
Abstract
Sensory gating, indexed by P50 suppression, and sensorimotor gating, indexed by prepulse inhibition (PPI), are impaired in schizophrenia spectrum disorders. There is considerable evidence that schizophrenia patients treated with atypical antipsychotics exhibit relatively less gating deficits than do other patients with schizophrenia. Some recent studies have investigated the effects of antipsychotic medications on gating in healthy volunteers exhibiting low levels of gating, rather than in patients. Therefore, the current study investigated the influence of sertindole versus placebo in two separate experimental sessions, on PPI, P50 suppression, and cognition in 30 male volunteers stratified for low and high baseline gating levels. Sertindole increased PPI and P50 suppression in healthy subjects exhibiting low baseline PPI and low baseline P50 suppression, respectively, while sertindole attenuated gating in subjects exhibiting high baseline gating. Furthermore, subjects exhibiting low PPI chose worse strategies in a spatial working memory task. These findings suggest that mixed D2/5-HT2 receptor antagonists enhance both PPI and P50 suppression in a way that enhances it in healthy subjects exhibiting low baseline gating. Furthermore, the results militate in favor of the concomitant assessment of PPI, P50 suppression and cognitive measures while investigating the effect of antipsychotic medication in healthy subjects.
Introduction
Gating, an essential feature of early information processing, reflects the ability to inhibit extraneous stimuli and to attend to salient features of the environment. Two measures used to operationalize gating are prepulse inhibition (PPI) of the acoustic startle response, considered a form of sensorimotor gating, and suppression of the P50 auditory event-related potential (AEP) in a condition–test paradigm (P50 suppression), reflecting sensory gating. PPI refers to the attenuation of the reflexive startle reaction elicited by an intense pulse stimulus when its presentation is preceded shortly (30–300 ms) by a weak prepulse stimulus (Graham, 1975; Hoffman and Ison, 1980). P50 suppression refers to the decrement of the P50 AEP to the second stimulus (S2) versus the first stimulus (S1) of two identical auditory stimuli presented in succession at an interstimulus interval of approximately 500 ms. It has been shown repeatedly that both PPI and P50 suppression are impaired in schizophrenia spectrum disorders (Adler et al., 1982, 2004; Baker et al., 1987; Cadenhead, 2002; Csomor et al., 2008a; Light and Braff, 1999; Perry et al., 2001). Theoretically, deficient gating is associated with a general reduction of the ability to gate intrusive sensory, motor, and/or cognitive information (Braff and Geyer 1990; Geyer et al., 1987).
There is considerable evidence suggesting that schizophrenia patients treated with atypical antipsychotic medications exhibit relatively less PPI and P50 suppression deficits than do other patients with schizophrenia (Adler et al., 2004; vrim-Ucok et al., 2008). In order to bridge the gap between basic and clinical research, some recent studies have investigated the effects of antipsychotic medications on gating in healthy volunteers exhibiting low levels of gating, rather than in patients. In this context, it has been shown that clozapine, as well as quetiapine, increased PPI in healthy subjects exhibiting low levels of sensorimotor gating at baseline (Swerdlow et al., 2006b; Vollenweider et al., 2006). In contrast, the typical antipsychotic haloperidol does not have such a PPI-enhancing effect (Csomor et al., 2008a). The translational approach of examining pharmacological manipulations in healthy individuals exhibiting naturally low levels of gating has also been adopted in a study assessing P50 suppression. Our group has shown that haloperidol increases P50 suppression in subjects exhibiting low P50 gating while it attenuated P50 suppression in subjects with high P50 gating (Csomor et al., 2008a). Others (Knott et al., 2009) have used a similar approach to localize the sources of the P50 response. Such concepts based on a selected cohort of healthy volunteers exhibiting traits similar to those observed in patients (i.e. low gating) might be useful in translational medicine as part of the discovery cycle in the search for novel compounds with antipsychotic properties.
The current study investigates the influence of the atypical antipsychotic sertindole, which acts as a potent antagonist at dopamine D2 receptors, serotonin 5HT2A receptors, and α1-adrenoceptors, on gating and cognition in healthy volunteers exhibiting either low or high baseline gating levels. Although no previous studies have investigated the effects of sertindole on PPI or P50 suppression in humans, there is evidence from experiments with rodents that sertindole has the potential to increase PPI (Depoortere et al., 1997; Paabol Andersen and Pouzet, 2001).
Furthermore, we (Vollenweider et al., 2006) and others (Swerdlow et al., 2006b) have shown that antipsychotics such as clozapine and quetiapine, which have preferential antagonistic activity at D2 and 5HT2A receptors, can enhance PPI in healthy subjects with low baseline gating performance. Based on these findings, and the fact that sertindole shares certain mechanisms of action (dopamine D2 and serotonin 5HT2A antagonism) with clozapine and quetiapine (Hertel, 2006), we hypothesized that sertindole would improve sensorimotor and sensory gating in healthy subjects exhibiting relatively low baseline levels of PPI or P50 suppression. In addition, the current investigation assessed the extent to which cognition is modulated by sertindole, and also potential differences in cognitive performance between the low and high gaters. Interestingly, performance in cognitive tasks relying on prefrontal cortical functioning appears to differ between subjects with low and high sensorimotor gating. It has been shown that strategy formation and planning are diminished in healthy volunteers with low levels of PPI (Bitsios et al., 2006; Csomor et al., 2008a; Giakoumaki et al., 2006). With a translational approach in mind, these impairments parallel the findings of cognitive deficits, especially measured by (pre)frontal tasks, in schizophrenia spectrum disorders (Badcock et al., 2005; Hutton et al., 1998; Manoach, 2003; Minzenberg et al., 2009; Weickert et al., 2000).
In summary, we hypothesized that a moderate but clinically relevant dose of sertindole would enhance PPI and P50 suppression in healthy volunteers exhibiting low baseline gating. Furthermore, we predicted a replication of previous findings of reduced cognitive ability in subjects with low sensorimotor gating. To this end, healthy male volunteers stratified for low and high baseline gating levels were given12 mg (p.o.) sertindole and placebo in two separate experimental sessions, and PPI, P50 suppression, and cognition were assessed.
Methods and materials
Subjects
In total, 30 healthy male volunteers were recruited by local advertisement. Due to the reported gender differences in PPI (Swerdlow et al., 1993), only male subjects were included. The study was approved by the ethics committee of Zurich canton and Swissmedic. All subjects gave their informed written consent, were without a history of mental and neurological disorders, had no history of an axis I disorder amongst their first-degree relatives, were free of any medication, and denied the use of illicit drugs, which was confirmed by urine toxicology. To ascertain the subjects’ mental status, all subjects were screened by the DIA-X diagnostic expert system (Wittchen and Pfister, 1997), a semi-structured psychiatric interview and the Hopkins Symptom Checklist (SCL-90-R) (Derogatis, 1977). Furthermore, all of the volunteers underwent clinical examination that included electrocardiography and blood analysis. Hearing was evaluated in all subjects, using a pure tone (tone frequencies: 500, 1000, 2000, 4000, 6000 Hz) audiometer (Earscan 3, Micro Audiometrics Corp, NC, USA). None of the subjects was excluded due to hearing difficulties (hearing threshold >30 dBHL). All subjects were instructed to abstain from drinking alcohol for at least 24 h before each test session, not to drink any caffeine-containing beverages on the day of testing, and to keep their usual smoking habits. Potential drug abuse was checked by urine toxicology. Smoking was not allowed for 1 h prior to the recording session.
Experimental design
In a double-blind, placebo-controlled within-subjects design, participants received orally 12 mg sertindole (4 + 4 + 4 mg given at 24-h intervals) or placebo (0 + 0 + 0 given at 24-h intervals) in two experimental blocks 14–21 days apart. Sertindole (Serdolect®) and placebo (lactose) was obtained from Lundbeck (Lundbeck AG, Glattbrugg, Switzerland). On each experimental day, 8 h after the last drug administration (sertindole maximum plasma levels are reached at about 8–10 h after administration), subjects underwent the PPI assessment followed by a short break prior to the P50 suppression session. After detaching all electrodes used in the electrophysiological recordings, subjects underwent neuropsychological testing using a subset of CANTAB tests. After testing, subjects were monitored clinically until side effects were diminished.
