
Abstract
Cognitive deficits are highly prevalent in alcohol-dependent (AD) patients and may have a detrimental impact on treatment response and treatment outcome. Enhancing cognitive functions may improve treatment success. Modafinil is a promising compound in this respect. Therefore, a randomized double-blind placebo-controlled trial was conducted with modafinil (300 mg/d) or placebo in 83 AD patients for 10 weeks. Various cognitive functions (digit span task, Tower of London task, Stroop task) were measured at baseline, during and after treatment. Compared to placebo, modafinil improved verbal short-term memory (number of forward digit spans) (p=0.030), but modafinil exerted a negative effect on the working memory score of the digit span task (p=0.003). However, subgroup analyses revealed that modafinil did improve both working memory and verbal short-term memory in AD patients with a poor working memory ability at baseline (25% worst performers), whereas no significant treatment effect of modafinil was found on these two dependent variables in patients with good working memory skills at baseline (25% best performers). No effect of modafinil was found on measures of planning (Tower of London task) and selective attention (Stroop task). Further research is needed to better understand the relationship between cognitive remediation and treatment outcome in order to design targeted treatments.
Introduction
Cognitive impairments are common in alcohol-dependent (AD) patients. In particular, impairments in attention, working memory and executive functions such as planning and response inhibition are highly prevalent (Fernandez-Serrano et al., 2011; Goudriaan et al., 2006; Moselhy et al., 2001; Tedstone and Coyle., 2004; Van Holst and Schilt, 2011). Although it remains difficult to know whether cognitive deficits are a consequence of prolonged alcohol use or whether cognitive deficits are a vulnerability factor for developing alcohol dependence, it is well-known that cognitive deficits, such as impairments in verbal memory, working memory, inhibition and visuomotor functions, can have a negative impact on treatment response and relapse (Blume et al., 2005; Moselhy et al., 2001; Teichner et al., 2001, Wölwer et al., 2001). However, tests of the direct influence of cognitive impairment on treatment outcome in alcohol dependent patients have yielded only weak and inconsistent results (Bates et al., 2002). Therefore, it is likely that the relationship between cognitive functioning and treatment outcome is rather indirect. For instance, poor cognitive functioning may lead to poor treatment outcome through an inability of the patient to integrate new information in real life or to manage stressful situations. Therefore, enhancing cognitive functions after detoxification may support AD patients to maintain abstinence and to improve treatment success. Spontaneous recovery of cognitive deficits as a result of prolonged abstinence may take place (Kopera et al., 2012; Van Holst and Schilt, 2011), however such improvements tend to occur very slowly and are often restricted to the first months after abstinence (Bartels et al., 2007; Bates et al., 2005). Furthermore, not all cognitive functions improve (Fernandez-Serrano et al., 2011; Manning et al., 2008). So a clear need arises within the field of alcohol dependence to develop new effective treatments to enhance cognitive functions.
A potential compound in this respect is modafinil (2-[(diphenylmethyl) sulfinyl] acetamide), a wakefulness-promoting drug that is currently approved by the Food and Drug Administration for the treatment of narcolepsy. One of the main effects of modafinil is inhibition of the dopamine (DA) and noradrenaline (NA) transporter resulting in increased levels of extracellular DA and NA (Minzenberg and Carter, 2008; Volkow et al., 2009). Besides its wakefulness-promoting effects, modafinil is also known for its cognitive enhancing effects. Modafinil improves memory, planning abilities, divided attention and sustained attention in healthy individuals as well as in different patient populations, such as patients with attention deficit hyperactivity disorder (ADHD), major depressive disorder, schizophrenia and substance use disorders (for reviews see Joos et al., 2010; Minzenberg and Carter, 2008). Furthermore, modafinil reduced state impulsivity in alcohol dependent patients, but had no positive effect on clinical outcome measures in a sample of alcohol dependent patients (Joos et al., 2013). However, effects of modafinil were found to be baseline dependent. Results of our clinical trial indicated that modafinil reduced the number of drinking days in alcohol dependent patients with poor response inhibition (measured with the Stop Signal Task), whereas patients with better baseline response inhibition demonstrated detrimental effects of modafinil on alcohol use (Joos et al., 2013). Comparable differential effects of modafinil have also been reported by Kalechstein et al. (2010) in methamphetamine dependent patients, by Finke et al. (2010) in healthy volunteers with high versus low performance on a sustained attention task, by Zack and Poulos (2009) in pathologic gamblers with high versus low self-reported impulsivity levels, and by Schmaal et al. (2013) in alcohol-dependent patients with high versus low baseline levels of response inhibition.
In summary, cognitive impairments are common in AD patients and may result in poor treatment response and treatment outcome. Therefore, improving cognitive functions with a cognitive enhancer such as modafinil may reduce the number of treatment failures. However, these effects might be more prominent or may occur only in patients with poor baseline cognitive functioning. So far, the effect of modafinil on impulsivity and on clinical outcome measures has been previously examined (Joos et al., 2013; Schmaal et al., 2013; Zack and Poulos, 2009), but no results are available concerning the effect of modafinil on cognitive functions in AD patients. Therefore, we conducted a randomized, double-blind, placebo-controlled trial with modafinil in treatment seeking AD patients. It was hypothesized (a) that a 10-week treatment with modafinil in AD patients improves cognitive performance on all cognitive tasks, and (b) that subgroups with poor cognitive functioning at baseline benefit more from modafinil than subgroups with better baseline cognitive abilities. In addition, baseline cognitive functioning was also measured in a sample of 30 healthy controls, in order to examine whether AD patients performed worse on cognitive tasks compared to healthy controls at baseline. However, this hypothesis is beyond the scope of this paper and therefore comparisons of the demographic and performance characteristics between the AD group and the healthy controls are presented in the supplementary material.
