
Abstract
This post-hoc analysis evaluated resilience as a predictor of treatment response in patients with posttraumatic stress disorder (PTSD). Data were pooled from two randomized, double-blind studies conducted with adult outpatients treated with flexible doses of venlafaxine extended release (ER) 37.5 to 300 mg/day or placebo. The 17-item Clinician-Administered Posttraumatic Stress Disorder Scale (CAPS-SX17) was the primary outcome measure. Baseline Connor–Davidson Resilience Scale (CD-RISC) scores for the 25-, 10-, and 2-item versions were used to predict changes in PTSD symptom severity at week 12 and symptomatic remission (CAPS-SX17 ≤ 20). Analyses were conducted for the overall population and separately for the individual treatment groups. In total, pretreatment resilience predicted a positive treatment response. For the overall population, all versions of the CD-RISC predicted CAPS-SX17 change scores and remission after controlling for variables such as treatment group and baseline symptom severity. For venlafaxine ER-treated patients, all versions of the CD-RISC were predictive of remission, but only the 10-item version was predictive of CAPS-SX17 change score. Our results suggest that higher pretreatment resilience is generally associated with a positive treatment response. Future research may be warranted to explore the relationship between response to active treatment and the spectrum of resiliency.
Introduction
Although the majority of individuals in the general population will experience a traumatic event at some point in their lives (Breslau et al., 1998; Kessler et al., 1995), data from the National Comorbidity Survey indicate that only 7% of the population will develop posttraumatic stress disorder (PTSD) (Kessler et al., 2005). This discrepancy may be partially explained by interindividual differences in the vulnerability to the effects of traumatic stress. ‘Resilience’ describes the ability to thrive in the face of adversity or to bounce back from challenges or setbacks, and is one of several factors that can influence how individuals respond to stress (Connor and Davidson, 2003; Yehuda, 2004). In terms of treating patients with PTSD, resilience has not been widely studied. Instead, clinical trials generally focus on the reduction of PTSD symptoms rather than the promotion of wellness or positive emotions.
The Connor–Davidson Resilience Scale (CD-RISC) is an instrument with demonstrated reliability and validity which was developed to measure resilience. The CD-RISC is composed of 25 items that are each rated on a five-point scale (0(Rarely true) to 4 (True nearly all of the time)) (Connor and Davidson, 2003). These items include the ability to adapt to change or to bounce back from challenges, and the extent ofthe individual’s social support network. The CD-RISC nowexists in three forms that have also been validated using conventional psychometric approaches: the full 25-item scale (referred to as the ‘CD-RISC’); a 10-item scale (CD-RISC-10) developed by Campbell-Sills and Stein (2007); and a 2-item scale (CD-RISC-2) (Vaishnavi et al., 2007). The two shorter versions were developed through different means; theCD-RISC-10 is based on factorial homogeneity and the CD-RISC-2 is primarily meant to serve as a very brief screening instrument. The CD-RISC-2 includes the items that address the ability to bounce back and adapt to change. The two shorter versions are being used with increasing frequency, but less is known about their relationship to treatment outcomes. As a result, we decided to take advantage of their inclusion within the 25-item scale and include them in these analyses to potentially enhance our understanding of these results. Additional information on the validation and content of these scales can be found in the principal references noted above.
The CD-RISC has demonstrated sensitivity to change during short-term pharmacotherapy and psychotherapy, modalities which have been found to increase resilience in patients with PTSD (Davidson et al., 2005). The CD-RISC also has been previously used in predictor analyses in patientswith mood, anxiety, and substance abuse disorders. Camardese et al. (2007) found that baseline resilience was associated with an increased likelihood of achieving remission in patients with major depressive disorder (MDD), whereas Roy et al. (2007) found that CD-RISC score predicted suicide attempts in a population of substance abuse patients. In PTSD patients, the baseline rating of CD-RISC item 6 (‘Seeing the humorous side of things when under stress’) predicted remission in a mixed sample of patients drawn from different studies (Davidson et al., 2005). However, because no study has evaluated resilience as a predictor of treatment outcome in the context of adouble-blind, placebo-controlled trial, to the best of our knowledge, the findings we report here comprise the first such analysis.