PPI and P50 suppression session definition
The PPI test session was composed of a mixture of pulse-alone trials, prepulse–pulse trials and trials in which no discrete stimulus other than the constant background noise was presented (denoted hereafter as ‘no-stimulus’ or ‘NS trials’). All stimuli (background noise, pulses, and prepulses) used in the experiment consisted of broadband white noise. The intensity of the background noise was set at 70 dBA. Pulse stimulus intensity was set at 115 dBA and the prepulse stimulus intensity at 86 dBA. The stimulus duration was 40 ms for pulse stimuli and 20 ms for prepulse stimuli. Rise and fall times of the stimuli were less than 1 ms. The four stimulus onset asynchronies (SOA) between the prepulse and pulse stimuli on prepulse–pulse trials were 30, 60, 120, and 2000 ms (SOA 30, SOA 60, SOA 120, and SOA 2000). The session began with a 2-min period of acclimatization to the background noise, followed by the presentations of 47 discrete trials according to a variable intertrial interval ranging from 7–13 s (mean: 9.9 s). The first block consisted of three consecutive pulse-alone trials, although data from the first trial were discarded. The last block consisted of two consecutive pulse-alone trials. The middle block consisted of 42 trials, that is seven trials of each of the six conditions (pulse-alone, prepulse–pulse combinations, and NS trial). The sequence of presentation was pseudo-randomized. The PPI test session lasted approximately 11 min.
The P50 suppression test session was composed of 80 pairs of auditory clicks with a 500-ms interclick interval presented every 10 s. Stimuli consisted of 85 dBA white noise with a duration of 1 ms. The P50 suppression session lasted for approximately 15 min.
Apparatus, data recording and data processing
Detailed information about apparatus and data processing can be found elsewhere (Csomor et al., 2008a). In short, a sampling rate of 4096 Hz for the PPI paradigm, and 512 Hz for the P50 paradigm was used. For the PPI paradigm, electromyography (EMG) activity was band-pass filtered (30–500 Hz), downsampled to 1000 Hz, and then rectified. Segmentation was performed from 50 ms prior to the onset of the relevant stimulus (the prepulse in prepulse–pulse trials, and the pulse in pulse-alone trials), and lasted to 2300 ms after stimulus onset for the PPI trials, and to 450 ms for the startle trials. EMG data were smoothed (time constant: 5 ms), and every trial was scored separately using emgBLINK version 1.2 (CST, Switzerland). Baseline amplitude was calculated by the mean response amplitude of the first 50 ms before pulse stimulus onset. Stimulus response amplitudes were assessed as peak response minus baseline value of the respective trial. Peak response was defined as the highest reaction in the time window between stimulus onset and 150 ms after stimulus onset. Response amplitudes on NS trials were scored as peak response sampled between 51 and 201 ms minus baseline value of the respective trial. Every trial was examined for sign of corrupted EMG signal.
P50 suppression data were band-pass filtered (2–70 Hz, 50 Hz notch). Independent component analysis was used to remove artifacts due to eye movements and blinks, electroencephalography data were re-referenced to the average and segmented from 500 ms before to 1000 ms after the first click. For P50 amplitude, the artifact-free segments were band-pass filtered (10–40 Hz) and then re-segmented 100 ms before click onset to 400 ms after click onset separately for both stimulus conditions (S1 and S2) and then averaged. The P50 component of the AEP was identified as the most positive deflection 40–80 ms after stimulus presentation and scored as described elsewhere (Nagamoto et al., 1989). The P50 amplitude was scored as the absolute difference between the P50 peak and the preceding negative trough. Only data from the Cz location were analyzed where the maximum activity for the P50 AEP was expected (Clementz et al., 1998).
Assessed parameters
For the PPI paradigm, the following startle measures were examined: (1) Pulse-alone: the mean startle reactivity elicited by the pulse-alone stimulus in each of the three pulse blocks was calculated for each subject; (2) PPI: Percentage PPI (%PPI) was calculated for each SOA by the formula: [(1-(amplitudeprepulse-pulse)/(amplitudepulse-alone(block2))] × 100%; (3) Percentage Habituation: The reduction of the startle amplitudes between the first and last blocks was calculated according to the formula: [1-(amplitudepulse-alone(block3))/(amplitudepulse-alone(block1))] × 100%.
For the P50 suppression, paradigm the following AEP measures were examined: (1) P50 amplitudes evoked by S1 and S2; (2) P50 suppression: Percentage P50 suppression was calculated by the formula: [1-(amplitudes2)/(amplitudes1)] × 100%; (3) Latency of P50 amplitudes1 and amplitudes2.
As summarized briefly below, three tests of the CANTAB were administered using an IBM-compatible PC with a touch-screen monitor (Elo IntelliTouch®, Tyco Electronics, PA, USA): (1) Motor screening (MOT): all subjects were introduced to the touch-screen procedure by completing a simple motor screening task consisting of touching the center point of flashing crosses on the screen as soon as possible after its presentation; (2) Rapid visual information processing (RVP): this task is a visual continuous performance task using predefined sequences of three digits presented at a rate of 100 per minute so as to assess sustained attention over a period of 4 min. RVP performance was assessed by total correct responses to target sequences (total hits), the sensitivity to detect target sequences (A’), the signal detection measure of the strength of trace required to elicit a response (B’), and the mean latency to target sequences; (3) Spatial Working Memory (SWM): this is a test of spatial working memory and strategy performance. The subject had to find a blue ‘token’ in each displayed box, while not returning to boxes in which a blue token had already been found. Performance was indexed by a strategy score, which represents the number of times the subject begins a new search with the same box. A high score represents poor use of this strategy and a low score equates to effective use. Furthermore, the total number of errors and between errors (searching a token in a box where one had already been found) was assessed.
Statistical analysis
All statistical analyses were conducted using the statistical software Statistica 7 for Windows (Statsoft Inc., OK, USA).
The distribution of the startle amplitudes in patients and controls was positively skewed in most of the blocks. In the P50 suppression paradigm distribution, most of the S1 and S2 amplitudes were positively skewed. After ln-transformation, startle amplitudes did not deviate significantly from normality. Similarly, square-root-transformation (sqrt-transformation) of P50 amplitudes elicited by S1 and S2 resulted in a normal distribution. While statistical comparisons of pulse-alone elicited startle reactivity were based on ln-transformed startle data and P50 amplitudes were based on sqrt-transformed P50 amplitudes, the calculation %PPI and %P50 suppression were based on non-transformed data. Furthermore, analyses of P50 latencies were based on non-transformed data.
Startle and PPI data from eight subjects were not included in the final analysis (due to a startle amplitude of <10 µV), reducing the sample to 22 valid subjects. Startle amplitudes were analyzed using repeated measures analysis of variance (ANOVA) block (1 to 3) and treatment (placebo vs. sertindole) as within-subject factors and group (low vs. high) as between-subject factors. Similarly, %PPI values for the inhibitory SOAs (30, 60, 120 ms) were subjected to a 3 × 2 × 2 (SOA × treatment × group) repeated measures ANOVA. Analyses of prepulse facilitation (PPF) (SOA: 2000 ms), NS stimulus condition, and %habituation were done separately using one-way ANOVAs.
P50 suppression data of five subjects had to be excluded because no distinct P50 component could be identified, reducing the sample to 25 valid subjects. P50 amplitude and latency were analyzed by separate repeated-measures ANOVAs with stimulus number (S1 and S2) and treatment (placebo vs. sertindole) as within-subject factors and group (low vs. high) as between-subject factor. The %P50 suppression data were analyzed by a 2 × 2 (treatment × group) repeated-measures ANOVA.
To test whether sertindole has a differential effect on subjects exhibiting low or high placebo gating measures, subjects were grouped by a median-split procedure into low and highperformers. For PPI, this split was based on the resultsof %PPI in the SOA 60 placebo condition (medianPPI = 60.92%). Similarly, for the P50 suppression paradigm, the median split was applied using the %P50 suppression scores in the placebo condition (medianP50 = 43.40%). An alternative grouping by a mean split was considered (meanPPI = 57.50%; meanP50 = 43.31%), but was found to result in almost identical PPI groups, differing only by three subjects, and virtually the same P50 groups, differing only by one subject.
CANTAB was recorded successfully in all 30 subjects. Separate two-way ANOVAs with group (separately for P50 and PPI low and high subgroups) and treatment were used to examine the effect of sertindole on the performance of MOT and RVP CANTAB tasks. For the SWM task, the additional factor ‘difficulty’ was introduced.
Similarly, differences in SCL-90 global factor scores between the high and low gating subgroups were assessed by separate one-way ANOVA.
