
Abstract
Despite an increasingly recognized relationship between depression and smoking, little is known about the degree to which treatment studies for depression consider the impact of smoking on outcomes. The aim of this study is to examine the extent to which smoking is considered in current antidepressant treatment research. We conducted a MEDLINE search of recent randomized clinical trials of pharmacotherapy for depression published between 1 January and 31 December 2007, and a search of current pharmacological intervention studies for depression using www.ClinicalTrials.gov. Only 5% of the 107 pharmacological trials for depression published in 2007 reported the smoking status of their samples. Two studies (1.9%) controlled for smoking in the analyses and no studies analyzed outcomes by smoking status. Excluding the eight studies of combined treatment for depression and nicotine dependence, no other study on www.ClinicalTrials.gov (total n = 920) reported an intention to analyze outcomes by smoking status. Emerging data link smoking and depression, however, little attention has been directed toward the effects of smoking on antidepressant treatment outcomes. Conducting research to understand how nicotine and smoking affect responsiveness to antidepressants would advance our understanding of the neurobiology of depression and the development of new and targeted treatments.
Introduction
Major depression is one of the greatest causes of disability throughout the world (Murray and Lopez, 1997), and one of the most common psychiatric illnesses in the United States with a lifetime prevalence of 16.2% and a 12-month prevalence of 6.6% (Kessler et al., 2003). The effects of depression are wide-reaching and include increased morbidity and mortality, diminished functioning, treatment expenditures, increased work absenteeism and impaired work performance (Broadhead et al., 1990; Kessler et al., 2003; Klerman and Weissman, 1992; Luppa et al., 2007; Wang et al., 2008), all of which add up to billions of dollars of societal costs each year (Greenberg et al., 2003). While interventions can improve psychological well-being, health, and work performance (Wang et al., 2008), a significant proportion of patients do not receive adequate treatment for depression (Kessler et al., 2003). Even when patients do receive treatment, a sizable number do not find relief from depressive symptoms with the use of FDA-approved antidepressant pharmacotherapies (Mathew and Charney, 2009). Identifying and studying factors associated with non-response to antidepressants can help in the development of novel or targeted treatments that reach the greatest number of those with depression.
Although smoking and depression have been linked through epidemiological, neurobiological, and clinical research, the effects of smoking on antidepressant treatment outcomes have rarely been examined. The purpose of this review is to: (1) consider why it is important to examine the relationship between smoking and antidepressant treatment outcome and (2) examine the extent to which smoking status is considered in current clinical trial research on antidepressant agents.
The relationship between smoking and depression
Adults with depression are much more likely to smoke than adults in the general population (36.6% versus 22%) (Husky et al., 2008; Lasser et al., 2000). Nicotine dependence, which is defined as daily smoking, lack of aversive effects from nicotine (e.g. nausea), and the presence of withdrawal symptoms upon smoking cessation (e.g. cravings, anxiety, dysphoria, increased appetite) (APA, 1994), is also more likely to be found in adults with depression than non-depressed adults (30% versus 12.8%) (Dierker and Donny, 2008; Grant et al., 2004). The presence of depression has been linked to difficulty with smoking cessation and increased smoking relapse (Anda et al., 1990; Glassman et al., 1990; Kinnunen et al., 1999; Walsh et al., 2008; Wilhelm et al., 2006) and smoking cessation may precipitate new depressive episodes for smokers with a history of depression (Glassman et al., 2001). Conversely, smokers report greater symptoms of depression, more frequent episodes of depression, and higher rates of suicidal ideation and suicide than non-smokers (Wilhelm et al., 2006). Although there have also been conflicting findings (e.g. Hitsman et al., 2003; Niaura et al., 1999; see Ziedonis et al., 2008 for a review), a number of studies report that smokers with depression have a more difficult time quitting smoking and avoiding relapse (e.g. Kinnunen et al., 1999; Walsh et al., 2008; Wilhelm et al., 2006).
The role of nicotinic acetylcholine receptors in smoking, depression, and antidepressant response
Nicotinic acetylcholine receptors (nAChRs), located throughout the brain and soma, are the primary target of nicotine in the brain and modulate pathways involved in response to stress and depression (Picciotto et al., 2002, 2008). Through nAChRs, nicotine modulates multiple neurotransmitters (e.g. serotonin, dopamine, acetylcholine), and chronic nicotine exposure results in changes to nAChRs including receptor desensitization and upregulation of nicotine binding sites (Picciotto et al., 2002, 2008).
