
Abstract
Background:
Malignant bowel obstruction is a life-threatening condition associated with advanced cancer that causes severe pain, nausea and vomiting. Decision-making requires input from multiple specialities, outcomes are uncertain and clinical communication is challenging. Better understanding of the mechanics of shared decision-making would improve the management of this condition.
Aims:
To investigate behavioural and structural influences on decisional deliberation during the management of malignant bowel obstruction and develop strategies for improved communication.
Design:
A realist review following RAMESES guidelines; protocol registered in PROSPERO (CRD42022308251).
Data sources:
Iterative literature searches were conducted from December 2021 to January 2023, with an update search conducted in January 2024. All relevant data sources relating to shared decision-making in the management of malignant bowel obstruction were included.
Results:
Seventy-one papers were included. Realist synthesis led to the development of context-mechanism-outcome configurations in four conceptual areas to explain influences on practitioner, patient and caregiver engagement in shared decision-making: (1) implicit misunderstandings, (2) the nature of the decision, (3) interpersonal dynamics and (4) a fragmented ethos of care. Implicit social mechanisms can affect the transparency of shared decision-making and the value individual decision-makers assign to the process, and motivation to participate is likely to vary as circumstances change.
Conclusions:
Communication around patients with advanced cancer and malignant bowel obstruction is characterised by ambiguity, unrealistic expectations and a lack of interdisciplinary coordination. Crucial features of effective decisional deliberations include alignment of goals of care, unambiguous explanation of treatment limitations and iterative communication to facilitate the formation of realistic expectations.
Keywords
Malignant bowel obstruction causes severe symptoms, and most people die within months unless there is a localised, operable tumour.
Decision-making requires input from many different specialities, outcomes are uncertain and communication and decision-making can be challenging for people with bowel obstruction, their families, and the practitioners involved in their care.
A framework informed by evidence and theory that explains how implicit influences affect the transparency and perceived value of shared decision-making in the management of malignant bowel obstruction in advanced cancer.
Practitioner-focused strategies to improve complex, high-stakes shared decision-making in advanced disease.
Palliative care teams can play a lead role in helping patients with malignant bowel obstruction to engage in shared decision-making by encouraging unified, consistent and timely interdisciplinary communication.
Transparent, ‘non-binding’ communication about all treatment options (including palliative care) is vital to inform shared decision-making and increase patients’ sense of control and motivation to engage.
Incremental and iterative involvement of patients, supported by active validation of their values, goals and family circumstances, will enable them to adapt as their circumstances change.
Background
About one in six people with cancer experience bowel obstruction. 1 It causes severe, sometimes intractable vomiting, 2 with pain and nausea, and can have a poor prognosis. Management options include systemic anticancer treatment, surgery or stenting and symptom control using medication, intestinal drainage or palliative surgery. Individualised decision-making is essential. While surgery offers an option for long-term survival in people with localised, curable cancer, there are currently no nationally or internationally agreed treatment guidelines for non-curative treatment. 3 People with malignant bowel obstruction feel burdened and distressed by the uncertainties surrounding treatment decisions, and this is aggravated by conflicting clinical advice 4 and a focus on quantity, rather than quality, of life. 5
The challenge of shared decision-making
Shared decision-making is defined as a process that supports people to (a) understand their treatment and support options, and the associated risks, benefits and consequences and (b) make a decision about a preferred course of action, based on clinical evidence and personal preferences. 6 Shared decision-making is recognised as a moral principle underpinning person-centred care and can increase quality of life7,8 and satisfaction with care, 9 but can be challenging in practice. 10
The original focus of shared decision-making theories on dyadic interaction have shifted to consider an interprofessional standpoint more reflective of complex care.11,12 However, while the stepwise components of shared decision-making have been described, we still know little about the deliberations that happen between people during the shared decision-making process 13 and how these are influenced by agentic and structural contexts. In this review we explore the implicit mechanisms that enable or constrain shared decision-making during the management of malignant bowel obstruction.
The review (PROSPERO registration: CRD42022308251) comprised Phase 1 of a three-phase research study. 14 Its aims were to:
use a broad range of evidence to theorise how the intention to share treatment decisions works during the management of malignant bowel obstruction;
hypothesise causal processes (contexts, mechanisms and outcomes) that influence the intention to engage in shared decision-making, and how this varies in different circumstances;
develop a theoretically informed framework to explain how shared decision-making might work best in the management of malignant bowel obstruction.
