (n = 13), thermally aggressive food (n = 8),60,61,68,69,80,85,102,103 sugary food (n = 20) or acidic food (n = 12). Few guidelines gave recommendations for specific food items or dishes. A Danish clinical practice guideline recommended sage tea and thin oat soup (thynd havresuppe) to alleviate sore mucosa due to dry mouth, 75 and three other guidelines recommended papaya.68,77,94
Medication (n = 40)
The pharmacological interventions most mentioned included pilocarpine (n = 37), bethanechol (n = 8), and cevimeline (n = 10).
Pilocarpine (n = 37)
Pilocarpine was recommended in 37 guidelines, with no consensus on dosage, form or frequency:
Pilocarpine eye drops (off-label; n = 9)57,60,75,76,91,97,100,102,105: pilocarpine 4% with dose ranging from 1 (~2 mg) to 5 (~10 mg) drops 3×/day; pilocarpine 1% with dose ranging from 5 (~2.5 mg) to 20 drops (~10 mg) 3×/day.
Pilocarpine tablets (n = 13)52,72,86,90–92,94,95,102,103,106,108,109: dose ranging from 2.5 to 10 mg 3×/day.
Pilocarpine rinse (n = 2)99,100: pilocarpine 1 mg/ml with a dose of 5–10 ml (5–10 mg) 3×/day.
32 clinical practice guidelines recommended pilocarpine for all patients with dry mouth, while five clinical practice guidelines recommended pilocarpine for radiotherapy-induced dry mouth only.68,82,88,115,116
Bethanechol (n = 8) and Cevimeline (n = 10)
Bethanechol as a pharmacological saliva stimulant was mentioned in eight clinical practice guidelines.68,69,87–89,91,94,105 Advice on dosage was provided in two guidelines: 10 mg 3×/day or 10–25 mg 3×/day.91,105 Cevimeline was mentioned in 10 clinical practice guidelines,68,69,81,88,89,91,93,96,102,119 of which two advised on dosage: 30 mg 3×/day.91,102 Cevimeline and bethanechol were only recommended for radiotherapy-induced xerostomia in two guidelines.69,88
Other medication
Other dry mouth medication mentioned were: anethole trithione (n = 3),69,87,91 local application of physostigmine (n = 1), 81 methacholine (n = 1) 94 and yohimbine (n = 2).87,94
Collaboration and referral (n=12)
Several guidelines (n = 12) emphasised the need for strong collaboration between healthcare professionals. This included seeking additional support from dieticians/nutritionists and speech and language therapists.
Theme 4: Patient education and family involvement (n = 43)
Most guidelines (n = 43) recommended educating patients and family on the importance of oral care and providing specific instructions. Other recommendations focussed on providing information on dry mouth, its complications and its treatment; answers to questions on the thirst versus dry mouth debate in end-of-life care; instructions to self-assess and monitor dry mouth regularly; and advice for substituting and stimulating saliva. One guideline provided written-out conversation guides for patient education. 93
Specific resources such as brochures or websites were recommended in 10 clinical practice guidelines.51,52,66–68,75,101,104,107,115 These corresponded with the recommendations provided in the clinical practice guidelines for professionals.
