
Abstract
Background:
Healthcare assistants delivering home-based palliative and end-of-life care face complex emotional and clinical demands with limited workplace support. Peer support had been suggested as a potential solution, yet no reviews of such interventions exist.
Aim:
To understand and explain how, why, for whom and in what contexts workplace peer support interventions for healthcare assistants work (or do not work) in palliative and end-of-life care delivery at home.
Design:
Realist review registered with PROSPERO (registration number CRD42024606133).
Data sources:
CINAHL, MEDLINE, AMED, Scopus and grey literature with no date restrictions. Searches undertaken November-December 2024. All study designs containing data relevant to programme theory were included. Evidence was assessed for relevance, trustworthiness and rigour.
Results:
Synthesis of 24 sources generated 12 context-intervention-mechanism-outcome configurations used to develop initial programme theory. Four workforce outcomes of intervention include: enhanced wellbeing and resilience, reduced loneliness and isolation, development of a sense of community of practice and strengthened role identity. Three intervention strategies: peer-facilitated group meetings, 24/7 peer support access, and informal peer mentorship, create psychologically safe spaces, where individuals feel validated, valued, connected with others, enabling social learning. The intervention elements align with the fulfilment of three basic psychological needs: competence, autonomy, and relatedness.
Conclusions:
The initial programme theory reveals peer support may address core workforce challenges through psychologically safe peer connections and social learning, aligning with fulfilment of basic psychological needs. It provides a foundation for designing and testing evidence-informed peer support interventions for this workforce.
Keywords
Healthcare assistants providing palliative and end-of-life care at home face emotional labour, loneliness and isolation, with limited access to workplace training, managerial and peer support.
Healthcare assistants’ titles, training and regulation vary widely across countries, with many beginning their roles with minimal preparation and learning on the job.
Peer support was shown to enhance staff wellbeing, foster resilience and improve team dynamics among healthcare professionals, but no reviews have examined how such interventions work for healthcare assistants.
Peer support works by creating psychologically safe spaces and relationships where healthcare assistants feel validated, valued, and connected with others and through social learning among peers who share similar experiences.
This realist review develops an initial programme theory – a theoretical explanation of how, why, and in what circumstances peer support interventions work – with 12 configurations, that link contexts, interventions, mechanisms and outcomes, explaining how workplace peer support interventions may work for healthcare assistants delivering palliative and end-of-life care at home.
Four main workforce outcomes were identified: enhanced wellbeing and resilience, reduced loneliness and isolation, development of a sense of community of practice and strengthened role identity.
Organisations may consider implementing peer support with multiple adaptive components (facilitated meetings, 24/7 access, peer mentorship), trained peer facilitators, and organisational endorsement positioning peer support as valued professional practice.
The initial programme theory provides a foundation for designing evidence-informed interventions that can be tested and refined across diverse healthcare contexts.
Introduction
The global rise in ageing populations and chronic illness has significantly increased the demand for palliative care delivered in home settings.1–5 Increasing demand, financial constraints and workforce shortages have led to greater reliance on assistive personnel, such as healthcare assistants, across various care settings, including palliative and end-of-life care.6–8 Although support workers are common across global healthcare systems, their titles, training and regulation vary widely.9,10 We use the term ‘healthcare assistant’ in this paper but several other titles, such as Unregulated care providers (UCPs), Homecare workers, Nurse assistants (NAs), will be mentioned when providing quotes, due to being used interchangeably within the literature.
In some settings healthcare assistants begin their roles with minimal preparation, learning on the job without structured mentorship or supervision.11–14 Opportunities for reflective practice, debriefing or peer learning are rare, particularly in lone working environments.11,15,16 This absence of support undermines healthcare assistants’ confidence and professional development and may have negative consequences to the quality of care provided.13,17 Without access to ongoing training and peer networks, healthcare assistants, similarly to other healthcare professionals, may struggle to manage complex care situations, leading to emotional exhaustion and high turnover.11,18,19
A defining aspect of healthcare assistants’ work is the significant emotional labour involved.20–22 Providing end-of-life care in the home often involves witnessing suffering, managing grief and supporting families through distressing circumstances.11,20,23 The unpredictable nature of end-of-life care places additional stress on healthcare assistants, who often work alone to meet complex physical, emotional, social and spiritual needs.6,17,22,24,25 The emotionally charged experiences can accumulate over time, leading to compassion fatigue, stress and burnout among healthcare workers.18,26 Healthcare assistants may carry the weight of their work into their personal lives, with limited opportunities to process these experiences in a supportive environment, leaving many to navigate their emotional wellbeing alone.20,21,27
Recruitment and retention of healthcare assistants remain a persistent challenge in the healthcare sector. 28 High turnover rates are driven by low pay, limited career progression and the emotional toll of the work among other factors.29–31 The sector’s reliance on a predominantly female, often migrant workforce further complicates these dynamics, as issues of gender differences, discrimination and precarious employment intersect with care delivery.32,33 To sustain this workforce and ensure quality care, changes are needed. These include the development and facilitation of peer support interventions repeatedly reported as lacking and needed by healthcare assistants.11,12,33–35
Given these workforce challenges, attention has turned to supportive interventions. Peer support within a workplace, defined as mutual emotional and professional support among colleagues, was shown to enhance staff wellbeing, foster resilience and improve team dynamics and patient safety.36,37 However, there is a notable lack of research exploring how such support mechanisms function within the healthcare assistants’ workforce, especially in home-based palliative and end-of-life care. While existing literature has examined the broader role of healthcare assistants22,25,38 and the value of workplace peer support among healthcare professionals,36,39,40 no realist review has yet investigated how peer support interventions may support palliative and end-of-life care delivery by healthcare assistants. Unlike traditional systematic reviews that focus on whether interventions work, a realist review seeks to explain how and why they work, for whom, and in what circumstances. By synthesising both empirical and grey literature through a theory-driven lens, realist review could offer valuable insights into the mechanisms and contexts that enable peer support to achieve desired outcomes. Addressing this evidence gap is essential to developing sustainable, supportive practices that enhance both staff wellbeing and care quality.
Aim
To identify how, why, for whom and in what circumstances workplace peer support interventions for healthcare assistants are used and to develop initial programme theory for how they may work (or may not work) across varied contexts.
Review questions
What are the mechanisms by which workplace peer support interventions produce their outcomes (intended and unintended)?
What are the contexts in which these mechanisms are activated?
What outcomes do these mechanisms, in the right contexts produce for various stakeholders?
Methods
The review protocol was published 41 and registered with PROSPERO (registration number CRD42024606133). A realist approach was selected because it makes causal mechanisms and contextual conditions visible, generating programme theory that can inform the design of context-sensitive interventions.42–44 It does so by identifying causal configurations in the form of context, mechanism and outcome (CMO). 45 Context refers to the conditions in which the programmes (interventions) operate, which can include social norms, values, relationships and resources that exist within a particular setting. 46 Mechanisms are invisible generative forces activated by the resources or opportunities provided by an intervention within a specific context. 47 Outcomes, both intended and unintended, are a result of the interaction between context, mechanism and intervention components. 45 Together, these configurations form the foundation of programme theory, offering a structured theoretical explanation of how and why an intervention produces its outcomes.