For all statistical tests, the significance level was set to p < 0.05. Post-hoc pair-wise comparisons were conducted using Fisher’s Least Significant Difference (Fisher LSD). In the case of significant effects, the effect size expressed as partial eta-squared
Results
Subjects demographics and psychometric measures
The low and high subgroups, stratified according to either PPI or P50 suppression, did not differ in age, IQ, or alcohol or nicotine consumption. Furthermore, the groups did not differ in the SCL-90 global indices or subscale scores (see Table 1 and Table 2).
Demographic characteristics and SCL-90 scores of the subjects stratified into low and high PPI groups
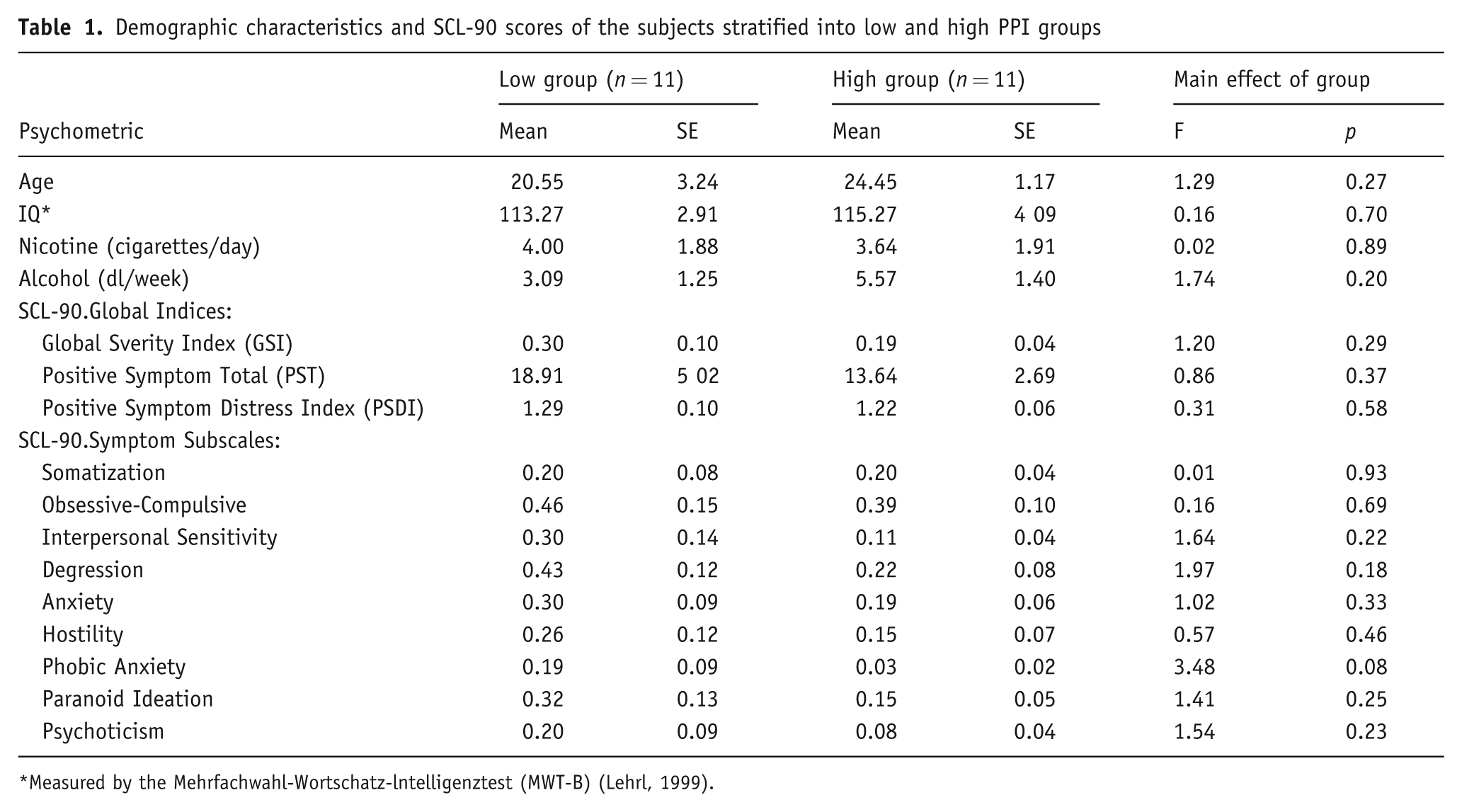
Measured by the Mehrfachwahl-Wortschatz-lntelligenztest (MWT-B) (Lehrl, 1999).
Demographic characteristics and SCL-90 scores of the subjects stratified into low and high P50 groups
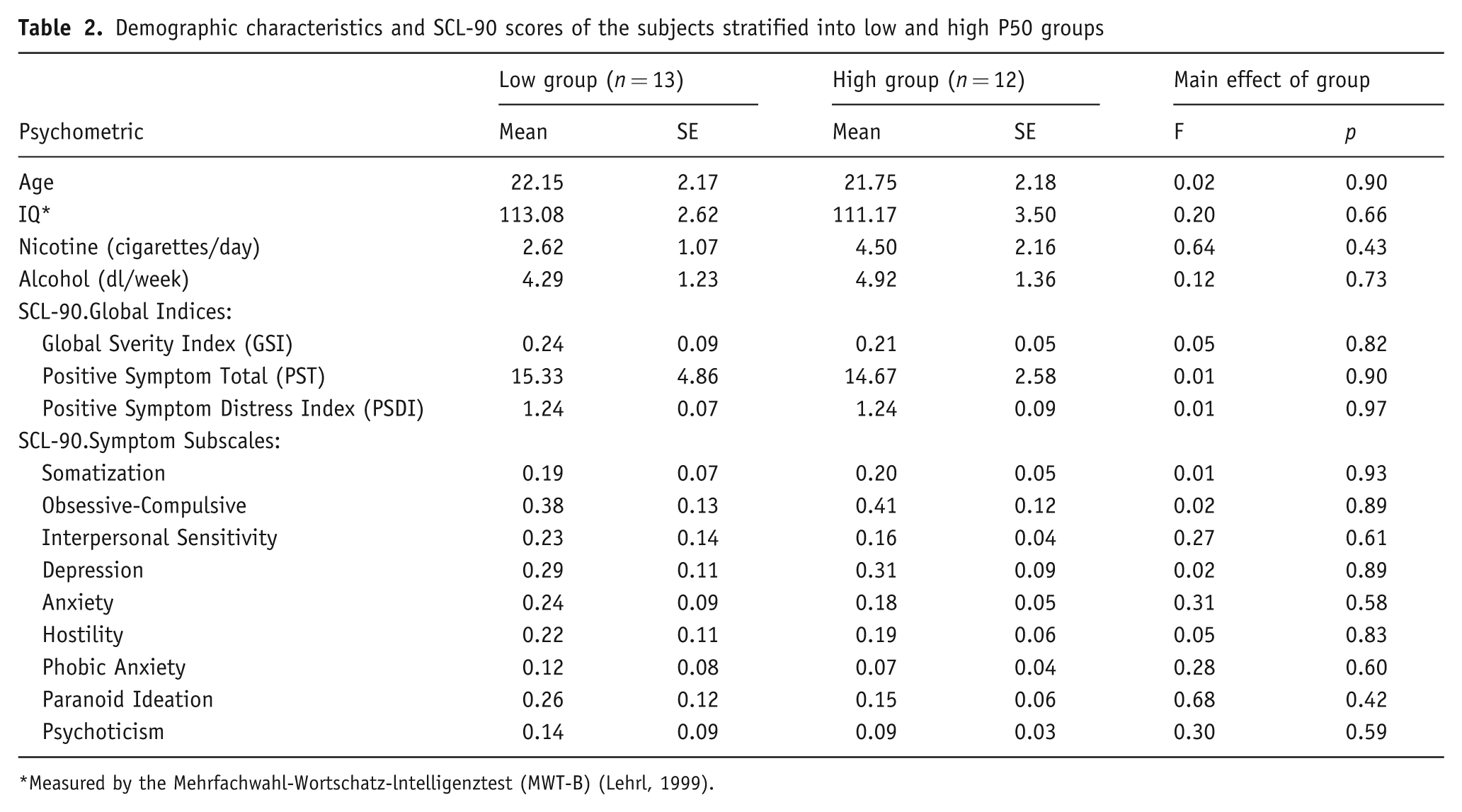
Measured by the Mehrfachwahl-Wortschatz-lntelligenztest (MWT-B) (Lehrl, 1999).