Methods
Realist methods acknowledge the influence of human behaviour and cognition on how we practice health care in the ‘real’ world. Pawson et al.’s realist review methodology 15 is well-placed to develop our understanding of the mechanisms of shared decision-making and how they change in relation to the contexts in which decision-making plays out – ‘context’ referring to the places, people and material circumstances that encourage or inhibit this process. 16 We developed and refined programme theory in four stages (below), as outlined by McEwan et al. 17
Stage 1: Brainstorming – formulating initial explanatory frameworks
The initial theory gleaning phase drew on brainstorming for ‘tacit theories’ 18 in a series of research team meetings (clinicians, clinical academics, and applied health researchers). Four initial explanatory frameworks were developed: decision-making in uncertain circumstances, multidisciplinary dynamics, the circumstances of sharing unique to bowel obstruction and the variability of connected resources (see Supplemental File 1). We developed multiple explanatory theories to enable us to explore the complex interactions between decisional contexts characteristic of malignant bowel obstruction. In parallel, stakeholder consultation with clinicians and people with experience of bowel obstruction was conducted online through sharing a lay-language summary of the explanatory frameworks, created with a Patient and Public Involvement (PPI) representative with caregiver experience. The online form was widely distributed through the team’s clinical networks, patient representatives, charities and clinical organisations connected with cancer care, nursing, palliative care and dietetics via professional networks and social media. Stakeholders responded anonymously, and were asked only to state their role. Filling in the online form was taken as consent to participate.
Nineteen stakeholders responded with comments (11 clinicians, 5 patients, 3 caregivers). Comments were coded into themes, and the thematic concepts were integrated into the explanatory frameworks without using direct quotations. NVivo™ was used to manage the data. The frameworks were revised into three working initial programme theories explaining the potential social and structural influences on shared decision-making in the management of malignant bowel obstruction, to be taken forward for refinement using sources of evidence located during the review: Theory 1 Decision-making in the grey area: dealing with ambiguity and uncertainty; Theory 2 Relationship dynamics: doctor/patient challenges; Theory 3 Role dynamics: the challenges of disciplinary variability (see Supplemental File 1).
Stage 2: The literature review – testing the explanatory framework
Literature searching was conducted by an information specialist (SG). Guidance for initial search concepts was drawn from team members’ recent published reviews on related topics3,5: draft strategies were tested against known relevant reference sets retrieved during these reviews. Searches took place from December 2021 to January 2023, and were updated in January 2024.
Search strategies
Four searches were performed (search strategies available on request; see Supplemental File 2 for an example). The design of each search was iteratively informed by ongoing data extraction and analysis to address gaps in the evidence relating to the initial programme theories. As searching progressed, MeSH terms were reviewed and refined using PubMed PubReminer. No limitations were imposed in relation to study design, language or date. Articles were included where they offered data focused on: (1) aspects of clinician and patient/family decision-making in malignant bowel obstruction and (2) concepts related to oncological and palliative decision-making aligned with the initial programme theories that offered further depth for theory refinement.
Search 1 was designed to retrieve academic papers and grey literature related to the management of or experiences of people with malignant bowel obstruction that referred to decisions or the decision-making process. Search 2 retrieved literature focused on advanced cancer that referred to shared decision-making, and oncological and palliative decision-making frameworks relevant to the management of malignant bowel obstruction. Search 3, which also included a Twitter search for posts related to malignant bowel obstruction conducted via the Mozdeh interface, 19 was designed to identify experiences of people with malignant bowel obstruction and related treatments. Search 4 identified theories and models of interdisciplinary shared decision-making.
Screening was conducted in Covidence by AB, with 10% of retrieved records and full texts double-screened by MPa. Included studies were appraised using Wallace et al.’s 20 criteria for evaluating multiple study designs, enabling consideration of the strengths and weaknesses of different aspects of studies rather than an overall assessment of quality.
The flow of studies through the review is shown in Figure 1. Using a data extraction form, statements from included papers were matched against the global areas and subthemes of the initial programme theories.
Flow of studies through the review.
Stage 3: Development of causal statements
Causal statements were developed by moving back and forth between the explanatory frameworks and data extracted from the literature, considering how shared decision-making had been achieved or not. Initial attempts to distinguish between contexts, mechanisms and outcomes to create causal statements felt ‘messy’,18,21 reflecting the subjectivities of shared decision-making in its conception as an intervention and/or an ethos and the qualitative, interpretive nature of the analytic process (see Supplemental File 1 for an example of configurational analysis).