Venlafaxine extended release (ER) is a serotonin-norepinephrine reuptake inhibitor that is approved for the treatment of generalized anxiety disorder, social anxiety disorder, panicdisorder, and MDD (Baldwin et al., 2005; Wyeth Pharmaceuticals Inc., 2006). This pooled analysis, which was conducted using data from two studies that demonstrated the efficacy of venlafaxine ER for treating PTSD (an unapproved indication) (Davidson et al., 2006a, 2006b), was designed to evaluate the predictive effect of pretreatment resilience on treatment response in patients with PTSD. A previously conducted analysis using data from the 6-month study demonstrated the efficacy of venlafaxine ER for improving resilience, as measured by total and individual-item CD-RISC scores (Davidson et al., 2008), suggesting that resilience is modifiable in the short term, despite being viewed as a trait characteristic. The effect of short-term antidepressant treatment on resilience is further supported by the findings from a recent study of family dementia caregivers treated with escitalopram (Lavretsky et al., 2010). For the current analyses we hypothesized that resilience would be predictive of a better treatment response, but we did not know the extent to which this would apply separately to active treatment versus placebo, nor did we know whether the three versions of the CD-RISC would perform differently. Finally, we sought to assess whether any observed effects ofresilience on treatment response would be maintained after accounting for other predictors, such as PTSD symptomseverity, study protocol, or the treatment that was administered.
Materials and methods
For this analysis, data were pooled from two double-blind clinical trials, one of 3 months duration and the other of 6 months duration, in which patients were randomly assigned to flexible doses of venlafaxine ER (37.5–300 mg/d) or placebo. Both studies enrolled medically stable adult outpatients with a primary diagnosis of PTSD based on the criteria described in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Study participants were required to have been experiencing symptoms for at least 6 months with a baseline 17-item Clinician-Administered PTSD Scale (CAPS-SX17) (Blake et al., 1995) score ≥ 60. Immediately following confirmation of eligibility for inclusion, all baseline assessments were conducted prior to random assignment to venlafaxine ER or placebo.
Statistical analysis
For this investigation, baseline CD-RISC, CD-RISC-10, and CD-RISC-2 scores were evaluated to identify predictors of treatment response, defined as the percentage of patients meeting remission criteria (CAPS-SX17 ≤ 20) at week 12, and week 12 mean change from CAPS-SX17 baseline scores. The last-observation-carried-forward (LOCF) method was used to account for missing patient data due to early withdrawal. All analyses were performed separately for the combined treatment groups, for the placebo group alone, and for the venlafaxine ER group alone. All analyses were adjusted for baseline CAPS-SX17 score and study protocol. For the combined treatment groups, the analyses also were adjusted for treatment group assignment. No adjustments were made for multiple statistical comparisons.
Two-way interactions of treatment-by-study were found to not be significant for each version of the CD-RISC. In addition, treatment-by-factor interactions, where factor denotes any of the three CD-RISC scales, were not significant; therefore, all analyses and final models did not include two-way interaction terms. As a result, models with no interaction terms were used.
Results are presented for (i) the combined groups (i.e. both the drug- and placebo-treated patients), (ii) placebo, and (iii)venlafaxine ER, to identify the predictors that are specifically related to treatment with venlafaxine ER and those that are nonspecific.
Remission as binomial outcome
Separate logistic analyses of remission were conducted for each version of the CD-RISC to determine if any of the scales were significant predictors. All logistic analyses were adjusted for total CAPS-SX17 score at baseline, study protocol, and, for the combined treatment group analysis, treatment group enrollment. All analyses were performed for the total population (i.e. combining the venlafaxine ER and placebo groups) and separately for each treatment group.