Method
Participants
Treatment-seeking AD patients between 18–60 years were consecutively recruited from one of two addiction treatment services in Belgium (Antwerp) with a residential and/or day care setting. Eligibility for participation was screened by examination of the psychiatric history according to the MINI-plus International Neuropsychiatric Interview (Van Vliet and De Beurs, 2007) and confirmed by clinical evaluation, laboratory tests (blood, liver functioning, urinalysis) and an electrocardiogram. Inclusion criteria were (a) a current diagnosis of DSM-IV alcohol dependence, and (b) participation in the cognitive behavioral treatment program.
Exclusion criteria were: (a) current diagnosis of DSM-IV substance dependence other than alcohol (MINI-plus; except for nicotine and cannabis); (b) current use of psychoactive medications (with exception of sleep medication with a maximum half-life of eight hours); (c) history of psychotic disorders, current mood or anxiety disorders; (d) IQ below 75 based on the Dutch version of the National Adult Reading Test (NART; Schmand et al., 1992); (e) amnesic and neurological disorders (trauma, epilepsy); (f) severe somatic disorders (hypertension, myocardial infarct, liver cirrhosis); and (g) color blindness. Additional exclusion criteria for AD patients were (h) being on an active low-calorie diet (<1000 calories/day), (i) hypersensitivity for modafinil and/or lactose, and (j) for women, being pregnant or breastfeeding.
All participants gave written informed consent and received a monetary remuneration of €40. Simultaneously, the patient group participated in a study that investigated the effect of modafinil on relapse and on clinical characteristics such as impulsivity; results of this study are published in Joos et al. (2012). The trial was approved by the medical ethics committee of the Antwerp University Hospital (Belgium) and was registered at the Dutch Trial Register (NTR1736; www.trialregister.nl).
Study design
The study used a randomized double-blind placebo-controlled design with an active medication (modafinil 300 mg) and a placebo (lactose) condition. After screening, patients were randomized (with a computer generated code) to one of the two treatment conditions, by using a stratified, permuted block randomization with gender as the only stratum. Blocks contained random sizes of two, four or six allocations for males, and two or four allocations for females. All research personnel, i.e. those who enrolled, treated, and assessed the patients, was blind to the medication assignment until the study was concluded.
Modafinil 100 mg immediate release tablets and matching placebos were manufactured by TioFarma, Oud-Beijerland, The Netherlands. A single morning dose was administered for 10 weeks and was slowly titrated (100 mg/day at day 1–4; 200 mg/day at day 5–8; 300 mg/day at day 9–70). In case of adverse effects the treatment dose was reduced by 100 mg at a time. For safety reasons, physical examinations like blood pressure, pulse and temperature were done daily at the start, and weekly when these parameters and the medication dosage were stable. After 10 weeks, the study medication was discontinued without taper.
Measures
Clinical characteristics
Sociodemographic characteristics were collected by means of a structured interview. Mean alcohol use in the 30 days before admission and the number of abstinence days before cognitive testing were surveyed with a Time Line Follow Back interview (Sobell and Sobell, 1992). To promote comparison between participants, the amount of alcohol consumed was converted into standard alcohol drinks of approximately 10 g alcohol per drink (Lemmens, 1994). Furthermore, years of heavy drinking was assessed, defined as drinking alcohol at least three times a week (regardless of the dosage) or during two consecutive days (Hendriks et al., 1989).
Cognitive functions
A detailed description of the cognitive function tasks is given in the supplementary material. The digit span task (Wechsler, 1997) was used to measure verbal working memory (WAIS-III, Dutch version, Swets Test Publishers, 2000). The verbal working memory measure used as a primary dependent variable was the total number of correctly reproduced backward digit spans divided by the total number of correctly reproduced forward digit spans (Goudriaan et al., 2006). A higher score corresponds to a better verbal working memory ability. Scores of the forward digit span task were used as a secondary outcome measure representing immediate short-term memory.
A computerized Tower of London (ToL) task was administered to measure spatial planning abilities (Van den Heuvel et al., 2003). The primary dependent measure of this task was the accuracy or the number of correct responses, calculated as a weighted sum that takes into account the difficulty level of each trial (number of correct two-step trials×2) + (number of correct three-step trials×3) +… etc.). The latency or the average time needed per trial to give a response was used as a secondary dependent variable.
A computerized version of the classic Color-Word Stroop task was applied to measure selective attention/cognitive interference (Cox et al., 2006). The primary dependent variable was the interference score, calculated by subtracting the mean reaction time (s) on the congruent stimuli from the mean reaction time on the incongruent stimuli for all correct trials. Secondary outcome measures of the Stroop task were the accuracy or the percentage of correct responses on the congruent trials and the accuracy on the incongruent trials.
