
Abstract
Alcohol intoxication and psychiatric medication overdoses, including antidepressants, are common emergency room events. Heavy alcohol and antidepressant exposure are able to induce changes in cytokines disturbing normal physiology. We examined the inflammatory and physiological effects of selective serotonin reuptake inhibitor (SSRI) medication after heavy alcohol exposure. Rats were randomly divided into Alc (EtOH 5g/kg, intravenous infusion for 3 h), SSRI (paroxetine oral intake) and Alc+SSRI groups. Serum samples were collected to measure blood ethanol, aspartate transferase, alanine transferase, creatine phosphokinase, lactate dehydrogenase, amylase, tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) levels. Lactate dehydrogenase levels in bronchoalveolar lavage fluid were also examined. Liver, pancreas and lungs were removed after sacrifice and any pathological changes were catalogued. Ethanol infusion resulted in blood levels of ethanol of >100 mg/dL after ethanol infusion. Serum levels of aspartate transferase, alanine transferase, creatine phosphokinase, lactate dehydrogenase, amylase, TNF-α and IL-6 in the Alc+SSRI group were lower than in the Alc group. Moreover, pathological damages to the liver, pancreas and lungs were slightly lower in the Alc+SSRI group than in the Alc group. These findings suggested that SSRI is able to decrease the release of pro-inflammatory cytokines and thereby reduce liver and pancreas damage after heavy alcohol exposure.
Introduction
Alcohol is a common substance and is often abused by humans, resulting in profound public health impacts. A number of physical diseases have been identified as being caused by alcohol intoxication directly (Szab and Bala, 2010), such as hepatitis, gastritis, pancreatitis and kidney damage. Alcohol also affects innate immune responses and causes organ damage (Goral et al., 2008). Heavy alcohol exposure increases pro-inflammatory cytokine levels, including tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), which contribute to inflammation and organ damage (Goral et al., 2008; Romeo et al., 2007). Acute alcohol intoxication causes several metabolic alterations, including hypoglycemia and lactic acidosis, and may induce acute alcoholic hepatitis, cardiovascular effects, respiratory depression and acute pancreatitis (Vonghia et al., 2008). Alcoholic liver disease (ALD) is a major heath consequence of chronic alcohol use. Activation of the inflammatory cascade is a key element in ALD (Arteel et al., 2003; Szabo, 2007). ALD is a multi-step disease process that typically progresses through stages of acute alcoholic hepatitis and alcoholic cirrhosis, eventually becoming end-stage liver disease. Inflammation may also be involved as a cofactor in both acute and chronic alcoholic pancreatitis (Vonghia et al., 2008). Consistent with this, chronic alcohol use also increases the risk of lung infection.
Alcohol use is not the only problem among patients with alcohol intoxication. Co-use of other psychiatric therapeutics, especially antidepressants, is common among the patients. Antidepressants also induce changes in cytokines. Dysregulation of the functional activity of the immune system during depression has been described (Raison et al., 2006) and it has been hypothesized that excess inflammation plays a role (Dantzer et al., 2008). Cytokine-mediated inflammation has been implicated in the development and presentation of psychiatric disorders, including depression (Abdel-Salam et al., 2004; Nawa and Takei, 2006; Raison et al., 2006). The neuropsychiatric symptoms may only disappear after termination of cytokine administration, or treatment with antidepressants, for example selective serotonin reuptake inhibitors (SSRIs) (Taler et al., 2008). SSRIs are the most widely used antidepressants (Weathermon et al., 1999). Kubera et al. have showed that an increase in the concentration of serotonin following SSRI administration is associated with an increase in anti-inflammatory cytokines and a decrease in pro-inflammatory cytokines (Kubera et al., 2000). SSRIs are effective when treating cardiovascular disease associated with depression, and they have been demonstrated in animal models to have an anti-inflammatory effect (Abdel-Salam et al., 2004; Shen et al., 1999).
Heavy alcohol drinking and antidepressant abuse are both important public health problems and both are also related to inflammatory responses. Some patients with depression use alcohol while under antidepressant treatment (Scott et al., 1998). In a clinical situation, psychiatric therapeutics is commonly used during antidepressant treatment of alcohol abusers in order to improve their emotional problems. In this study, our aim was to discover whether individuals with acute alcohol poisoning are less damaged if they are taking SSRIs. In this context it is essential to have an understanding of the physiological responses that occur when antidepressants are used in the situation where there is alcohol intoxication; this will allow the possible effects on patients to be clearer when treating patients. In this study, we examined the effects of SSRIs, when these antidepressants are used during the intoxication stage of alcohol use. We found that the physiological and inflammatory changes associated with heavy alcohol exposure are changed in the presence of SSRI medication.