Response as continuous outcome
The relationship between total CD-RISC score and change from baseline CAPS-SX17 score was examined in a manner similar to that described for the remission analyses, except utilizing a linear regression analysis instead of a logistic analysis.
Results
The pooled population comprised 687 patients with PTSD (venlafaxine ER (n = 340); placebo (n = 347)). Of the enrolled patients who received at least one dose of study drug, 224 withdrew prior to study completion. Demographic data, including trauma type and baseline CAPS-SX17 and CD-RISC scores, are presented in Table 1. No differences in baseline characteristics were observed between treatment groups. The current analyses build on the results of the primary publications of these data, which demonstrated that the percentage of patients meeting CAPS-SX17 remission criteria was higher for the venlafaxine ER treatment group compared with the placebo group in both studies (Davidson et al., 2006a, 2006b). The percentage of patients meeting criteria for remission at week 12 for the individual studies were as follows: venlafaxine ER, 43%; placebo, 28%; and venlafaxine ER, 30%; placebo, 20%, respectively.
Baseline demographic characteristics
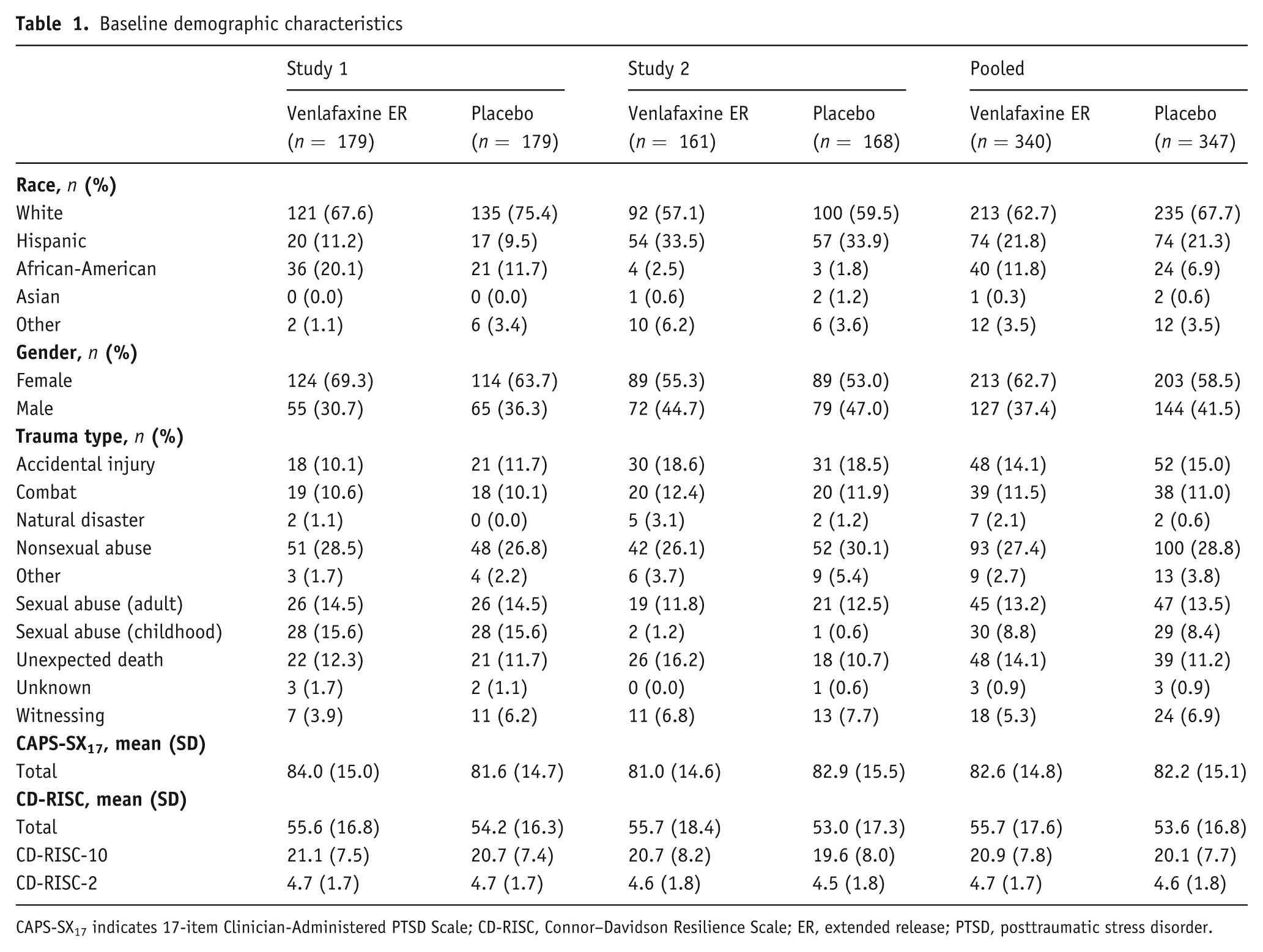
CAPS-SX17 indicates 17-item Clinician-Administered PTSD Scale; CD-RISC, Connor–Davidson Resilience Scale; ER, extended release; PTSD, posttraumatic stress disorder.
Predictors of CAPS-SX17 remission: CD-RISC 25-, 10- and 2-Item versions
