
Abstract
Our objectives were to (i) estimate lifetime prevalence of psychiatric comorbidity in heroin users and (ii) evaluate psychiatric comorbidity as a predictor of drug-related hospitalization following either (a) methadone maintenance or (b) naltrexone implant treatment.
Our method consisted of retrospective, longitudinal follow-up using prospectively collected, state-wide hospital data on two cohorts of heroin-dependent persons (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition), first time treated with naltrexone implant (n = 317) or methadone (n = 521) between January 2001 and December 2002. Outcome measures were: (i) prevalence of comorbidity and (ii) changes in risk for drug-related hospitalization – categorized as ‘opioid drugs’, ‘non-opioid drugs’, and ‘any drug’ – to 3.5 years post-treatment.
Nearly 32% had psychiatric comorbidity. In both cohorts, comorbid patients generally had significantly greater odds of drug-related hospitalization pre-treatment compared with non-comorbid counterparts. These differences generally reduced in magnitude post-treatment. Comorbid naltrexone-treated patients had less ‘opioid’ and ‘any drug’ related hospitalizations post-treatment. Similarly, comorbid methadone-treated patients had reduced hospitalization risk for ‘non-opioid’ and ‘any drug’ related hospitalization post-treatment. Treatment of persons without depression, anxiety, or personality disorder with naltrexone implant was associated with increased risk of ‘non-opioid’ drug-related hospitalization, while methadone treatment was associated with increased risk of ‘opioid’ drug-related hospitalization.
Although comorbid heroin users entered treatment with significantly higher risk of drug-related hospitalization than non-comorbid users, substantial reductions in drug-related hospitalization were generally observed post-treatment. This challenges the view that comorbidity predicts poor drug treatment outcomes. Differences in research methodology were noted; recommendation for rigorous analytical methodology in future research on assessing treatment outcomes was accordingly offered.
Keywords
Introduction
The coexistence of mental illness and addictive disorders is well established (Kessler et al., 1996; Regier et al., 1990). Among opioid abusers, comorbidities of depression, anxiety, and personality disorders are most common (Strain, 2002), with a lifetime prevalence of mood, anxiety, or personality disorders as high as 73%, 61%, and 65%, respectively (Conway et al., 2006; Darke et al., 1998). The odds for having a mood, anxiety, or personality disorder in the opioid-using population are up to 11, 8, and 6 times that of the general population, respectively (Brooner et al., 1997; Conway et al., 2006).
Early research on the prognostic impact of psychiatric comorbidity on opioid dependence treatment suggested that comorbid disorders are likely to adversely impact on treatment outcomes (Compton et al., 2003; Rounsaville et al., 1982, 1987). Nevertheless, recent research has found no differential prognostic significance of psychiatric comorbidity on long-term course of drug dependence (Trafton et al., 2006; Verthein et al., 2005) or general health outcomes (Gelkopf et al., 2006). Another study reported better outcomes among comorbid, treatment-resistant heroin addicts as compared to non-comorbid counterparts (Maremmani et al., 2008).
These seemingly disparate findings may in part be due to different choices of research methodologies. Specifically, some studies (Compton et al., 2003; Gelkopf et al., 2006; Rounsaville et al., 1987) only assessed between-group differences in drug-related outcomes at post-treatment, while neglecting within-group changes. Conversely, some studies evaluated within-group changes, without considering pre-existing, between-group differences (Trafton et al., 2006). Yet, others assessed both within-group changes over time (before–after) as well as between-group differences (comorbid versus non-comorbid) concurrently (Cacciola et al., 2001; Verthein et al., 2005). It is also unclear whether type of treatment influences outcomes, as, typically, reports are based solely on methadone maintenance treatment (MMT) (Brooner et al., 1997; Cacciola et al., 2001; Musselman and Kell, 1995; Trafton et al., 2006) or combined treatments (Kosten et al., 1989; Verthein et al., 2005), with few studies comparing the outcomes for different treatments (Gerra et al., 2006).
There are three main objectives for this study. First, lifetime prevalences of psychiatric diagnostic categories (depression, anxiety, personality, and any mental disorders) are estimated for each treatment cohort separately and in combination. Second, we examine the general (but not extensively confirmed) finding that pre-existing psychiatric comorbidity is predictive of inferior drug-related outcomes following MMT (Compton et al., 2003; Rounsaville et al., 1982, 1986). The third objective replicates the second but applies to the novel naltrexone implant treatment (NIT) for opioid dependence. Outcomes are discussed with the MMT cohort as the reference group. We assess both the between-group (psychiatric versus non-psychiatric) differences at baseline and at 3.5 years follow-up, and the within-group changes over time (post- versus pre-treatment). This extends our previous study (Ngo et al., 2008b) which reported a significant reduction in opioid drug-related morbidity but a significant increase in non-opioid drug-related morbidity in NIT patients. Conversely, the only significant change observed among MMT patients was a short-term (to 6 months post-treatment) increase in overdoses on non-opioid drugs in the older age groups. This earlier study (Ngo et al., 2008b) did not assess the prognostic significance of pre-existing psychiatric comorbidity on treatment outcomes. The current paper completely reanalyses the data from our previous study (Ngo et al., 2008b), adding a special focus on the role of pre-existing psychiatric comorbidity in drug-related outcomes following opioid pharmacotherapies with MMT or NIT.
Method
Participants
All participants met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for opioid-dependence and received either NIT or MMT for opioid dependence for the first time between January 2001 and December 2002 (Ngo et al., 2008b).