Materials and methods
Preparation of animals
Thirty-six male Wistar rats, weighing 290–310 g, were housed two per cage and kept on a 12:12 hour reversed light:dark cycle (lights on at 07.00) in a temperature-controlled room (22 ±1oC). Food and water were available ad libitum. Animals were anesthetized by ether inhalation for 10 min. During the period of anesthesia, a femoral artery was catheterized for blood sampling, while the femoral vein was catheterized for intravenous administration of fluids. The operation was completed within 15 min and the insertion wound was stitched up with 3.0 catgut suture. After the rats had awakened, their hemodynamics were allowed to stabilize for 30 min, then the animals were placed in a metabolic cage individually (Shingshieying Instruments, Hualien, Taiwan) and rested overnight. The protocols used were approved by the Institutional Animal Care and Use Committee of Tzu Chi University (No. 98070) and were consistent with the standards for the care and use of laboratory animals as outlined in the NIH Guide.
Experimental design
The rats were randomly divided into three groups: the SSRI group, the Alc group and the Alc+SSRI group. The Alc and Alc+SSRI groups both received ethanol 5 g/kg body weight via three hours of slow intravenous (i.v.) infusion by an infusion pump (Aladdin, WPI-Europe). The alcohol was diluted with distilled water to give a 40% (volume/volume (vol./vol.)) concentration. The SSRI group received three hours of slow i.v. infusion of the vehicle (distilled water) followed by SSRI administration. The SSRI and Alc+SSRI groups were given SSRI (paroxetine, 0.33 mg/kg body weight) via a feeding tube after the ethanol infusion. The dosage of this antidepressant was referenced against a normal 60 kg adult daily dose. For example, the suggested daily dose of paroxetine for adults is 20 mg/day. Regarding the dosage of ethanol, the symptoms of acute alcohol exposure are usually related to blood alcohol concentration (BAC) in humans (Vonghia et al., 2008). Death has been observed at relatively low BACs in ‘nontolerant’ subjects (300 mg/dL) and recovery has been reported at higher levels (200mg/dL). We have established an intravenous injection rat model that mimics the nontolerant situation in order to assess the effects of acute alcohol exposure at different dosages from 1 to 10 g/kg (data not showed). In the study, acute alcohol intoxication occurs at a BAC higher than 400 mg/dL and at this level there is an increased risk of mortality rate with death regularly occurring in high dose ethanol groups (71.43% for ethanol 10 g/kg). In addition, dose-dependent changes in biochemical values (glutamic oxaloacetic transaminase (GOT), glutamic pyruvic transaminase (GPT), and lactate dehydrogenase (LDH)) and serum TNF-α can be demonstrated after alcohol administration. A dose of ethanol at 5 g/kg represents a middle injury score that mimics a 300–400 mg/dL BAC, and has a zero mortality rate. Therefore, we have chosen ethanol 5 g/kg for this animal study. In this study, the clinical situation we are trying to model is a patient who takes antidepressants as part of their alcohol abuse treatment, specifically when antidepressants are used during the acute alcohol intoxication stage.
Blood sample analyses
Blood samples were taken from the femoral arterial catheter before alcohol infusion (marked as Pre in the Figures), and at 0 (the time point at which the infusion finished), 1, 3, 6, 9, 12, 24 and 48 h after the 3 h of alcohol infusion. We used a simple technique described previously that maintains the rats without restraint and/or anesthesia, while making it easy to withdraw blood without inducing pain and fear (Lee et al., 2002). A blood sample of 0.5 mL was drawn each time, while an equal volume of normal saline (NS) was simultaneously replaced. BACs were measured immediately after blood was withdrawn. Next, the samples were centrifuged at 3000 r/min for 10 min. The serum was decanted and separated into two parts; one part of the serum was stored at 4oC for biochemical examination within 1 h after collection. The other part was stored at −80oC for TNF-α and IL-6 analysis. The former was used to measure the levels of blood alcohol, aspartate transferase (AST), alanine transferase (ALT), LDH, creatine phosphokinase (CPK) and amylase.
LDH in bronchoalveolar lavage fluid measurement
Bronchoalveolar lavage fluid (BALF) was also obtained at 48 h. Animals were anesthetized by pentobarbital (50 mg/kg) via femoral artery catheter before sacrifice. The trachea was cannulated and left lung ligation was carried out. The right lung was then washed with 10 mL/kg of sterile normal saline. The lavage fluid was collected and centrifuged at 3000 r/min for 10 min. The supernatant was collected and its LDH level measured.
