
Abstract
Background:
High-quality palliative care is an international human right. Despite reduced life expectancy, people with severe mental illness face major disparities in access and quality.
Aim:
This study explored requirements for good palliative care for people with severe mental illness as perceived by stakeholders.
Design:
This Group Concept Mapping study used a mixed-methods participatory design with two phases: (1) an online brainstorming period (25 days), in which participants could respond several times to the focus prompt about good palliative care for patients with severe mental illness, and (2) individual sorting and rating of statements, followed by data analysis using multidimensional scaling and hierarchical cluster analysis.
Setting/Participants:
This study included 163 broadly defined stakeholders involved in severe mental illness care in the Netherlands, predominantly healthcare professionals, including client representatives and relatives.
Results:
Based on 98 unique statements derived from 515 responses, a concept map of seven clusters emerged: “Selfcare for healthcare professionals,” “Expertise,” “Communication in advance care planning (highest rated cluster),” “Care chain,” “Organization and policy making,” “Advance care planning” and “Patient centred care.” Statement 66, “Centralize the patient,” was considered most important.
Conclusions:
Good palliative care for people with severe mental illness is challenged by complexity, stigma and varied stakeholder demands. As basic requirements are often unmet in mental health care, individuals with severe mental illness are at increased risk of being deprived of their rights to receive quality palliative care. This study underscores the need to extend care recommendations and improve professional training, focusing on self-care and interdisciplinary education.
People with severe mental illness die significantly earlier than the general population and have complex psychiatric, physical, and social needs.
End-of-life care for this group is understudied and complicated by communication issues, decision-making challenges, and poor integration of mental health and palliative care.
Limited guidelines and training cause role uncertainty and reinforce the gap between psychiatric and palliative services.
Findings highlight the requirements for good palliative care for people with severe mental illness, as identified and rated in importance by professionals across psychiatry, somatic care, and palliative healthcare.
Training is needed: in self-care for professionals, and in cross-education between palliative and mental healthcare.
Stigma must be addressed, as it undermines care quality for people with severe mental illness and cuts across all identified themes.
Introduction
Palliative care is a holistic approach to improving quality of life for people facing life-threatening illness or frailty, across physical, psychological, social, and existential domains.1 –3 While increasingly recognized as a human right3 –5 and well-supported in oncology, 6 its application beyond cancer remains limited7 –9—particularly for people with severe mental illness such as schizophrenia, bipolar disorder, or recurrent major depression.10 –12
People with severe mental illness die 10–20 years earlier than the general population, often from preventable conditions like cardiovascular disease, cancer, and respiratory illness.13 –15 In the Netherlands, 400–450 institutionalized patients with severe mental illness die yearly from such causes, yet access to timely and appropriate palliative care remains limited. 16
Although no Randomized Controlled Trials exist for palliative care in severe mental illness, observational studies in France show that people with severe mental illness sometimes receive earlier palliative care and less aggressive end-of-life treatment than those without mental illness.17 –19 However, this likely reflects clinical hesitancy—due to stigma, doubts about decision-making capacity, and fear of destabilizing psychiatric symptoms—rather than person-centred care. 20 These studies focus only on the last month of life and overlook palliative care’s broader potential earlier in the illness trajectory.
Qualitative research shows patients with severe mental illness are often excluded from end-of-life decisions, and their preferences rarely documented—unlike the general population, where most receive timely palliative care.21 –23 Structural issues deepen this gap: since 2017, Dutch general hospitals must have palliative care teams, but this does not apply to long-term mental healthcare institutions. 24
A recent scoping review highlighted limited autonomy, unequal access, stigma, and potential benefits of integrating palliative care into psychiatry. 25 Empirical research involving both mental health and palliative care professionals remains scarce. This study explores what professionals—across psychiatry, somatic care, addiction services, and palliative care—view as essential for good palliative care for people with severe mental illness.
Method
We applied Group Concept Mapping, a methodology that integrates quantitative and qualitative research methods to organize all ideas from a group of stakeholders.26,27 Group Concept Mapping is a well-established, structured approach for visualizing the interrelation of these ideas, particularly useful for complex and multidimensional concepts 27 like palliative care. The method consists of three phases: first, brainstorming to identify ideas related to requirements for palliative care for people with severe mental illness; second, sorting and rating each idea identified during the brainstorming phase; and third, grouping ideas into conceptual clusters (analysis). Data were collected and analyzed using groupwisdom™ software, 28 resulting in a concept map. 26
The study protocol was approved by the scientific committees of the two participating mental health care organizations (GGz Centraal and GGz Drenthe). The Medical Ethics Review Committee stated that the Medical Research Involving Human Subjects Act does not apply to this study and that an official approval is not required. 29 Informed consent was obtained from all participants prior to data collection.