Animal models
Effects of antidepressant agents, nicotine, nicotinic agents, and nicotinic receptor knockouts in animal models of depression
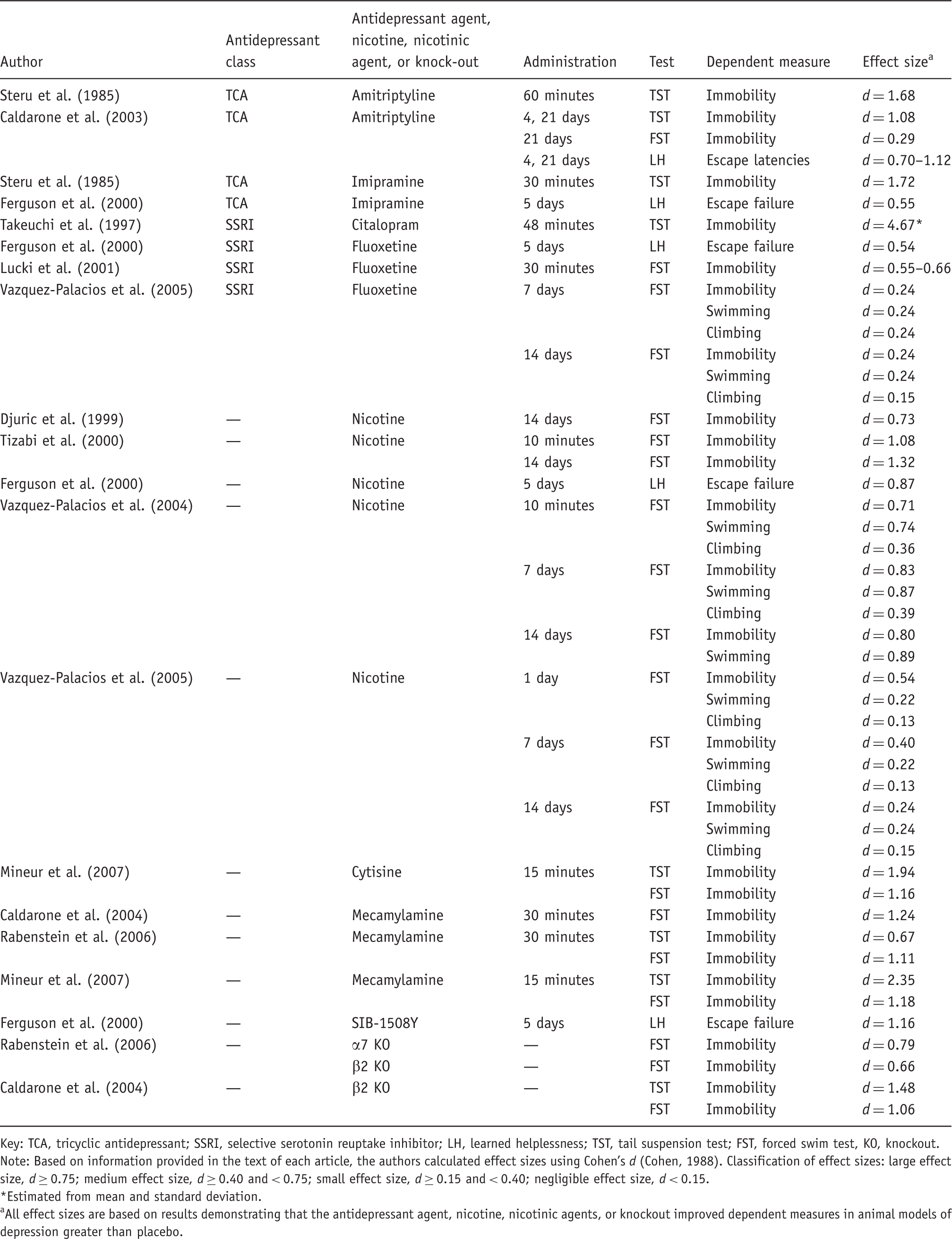
Key: TCA, tricyclic antidepressant; SSRI, selective serotonin reuptake inhibitor; LH, learned helplessness; TST, tail suspension test; FST, forced swim test, KO, knockout.
Note: Based on information provided in the text of each article, the authors calculated effect sizes using Cohen’s d (Cohen, 1988). Classification of effect sizes: large effect size, d ≥ 0.75; medium effect size, d ≥ 0.40 and < 0.75; small effect size, d ≥ 0.15 and < 0.40; negligible effect size, d < 0.15.