The full eligible NIT cohort consisted of 364 participants who were treated with a 2.2 g O’Neil naltrexone implant. Previously, we have reported 361 participants after excluding three cases with early implant removal (<7 days post-treatment) (Ngo et al., 2007, 2008b). For the current study, however, these three cases are included to more accurately reflect our intention-to-treat approach to data analysis. Of the 364 participants, we identified 336 through the Western Australian Data Linkage System (WADLS). The main analyses used 317 individuals, after 19 treatment crossover (either NIT to MMT or MMT to NIT) cases were removed. The males (n = 187, 59%) were significantly older than the females (29.0 years [SD 7.6] versus 27.1 years [SD 8.1], t = 2.17 [315], p = .031).
The full eligible MMT cohort previously included 655 patients (Ngo et al., 2008b). In processing data for socio-economic status for the present study, however, we have discovered one duplicate case that was subsequently removed from all analyses. Of the 654 eligible patients, 540 were identified via record linkage. After excluding the aforementioned 19 treatment crossover cases, the final cohort (n = 521) contained 198 (38%) females with a mean age of 30.3 years (SD 9.0) who were significantly younger than the males (32.1 years [SD 8.9], t = 2.29 [519], p = .022).
Treatment
We have previously described the treatments in detail (Ngo et al., 2008b). In brief, MMT patients were initially inducted at a centralized State Government drug treatment service in Western Australia. Methadone syrup was subsequently prescribed by medical practitioners and dispensed generally daily by community pharmacies (Drug and Alcohol Office, 2006a). The NIT cohort was treated at a ‘not-for-profit’ community clinic as a day procedure, which involved rapid opioid detoxification prior to implant insertion under local anaesthetic (Hulse et al., 2004). In the initial treatment (‘stabilization’) period, all MMT and NIT patients were offered standard individual and group therapy for their drug use and related psychosocial functioning issues. Referrals to mental health services were also available as required.
Procedure
As with its preceding study (Ngo et al., 2008b), the two cohorts in this study were followed up retrospectively and longitudinally via record linkage, enabled by the well-established WADLS (Holman et al., 1999). This system uses probabilistic matching to identify and link hospital admissions and mortality data concerning the same individual over time and includes data from all public and private hospitals in Western Australia.
Definitions
The hospital morbidity data provide a primary discharge diagnosis and allow multiple secondary diagnoses. These are converted into codes available in the International Statistical Classification of Diseases and Health-related Problems (ICD). Drug-related hospital admissions defined the outcome variables, which were classified as ‘opioid’, ‘non-opioid’, or ‘any’ drug-related admissions. If an admission received diagnoses concerning both opioid and non-opioid drugs, it was classified as ‘opioid’ related. Drug-related hospitalizations were due to ‘overdoses’ (i.e. poisoning) or other causes, such as withdrawal, dependence, or intoxication (Ngo et al., 2008b).
Substance-independent psychiatric comorbidities were categorized as ‘depression disorders’, ‘anxiety disorders’, ‘personality disorders’, and the umbrella classification, ‘any mental disorder’. Consistent with our earlier methodology (Ngo et al., 2007), research categories of psychiatric comorbidity may not be mutually exclusive for a given admission. Thus, for instance, an admission with a principal diagnosis of F32.3 (severe depressive episode with psychotic symptoms) and two additional diagnoses of F41.0 (panic) and F60.0 (paranoid personality) would be concurrently categorized as a ‘depression’, an ‘anxiety’, a ‘personality’, and an ‘any mental disorder’ event.
Socio-economic status was included as a potential confounder in assessing the relationship between psychiatric comorbidity and outcomes. Socio-economic status was derived from the Australian Bureau of Statistics’ Index of Relative Socio-Economic Advantage scores, primarily based on education, professional occupation, household income, housing ownership, and location.
Analysis
Data were analysed using SAS version 9.1.2 (SAS Institute Inc., Cary, North Carolina, USA).
First, approximate lifetime prevalence of (substance-independent) inpatient psychiatric morbidity at baseline was calculated for the two cohorts, separately (excluding 19 crossover cases) and combined (including the 19 crossovers). Lifetime prevalence for both inpatient and outpatient psychiatric morbidity was also calculated; however, outpatient data only include a primary diagnosis and were not used in the subsequent analyses.
Second, the raw distribution of cases with drug-related hospital morbidity was presented for each drug classification separately, cross-tabulated by treatment cohort (MMT and NIT), time (before and after treatment), and comorbidity group (depression, anxiety, personality, and any mental disorder). Readers should note that in reporting and discussing results, the terms ‘comorbid/non-comorbid’ and ‘psychiatric/non-psychiatric’ are used interchangeably, respectively, to refer to patients who had received hospital treatment for a substance-unrelated psychiatric condition within 3.5 years prior to opioid treatment entry. These terms do not necessarily indicate the patient’s psychiatric comorbidity status after treatment (which is not the subject of this research paper). The 3.5-year pre-treatment period was used as the cut-off point in determining the patients’ psychiatric comorbidity status, in order to match with the same period investigated for drug-related hospitalization outcomes (see also Ngo et al., 2008b).
Third, we used logistic regression modeling to statistically evaluate the above raw data. There are 24 analyses (two treatment cohorts [MMT and NIT] × three drug classes [opioid, non-opioid, any drug] × four psychiatric categories [depression, anxiety, personality, any psychiatric disorder]) in total. In each analysis, risk of hospitalized drug-related morbidity served as the dependent variable. To facilitate both between- and within-group comparisons, for each analysis, we included pre-existing psychiatric comorbidity status (psychiatric versus non-psychiatric), time relative to treatment (post versus pre), and their interaction concurrently, as key (compulsory) explanatory factors for each analysis. Potential confounders, including age, gender, and socio-economic status plus their interactions with time relative to treatment and psychiatric comorbidity, were examined. Odds ratios (ORs) and their 95% confidence intervals (CIs) were calculated from the best-fit model for each analysis.