TNF-α and IL-6 measured by ELISA
Blood samples were taken from the femoral arterial catheter at 1, 3 and 24 h after the perfusion. The supernatant was collected to allow measurement of TNF-α and IL-6. The concentrations of TNF-α and IL-6 were measured using enzyme-linked immunosorbent assay kits (R&D Systems, Minneapolis, MN, USA). Each sample was duplicated and the amount of TNF-α and IL-6 determined by an automated ELISA reader at 450/540 nm wavelengths.
Histological examination
Rats were sacrificed by decapitation after the BALF procedure, and the liver, pancreas and left lung were removed immediately after sacrifice. These tissue specimens were fixed overnight in 4% buffered formaldehyde, processed by standard methods and stained with hematoxylin and eosin (H & E). The tissue specimens were examined by an observer blinded to the group assignment.
Statistical analysis
Data were expressed as mean ± SEM, and analyses were conducted using SPSS13.0 software. To assess the statistical differences between specific time points and the baseline, the data were subjected to one-way analysis of variance (ANOVA). Differences in mean values at the same time point between groups were analyzed using Duncan’s post-hoc multiple comparison. Statistical significance was set at p ≤ 0.05 (two-tailed).
Results
BAC and mean arterial pressure
The rat’s BAC significantly increased after the start of ethanol infusion (point 0) in the Alc and Alc+SSRI groups (Figure 1(a)), and the mean BAC values reached about 475 mg/dL. The BAC levels showed no difference between the measurements taken over time within the SSRI group. The average mean arterial pressure (MAP) before alcohol infusion was not significantly different across the three groups. However, hypotension occurred at 1, 3, 6 and 9 h after the start of infusion in the Alc group. Furthermore, the MAP of the Alc+SSRI group decreased gradually from 1 h (p=0.021) until 9 h (p=0.014); however, these MAP levels were higher than those of the Alc group (Figure 1(b)).
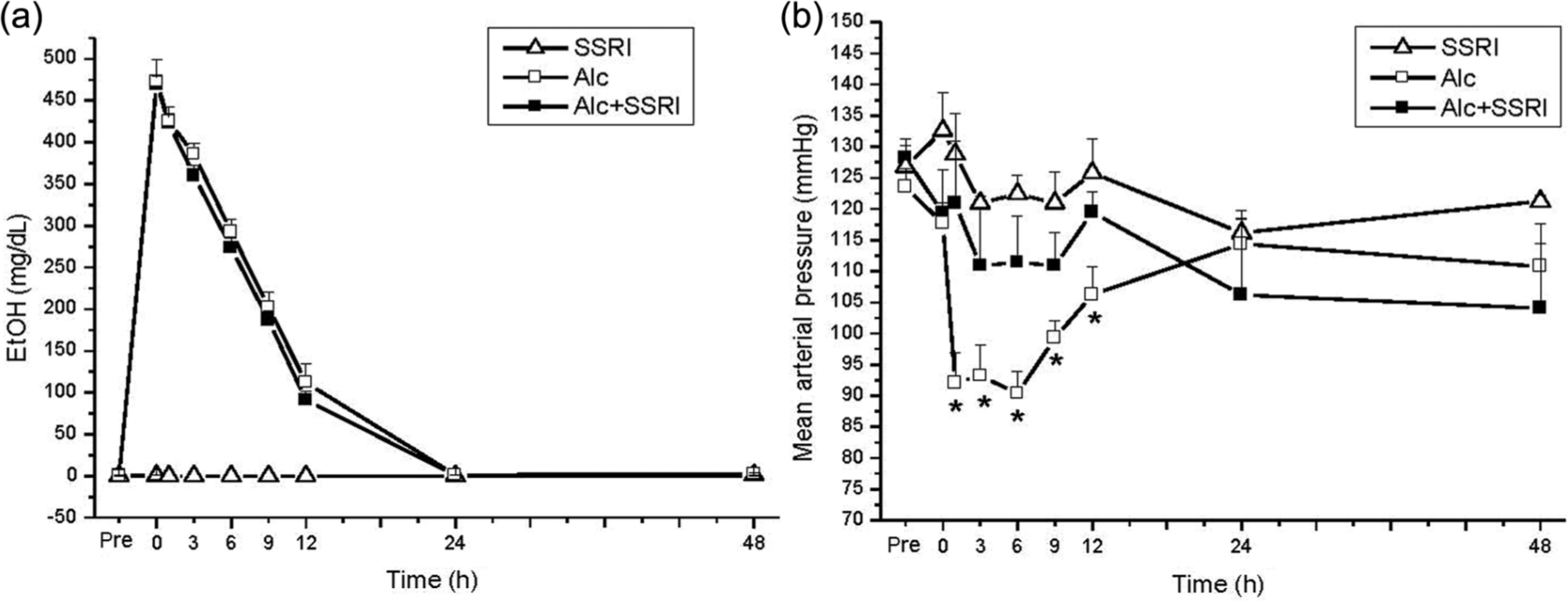
Serum blood alcohol concentration (BAC) and mean arterial pressure (MAP) after intravenous alcohol infusion. (a) BAC; (b) MAP.