Stage 4: Application of substantive theory
During configurational analysis, contexts and mechanisms were often difficult to separate, and outcomes drawn from the literature were not uniformly defined in relation to shared decision-making. Before developing final propositions, we turned to substantive theory for conceptual clarification. We considered models of collaborative decision-making (Bekker’s Making Informed Decisions Individually and Together framework 22 and the Interprofessional Shared Decision-Making model11,12) and the broad behavioural concepts of Waldron et al.’s 23 theory of shared decision-making. We also considered four behavioural theories: the Theory of Planned Behaviour, 24 Prospect Theory 25 (decision under circumstances of risk) in application to palliative care decision-making, 26 Self-Determination Theory, 27 and the COM-B. 28 We found that Self-Determination Theory’s focus on relatedness, competence and autonomy resonated with the decision-making data and offered a broad range of relatable ‘regulatory processes’ (theoretical causal mechanisms) that could be mapped along a continuum of motivation, explaining fluctuations in personal autonomy and the intention to engage in shared decision-making over time (see Supplemental File 1). These concepts were applied to our messy causal statements to refine boundaries between contexts, mechanisms and outcomes and to re-shape outcome terminology to increase the focus of initial programme theories on motivation to engage in shared decision-making (see Supplemental File 1). Propositional maps (a set of categorised and summarised context-mechanism-outcome chains) were developed for each context.
Results
Characteristics of the 71 included articles are shown in Table 1. Definitions of context, mechanism and outcome in relation to the review strategy are given in Table 2. The final programme theory proposes four key characteristics of shared decision-making in the management of malignant bowel obstruction that influence its effectiveness: (1) implicit misunderstandings, (2) the nature of the decision, (3) interpersonal dynamics and (4) a fragmented ethos of care.
Characteristics of included articles.
Definitions of context, mechanism and outcome.
Associated context-mechanism-outcome statements (CMOs) are shown in Figure 2, illustrating the contexts of malignant bowel obstruction that shape decision-making behaviour, and the mechanisms (implicit social processes/behaviours) linked with specific outcomes in shared decision-making (SDM). The influence of these components is summarised below, exploring their implications for the outcomes of shared decision-making.
Theory propositions map showing the contexts of malignant bowel obstruction that shape decision-making behaviour, and the implicit social processes and behaviours linked with shared decision-making (SDM) outcomes.
Component 1: How implicit misunderstandings can affect shared decision-making
Implicit misunderstandings can arise from clinicians’ motivation to ease patients’ feelings of overwhelm, the use of ambiguous language to frame clinical uncertainties and facilitate adaptation and the challenge of balancing hope with realistic expectations of treatment.
Blindsiding and overwhelm: People with bowel obstruction may experience a ‘false’ sense of shared decision-making when the implications of treatment are deliberately left implicit to avoid distress. Key papers describe ‘communication misadventures’ 35 during shared decision-making – hidden misunderstandings between patients and clinicians that lead to a false sense of choosing in partnership, and a consequent misalignment in expectations of treatment.34,35,49,52,53,60,77,83,84,86,95 Where sufficient information is provided to make a decision, people with bowel obstruction and their families may feel overwhelmed or blindsided, 13 lack a sense of control, 90 struggle to reconcile their situation with their everyday world and resist a realistic understanding of their situation.39,73
Ambiguity and uncertainty: The trajectory and implications of malignant bowel obstruction are often unclear to people when diagnosed.34,48 Clinicians experience uncertainty around treatment choices, as potential outcomes can be ambiguous. 56 Outcomes valued by individual patients are not always well explored.37,39,56 Where more than one reasonable path of action exists, the effects of uncertainty can be magnified.34,48,54 Discussion of potential good outcomes can make uncertainty easier to tolerate. 92 Honesty about prognosis may need to unfold incrementally to allow adaptation,89,91 but an acknowledgement of uncertainty may increase a personal sense of control. 91
Unrealistic expectations: People with bowel obstruction often do not feel sufficiently well informed to contribute to decision-making.21,34,40,48,95 When definitive answers about treatment are not forthcoming, they can feel abandoned.34,92 Murphy et al. 95 questions ‘the degree to which patients are serving as active partners in SDM’(p6): patients with an obstruction often underappreciate the risks of treatment 95 and form unrealistic expectations,60,63,74,92,93,95,97 and it can be challenging to maintain a realistic outlook.14 –17,62,97 People can hold mutually exclusive goals, and clinicians may ‘sugarcoat’ treatment to avoid patients feeling abandoned.13,19,49,76,82 The maintenance of hope as grounds for surgery, in particular, may not be in the best interests of the individual. 19 Some people hold on to hope in a way that inhibits realistic goals of care,21,70 others can recalibrate their expectations, 40 but clinicians can be reluctant to pursue these conversations.23,61,65 Treatments that most often lead to unexpected outcomes are surgery and parenteral nutrition. Some patients expect non-curative surgery to ‘fix’ the obstruction. 61 If practitioners do not clearly describe how parenteral nutrition works, patients can find this intervention more invasive than anticipated.40,94 Painting a picture 98 of multiple potential outcomes is imperative to enable successful engagement in shared decision-making3,27,60,87,98
Component 2: How the nature of the decision can affect shared decision-making
Intentions to share decisions can be affected by perceptions of a lack of choice, the unpredictability of decisional outcomes and iterative revisiting of decisions and the failure to acknowledge or prepare for potential tipping points when stopping treatment may increase remaining quality of life.
