
Abstract
Cannabidiol (CBD) is one of the main components of Cannabis sativa and has a wide spectrum of action, including effects in the sleep-wake cycle.
Objective:
The objective of this paper is to assess the effects on sleep of acute systemic administration of CBD.
Method:
Adult male Wistar rats were randomly distributed into four groups that received intraperitoneal injections of CBD 2.5 mg/kg, CBD 10 mg/kg, CBD 40 mg/kg or vehicle (n=seven animals/group). Sleep recordings were made during light and dark periods for four days: two days of baseline recording, one day of drug administration (test), and one day after drug (post-test).
Results:
During the light period of the test day, the total percentage of sleep significantly increased in the groups treated with 10 and 40 mg/kg of CBD compared to placebo. REM sleep latency increased in the group injected with CBD 40 mg/kg and was significantly decreased with the dose of 10 mg/kg on the post-test day. There was an increase in the time of SWS in the group treated with CBD 40 mg/kg, although this result did not reach statistical significance.
Conclusion:
The systemic acute administration of CBD appears to increase total sleep time, in addition to increasing sleep latency in the light period of the day of administration.
Keywords
Introduction
Cannabidiol (CBD) is one of the main components of Cannabis sativa and has a wide spectrum of action, including anxiolytic (Bergamaschi et al., 2011), antipsychotic (Zuardi et al., 1982; Zuardi et al., 2009), antidepressant (Saito et al., 2010; Zanelati et al., 2010), anti-inflammatory and neuroprotective properties (Iuvone et al., 2009; Zuardi, 2008).
Although CBD was long shown to affect the sleep-wake cycle, its effects at different doses and means of administration are still unclear, with reports ranging from increased wakefulness to sedative and hypnotic effects (Nicholson et al., 2004; Zuardi, 2008). The knowledge concerning the effects of CBD in the neurobiology of the sleep-wake cycle contributes to elucidating the role of the endocannabinoid system not only in sleep phases, but also with respect to the full spectrum of action of CBD.
In healthy volunteers with at least six hours of sleep, CBD (600 mg) induced sedative effects (Zuardi et al., 1993). In volunteers with complaints of insomnia, CBD was associated with subjective reports of increased sleep time and less frequent arousals at 160 mg/day (Carlini and Cunha, 1981). Also, volunteers’ reports suggested that CBD reduces dream recall and causes no ‘hangover’ at 40, 80, and 160 mg/day, although no objective measure of these parameters has been made (Carlini and Cunha, 1981). In the opposite direction, the administration of low doses of CBD (15 mg/day) and of CBD combined with delta-9-tetrahydrocannabinol (THC) (15 mg/day) increased wakefulness (Nicholson et al., 2004). Despite the fact that subjective and objective measures are being compared here, it seems likely that these differences are a manifestation of the well-known biphasic effect of CBD (stimulatory at low doses and sedating at high doses) (Zuardi, 2008).
Few clinical trials and studies using animal models exist concerning the effects of CBD on sleep. The first investigation assessing the effect of the systemic administration of CBD on sleep found decreased slow-wave sleep (SWS) latency with 20 mg/kg and increased duration of SWS and decreased wakefulness with 40 mg/kg, with no significant changes in the rapid eye movement (REM) sleep phase (Monti, 1977). In that study the effects of CBD were recorded for five hours after administration. After this pioneering investigation there was a large gap in basic research on sleep and CBD.
Recently, two studies used intraventricular administration (Murillo-Rodriguez et al., 2006) and lateral hypothalamus infusion (Murillo-Rodríguez et al., 2011a) and found contrasting effects to those of Monti (1977). Intraventricular administration of CBD (10 ug/uL) increased waking one and four hours after CBD and reduced the duration of REM sleep, with no changes in SWS (Murillo-Rodriguez et al., 2006). The injection of CBD in the lateral hypothalamus also increased waking and reduced REM sleep time, in addition to significantly decreasing SWS (Murillo-Rodríguez et al., 2011a).
These results from clinical and animal studies highlight the need to assess the effects of the systemic administration of CBD for longer periods and at different doses. Therefore, we assessed the effects of CBD on sleep using intraperitoneal injections of placebo and CBD 2.5, 10, and 40 mg/kg for a period of 48 hours in adult rats.
Methods
Animals
Adult male Wistar rats (300–400 g) bred at the animal facility CEDEME Universidade Federal de São Paulo (UNIFESP) were used in this study. Animals were kept in standard polypropylene cages with free access to food and water, in a temperature-controlled room (22 ± 1°C) with a 12:12-h light-dark cycle (lights on at 07:00).