Participants
Stakeholders were recruited from May 9 through June 15, 2023. We used purposive and snowball sampling methods, reaching out via email to network contacts and posting a call on the online social network LinkedIn. Potential stakeholders were encouraged to share the call within their own networks. The targeted groups included employees of general practices, mental health and addiction care institutions, general and hospital consultation teams for palliative care, home care teams specializing in palliative care, hospices, spiritual caregivers, social caregivers, client councils of mental health institutions, relatives of patients with severe mental illness and a palliative care indication, and organized palliative care networks, including palliative care policy officers. Participants were asked to provide information about their age, sex, profession, work setting, and experience with palliative care. They were also asked to sign informed consent.
Procedure
Phase 1—Preparation
Group Concept Mapping starts with the formulation of a focus prompt. A proper focus prompt is crucial to guide the brainstorm and generally comprises one or two sentences to be completed with as many ideas as possible by the participants. After literature research 1 and discussion within the research team, we agreed on the following focus prompt: “Good palliative care (for severe mental illness patients), i.e., care for individuals whose death within 12 months would not be surprising, must consist of . . . ?” Members of the research team personally approached several individuals from their professional networks to ensure that the prompt was clear, understandable, and appropriately formulated. The explanation made explicitly clear how palliative care was defined (see introduction) and clarified that the focus prompt only concerned people with severe mental illness.
In total, 508 stakeholders received an invitation by e-mail and 163 participated online between May 11 and June 5, 2023. Participants were asked to complete the focus prompt with as many ideas as possible and could log in multiple times to submit additional responses throughout the period. Participants’ statements were immediately anonymized and visible to all participants. The 163 participants provided a total of 515 statements. The 515 statements generated during the brainstorming session were systematically reduced to a final set of 98 unique statements through a structured idea synthesis process, in line with Group Wisdom guidelines. 2 The steps, performed by the authors Briek and Shabani and critically reviewed and discussed step by step by all other authors, were as follows:
Export to Excel: Statements were exported to a spreadsheet to systematically track revisions.
Splitting compound statements: Statements with multiple ideas were divided so each reflected a single concept (e.g. “A designated palliative care coordinator within each team! Greater attention to the four domains, advance care planning, and the use of the Surprise Question. I believe there is a significant knowledge gap” was split into four statements: “A designated palliative care coordinator within each team!,” “Greater attention to the four domains,” “Advance care planning,” and “The use of the Surprise Question.”
Keyword assignment: Keywords were assigned to enable grouping and comparison (e.g. advance care planning, multidisciplinary collaboration, quality of life, communication, training, euthanasia).
Removal of duplicates: Identical statements were removed to reduce redundancy (e.g. “Destigmatization” and “Destigmatization”).
Statement clarification: Wording was edited for clarity while preserving meaning (e.g. “Honest, gentle care focused on comfort” became “Comfort care”).
Final reduction/theme refinement: Overlapping statements were merged and refined, reducing the set to 94 statements for sorting and rating (e.g. protocol-related statements merged into “Substantiated deviations from applicable protocols may occur”). After author discussion, some were further split or merged to capture nuances, resulting in 98 final statements, each representing a distinct idea.
Phase 2—Sorting and rating
For the sorting phase, participants needed to represent the brainstorming population and have relevant expertise. 26 In line with Group Concept Mapping guidelines, 26 36 out of 163 brainstorming participants (22%) were purposively invited by email to ensure representation across professions, work areas, and palliative care experience. Relatives of patients were invited but none chose to participate. Of the 36 invited participants, 24 (66.7%) completed the sorting phase (2 did not respond, 2 declined, and 8 did not complete sorting before the deadline).
These 24 participants individually sorted all statements into categories according to their own perception of similarity. Following Group Concept Mapping guidelines, 26 participants grouped statements into 5–20 clusters (minimum two statements each) and named each based on its content. Researchers (Briek and Shabani) were available for help if needed.
Subsequently, participants rated the individual statements according to their importance for the concept of successful treatment on a five-point Likert scale (1 = unimportant; 5 = very important). 26 Data from one participant was considered unreliable as she rated all statements exactly the same (nurse).
Phase 3—Analyses
First, we counted the number of participants who sorted each pair of statements together, creating a similarity matrix. Based on this similarity matrix, two-dimensional nonmetric multidimensional scaling was performed, resulting in the statements being plotted in a two-dimensional point map. For this point map, a stress value was calculated (ranging from 0 to 1) to indicate the fit of the two-dimensional map. Stress values usually range from 0.21 to 0.37. 26 A high stress value implies a greater discrepancy between the similarity matrix and the representation of these data in the two-dimensional point map. 26 A bridging value was calculated for each statement (ranging from 0 to 1). A lower value indicates that a statement is more anchored, reflecting the content in its vicinity on the map because it was sorted more often with nearby statements. A higher value, known as a bridging value, indicates that a statement links more distant areas on the concept map. Such statements may serve as connections between conceptually different clusters, highlighting ideas that bridge multiple themes. 26
Subsequently, we performed hierarchical cluster analysis using the coordinates of the point map and evaluating the statements’ bridging values. This analysis assesses which number of clusters is most suited for describing the contents by examining which statements merged per solution. 26 We started with a 10-cluster solution based on an average of 7.9 clusters (SD = 3.0) found in a review of 104 concept mapping studies. 30 We then checked for a better fit by increasing or decreasing the number of clusters. Cluster membership is ambiguous for statements with high bridging values located on the edge of a cluster, which may even contribute to small overlap between clusters. Therefore, discussion focused on these high-bridging-values statements, evaluating their placement in relation to other statements in the same cluster and their coherence with other clusters on the map. Each (co-)author independently chose the preferred number of clusters, and consensus was reached through discussion. 26 This process resulted in a 7-cluster solution. Finally, we calculated average cluster ratings and produced a cluster rating map.