Serum biochemical examination
Blood levels of AST (Figure 2(a)) increased after 12 h when the Alc and Alc+SSRI groups were examined. Compared with the other groups, the Alc groups showed higher blood values of AST at 24 and 48 h. In Alc and Alc+SSRI groups, the levels of ALT (Figure 2(b)) increased after 12 h. The Alc group had higher blood values of ALT at 24 and 18 h after ethanol infusion compared with the other groups. The blood levels of AST and ALT of the SSRI group were unchanged. The Alc and Alc+SSRI groups had higher LDH levels after alcohol infusion than the SSRI group (Figure 2(c)). Compared with the Alc+SSRI group, LDH levels were found to have increased significantly at 3 (p=0.030), 24 (p=0.026) and 48 h (p=0.019) in the Alc group. The levels of CPK were found to have increased immediately after ethanol infusion (point 0) in the Alc and Alc+SSRI groups (Figure 2(d)). In the Alc group, CPK was found to have increased at 0, 3, 6, 9, 12 and 48 h compared with the SSRI group (Figure 2(d)). Compared with the Alc+SSRI group, the Alc group showed an increased CPK at 9 (p=0.032), 12 (p=0.023) and 48 (p=0.048) h (Figure 2(d)).
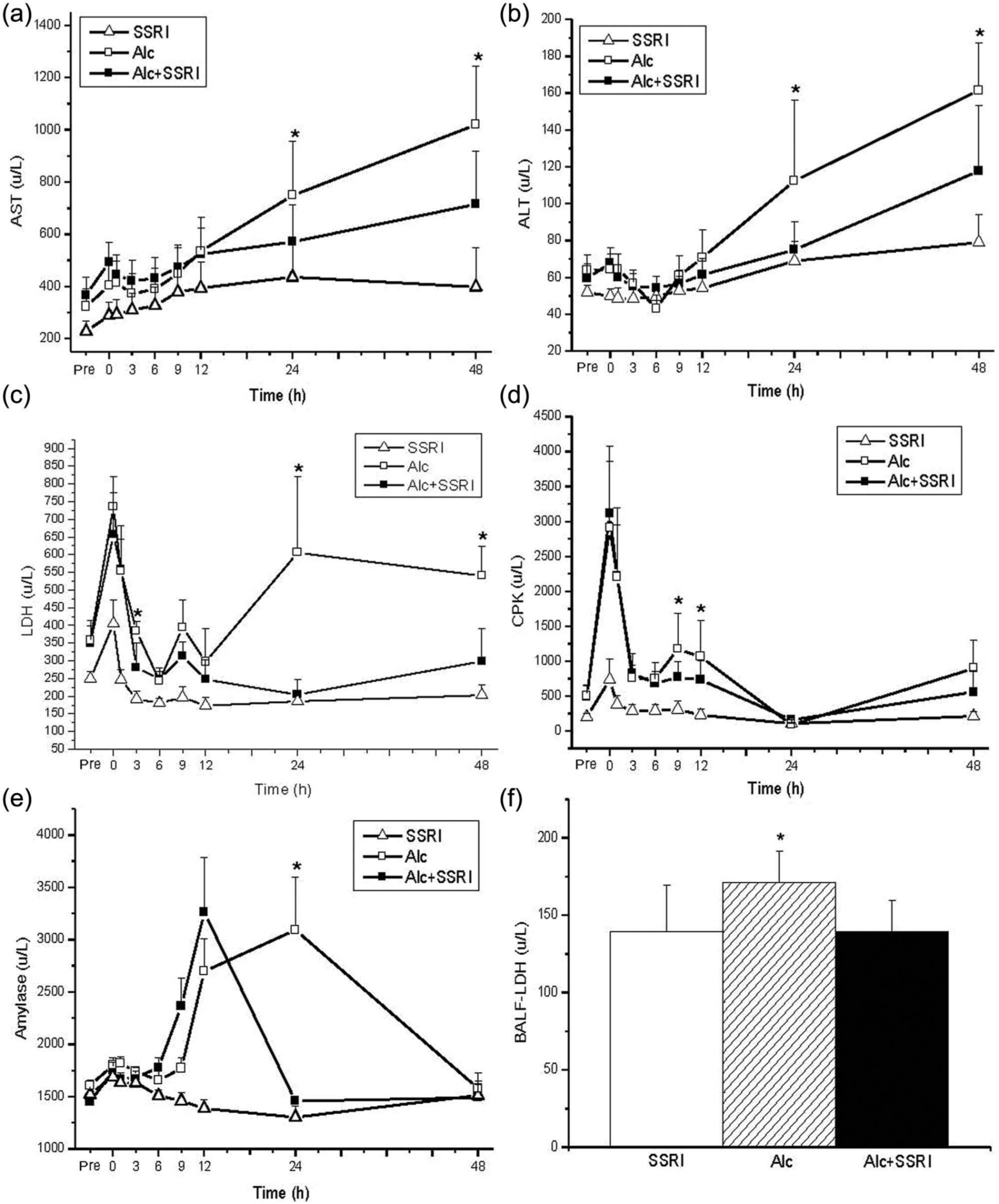
Levels in serum of aspartate transferase (AST) (a), alanine transferase (ALT) (b), lactate dehydrogenase (LDH) (c), blood creatine phosphokinase (CPK) (d) and amylase (e), and in bronchoalveolar lavage fluid (BALF) of LDH (f) after intravenous alcohol.