The experimental protocol was approved by the Ethics Committee of UNIFESP (process no. #1421/06). All the procedures used in this study were consistent with the Ethical and Practical Principles of the Use of Laboratory Animals (Andersen et al., 2004, 2010) and comply with current Brazilian government guidelines (National Council for the Control of Animal Experimentation – CONCEA).
Drugs
Cannabidiol (THC-Pharm, Frankfurt, Germany and STI-Pharm, Brentwood, UK) was prepared in Tween 80:saline (1:18) and administered intraperitoneally (i.p.) at 2.5, 10 and 40 mg/kg (0.1 mL/100 g weight). Animals in the control group were injected with similar volumes of vehicle alone.
Experimental protocol
After recovery of the stereotactic surgery and habituation to the sleep-recording apparatus, the animals were randomly distributed into four groups: CBD 2.5 mg/kg; CBD 10 mg/kg; CBD 40 mg/kg; and control (CTRL) (n = seven animals/group). Sleep recordings were made during light and dark periods of 12 h each for four days: two days of baseline recording, one day of drug administration (test), and one day after drug or post-test. All animals were injected between 07:00 and 08:00.
Stereotactic surgery and sleep recording
A stereotactic surgery was performed in order to implant electrodes, thus permitting the assessment of the rats’ sleep-wake cycle through electrocorticographic (ECoG) and electromyographic (EMG) activities. Animals were placed in a classic stereotaxic frame (Insight Instruments) while under deep anesthesia. Two bipolar electrodes with four stainless-steel screws (ø 0.9 mm) were put in the skull through small orifices drilled onto the right lateral frontoparietal region (one pair) for bipolar ECoG monitoring. Two flexible nickel-chromium wires were inserted into the neck muscles to monitor EMG activity. After surgery, the rats received penicillin (20,000 U in 0.1 mL intramuscular (i.m.)), diclofenac sodium (25 mg/mL i.p.), and ibuprofen (50 mg/mL oral). Seven days after surgery, the sockets were connected using flexible recording cables and a commutator to a polygraph and a computer. Before the sleep-wake cycle recording, the rats were habituated to the apparatus for at least 24 hours. The recordings were carried out in a Nihon Koden (TYO) model QP-223A apparatus using three channels for each animal. ECoG signals were amplified and filtered with a low-pass filter at 0.5 Hz and a higher cut-off of 35 Hz. EMG activity was filtered with a low-pass filter at 5.3 Hz (Andersen and Tufik, 2003; Hirotsu et al., 2010; Schutz et al., 2003; Sinha and Ray, 2006). Animals were maintained in their own cages inside a Faraday chamber during the experimental period. ECoG traces were visually and manually identified and scored according to procedures described by Timo-Iaria et al. (1970). The following sleep parameters were examined: percentage of total sleep time during the recording time, percentage of SWS throughout the recording, paradoxical sleep or REM sleep latency, sleep latency and arousals (events lasting at least 15 seconds and consisting of abrupt changes from the baseline ECoG frequency and the high-amplitude EMG activity followed by SWS, expressed in absolute numbers).
Statistical analyses
Parametric data were analyzed using one-way repeated-measures analysis of variance (ANOVA) with a mixed design to compare differences between groups, time effect (baseline, test and post-test days) and the interaction between time and group followed by Bonferroni correction for multiple comparisons. When the conditions of sphericity were not achieved, the degrees of freedom were established using Huynh-Feldt epsilon. Analyses were performed using SPSS version 17 and the level of statistical significance was set at α = 0.05. Data are expressed as means ± SEM.
Results
The results obtained in the light period are summarized in Table 1. A significant effect of time-group interaction (repeated-measures ANOVA) was observed with respect to the percentage of sleep time and latency to REM sleep. The percentage of sleep time increased in the groups treated with CBD (10 and 40 mg/kg) compared to placebo on test day, with no statistically significant differences on post-test day (Figure 1). REM sleep latency was significantly increased with the dose of 40 mg/kg on the test day and significantly decreased with the dose of 10 mg/kg on post-test day (Figure 1). The percentage of SWS showed a tendency to significant effects of time-group interaction (F6,48=1.84; p=0.1), with an increase of SWS in the group treated with CBD 40 mg/Kg (F2,12=4.63; p=0.032).
Sleep parameters recorded in the light period per group.