Do or die – having no choice: Decisions with surgeons about the operability of a bowel obstruction were perceived by people with bowel obstruction as a life-or-death option,3,76,85 and for some, involvement of palliative care suggested there was ‘no way out’ of their situation.90,92 They did not construe these situations as offering ‘choice’. Accepting parenteral nutrition (liquid nutrition delivered directly into a vein) when eating is not possible was also perceived as a ‘life-or-death’ decision,38,59,85,94 or an unviable decision because an individual might be unlikely to survive long enough to benefit from it. 38 Fast-paced decision-making was also construed as a ‘no-choice’ situation. 96 In no-choice situations, acceptance of treatment does not necessarily imply that a treatment decision is shared. Talking through acceptable variations or nuances in treatment can give people a sense of choice, 81 and the direct involvement of palliative care can be the most effective way to destigmatise palliative language.90,92
Decision spirals – the art of iterative decision-making: While do-or-die decisions are discrete, most treatment decisions are complex and evolving, and developing a shared understanding is an ‘artful’ process. 35 A combination of recurrent symptoms and uncertain outcomes make decision-making iterative rather than linear: the same decisions are revisited and made anew at different points.13,33,36,50,52,54,91,98 If a person with incurable malignant bowel obstruction resists discussion of their prognosis, fully informed shared decision-making might evolve over multiple consultations. 78 If past treatment choices have not led to improvements, they can lose investment in sharing decisions. 80 Limiting the number of clinicians involved in these conversations can encourage clearer, more unified advice. 59
Tipping points – identifying treatment boundaries: Iterative decisions can reach tipping points where standard therapies (e.g. chemotherapy) are not improving someone’s condition, and a change of care setting is appropriate. 30 The effective management of people’s hopes includes identifying points when the risks of treatment may outweigh the benefits, 30 preparing people for these moments in advance, 88 or adapting to their needs by temporarily reverting to iterative decision communication and encouraging exploration of their psychosocial needs. 76 An inability to tolerate distress during tipping point communication can present a barrier to shared decision-making. 91 Clinicians sometimes fail to acknowledge tipping points, even when people with bowel obstruction sense them, 89 or resist transfer to palliative approaches by mistakenly perceiving potentially beneficial therapy as incompatible with end-of-life care. 52
Component 3: How interpersonal dynamics can affect shared decision-making
Pre-existing relationship dynamics can sometimes delay understanding of the significant change in health circumstances and complexify shared decision-making: at the point of diagnosis, close doctor-patient relationships can inhibit the timely involvement of other specialities, in particular palliative care teams; throughout treatment, pre-existing dynamics within families can influence the direction of patients’ decisions.