Procedure
For the patients, baseline testing took place when they were fully detoxified, were not taking benzodiazepines, and had a score below 12 on the Short Alcohol Withdrawal Scale (SAWS; Gossop 2002). Baseline data (T0) were collected on two separate days: a first test session when screening information (e.g. MINI-Plus, NART), demographic and alcohol use characteristics were collected; and a second session when cognitive tasks were performed. With regard to the healthy control subjects, baseline testing took place on one single test day, with a break of 15 min after each hour of testing. The order of the test administration was the same for all participants. Subsequently, concerning the retesting of the AD patients, testing during treatment (T1) occurred in week 5 or 6 of the treatment period and testing after treatment (T2) occurred after a medication wash-out period of at least one week. It was expected that cognitive functions improve with modafinil between baseline and T1. Furthermore, based on results of Swanson et al. (2006) who reported the absence of a rebound effect of modafinil (two-week follow-up) after discontinuation of modafinil in children with ADHD, it was hypothesized that these improvements are maintained at T2.
During inpatient stay, medication was administered under supervision, in all other cases medication compliance was measured by means of self-report and pill count of returned containers. Patients who participated from home were screened on alcohol and drug use with breath and urine analysis before each testing. Inpatients were regularly screened on drug and alcohol use during their standard treatment. Relapse in alcohol use during treatment was no reason to stop participation, but patients needed to be sober while performing the tests in order not to bias the test results. Data were excluded from analyses when a patient returned a positive urine test for any drug, including cannabis.
Statistical analysis
Our sample size was based on a previous reported trial with modafinil for cocaine dependence (Dackis et al., 2005). Initially, we attempted to collect 100 participants, which would allow us to detect a standardized effect size of minimal d=0.70 for our main analyses with 80% power, calculated with G*Power (Buchner et al., 1997) and based on independent two-tailed sample t-test analysis with alpha=0.010 after Bonferroni correction for multiple comparisons (see below). However, due to time and practical considerations, the trial ended with 83 randomized patients, resulting in a reduced power of 70% to find group differences in the primary outcome measures in the total sample.
First, to explore baseline differences in demographic characteristics and baseline cognitive test results between patients and controls and between the modafinil and the placebo group, independent sample t-tests were used for continuous variables and chi-square tests were used for categorical variables.
Second, mixed-effects repeated-measures analyses (Time (Baseline, T1, T2), Treatment (modafinil or placebo), Time×Treatment), assuming that data are missing at random, were conducted to analyze the effect of modafinil on cognitive functions compared to placebo in AD patients.
Third, to explore whether low cognitive performers were more likely to respond to modafinil administration than high cognitive performers, the 25% of patients with the highest baseline cognitive scores and the 25% of patients with the lowest baseline cognitive scores on each of the three primary dependent variables (working memory score of the WAIS digit span task, accuracy measure of the ToL and interference score of the Stroop task) were selected. This resulted in three different subgroup variables, which were each entered as a third variable into the mixed model, resulting in a model with three main effects (Time, Treatment, Baseline cognition), three corresponding two-way interactions and one three-way interaction (Time×Treatment×Baseline cognition). However, given the randomized design, it is allowed to fit a three-way interaction model without including the main effect of treatment and the two-way interaction Treatment×Baseline cognition in the model (Fitzmaurice et al., 2004: 126–127) in order not to jeopardize the power of the study. Subsequently, the meaning of each significant three-way interaction was explored by analyzing a two-way Time×Treatment interaction in each subgroup.
To correct for multiple comparisons, a Bonferroni correction was applied to the mixed-effects repeated-measures analyses (p<0.017; α=0.05/3 primary outcome variables) and to the subgroup analyses (p<0.006; α=0.05/9). For exploratory analyses on secondary outcomes the significance level was set at p<0.05. All analyses were performed with SPSS Statistics 20.0.
Results
Participant flow
Overall, 706 treatment seeking AD patients were consecutively admitted to the participating treatment services, of which 113 patients met inclusion criteria. Of those patients, 30 declined to participate and the remaining 83 patients (mean age=41.8 years; standard deviation (SD)=9.4; 85.5% males) were randomized to the modafinil (n=41) or the placebo (n=42) condition. Drop-out was similar in the modafinil (n=17; 41.5%) and the placebo group (n=15; 33.4%) (χ2=0.29, p=0.591), and no significant difference was observed between groups with regard to time to drop-out (log-rank (Kaplan-Meier): χ2=0.54, p=0.544). No between-group differences occurred with regard to medication compliance (mean modafinil group: 0.83 (SD=2.2) pills; mean placebo group: 0.86 (SD=1.7) pills; t=0.044, p=0.965). Relapse in alcohol use occurred at the same rate in both treatment groups (any relapse: χ2=3.76, p=0.289; relapse in heavy drinking: χ2=5.75, p=0.124; see Supplementary Material, Table S2 for more details).
Baseline test performance
No significant differences were found between the modafinil and the placebo group with regard to the demographic characteristics and the alcohol and substance use measures. However, treatment groups significantly differed on the number of correctly reproduced backward digit spans, likewise resulting in a significant difference on the working memory score (see Table 1 for means and standard deviations). Therefore, the baseline backward digit span task score was entered as a covariate in the mixed-effect repeated measures analyses hereafter when the digit span working memory score was entered as a dependent variable. For more details regarding participant flow (only AD patients), drop-out, adverse events and treatment compliance, we refer the reader to the flow chart (Figure 1).
Baseline characteristics of the modafinil and the placebo group with means, standard deviations (SDs) and p-values (t- or chi-square test).