In the WADLS, mental health records date from 1966 and general hospital records from 1970. In estimating the lifetime prevalence of mental health disorders, 23% of the cohort was born before 1966. For those born before 1966, as of the 1 January 1966 the mean age was 7.0 (SD 5.9). This means that the likelihood of the WADLS failing to capture psychiatric hospital morbidity of these individuals is minimal.
Ethics
This study received ethics approvals from the Human Research Ethics Committees of both the University of Western Australia and the Western Australian Department of Health – the latter controls access to hospital data via the record linkage system. The approval was for access to de-identified data on the NIT cohort who provided written consent and non-identifiable data on the MMT cohort who did not give written consent. Access to non-identifiable data is common practice in epidemiological research and ensures that the privacy of individuals is protected.
Results
Lifetime inpatient hospital prevalence of psychiatric illness in two study cohorts at baseline
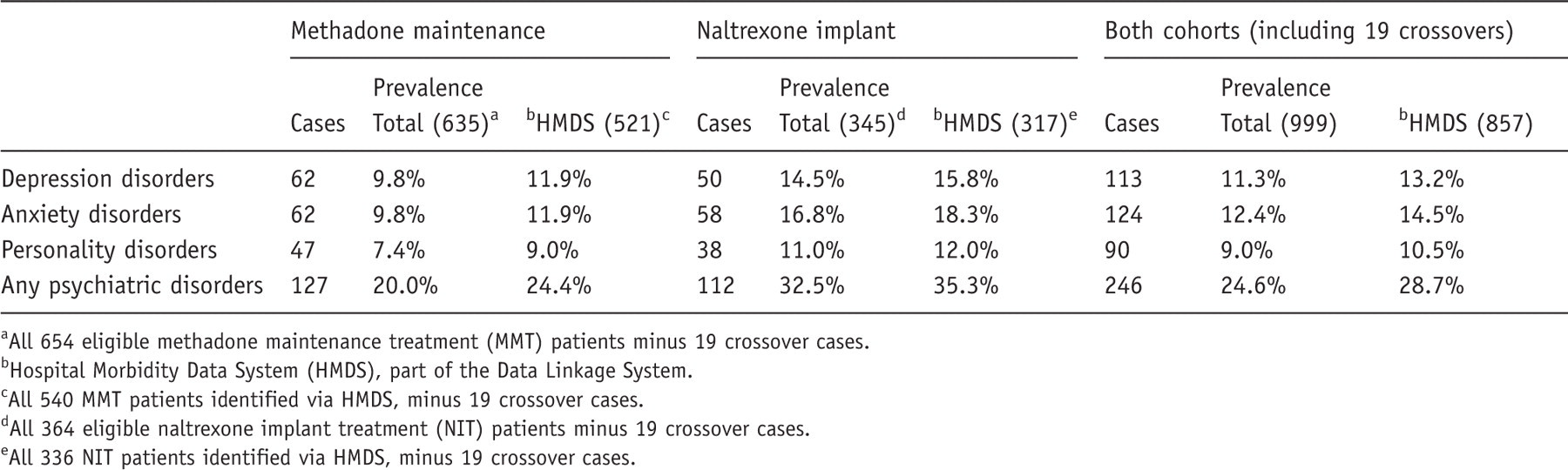
All 654 eligible methadone maintenance treatment (MMT) patients minus 19 crossover cases.
Hospital Morbidity Data System (HMDS), part of the Data Linkage System.
All 540 MMT patients identified via HMDS, minus 19 crossover cases.
All 364 eligible naltrexone implant treatment (NIT) patients minus 19 crossover cases.
All 336 NIT patients identified via HMDS, minus 19 crossover cases.
Lifetime prevalence of (inpatient and outpatient) psychiatric illness in two study cohorts at baseline
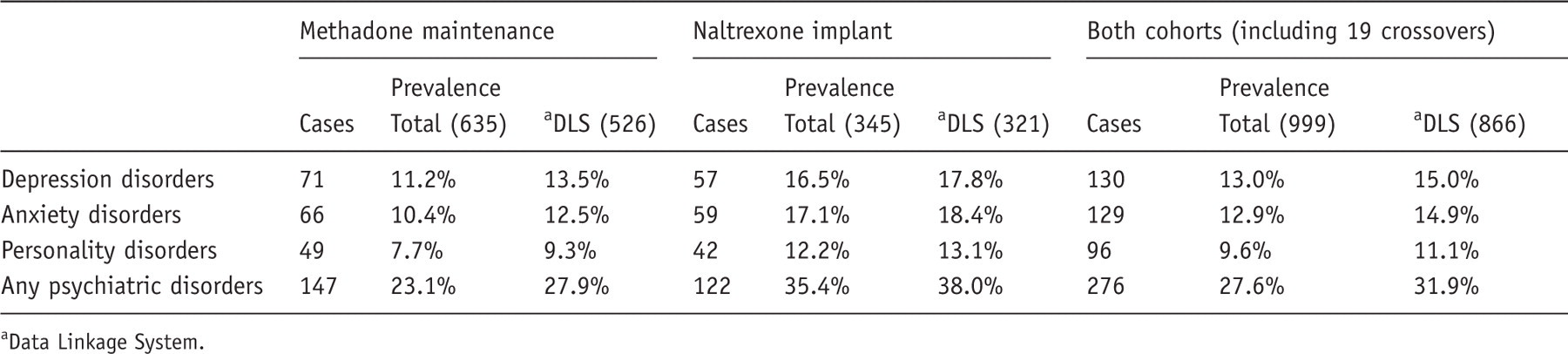
Data Linkage System.