Pre-existing relationships: Most patients with malignant bowel obstruction have undergone active treatment for diagnosed cancer and have a pre-existing relationship with an oncologist. 50 Pre-existing relationships give a sense of safety because patients feel known, 90 which is crucial to motivation to engage in decision-making. 96 Positive qualities of long-term relationships, such as trust and hope, encourage reciprocity.34,50,66,72,76 While reciprocity is often a positive aspect of interaction, it can inhibit honest communication 95 and lead to a lack of neutrality on the part of clinicians 95 and increased distress when sharing decisions around goals of care. 34 Metaphors around treatment established in pre-existing relationships run the risk of stalling shared decision-making if neither party wishes to admit that a previous analogy has become inappropriate. 32 For example, if cancer has been construed as a battle, clinicians may fear ‘therapeutic impotence’. 29 Handing over decision-making to another clinician can be difficult for both parties. Concurrent care assists transition but can be hard to operationalise across disciplinary settings. 50 Where pre-existing rapport is missing (e.g. where there is no prior cancer diagnosis), eliciting goals of care and communicating potential outcomes is more difficult, especially in the absence of good interdisciplinary networking. 31 Early palliative care involvement for symptom relief can build relationships which make later decisions to refer easier.45,55,56,69
Power differentials: Where personal values and psychosocial issues are inadmissible in a treatment communication, whether the person with an obstruction is present or not, they may sense that they do not have a role in decision-making and defer or delegate decisions.3,13,39,56,65,75,85 Making people feel ‘known beyond their disease’ encourages motivation to engage with treatment decisions, 96 and enabling them to ‘opt out’ of decisions can reduce burden. 75 Relationships with families (or the absence of these) can facilitate or inhibit the acknowledgement of individual values and goals. Pressure from family members to eat or drink as a sign of wellness, or to take part in normative social routines, 40 can emerge from a fear of death from starvation (this can be unacceptable on an individual or cultural level) and parenteral nutrition may seem imperative.68,97
Nurses provide a critical role in explaining treatments and supporting shared decision-making,36,42,57 and are often well placed to advocate or encourage active involvement.57,90 Advocacy validates the individual, and the conscious involvement of families, where appropriate, can increase people’s sense of control.57,68,96 If goals of care are not discussed and a person loses capacity, families can find it difficult to resolve conflict between available treatments and the person’s last known wishes. Proactive planning with surrogate decision-makers can alleviate difficulties37,46,71,90 but can also compound them where there is no clear understanding of likely outcomes. 47
Component 4: How a fragmented ethos of care can affect shared decision-making
In multidisciplinary teams, the act of sharing decisions is complexified by fragmented clinical aims and objectives, the physical separation of teams, and a lack of familiarity with palliative and nutritional approaches to bowel obstruction management. From the patient’s perspective, discontinuity in decision-making can increase uncertainty and lead to a lack of motivation to engage.
Role fragmentation: A breadth of expertise is required to manage bowel obstruction, with decision-making spread across multiple locations – often the person with bowel obstruction is not present during decision-making,58,74,84,85 and experiences care as fragmented and discontinuous.29,38,43,92 Each clinical discipline has its own ethos of care; these do not always intersect, and role perceptions about ownership of decisions can lead to disjointed aims.34,59 For example, alignment of treatment decisions with personal goals of care is not part of the ‘rescue-oriented’,37,41 ‘fix-it’ culture 61 of surgery, where advance care planning is often poorly addressed.37,61 Decisions made with surgeons can be perceived as less flexible and less easy to ‘own’ than decisions made with oncologists. 64
Where terminology around treatment and goals of care are defined differently, people with bowel obstruction experience confusion.60,74,83,84 Shared decision-making is at its most effective when a harmonious ethos of care is deliberately ‘orchestrated’, 82 but there is currently a lack of consensus around what constitutes good interdisciplinary care in malignant bowel obstruction. 77 The ethos of holism common to palliative care can facilitate a positive paradigm shift, 56 but clinicians can be reluctant to refer.31,43 Early contact with palliative care can enable relationship-building that becomes invaluable later in the care trajectory.55,56 It can also help avoid aggressive treatment that compromises quality of life and causes chaotic experiences of death and dying.45,67 Palliative care teams have expertise in managing severe distress 72 and exploring values and goals,35,37,43,49 enabling articulation of realistic hope. 29 They can also act as a ‘sounding board’ in multidisciplinary discussions. 40
Structural fragmentation: The way that clinical communication between key decision-makers is configured and maintained influences the effectiveness of decision-making. 31 Collaboration is increased by the physical proximity of different disciplines.35,36,75 Where decision-making is partially conducted ‘outside the room’ 74 in corridor conversations, key decision-makers may be missing.84,85 Institutional norms around communication can also influence practitioners’ comfort with honesty around potentially poor outcomes. 91 Decisional choices can be restricted by clinicians’ perceptions of some interventions as subsidiary – in particular, nutritional and palliative approaches to bowel obstruction.38,51,59 Deliberate networking between oncology, surgery, radiology, palliative care, nutrition teams and related nurse specialists around individual patients can ensure consideration of all appropriate interventions, continuity of care and unified communication.33,34,39,44,75,82 With the patient as the central point of contact, the successful consolidation of different disciplinary opinions can remove complexity at the point of liaison34,39 – for example, a single practitioner can summarise multidisciplinary perspectives into a unified message.33,36,44,75,77 Where unified communication is missing, people do not feel ‘known’, and are less likely to engage in decision-making. 96
Implications for shared decision-making
The findings of this review suggest wider implications for shared decision-making with people who are seriously unwell with cancer and face high stakes decisions. Outcomes shown in Figure 2 suggest that across all contexts, shared decision-making can occur on ‘false terms’. The value of shared decision-making can be perceived differently by people in different roles and across different contexts, and the motivation to engage can fluctuate based on people’s sense of control, feelings of decisional competence and the behaviour of other decision-makers. People faced with severe health problems associated with high stakes decision-making do not always feel sufficiently informed, motivated or competent to share decisions. Incremental involvement can be an effective approach to enable adaptation to a sudden change in health circumstances, but where people are willing to engage with practitioners in decision-making, this can be inhibited by the social dynamics of decisional deliberations. Figure 3 summarises the implications for transparency, perceived value and motivation to engage and suggests related strategies for change.
