
Abstract
Terrorist acts have an enormous potential to produce trauma, especially in vulnerable groups such as children and adolescents. However, few studies have analysed the potentially adverse effects of terrorism on child victims. The present article systematically reviews the literature on the psychological consequences which exposure to acts of terrorism can have for children. A total of 54 publications were reviewed, the majority originating from the USA (72.22%) and linked to the 9/11 attacks in New York (50%). Most of the studies analysed post-traumatic symptoms (64.81%) in children who were indirect victims through exposure to media reports about the attack (33.33%). There is a need for trained professionals to work with child victims of terrorism; they must be able to recognize the symptoms associated with these experiences, as well as the damaging effects they may have on children.
From the perspective of victimology, acts of terrorism can be considered as a form of interpersonal victimization, one that has an enormous potential to produce trauma owing to the interaction between various aspects of the experience, i.e. its malevolence, the feeling of having been betrayed by another human being, the very injustice of the act, and the fact that it goes against socially established norms (i.e. it is immoral) (Finkelhor, 2007).
With this in mind the aim of the present study was to conduct a critical analysis of published studies concerning the psychological effects which acts of terrorism may, directly or indirectly, have on children. Although a number of theoretical reviews have been published in English on war, terrorism and political violence (notably the recent paper by Comer and Kendall, 2007), there has been no systematic review focused exclusively on the possible effects that terrorism can have on children. Thus, the aim of this review is presenting the main results of published studies in this frequently neglected area, hence becoming a useful contribution to the field of children and terrorist violence.
Terrorism, violence and their effects on victims
Terrorism shares certain characteristics with other forms of interpersonal violence such as acts of war or assaults, and in fact much of our knowledge about the effects of terrorism comes from studies of those events. However, terrorist acts are more unpredictable and episodic, and imply an undefined threat. Furthermore, they have a profound and lasting effect on the community as they are the manifestation of an ideological conviction that violence can and should be used to threaten and intimidate a much larger group than that which is directly affected (Shaw, 2003). The choice of victims is another distinctive element, and forms part of the terrorist tactic. Indeed, the aim is rarely the act in itself, but rather to terrorize and intimidate the population as far as possible (Comer and Kendall, 2007; Yehuda and Hyman, 2005), creating a climate of fear, uncertainty and vulnerability, mainly through the dimension of communication or propaganda (De la Corte et al., 2008; Silke, 2005).
Terrorists tend to use violence as a way of influencing, persuading or intimidating, and seek to have an effect beyond those who are directly affected. Indeed, victims can be chosen for their propaganda value, whether this be their relevance within the social group that is the target of the terrorist act (focused terrorism), or precisely because they have no direct relationship with that group’s interests (indiscriminate terrorism). Terrorists frequently use non-conventional military tactics such as sneak attacks or the specific choice of innocent targets, such as children. It should also be noted that the members of terrorist groups usually show absolute loyalty to their organization, which leads them to avoid considering the consequences of their acts and to justify them as necessary (Hills, 2002).
In terms of victimology, terrorism combines two threats to the individual which produce deep feelings of insecurity and terror, and it is these threats that distinguish terrorism from other acts of interpersonal violence. Terrorism is both an act of intentional violence against the community, with all the harm that this can cause, and also an example of random violence, something unexpected that could happen at any time, and which could therefore affect oneself and one’s family (Pine et al., 2005). As a result, both those who are physically present in the attack and the wider community in which it occurs become victims of terror. Given this, it has been argued that terrorist acts are the purest way of producing trauma, as they combine the perception among victims of malevolent intent with the threat or real existence of extreme physical and/or psychological harm. Consequently, victims develop a genuine fear of the future, and the basic human assumption of safety is violated (Echeburúa et al., 1998).