In the combined treatment group models, total baseline score on all versions of the CD-RISC was found to be predictive of remission (Table 2), as was baseline CAPS-SX17 score (odds ratio (OR) = 0.971 (95% confidence interval (CI): 0.958, 0.985; p < 0.0001), study protocol (OR = 0.478 (95% CI: 0.327, 0.697; p = 0.0001), and treatment group assignment (OR = 0.502 (95% CI: 0.343, 0.733; p < 0.001)) (data not reported in the table). Very similar results were seen for baseline CAPS-SX 17 in the analyses of CD-RISC 10 and CD-RISC 2; all values were statistically significant (i.e. CIs did not cross 1.0).These associations suggest that patients with higher baseline resilience had a greater chance of achieving remission, as did those with lower PTSD symptom ratings, those treated in the non-US study, and those treated with venlafaxine ER. In the US study, remission was half as likely to occur as in the non-US study, so separate analyses were performed for each study. For the three CD-RISC scales, the OR in the logistic models and the estimates in the linear regression models are much larger and more significant for study 2 compared with study 1 (Davidson et al., 2006a, 2006b). Therefore, all analyses should be viewed with this limitation in mind, although the nature of the relationship between baseline resilience and chance of remission was similar in both studies. For the combined treatment group analyses, the ORs (95% CI) of achieving remission in relation to CD-RISC total, CD-RISC-10, and CD-RISC-2 were 1.026 (1.104, 1.038; p < 0.0001), 1.058 (1.031, 1.086; p < 0.0001), and 1.279 (1.142, 1.434; p < 0.0001), respectively, suggesting that for each additional point on these scales there was a 2.6%, 5.8%, and 27.9% increased likelihood of attaining remission. After accounting for the different number of items, the ORs for these subscales are comparable.