In the context of the weakened or dying patient, 26 clinical practice guidelines specifically recommended to actively involve the family in providing oral care, such as cleaning and lubricating the mouth and lips. It was mentioned that this can provide the family with a sense of usefulness and an active role in comforting their loved one.71,93,98 However, as some might find it too distressing or difficult, one guideline warned to not force the family to be involved in mouth care. 89
Discussion
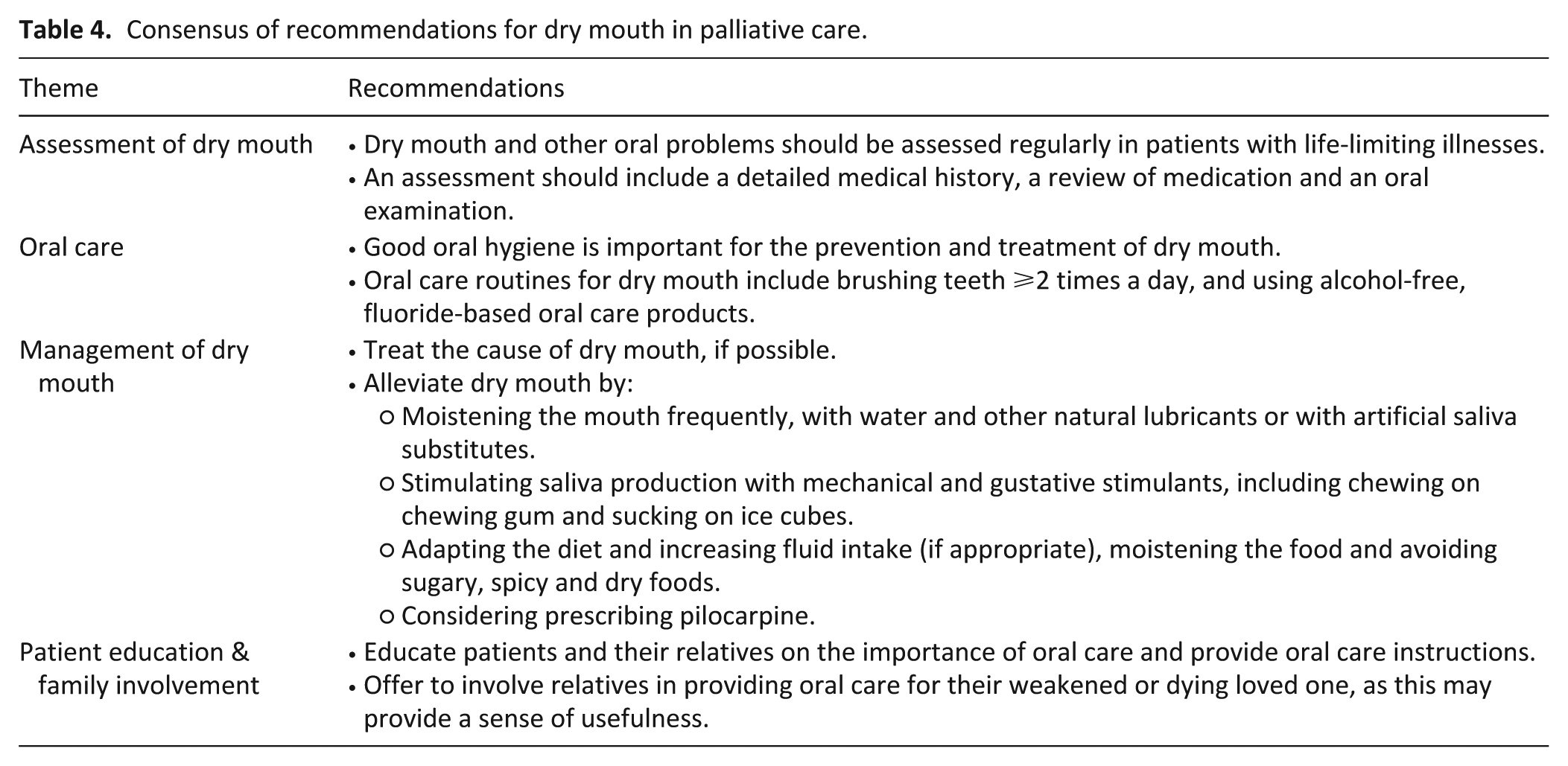
This systematic review analysed the quality and content of clinical practice guidelines for dry mouth in palliative care. 72 guidelines across 42 countries were identified. Comprehensiveness of dry mouth specific recommendations was limited, with only 12 guidelines having a major focus on dry mouth. Methodological quality of the clinical practice guidelines was low to moderate, and the evidence base underlying the recommendations was limited. However, recommendations were largely consistent for the four main themes of dry mouth care practices: the assessment of dry mouth, the importance of oral care, the management of dry mouth, and patient education and family involvement (see Table 4).
Consensus of recommendations for dry mouth in palliative care.