Comer and Kendall (2007) consider the different ways in which children and adolescents may be exposed to terrorism. Direct exposure is when they are the actual victims of a terrorist attack or live in an area where such acts occur. Interpersonal exposure refers to the loss of a loved one or acquaintance in an attack, what Baca et al. (2003) refer to as the victim’s relatives. Exposure may also occur through the media, whereby children witness terrorist acts and their devastating consequences by watching television, etc. Finally, there is exposure to the climate of threat, expectation and the state of alert (sometimes referred to as second-hand terrorism) that these acts produce within the child’s community, school and family, and which may generate or exacerbate a wide range of psychological problems and hinder the child’s development.
The direct exposure of children to a terrorist attack produces terror and confusion and disturbs the daily routines and stability that are essential for their development. Indeed, children who have been directly exposed to terrorism are at very high risk of developing various psychological disorders (Comer and Kendall, 2007). It should be noted, however, that even if children were not present during the actual attack, the unexpected death of a loved one (especially one of their main carers) as a result of a terrorist act can have an enormous emotional impact. This may then trigger a pathological mourning process or lead to various disorders, mainly those related to a depressed mood and symptoms of anxiety, although it can also take the form of confrontational and disruptive behaviour, or externalizing behaviour problems, especially among boys. These gender differences in internalizing and externalizing symptoms have been demonstrated in studies of developmental psychopathology with community samples (Leadbeter et al., 1999), and child and adolescent victims of trauma (Pine and Cohen, 2002).
All these kinds of disturbances can have serious long-term consequences (Dowdney, 2000). It is therefore important to analyse the impact that traumatic events may have on children, whether this be via the mass media or through the indirect influence of the event’s effect on their family and community. Indeed, what has been referred to as distant trauma may generate the same adverse symptoms as a directly experienced trauma (Terr et al., 1999).
Following the 9/11 attacks on the World Trade Centre in New York there developed a wider interest in acts of terrorist violence and their effect on children, one which has gone beyond classical studies of the effects of family violence on a child (Prinz and Feerick, 2003). Nevertheless, this remains a new focus of research and relatively few studies have been published in this regard.
The process of selection and coding of the studies
(a) Selection of studies
The principal criterion for selection was journal articles (not doctoral theses or book chapters) that described an empirical study of the psychological consequences of terrorism for children who have been the direct or indirect victims of an attack. The search was conducted via the most relevant databases in the field of health sciences (Medline, Scopus, Psycinfo of the Web of Science) and used the following search terms: (terrorism) AND (baby OR childhood OR child OR children OR infancy OR infant OR toddler OR adolescence OR adolescent OR youth OR teenager OR youngster OR minor) AND (victimization OR victimology OR victim OR violence) AND (consequences OR effects). The SciELO database and any relevant publications included in Latindex were also reviewed. As a complement to the above the reference lists of previously published reviews, such as those of Comer and Kendall (2007) and Freemont (2004), were examined in order to locate any other relevant papers not already included. Articles were excluded if their abstract did not include the established review topics, or if they only made reference to topics that were related but not directly linked to the focus of the present review − for example, the consequences of war, community violence or refugee children.
Following the initial search (which yielded 267 potential publications), any duplicate or irrelevant papers were eliminated, leaving a total of 104 abstracts to be read. This process resulted in 54 articles being included in the review.
(b) Coding of studies
The articles were coded according to a series of variables related to the study characteristics, design and methodology: (a) year of publication; (b) country in which the study was conducted; (c) number of participants; (d) whether the study was descriptive only or included a comparison/control group; (e) informant (parent, child, other); (f) method used to assess the child (questionnaire, interview, etc.); and (g) time of assessment (days, months, years after the attack). Variables related to the children and the terrorist act were also coded: (a) sex of the participating children (boys, girls, both); (b) range or mean age of the sample (in years); (c) ethnic group of the participants; (d) type of victimization (direct, interpersonal or indirect, i.e. via the media or second-hand terrorism); and (e) description of the terrorist attack. Finally, the analysis considered the psychological consequences that were assessed and which were associated with the terrorist act (e.g. post-traumatic stress disorder, depression, behavioural problems).