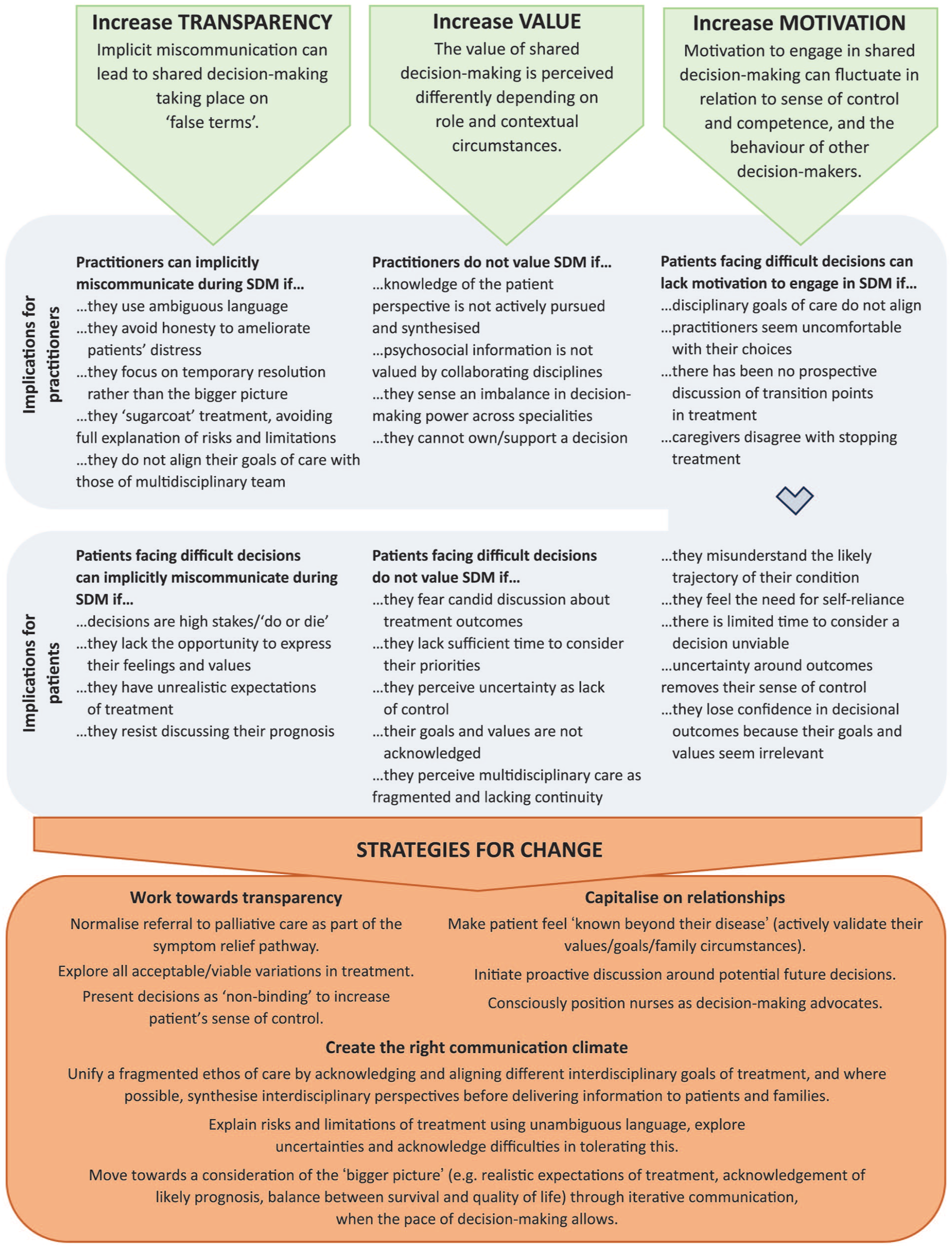
Implications for shared decision-making: influences on transparency, value and motivation to engage and actionable strategies to improve these qualities during decisional interactions.