CTRL: control; CBD: cannabidiol; ANOVA: analysis of variance; SWS: slow-wave sleep; REM: rapid eye movement; NS: not statistically significant.
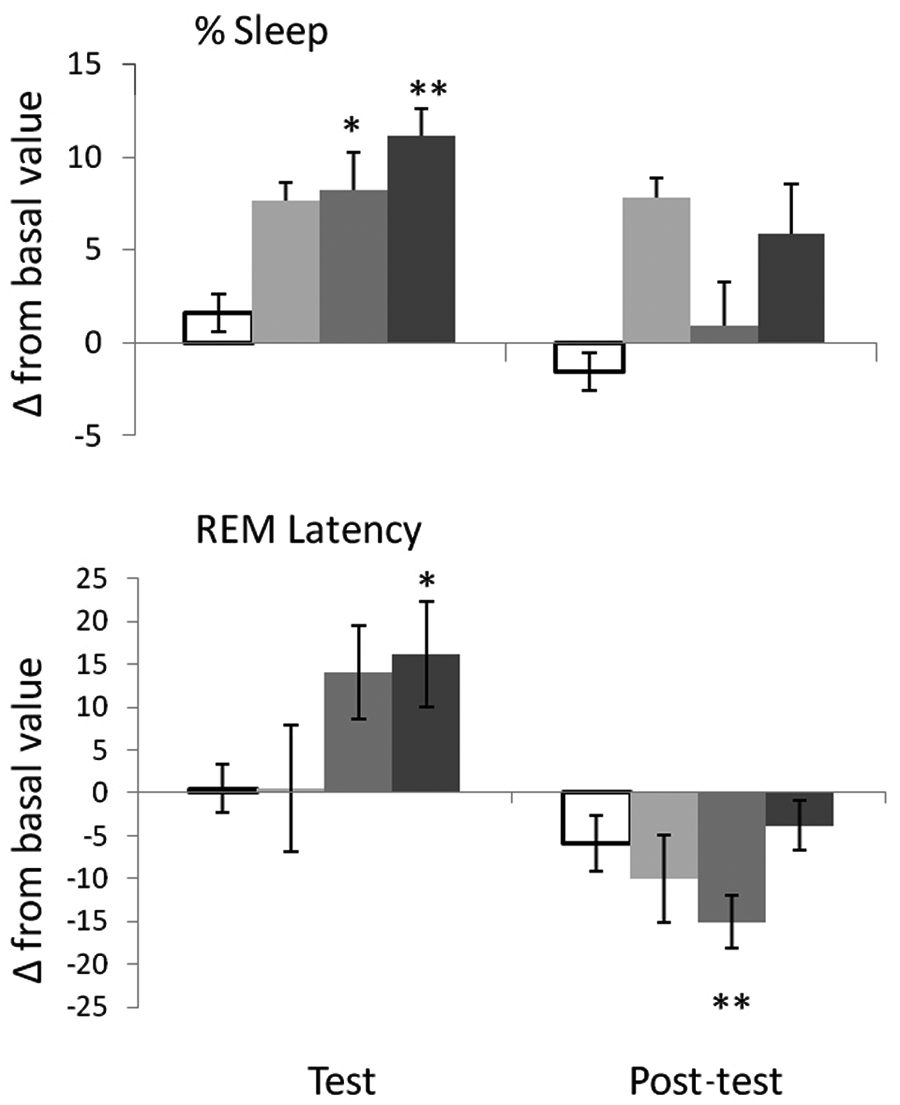
Variation from basal value in the light period. Error bars represent standard error of the means. Asterisk indicates significant difference from basal measures (*p<0.05; **p<0.01, pairwise comparisons with Bonferroni correction for multiple comparisons).
In the dark period, the repeated-measures ANOVA showed no time-group interactions in any of the measures.
Discussion
CBD doses of 10 and 40 mg/kg led to an increase in the total percentage of sleep in the light period, with the dose of 40 mg/kg increasing the latency to REM sleep on the test day and the dose of 10 mg/kg decreasing it on the post-test day.
The study by Monti (1977) was the only one besides ours to use intraperitoneal injections of CBD to assess its effects on sleep in animal models. Our results are similar to those of Monti’s acute trial that assessed sleep for five hours after the administration of CBD. Indeed, there seems to be an increase in the total time of sleep, as both investigations found this using CBD 40 mg/kg. The same dose of CBD seems to induce an increase in the percentage of SWS, which was statistically significant in the study by Monti and had a similar trend in our study.