The studies included
Table 1 lists the 54 empirical studies on the psychological consequences of terrorism for children, the large majority of which (72.22%) were conducted in the USA, followed at a considerable distance by Israel (20.37%). The sample size differed widely among studies, ranging from 22 to 8,236 participants (M = 952.52, SD = 1532.03).
Descriptive summary of the studies reviewed.
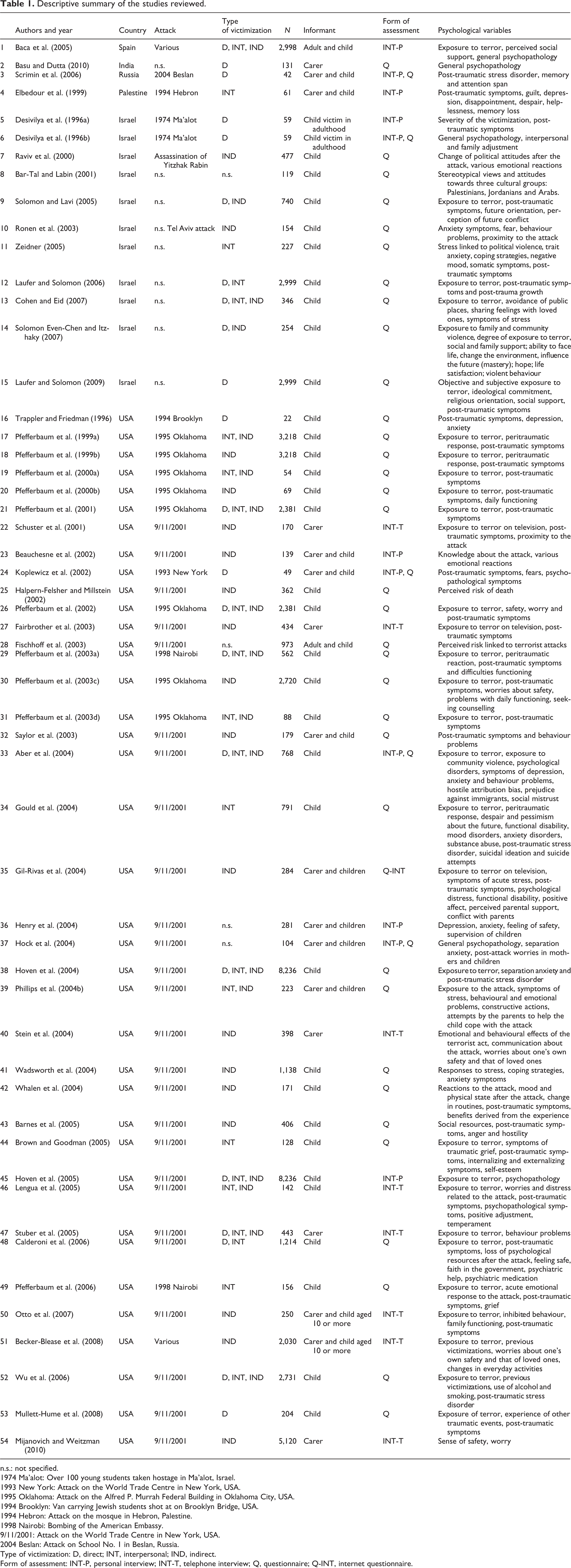
n.s.: not specified.
1974 Ma’alot: Over 100 young students taken hostage in Ma’alot, Israel.
1993 New York: Attack on the World Trade Centre in New York, USA.
1995 Oklahoma: Attack on the Alfred P. Murrah Federal Building in Oklahoma City, USA.
1994 Brooklyn: Van carrying Jewish students shot at on Brooklyn Bridge, USA.
1994 Hebron: Attack on the mosque in Hebron, Palestine.
1998 Nairobi: Bombing of the American Embassy.
9/11/2001: Attack on the World Trade Centre in New York, USA.
2004 Beslan: Attack on School No. 1 in Beslan, Russia.
Type of victimization: D, direct; INT, interpersonal; IND, indirect.
