
Abstract

We thank Delisle and colleagues (Delise et al. 2011) for their constructive comments on our recent meta-analysis focusing on selective serotonin reuptake inhibitors in patients recovering from acute coronary syndromes (Mazza et al., 2010) specifically challenging data abstraction and pooling methods.
Indeed, we have repeated data abstraction from Lesperance et al. (2007) and Glassman et al. (2002), and updated meta-analytic pooling for rehospitalization and change in depression score. We thus found that differences in the risk of rehospitalization were no longer statistically significant, despite the persistence of a strong clinical and statistical trend in favor of selective serotonin reuptake inhibitors (fixed-effect risk difference = −3% (95% confidence interval from −6% to 0%), p for effect = 0.09; random-effect risk difference = −4% (from −9% to 0%), p for effect = 0.07; p for heterogeneity = 0.29, I 2 = 19%) (Figure 1). Conversely, both statistical and clinical significance were confirmed in favor of selective serotonin reuptake inhibitors when focusing on their impact on changes in depression score (fixed-effect weighted mean difference = −1.7 (from −2.0 to −1.4), p for effect < 0.001; random-effect weighted mean difference = −3.2 (from −4.8 to −1.7), p for effect < 0.001; p for heterogeneity < 0.001; I 2 = 94%) (Figure 2).
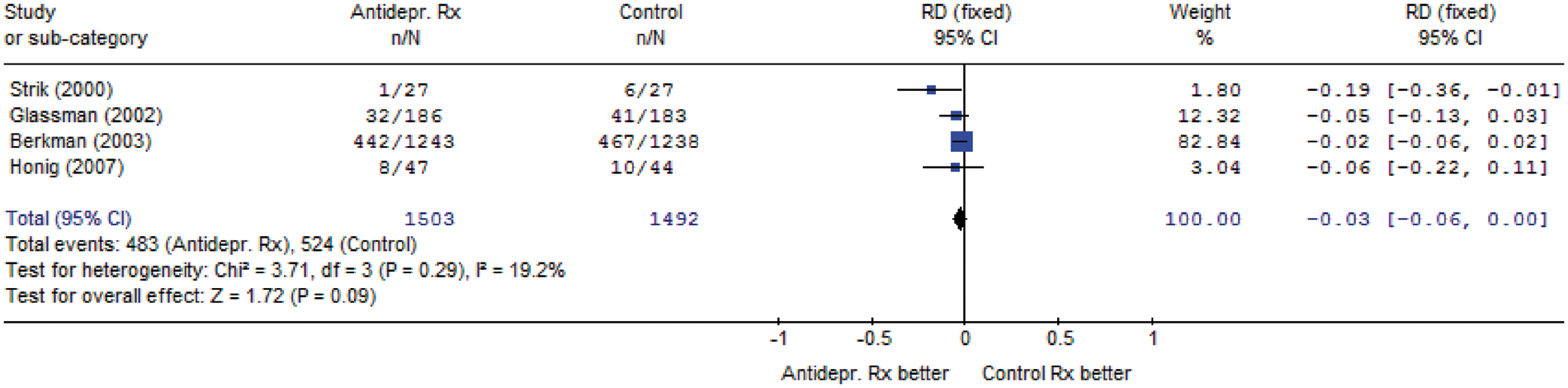
Meta-analytic pooling for the risk of rehospitalization. CI: confidence interval, RD: risk difference, df: degrees of freedom, I 2: inconsistency.
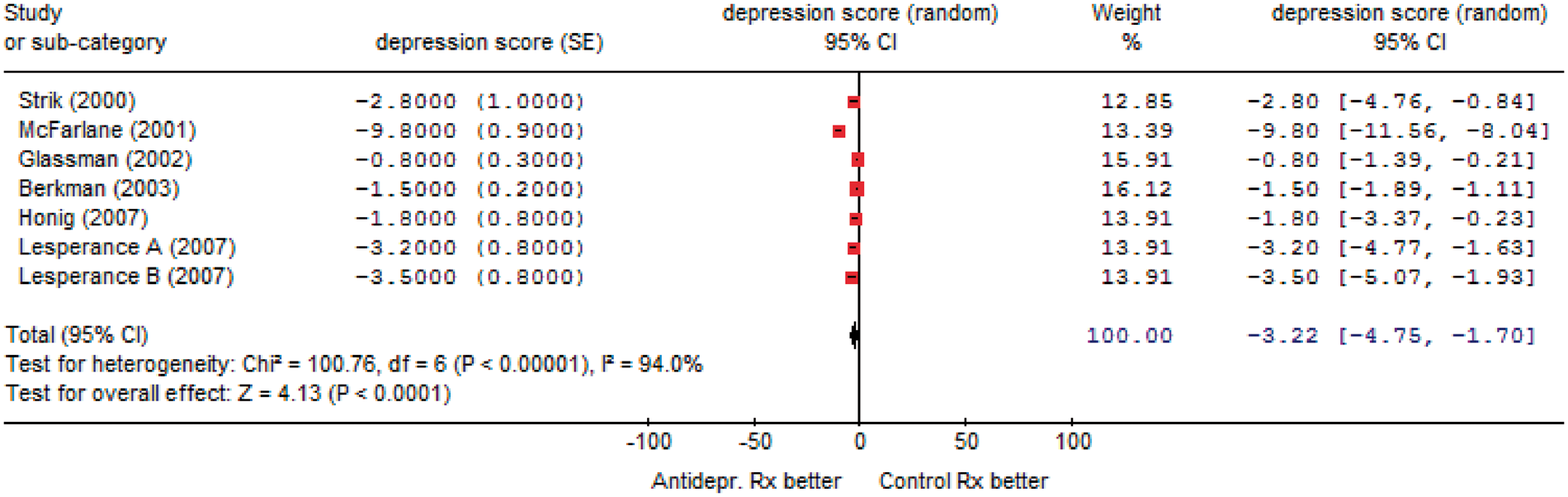
Meta-analytic pooling for the change in depression score. CI: confidence interval, df: degrees of freedom, I 2: inconsistency,SE: standard error.
As for the use of fixed versus random-effect methods, we understand Delisle et al.’s concern on the difficulty in choosing between fixed and random-effect meta-analytic pooling in the absence of significant heterogeneity. However, we should clarify that no single approach is by definition correct. Indeed, whereas fixed-effect methods may rely too much on large trials with several events and provide spuriously precise effect estimates (Cappelleri et al., 1996), random-effect methods can weigh too much on small trials with sparse events and thus yield effect estimates biased by such small studies (Poole and Greenland, 1999). Thus, our choice of flexibly using fixed- and random-effect methods depending on the extent of statistical heterogeneity and inconsistency, maintained also in the present work (Figures 1 and 2), can be scientifically defended and has already been adopted by our research group in other reviews previously published in scholarly journals (Landoni et al., 2007; Lipinski et al., 2007). In fact, the reporting of the above findings with both random-effect and fixed-effect methods clearly show that the former approach may lead to overoptimistic estimates of effect for changes in depression score.
Finally, we agree with Delisle and colleagues that meta-analyses are among the most important sources of evidence for researchers and clinicians, and thus thank them for offering us the opportunity to provide more precise results stemming from our comprehensive systematic review and meta-analysis.