Prepulse inhibition paradigm
Neurophysiological characteristics of PPI assessment are summarized in Table 3.
PPI characteristics of low and high gating groups receiving treatment with placebo or sertindole
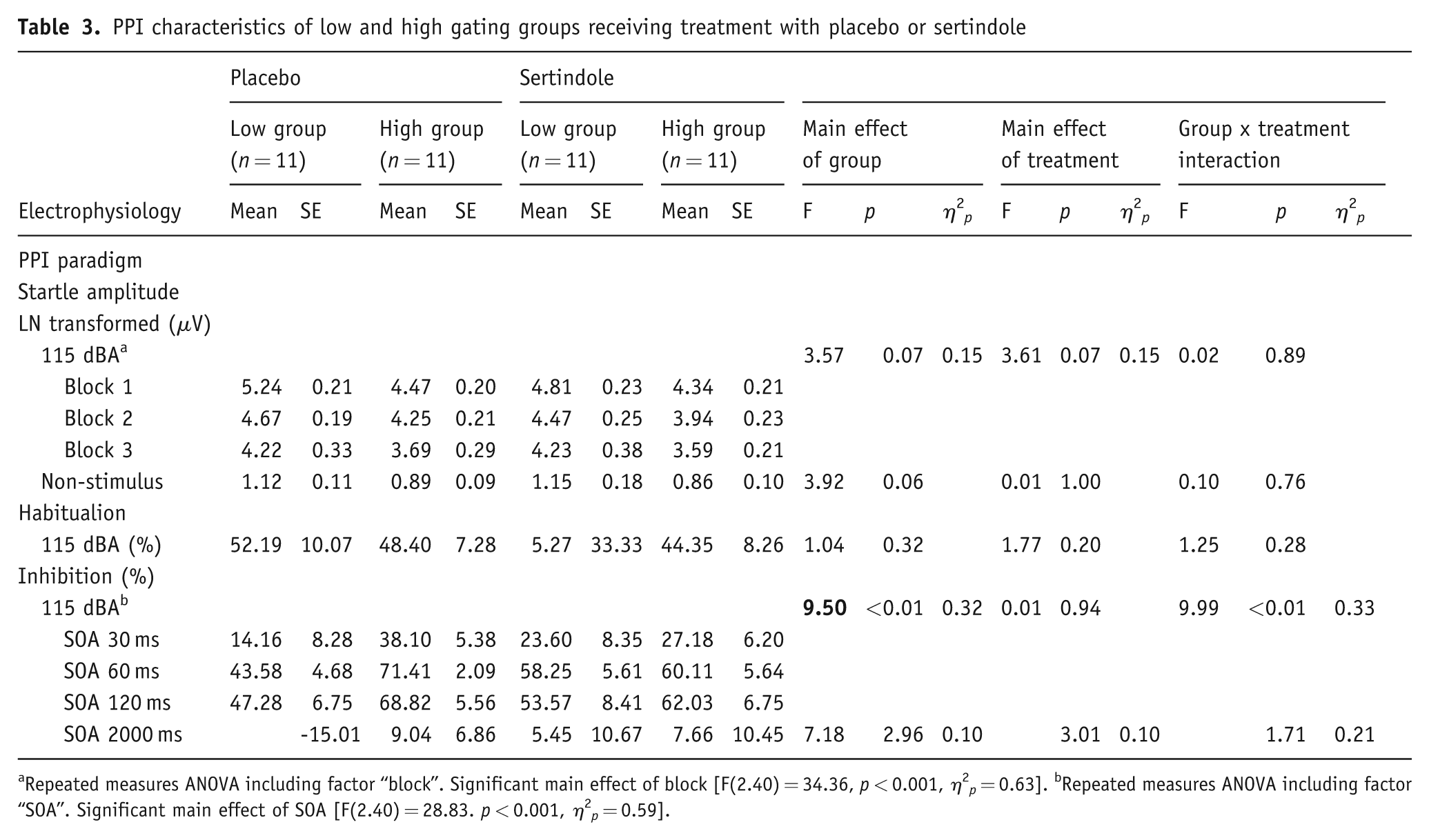
Repeated measures ANOVA including factor “block”. Significant main effect of block [F(2.40) = 34.36, p < 0.001,
Startle reactivity
Startle amplitude between the low and the high subgroup exhibited a statistical trend for higher startle in the low PPI subgroup. As expected, startle amplitude significantly diminished over the three blocks of the test session. Post-hoc pair-wise comparisons revealed no differences in startle reactivity in relation to treatment condition and block between the two groups. Moreover, treatment with sertindole yielded a statistical trend (p = 0.07) for reduced startle reactivity. To further investigate the influence of sertindole on startle reactivity, additional one-way ANOVA of startle reactivity in the PPI-relevant block 2 with factors group and treatment was performed, revealing a significant main effect of treatment [F(1,20) = 10.49, p < 0.01,
Prepulse inhibition
%PPI was significantly different between the two groups due to the median-splitting of subjects into low and high sensorimotor gaters. As expected, there was a significant main effect of SOA. Moreover, results of the ANOVA revealed a significant treatment × group interaction. Post-hoc pair-wise comparisons revealed that sertindole significantly increased %PPI in the low subgroup (p < 0.05) while it decreased it in the high subgroup (p < 0.05). There was no significant interaction for treatment × SOA × group. Nevertheless, based on our a priori hypothesis that sertindole would modulate PPI differentially in subjects with high or low baseline %PPI levels and due to the findings of our earlier study, where clozapine influenced PPI in low-gating subjects at short SOAs (Vollenweider et al., 2006), post-hoc pair-wise comparisons were performed. Sertindole treatment increased %PPI in the low PPI group at the SOA 60 (p < 0.05), but did not attenuate PPI significantly in the high group or in other SOA conditions in the low group (Figure 1). Additional analysis was done by the use of %P50 suppression group splitting for PPI. Except for SOA [F(2,36) = 25.25, p < 0.001,
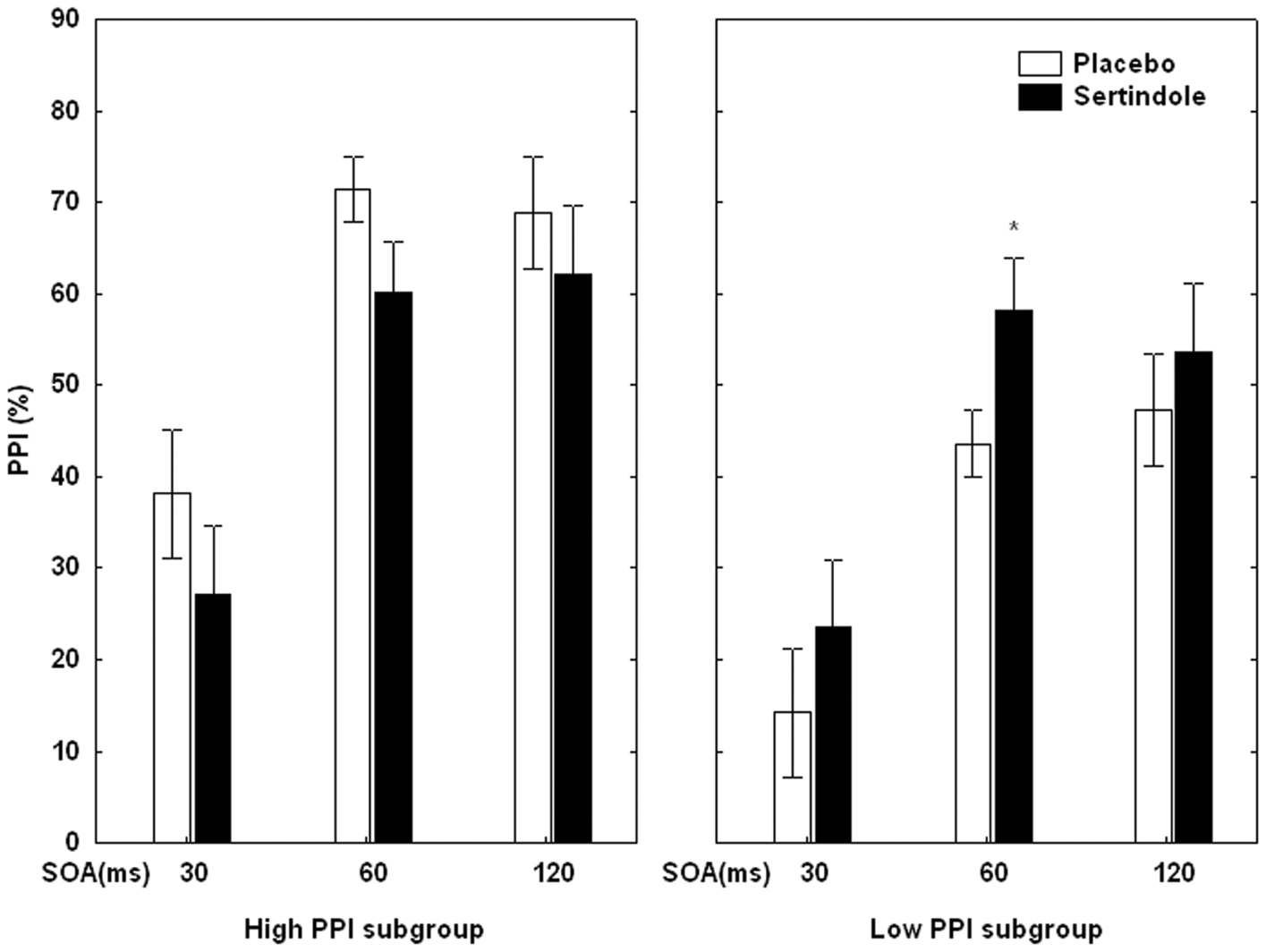
Percentage PPI at the three prepulse-pulse conditions (SOA: 30, 60, and 120 ms) in the low and the high PPI subgroups during placebo (white bars) and sertindole (black bars) treatment. Error bars refer to ±SE. PPI, prepulse inhibition; SOA, stimulus onset asynchrony.