Form of assessment: INT-P, personal interview; INT-T, telephone interview; Q, questionnaire; Q-INT, internet questionnaire.
The act of terrorism that featured most frequently in the studies was the 9/11 attack on the World Trade Centre in New York in 2001 (50.00%), followed by the 1995 attack on the Alfred P. Murrah Federal Building in Oklahoma City (14.81%). In the majority of cases the children analysed were indirect victims, through exposure to information about the attack in the media (33.33%). However, some studies were conducted with direct victims, i.e. children who were actually present during the attack (14.81%), or those who had been the victim of interpersonal terrorism through the death of a loved one or acquaintance (7.41%). The point at which the study was carried out varied widely, from two days after the attack (e.g. Bar-Tal and Labin, 2001) to 17 years later (Desivilya et al., 1996a, 1996b).
Except for one study that focused exclusively on boys (Trappler and Friedman, 1996), the children analysed were of both sexes, and in comparable proportions. Most of the study samples involved children aged ten or over, although in one study (Basu and Dutta, 2010) children as young as one and a half years were included. Overall, the studies cover a range of ethnic groups, owing principally to the demographics of the country in which they were conducted, although participants were most commonly Caucasian (42.59%), with the remainder being distributed among a number of ethnic and religious groups (for example, Jews, Sephardic Jews, Arabs, Muslims, Hindus, Africans, Afro-Americans, Latinos and Asian-Americans: 37.04%). Ethnicity was not recorded in 20.37% of the studies reviewed.
The assessment was mainly based on the children themselves (64.81%), followed by a multi-informant method involving both children and parents (22.22%). The most widely used instruments for obtaining this information were pencil-and-paper questionnaires (62.96%) and interviews (25.92%). There were only five cases in which both these techniques were used (9.26%). One study involved the use of an online questionnaire (1.85%). In addition to evaluating the extent to which the child had been exposed to the terrorist attack (59.25%), the most common psychological variable analysed was symptoms of post-traumatic stress (64.81%), followed by other general psychological disorders (11.11%).
Results of the review
This article presents a systematic review of the literature on the psychosocial impact of terrorism on children, doing so from the perspective of developmental victimology − the comprehensive study of childhood victimization (Finkelhor, 2007).
In general, the children analysed were most likely to present internalizing symptoms, principally those characteristic of post-traumatic stress disorder. It should be noted, however, that this finding could be due to the fact that this is also the kind of symptomatology which is most often assessed (Comer and Kendall, 2007). On a broader spectrum the children also reported symptoms of depression, generalized anxiety, separation anxiety and agoraphobia (Hock et al., 2004; Hoven et al., 2004, 2005). Only a few studies (e.g. Hoven et al., 2005; Lengua et al., 2005; Wu et al., 2006) examined the presence of externalizing symptoms, such as behavioural disorders or substance abuse, among child victims of terrorism, and this prevents any reliable conclusions from being drawn in this regard. With respect to the overall prevalence of psychological disorders, both internalizing and externalizing, victims of terrorism present more symptoms on all the problems assessed when compared with matched controls, i.e. children with similar sociodemographic characteristics who have not been victims of terrorism (Basu and Dutta, 2010; Desivilya et al., 1996a, 1996b).
Gender differences showed that girls present more internalizing symptoms and disorders (in North American samples: Hoven et al., 2004, 2005; Pfefferbaum et al., 2003a; Stein et al., 2004; but also in Israeli and Palestinian studies: Cohen and Eid, 2007; Elbedour et al., 1999; Laufer and Solomon, 2009; Raviv et al., 2000; Zeidner, 2005), while boys develop more behavioural disorders (Hoven et al., 2005; Lengua et al., 2005), hostility (Elbedour et al., 1999) and impulsivity (Wadsworth et al., 2004), although these differences were not found in all the studies (Phillips et al., 2004b; Ronen et al., 2003).