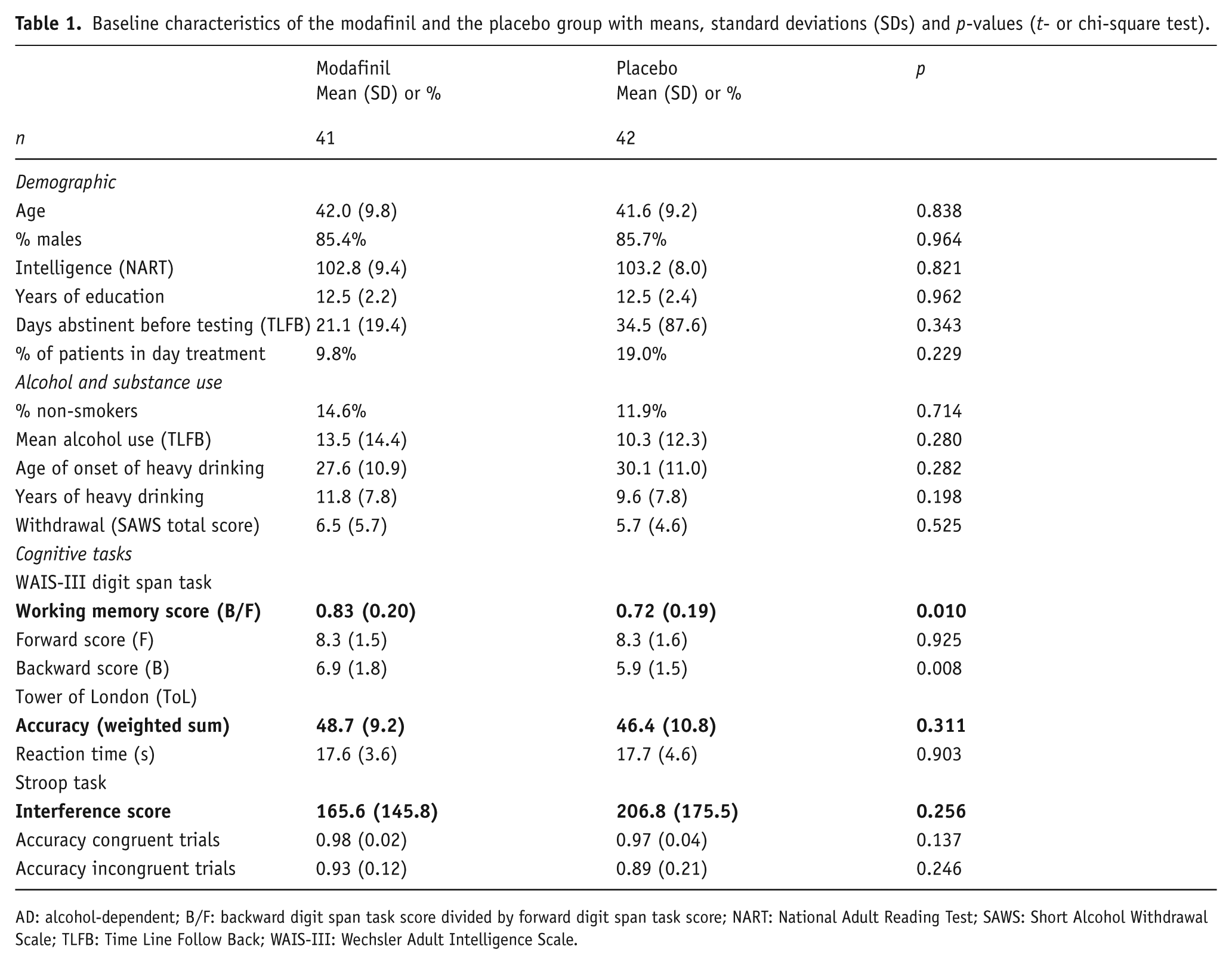
AD: alcohol-dependent; B/F: backward digit span task score divided by forward digit span task score; NART: National Adult Reading Test; SAWS: Short Alcohol Withdrawal Scale; TLFB: Time Line Follow Back; WAIS-III: Wechsler Adult Intelligence Scale.
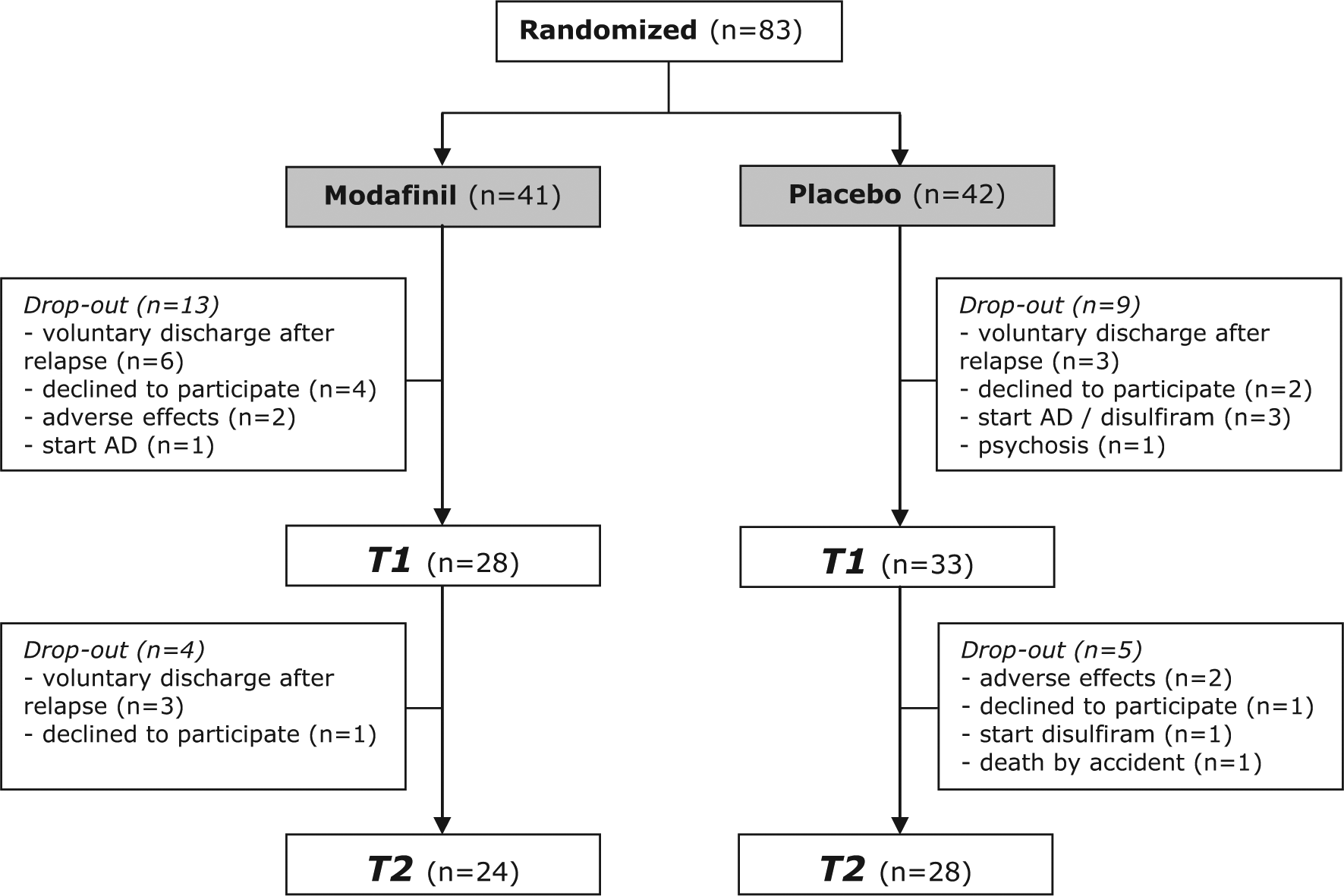
Study participants (alcohol dependent patients) flow diagram. Reasons for drop-out are reported.
Treatment effect modafinil
Detailed test results of the neuropsychological measures on T0, T1 and T2 (modafinil versus placebo) can be found in Supplementary Material, Table S3.
Main performance indicators
A significant time by treatment interaction (Bonferroni: p<0.017) was found for the digit span working memory score (F(2,192)=5.910; p=0.003), indicating that patients achieved a lower working memory score over time in the