Results
The 163 participants were on average 47.5 years and 77.9% were females. Nearly half (76/163; 46.6%) were involved in palliative care for three or more cases per year. The professional background was diverse, including among others: nurses at all levels, doctors, psychiatrists, psychologists, spiritual counselors, social workers, experienced healthcare experts, project leaders, a pharmacist, a nursing teacher, and relatives of deceased patients. In terms of work setting, mental health care, general health care, care for the mentally disabled, and the social domain were represented. See Table 1 for more details and selection of participants for phase 2.
Characteristics of study participants of phase 1 (n = 163) and phase 2 (n = 23).
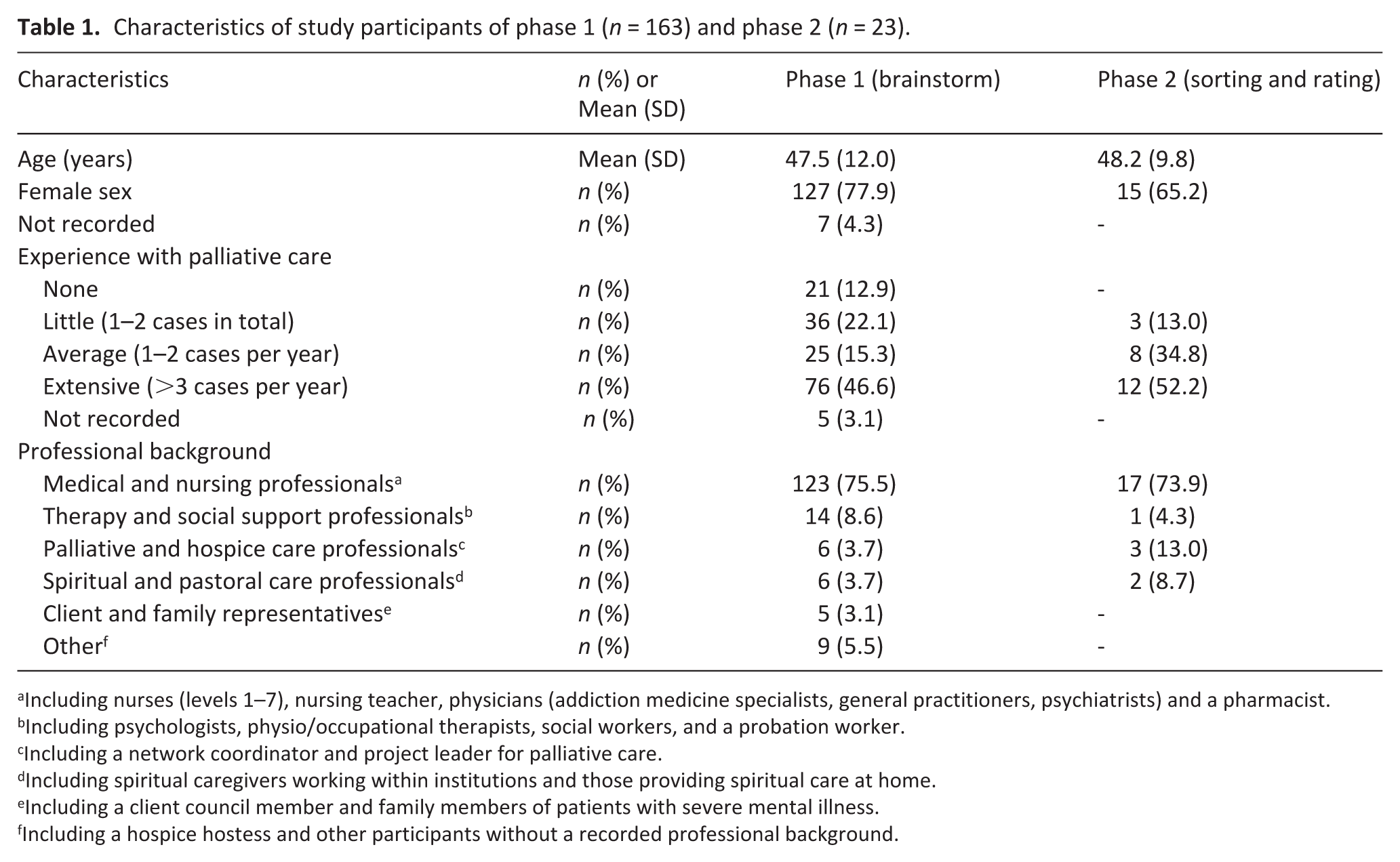
Including nurses (levels 1–7), nursing teacher, physicians (addiction medicine specialists, general practitioners, psychiatrists) and a pharmacist.