Conversely, two recent studies (Murillo-Rodríguez et al., 2006; Murillo-Rodríguez et al., 2011a) that injected CBD directly into the lateral hypothalamus and brain ventricles reported increased waking and decreased REM sleep. One study that used local injection of CBD into the amygdala to assess its effects on sleep disruption induced by experimental models of anxiety found that CBD blocked REM sleep suppression with virtually no alterations in the non-REM phase (Hsiao et al., 2012). These data suggest that the effects of CBD vary according to the means and locality of administration. Another possibility that could explain the paradoxical results of these studies refers to the doses used. The biphasic effects of CBD are well known, with lower doses increasing wakefulness and higher doses causing sedating effects. In this same sense, studies with humans have shown discrepant effects of CBD at different doses: whereas Carlini and Cunha (1981) found increased sleep time and fewer arousals with doses of 40–160 mg/day, Nicholson et al. (2004) used 16 mg/day and found increased waking time, although the latter used CBD associated with THC.
The intraventricular administration of CBD was reported to increase the expression of c-Fos, a marker of neuronal activity, especially in hypothalamic areas related to wakefulness and in the dorsal raphe nuclei (Murillo-Rodríguez et al., 2006), suggesting the involvement of the monoaminergic system in the action of CBD in the sleep-wake cycle. CBD has a broad spectrum of pharmacological activities and its paradoxical effects on the sleep-wake cycle might reflect differences in the dose, site, and form of administration.
Among other things, CBD can increase the levels of anandamide, a CB1 endocannabinoid agonist, through reuptake blockade and inhibition of its hydrolysis by the fatty acid amide hydrolase (FAAH) enzyme. Anandamide has been suggested to increase the time of sleep and of the slow-wave phase (Murillo-Rodríguez et al., 1998; Murillo-Rodríguez et al., 2001; Murillo-Rodríguez et al., 2003). The CB1 receptor is present in many brain regions; however, its distribution in the pons and basal forebrain are of fundamental importance here, given that the action of anandamide on these receptors could activate cholinergic neurons, increasing the release of acetylcholine and total sleep time (Arias-Carrion et al., 2011). These regions may be important to explain the increase in sleep time and the tendency to increase in the time of SWS following the systemic administration of CBD.
On the other hand, the action of CBD could be dependent on the brain area. The administration of the FAAH enzyme (which also decreases the catabolism of anandamide and two other fatty acids, oleoylethanolamide and palmitoylethanolamide) into the ventricles, lateral hypothalamus, and dorsal raphe has been associated with increased waking time (Murillo-Rodríguez et al., 2007; Murillo-Rodríguez et al., 2011b). Similar findings were obtained with the administration of CBD into those same regions, with ensuing increases in dopamine, serotonin, and noradrenaline in the accumbens, which also points in the opposite direction of our findings (Murillo-Rodriguez et al., 2006, Murillo-Rodriguez et al., 2011a). Also, experimental in vitro evidence suggests that CBD was able to antagonize the binding of CB1 and CB2 receptor agonists (Thomas et al., 2007). One hypothesis to explain the paradoxical findings related to the local and systemic administration is that the systemic administration would lead to a widespread distribution of anandamide in the central nervous system (CNS), and therefore to a regulation among the many regions involved with the sleep-wake cycle that have CB1 receptors. According to this hypothesis, the sum of the effects in these regions would result either in increased sleep time or increased wakefulness. For example, regions such as the basal forebrain and pons seem to be related to increases in sleep, whereas the lateral hypothalamus and dorsal raphe appear to mediate increases in wakefulness (Murillo-Rodríguez et al., 2003; Murillo-Rodríguez et al., 2011a).
It is important to mention the absence of data regarding neurochemical and neuronal activity as one of the limitations of our study. Nevertheless, our results are consonant with previous evidence concerning the systemic acute administration of CBD using a longer period of observation.
Conclusion
The systemic acute administration of CBD appears to increase total sleep time in addition to increasing REM sleep latency at 40 mg/kg in the light period of the day of administration. In the light period of the first day following the administration of CBD, there was a decrease in REM sleep latency with the dose of 10 mg/kg. Similar investigations using different doses, means, and times of administration and with different pharmacological challenges are warranted to establish the action of CBD on the sleep-wake cycle.
Footnotes
Acknowledgements
M.L.A, S.T., A.W.Z., J.E.C.H., and J.A.S.C. are recipients of a Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, Brazil) fellowships award.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.