modafinil group compared to the placebo group (see Figure 2), i.e. in contrast to our expectations modafinil did not improve but worsened working memory compared to placebo in the total sample of AD patients.
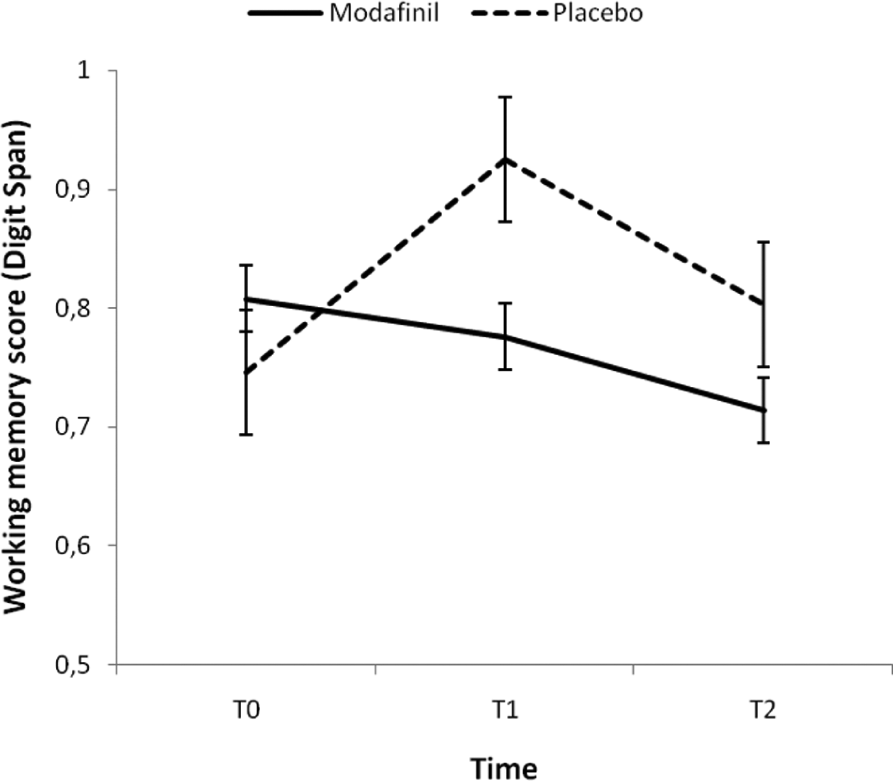
Time by treatment (modafinil (n=41) vs placebo (n=42); total sample) interaction based on mixed-model repeated measures (MMRM) analysis of working memory score (digit span: backward/forward score), adjusted for baseline backward digit span score and with error bars representing standard errors.
The accuracy score of the ToL task improved over time (F(2,191)=6.956; p=0.001), but the rate of change did not differ between treatment groups (time by treatment interaction: F(2,191)=0.188; p=0.829). Finally, no significant main or interaction effects were found for the interference score of the Stroop task.