Estimated from mean and standard deviation.
All effect sizes are based on results demonstrating that the antidepressant agent, nicotine, nicotinic agents, or knockout improved dependent measures in animal models of depression greater than placebo.
Potentiation of effects when nicotine, nicotinic agents, or nicotinic receptor knockouts are combined with antidepressant agents in animal models of depression
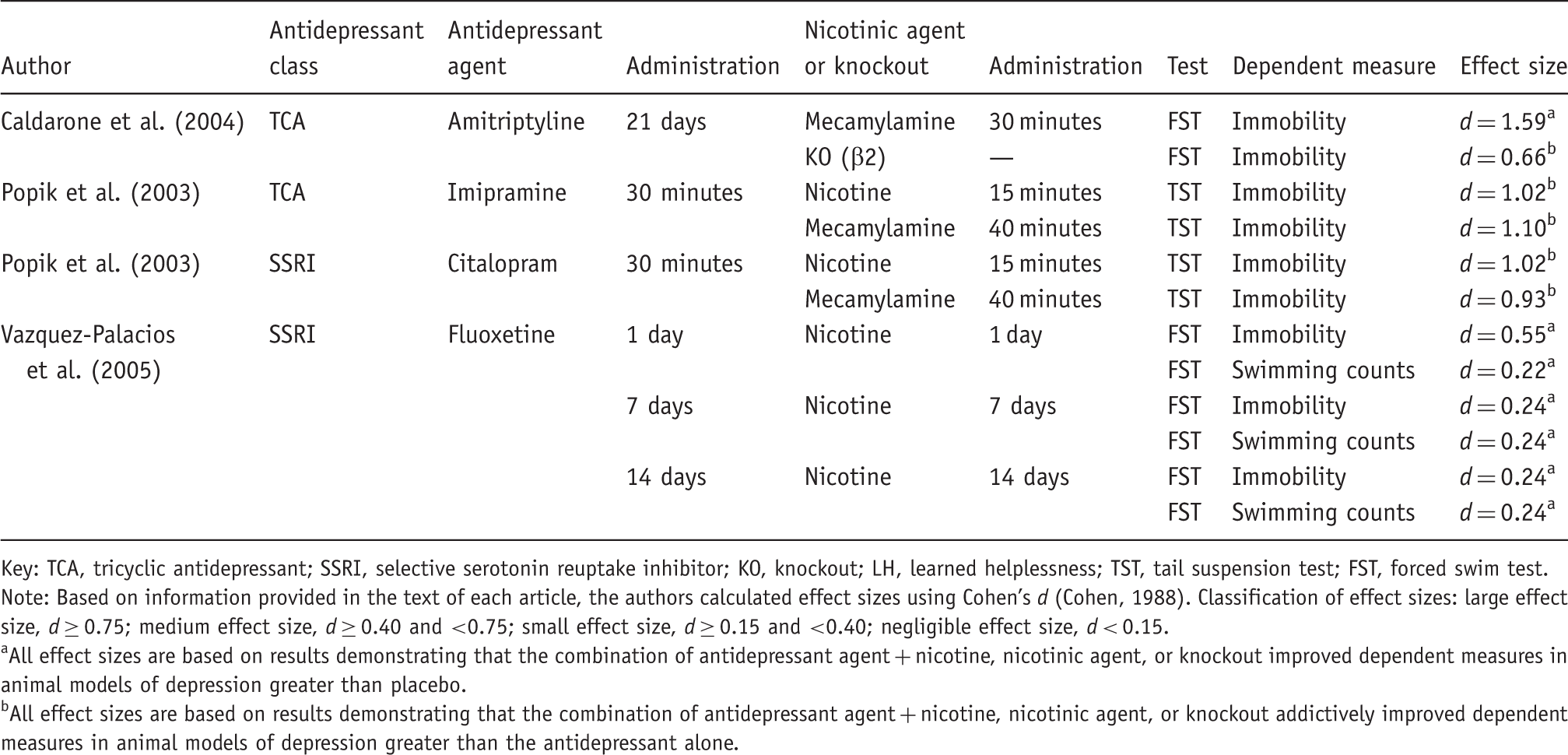
Key: TCA, tricyclic antidepressant; SSRI, selective serotonin reuptake inhibitor; KO, knockout; LH, learned helplessness; TST, tail suspension test; FST, forced swim test.