25-item baseline CD-RISC and subscale prediction of remission *
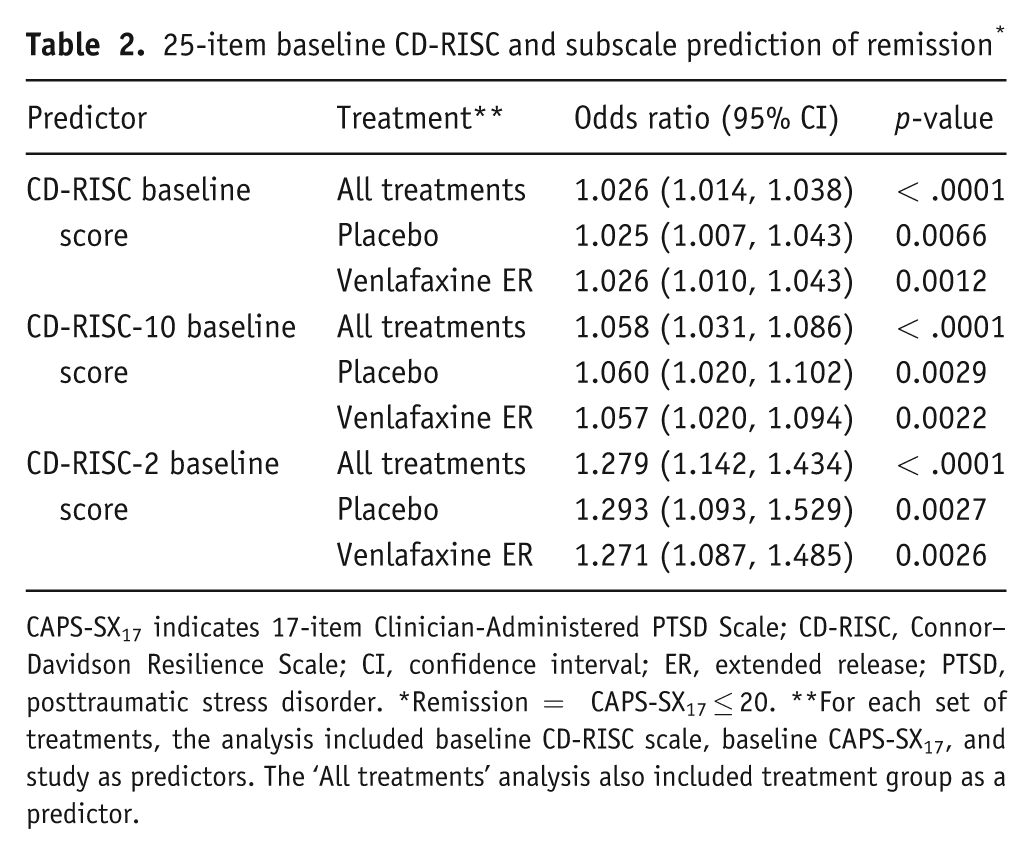
CAPS-SX17 indicates 17-item Clinician-Administered PTSD Scale; CD-RISC, Connor–Davidson Resilience Scale; CI, confidence interval; ER, extended release; PTSD, posttraumatic stress disorder. *Remission = CAPS-SX17 ≤ 20. **For each set of treatments, the analysis included baseline CD-RISC scale, baseline CAPS-SX17, and study as predictors. The ‘All treatments’ analysis also included treatment group as a predictor.
When analyzing the placebo and venlafaxine ER groups separately, similar results were observed. A significant predictive effect of remission was found for all three versions of the CD-RISC, as well as for baseline CAPS-SX17, study enrollment, and treatment group assignment. The ORs (95% CI) relative to remission for the CD-RISC total, CD-RISC-10, and CD-RISC-2 among patients receiving placebo were 1.025 (1.007, 1.043), 1.060 (1.020, 1.102), and 1.293 (1.093, 1.529). For the venlafaxine ER group, the ORs (95% CI) were 1.026 (1.010, 1.043), 1.057 (1.020, 1.094), and 1.271 (1.087, 1.485). Although these ORs are relatively low, none of the CIs cross 1.0, indicating statistical significance.