Secondary performance indicators
A significant (p<0.05) time by treatment interaction was observed for the forward digit span task (F(2,192)=3.581; p=0.030). Results showed that patients could reproduce more correct forward spans with modafinil compared to placebo (see Figure 3).
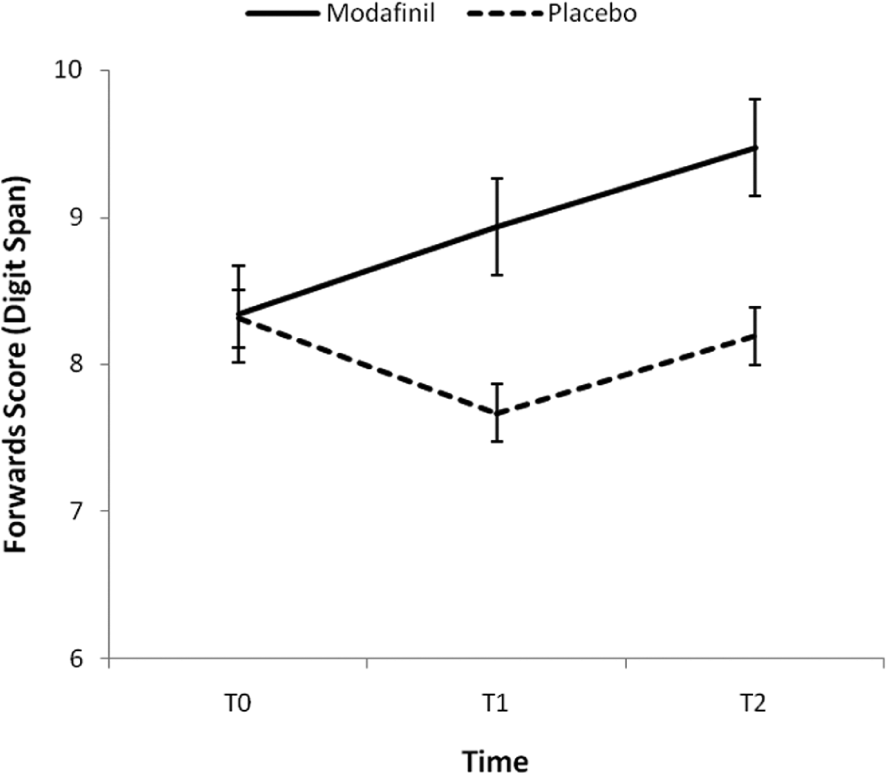
Time by treatment (modafinil (n=41) vs placebo (n=42); total sample) interaction based on mixed-model repeated measures (MMRM) analysis for forward digit span task score (digit span), with error bars representing standard errors.
The latency of the ToL task significantly changed over time (F(2,191)=23.387, p<0.001 respectively), with a decrease between baseline and T1 and an increase in reaction times between T1 and T2, but there was no significant time by treatment interaction.
Finally, no significant main or interaction effects were found for the accuracy measures of the Stroop task, with exception of a significant main effect of treatment for the accuracy score on the incongruent trials of the Stroop task (F(1,191)=4.009, p=0.047). These results indicate an overall higher accuracy in the modafinil group compared to the placebo group, but this difference did not change over time, as there was no significant time by treatment interaction for the accuracy score on the incongruent trials of the Stroop task (F(2,191)=0.057, p=0.945).
Subgroup analyses
A significant time×treatment×baseline cognition (three-way) interaction (Bonferroni: p<0.006) was only found for the 25% highest (n=24) versus 25% lowest (n=18) performing subgroups based on the working memory score of the digit span task with the working memory score as dependent variable (F(3,97)=5.809; p=0.001). These results indicate that the effect of modafinil compared to placebo depends on the baseline working memory capacity of the AD patients. No differences occurred with regard to age, gender, years of education, number of days abstinent before testing and baseline alcohol intake between the two high performing groups (modafinil vs placebo) and the two low performing groups (modafinil vs placebo) (see details in the Supplementary Material, Tables S4(a) and S4(b)). In order to better understand the direction of this significant three-way interaction, separate treatment×time interaction models were fitted for the two subgroups; patients with poor working memory capacity at baseline achieved a better working memory score with modafinil compared to placebo (F(2,39)=5.746; p=0.006), whereas no significant treatment effect was found in the subgroup of patients with the 25% best working memory score at baseline (F(2,58)=2.377; p=0.102) (See Figure 4). However, although this latter result did not reach significance, the data suggest a decline and not an increase of the working memory score with modafinil compared to placebo in high performing patients at baseline.