Note: Based on information provided in the text of each article, the authors calculated effect sizes using Cohen’s d (Cohen, 1988). Classification of effect sizes: large effect size, d ≥ 0.75; medium effect size, d ≥ 0.40 and <0.75; small effect size, d ≥ 0.15 and <0.40; negligible effect size, d < 0.15.
All effect sizes are based on results demonstrating that the combination of antidepressant agent + nicotine, nicotinic agent, or knockout improved dependent measures in animal models of depression greater than placebo.
All effect sizes are based on results demonstrating that the combination of antidepressant agent + nicotine, nicotinic agent, or knockout addictively improved dependent measures in animal models of depression greater than the antidepressant alone.
Clinical research
Effects of nicotine on symptoms of depression in humans
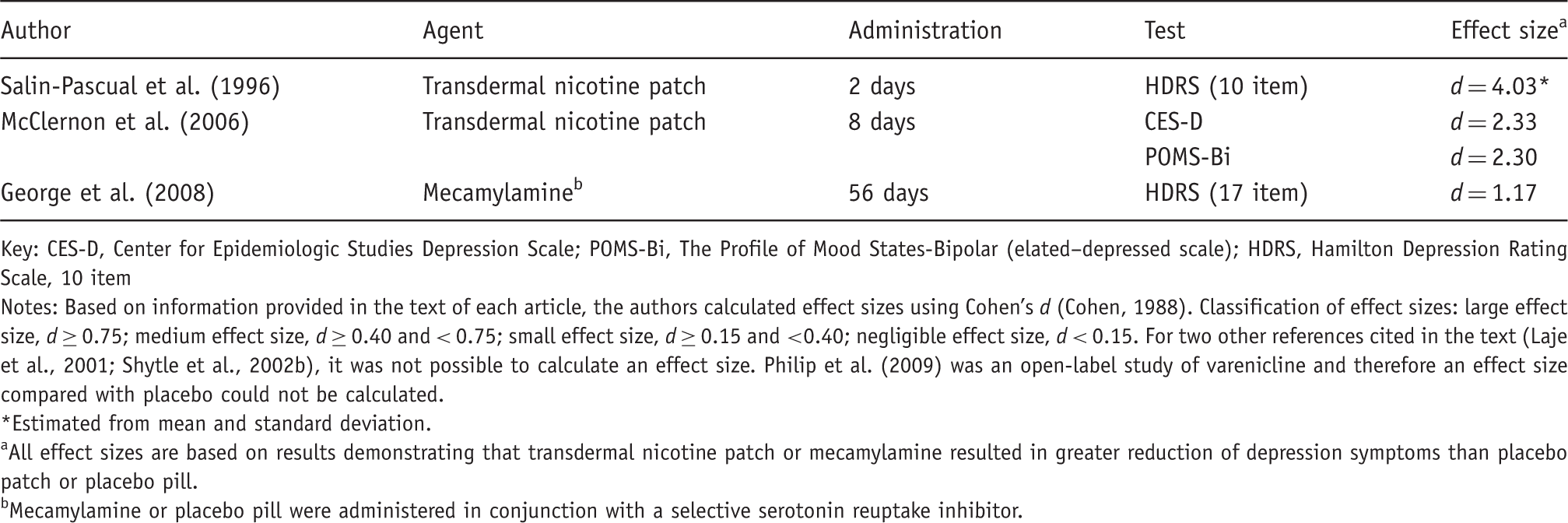
Key: CES-D, Center for Epidemiologic Studies Depression Scale; POMS-Bi, The Profile of Mood States-Bipolar (elated–depressed scale); HDRS, Hamilton Depression Rating Scale, 10 item
Notes: Based on information provided in the text of each article, the authors calculated effect sizes using Cohen’s d (Cohen, 1988). Classification of effect sizes: large effect size, d ≥ 0.75; medium effect size, d ≥ 0.40 and < 0.75; small effect size, d ≥ 0.15 and <0.40; negligible effect size, d < 0.15. For two other references cited in the text (Laje et al., 2001; Shytle et al., 2002b), it was not possible to calculate an effect size. Philip et al. (2009) was an open-label study of varenicline and therefore an effect size compared with placebo could not be calculated.
Estimated from mean and standard deviation.
All effect sizes are based on results demonstrating that transdermal nicotine patch or mecamylamine resulted in greater reduction of depression symptoms than placebo patch or placebo pill.
Mecamylamine or placebo pill were administered in conjunction with a selective serotonin reuptake inhibitor.
Would smokers and nonsmokers be expected to differ in their response to antidepressants?