Predictors of CAPS-SX17 change scores: CD-RISC 25-, 10- and 2-Item versions
In the linear regression models, all three versions of the CD-RISC, as well as baseline CAPS-SX17 score, study protocol and treatment group, were found to be predictive of response as measured by week 12 CAPS-SX17 mean change from baseline score (Table 3). In the combined treatment group analysis and the separate analyses of the venlafaxine ER and placebo groups, the linear regression analyses demonstrated that the three versions of the CD-RISC, with the exception of the CD-RISC and CD-RISC-2 for venlafaxine ER, predicted change from baseline in CAPS-SX17 score after controlling for other predictor variables. For the combined treatment group, the CD-RISC, CD-RISC-10, and CD-RISC-2 were significant (p <0.001) predictors, with regression coefficients of −0.25, −0.55, and −2.19, respectively. For the placebo group analysis, the three CD-RISC scales were also significant (p < 0.01) predictors, with regression coefficients of −0.34, −0.70, and −2.70, respectively. However, for the venlafaxine ER group, only the CD-RISC-10 was found to be significant with a regression coefficient of −0.41 (p < 0.05). After taking into account the number of items in each scale, it can be seen that the regression estimate is largest for the CD-RISC and smallest for the CD-RISC-2 (i.e. −0.25*25 = −6.25 for CD-RISC; −0.55*10 = −5.5 for CD-RISC-10; and −2.19*2= −4.38 for CD-RISC-2). An additional analysis was conducted that included a treatment by baseline CD-RISC interaction in the model, which provided the same results, with no significant interaction being observed.
25-item baseline CD-RISC scales’ prediction of CAPS-SX17 change from baseline *
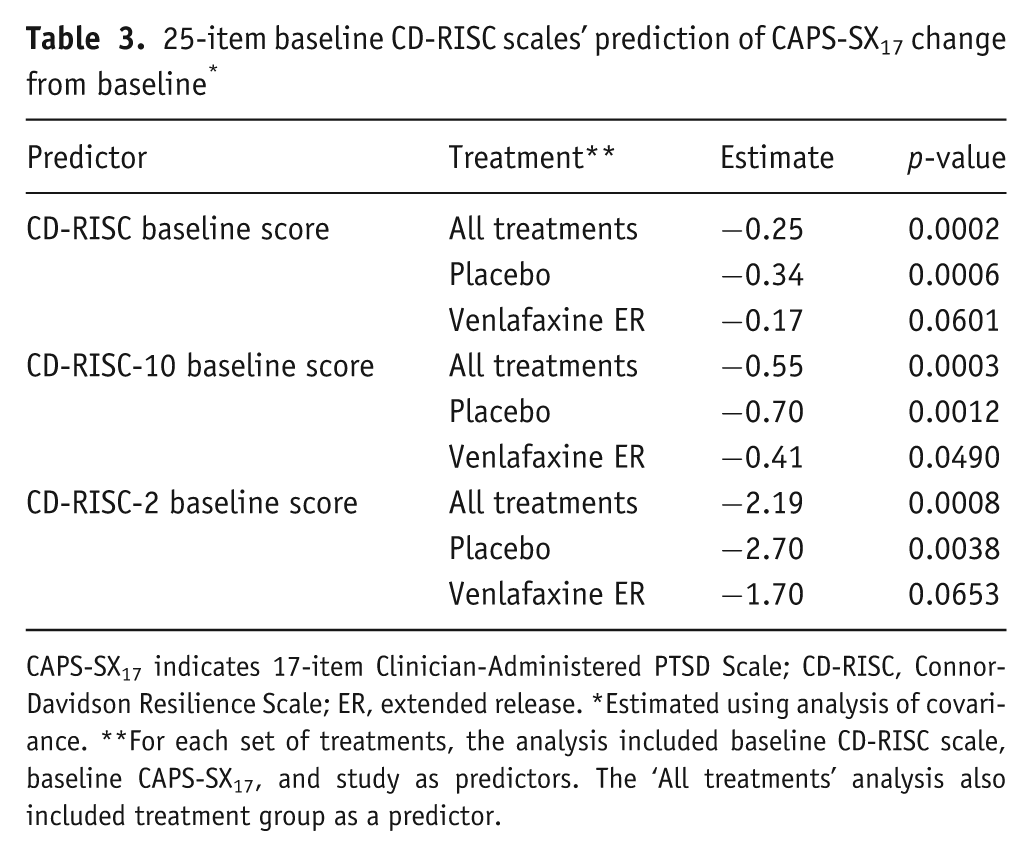
CAPS-SX17 indicates 17-item Clinician-Administered PTSD Scale; CD-RISC, Connor-Davidson Resilience Scale; ER, extended release. *Estimated using analysis of covariance. **For each set of treatments, the analysis included baseline CD-RISC scale, baseline CAPS-SX17, and study as predictors. The ‘All treatments’ analysis also included treatment group as a predictor.