Distribution of drug-related (‘opioid’, ‘non-opioid’, and ‘any drug’) hospital cases, cross-tabulated by pre-treatment psychiatric comorbidity
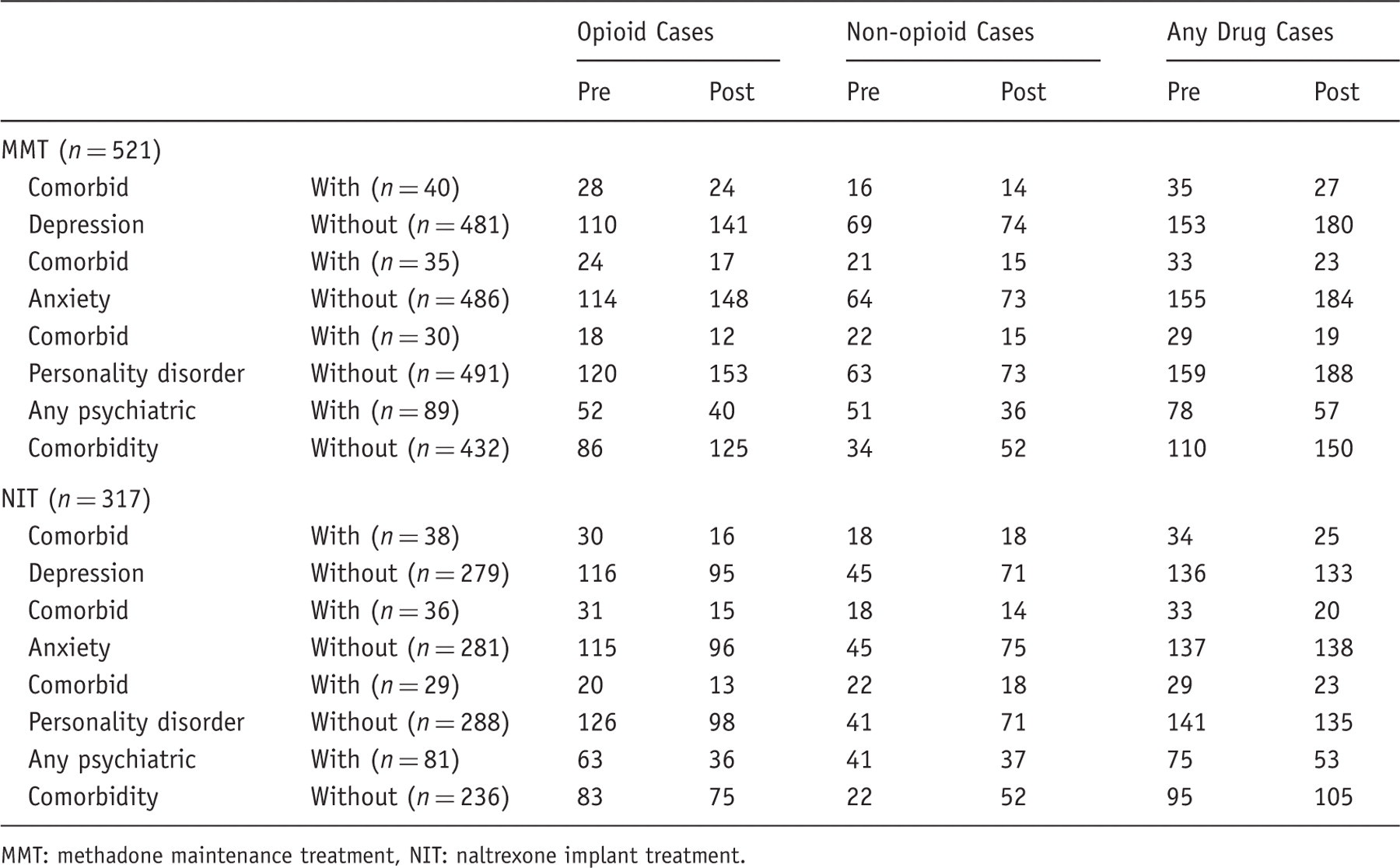
MMT: methadone maintenance treatment, NIT: naltrexone implant treatment.
Comparing (between-group) drug-related outcomes in psychiatric versus