Realist reviews are especially well suited to exploring complex interventions with multiple interacting components, uncertain outcomes and context-dependent variability.48–50 Peer support interventions are inherently complex due to their diverse formats and contextual influences on their implementation and outcomes. This review will help to identify the mechanisms through which peer support may bring desired outcomes, and the contextual factors that enable or hinder its effectiveness. Such evidence is critical for informing the design of sustainable, context-sensitive support strategies for healthcare assistants in palliative and end-of-life care settings. This review forms part of the wider study aiming to develop peer support intervention following INDEX guidance (IdentifyiNg and assessing different approaches to DEveloping compleX interventions). 51
The review was conducted in accordance with the five-stage realist review framework proposed by Pawson et al.42,43 and follows Realist and Meta-narrative Evidence Synthesis Evolving Standards (RAMESES). 52 More detail on each stage can be found in the published protocol. 41 The review was completed between October 2024 and July 2025. The review was conducted in accordance with the published protocol with no substantive deviations from the planned methodology.
Step 1: Locate existing initial programme theories
Exploratory database searches informed the development of the preliminary programme theory and search strategy. The lead author (KP) consulted with the research team, Research Advisory Group, information specialists and Patient and Public Involvement (PPI) groups to identify search terms, drawing on their experiential and content expertise. Based on this input and the findings from scoping searches, the search strategy was adapted and KP developed the preliminary programme theory of workplace peer support intervention, which was refined against evidence gathered in subsequent stages of the review.
Step 2: Searching for evidence
Evidence was sourced to confirm, refute, or refine elements of the preliminary programme theory. 53 Academic literature searches were conducted across CINAHL, MEDLINE, AMED and Scopus, from their inception to the present, using controlled vocabulary and targeted keywords (Supplemental material).
A broad definition of ‘healthcare assistant’ was adopted, as demonstrated by the extensive list of search terms (Supplemental material) as multiple role definitions and descriptions are used worldwide. 9 All studies involving healthcare assistants providing care for people who were dying in their own homes were considered, regardless of the underlying condition or the primary service involved–whether hospice care, long-term home care, dementia services or support for individuals with learning disabilities.
To supplement database searches, we employed forward and backward citation tracking and consulted expert stakeholders to identify additional relevant sources. Grey literature has also been included to capture contextual and evaluative insights not found in peer-reviewed sources. 54 Searches were conducted via Google, Trip and National Institute for Health and Care Excellence (NICE), with alerts set through Google Scholar and library services.
Step 3: Selection and appraisal of evidence
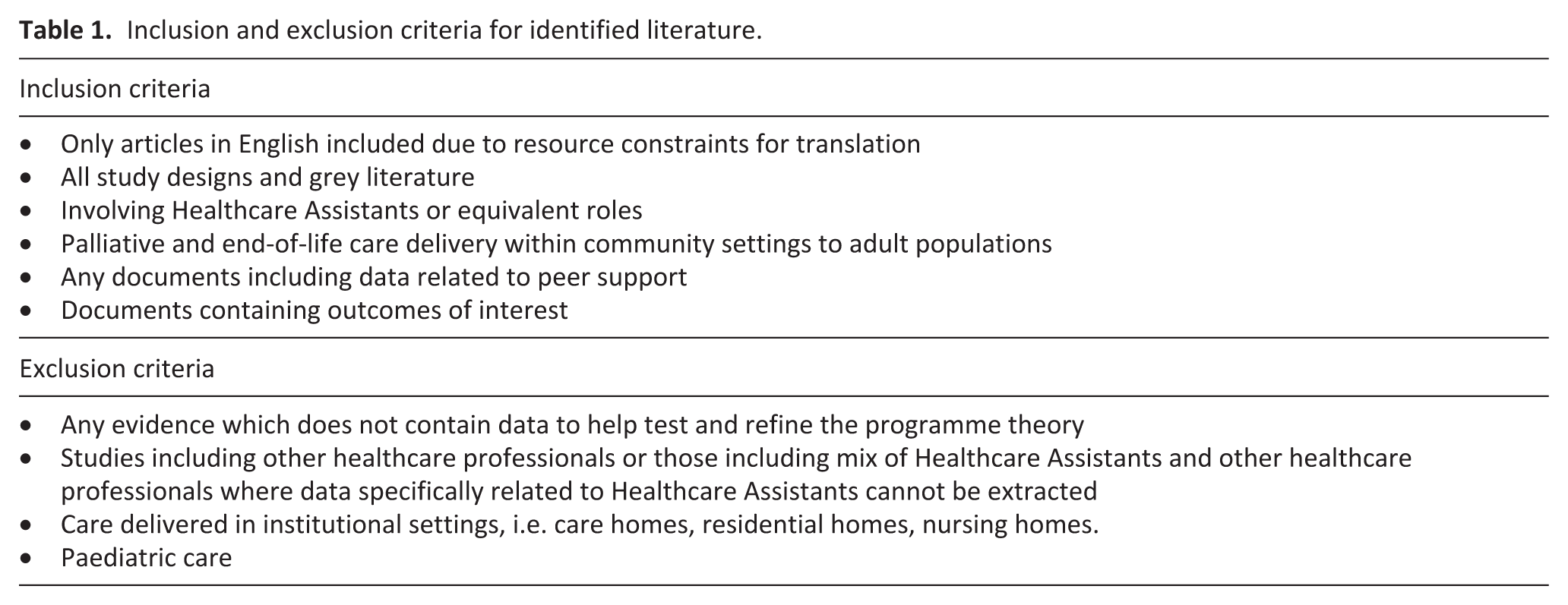
To ensure consistency, KP conducted identification, selection, and appraisal steps, with FH independently assessing a random 10% sample of excluded and included papers for quality assurance. 55 Papers were screened by title and abstract, then by full text using Covidence software, applying the inclusion and exclusion criteria listed in Table 1. In line with realist review methodology, appraisal was not applied as a threshold for inclusion or exclusion but was conducted iteratively during analysis to assess each source’s contribution to the programme theory. Following Wong et al.’s criteria, 56 each source included in the review was assessed for its relevance to the programme theory, its interpretive contribution as context, intervention, mechanism or outcome data, and the trustworthiness of the evidence to warrant changes to configurations or the programme theory.
Inclusion and exclusion criteria for identified literature.
Step 4: Extracting and organising the data
Full text documents were uploaded to Zotero and read thoroughly by KP, who made initial reflective notes regarding content relevance to the programme theory. Documents were then uploaded to NVivo 15 for coding in alphabetical order by first author surname. Coding was both deductive (against preliminary programme theory categories from Step 1) and inductive (for data not fitting existing categories). Codes served as descriptive ‘conceptual buckets’ for evidence gathering (Supplemental material). Codes were refined, merged and reorganised during analysis. Document characteristics were exported from NVivo 15 to Microsoft Excel (Supplemental material), with relevance, trustworthiness and rigour assessed using Wong et al.’s criteria. 56
Step 5. Data analysis and synthesis
Coded data was extracted from NVivo 15 into Microsoft Word files to enable flexible exploration of causal configurations and synthesis narrative development. 57 We applied a realist logic of analysis using ‘context-intervention-mechanism-outcome’ (CIMO) framework, which originated in evidence-based management and design science literature as a means of developing solution-oriented knowledge. 58 We adapted the context-mechanism-outcome (CMO) framework 45 to include intervention components, allowing a clearer distinction between modifiable intervention factors and contextual factors.59–61 Within this framework, we define contextual conditions as the pre-existing social norms, organisational cultures, leadership arrangements, and structural resources that are already present within a given setting in which the intervention operates. These are not easily amenable to change through intervention design alone. Intervention components, by contrast, refer to the elements that are actively introduced, designed, or modified as part of the workplace peer support intervention. We acknowledge that in practice some elements may function simultaneously as enabling contextual conditions and as modifiable intervention components. Data used to construct configurations was drawn from multiple sources, as individual documents rarely contained all the necessary elements. Synthesising information across various texts allowed for greater explanatory power in developing a more complete and robust list of configurations. Quotations directly extracted from the included documents and coded in NVivo were gathered to help clarify and exemplify the configurations, contributing to the depth and coherence of the synthesis.