While smoking has been found to be linked to depression through epidemiological and neurobiological research, the effects of smoking on treatment outcomes have been rarely examined and it is therefore unclear whether adult smokers differ from adult non-smokers in their response to antidepressant medications. While adults with depression exhibited a greater decrease in symptoms with a combination of a selective serotonin reuptake inhibitor (SSRI) and mecamylamine than an SSRI alone (George et al., 2008), secondary analysis showed that smokers responded less well than non-smokers to the combination. Because antidepressants work in part through nAChRs and chronic nicotine exposure results in nAChR receptor changes including receptor desensitization and upregulation of binding sites (Picciotto et al., 2008), differential response to mecamylamine by smoking status may have been due to smoking-related changes in nAChR function. If so, this suggests that while nAChRs antagonists may be a useful adjunct to antidepressant pharmacotherapies, adult smokers with depression may respond differently to such treatments. While nicotine might enhance response to antidepressants, the nAChR system is complex and smoking-related changes in the system might alter the functionality of nAChR agents in a positive or negative direction. The complexity of this relationship (Picciotto et al., 2002) highlights the importance of conducting controlled research to understand how nicotine affects nAChRs and responsiveness to antidepressant medications (Picciotto et al., 2008).
Aims of the current review
The purpose of this review is to examine the frequency with which contemporary clinical trials of antidepressant agents include information about the smoking status of participants, control analyses for smoking status, or analyze outcomes by smoking status. We reviewed all pharmacological trials of depression published during the year 2007 listed in MEDLINE, and all interventional studies for depression listed on ClinicalTrials.gov. It was expected that a minority of these studies would report baseline smoking status or examine treatment outcomes by smoking status.
Methods and materials: study design
We first conducted a MEDLINE search of recent randomized clinical trials of pharmacotherapy for depression published between 1 January and 31 December 2007. Data on the journal of publication, type of funding, and sample size were collected from each paper. Each article was classified (yes/no) as to whether it (1) reported the rate of smoking in the sample, (2) examined trial outcomes by smoking status, (3) included smoking status as a covariate in the analyses, and (4) reported smoking rates at the end of the clinical trial.
To further examine the inclusion of smoking status in clinical trials of depression using the most current data available, we conducted a second search on ClinicalTrials.gov. The ClinicalTrials.gov website is a registry of over 68,000 clinical trials conducted in the United States and around the world. US Public Law 110-85 (Food and Drug Administration Amendments Act of 2007; FDAAA), Title VIII, Section 801 mandates that clinical trials of drugs, biologics, and devices be registered at ClinicalTrials.gov. ClinicalTrials.gov was accessed on 9 February 2009 and a search was conducted using the terms ‘interventional study’ and ‘depression’. The records identified through this search were individually examined to determine whether smoking status was listed as part of the inclusion or exclusion criteria, study design, or analysis plan.
Results
Results of the MEDLINE search
Of 222 original articles published during 2007, 72 were excluded because they were not randomized clinical trials (n = 53), were trials of a condition other than depression (n = 13), or were not published in English (n = 6). An additional 43 studies were excluded because they were clinical trials only of behavioral treatments for depression (i.e. no pharmacological treatments were provided). The 107 randomized clinical trials of pharmacological treatments for depression that were included in the review were published in 74 different journals.
Within the 107 pharmacological trials, sample sizes ranged from 18 to 4041 participants (mean = 338; standard deviation = 586). The majority of articles focused on a subpopulation with depression including patients with a medical disorder (e.g. patients with stroke or chronic obstructive pulmonary disease; n = 16), older or geriatric adults (n = 13), patients with a co-morbid psychiatric or substance use disorder (n = 14), and adolescents (n = 7). Studies were split between those examining pharmacological treatments alone (58%) and those examining a combination of pharmacological and behavioral treatments (42%). Twenty-four percent of the studies reported receiving funding from the National Institutes of Health (NIH), 58% reported funding from other sources (e.g. pharmaceutical companies), and 18% did not list the source of funding.
The majority of studies (n = 102; 95.3%) did not report the rates of smoking in their samples. Within the five studies that reported smoking status, the percent of smokers ranged from 4% to 60% (mean = 30%). Two studies (1.9%) controlled for smoking in their analyses. No study included smoking as a variable in their analysis and no study reported the smoking status of their participants at the end of the clinical trial.