Discussion
The major finding of this pooled analysis is that pretreatment resilience is predictive of positive treatment outcomes in patients with PTSD treated with venlafaxine ER or placebo. The findings we describe here go beyond our earlier analyses of the effect of venlafaxine ER treatment on resilience in patients with PTSD by exploring the predictive value of the scale in the treatment of PTSD. Using the three versions of the CD-RISC, we found that a higher degree of resilience at baseline was associated with a greater likelihood of achieving remission after 12 weeks of treatment with either venlafaxine ER or placebo. This result held up, even after taking into account the effects of PTSD symptom severity and venlafaxine ER treatment, which were separately found to be associated with a positive treatment response. The predictive influence of baseline resilience remained when each treatment group was assessed individually, suggesting that the more resilient patients with PTSD are more likely to do well after receiving 12 weeks of treatment with active drug or placebo. Scores on the shorter versions of the CD-RISC also were found to be predictive of treatment response. These results are consistent with those described by Camardese et al. (2007) who found that patients with MDD who had a greater degree of resilience, also measured with the CD-RISC, were more likely to remit when receiving active drug therapy.
Resilience is one of several factors that may determine the risk of developing or recovering from PTSD. It may, for example, influence (or be affected by) cognitive styles related to optimism and self-efficacy. For instance, perceived threat levels, mediated by an individual’s confidence in his/her ability to adapt to stressful situations, may play a role in how that person responds to threats. It has been proposed that those who lack the belief that they can emerge from a potentially catastrophic event without significant, long-term, negative consequences may be at a greater risk for developing PTSD. Benight and Harper (2002) suggest that the presence of high coping self-efficacy plays a role in preventing a natural acute stress response from becoming pathological PTSD. In a 2-year, prospective, follow-up study of firefighters, a low level of pretraumatic self-efficacy significantly predicted the development of PTSD symptoms (Heinrichs et al., 2005). In addition, other studies have demonstrated that resilience, in the form of self-efficacy, affects responses to traumatic experiences (Benight et al., 1997; Saigh et al., 1995), as well as to PTSD treatment response (Benight and Bandura, 2004).
One priority for clinicians may be to identify patients who have low levels of pretreatment resilience, and as a result may be less likely to respond to first-line treatment. For these patients, the incorporation of resilience-promoting approaches that enhance optimism and tenacity might bring an added benefit and protection from further episodes of PTSD. Such approaches could involve pharmacotherapy, psychotherapy, or other treatment modalities (e.g. meditation, altruistic service) (Davidson et al., 2003, 2005; Fava et al., 1998, 2005; Pagano et al., 2004). In addition, identifying those aspects of resilience, whether biological or psychological, which are prognostic for recovery, may lead to improved treatments for PTSD.
Fully exploring the neurobiology of resilience is beyond the scope of this report, but Charney et al. (2004) concluded that many systems are involved in successful adaptation to severe stress: reward, motivation, fear, memory, and social behavior. Numerous neurotransmitters, neuropeptides, and neurohormones, including serotonin, norepinephrine, dopamine, and neuropeptide Y, are likely to be involved in the neural mechanisms underlying resilience. It has also been proposed that an endophenotype is associated with resistance to hopelessness in the face of stress which is characterized by a more highly functional dopamine system (Charney, 2004; Lenox et al., 2002).