Discussion with stakeholders and members of the public
A Research Advisory Group was established comprising members of the public, researchers, healthcare assistants, managers and other relevant stakeholders. KP also consulted established Patient and Public Involvement group Marie Curie Research Voices. The groups were consulted during Step 1 and Step 5 to develop programme theory, inform search strategy, suggest additional sources of evidence to complement the formal literature search, contextualise findings and refine emerging insights.
Engagement with substantive theory
As the analysis evolved, we explored a range of substantive theories proposed by stakeholders and found in the literature. Substantive theories are well-established theories from different fields that help explain why phenomena occur the way they do and provide researchers with a theoretical lens to produce insights on social behaviour. 62 There is flexibility in how to use theories in realist reviews, though most commonly they are used to make sense of the patterns found in the data or to provide a framework to help pull together seemingly unrelated findings and increase the explanatory power of programme theories.63,64 In this review we incorporate reference group theory65,66 and community of practice theory67–69 within the results section to substantiate the extrapolations made during the data analysis about contexts, mechanisms and outcomes. 70 We then use self-determination theory71,72 within the discussion section to provide a theoretical framework to bring together and explain the importance of the intervention outcomes.
Results
Search results
In total 1027 articles were identified through database searches, with an additional 18 articles identified from other sources: grey literature and citation searches, stakeholder recommendations, relevant literature known to authors, Google (in incognito mode) searches and library alerts. There were 71 full text articles assessed, with 24 articles included in the review. The screening and selection process is outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram 73 (Figure 1).
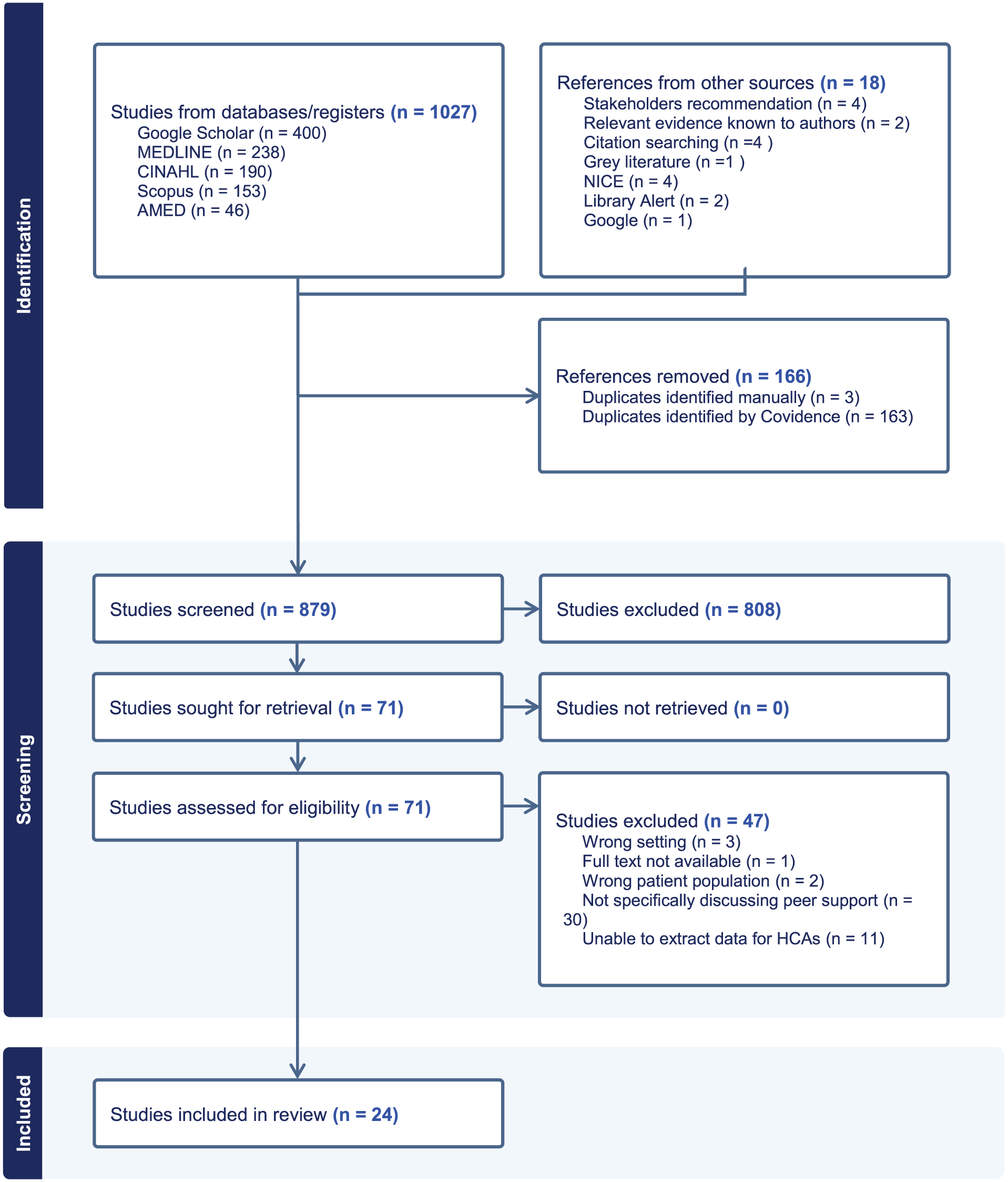
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Overview of included evidence
The literature included in this review reflects the diversity of healthcare system delivery across different countries and encompasses a diverse international body of research focused on healthcare assistants in the context of palliative and end-of-life care at home. Of the included evidence, twelve were qualitative11,12,21,23,27,32,34,74–78, five were quantitative79–83, three were mixed-methods13,22,84, two were reviews.17,20 Studies were conducted across countries such as the UK,11–13,74,80,84 US,21,32,34,77,78,81–83 Canada,22,76 Sweden,23,75,79 and South Africa. 27 These studies explore a range of themes related to peer support and the effectiveness of specific interventions such as COMPASS program34,82,83 and Computer-Mediated Sharing Circles.32,77,78 Included papers contain both published and unpublished work such as theses and project reports, all assessed for their trustworthiness, rigour and relevance to programme theory.56,85 Information on the characteristics of the studies included and mapping of overarching context-intervention-mechanism-outcome configurations to included papers are shown in Supplemental material.
Findings
Findings are presented according to four main outcomes directly influenced by peer support intervention: enhanced wellbeing and resilience, reduced loneliness and isolation, the emergence of a sense of community of practice and strengthened role identity. The intervention itself comprises three interrelated components – peer-facilitated group meetings, informal peer mentorship and 24/7 peer support via chat, calls or text messaging, which operate in combination rather than in isolation (Figure 2). Table 2 presents the twelve Context-Intervention-Mechanism-Outcome (CIMO) configurations, which are detailed causal explanations underpinning the four outcomes. Each outcome is then explored in turn through descriptive narrative and supporting extracts from the included literature.