PPF
PPF induced by the SOA condition of 2000 ms did not differ between the low and high subgroups and was not affected by sertindole treatment.
Habituation
There were no significant treatment effects or any significant interactions between the two subgroups on habituation of the startle reflex.
P50 suppression paradigm
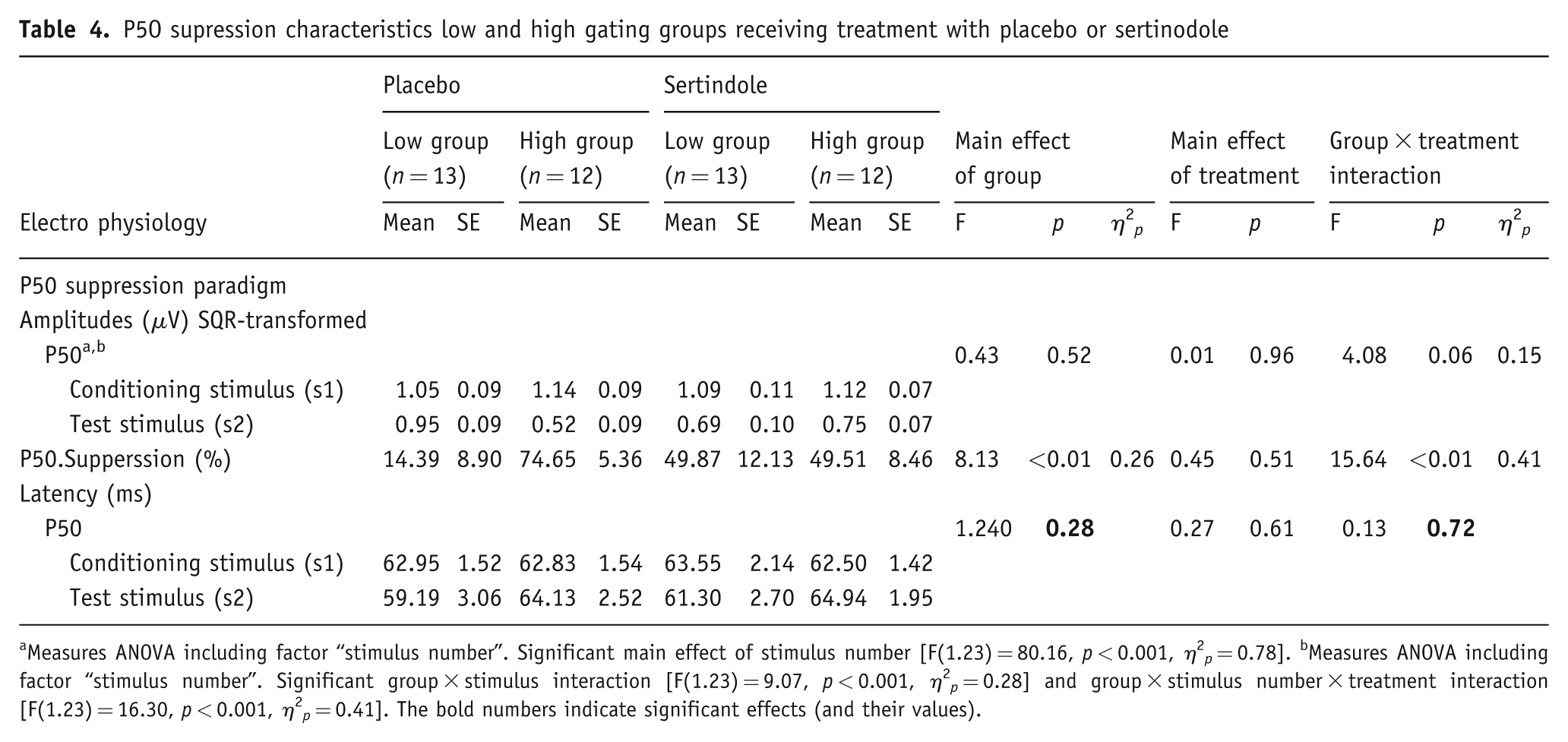
All results are summarized in Table 4.
P5O supression characteristics low and high gating groups receiving treatment with placebo or sertinodole
Measures ANOVA including factor “stimulus number”. Significant main effect of stimulus number [F(1.23) = 80.16, p < 0.001,
P50 amplitude
There was a significant main effect of stimulus number (S1 vs. S2), confirming the occurrence of P50 suppression. The interaction of group × treatment reached a statistical trend level (p = 0.06). Moreover, the interactions of stimulus number × group and stimulus number × treatment × group attained statistical significance. Post-hoc testing revealed that sertindole decreased the amplitude elicited by S2 in low P50 subgroup (p < 0.001) while it increased it in the high P50 subgroup (p < 0.01). No such effect in regard to treatment was found for the amplitude elicited by S1. Furthermore, in the high subgroup, S1 and S2 amplitudes differed significantly in both the placebo (p < 0.001) and sertindole conditions (p < 0.001), while in the low subgroup the two amplitudes differed only in the sertindole condition (p < 0.001). This finding confirms that sertindole increased P50 suppression in the low group due to an increased proportion of the two amplitudes of the two stimuli.
P50 suppression
The low and high groups differed in P50 suppression, indexed by percent suppression, as forced by the splitting of the subject group into low and high P50 gaters. No significant main effect of treatment was found. Moreover, the interaction between treatment and group attained significance. Post-hoc testing revealed that sertindole increased P50 suppression significantly in the low group (p < 0.01) while reducing the high group’s gating performance (p < 0.05). Similarly to the analysis of PPI (see above), an additional analysis was done using the PPI group splitting for %P50 suppression. No significant main effects or interactions were found, clarifying that a group splitting into high and low subjects did not lead to a regression to the mean.
P50 latency
No significant main effects or interactions were found for the factor latency. Correlations between PPI and P50 suppression.
Pearson correlations between PPI and P50 suppression were low and not statistically significant (placebo: r SOA30 = −0.07; r SOA60 = −0.07; r SOA120 = 0.03).
Neuropsychological testing
The high and low PPI subgroups differed in strategy score of the SWM task, indicating superior performance by the high PPI subgroup. Moreover, a significant interaction of treatment × difficulty was found for SWM between errors. Post-hoc comparisons revealed a significant increase of errors in both groups in the most difficult condition under sertindole treatment (p < 0.01). There were no further differences in cognitive performance in the other tests between the two PPI subgroups (see Table 5).