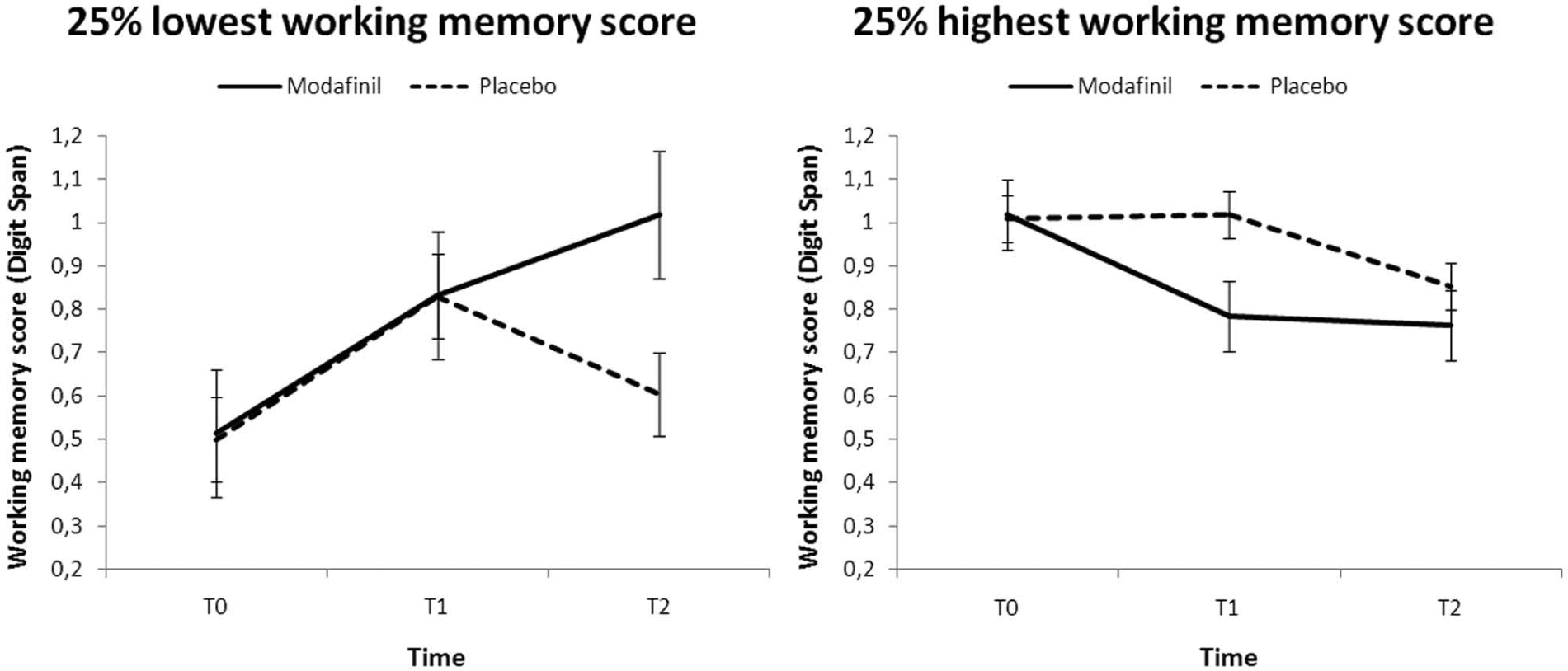
Time by treatment (modafinil vs placebo) interaction based on mixed-model repeated measures (MMRM) analysis with working memory score as dependent variable (digit span: backward/forward score) in subgroups of alcohol dependent patients with the 25% highest (n=24; working memory score>0.875) versus the 25% lowest (n=18; working memory score<0.636) working memory score on the digit span task, adjusted for baseline backward digit span task score and with error bars representing standard errors.
Discussion
This study investigated whether modafinil can enhance cognitive functioning in abstinent medication-free AD patients. The results confirmed our hypothesis that modafinil compared to placebo improves immediate verbal short-term memory in the total sample of AD patients, and that modafinil improves working memory, but only in AD patients with poor working memory capacity at baseline. However, in contrast to our hypotheses, no differences between the modafinil and the placebo group were observed on the ToL measuring spatial planning and the Stroop measuring selective attention. In contrast to our results, previous research with modafinil in a population of cognitively impaired alcohol dependent patients did not find any significant differences of modafinil compared to placebo in various psychometric tests (Saletu et al., 1990). However, modafinil tended to improve memory and attention, although not significantly (Saletu et al., 1990).
An important finding of this study is that baseline cognitive functioning must be taken into account before prescribing modafinil to a non-selected sample of AD patients. Namely, although modafinil exerted negative effects on working memory in the total sample of AD patients, results showed that one specific subsample of AD patients (i.e. with low baseline performance) did benefit from modafinil. Comparable effects of modafinil have been published previously (Dean et al., 2011; Eagle et al., 2007; Finke et al., 2010; Heinzerling et al., 2010; Joos et al., 2013; Kalechstein et al., 2010; Schmaal et al., 2013; Zack and Poulos, 2009). These bi-directional findings might be related to differences in brain dopamine (DA) and noradrenaline (NA) levels between high versus low performing subjects. In their theory on the ‘inverted-U-shape’ relation between baseline catecholamine levels and the effect of catecholaminergic drugs, Cools and D’Esposito (2011) state that the efficacy of a catecholaminergic drug such as modafinil depends on basal DA/NA levels; subjects with low brain DA/NA levels might benefit from this drug, whereas the opposite is true for subjects with high brain DA/NA levels. First, the fact that modafinil worsened working memory in the whole sample of alcohol dependent patients might be explained by this theory, as alcohol dependent patients did not significantly differ in performance compared to the healthy control group at baseline (see Supplementary Material, Table S1). Second, Cools and D’Esposito (2011) assume that distinct optimum levels of DA/NA exist for different cognitive functions, which implicates that although a specific drug might improve performance on one task, the same drug might worsen performance on another task. Our results confirm this theory; performance worsened with modafinil in the total sample of AD patients, while performance on the forward digit span task improved with modafinil compared to placebo. Overall, the inverted-U-shape function emphasizes not only the importance of baseline screening before prescribing modafinil, but also the need to be attentive for possible paradoxical consequences on different cognitive processes.