non-psychiatric patients, at pre- and post-treatments
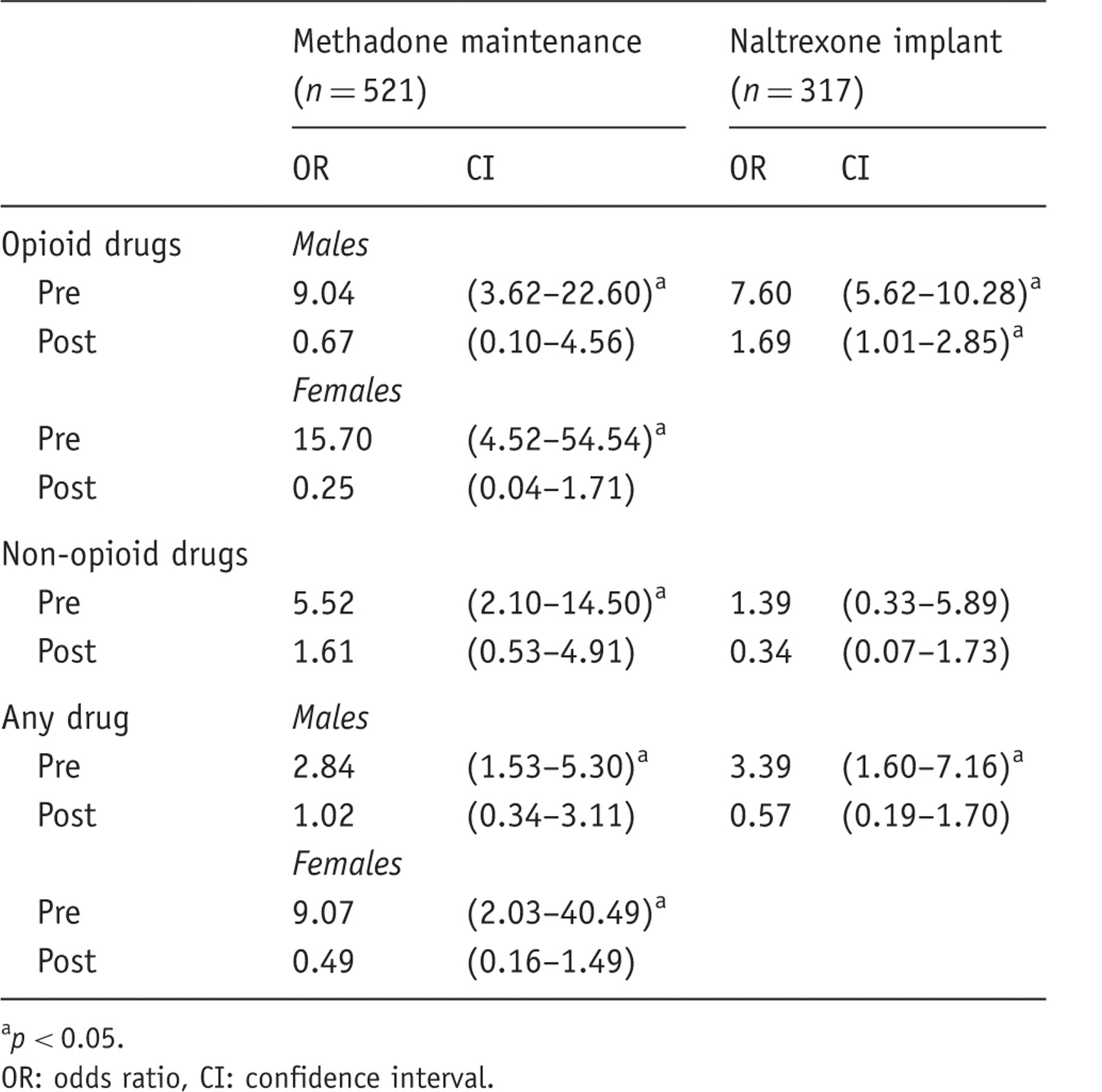
p < 0.05.
OR: odds ratio, CI: confidence interval.
Comparing (within-group) drug-related outcomes post- versus pre-opioid pharmacotherapy, for psychiatric and non-psychiatric patients
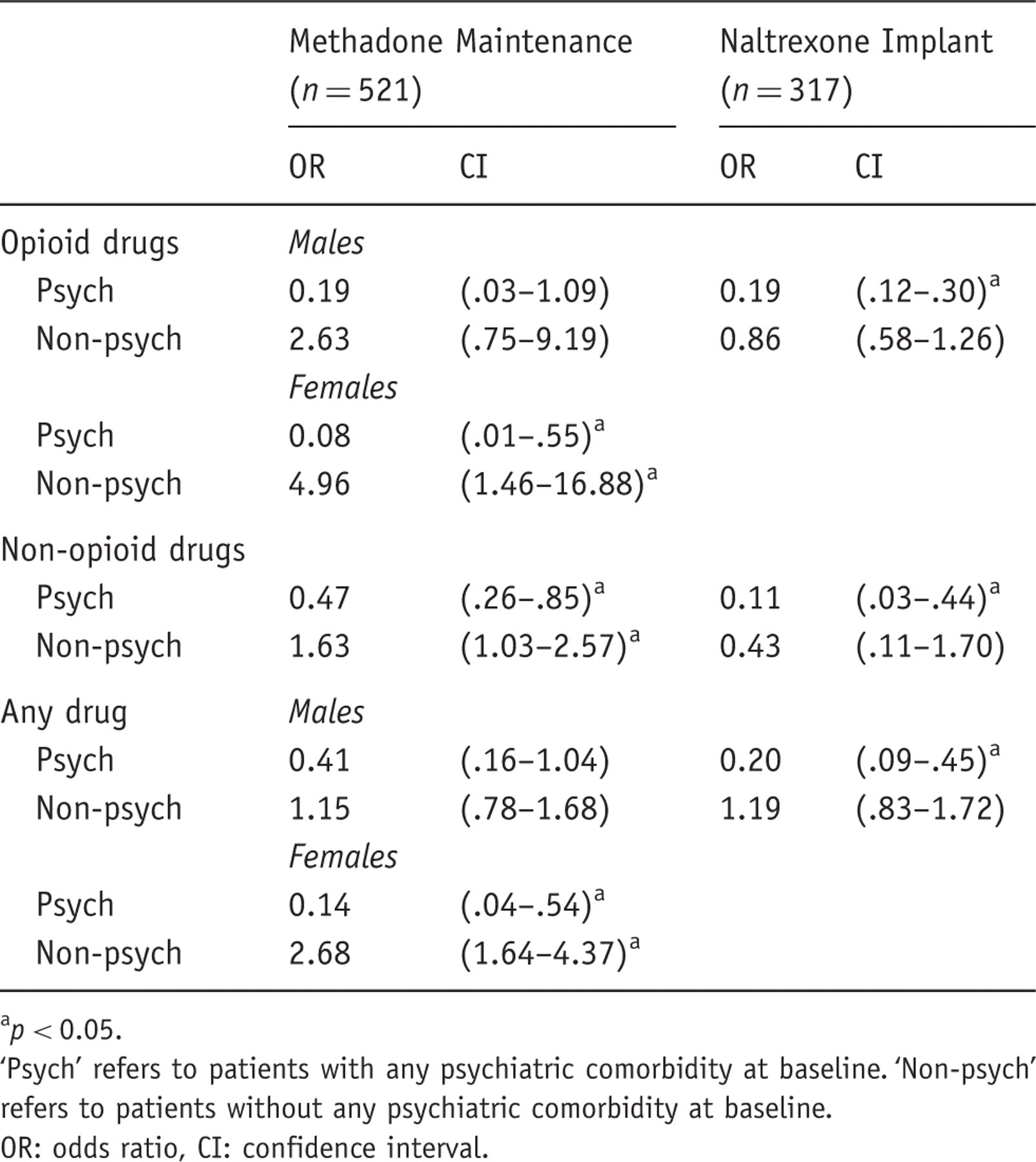
p < 0.05.