Most of the papers reviewed focused on assessing disorders that are included in clinical manuals, especially post-traumatic stress disorder (Hoven et al., 2009), and avoided carrying out a broader analysis of the psychological consequences of terrorism for children (Comer and Kendall, 2007; Pfefferbaum et al., 2005). Indeed, very few studies have considered this broader perspective, although those that have (e.g. Hoven et al., 2005) have shown that child victims of terrorism present a high prevalence of various psychological difficulties, not simply those included in classical assessment manuals; examples of such difficulties include functioning at home and problems with the peer group or at school (e.g. Pfefferbaum et al., 2003d).
In light of the above it is necessary to distinguish between pathological reactions to a terrorist act and what could be considered a normal response to an abnormal event (Pynoos et al., 1999). This requires that any assessment takes into account not only symptomatology but also the extent to which the child’s usual functioning is affected in all his or her developmental contexts (La Greca, 2007). Indeed, children can present a range of normal reactions to an act of terrorist violence (see Joshi and Lewin, 2004; Williams, 2007), and these should not be confused with psychopathological problems because, in the majority of cases, the children will recover from their exposure to terror once they have had enough time to readapt. In fact, those studies that do assess the effects on children’s everyday functioning conclude that, in most cases, and depending on certain factors that will be discussed below, the impact of terror is minimal, transitory and does not become generalized (Pfefferbaum et al., 2003a, 2003b).
(a) Consequences of exposure to terrorism through the mass media
Research has demonstrated a dose-response effect on children who have been exposed to terrorism, i.e. the greater the child’s direct experience of the attack the greater the symptomatology, whether internalizing (e.g. Baca et al., 2005; Hoven et al., 2004; Koplewicz et al., 2002; Lengua et al., 2005; Pine et al., 2005) or externalizing (Solomon Even-Chen and Itzhaky, 2007; Wu et al., 2006). However, one of the limitations of this research is that most of the studies describe the psychological consequences in children who have been indirect victims, through media exposure, to material concerning a terrorist attack (Pfefferbaum et al., 2005). Nonetheless, and as Pfefferbaum and co-workers point out (2003b), it is worthwhile investigating the effects on children of indirect exposure to terrorism because one of the objectives of terrorist violence is to provoke fear within the wider community.
Children are clearly affected by the images they see in the media following an act of terrorism, and this accounts for the emotional distress reported by children and adolescents who were physically distant from the actual attack (e.g. Fairbrother et al., 2003; Gil-Rivas et al., 2004; Mijanovich and Weitzman, 2010; Pfefferbaum et al., 2000b, 2001, 2003d; Schuster et al., 2001). Studies of children who have been indirect victims of terrorism have found symptoms of post-traumatic stress, anxiety, sadness, isolation and general psychological distress (e.g. Barnes et al., 2005; Fairbrother et al., 2003; Gil-Rivas et al., 2004; Hock et al, 2004; Lengua et al., 2005; Mijanovich and Weitzman, 2010; Otto et al., 2007; Pfefferbaum, 2003d; Schuster et al., 2001; Stein et al., 2004; Whalen et al., 2004), as well as a tendency to see the world as a more dangerous place (Halpern-Felsher and Millstein, 2002; Phillips et al., 2004b), an altered view of the future (Fairbrother et al., 2003) and a heightened sense of the risk of death (Halpern-Felsher and Millstein, 2002), concern for one’s own safety and changes in everyday activities (Becker-Blease et al., 2008; Pfefferbaum et al., 2003c), and problems of an externalizing nature (Lengua et al., 2005).
Furthermore, exposure of children who were directly affected by an attack to subsequent news reports about it can lead to a serious deterioration in their emotional state. These children are more likely to suffer post-traumatic symptoms, mainly of the intrusive kind such as nightmares or recurrent flashbacks (Pfefferbaum et al., 2001); this was the case following the bomb at the Alfred P. Murrah Federal Building in Oklahoma City in 1995 (Pfefferbaum et al., 1999a, 2000a, 2003d) and after the 9/11 attacks on the World Trade Centre in New York in 2001 (Saylor et al., 2003).