The three components of workplace peer support intervention for Healthcare Assistants identified in this review. The components operate in combination rather than in isolation, with each contributing to the four workforce outcomes described in the findings.
Context–Intervention–Mechanism–Outcome (CIMO) configurations.
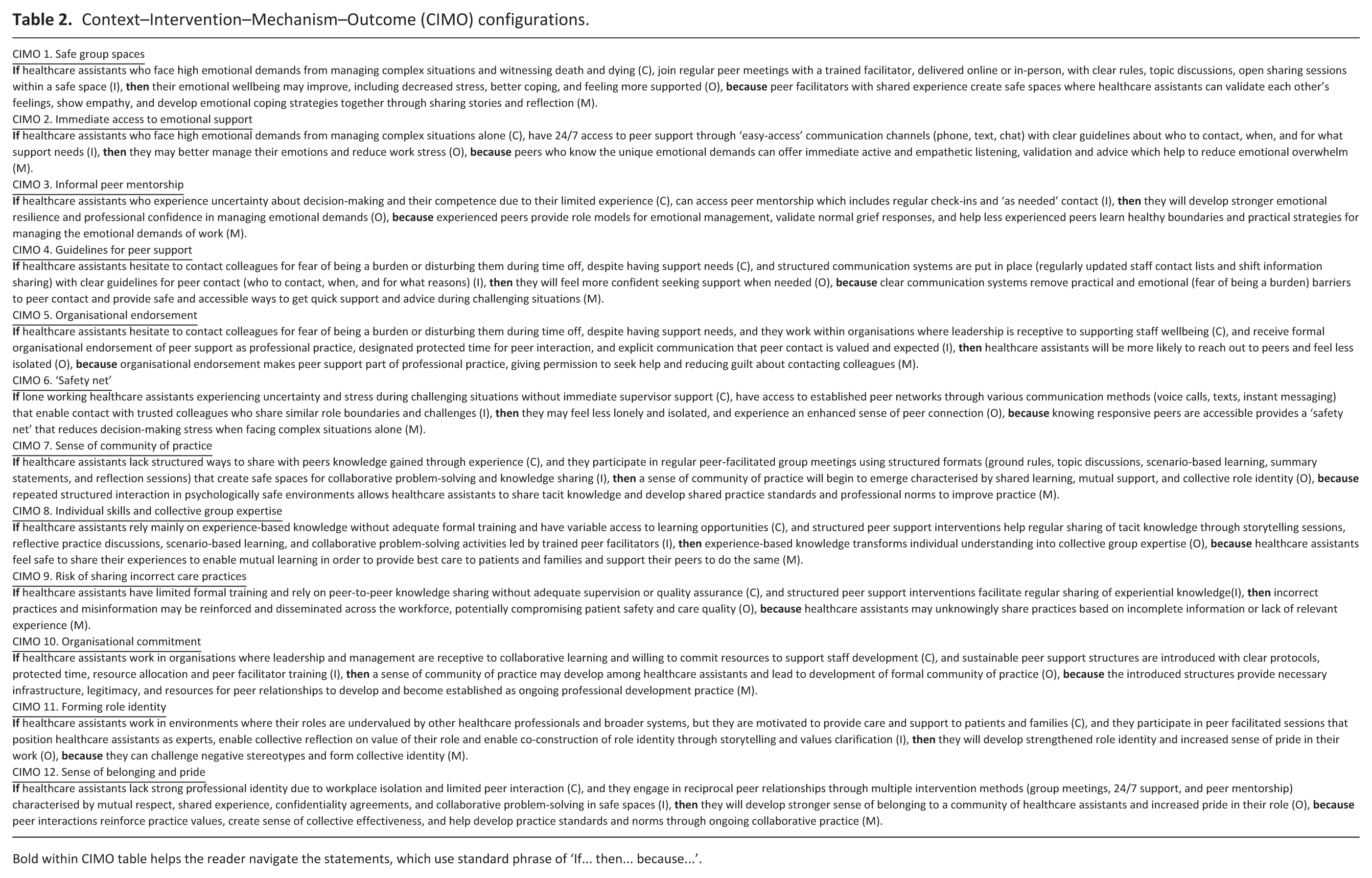
Bold within CIMO table helps the reader navigate the statements, which use standard phrase of ‘If… then… because…’.
Outcome 1. Reciprocal peer emotional support may enhance wellbeing and resilience
This outcome explains how emotional support provided by peers can significantly improve the emotional wellbeing of healthcare assistants, who frequently work in isolation, manage complex needs of patients and families and form close bonds with them, especially in end-of-life care, which can lead to emotional strain, grief, and burnout.17,20,75,86,87
The intervention operates mainly through regular facilitated meetings that provide structured opportunities for collective emotional processing.32,34,77,78,82 However, additional support may be accessed via 24/7 support that enables immediate access to peer assistance during emotionally challenging moments, and informal peer mentorship relationships that develop through ongoing peer interaction, providing sustained emotional guidance and role modelling.11,78,80,86
The group sessions provide opportunities to facilitate safe, confidential, and non-judgemental spaces,32,34 where peers could get to know each other, share their contact details and extend the support outside group settings.11,32,77,78 Group sessions need to be facilitated by a trained peer facilitator to activate reciprocal peer-to-peer emotional support, including validation of feelings, empathy, venting, reassurance, mutual understanding and sharing of coping strategies.11,27,32,34,74,75,78,82,84,86,88 This is because healthcare assistants are more likely to open up and share their emotional burdens with peers who have shared experiences of providing care at home.27,32,78,84 The opportunity to interact with peers helps healthcare assistants regulate their emotions and develop resilience.11,21
The outcomes include subjective improvement in emotional wellbeing such as feeling ‘lighter’, more in control, and more willing to prioritise their own wellbeing,34,82 behavioural changes such as increased help-seeking,34,82,84 ultimately contributing to enhanced resilience and professional confidence in managing the emotional labour of palliative care work.
Data extracts
Kelleher, et al. (2024)
84
By positioning HCWs [homecare workers ] as the ‘experts’, facilitators promoted reflective group discussions, which offered reassurance for many that they were not alone in their struggles
Mabry, et al. (2018)
34
For most, COMPASS provided their first supportive network, a unique “opportunity to open and say things that you never would be saying at other classes” (Adair, June 10, 2015). ‘I had been holding it all in, [but after sharing with my group], I felt good. Sometimes . . . you’re just thinking you’re going to scream, but you cannot scream. I felt that way . . . I felt like I got rid of something. (Olive, May 23, 2015)’
Olson, et al. (2015)
82
Observed well-being and related psychosocial improvements are important for a population that is known to be socially isolated, lacking normal social support structures, and at risk of mental health problems. (. . .) After 6 months, the intervention produced statistically significant improvements in individual-level well-being, as well as small to moderate changes in a wide array of psychosocial, stress, and behavioral outcomes (including safety changes).
Patynowska, et al. (2023)
11
Similarly to previous research,63–65,67–72 sourcing peer support (i.e. support provided by healthcare assistants to other healthcare assistants) was reported as helping to cope with the emotional challenges of practice coupled with a positive impact on the care provided, while enhancing competence, confidence and building participants’ resilience.’