Neuropsychological characteristics of the low and high PPI subgroups receiving treatment with placebo or sertindole
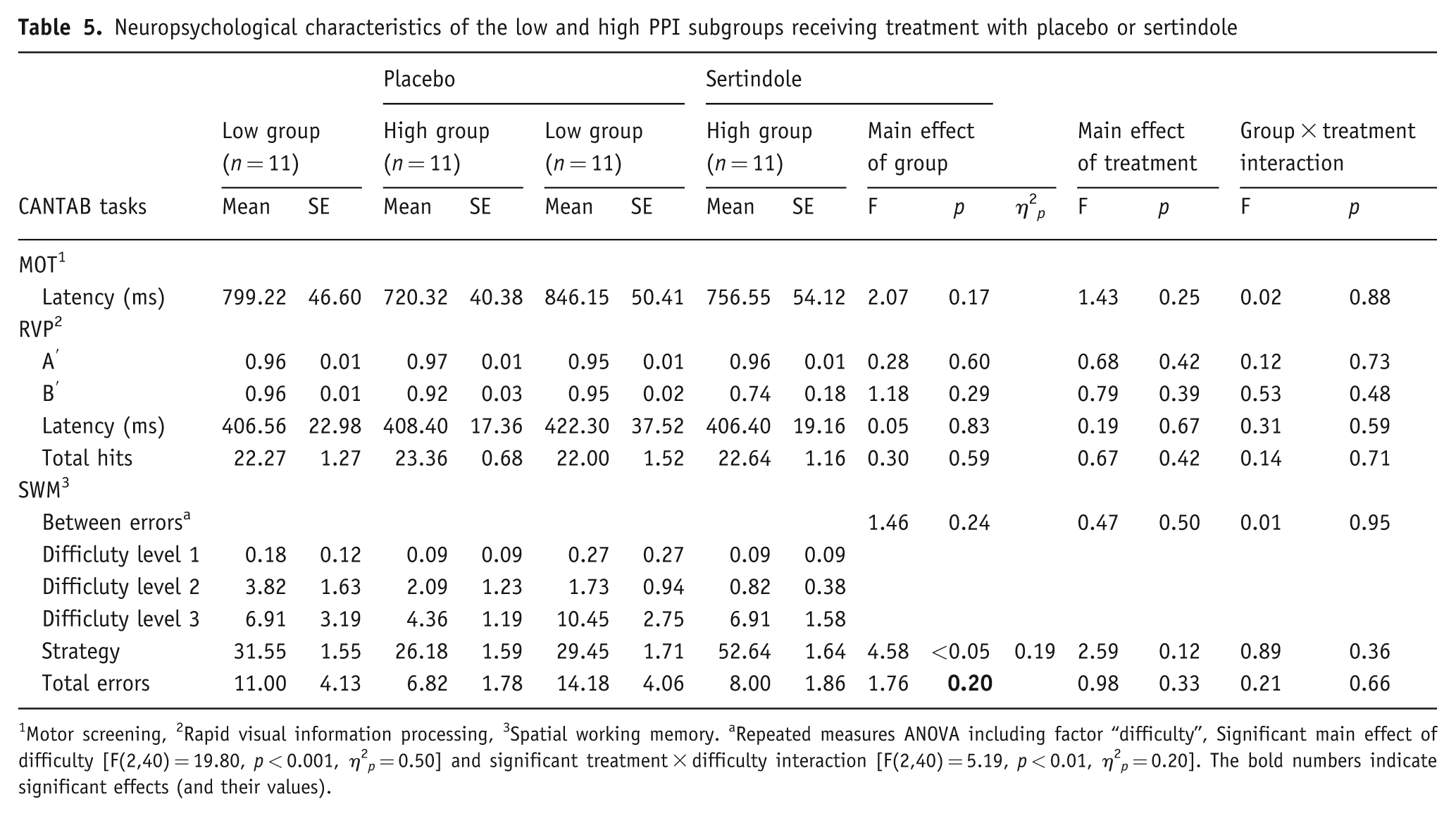
Motor screening, 2Rapid visual information processing, 3Spatial working memory. aRepeated measures ANOVA including factor “difficulty”, Significant main effect of difficulty [F(2,40) = 19.80, p < 0.001,
Analyzing cognitive performance in CANTAB tasks according to high and low P50 subgroups revealed several treatment effects, dependent on group affiliation (see Table 6). Sertindole decreased the high subgroup’s performance in the RVP task, as indicated by a significant group × treatment interaction, indexed as well by A’, and Total hits. Therefore, separate post-hoc comparisons for both measures showed significant decreases for the high group performance (p < 0.05) while no significant effect was found for the low group. Moreover, treatment with sertindole led to a significantly better performance in SWM strategy score, indicated by a significant main effect of treatment, which was limited tothe high P50 subgroup (p < 0.05). Beyond that, a worse performance under sertindole condition in SWM task isdenoted by a significant interaction of the factors treatment × difficulty in SWM between errors, and a significant post-hoc comparison indicating significantly worse performance in the most difficult condition under sertindole treatment (p < 0.05).
None of the Pearson correlations between PPI or P50 suppression versus cognitive performances attained statistical significance. Pearson correlations between %PPI and SWMstrategy score were relatively high but did not attain statistical significance (placebo: r SOA30 = −0.55; r SOA60 = −0.38; r SOA120 = −0.28).
Neuropsychological characteristics of the low and high P50 subgroups receiving treatment with placebo or sertindole
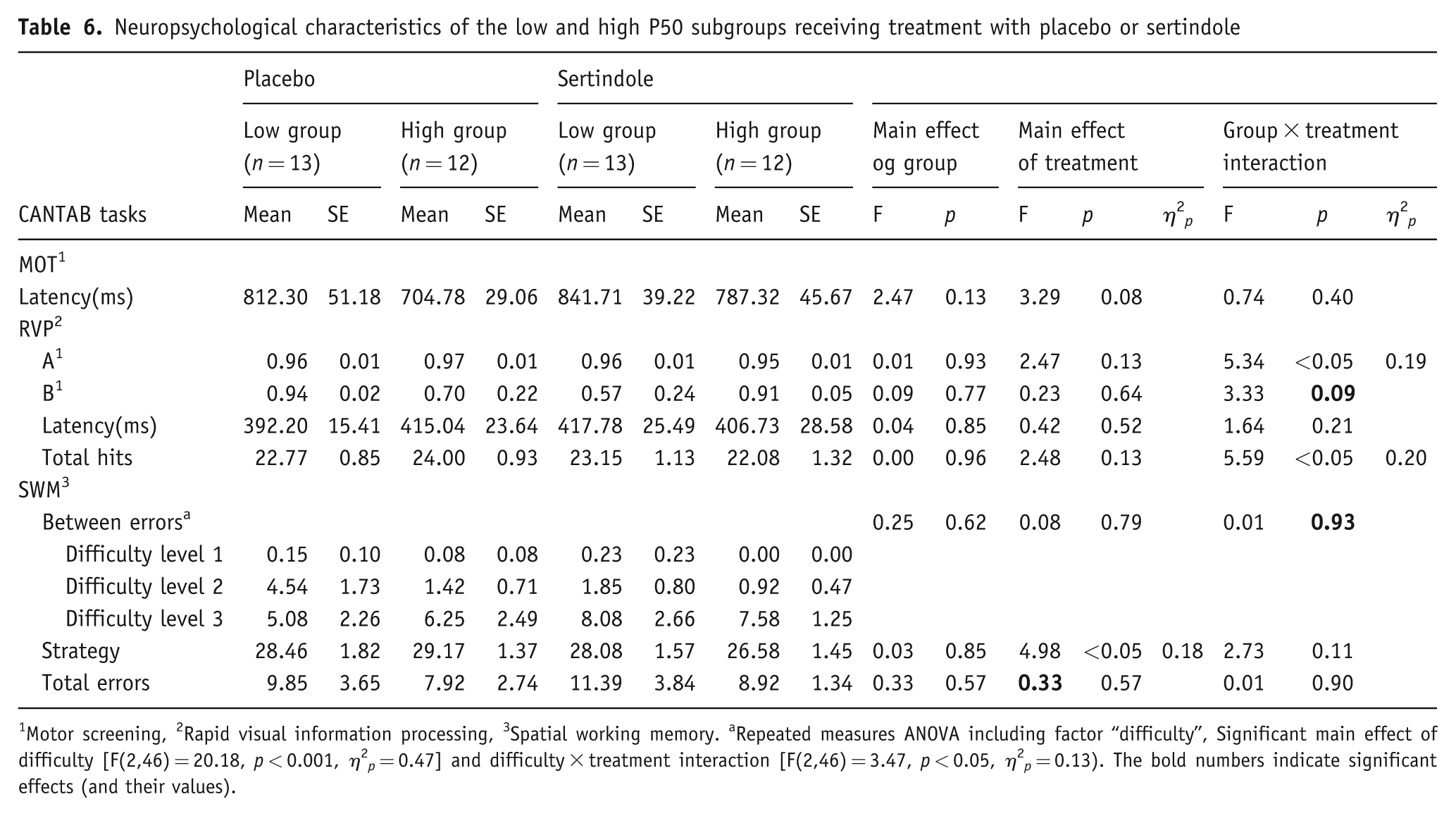
Motor screening, 2Rapid visual information processing, 3Spatial working memory. aRepeated measures ANOVA including factor “difficulty”, Significant main effect of difficulty [F(2,46) = 20.18, p < 0.001,
Discussion
To our knowledge, this is the first study investigating the influence of sertindole on gating measures in humans. The current results revealed that sertindole increases PPI and P50 suppression in healthy subjects exhibiting low baseline PPI or low baseline P50 suppression, respectively. On the other hand, sertindole attenuated PPI and P50 suppression in subjects exhibiting high levels of baseline gating. Cognitive performance as measured by a subset of tests from the CANTAB battery was not generally impaired by sertindole, which is in contrast to previous studies with other antipsychotics (Csomor et al., 2008a; McCartan et al., 2001; Vollenweider et al., 2006). Furthermore, subjects exhibiting low PPI at baseline performed significantly worse in the SWM strategy score compared with subjects with high PPI, which is a replication of previous findings (Bitsios et al., 2006; Csomor et al., 2008a; Giakoumaki et al., 2006).