Discussion
The unique circumstances posed by malignant bowel obstruction bring complexities, such as overwhelming symptoms, an immediate threat to life, high-stakes fast-paced decisions, poor disciplinary goal concordance and a strong investment in survival where people have pre-existing relationships with oncology (often at the cost of quality of life). There is an imperative to reconceptualise fragmented disciplinary expertise into a unified approach for the benefit of people diagnosed with malignant bowel obstruction. In exploring the mechanics of shared decision-making, we highlight the influence of interpersonal and interdisciplinary dynamics and the nature or shape of decision-making associated with this condition. We also demonstrate that the value of shared decision-making and the motivation to engage can vary depending on social dynamics and the timing of decisions, and that decision-makers do not always engage with transparency, even when they may intend to do so and can engage in the process on false terms.
Models of interdisciplinary shared decision-making have been slow to evolve, and are conceptualised around a stepwise process of information provision, incorporation of personal values, guided evaluation and clarification, implementation and outcomes.12,99 –101 While decision-makers’ roles are identified, and the shared decision-making process is acknowledged to flex and change across contexts, what has remained unexplored are the mechanisms of deliberations that coalesce (or inhibit the coalescence of) decision-makers’ understanding. These are represented in Légaré et al.’s interdisciplinary shared decision-making model (IP-SDM) 12 by empty boxes at the axes where roles align with decisional steps. While we recognise broad mechanisms that shape the behaviours of health care professionals, patients and families in shared decision-making, 23 it is crucial that we drill down further, exploring how key contexts affect decisional deliberation and its outcomes. In this way, we can gain a more transparent understanding of the influences at play in relation to specific health conditions and/or their associated organisational settings.
Existing evidence has demonstrated that setting, attitude and tone influence shared decision-making. 102 Decision-makers need to be ‘on the same page’, and the checking of shared meaning is vital to combat implicit and invisible miscommunication. For individual clinicians, aligning with a person’s needs for balancing hope and honesty are critical, and can impact heavily on psychosocial outcomes.102,103 For multidisciplinary teams managing the complexities of malignant bowel obstruction, aligning goals of care prior to discussing treatment options can clarify anticipated outcomes. In cancer, people’s needs and goals evolve over the course of their treatment trajectory. 104 Interpersonal dynamics are made complex by variable treatment needs and psychological responses to a life-threatening situation. Personal preferences for autonomy vary101,105 –107 – some need information to be withheld to cope with their situation, and for clinicians, this can sometimes erode trust. 108 Personal characteristics and preferences for engaging in decision-making or taking the lead vary, not only between individuals, but across time104,109; this variability is not always incorporated into generic decision aids. 110 A greater understanding the mechanisms of deliberation will increase decision-makers’ ability to adapt to one another’s needs.
For people with malignant bowel obstruction, the motivation to engage in decisions if influenced not only by uncertainties around treatment outcomes, but also by how interdisciplinary care is happening around them, ambiguity around clinicians’ roles and uncertainties around treatment outcomes. The effects of busy secondary care environments on shared decision-making are not always positive. 10 This is set against a backdrop of feeling overwhelmed by physical symptoms, reflecting the practical and existential concerns encapsulated in the concept of ‘total uncertainty’. 111 A more nuanced understanding of the challenges in shared decision-making requires a deeper exploration of the implicit mechanisms of deliberation in decision-making models, and an understanding of how these mechanisms are affected by specific contexts around and within the management of complex conditions.
Implications for practice
People with bowel obstruction need to be supported to maximise the time they have to adapt after the shock of diagnosis, often in the context of a rapidly deteriorating condition. Health care practitioners are best placed to create the right communication climate for these patients, ensuring transparency by understanding and avoiding the potential for miscommunication. Increasing patient and family investment in shared decision-making, and their sense of control and motivation to participate, can emerge from a conscious effort to make them feel known and by acknowledging and actively combatting the fragmented and discontinuous nature of multidisciplinary communication around this complex condition with protocols for unified, collaborative management. People with bowel obstruction are more likely to engage in shared decision-making over time in settings where care feels relational, goals of care feel unified across clinical specialities and communication feels consistent.