According to the study by Saylor et al. (2003), in which the parents of primary school children were asked about the degree to which their sons and daughters had been exposed, either via the internet or on television, to explicit images of the 9/11 attacks (for example, the planes crashing into their targets, wounded people or people jumping from the towers), only 15% of children had not had access to these images. Furthermore, even what were regarded as positive images, such as the President addressing the nation, the altruism of ordinary citizens or the help and rescue efforts, produced an increase in the number of post-traumatic symptoms. Given the negative effects that this exposure seems to have on children it is noteworthy that, in the studies reviewed, parents did not restrict access to these stimuli, this being especially the case with older children (e.g. Becker-Blease et al., 2008; Lengua et al., 2005; Phillips et al., 2004b; Schuster et al., 2001). Moreover, on occasions it was the school that did not restrict access. For example, the study by Saylor et al. (2003) found that 50% of the children surveyed reported having seen images of the attacks while at school.
In the only study to have compared the differential effects on children of exposure to radio, television and the printed press, it was the latter which was most associated with a longer duration of post-traumatic symptomatology (Pfefferbaum et al., 2003d). The authors suggest that this finding could indicate that those children who are most affected by an attack show greater interest in it, seeking out more information; alternatively, it may be that the reading and retention of static images, which are perhaps the most striking, has a more profound effect as it involves the processing of a different kind of information from the dynamic images that are broadcast on television. Similar results were obtained when analysing the use of internet as a source of information about the 9/11 attacks, with more post-traumatic symptoms being reported among children who used this form of media (Saylor et al., 2003).
It should be noted that research in this area is limited by the difficulty of assessing subsequent to the event how much access children had to images of a terrorist attack. Nevertheless, the findings to date, which are consistent across the studies reviewed, suggest that families and public authorities should be aware of the risks involved in exposing children and adolescents to this kind of material, regardless of whether they have been direct victims of the attack or were physically far removed from it (Comer and Kendall, 2007; Pfefferbaum et al., 2003d; Phillips et al., 2004b; Pine et al., 2005; Schuster et al., 2001).
(b) Consequences of interpersonal exposure to terrorism
Another common focus of analysis concerns children who are relatives of victims or who experience interpersonal exposure through their relationship to someone who has been directly affected by the attack. In this regard, research in the US (Pfefferbaum et al., 1999a, 1999b, 2003d; Pine and Cohen, 2002) and research carried out with Palestinian and Israeli children (Cohen and Eid, 2007; Elbedour et al., 1999; Ronen et al., 2003) have documented the serious psychological repercussions that these forms of exposure may have for children. The findings are consistent with the effects reported in adult victims in Spain (Baca et al., 2003). Indeed, high rates of post-traumatic stress disorder are found among children who have suffered the death of a parent due to terrorism, with one study reporting that 50% of girls and 33.1% of boys who lost a parent in the attack on the Hebron mosque in 1994 were subsequently diagnosed with this disorder (Elbedour et al., 1999).
A study by Pfefferbaum and co-workers (2000b) analysed symptoms of post-traumatic stress among children who were indirectly affected by the 1995 Oklahoma City bombing, i.e. children who reported that a friend or acquaintance was killed in the attack. The authors found that even this kind of indirect interpersonal relationship was associated with more symptoms than were observed among children who were not exposed in this way.
It should be noted that a child’s adaptation in the aftermath of a terrorist attack will largely depend on the degree of adaptation present in his or her immediate environment (mainly the family and school), as well as the child’s perceived degree of social support (Basu and Dutta, 2010; Gil-Rivas et al., 2004). Indeed, children process traumatic events in relation to the reactions of those around them, searching for signs and indicators that enable them to interpret the event and react in a socially expected way (Yehuda and Hyman, 2005).
Despite this, no published studies have yet analysed specifically the effect of distress among educational staff on the emotional state of children in the aftermath of a terrorist attack (Comer and Kendall, 2007), although reactions of fear among teachers during an attack have been related to more post-traumatic symptoms in the children for whom they are responsible (Pfefferbaum et al., 2003c).