Prepulse inhibition
In accordance with previous studies investigating the effect of atypical antipsychotic medications on sensorimotor gating (Swerdlow et al., 2006b; Vollenweider et al., 2006), treatment with sertindole increased PPI in subjects exhibiting low baseline gating.
Even though the present results of a PPI-increasing effect induced by atypical antipsychotics in healthy volunteers with low baseline gating are in line with previous studies, this effect seems not as pronounced as seen with clozapine (Vollenweider et al., 2006) or quetiapine (Swerdlow et al., 2006b). Sertindole significantly increased low levels of PPI primarily at the SOA 60 ms condition, consistent with the effect of clozapine to low PPI level at SOA 60 and 120 ms (Vollenweider et al., 2006). In contrast, quetiapine exerted its PPI-elevating properties at short SOA conditions of 20 and 30 ms (Swerdlow et al., 2006b). PPI of the present low PPIsubgroup under the placebo condition (meanSOA60 = 43.58 ± 4.68%) is comparable with that of our previous study with haloperidol (meanSOA60 = 43.8 ± 13.8%) (Csomor et al., 2008a), but much higher than in the studies with clozapine (meanSOA60 = 8.8 ± 3.3%) (Vollenweider et al., 2006) and quetiapine (%PPI cutoff for low gaters <16%) (Swerdlow et al., 2006b). This difference between studies may have contributed to the fact that the enhancing effect of sertindole was less pronounced compared with the effects of clozapine or quetiapine. To assess this possibility and potentially validate the present findings, additional analyses using the extreme tertiles of the study group (7 vs. 7 subjects) was performed for PPI and for cognitive performance. The results of these analyses (data not shown) were very similar to those found with the median-split approach.
Another possible contributor to these study differences is that clozapine significantly reduced startle reactivity (Vollenweider et al., 2006), which might have influenced the measure of sensorimotor gating as indexed by %PPI (Csomor et al., 2008b). It should be noted, however, that there was a trend for sertindole to attenuate startle reactivity in the present study. A systematic investigation of a potential influence of the magnitude of startle reactivity on PPI suggests that low startle is associated with high PPI and vice versa (Csomor et al., 2008b). However, the sertindole-induced change in startle reactivity does not appear to account for the observed changes in %PPI. After treatment with sertindole, the high PPI group showed a significant decrease of startle in the PPI-relevant block 2. Furthermore, no significant decrease of startle was found for the low group. Although startle reactivity was reduced in the low (block 2: from 129.68 to 115.85 µV, non-transformed) and the high (block 2: from 85.43 to 66.16 µV, non-transformed) subgroup to a similar extent, the PPI enhancement was restricted to the low subgroup. Thus it can be concluded that changes in startle did not account for the observed changes in PPI in the current study.
Nicotine consumption, a potential confounding factor for an increasing effect on PPI (Braff et al., 2001), was controlled in the present study, since the high and low PPI groups had similar smoking habits and were not totally smoking-deprived.
The finding of an enhancing effect of atypical antipsychotics on low PPI gating is in line with the majority of studies showing that patients suffering from schizophrenia treated with atypical antipsychotic medication exhibit PPI values comparable with those of healthy controls (Kumari and Sharma, 2002; Kumari et al., 1999, 2000, 2002, 2007; Leumann et al., 2002; Oranje et al., 2002b; Swerdlow et al., 2006a). Nevertheless, other investigations have observed no beneficial effects of either typical or atypical medication on PPI in schizophrenia patients (Duncan et al., 2003a, 2003b; Perry et al., 2002; Mackeprang et al., 2002). Furthermore, the present results are in line with investigations showing a PPI-increasing effect of sertindole in Wistar rats with low baseline PPI (Depoortere et al., 1997) and rats with amphetamine-disrupted PPI (Paabol Andersen and Pouzet, 2001).
With regard to the discussed neurotransmitter systems relevant for schizophrenia spectrum disorders, animal and human studies have shown that PPI can be modulated by dopaminergic, serotonergic, and glutamatergic interventions (Braff et al., 2001; Geyer et al., 2001; Swerdlow et al., 2000). Sertindole has a mixed receptor profile, acting not only as an antagonist at D2 and 5HT2 receptors (Arnt and Skarsfeldt, 1998; Dunn and Fitton, 1996), but also at α1-adrenergic and dopamine D3 receptors. Hence conclusions about the impact of the neurotransmitters involved in the modulation of PPI based on the present study are limited. However, previous findings have shown that presumably the dopamine D2 antagonistic effect of antipsychotic medication might not account for the increasing effect in low baseline PPI subjects, since the D2 antagonist haloperidol had no such effect (Abduljawad et al., 1998; Csomor et al., 2008a; Oranje et al., 2004b). In addition, haloperidol typically has no effect on PPI (Abduljawad et al., 1999; Graham et al., 2001, 2002, 2004; Kumari et al., 1998; Liechti et al., 2001), and some studies report an attenuation (Abduljawad et al., 1998; Csomor et al., 2008b; Oranje et al., 2004b). In contrast, a contribution of serotonin receptor antagonist actions in PPI-increasing effects of atypical antipsychotics seems credible. Both clozapine and quetiapine, as well as sertindole, have mixed antagonistic activity at D2 and 5HT2A receptors, and enhance PPI in healthy subjects with low baseline gating capacity (Swerdlow et al., 2006b; Vollenweider et al., 2006). Consequently, we assume that the observed enhancing effect of sertindole on %PPI in healthy subjects exhibiting low baseline sensorimotor gating appears due to the combined impact on serotonergic and dopaminergic neurotransmission. This hypothesis is consistent with descriptive observations associating normal gating functions with optimal levels of monoaminergic neurotransmission and synergistic interactions between serotonergic and dopaminergic systems (Mann et al., 2008).