‘Psych’ refers to patients with any psychiatric comorbidity at baseline. ‘Non-psych’ refers to patients without any psychiatric comorbidity at baseline.
OR: odds ratio, CI: confidence interval.
Opioid drug-related hospitalizations
Between-group (psychiatric versus non-psychiatric) comparisons, at pre- and post-treatment times separately
For both MMT and NIT cohorts, at baseline, the odds of hospitalization for opioid drug-related causes among psychiatric patients were at least five times greater than that among non-psychiatric patients (Table 3). After treatment, this difference disappeared among MMT patients and was moderated among NIT patients. A significant (Wald’s χ2 = 4.7197, d.f. = 1, p = 0.0298) three-way interaction of time × comorbidity × sex was noted for the MMT cohort, indicating the (negative) association between psychiatric comorbidity collectively and opioid drug morbidity at baseline was more pronounced in females than in males.
For the three specific comorbidities (Supplementary Table 3), comorbid patients similarly experienced a much higher risk for opioid drug-related hospitalization at baseline than their non-comorbid counterparts. Again, this between-group difference at baseline also became insignificant post-treatment. The only exception was that comorbid depressed MMT patients still did worse than their non-depressed counterparts at post-treatment.
Within-group comparison: post- versus pre-treatment, within psychiatric and non-psychiatric subgroups separately
Psychiatric female patients fared exceptionally well post-MMT (OR 0.08, CI 0.01–0.55). Similarly, psychiatric NIT patients also gained a marked reduction in odds (OR 0.19, CI 0.12–0.30) for opioid drug-related hospitalization after treatment. In contrast, non-psychiatric patients either suffered almost a fivefold increase in odds for opioid drug-related hospital admission post-MMT (OR 4.96, CI 1.46–16.88) among females, or experienced no significant changes among males undertaking MMT and all NIT patients (Table 4).
In terms of specific comorbidities (Supplementary Table 4), the NIT cohort exhibited a similar pattern to that seen in the umbrella psychiatric category, with comorbid patients consistently improving post-treatment. With regards to personality disorders, patients experienced a reduced hospitalization risk post-NIT, regardless of comorbidity status, although this reduction appeared more substantial in magnitude for comorbid patients. The pattern in the MMT cohort was somewhat less positive, however. Specifically, non-comorbid patients experienced an elevated admission risk post-MMT; whereas their comorbid counterparts either experienced no significant change in risk (depression or anxiety) or a decreased risk (personality disorders) post-MMT.
Non-opioid drug-related hospitalizations
Between-group (psychiatric versus non-psychiatric) comparisons, at pre- and post-treatment times separately
Similar to the pattern observed for opioid drug-related hospitalization, psychiatric MMT patients were worse off than their non-psychiatric counterparts at baseline (OR 5.52, CI 2.10–14.50), but this between-group difference disappeared at post-treatment (Table 3). For the NIT cohort, however, the risk of non-opioid drug-related hospitalization was not significantly different between psychiatric and non-psychiatric patients, either pre- or post-treatment.
Unlike the above analysis for psychiatric comorbidity collectively, the subgroups with specific comorbidities of depression, anxiety, or personality disorders still remained at higher risk for non-opioid drug-related hospitalizations post-MMT, although such risk differences were narrowed (Supplementary Table 3). This pattern was also observed for the NIT cohort, except that comorbid anxious patients appeared to improve, such that the risk difference between this subgroup and their counterparts (without anxiety comorbidity) was no longer significant.
Within-group (post- versus pre-treatment) comparisons, for psychiatric and non-psychiatric patients separately
For both cohorts, significant reductions in non-opioid drug-related hospitalization risk were noted after treatment for psychiatric patients. Further, the NIT cohort benefited a sharper decrease in odds (OR 0.11, CI 0.03–0.44) than the MMT cohort (OR 0.47, CI 0.26–0.85). Among non-psychiatric patients, while the MMT cohort experienced a sizeable increase in risk for admission (OR 1.63, CI 1.03–2.57), the NIT cohort exhibited no significant change in risk after treatment (Table 4).
With specific reference to comorbidities of depression, anxiety, and personality disorders (Supplementary Table 4), no significant before–after changes in non-opioid drug-related hospitalization risk were observed for MMT patients, regardless of their comorbidity status. On the contrary, hospitalization risk increased post-NIT for non-comorbid patients, while staying relatively unchanged among comorbid patients.
Any drug-related hospitalizations
Between-group (psychiatric versus non-psychiatric) comparisons, at pre- and post-treatment times separately
For both MMT and NIT cohorts, similar to the pattern observed for opioid drug-related hospitalization, psychiatric patients entered treatment with a higher risk for any drug-related hospitalization than non-psychiatric counterparts. This association was particularly strong for MMT female patients. After treatment, however, the negative association between pre-existing psychiatric comorbidity and drug-related hospitalizations was no longer significant for either cohort (Table 3).
The results for the three specific comorbidities (Supplementary Table 3) generally mimicked those seen for the collective psychiatric comorbidity analysis for both cohorts. An exception to this was that depressed and non-depressed patients entered NIT with rather comparable risk for drug-related hospital morbidity.