Our review shows a lack of robust clinical guidance for dry mouth in palliative care, with only two guidelines being ‘recommended for use’ based on current quality.51,52 The AGREE II domains Rigour of Development and Applicability scored particularly poorly, largely due to a lack of information on search strategy and evidence grading, and of implementation strategies. Contributing factors for low quality of the clinical practice guidelines include a scarcity of scientific evidence in dry mouth and palliative care research,30–32 and palliative care being a relatively new and evolving practice, with limited funding in certain geographic regions.38,44–47 Interestingly, methodological quality did not seem to influence content or clinical validity of recommendations across clinical practice guidelines. For example, clinical practice guidelines with higher and lower methodological quality (e.g. Netherlands 52 and Germany 51 vs France 84 and Cameroon, 64 respectively) all provided consistent and appropriate recommendations for dry mouth care, such as similar oral care instructions and saliva substitutes and stimulants. This is in line with previous research suggesting that the methodological quality of clinical practice guidelines is not directly associated with the content or the clinical validity of the recommendations.35,123,124
Consistency of recommendations also applied across country and economic status, with few guidelines addressing local practices or adapting recommendations to the specific context. For example, some guidelines recommended medication unavailable within their region (e.g. cevimeline is unavailable in Europe)102,125 and most did not provide information on the cost of different treatment options (e.g. artificial saliva products or dental care are uncompensated care in many countries). While it is encouraging that most guidelines share similar best practices, the uptake of clinical practice guidelines could be improved by adapting recommendations to the local context. 126
Few guidelines gave instructions for clinicians to conduct a structured assessment of dry mouth through anamnesis or oral examination. Guidelines lacked detail on the frequency of assessment, advice on which questions to ask, and consensus on assessment instruments. Assessment is a critical step for adequate recognition and treatment of dry mouth,15,127 acting early to manage symptoms when they develop, acknowledging the severity of symptoms and being aware of potential contributing factors. Given that many healthcare professionals lack confidence in conducting these assessments,25,26 this is a key area where implementation of guidelines into the education of clinicians has potential to increase awareness and help the management of dry mouth.
There was a lack of clear consensus for pharmaceutical interventions for dry mouth in palliative care, in particular for the use of pilocarpine. This included different recommendations on the use of pilocarpine in specific patient groups (i.e. only for radiotherapy-induced or all cases of dry mouth), on dosage and form. These inconsistencies likely stem from a lack of high-quality scientific evidence for pharmacological interventions for dry mouth in palliative care, including pilocarpine.31,32 To illustrate this, a recent scoping review of Kakei et al. (2024) revealed only two intervention trials in the palliative care setting. 31 Both trials showed limited effectiveness with moderate to severe side effects. Latest pilocarpine research has focussed on feasibility trials with topical forms of pilocarpine to retain the effectiveness but limit the side effects.128–130 Building this evidence base for the effectiveness and recommended use of pilocarpine should continue to be a priority in palliative care research.
It was notable that little emphasis was placed in the guidelines on managing the psychosocial distress induced by dry mouth. Only eight guidelines mention prompts about quality of life during assessment of dry mouth69,81,86,89,90,94,99,117 and one guideline as part of patient education. 88 This is not surprising as both patients and health care professionals have previously reported a lack in acknowledgement of the dry mouth symptom itself as well as the negative impact on quality of life by dry mouth.19,26 However, dry mouth can severely interfere with speaking, eating, intimacy and sleeping 20 – arguably activities that are specifically important for patients and their loved ones in the palliative care setting. By not addressing dry mouth and its physical and psychosocial consequences, health care professionals may unknowingly contribute to its high symptom burden. By incorporating all dimensions of palliative care (physical, psychological, social and spiritual) 38 in guidelines for dry mouth, it may increase the perceived importance of addressing dry mouth in all its facets.
Strengths and limitations
A key strength of this systematic review is the comprehensive search strategy, which combined conventional search methods in scientific databases with grey literature searches and a stakeholder outreach campaign to enhance scope and inclusivity of findings. 40 With a broad definition of clinical practice guidelines, no restrictions on type of life-limiting illness, and no language restriction, the review achieved extensive geographic representation, covering six continents, and ensuring greater inclusion of low- and middle-income countries.
Despite this, the review cannot be seen as exhaustive as some clinical practice guidelines may still not have been identified due to accessibility barriers, a country’s use of local resources rather than national guidelines or missing newly published guidelines. In addition, the extent to which the identified clinical practice guidelines are implemented in practice remains unknown. While efforts were made to verify the use of clinical practice guidelines with palliative care stakeholders, confirmation was not possible for all guidelines (see Supplemental File 3). Finally, the absence of restrictions on illness type may limit the specificity of recommendations for some patient groups, as the aetiology and contributing factors of dry mouth vary across patient populations.