Poon, Luebke, et al. (2023)
32
focus on narrative storytelling enabled participants to address multiple support needs. Sharing common experiences created emotional support through commiseration and empathetic relating. (. . .) HCWs [Home Care Workers] do have a need for emotionally affirming and informational support, and creating accessible online support groups is also relevant as HCWs [Home Care Workers] are geographically distributed and face barriers to meeting peers in-person.
Poon, et al. (2021)
78
peer support was instrumental for HCWs [Home Care Workers] to address challenging aspects of their work, such as the emotional labor of home care and conflicts with patients and other healthcare professionals. Peers provided effective emotional support, helped HCWs [Home Care Workers] regulate their emotions, and refined strategies for performing emotional labor.
Yeh, et al. (2019)
74
In the absence of professional support, informal networks amongst homecare workers had evolved as a way of connecting and supporting each other. Forming supportive bonds with other homecare workers also helped to alleviate some of the loneliness experienced on the job, as well as facilitated knowledge sharing between new and more experienced staff. These networks also provided an outlet for the pressures of care work that occasionally build up
Outcome 2. Accessible peer communication systems may reduce professional isolation
This outcome addresses the persistent issue of loneliness and isolation among community healthcare assistants, who often work alone in unpredictable and emotionally demanding environments.11,17,20,22 The nature of home care, characterised by physical separation from colleagues, limited supervision and irregular communication–can leave healthcare assistants feeling unsupported and reluctant to seek help.12,17,22,23,32,34,74,76,77,80,82,84,87
This intervention component focuses on facilitating communication through practical strategies such as maintaining up-to-date contact lists, promoting norms around peer communication and encouraging a shared understanding of boundaries (i.e. who to contact, when and for what reasons). 80 These measures are essential because many healthcare assistants hesitate to reach out for fear of being a burden or unsure whether it is appropriate to contact a colleague outside of formal channels.11,80 However, for these measures to be successful it requires leadership and workplace culture that is supportive and facilitates such peer contact.32,79,81,84
When these supportive measures are in place healthcare assistants are more likely to initiate contact with peers because they feel reassured that it will be welcomed and supported by both peers and management12,80,84 and because they are motivated to provide best care by sharing tacit knowledge with their peers.27,76,80,84,88
The outcome is a reduction in feelings of loneliness and workplace isolation, and an enhanced sense of peer connection. Healthcare assistants report that even knowing someone is available to contact (via text or call) can alleviate stress, especially during challenging shifts.11,34 These informal support systems are particularly valuable during first solo shifts or emotionally intense situations, where quick access to peer reassurance and advice can make a significant difference.11,17,76
Data extracts
Critchley (2024)
80
[it would be helpful to have] full sight of who is working at the same time as yourself across all teams and levels, we don’t know their number or if they are working.
If they are busy with a patient elsewhere or if they are not working I would be reluctant to contact them on their day off.
I find it easy personally–but not sure everyone feels as confident in asking for peer support from colleagues
Forward, et al. (2024)
17
Homecare workers practice outside of the healthcare structure and yet are expected to work with an increasingly complex client group, often outside of ‘normal’ working hours (with little access to advice from other service workers) and alongside the additional support services which accompany this: “You’re calling and calling. You’re by yourself and no one picks up at the agency. You’re stranded with the client, and you don’t know what to do and you need help. It’s a huge problem.” [38, p5].
Kelleher, et al. (2024)
84
‘Initial buy-in was the key barrier to achieving a higher intervention dose, influenced by agency management, culture and priorities. (. . .) ‘Our findings align with research in care homes, showing that leadership style and how well managers understand, value and engage with an intervention are key to implementation [19].
Mabry, et al. (2018)
34
The work often created on-the-spot exigencies requiring quick thinking. Working alone, HCWs [Home care workers] reported no opportunities to communicate with colleagues to try to determine the optimal response.
Patynowska, et al. (2023)
11
Participants valued the responsiveness and understanding of their peers who had the same responsibilities, role boundaries and similar challenges. Peer support was particularly significant during the first solo shifts when participants felt apprehensive.’
Initially I found it quite anxiety provoking because I have always been with somebody. Even if I’ve been working on my own . . . always been somebody else around. But what I find quite reassuring is that there are other. . . workers on the evening or an overnight and they are a phone call away or a text message away if I need some backup or some guidance so I would refer to them if I’ve got an issue. McPherson, et al. (2019)
22
In contrast, UCPs [unregulated care providers] in the home tend to work independently, and supervision is at a distance. The home setting is also more unpredictable; UCPs [unregulated care providers] in the home, therefore, have to deal with a highly variable and changing working environment. (. . .) UCPs [unregulated care providers] had to deal with issues as they arose. Changes in the client’s condition meant that UCPs [unregulated care providers] had to adapt to changing situations.
Poon, Guerrero, et al. (2023)
77
HCWs are a distributed workforce that usually does not work alongside coworkers or supervisors. Instead, they are in close contact with patients and patients’ families, making HCWs [Home Care Workers] more vulnerable to interpersonal challenges and abuse in the environment of the home [36]. These circumstances result in HCWs [Home Care Workers] feeling isolated and poorly supported in their job, emotionally strained, and unrecognized and unrespected for their expertise and contributions to the healthcare system [85].’
Outcome 3. Facilitated peer meetings may influence development of a sense of community of practice and improve care quality
This section explains how healthcare assistants providing palliative and end-of-life care at home, who report working in isolation and with limited or inconsistent training and workplace support,11,12,22,23,87 can benefit from structured opportunities to connect with peers. These interactions can foster the development of a sense of a community of practice–a group of individuals who share a concern or passion for their work and learn how to do it better through regular interaction.67–69
This intervention component may consist of regular facilitated peer-led meetings delivered in-person and/or online. While healthcare assistants generally demonstrate a preference for in-person interactions,11,32,78 there is broad consensus that online platforms offer greater practical advantages in terms of accessibility and convenience.32,77,78,84 However, online platforms may be missing the backchannel opening–opportunistic relationship building facilitated by in-person meetings.32,34 Peer-led and peer-facilitated models are particularly effective, as they draw on shared lived experience to build credibility and engagement among healthcare assistants.27,77 However, facilitation of such meetings needs to be supported by leadership and managers and embedded in organisational culture as without such support, barriers like staff shortages and lack of protected time can hinder participation and sustainability of the intervention.80,84
Through these regular interactions with peers, who they can identify with due to their shared experience, they develop trust and psychological safety, sense of belonging to the team, grounded in shared motivation to provide best care to patients and their families.27,80,88
The peer-facilitated meetings provide a space for healthcare assistants to exchange tacit knowledge27,32,34,77,78,80,84 and facilitate collaborative problem-solving when healthcare assistants discuss issues from practice and work through potential solutions and learn new skills to use in practice to help improve palliative and end-of-life care provided at home.12,34,83,84 However, without adequate oversight and quality assurance mechanisms, peer knowledge sharing may inadvertently perpetuate poor practices or inaccurate information.11,78,80,87
Due to the opportunities provided by this component of the intervention, building blocks of a community of practice are beginning to emerge.11,32,34,74,78,82,83
Data extracts
Kelleher, et al. (2024)
84
Not only are we benefiting but primarily our people who we’re looking after are benefiting. It is just fabulous, and you can make even more difference to those people and their families with the support that you can offer if we’ve got some more strategies, like we’ve learned from talking to each other. (Agency4, HCW2, Focus Group). Mabry, et al. (2018)
34
In near-unanimity, interviewees extolled the benefits of group brainstorming and problem-solving as “hugely helpful to me in my own work, even [when] the problem wasn’t mine. A lot of the solutions [were] things I wouldn’t have thought of” (Phillipa, May 26, 2015). (. . .) COMPASS’s greatest contribution was opportunity to learn from and share with peers and develop supportive relationships. (. . .) not only demonstrated the value of its group approach but also predicted a longerterm outcome: self-sustained communities of practice.