As regards the family, research has shown that the sons and daughters of adults who have been highly exposed to terrorism (e.g. evacuees from the World Trade Centre during 9/11 and professionals involved in rescue efforts) report more psychological problems (mainly post-traumatic stress disorder) than do children whose parents were less exposed, this being the case even if the children themselves were not present during the attack. This effect was especially evident when both parents and children were highly exposed (see Hoven et al., 2004, 2005) and, in the case of adolescents, who are sufficiently mature to understand the danger that their parents had been in (Stuber et al., 2005). Studies have also shown that parental expressions of suffering following the 9/11 attacks, for example, crying or the presence of post-traumatic symptoms, were associated with the development of more symptoms of this kind in their sons and daughters (Fairbrother et al., 2003), as well as with other disorders and difficulties (Stuber et al., 2005). Although there is empirical evidence to suggest that family communication in the aftermath of a terrorist attack acts as a buffer against the development of psychological problems in children (Stuber et al., 2005), longer discussions with parents about the attack have also been associated with greater emotional and behavioural maladjustment in children (Stein et al., 2004). This same pattern was observed in a study conducted with Israeli Jewish and Arab families, whereby the highest levels of post-traumatic symptoms were found among those adolescents whose parents shared more information and feelings about terrorism with them (Cohen and Eid, 2007). Taken together, these results suggest that adults should reflect carefully before expressing certain negative emotions in front of children, especially if the latter have yet to develop a level of understanding that would enable them to take on board a subsequent explanation given to reassure them.
The dose-response effect can also be observed in these studies, such that the nature of the relationship with a direct victim of an attack influences the degree of psychological problems presented by a child. Specifically, the closer the relationship the greater the number of symptoms (Pfefferbaum et al., 2000a, 2006), and this is especially the case when the victim is a parent of a child of pre-school age (Basu and Dutta, 2010). It is worth noting, however, that in the study by Pfefferbaum et al. (1999a) of 10−16 year olds the highest levels of post-traumatic symptoms were reported by those who had lost a sibling in a terrorist attack, followed by those who had lost a parent.
The possible presence of pathological grief is only considered in two of the studies reviewed (Brown and Goodman, 2005; Pfefferbaum et al., 2006). As such, it is a topic that requires further analysis, not least when one considers the large numbers of children and adolescents who lose a loved one in this kind of violent act (La Greca, 2007) and the adverse effects that are known to be associated with pathological mourning − for example, an increased rate of post-traumatic symptoms (Brown and Goodman, 2005; Dowdney, 2000; Pfefferbaum et al., 1999b, 2006).
(c) Consequences of direct exposure to terrorism
Studies that focus on children who have been the direct victims of a terrorist attack (e.g. Koplewicz et al., 2002) tend to be based on small samples and often lack a comparison/control group. While this limits the results obtained in these studies, they nonetheless provide an initial approach to this important topic (Comer and Kendall, 2007; Pfefferbaum et al., 2005).
There are a number of studies which are based on the reports of parents of affected children (e.g. Fairbrother et al., 2003; Phillips et al., 2004b; Schuster et al., 2001), although it needs to be acknowledged that this form of assessment can be problematic. Adults tend to underestimate the psychological distress experienced by children, and often consider that any distress which is present will, in time, disappear of its own accord (see, for example, the study by Koplewicz et al., 2002). The appraisal of anxiety disorders, which are the most common among victims of violence, provides a case in point: adults tend to underplay the presence of symptoms in children, and thus false negatives are common in studies that only take into account the view of parents (Kendall and Flannery-Schroeder, 1998). A further point is that parents who themselves have an intense emotional reaction to a terrorist attack tend to regard their children as having been more affected by it (Hock et al., 2004; Phillips et al., 2004b; Schuster et al., 2001), this being an aspect that should be taken into account when contemplating treatment (Stuber et al., 2002). It is worth noting, however, that children’s distress also has a negative influence on the psychological state of their parents or carers, there being a feedback loop between the two that can heighten any psychopathology present (Phillips et al., 2004a). For example, three months after the 2004 attack on School Number 1 in Beslan (Russia), 95% of main carers and 77.3% of children (appraised by their carers) had a diagnosis of post-traumatic stress disorder (Scrimin et al., 2006).