Results of the ClinicalTrials.gov search
At the time that ClinicalTrials.gov was accessed, there were 920 studies registered as interventional studies of depression (including phase I, II, III, and IV studies). Of these 920 studies, eight studies reported a focus on combined treatment for both nicotine dependence and depression, three studies listed smoking or nicotine dependence as criteria for exclusion, and one study stated under their inclusion criteria that both smokers and non-smokers could participate. Twelve additional studies reported that they would exclude participants with substance dependence ‘not including nicotine’. Excluding the eight studies of combined treatment for smoking and depression, no other study reported an intention to analyze outcomes by smoking status.
Discussion
The current study examined the frequency at which smoking status is reported and considered in treatment outcomes in pharmacotherapy trials for depression published during the year 2007 and in interventional studies listed on ClinicalTrials.gov. Both reviews showed that studies for depression are not analyzing outcomes by smoking status to determine whether smokers and nonsmokers show a differential response to antidepressant medication. Epidemiological and neurobiological evidence indicate a strong link between smoking and depression. Both smoking and depression affect the nAChR system and a significant amount of preclinical research has found that nicotinic agents exert antidepressant effects in traditional models of depression in animals. Many antidepressants have affinity for nAChRs, and nAChRs have been proposed as potential therapeutic targets for depression (e.g. Laje et al., 2001; Picciotto et al., 2002; Shytle et al., 2002a). Preclinical research has shown that nicotinic agents modify the effects of FDA-approved antidepressants and clinical research has offered preliminary research that augmenting antidepressant treatment with nicotinic agents improves the outcomes for treatment-resistant adults with depression.
While evidence discussed above suggests that nAChR agents including varenicline might have antidepressant properties, there has been significant controversy regarding whether varenicline increases suicidal ideation in smokers trying to quit. These concerns have led the FDA to issue a black box warning for varenicline. A recent report (Tonstad, 2010) that examined all controlled clinical trials of varenicline for smoking cessation on record with the pharmaceutical manufacturer (Pfizer, Inc.) found no increase in psychiatric disorders (including suicidal ideation or behavior) for participants receiving varenicline (n = 3091) compared with participants receiving placebo (n = 2005). Further, an examination of 80,660 adults in the United Kingdom found no increase in depression, suicidal thoughts, or self-harm for participants receiving varenicline as compared with nicotine replacement therapy or bupropion (Gunnell et al., 2009). Because smoking is associated with an increased risk of suicidal behavior (Wilhelm et al., 2006) and smoking cessation may lead to episodes of depression in smokers with a history of depression (Glassman et al., 1990, 2001), symptoms of depression including suicidal ideation should be monitored closely during any quit attempt whether it is done as part of a clinical research trial or in a clinical setting. Monitoring of suicidal symptoms should be conducted with a validated and treatment-sensitive measure, such as the Sheehan Suicide Tracking Scale (Coric et al., 2009).
While nicotine might enhance response to antidepressants, the nAChR system is complex and smoking-related changes in the system might alter the functionality of nAChR agents in a positive or negative direction (Picciotto et al., 2008). Current questions concerning the efficacy of antidepressants (Mathew and Charney, 2009) and the controversy regarding varenicline and suicidal behavior highlight the importance of conducting controlled research to understand how nicotine affects nAChRs and responsiveness to antidepressant medications. Research is needed to understand whether and what type of effects smoking has on depression in antidepressant treatment outcomes. Nonetheless, the very low rate at which smoking status of study participants is reported (<5% of studies published in 2007) suggests that the effects of smoking are rarely considered in assessing antidepressant outcome. Such knowledge would advance our understanding of the neurobiology of depression and the development of new and targeted treatments.
Several limitations of the current study must be acknowledged. Because only published studies from the year 2007 were reviewed, it is unclear whether the attention paid to smoking in depression research has increased or decreased over time. In addition, the authors were only able to include clinical trials in the review that were published and accessible on MEDLINE. Research has found that studies of antidepressant medications with negative findings are more likely to not be published than studies with positive outcomes (Turner et al., 2008). In terms of information reported through ClinicalTrials.gov postings, although the registry requires researchers to describe the planned primary and secondary analyses and provide a summary of each study, it does not specifically compel researchers to provide information about all assessed variables. Consequently, it is possible that some researchers assess smoking status but do not report this information. Nonetheless, the very low rate at which smoking status of study participants is reported suggests that the effects of smoking are rarely considered in assessing antidepressant outcome.
Footnotes
Acknowledgements
We would like to thank Merritt Piro, Erin Reutenauer, and Monica Solorzano for their contributions to the literature review.