The Alc group had higher amylase levels than the SSRI group at 9, 12, and 24 h after alcohol infusion (Figure 2(e)). Compared with the Alc+SSRI group, the amylase levels were higher at 24 h (p=0.016) in the Alc group. The LDH levels in BALF were also found to be significantly higher in the Alc group than the SSRI and Alc+SSRI groups at 48 h (p=0.039) after the start of alcohol infusion (Figure 2(f)).
Serum TNF-α and IL-6 levels
Administration of alcohol greatly increased the level of serum TNF-α, which peaked at 3 h in the Alc group (Figure 3(a)). Compared with the SSRI and Alc+SSRI groups, the TNF-α levels were higher at 0 (p=0.019), 1 (p=0.012) and 3 h (p=0.030) (Figure 3(a)) in Alc group. In the Alc+SSRI group, the TNF-α level was higher than that of the SSRI group at 1 (Figure 3(a)). When the IL-6 levels were examined, it was found that the levels were higher at 0, 1, 3 and 24 h after alcohol administration. The Alc group had a higher serum value of IL-6 at 0 (p=0.001), 1 (p=0.006) and 3 h (p=0.021) compared with the SSRI and Alc+SSRI groups (Figure 3(b)).
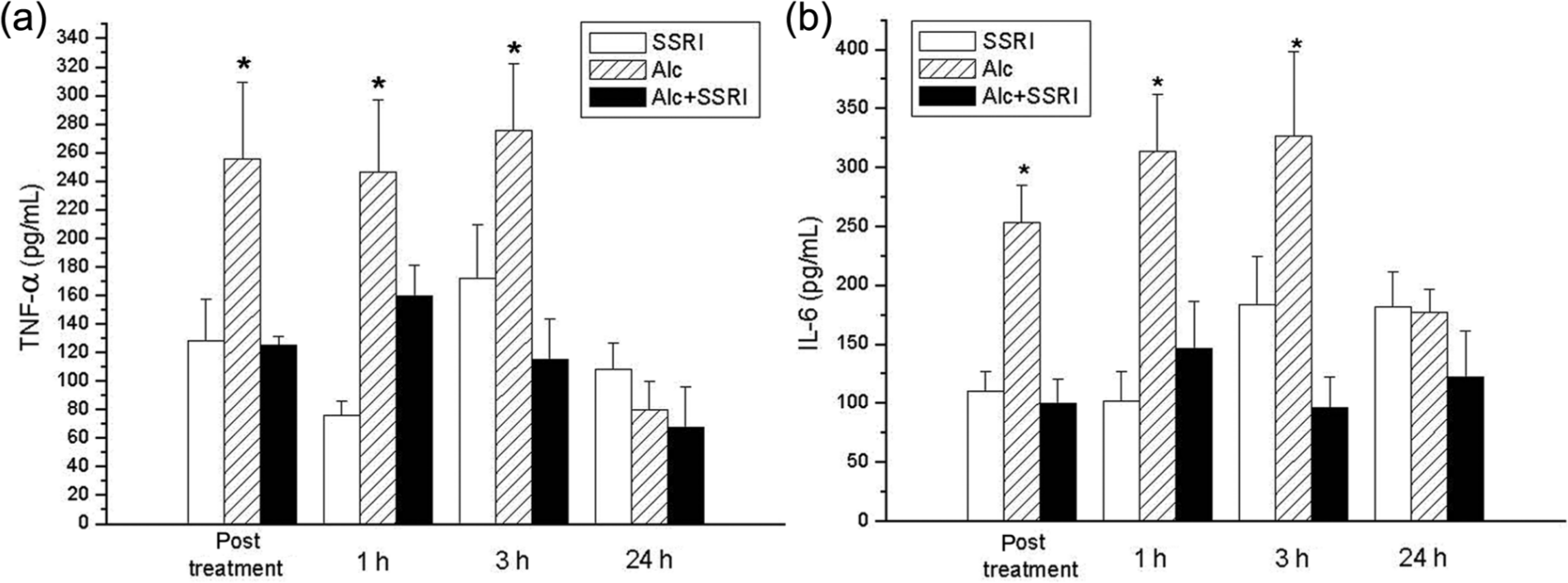
Serum levels of tumor necrosis factor-α (TNF-α) (a) and interleukin-6 (IL-6) (B) after alcohol infusion.
Histopathology examination of the rats’ organs
Histopathological analysis of the tissue sections using H & E staining revealed that the SSRI group presented normal histopathology images of the liver (Figure 4(a)). This contrasted with the Alc group, which showed moderate leukocyte infiltration and severe hemorrhage in the liver (Figure 4(b)). The Alc+SSRI group showed mild hemorrhage in