Within-group (post- versus pre-treatment) comparisons, for psychiatric and non-psychiatric patients separately
For female comorbid MMT patients and for all comorbid NIT patients, drug-related hospitalization risk was lower at post-treatment than pre-treatment. For their non-comorbid peers, however, this pattern did not exist in NIT patients and was reversed for female MMT patients. Among male MMT patients, the difference in risk for hospitalization at post- versus pre-treatment did not reach statistical significance, regardless of comorbidity status (Table 4).
Regarding the three specific comorbidities, among MMT patients, a sharp contrast was noted between comorbid and non-comorbid patients’ outcomes. Specifically, comorbid patients consistently benefited from a reduced risk for all drug-related hospitalizations post-MMT, whereas non-comorbid patients suffered an increased risk post-MMT. Comorbid patients also benefited from NIT, evidenced by a reduction in hospitalization risk, while non-comorbid patients experienced no significant change in risk post-NIT.
Discussion
As expected, both MMT and NIT cohorts had a high prevalence of comorbid mental health disorders before entering opioid pharmacotherapy with approximately one-third having a substance-unrelated psychiatric diagnosis. For the categories of depression, anxiety, and personality disorder the figures were 15%, 15%, and 11%, respectively. The lifetime prevalence was estimated from both inpatient and outpatient hospital data, with the bulk of incidents (89%) identified from hospital admissions. Assuming that hospitalization is a marker for more severe psychiatric morbidity, these data indicate that the majority of psychiatric morbidity among treatment-seeking heroin users is of a more significant nature.
Our estimated lifetime psychiatric prevalences are comparable with those from some previous studies (Rounsaville et al., 1982; Strain, 2002) for depression (4–54%) and anxiety (3–39%), but at the lower end of the range for personality disorders (10–55%) (Darke et al., 1994; Strain, 2002). While our study found approximately 32% of the participants had been treated for their psychiatric illness collectively before entering opioid pharmacotherapy, epidemiological studies in the United States have reported that up to 53–65% of the drug-dependent population will have received a psychiatric diagnosis in their lifetime (Kessler et al., 1996; Regier et al., 1990). Differences in prevalence estimates could be due to different cut-off time points (e.g. at treatment entry versus projected for whole lifetime), case attainment methods (e.g. diagnosed following hospitalization versus via structured diagnostic interviews), and/or types of drugs abused (e.g. opioid versus any drug). For example, in reviewing previous studies, Strain (2002) found that lifetime prevalence of psychiatric comorbidity among opioid users ranged from 40% to 80%. Similarly, the rate of comorbid depression also varied widely, between 4% and 54%.
Depression is thought to motivate treatment entry and retention but also to interfere with the effectiveness of treatment (Compton et al., 2003; Nunes et al., 2004). For our MMT cohort, while exhibiting no prognostic significance in non-opioid drug-related health outcomes, comorbid depression was a protective factor for health outcomes related to opioids and all drugs collectively. Similarly, comorbid depressed patients undertaking NIT consistently benefited more from the opioid pharmacotherapy than their non-depressed counterparts with respect to all types of drug-related outcomes. Consistent with our previous study (Ngo et al., 2008b), most NIT patients (i.e. those without depression comorbidity) did worst on non-opioid drug-related outcomes, with the odds of hospitalization increasing almost twofold. In contrast, the majority of MMT patients (i.e. non-depressed) did particularly poorly on outcomes related to opioid drugs and all drugs collectively.
Apart from depressive disorders, anxiety and personality disorders are two other psychiatric comorbidities most commonly found in the opioid-dependents (Darke et al., 1994; Strain, 2002). Yet, research on their prognostic influence in opioid pharmacotherapy outcomes seems somewhat limited. As shown in Supplementary Table 4, almost identical patterns described above for the predictive relationship of comorbid depression and drug-related hospitalizations also apply for comorbid anxiety, for both MMT and NIT cohorts. This implies that depression and anxiety comorbidities have very similar prognostic (generally protective) influences on opioid dependence treatment outcomes. Our findings clearly contradict previous research that reported inferior treatment outcomes among users with comorbid post-traumatic stress disorder (PTSD) (Ouimette et al., 1999) or generalized anxiety disorders (Compton et al., 2003). Yet, other research (Trafton et al., 2006) detected no substantial difference in drug use outcomes between those with and those without comorbid PTSD, which concurs with our results concerning non-opioid drugs in the MMT cohort.
Personality disorders are generally associated with worse drug treatment outcomes (Compton et al., 2003; King et al., 2001), although some research reported similar outcomes for those with and without antisocial (Darke et al., 1994) or borderline (Darke et al., 2007) personality disorders. These latter findings (Darke et al., 1994, 2007) are also in line with ours in that personality disorders bore no significant prognostic value on non-opioid drug-related hospitalizations in the MMT cohort. Nevertheless, in terms of opioid drug-related outcomes, presence of comorbid personality disorders was associated with remarkably reduced risk for hospitalization whereas their absence was associated with a sizeable increased risk, following MMT or NIT. This pattern was also replicated for all drug-related outcomes in the MMT cohort. For the NIT cohort, however, similar to that observed for depression and anxiety comorbidities, users with personality disorders had their overall drug outcomes enhanced and non-opioid drug outcomes unchanged; either way, their outcomes were consistently superior to their non-comorbid peers.
Considering all mental disorders collectively, psychiatric comorbidity clearly represented a protective factor against drug-related hospitalization risk following opioid pharmacotherapy. It is possible that extra clinical attention or intervention for psychiatric comorbidity resulted in post-treatment reductions in drug-related hospitalizations among comorbid patients, which was not generally observed among non-comorbid patients. However, it was unclear whether the increased contacts with mental health professionals (Nunes et al., 2004) or added medications (Hesse, 2004) enhanced the comorbid patients’ drug treatment outcomes. Nevertheless, such data are not available in our study, to allow these possibilities to be further investigated.