Strengths and limitations
This review draws on a wide range of evidence, including oncological, surgical, nutritional, palliative and patient/family perspectives on shared decision-making in malignant bowel obstruction. It synthesises perspectives around high-stakes shared decision-making in complex conditions in a way that might offer transferability to other areas of complex care for people with advanced cancer, in particular in conditions which benefit from the involvement of palliative expertise. Data retrieval and selection involved an information specialist with experience of realist reviews; iterative discussion among a research team with clinical expertise contributed to programme theory development, and a Patient and Public representative helped to shape stakeholder consultation. Stakeholder involvement of clinicians and people-with-lived-experience provided rigorous foundations for developing explanatory frameworks and exploring their resonance with current day-to-day health care practice.
Limitations included a focus in the included papers on role-specific clinical perspectives; collaborative interdisciplinary perspectives were lacking. Few papers specifically explored ways of operationalising shared decision-making. We lack evidence of first-hand personal experiences of malignant bowel obstruction, likely due to severe symptoms and short prognosis. Experiential knowledge of this condition – in particular patient and caregiver perspectives on sudden high stakes decision-making – is vital to our understanding of decisional deliberations, in particular when advanced cancer increases uncertainties around treatment outcomes. Research design can address this gaps by extending recruitment periods to allow more patients and caregivers the opportunity to participate in research, and by considering joined-up site recruitment to capture potential participants as they are discharged from hospitals into hospices.
Conclusion
In situations of clinical uncertainty combined with fast-paced, high stakes decisions, shared decision-making is not straightforward. Treatment for malignant bowel obstruction is characterised by ambiguity, unrealistic expectations of treatment and a lack of interdisciplinary coordination. Where the condition crosses a threshold into incurability, clinicians require advanced skills in prognostic communication and hope management to enable shared decision-making. For people with bowel obstruction, the value of sharing decisions varies across time and circumstances, and their motivation and feelings of competence to engage are not stable, but influenced by their physical, psychological and situational experiences at any given moment. Iterative decision-making can enable gradual adaptation. These conclusions suggest the need to develop working models of interdisciplinary decision-making that consider the role of implicit behavioural mechanisms in decisional deliberations, and how they are contextualised by the characteristics of complex health conditions.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163261446132 – Supplemental material for Exploring Pathways to Optimise Care in malignant bowel obstruction (EPOC): A realist review of shared decision-making with people with advanced cancer and severe symptoms
Supplemental material, sj-docx-1-pmj-10.1177_02692163261446132 for Exploring Pathways to Optimise Care in malignant bowel obstruction (EPOC): A realist review of shared decision-making with people with advanced cancer and severe symptoms by Alison Bravington, Miriam Johnson, Sarah Greenley, Michael Patterson, Jason W. Boland, Fliss E. M. Murtagh, Michael Lind and Mark Pearson in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163261446132 – Supplemental material for Exploring Pathways to Optimise Care in malignant bowel obstruction (EPOC): A realist review of shared decision-making with people with advanced cancer and severe symptoms
Supplemental material, sj-docx-2-pmj-10.1177_02692163261446132 for Exploring Pathways to Optimise Care in malignant bowel obstruction (EPOC): A realist review of shared decision-making with people with advanced cancer and severe symptoms by Alison Bravington, Miriam Johnson, Sarah Greenley, Michael Patterson, Jason W. Boland, Fliss E. M. Murtagh, Michael Lind and Mark Pearson in Palliative Medicine
Footnotes
Acknowledgements
We would like to acknowledge the support of Patient and Public Representative Rashmi Kumar in developing the stakeholder consultation for this review.
ORCID iDs
Author contributions
Conceptualisation: Alison Bravington, Mark Pearson, Miriam Johnson, Jason Boland, Michael Patterson, Fliss Murtagh, Michael Lind. Clinical input: Miriam Johnson, Jason Boland, Fliss Murtagh, Michael Lind, Michael Patterson. Data curation: Alison Bravington, Michael Patterson, Sarah Greenley. Formal analysis: Alison Bravington, Mark Pearson, Miriam Johnson, Jason Boland, Michael Patterson, Fliss Murtagh, Michael Lind. Funding acquisition: Alison Bravington, Miriam Johnson. Investigation: Alison Bravington, Michael Patterson, Sarah Greenley. Methodology: Alison Bravington, Mark Pearson, Sarah Greenley. Project administration: Alison Bravington, Michael Patterson. Manuscript preparation: Alison Bravington drafted the manuscript. All authors contributed to revisions and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The registered charity Yorkshire Cancer Research funded this study. Award reference number: HEND405AB. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. Fliss E. M. Murtagh is a National Institute for Health and Care Research (NIHR) Senior Investigator. The views expressed in this article are those of the authors and not necessarily those of the NIHR, or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Research materials related to this paper are available from the corresponding author on request.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.