the liver (Figure 4(c)). In the Alc group, leukocyte infiltration with cell lysis was more obviously in the pancreas (Figure 4(e)) compared with either the Alc+SSRI group (Figure 4(f)) or the SSRI group (Figure 4(d)). In addition, the Alc group showed severe pulmonary edema and interstitial cell infiltration of the lungs (Figure 4(h)), while the Alc+SSRI group showed mild to moderate hemorrhage in the lungs (Figure 4(i)). Compared with the SSRI group, SSRI alone did not produce any significantly histopathological changes in the liver, pancreas and lung.
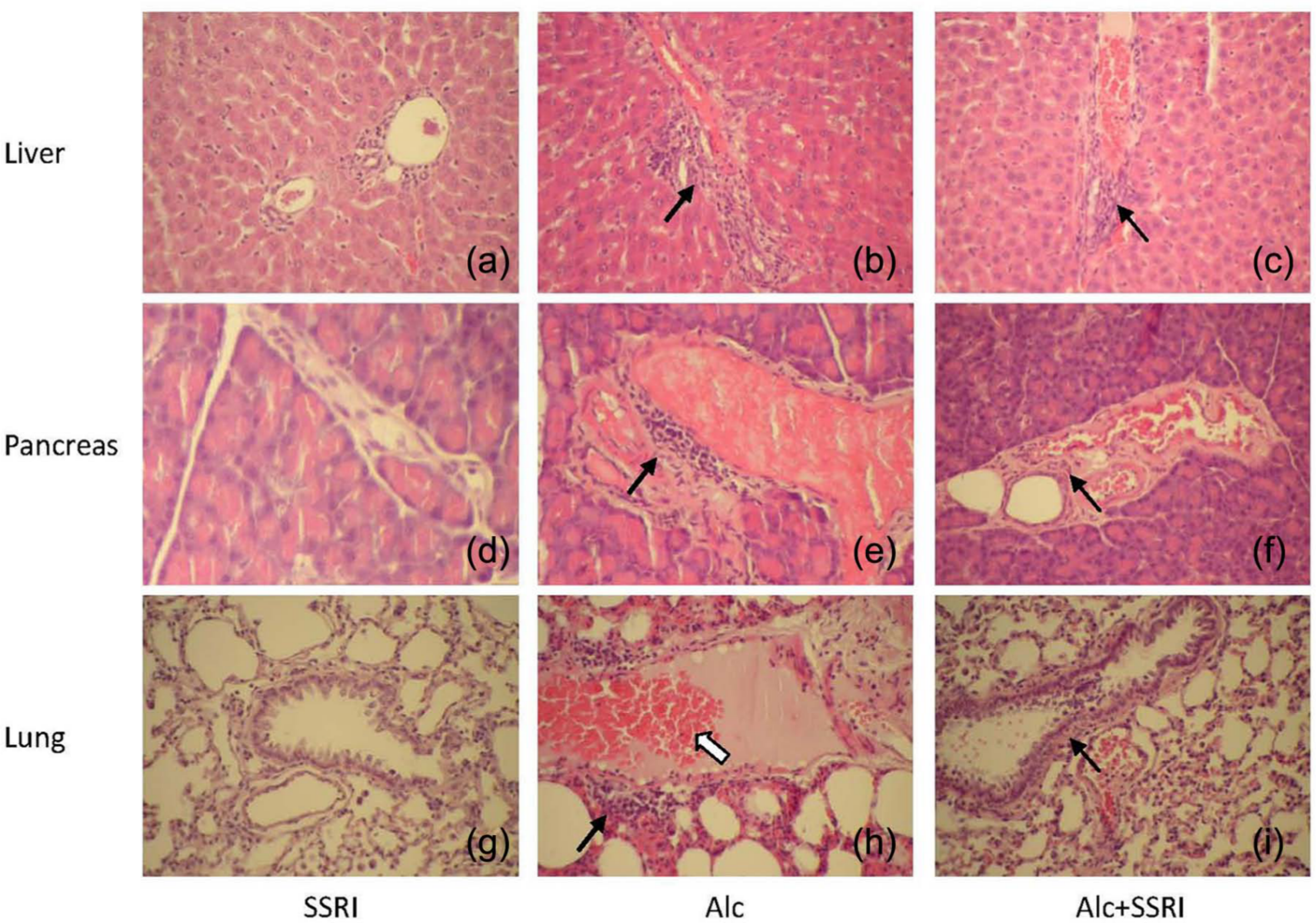
Histological sections from the liver ((a), (b), (c)), pancreas ((d), (e), (f)), and lungs ((g), (h), (i)) were stained with hematoxylin and eosin to observe the presence of histopathological changes in the SSRI group ((a), (d), (g)), Alc group ((b), (e), (h)) and SSRI+Alc group ((c), (f), (i)). The black arrow indicates inflammatory cell accumulation. The white arrow indicates a hemorrhage (original magnification × 200).
Discussion
The main methods used in acute alcohol exposure studies are intubation, infusion, inhalation and intraperitoneal injection (Abel, 2005). The major disadvantage of the intubation method is that the gavage procedure requires the animals to be handled and this may be stressful to the animals. The inhalation method also has major disadvantages, including local irritation of the eyes, mucous membranes and respiratory passages. The dangers of puncturing the intestine or another organ and local irritation of the site of the injection are the major disadvantages of intraperitoneal injection (Abel, 2005). Alcohol administration via 3 h of slow intravenous infusion was chosen as the model for the present study because this method was able to reach a consistent BAC when there was acute ethanol exposure in our pilot study (data not showed). In addition, this method does not have any acute side effects such as stress due to handling, irritation of mucous membranes, irritation of the injection site and possible puncture of the internal organs. Physiological disturbances to the animals’ blood inflammatory cytokines and organ damage to the lungs, kidney and liver were used to evaluate the feasibility of the model. Our study revealed that multiple-organ damage could be demonstrated to occur when this alcohol intravenous infusion model was used. The animal model used in this study shows good sensitivity when predicting multiple-organ damage as well as changes to the innate immune response after ethanol intoxication. The present results are similar to those of humans under acute alcohol exposure. In the present study, the BAC significantly increased and the mean BAC values were maintained above 50 mg/dL, which produced pharmacologically meaningful BACs (McBride and Li, 1998) after ethanol infusion. Furthermore, there were lower MAPs simultaneously with the higher BACs from 1 h until 12 h in the Alc group. However, the administration of SSRI retarded the MAP decrease that occurred after ethanol infusion.