We hoped our results would deepen the understanding of the relationship between specific features of resilience and venlafaxine treatment by exploring how the individual CD-RISC items relate to treatment response. We did not obtain any consistent findings, however, although an association was found to exist between optimism/tenacity (CD-RISC item 16) and a positive response. We expect that to find such relationships, a larger, more homogeneous, sample would be required.
Several limitations, such as the limited data collected about the experienced traumas, are worth noting. For instance, if we knew the age at which the trauma occurred or the time elapsed since the trauma, it may have been possible to determine how such factors relate to treatment response and resilience. In addition, the CD-RISC measures agreement with statements about resilience, and therefore may not fully correspond with resilient actions or behaviors, which potentially may be assessed using more objective means (Morgan III et al., 2000). Furthermore, the exclusion criteria used in these studies established a population that may not be representative of the overall population of patients with PTSD in the community. Within this PTSD population, the predictors we found may, to some extent, characterize patients who are more likely to recover during a 12-week treatment period. However, despite these limitations, to the best of our knowledge, this population comprises one of the largest in which the effect of resilience was assessed as a predictor of response in a controlled trial. Future research is warranted to further clarify the relationship between resilience and treatment response in PTSD and other conditions, such as depression, mild traumatic brain injury (Hoge et al., 2008), and suicidal behavior associated with substance abuse (Camardese et al., 2007; Roy et al., 2007). Further study could determine whether treatments that promote resilience as a whole, or just in certain aspects, can provide further benefit, as suggested in the case of depression and generalized anxiety disorder (Fava et al., 1998, 2005).
Footnotes
This analysis was sponsored by Wyeth Research, Collegeville, Pennsylvania, which was acquired by Pfizer Inc. in October 2009. Medical writing support for this manuscript was funded by Wyeth and was provided by Dennis Stancavish, MA, of Embryon, LLC, A Division of Advanced Health Media, LLC (formerly Medesta Publications Group, A Business of Advogent).
Jonathan Davidson, MD conflict of interest disclosures over past 12 months: Speaking: Glaxo Smith Kline, CME Institute of Physicians Postgraduate Press Research and Other. Support: None. Stock: None. Advisor: Astra Zeneca. Royalties and Licence Fees: Connor-Davidson Resilience Scale, Multi Health Systems Inc. (for Davidson Trauma Scale), Guilford Publications, American Psychiatric Association, Social Phobia Inventory.
Dan J. Stein, MD, PhD has received research grants and/or consultancy honoraria from Astrazeneca, Eli-Lilly, GlaxoSmithKline, Jazz Pharmaceuticals, Johnson & Johnson, Lundbeck, Orion, Pfizer, Pharmacia, Roche, Servier, Solvay, Sumitomo, Takeda, Tikvah, and Wyeth.
Barbara O. Rothbaum, PhD does not have any conflict of interest to disclose related to this paper.
Ron Pedersen Employee: Pfizer. Stock/Shareholder: Pfizer.
Annette Szumski, MA Employee: Pfizer.
David S. Baldwin makes the following declaration of interests: I do not have shares in any pharmaceutical company, nor do family members. I do not accept any personal retainer from any pharmaceutical company. I have acted as a consultant to a number of companies with an interest in anxiety disorders (Asahi, AstraZeneca, Cephalon, Eli Lilly, GSK, Lundbeck, Organon, Pharmacia, Pierre Fabre, Pfizer, Roche, Servier, Sumitomo, Wyeth). I hold or have held research grants (on behalf of my employer) from a number of companies with an interest in anxiety and depressive disorders (Cephalon, Eli Lilly, GSK, Lundbeck, Organon, Pfizer, Pharmacia, Roche, Wyeth). I have accepted paid speaking engagements in industry supported satellite symposia at international and national meetings. I do not accept hospitality or travel not related to a speaking engagement. I am co-author of the British Association for Psychopharmacology evidence-based guidelines on the treatment of anxiety disorders. I am a medical patron of Anxiety UK (formerly National Phobics Society).