Misurka, (2016)
76
The participants were unanimous in their goal to provide the best care possible for their clients. As Mary put it, “I’m doing the best job that I can do and working hard, and to me, that’s all I am concerned about.” All of the participants spoke about wanting to do their job well, not only for their client’s benefit but also for their coworkers. As another participant suggested, striving to provide the best care instilled confidence that he was contributing positively to the lives of those he cared for, and at the same time, worked to encourage his coworkers to also strive to do their very best.
Olson, et al. (2016)
83
The intervention produced a statistically significant and sustained improvement in experienced community of practice (6-month d= 0.36; P= .023; 12-month d= 0.37; P= .024). (. . .) The sustained and significant improvement in experienced community of practice is particularly salient given HCWs’ [Home Care Workers] general isolation and lack of workplace social support. If sustained, such professional networks could produce long-lasting benefits for individual workers and home care systems.
Poon, et al. (2021)
78
participants also recognized that not all knowledge shared by HCWs [Home Care Workers] was correct. All of our participants felt that there were a lot of bad practices conducted by other workers, enabled by infrequent and ineffective supervision, lack of communication between HCWs [Home Care Workers], or simply inexperience
Poon, Luebke, et al. (2023)
32
Through this process, HCWs [Home Care Workers] could share informational and emotional support around the experiential and relational aspects of home care work and potentially create discourses that lead to knowing and transformative understanding [31, 70]. (. . .) Besides workplace norms and situations, participants also felt that the sharing circles were valuable for learning about and building efficacy in their work as HCWs [Home Care Workers]. HCWs [Home Care Workers] used the program to give each other advice on proper practice, which could lead to confidence in handling different situations and improved practice. (. . .) Especially valuable for newcomers, HCWs [Home Care Workers] felt more confident in handling potential care situations after hearing the stories of peers and felt that the variety of experiences was particularly valuable to expanding their understanding of the environment and practice of home care. By recreating the environment through storytelling, online professional development programs may be able to teach tacit knowledge even in removed contexts [130].
Outcome 4. Structured peer support and reflective practice may strengthen role identity
This section explains how healthcare assistants, despite working in environments where their roles are often undervalued by other healthcare professionals and broader systems,12,17,20,21,27,32,34,76,78 can still develop a strong role identity and sense of pride in their work through peer support and reflective practice.
Many healthcare assistants are intrinsically driven by a desire to care for patients and their families, finding meaning in emotionally demanding relationships built through their work.21–23,75,87 However, this intrinsic motivation alone is insufficient for developing a robust role identity, especially when healthcare assistants are isolated from peers in similar roles.11,12,17,22,23,32,74,77
Structured peer support interventions delivered through both online and in-person facilitated sessions create opportunities for healthcare assistants to connect with peers who share similar experiences.27,32,78,84 These sessions facilitate relationship-building,11,32,77 sharing meaningful care stories and collective reflection on their roles.32,34,77 Through this process, healthcare assistants are able to articulate the value of their work, receive affirmation and validation from peers, and co-construct a shared understanding of their role identity.27,32,77 Reciprocity between peers and ability to share in confidential and safe space are important to enable such processes.77,88
These mechanisms are supported by
Healthcare assistants reframe their work as skilled and essential, challenge negative stereotypes and assert role boundaries. 78 This process strengthens their confidence and pride and contributes to the development of a cohesive role identity.32,78,84
Ultimately, even in the absence of systemic recognition, peer support intervention may enable healthcare assistants to feel valued and empowered in their roles.
Data extracts
Franzosa et al. (2019)
21
When aides felt seen and respected by clients, supervisors, and clients’ families, they were better able to manage day-to-day challenges. But when they were not, the work “took a toll,” leaving them exhausted, stressed, and even considering leaving the job. Kelleher et al. (2024)
83
Participants reported increased confidence in their skills, with some feeling empowered to advocate for change. (. . .) Kupa and Geyer (2020)
27
Home-based care workers (HBCWs), like other healthcare practitioners, found themselves working with the most challenging health problems, in circumstances where poverty and hopelessness are prevalent. The potential for demotivation is high given the fact that often there is little recognition for the work they do. (. . .) The programme was facilitated through group work methods that are specific to working with adults and allowed HBCWs [Home-based care workers] to openly share their views of reality and challenge with one another and in the process gain new insights, develop a group identity and achieve mutual understanding over time.’ (. . .) ‘participants found their work stimulating, and contributing in some ways to personal or professional growth and fulfilment. Misurka (2016)
76
When relationships with members of the larger care team were poor and unsupportive, the participants felt as if they were not as valuable, leading to feel that they were not really a part of the same team. Peter summarized how he and his fellow care aides felt when he said: It’s the home care workers – very, very dedicated to what they are doing. They want to work. They want to be treated fairly and they want to make sure that somebody out there is really. . .I think that what they really want is to be supported. To be given the chance to be on the team that you say we are supposed to be on. They do not feel like they are a part of anybody’s team.’ Poon, Luebke et al. (2023)
32
The support group allowed HCWs [Home Care Workers] to speak on and raise awareness around common job-related problems and grievances. Because their audience was other HCWs[Home Care Workers], for whom this information was very relevant, participants felt like they had an effective “voice” in the support program. One participant described that it was important to have this voice in the sharing circles due to a lack of it in the workplace. (. . .) hearing stories of similar experiences also helped create common ground between participants, reinforced this shared identity, and may help create a community that can advocate for and create praxes that contest experiences of marginalization and works towards shared interests. Poon et al. (2021)
78
HCWs [Home Care Workers] also faced negative perceptions of their work as unskilled or domestic, and in response, peers worked to strategically frame HCW [Home Care Workers] practice as skilled and essential by cultivating a body of expertise, setting norms around practice, and encouraging HCWs [Home Care Workers] to stand up to pressure to do work that was outside their job description. (. . .) HCWs [Home Care Workers] engaged in several actions targeted at peers to strategically define the scope of their work and promote the perception of it as a skilled and specialized practice.