Including psychologists, physio/occupational therapists, social workers, and a probation worker.
Including a network coordinator and project leader for palliative care.
Including spiritual caregivers working within institutions and those providing spiritual care at home.
Including a client council member and family members of patients with severe mental illness.
Including a hospice hostess and other participants without a recorded professional background.
Sorting and rating
The 24 stakeholders each sorted the 98 statements into 2–19 clusters, averaging 10. The hierarchical cluster analysis revealed a seven-cluster solution as most optimal (see Figure 1). The stress value of the results was 0.30 indicating that the results are interpretable (range 0.1–0.35).
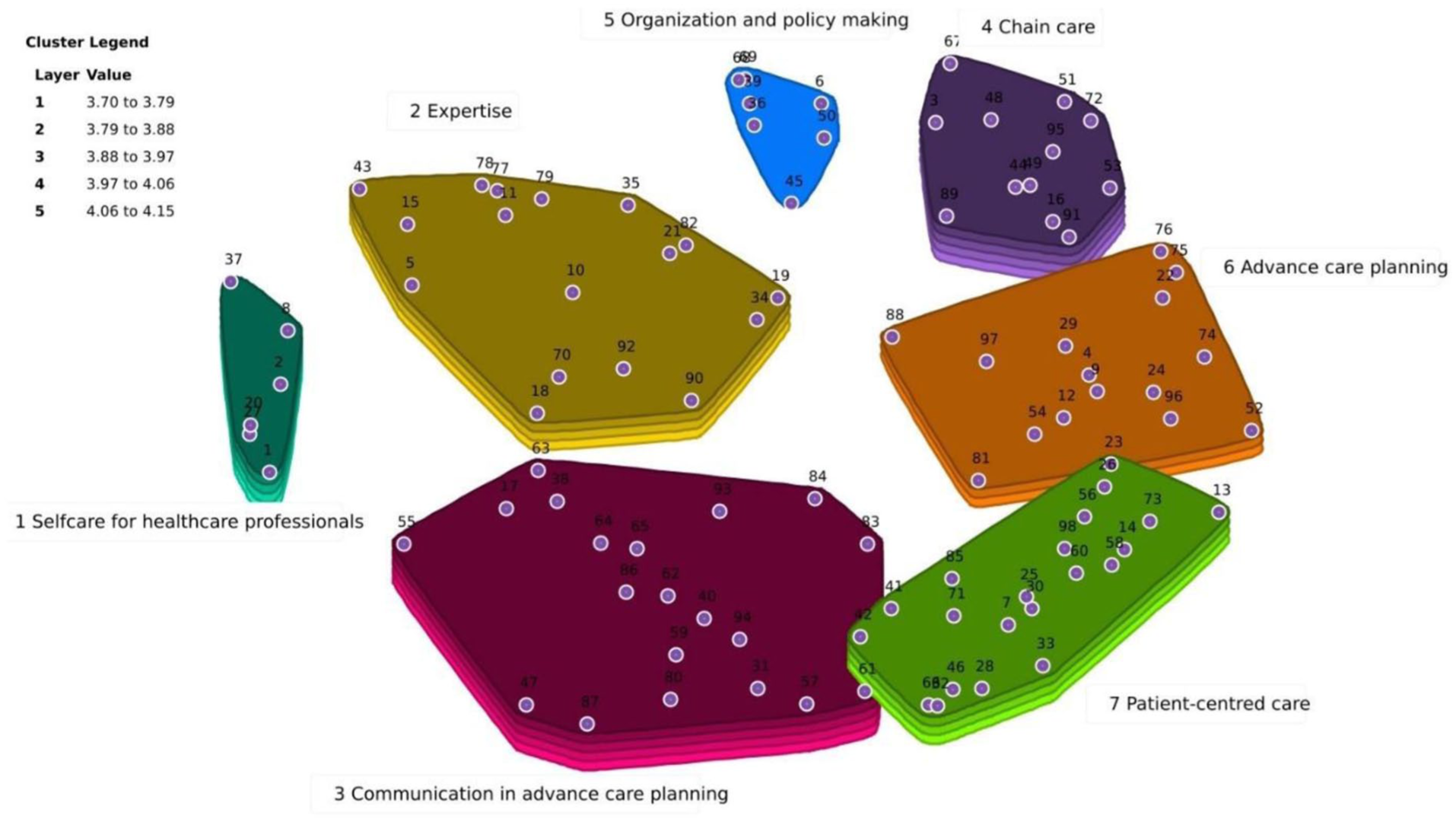
Cluster map with 7 clusters, including the importance. Footnote: Each dot is accompanied by a number that represents the statements as presented in Table 2.