P50 suppression
The present study investigated the effect of an atypical antipsychotic on P50 suppression in healthy volunteers. Comparable with the results of our previous investigation with the typical antipsychotic haloperidol (Csomor et al., 2008a), sertindole increased P50 suppression in subjects exhibiting low P50 gating while attenuating sensory gating in subjects with high P50 suppression. Another study conducted in healthy volunteers revealed that a combination of haloperidol and ketamine lead to a decrement of P50 suppression whereas the application of ketamine alone did not affect P50 suppression (Oranje et al., 2002a). Until now, studies investigating the effect of antipsychotic medication on P50 suppression in healthy volunteers are scant. The majority of studies investigating schizophrenia patients treated with atypical compared with typical antipsychotics showed improved P50 suppression (Adler et al., 2004; Becker et al., 2004; Light et al., 2000) compared with non-improvement (Hong et al., 2009). These findings in patients suffering from schizophrenia and the results from studies investigating the influence of various pharmacological manipulations such as dopaminergics (L-dopa, bromocriptine, amphetamine, or tyrosine/phenylalanine depletion), serotonergics (selective serotonin reuptake inhibitors such as escitalopram, tricyclic antidepressants such as imipramine, tryptophan depletion, or N, N-dimethyltryptamine), and alkaloidergics (yohimbine) on P50 suppression in healthy volunteers (Adler et al., 1994; Hammer et al., 2007; Jensen et al., 2008; Light et al., 1999; Mann et al., 2008; Oranje et al., 2004a; Riba et al., 2002), suggest that a dysfunction in several neurotransmitter systems might contribute to the observed P50 suppression deficits in schizophrenia. The somewhat inconsistent findings of the involvement of different neurotransmitter in the regulation of P50 suppression in healthy volunteers might be due in part to different reactions to pharmacological interventions according to subjects’ baseline levels. All of the above-cited studies except one (Csomor et al., 2008a) did not compare groups of high versus low baseline P50 suppression subjects. Potential pharmacological effects on P50 suppression might be hidden by the mean of all subjects and one might expect to obtain different results by stratifying subjects according to their baseline gating levels. Moreover, a possible explanation for the findings that sertindole improves sensorimotor gating as well as sensory gating in subjects exhibiting low baseline gating while it clearly reduces sensory gating and seems to attenuate sensorimotor gating in subjects exhibiting high baseline gating might be that treatment with sertindole led to an inverted U-shaped dose response. To further clarify such a possibility, larger study sample sizes would be required to identify adequate tertile or quartile groupings for further characterization of drug effect across doses.
There is some indication that atypical antipsychotics may ameliorate sensory gating deficits in schizophrenic patients, as shown for clozapine (Becker et al., 2004; Light et al., 2000; Nagamoto et al., 1996), olanzapine (Light et al., 2000), and risperidone (Light et al., 2000; Yee et al., 1998). The present results with healthy volunteers lead to the conclusion that sertindole might also increase P50 suppression in patients suffering from schizophrenia, but this speculation has to be examined in a study investigating the effect of sertindole in schizophrenic patients.
Furthermore, groups of patients with schizophrenia exhibit deficits in both PPI (Braff et al., 1978, 2001) and P50 suppression (Adler et al., 1982; Baker et al., 1987; Cadenhead, 2002; Light and Braff, 1999; Takahashi et al., 2008). Nevertheless, it cannot be concluded that individual patients with schizophrenia exhibit deficits in both forms of gating, since both the present results and many other observations demonstrate that the measures are not correlated in either patients or healthy volunteers (Braff et al., 2007; Brenner et al., 2004; Light and Braff, 2001; Oranje et al., 2006; Schwarzkopf et al., 1993). For a detailed review of the literature see Braff and Light (2005), Light and Braff (1999), Patterson et al. (2008), Swerdlow et al. (2008), and Oranje et al. (2006).
Cognitive performance
It is noteworthy that high and low PPI subjects performed differentially in a test of spatial working memory as indexed by the SWM strategy score. Subjects exhibiting high PPI chose a better strategy in solving the problem while performances in total and between errors did not differ significantly. We recently reported that subjects with low and high PPI significantly differ in their performance in the SWM task of CANTAB (Csomor et al., 2008a). High PPI levels predicted superior strategy formation. Furthermore, a significant negative correlation between strategy score and PPI at the SOA 60 level was found (Csomor et al., 2008a), confirming independent reports of others (Giakoumaki et al., 2006). Contrary to our previous findings (Csomor et al., 2008a), there were no group differences in SWM error scores, leading to the conclusion that, even though the high PPI group chose a superior strategy, there were no performance differences between the two groups. The absence of performance differences might be an explanation for why no correlation between strategy score and PPI was observed in the present study. Furthermore, performance in SWM relies on the integrity and efficiency of specific cognitive domains, for example relying on prefrontal cortical functioning. Hence, the present findings support the assumption of an involvement of this area in the modulation of human PPI (Bitsios et al., 2006; Csomor et al., 2008a; Giakoumaki et al., 2006), which is consistent with animal studies (Swerdlow et al., 2000, 2001, 2008). Therefore, the present result is a notable replication of the findings of our earlier study, and the suggested role of the prefrontal cortex in the modulation of PPI is supported by the different performance of high and low baseline PPI subjects in these cognitive domains. Further support for the involvement of the prefrontal cortex in the modulation of sensorimotor gating comes from a study showing a positive correlation between dorsolateral prefrontal cortex grey matter volume and PPI level in schizophrenia patients (Kumari et al., 2008). Moreover, rats with low PPI showed cognitive deficits comparable with psychiatric disorders, including reduced sensorimotor gating, reduced motivation, and deteriorated social behavior (Dieckmann et al., 2007; Freudenberg et al., 2007). Both human and animal investigations have considered the degree to which PPI and cognition are directly associated, as reduced PPI is associated with decreased cortical task-related activation in schizophrenia (Geyer, 2006; Molina et al., 2010) and perfusion measured with single photon-emission tomography was significantly lower in the prefrontal and premotor regions of schizophrenia patients (Scholes and Martin-Iverson, 2009). Moreover, Kedzioret al. (2007) concluded that the relationship between PPI and cognitive performance appears to be mediated by common attentional processes active in both tasks, rather than by common underlying neurophysiological inhibitory processes. Contrary results of no statistically significant correlations between PPI and neuropsychological performance have also reported (Molina et al., 2009).
Furthermore, it can be assumed that superior ability in cognitive performance in this domain is related to more efficient early information processing (Mathes et al., 2005). Moreover, cognitive deficits in schizophrenia spectrum disorders, especially measured by (pre)frontal tasks and confirmed by alterations in neuronal activity, are well established (Badcock et al., 2005; Hutton et al., 1998; Manoach, 2003; Minzenberg et al., 2009; Weickert et al., 2000) and have substantial impact on quality of life and functional outcome (Brekke et al., 2005; Green, 2006).
Compared with the findings with high and low sensorimotor gaters, P50 subgroups did not differ in their cognitive performance, which was also the case in our earlier study (Csomor et al., 2008a). Under treatment with sertindole, the high group chose a better strategy in the SWM task, while performance as indexed by the number of errors was worse in the most difficult condition. Moreover, under sertindole treatment, the high group’s performance was decreased in attention and working memory (indicated by A’ and total hits in RVP task) while the low group’s performance was not affected. Therefore, treatment with sertindole did not lead per se to a general reduction of cognitive performances but attenuates cognitive performance in the most difficult condition of the SWM task and in attention and working memory in the high group. One might speculate that the high group’s performance was reduced because of potential ceiling effects but, contrary to the present findings, it is more common that cognitive performance in healthy volunteers is generally diminished by typical or atypical antipsychotic medication, possibly caused by sedative side effects (Csomor et al., 2008a; McCartan et al., 2001; Vollenweider et al., 2006). Moreover, considerations about a positive impact on cognitive functions of sertindole have come from a study with patients suffering from schizophrenia where treatment with sertindole was compared with haloperidol (Gallhofer et al., 2007).
Conclusions
The influence of antipsychotics on sensory and sensorimotor gating in healthy volunteers seems to be dependent on baseline gating levels. In summary, there is increasing evidence that mixed D2/5-HT2 receptor antagonists enhance PPI as well as P50 suppression in healthy subjects with low baseline gating in a way that is comparable with observations in studies with schizophrenia patients. Moreover, both cognitive performance and PPI seem to be dependent on proper prefrontal cortical functioning, as suggested by the replication of the finding that high PPI subjects show significantly better SWM strategy performance. Furthermore, the results of the present study militates in favor of the concomitant assessment of PPI and P50 suppression as well as cognitive measures while investigating the effect of antipsychotic medication in healthy volunteers stratified into low and high baseline gating subgroups. The combined use of PPI and P50 suppression in a single study might represent an excellent tool for translational research. Nevertheless, to gain further evidence of the influences of sertindole on gating functions as well as their relation to psychopathology and cognition, a clinical study in patients suffering from schizophrenia should be undertaken, where the effect of sertindole on the above-mentioned parameters, as well as on psychopathologic symptomatology, should be investigated and compared with other atypical antipsychotic medication in a longitudinal study design.
Footnotes
Acknowledgement
We thank Prof Dr Boris Quednow for informative discussions, and we wish to express our great appreciation to Milena Holstein and Petra Schaefle for their technical support.
The present study was supported by an unrestricted grant given by Lundbeck (Switzerland). Lundbeck had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and the decision to submit the paper for publication.
None of the authors have any conflicts of interest to declare.