Initial programme theory
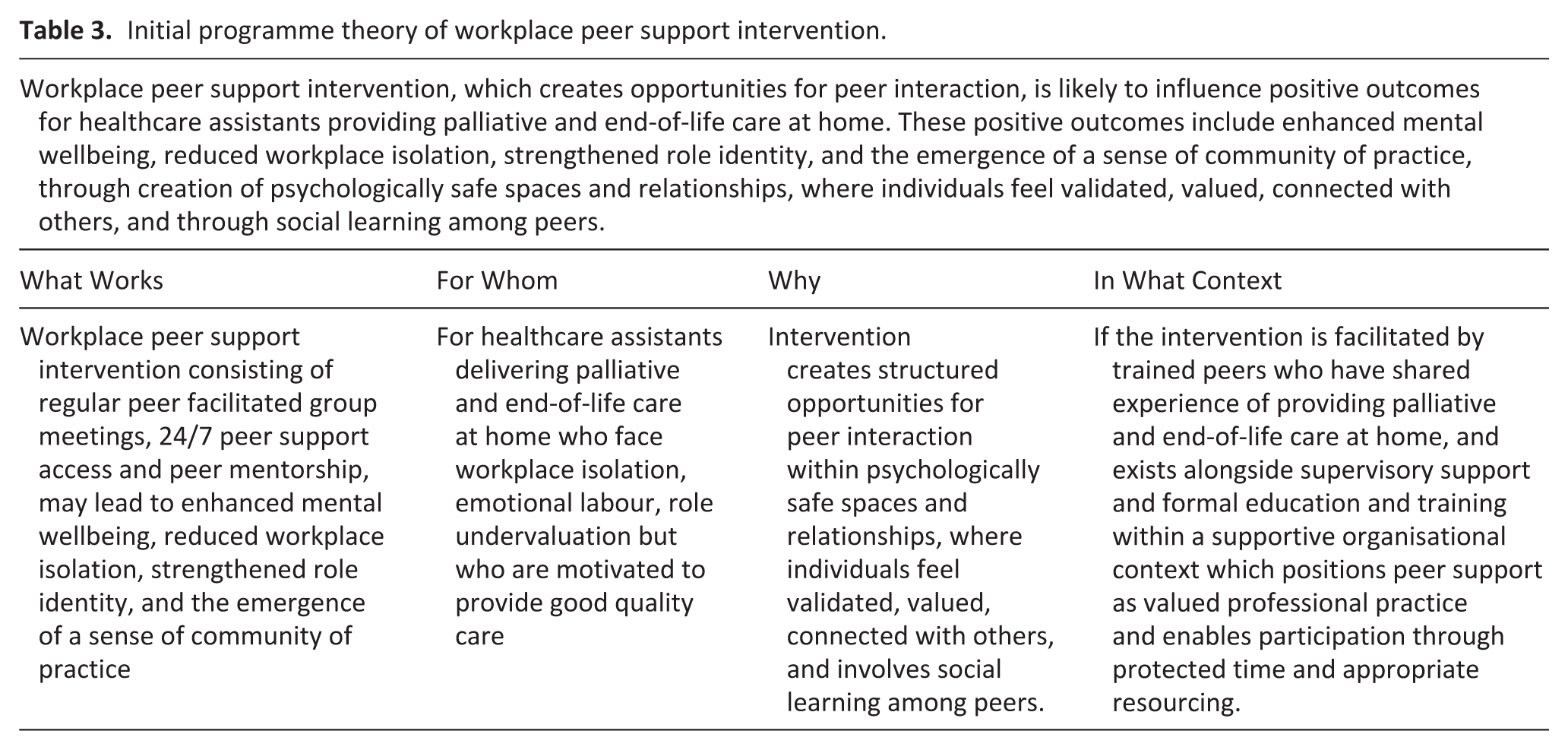
The initial programme theory (Table 3) developed following literature synthesis demonstrates that peer support creates a complex adaptive system where healthcare assistants develop capacity to manage the emotional and practical challenges of delivering palliative and end-of-life care in unpredictable home environments. The reciprocal nature of peer support creates self-sustaining networks that become increasingly independent of external facilitation as participants develop stronger peer relationships and enhanced confidence in supporting colleagues. The realisation of these outcomes is dependent on a set of organisational enabling conditions, including leadership receptiveness to supporting staff wellbeing, endorsement of peer support as valued professional practice, allocation of protected time for participation and resourcing of peer facilitator training. Without these conditions, the mechanisms identified in this review are unlikely to be fully activated. This theory will be further refined during realist evaluation forming the next stage of this research.
Initial programme theory of workplace peer support intervention.
Across the four outcomes, recurring patterns suggested that workplace peer support may operate by addressing three fundamental psychological needs of competence, autonomy and relatedness, which we interpret through
Discussion
Healthcare assistants are an essential but often undervalued workforce in palliative and end-of-life care, facing significant challenges including emotional labour, loneliness and isolation, with inconsistent access to workplace training, managerial and peer support.11,20,25,38 This realist review demonstrates that peer support interventions are limited and inconsistent, yet workplace support among peers may improve wellbeing, reduce isolation and loneliness, influence development of a sense of community of practice and strengthen role identity. The realist approach proved valuable in uncovering causal mechanisms activated in response to intervention elements within specific contexts, that influence observed outcomes, presented as an initial programme theory (see Table 3).
Building on the patterns identified in the results, our findings suggest that workplace peer support may address three basic psychological needs proposed by self-determination theory: competence, autonomy and relatedness.71,72 As outlined in our methods, we apply this theoretical framework to increase the explanatory power of our programme theory. Enhanced wellbeing and resilience, and the emergence of a sense of community of practice, relate primarily to the need for competence developed through tacit knowledge exchange, collaborative problem-solving and the building of both practical and emotional skills. Reduced loneliness and isolation connect to the need for autonomy supported through structured communication systems that provide healthcare assistants with choice in how, when, and from whom they access support. All four outcomes, and particularly strengthened role identity and the sense of community of practice, address the need for relatedness fulfilled through psychologically safe peer connections, reciprocal support and the development of shared professional identity. These connections are explored in detail below.
Enhancing competence
Ryan and Deci 89 describe competence as feeling effective, skilled, and capable of achieving desired outcomes. Previous research demonstrates that healthcare assistants frequently experience inadequate preparation for their roles and inconsistent access to training and education opportunities,90–92 resulting in diminished confidence regarding their competence. 11 Workplace peer support interventions address healthcare assistants’ need for feeling competent through tacit knowledge exchange, reflection and collaborative problem solving, potentially fostering the development of both practical and emotional competence. Interactions between peers allow them to benchmark their practice and identify knowledge and skill gaps that can be addressed through collective expertise. However, peer knowledge sharing must be balanced with appropriate quality assurance mechanisms to prevent the inadvertent reinforcement of substandard practices or misinformation. This suggests that competence-building through peer support requires careful balance between leveraging experiential knowledge and maintaining quality assurance. Potential safeguards may include periodic oversight from registered professionals to review content shared during peer sessions, positioning peer support as complementary to rather than a substitute for formal training and education and establishing clear pathways for escalating clinical queries beyond peer expertise. However, the current evidence base offers limited guidance on specific mitigation strategies for this workforce, and further investigation is needed to determine how best to safeguard the quality of peer knowledge sharing in practice.
Beyond practical skills development, peer support interventions also facilitate the development of emotional competence – an ability to effectively manage and respond to emotions in social situations in ways that align with personal values and support healthy relationships. 93 Emotional competence encompasses a set of skills that can be systematically nurtured and developed. 94 Such skills include recognising and managing personal emotional responses to death and suffering, understanding how emotions function and are communicated interpersonally and developing empathic engagement with others’ emotional experiences. 93 Each of these skills represents a vital component of healthcare assistants’ work in palliative and end-of-life care settings and can potentially be enhanced through structured workplace peer support interventions, which facilitate social learning among peers.
The parallel development of practical and emotional competence through peer support intervention is important. Inadequate competence in either domain can directly compromise the quality and safety of care provided to patients and families, underscoring the importance of well-designed peer support systems that enhance competence while maintaining appropriate safeguards.
Supporting autonomy
The psychological need for autonomy is satisfied when individuals feel they have volition and are self-directed in their actions rather than externally controlled. 89 Healthcare assistants’ work presents a unique autonomy paradox. While working in patients’ homes provides inherent independence, healthcare assistants must simultaneously operate under the supervision of registered professionals, adhere to prescribed care plans and defined scopes of practice.90,95,96 Evidence indicates that many individuals are drawn to this work specifically because it offers a degree of control and autonomy, 97 highlighting the importance of understanding how workplace peer support interventions can facilitate the fulfilment of this psychological need.