Excessive alcohol use leads to increased risks of health problems including liver disease (Szab and Bala, 2010; Zhou et al., 2003). Blood biochemistry analysis, such as GOT, GPT, LDH and CPK levels, are commonly used indicators for liver and tissue cell injury (Lee et al., 2002). In this study, alcohol infusion increased the blood levels of GOT, GPT, LDH and CPK. In addition, ethanol increased liver damage based on the histopathological findings. The hepatic metabolism of ethanol is an oxidative process (McClain et al., 1998; Weathermon et al., 1999; Zhou et al., 2003). These oxidative reactions alter cellular metabolism and have a harmful effect on the liver. The indirect biochemical alterations caused by the formation of reactive oxygen species (ROS) have been identified in patients treated with antipsychotics. Researchers have found that fluoxetine can reduce ROS generation and decrease tissue damage (Han et al., 2012). Similar to previous studies, the presence of severe liver damage was related to heavy alcohol exposure in our study. However, SSRI administration was able to decrease the higher levels of GOT, GPT, LDH and CPK that are associated with ethanol infusion.
The initiation and progression of acute and chronic pancreatitis, are related to the presence of toxic metabolites, increased oxidative stress, higher levels of inflammatory cytokines and/or chemokine escape. Previous studies have demonstrated that alcohol selectively reduces pancreatic blood flow and microcirculation, increases free oxygen radical generation in the pancreas, and directly damages the pancreas via alcohol metabolites (Schneider and Haas, 2005). In addition, alcohol alters intracellular membranes’ functionality and permeability, which results in injurious inflammatory reactions (Werner et al., 2002). Amylase is a clinical indicator of pancreatitis. In this study, alcohol was found to consistently cause liver and pancreas injury. We found that higher amylase levels were associated with heavy alcohol exposure. On the other hand, SSRI treatment was able to reduce the increase in amylase associated with alcohol exposure.
Alcohol is known to adversely affect the lungs with most observations having focused on impairment of alveolar integrity, reductions in alveolar macrophage phagocytosis, compromised microbial clearance, poorer lung host defenses and the heightened susceptibility of alcoholics to infection (Szabo, 1999). The association between heavy alcohol consumption and lung disease is well established (Kershaw and Guido, 2008; Nelson and Kolls, 2002). Previous studies have examined the potential mechanisms underlying alcohol abuse and acute lung injury and have focused on cytokine mediated necrosis of alveolar epithelial cells (Joshi and Guidot, 2007) and increased epithelial permeability (Bechara et al., 2004). Our result revealed that the Alc group had a higher LDH level in BALF, which demonstrated the presence of increased epithelial permeability and damage to the alveolar cells. Our histological findings have also found that ethanol infusion is able to induce an increase in lung edema and interstitial cell infiltration.
There are significant alterations in host defense mechanisms after alcohol consumption (Romeo et al., 2007). Heavy alcohol exposure increases pro-inflammatory cytokine levels (Goral et al., 2008; Romeo et al., 2007). The pro-inflammatory cytokines, such as TNF-α, play a critical role in the initiation and development of alcoholic hepatitis (Szab and Bala, 2010). It has been revealed that alcohol induces hepatic TNF-α production (Zhou et al., 2003). TNF-α also promotes the secretion of other pro-inflammatory cytokines including IL-6. Inflammatory cytokines, such as TNF-α, are the signaling proteins that are produced in response to infection or cell damage (Subeq et al., 2009). In the present study, alcohol induced a number of changes in various biochemical values (GOT, GPT, BUN, creatinine, AST, ALT, CPK, LDH, and amylase). In addition, serum TNF-α and IL-6 were found to have increased after alcohol administration. The histological results confirmed the presence of alcohol induced organ damage in a number of systems.
In conclusion, multiple organ damage and an increase in the levels of pro-inflammatory cytokines were found to occur after ethanol was introduced into rats using our intravenous slow infusion model. The pathology related to alcohol is well known and is associated with a disruption of the cytokine balance and of cytokine functioning (Crews et al., 2006; Romeo et al., 2007). SSRI administration is known to be associated with an increase in anti-inflammatory cytokines. Our results provide evidence that SSRI administration is able to reduce liver, heart and pancreas damage by reducing the increase in pro-inflammatory cytokines that occurs after a heavy exposure to alcohol. The findings suggest that SSRI might be effective in reversing alcohol-induced pro-inflammatory cytokine production and organ damage. Antidepressant treatment of alcohol abusers may be not only improve their emotional problems but also help to avoid the inflammatory response and tissue damage induced by alcohol poisoning.
Footnotes
Acknowledgements
NTLi and RPL contributed equally to this work. The authors are grateful to Mike Biological Technologies (Second Floor, No. 150, Section 2, Roosevelt Road, Taipei, Taiwan) for their technical advice on conscious animal experimentation.
Conflict of interest
The authors declare that there are no conflict of interest.
Funding
This work was supported by the Tzu Chi University (grant numbers TCIRP 98004-1, TCRPP99016 and TCRPP99019).