In the MMT cohort, hospitalization risk post-treatment improved for comorbid patients and worsened for non-comorbid patients. Comorbid NIT patients also benefited from a substantial reduction in hospitalization risk whereas their non-comorbid peers’ risk stayed unchanged. Together these observations suggest that, while pre-existing psychiatric comorbidity enhanced drug-related outcomes with NIT, its absence was not necessarily associated with deteriorations in drug-related hospital outcomes as it was the case for MMT. On this basis, one may be tempted to conclude that NIT is a more broadly effective opioid pharmacotherapy than MMT. However, without a randomized controlled trial between the two treatments, such a direct comparison is not warranted.
Severity of psychiatric disorders has been reported to effect substance use treatment outcome; those with mild disorders are likely to respond better than those with more severe disorders (McLellan et al., 1983). While this study did not specifically assess ‘severity’, the majority of cases were identified as associated with hospitalization suggesting they fall at the more severe end of the spectrum. Quite encouragingly, however, these comorbid cases showed large improvements with treatment.
Gender differences
Previous research indicated that the relationship between comorbidity and adverse treatment outcomes is more apparent in males than females (Compton et al., 2003; Rounsaville et al., 1987). Males with psychiatric comorbidity were more likely to have worse drug treatment outcomes than non-comorbid males, whereas this association was not clearly observed in female patients. However, in our study, where gender difference existed in the prognostic relevance of psychiatric comorbidity to drug treatment outcomes, the opposite was found. Specifically, non-comorbid MMT females showed increased odds of both opioid and any drug-related hospitalization post-treatment; in contrast, comorbid MMT females showed significant declines. Such modifying effect of gender was not noted for the NIT cohort.
Strengths and limitations
To our knowledge, this is the first study that examines the role of psychiatric comorbidity in drug-related treatment outcomes for heroin users treated with naltrexone implants. Nevertheless, it is not without limitations. Firstly, as participants were not randomized to treatments, direct statistical comparisons of outcomes between treatments cannot be made. However, both cohorts did enter opioid pharmacotherapies over the same time and would have been exposed to similar historical factors, such as changes in the availability of heroin during the period of follow-up (Longo et al., 2004). A second potential limitation of the study is concerned with its employment of comorbidity at baseline as an explanatory variable; this does not allow for the dynamic nature of psychiatric disorders in that some participants may have incurred their first event after this time. However, earlier we have reported mental health outcomes of the NIT cohort approximately 1.8 years after their implant treatment (Ngo et al., 2007). We found no significant changes in patients’ risk for psychiatric hospitalization following NIT and the overall psychiatric hospitalization rate (except for mood disorders) dropped significantly post-treatment. At this stage we have not published similar findings for the MMT cohort.
Thirdly, the WADLS captures data on hospital diagnoses predominantly. As such, those with less serious problems may be treated in other settings such as primary care. Conversely, there may be severe cases who do not receive any treatment. Fourthly, retention in treatment with methadone or naltrexone may influence the study’s outcomes. These data however were not available for either cohort. Notwithstanding this, previous statistics suggested approximately 66% of patients generally remained on the Western Australia’s State MMT program for almost 1 year (Drug and Alcohol Office, 2006a,b; Ngo et al., 2008b). In contrast, naltrexone delivered by sustained implant treatment maintained therapeutic blood levels for some period between 2 (Hulse et al., 2009) and 4.5 (Ngo et al., 2008a) months. It is also likely that a significant percentage of the NIT cohort chose to be retreated with another naltrexone implant after the 2001–2002 period, as unpublished data from our recent randomized clinical trial (related to Hulse et al., 2009) indicated approximately 57% returned for another treatment with naltrexone implant within 1 year of randomization. Previous research has also shown that MMT patients with psychiatric comorbidity often had a lower treatment retention rate than their non-comorbid counterparts (Cacciola et al., 2001; Verthein et al., 2005), although others have reported the opposite (Gelkopf et al., 2006).
Conclusions
Consistent with previous research, our opioid-dependent cohorts exhibited a high prevalence of psychiatric comorbidity, with comorbid patients experiencing a heightened risk for drug-related hospitalization before commencing opioid pharmacotherapy, compared to non-comorbid patients. However, contrary to many previous findings (Compton et al., 2003; Rounsaville et al., 1982, 1987), our research shows that psychiatric comorbidity does not adversely impact on drug-related outcomes following opioid pharmacotherapy with MMT or NIT. Indeed, psychiatric comorbidity is associated with comparable or, in most cases, superior treatment outcomes, in comparison with its absence. This realization is important for two reasons. First, had our study not examined the interaction of between-group differences and within-group changes over time, we would most probably have concluded that comorbid patients did poorly in opioid pharmacotherapy. Therefore, we recommend future research in this area to evaluate and report these effects simultaneously. Second, we hope that clinicians will embrace our encouraging findings and become even more proactive and eager to treat comorbid opioid users, and not dismiss them into a ‘too-hard basket’. In fact, comorbid users also experience alleviated psychiatric symptoms as a side benefit from their drug dependence treatment (Nunes et al., 2004; Verthein et al., 2005).
Footnotes
Acknowledgement
Hospital morbidity and mortality data were extracted by the Data Linkage Unit at the Western Australia Department of Health.
Conflict of interest declaration
None of the authors have any personal conflicting financial interests to declare. This study is part of ongoing research funded by the National Health and Medical Research Council (353545) and the Office of Mental Health, Western Australia Department of Health. After this study, the authors have initiated further research on the naltrexone implants which are contracted to the University of Western Australia by Go Medical Industries under a Commonwealth Government Australian Industries Grant. The authors’ research unit has received donations from the Australian Medial Procedures Research Foundation to conduct work on addiction. The authors declare that Go Medical had no right of veto or input into study design, data analysis, or manuscript preparation.