Structured communication systems with clear guidelines that provide options and choice are essential for overcoming practical barriers to peer support. Such interventions should include clear protocols for peer contact and accessible communication channels, enabling healthcare assistants to maintain control over how, when and from whom they seek support. Previous research demonstrates that multiple support options are required, where peer support complements managerial supervision and reflective practice groups. 98 Mixed delivery modes of peer support are also needed to maximise opportunities for participation. 99
Research among home care workers indicates that experiencing autonomy in their role may contribute to higher job satisfaction and lower intention to leave.100–102 Therefore, when implementing workplace peer support systems, careful consideration must be given to ensuring that workers experience autonomy when accessing support systems.
Fostering relatedness
Relatedness is conceptualised by Ryan and Deci 89 as the need to feel connected to others and experience a sense of belonging and meaningful relationships. Our findings demonstrate that healthcare assistants have a fundamental need for connection with peers. However, they often experience loneliness, defined as distress from a perceived lack of quality workplace relationships, 103 which is associated with lower job performance and reduced wellbeing across various sectors. 104 Healthcare assistants face unique emotional and practical demands that are often difficult for others to fully understand, making peer connections particularly valuable.
Our review findings indicate that workplace peer support interventions address this need by creating psychologically safe spaces – environments that enhance employee performance, learning and work experience. 105 These safe spaces are characterised by confidentiality, non-judgemental attitudes, mutual respect and a collective willingness to provide support to colleagues. These characteristics enable healthcare assistants to experience authentic connections necessary for satisfying their relatedness needs. Within such environments, reciprocal emotional support develops when healthcare assistants recognise that their peers genuinely understand their distinctive emotional demands.
The reciprocal nature of peer support is particularly significant for meeting relatedness needs. Healthcare assistants serve not only as passive recipients of support but as active contributors, creating relationships that enhance their sense of connection and create a sense of belonging to a community of practice. This mutuality distinguishes peer support from other forms of workplace support and strengthens the relationships between workers. Additionally, research shows that the healthcare worker groups with lower status may experience reduced psychological safety, 106 potentially explaining why peer facilitation which removes hierarchical differences proves particularly favourable.
Summary
Research by Deci et al. 107 demonstrates that satisfaction of competence, autonomy and relatedness needs results in higher employee wellbeing and better work performance. Building upon this theoretical foundation, our findings suggest that workplace peer support interventions may address these fundamental psychological needs among healthcare assistants, potentially contributing to improved care quality and workforce sustainability. However, the current evidence base requires strengthening to establish definitive causal relationships between peer support interventions, satisfaction of psychological needs, and broader organisational outcomes.
Implications for practice, policy and research
Workplace peer support represents a potentially sustainable intervention model that leverages existing workforce expertise while minimising reliance on external resources. The reciprocal nature of peer support may create a model for a self-sustaining intervention that becomes increasingly independent of external facilitation as healthcare assistants develop stronger peer networks and enhanced confidence in supporting colleagues.
Organisations that wish to implement workplace peer support interventions could test the initial programme theory identified in this realist review of the literature following key design principles: embed interventions within supportive organisational contexts, offer multiple modalities for diverse working environments and position peer support as valued practice.
The programme theory of what works, for whom, and in what circumstances from this realist review provides a foundation for future research to develop an evidence-informed peer support intervention. Future research should also prioritise investigating existing workplace peer mentorship models, strategies for addressing potential poor practice sharing and long-term impacts on workforce retention and care outcomes.
Strengths and limitations
The limited number of included studies may restrict programme theory development. The evidence base was predominantly dependent on self-reported outcomes with limited intervention studies and no long-term follow-up studies to evaluate sustained impacts on workforce retention or patient outcomes. Potential publication bias exists as searches were limited to English-language publications. There was insufficient data to fully understand the links with staff retention and quality of care.
This review followed established frameworks and standards for realist reviews.42,43,52 Comprehensive search strategies accessed international evidence using a broad definition of healthcare assistants that acknowledged global variations in roles and titles. The inclusion of grey literature and stakeholder involvement throughout the review process enhanced the breadth and contextual relevance of findings. The review addresses an important evidence gap in an increasingly critical area of healthcare delivery, and provides a robust foundation for future intervention design and development. Integration with substantive theories enhanced explanatory power beyond the empirical findings alone.
Conclusion
This realist review has developed an initial programme theory explaining how workplace peer support interventions may strengthen healthcare assistants’ capacity to deliver palliative and end-of-life care at home. Using self-determination theory as an explanatory framework, we demonstrate that effective peer support may meet three basic psychological needs: enhancing competence via knowledge sharing, supporting autonomy through choice in accessing support and fostering relatedness through psychologically safe peer connections. The programme theory reveals that peer support functions as a complex adaptive system, which may address core workforce challenges including emotional labour, professional isolation and role undervaluation, while potentially improving care quality and workforce sustainability. The reciprocal nature of peer support offers promise for resource-constrained healthcare systems, potentially creating self-sustaining networks that leverage existing workforce expertise. However, the initial programme theory requires further empirical testing through realist evaluation to establish generalisability and refine implementation strategies across diverse healthcare contexts.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163261455213 – Supplemental material for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review
Supplemental material, sj-docx-1-pmj-10.1177_02692163261455213 for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review by Katarzyna A. Patynowska, Felicity Hasson, Tracey McConnell and Sonja McIlfatrick in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163261455213 – Supplemental material for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review
Supplemental material, sj-docx-2-pmj-10.1177_02692163261455213 for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review by Katarzyna A. Patynowska, Felicity Hasson, Tracey McConnell and Sonja McIlfatrick in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_02692163261455213 – Supplemental material for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review
Supplemental material, sj-docx-3-pmj-10.1177_02692163261455213 for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review by Katarzyna A. Patynowska, Felicity Hasson, Tracey McConnell and Sonja McIlfatrick in Palliative Medicine
Supplemental Material
sj-docx-4-pmj-10.1177_02692163261455213 – Supplemental material for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review
Supplemental material, sj-docx-4-pmj-10.1177_02692163261455213 for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review by Katarzyna A. Patynowska, Felicity Hasson, Tracey McConnell and Sonja McIlfatrick in Palliative Medicine
Supplemental Material
sj-docx-5-pmj-10.1177_02692163261455213 – Supplemental material for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review
Supplemental material, sj-docx-5-pmj-10.1177_02692163261455213 for Understanding workplace peer support among healthcare assistants providing palliative and end-of-life care at home: A realist review by Katarzyna A. Patynowska, Felicity Hasson, Tracey McConnell and Sonja McIlfatrick in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank the members of the Research Advisory Group and the Marie Curie Research Voices Patient and Public Involvement group for their valuable contributions to this review.
Ethical considerations
Formal ethical approval is not necessary for this review.
Author contributions
All authors made contributions to the design of this protocol (KP, FH, TM, SM). KP wrote the original draft of the article with input from all authors. All authors reviewed, edited and/or commented on drafts of the manuscript and approved the final version for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by HSC R&D Division, Public Health Agency [EAT/5776/24].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this realist review are available from the corresponding author, Katarzyna A. Patynowska (
Disclaimer
The content or views expressed are those of the authors and do not necessarily reflect the official views of the HSC R&D Division.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.