The above contradictory treatment effects may also be explained by the fact that the modafinil group had already a better baseline performance on the forward digit span task than the placebo group; such baseline differences were not present for the backward digit span task. However, given that we controlled for this baseline differences in our analyses, we suppose that this explanation can be ruled out. Finally, different neural mechanisms may also underlie these two cognitive measures, resulting in a differential effect of modafinil. Indeed, results from a functional magnetic resonance imaging (fMRI) study indicate that backward recall is associated with a dominant activation of the dorsolateral prefrontal cortex (DLPFC) and the occipital and parietal cortices, while forward recall, is associated with activation of the right frontal inferior gyrus (Sun et al., 2005). Apparently the DLPFC seems to play an important role in backward recall but not in forward recall. Furthermore, given that the DLPFC is involved in at least two of the four major dopamine pathways in the brain (mesolimbic and mesocortical pathway) (Cools, 2008), and given that bi-directional results might be caused by differences in basal DA/NA levels according to the inverted-U-shape function, this might explain why bi-directional effects are seen with modafinil on backward recall, but not on forward recall.
Not only pharmacological treatments (for review see: Brady et al., 2011) but also behavioral interventions such as working memory training (Houben et al., 2011), cognitive remediation therapy (Rupp et al., 2012) and goal management training (Alfonso et al., 2011) may improve cognitive functioning. In addition, the study of Rupp et al. (2012) also found that cognitive remediation therapy was associated with a reduction of craving and better well-being at the end of an abstinence-oriented treatment.
Overall, results show a clear connection between training and (cognitive) improvement, but only a few studies focused on the precise relationship between cognitive remediation and alcohol use (Houben et al., 2011) or treatment outcome (Rupp et al., 2012). It is however important to understand this relationship in order to design targeted treatments. Analyses in the same sample of patients concerning the effect of modafinil on relapse did not show any significant improvement of modafinil on various treatment outcome variables (percentage of abstinent days, percentage of heavy drinking days and mean alcohol use) (Joos et al., 2013). Therefore, we can conclude that the improved performance on the forward digit span task with modafinil that was reported in this manuscript was not related to a significant improvement in treatment outcome. In addition, the decreased performance on the working memory score did not exert any detrimental effects on treatment outcome. These results suggest that not a direct, but rather an indirect or more complex model between cognitive remediation and treatment outcome need to be addressed. For example, Houben et al. (2011) found that a working memory training improved working memory and reduced alcohol intake for more than one month after the training in problem drinkers. However, this effect was moderated by the participant’s level of automatic preferences or impulses for alcohol, or in other words, participants with strong automatic impulses to drink alcohol benefited the most from the working memory training. Further research is recommended to further explore the precise relationship between cognitive remediation and treatment outcome in AD patients.
Finally, our results should be viewed in the light of some limitations. Due to the limited sample size, this study was only able to detect large effect sizes of modafinil on cognitive functioning. This may have prevented smaller treatment effects from becoming statistically significant and may explain why we did not find an effect of modafinil on our spatial planning and cognitive interference tasks, as these results are in contrast to previous studies (DeBattista et al., 2004; Randall et al., 2005; Spence et al., 2005; Turner et al., 2003, 2004a, 2004b). On the other hand, this also means that the observed significant treatment effect of modafinil on working memory in the low baseline performing subgroup can be seen as a large treatment effect of high clinical relevance.
Notwithstanding these limitations we believe that the current study provides new insights into the use of modafinil in AD patients in order to enhance cognitive functioning. The results show a significant improvement of verbal short-term memory with modafinil in the total sample of abstinent AD patients and with modafinil improving working memory in AD patients with a low working memory capacity at baseline. However, negative effects may occur in patients with good baseline working memory skills and in unselected samples of AD patients. Overall, this study emphasizes the importance of baseline screening and thus patient treatment matching/personalized medicine before prescribing modafinil in AD patients. Further research is recommended to explore the precise relationship between cognitive remediation and treatment outcome in AD patients.
Supplemental Material
Supplemental Material, JOP503505_-_Supplementary_material – Effect of modafinil on cognitive functions in alcohol dependent patients: A randomized, placebo-controlled trial
Supplemental Material, JOP503505_-_Supplementary_material for Effect of modafinil on cognitive functions in alcohol dependent patients: A randomized, placebo-controlled trial by Leen Joos, Anna E Goudriaan, Lianne Schmaa, Wim van den Brink, Bernard GC Sabbe and Geert Dom in Journal of Psychopharmacology
Footnotes
Acknowledgements
The authors would like to thank the patients for their commitment and time and thank the participating hospitals: the Psychiatric Centre Brothers Alexians (Boechout, Belgium) and the Psychiatric Hospital Sint-Norbertus (Duffel, Belgium).
Conflicts of interest
Wim van den Brink is a consultant for Merck Serono (acamprosate) and Lundbeck (nalmefene) and has received speaker fees from Merck Serono, Lundbeck, Eli Lilly, Pfizer, and Schering-Plough. In addition, he has received unrestricted grants for investigator-initiated studies from Alkermes (naltrexone XR) and Neurosearch (tesofensine). Geert Dom has received speaker fees from Merck, Lundbeck, GlaxoSmithKline, Johnson & Johnson and Astra Zeneca. All other authors have no conflict of interest to declare.
Funding
Funding for this study was provided by the Netherlands Organization for Scientific Research (ZonMW), (Grant no: 31160003).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.