Based on content and category labels provided by stakeholders during sorting, the groupwisdom™ software 28 automatically generated cluster names. Cluster names were reviewed and adjusted by author consensus, then shared via email with sorting and rating participants for accuracy and relevance. This resulted in seven cluster domains (see Figure 1):
Cluster 1 “Selfcare for healthcare professionals” emphasizes the workload for professionals given the moral dilemmas and not being accustomed in working with people who will die in the foreseeable future.
Cluster 2 “Expertise” emphasizes the need of training in palliative care for (mental) health care workers.
Cluster 3 “Communication in advance care planning” emphasizes the need of adequate communication skills and especially a pro-active approach starting immediately after marking the palliative care need.
Cluster 4 “Chain care” emphasizes that need of involvement and close collaboration with the different stakeholders, especially across the different health care settings and echelons.
Cluster 5 “Organization and policy making” emphasizes the need for managerial and administrative support of the palliative chain care for people with SMI.
Cluster 6 “Advance care planning” emphasizes the importance of adequately performing all advance care planning activities tailored to the patient’s condition regarding his physical, psychological, social, and existential care needs.
Cluster 7 “Patient centred care” emphasizes the need for personalized care, acknowledging their autonomy and giving most priority to the peoples’ own wishes (and limits).
Ranking of the clusters based on the average importance of the statements on a 5-point rating scale, cluster 3 “Communication in advance care planning” ranks first (mean importance (I = 4.15), followed by cluster 4 “Chain care” (I = 4.13), cluster 1 “Selfcare for health professionals” (I = 4.07), cluster 7 “Patient-centred care” (I = 4.03), cluster 2 “Expertise” (I = 4.01), cluster 6 “Advanced care planning” (I = 3.95), and finally cluster 5 “Organization and policy making” (I = 3.70) being least important. Since clusters are close to each other, no cluster can be rated as unimportant.
Table 2 (extended version supplemental file online) presents the complete list of statements of the conceptual map, including the mean importance rated for each statement based on the 5-point rating scale and its bridge value.
The four most important statements, importance ratings (I) and bridging values (B) per cluster.
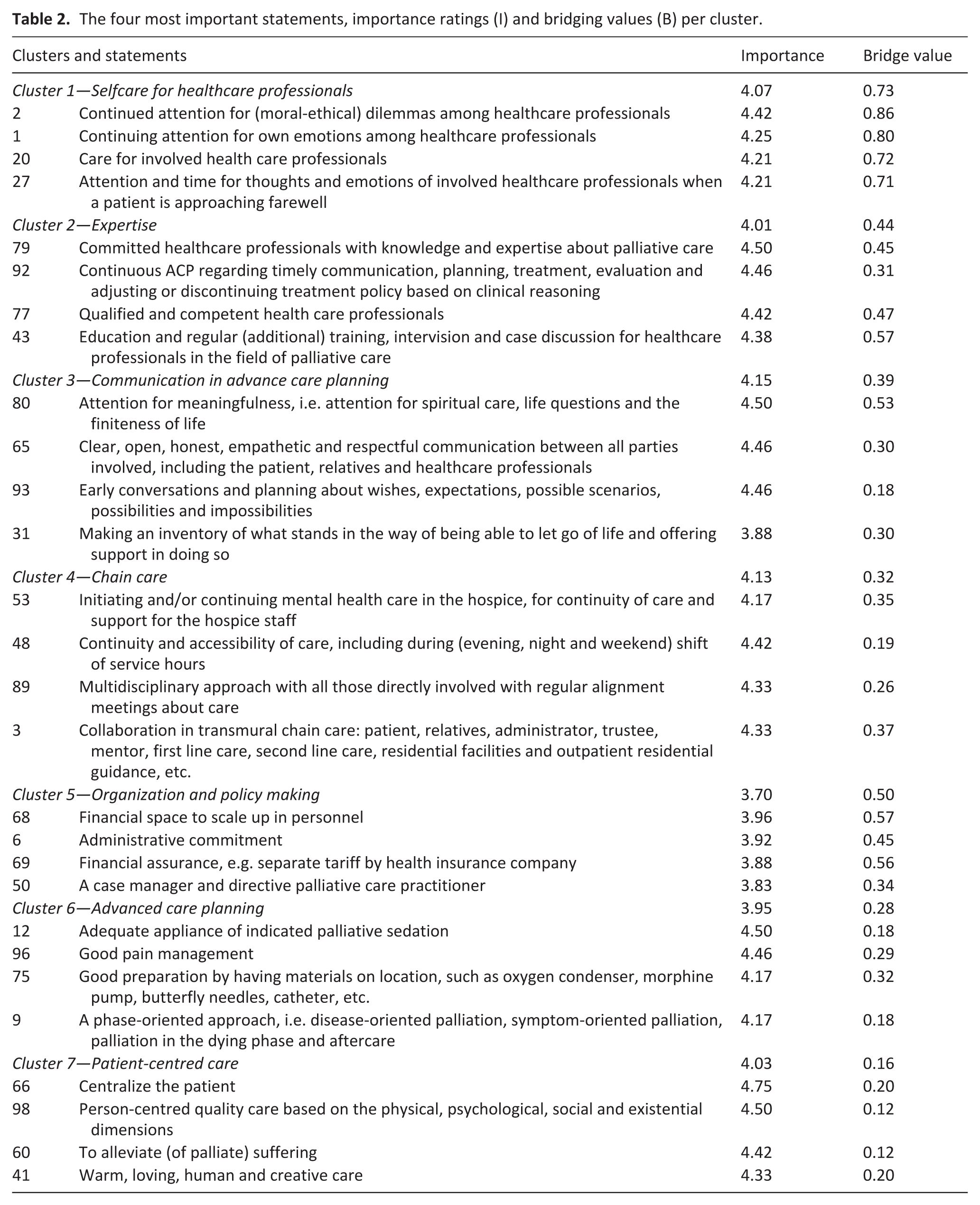
Figure 2 presents the importance per cluster based on the average importance of the statements on a 5-point rating scale between doctors (n = 8) and nurses (n = 9). Doctors rated cluster 4 “Chain care” highest (I = 4.20), compared to cluster 3 “Communication in advance care planning” among nurses (I = 4.11). Both rated cluster 5 “Organization of care” the lowest (doctors, I = 3.75); nurses, I = 3.52). The biggest difference is also in cluster 5, where doctors rate it higher (I = 3.75) than nurses (I = 3.52), followed by cluster 1 “Selfcare for healthcare professionals,” where nurses rate it higher (I = 4.07) than doctors (I = 3.88).
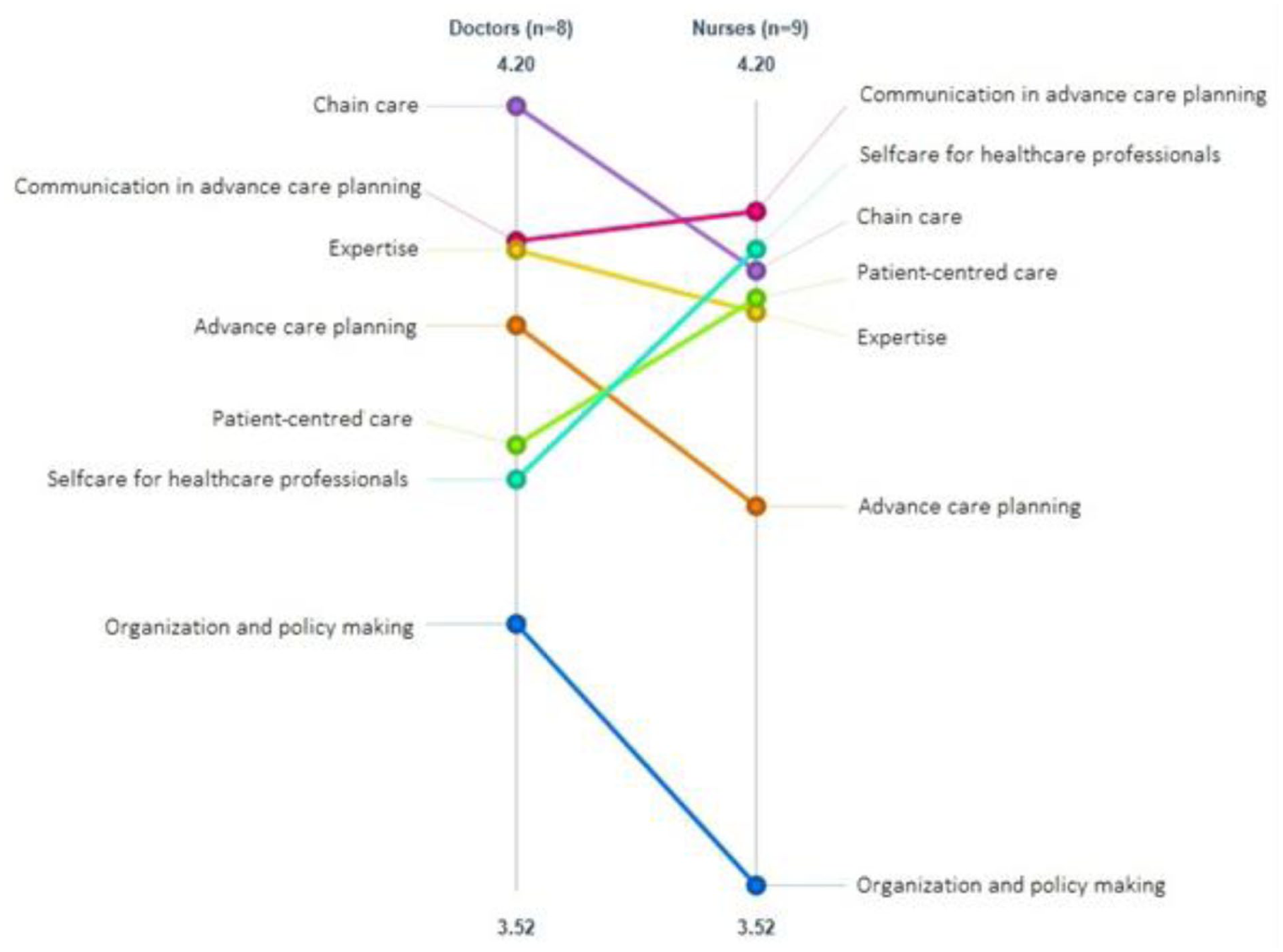
Pattern match of the clusters based on importance by doctors and nurses.