Implications for future research & clinical practice
This review demonstrated that most guideline recommendations for dry mouth care in palliative care are based on expert opinion or low-grade scientific evidence. This is in line with previous systematic reviews on interventions for dry mouth.31,32 Future research should therefore focus on evaluating current and new dry mouth care practices within the palliative care setting in robust clinical trials. Future research priorities should include comparing effectivity and acceptability between different saliva substitutes and stimulants, and researching optimal pharmacological treatment options (including pilocarpine and bethanechol). These studies should also assess the impact on dry mouth induced psychosocial distress.
This review highlights the need for guidelines that provide clear and specific recommendations addressing all relevant components of dry mouth assessment and management in palliative care. Improving clarity of recommendations is specifically important, as the lack of clear guidelines has been mentioned previously by health care professionals as an important barrier for the treatment of oral health problems in palliative care.23,26 Clear and easy-to-follow instructions have been marked as an important attribute for the uptake of guidelines by healthcare professionals. 131 Future guidelines should therefore include detailed instructions for the assessment, treatment and monitoring of dry mouth, such as when and how to use a particular treatment or how and how often to assess dry mouth. As goals of care and priorities for dry mouth management may differ across palliative care phases, including the disease-modifying, symptom-directed and terminal phase, guidelines should also consider phase-specific recommendations. 132 In addition, they should address the (psychosocial) impact on quality of life of patients.18,22 Most importantly, future efforts should prioritise the effective implementation of existing and new guidelines. This requires practical, user-friendly strategies, such as concise summaries and digital decision-support tools, and recommendations that are adapted to cultural and socio-economic contexts and to the specific characteristics of patient populations.
Conclusion
This systematic review analysed the quality and content of clinical practice guidelines for dry mouth in palliative care. The review found that the comprehensiveness of dry mouth recommendations was limited, the methodological quality of the clinical practice guidelines was low to moderate, and the evidence base underlying the recommendations was lacking. Despite this, many care practices appear to be shared worldwide, including oral care, saliva substitutes and stimulants, dietary advice and the use of pilocarpine. This review highlights the need for higher quality, easy-to-use guidelines that comprehensively focus on dry mouth in palliative care, and are effectively implemented in practice. Underpinning these guidelines is the need for future research evaluating treatment interventions specifically within the palliative care setting. These steps can make important contributions towards improving the quality of care for people with life-limiting illnesses suffering from dry mouth.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163261434188 – Supplemental material for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world
Supplemental material, sj-docx-1-pmj-10.1177_02692163261434188 for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world by A. I. van der Meulen, A. Stoppelenburg, M. Theunissen, E. J. M. de Nijs, M. H. J. van den Beuken-van Everdingen and Y. M. van der Linden in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163261434188 – Supplemental material for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world
Supplemental material, sj-docx-2-pmj-10.1177_02692163261434188 for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world by A. I. van der Meulen, A. Stoppelenburg, M. Theunissen, E. J. M. de Nijs, M. H. J. van den Beuken-van Everdingen and Y. M. van der Linden in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_02692163261434188 – Supplemental material for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world
Supplemental material, sj-docx-3-pmj-10.1177_02692163261434188 for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world by A. I. van der Meulen, A. Stoppelenburg, M. Theunissen, E. J. M. de Nijs, M. H. J. van den Beuken-van Everdingen and Y. M. van der Linden in Palliative Medicine
Supplemental Material
sj-docx-4-pmj-10.1177_02692163261434188 – Supplemental material for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world
Supplemental material, sj-docx-4-pmj-10.1177_02692163261434188 for Dry mouth in palliative care: A systematic review of clinical practice guidelines around the world by A. I. van der Meulen, A. Stoppelenburg, M. Theunissen, E. J. M. de Nijs, M. H. J. van den Beuken-van Everdingen and Y. M. van der Linden in Palliative Medicine
Footnotes
Acknowledgements
We thank the contacted stakeholders for their time and valuable input on local guidelines, and the medical information specialist Elmira van Galen (Walaeus Library, Leiden) for her help with the initial search strategy.
ORCID iDs
Author contributions
Both A.M. and A.S. were involved in the design of the study, the screening of articles and the quality analysis. Content analysis was performed by A.M. A.M. also drafted the manuscript of this paper, receiving feedback from all other authors (Y.L., M.B., A.S., M.T., E.N.).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review is part of a larger research project, financed by the Dutch organisation ZorgOnderzoek Nederland Medische Wetenschappen (ZonMw; grant number: NL08440012010001). This funding source had no role in the design, execution or analyses of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data (including the code book, content analysis data, list of contacted stakeholders) is available upon reasonable request to the corresponding author.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.