Some studies have based their assessment of symptomatology on the child victims themselves. For example, one study of children who had been directly affected by the 9/11 attacks found that two-and-a-half years later, 35% of them had been diagnosed with post-traumatic stress disorder, while around half had difficulties with everyday functioning (Mullett-Hume et al., 2008). Similarly, 28% of children involved in the Brooklyn Bridge shooting in 1994 suffered from post-traumatic stress disorder two months after the event, as well as symptoms of anxiety and depression (Trappler and Friedman, 1996). These findings highlight the need for multi-informant appraisal of pathological symptoms in children, in line with what is already recommended in the field of child psychological assessment (Achenbach et al., 1987). This is particularly relevant in relation to the assessment of internalizing symptoms, where consistency between informants is minimal (Kendall and Flannery-Schroeder, 1998).
Social and professional implications
To conclude, the present study provides a systematic and rigorous review of the psychological symptoms and disorders that are most commonly found among children who have been victims of terrorism. This information is of fundamental importance in terms of designing specific and effective treatment programmes and interventions − ones that are sensitive to the needs of the population and that need to be based on empirical evidence drawn from the study of thousands of children and adolescents around the world. Only thus will these programmes be able to be effectively implemented in the event of future terrorist attacks.
Although few reports have examined the issue of mental health programmes for children after a terrorist attack, the ones that have focused on this topic have shown the effectiveness of short periods of counselling and interventions when delivered in school settings (Stuber et al., 2002). The school context is easily accessible, normalizes the terror experience the child has to cope with, and reduces the stigma associated with the use of mental health services (Pfefferbaum et al., 2003b). However, as multiple negative consequences related to terrorist attacks affect children, multimodal trauma-loss treatment approaches are still needed (La Greca, 2007).
As members of society we can choose to despair in the face of such acts of extreme violence or to take action so as to eradicate their consequences (Myers-Walls, 2004). One such form of action is to conduct research that increases our knowledge of terrorism and its effects on victims (for guidelines about what makes a good study of the psychological effects of terrorism on children, see Kazdin, 2007; North and Pfefferbaum, 2002). This is especially relevant in relation to the most vulnerable victims, i.e. children, with whom will lie the responsibility of building a less violent society in the future.
In the field of developmental victimology (Finkelhor, 2007) there is a need for trained professionals who can work with children who have experienced a terrorist act, and who are able to recognize not only the symptoms associated with such experiences but also the harmful physical, psychological and social effects they may have in both the short and long term, not least because the ultimate aim of terrorism is to produce these negative effects in the community (Myers-Walls, 2004). It is particularly important to be able to help children and adolescents who have been the indirect victims of a terrorist attack, whether via the media or through what is termed second-hand terrorism, because it is precisely in this form that terrorism most often leaves its mark on society and its future generations. There is therefore a need for community interventions that can prevent children from developing distorted views about the future, about safety and about violence (Pfefferbaum et al., 2003b). In this sense, education and counsel for parents regarding what type of behaviours to expect from their children after a terrorist attack and the effect that their own reactions can have on the psychological well-being of children are essential. Also, guidelines for professionals, like the one presented by Hagan and the Committee on Psychosocial Aspects of Child and Family Health, and the Task Force on Terrorism (2005) for paediatricians, are a very useful initiative.
Although terrorism and its effects on childhood constitutes a recent area of research (La Greca, 2007) − one that has yet to receive the attention that a topic of such contemporary relevance merits (Kazdin, 2007) − a considerable body of descriptive information has already been compiled. This work, mainly conducted in the USA over the last ten years, provides the foundation for a new and promising field of investigation for professionals who work with victims of terrorism, whether as researchers or in healthcare settings.