Discussion
Main findings
This Group Concept Mapping study identified seven clusters of requirements for providing good palliative care to people with severe mental illness, from the perspective of clinical professionals (stakeholders). All clusters were rated highly relevant, with mean importance scores on a 5-point Likert scale ranging from 3.70 (“Organization and policy making”) to 4.15 (“Communication in advance care planning”). Autonomy in decision-making, access to care, and stigma reduction were considered most critical for good palliative care in this population. It should be noted that the findings primarily reflect the perspectives of clinical professionals, as people with lived experience and relatives participated only in the brainstorming phase and did not take part in the subsequent sorting and rating phases, which may have influenced the prioritization of needs.
What this study adds
Below we discuss the seven domains in detail.
Communication in advance care planning, advance care planning, and patient-centred care
The “Communication in advance care planning” cluster was rated highest and closely aligns with “Person-centred care” and “Advance care planning”, including statements on proactive communication skills, shared decision-making, and patient- and family-oriented attitudes. These themes are not yet fully realized for people with severe mental illness—particularly those with schizophrenia—due to stigma, limited disease knowledge, communication barriers, and late diagnoses of terminal conditions. 31 Palliative care involvement remains limited, hindering discussions about preferences and care planning.21,22 In the Dutch context, where patient autonomy, shared decision-making, and advance care planning are core healthcare principles, the limited use of advance care planning in mental health care for people with severe mental illness reveals a persistent gap between policy ideals and everyday clinical practice. Advance care planning, strongly endorsed by palliative care experts, may help reduce these disparities. 32 Although electronic systems support advance care planning documentation, their use in severe mental illness populations remains limited, reflecting a gap between recognizing disease progression and integrating palliative approaches. 32
Palliative care—especially early identification of the palliative phase and communication with patients and families—is still relatively new in mental health care, creating communication challenges for professionals. 10 This finding reflects the Dutch situation in which palliative care has traditionally been developed within somatic and primary care settings, while its integration into mental health care remains relatively underdeveloped, although awareness of this need has increased over the past decade. Nurses, who often bridge patients and doctors, rate communication in advance care planning higher than doctors, likely due to closer patient contact. 33 Stakeholders also emphasized the importance of spirituality and existential issues for patient well-being and quality of life.34,35
Selfcare of healthcare professionals
Concerns about healthcare professionals’ well-being are growing, and burnout-related costs are high. 36 Palliative care is emotionally demanding and may lead to stress and burnout,37 –39 particularly when caring for people with severe mental illness due to additional challenges. 10 Nurses especially face ethical dilemmas in communication and decision-making, 33 while doctors may struggle with increasing deaths in an aging society. 37 Self-care is both vital and an ethical imperative, as emphasized in the codes of various health disciplines, including psychology, medicine, and nursing. 40 Within the Dutch healthcare system in Netherlands, where workforce shortages and workload pressures are rising, the focus on self-care highlights the need for structural support for professionals working at the intersection of mental health and palliative care. Yet it is often overlooked in medical education and training. 40 Integrating self-care into training is essential for maintaining a healthy work-life balance. 23 Moral deliberation and tools using the steps: Concentrate, Postpone, Reflect, and Take Action, can help professionals navigate ethical challenges.40,41
Chain care
The “Chain care” cluster underscores the importance of seamless interdisciplinary coordination in palliative care. However, barriers remain for people with severe mental illness and terminal illness due to the separation of mental and somatic health care.10,42,43 This results in limited access to palliative care, 44 stigma-related challenges, 45 and inadequate involvement of somatic specialists.11,12 Given that high-quality palliative care is best achieved through multidisciplinary teamwork, 46 efforts to enhance formal and informal collaboration within the healthcare system are crucial. 47 In the Netherlands, where mental and somatic care remain largely separate, this fragmentation challenges timely, coordinated palliative care for people with severe mental illness, underscoring the need for prioritization and advocacy within regional palliative care networks.
Expertise
Delivering high-quality palliative care requires adherence to established advance care planning and palliative care frameworks.1,2 In the Netherlands, palliative care is generally generalist and often provided by less experienced staff. 37 Although the Netherlands has a well-developed palliative care infrastructure, expertise is unevenly distributed—especially in mental health services, where tailored guidance for people with severe mental illness is limited. Training exists but remains small-scale and unsystematic, highlighting the need for further development. Mental health professionals may misattribute physical symptoms as psychological, delaying diagnosis of life-threatening conditions. 48 Existing guidelines don’t address the specific needs of people with severe mental illness,1,2 who may have limited insight into their health.10,12,49 The cluster highlights the importance of knowledge, destigmatization, competency, education, training, and communication skills.10,50 Studies show mental health professionals are eager and able to train in palliative care as much as others.43,47,51,52 Training these elements strengthens palliative care expertise, though it is often resource-intensive. 53
Organization and policy making
Stakeholders emphasized the importance of organizational aspects in palliative care, including resources like case managers, managerial commitment, financial support, and care accessibility. Disparities in palliative care are evident, especially among people with schizophrenia. 31 Research such as the mixed methods systematic review and thematic synthesis of published case studies study 47 highlights the need for coordinated care to prevent vulnerable individuals from navigating the system alone and receiving inadequate care. Addressing this requires designated staff roles and shared care protocols linking mental health and palliative care services. 47 Providing palliative care is demanding, but tackling facilitators and barriers at individual, team, and organizational levels can ease the burden. Key issues include poor self-care, stigma among professionals, and fragmented healthcare systems.37,42,47 These findings are particularly relevant in the Netherlands, where care is highly regulated and protocol-driven, yet responsibility for coordinating palliative care for people with severe mental illness often remains diffuse across organizations and sectors.
Strengths and limitations
Our study is the first Group Concept Mapping on palliative care for people with severe mental illness, involving diverse stakeholders. However, three limitations apply. First, a key limitation of this study concerns the absence of patients themselves. While we consulted client representatives during study design, patients were not invited to participate due to the complexity and cognitive demands of the method. Their perspectives will be explored in a separate qualitative study using individual interviews.
As a result, the study primarily reflects a professional perspective. Although four relatives initially contributed to the brainstorming phase, they unfortunately did not participate in the subsequent sorting sessions. This relative homogeneity of the sample may have influenced the prioritization of statements, particularly those related to healthcare provider needs, and is therefore explicitly addressed as a limitation. Second, we did not assess stakeholders’ ethnic, religious, or cultural backgrounds. Third, palliative care models vary by country, so replication elsewhere is needed. Despite these limitations, given the generic themes identified, strong divergences are unlikely, but future studies including more people with lived experience could further refine the findings. Future research is underway to explore the preferences and needs of people with severe mental illness themselves, which will complement the findings of the current study.
Conclusion
Stakeholders identified and valued seven key concepts for palliative care in severe mental illness, with “Communication in advance care planning,” “Chain care,” and “Self-care for health professionals,” as crucial for quality care. Stigma severely limits palliative care quality for people with severe mental illness and affects all clusters of this Group Concept Mapping. Our findings align with general palliative care protocols and suggest that despite the lack of evidence for patients with severe mental illness, general recommendations for advance care planning, patient-centred care, and shared decision-making should also be available for them. Better training for healthcare professionals is essential: first, in self-care to sustain care, and secondly, in educating palliative care providers about psychiatric disorders and mental healthcare providers about palliative care.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163261446791 – Supplemental material for Good palliative care for people with severe mental illnesses: A Group Concept Mapping study
Supplemental material, sj-pdf-1-pmj-10.1177_02692163261446791 for Good palliative care for people with severe mental illnesses: A Group Concept Mapping study by Jojanneke Briek, Ajsha Shabani, Radboud M. Marijnissen, Heidi de Kam, Richard C. Oude Voshaar and Didi Rhebergen in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank the participants for their contributions.
Author contributions
J. Briek.: Data collection, conceptualization, methodology, validation, writing, review, editing, data curation. A. Shabani.: Data collection, conceptualization, methodology, validation, writing, review, editing, data curation. R. Marijnissen.: Study design, data collection, conceptualization, methodology, validation, writing, review, editing. H. de Kam.: Data collection, conceptualization, methodology, validation, writing, review, editing. R. Oude Voshaar.: Study design, conceptualization, methodology, validation, writing, review, editing. D. Rhebergen.: Study design, data collection, conceptualization, methodology, validation, writing, review, editing. All authors have thoroughly reviewed the manuscript draft to ensure it contains significant intellectual content. They have approved the final version for publication and have agreed to take responsibility for every aspect of the work. This includes addressing any questions regarding the accuracy or integrity of any part of the work by conducting the necessary investigations and resolving any issues.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Healthcare Support Fund and is known by its name “Palliatieve zorg voor patiënten met ernstige psychiatrische aandoeningen (PROM-18).”
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Transparency declaration
This manuscript provides a truthful, precise, and clear account of the study being reported. It includes all significant aspects of the study, with nothing important left out. Any deviations from the original study plan have been fully explained.
Supplemental material
Supplemental material for this article is available online, including an extended version of Table 2.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.