
Abstract
Accumulating evidence underscores the utility of ketamine in treating severely treatment-resistant depressed patients. We investigated the relationship between the rapid antidepressant effects of ketamine and hippocampal volume, a biomarker of antidepressant treatment outcome. We gave 16 medication-free, major depressive disorder (MDD) patients a single, sub-anesthetic dose infusion of ketamine (0.5 mg/kg, over 40 min). We assessed depression severity pre-treatment, and at 24 h post-treatment, with the Montgomery-Åsberg Depression Rating Scale (MADRS). Prior to treatment, patients underwent magnetic resonance imaging (MRI) to estimate their hippocampal volume: We obtained viable MRI data in 13 patients. Delta MADRS (post- minus pre-treatment) was significantly correlated with the pre-treatment volumes of the left hippocampus (r = 0.66; p = 0.01), but not the right hippocampus (r = 0.49; p = 0.09). The correlation between delta MADRS and the left hippocampus remained high (r > 0.6; p = 0.13), after controlling for several demographic and clinical variables, although the p value increased due to the reduced degree of freedom (df = 5). Ketamine exerts enhanced antidepressant effects in patients with a relatively smaller hippocampus, a patient population that has been repeatedly shown to be refractory to traditional antidepressants.
Keywords
Introduction
Treatment resistance is a critical issue in the management of major depressive disorder (MDD); for example, the STAR*D study reports that fewer than 50% of MDD patients respond to 3-month treatment with a monoaminergic re-uptake inhibitor (Trivedi et al., 2006). Identification of biological markers of treatment outcome will provide insight into the underlying pathology of treatment resistance and can potentially guide the development of novel therapeutics. In this brief report, we investigated the relationship between the rapid antidepressant effects of ketamine and hippocampal volume, a biomarker that was previously associated with treatment outcome in MDD patients treated with traditional antidepressants.
Convergent evidence has demonstrated aberrant glutamatergic function in mood and anxiety disorders. In animal models of depression, studies show reduced glutamate metabolism, abnormal glutamate release, reduced post-synaptic glutamate receptors and glutamate uptake deficits (Sanacora et al., 2011). These glutamatergic abnormalities are believed to precipitate excitotoxicity and structural changes leading to hippocampal volume reduction (Drevets et al., 2008). In human studies, smaller hippocampal volume is found in treatment-resistant depression (TRD) patients and has been consistently associated with a poor response to traditional antidepressants (Frodl et al., 2004, 2008; Hsieh et al., 2002; Kronmuller et al., 2008; MacQueen and Frodl, 2011; MacQueen et al., 2008; Vakili et al., 2000); however, the relationship between hippocampal volume and the novel glutamate-based antidepressant ketamine has not been previously reported.
This pilot study was conducted to determine whether smaller hippocampal volume is associated with the rapid antidepressant effects of the glutamate N-methyl-D-aspartate (NMDA) receptor antagonist, ketamine (Murrough et al., 2013; Zarate et al., 2006), in patients with TRD. Ketamine is an anesthetic that is found to exert rapid (within 4 hours) and potent (response rate 45–90%) antidepressant effects (Aan Het Rot et al., 2012). We addressed this question by conducting a trial of ketamine in patients with TRD and measuring their pre-treatment hippocampal volumes. We hypothesized that relatively small hippocampal volumes in TRD patients would be associated with an enhanced antidepressant response to ketamine. Consistent with this hypothesis, we also recently reported that riluzole, a glutamate-modulating agent with antidepressant and anxiolytic properties, exerts enhanced therapeutic effects in patients with smaller hippocampal volume (Abdallah et al., 2013).
Methods and materials
A subgroup of MDD patients who were enrolled in a randomized, double-blind, controlled clinical trial (ClinicalTrials.gov identifier: NCT00768430) of ketamine versus midazolam consented to participate in this neuroimaging study. Detailed procedures from the clinical trial are reported elsewhere (Murrough et al., 2013). All participants provided written informed consent, and an Institution Review Board (IRB) at Baylor College of Medicine in Houston, TX approved all procedures. All participants at the Baylor site who consented for the neuroimaging component who did not have magnetic resonance imaging (MRI) exclusion and were able to be scheduled within the constraints of the timing of the parent trial, were enrolled in our MRI study, blinded to their treatment assignment status. The parent trial randomly assigned patients under double-blind conditions to receive a single intravenous infusion of ketamine or midazolam, in a 2:1 ratio.
We gave 24 patients a baseline high-resolution MRI scan within 24 hours prior to their single intravenous infusion of ketamine (0.5 mg/kg over 40 minutes; n = 16) or midazolam (0.045 mg/kg over 40 minutes; n = 8). We excluded three participants in the ketamine group and two participants in the midazolam group whom had unsuccessful MRI scans, due to motion artifact. Our adult patients (age 21–80) were medication-free for 1 week (4 weeks for fluoxetine), had treatment resistance to at least three adequate antidepressant trials according to Antidepressant Treatment History Form (ATHF) criteria (Sackeim, 2001), and were currently in a major depressive episode according to Diagnostic and Statistical Manual (DSM)-IV TR criteria confirmed by a structured clinical interview (First et al., 1995). Major exclusion criteria included a lifetime history of a psychotic illness or bipolar disorder, alcohol or substance abuse/dependence in the previous 2 years, unstable medical illness, history of traumatic brain injury or neurological illness, taking contraindicated medications, or MRI contraindications such as metallic implants or claustrophobia.
Depressive severity was assessed at baseline, using the Montgomery-Åsberg Depression Rating Scale (MADRS) (Montgomery and Asberg, 1979), prior to the study drug administration and then repeated 24 hours following infusion.
For this pilot neuroimaging study, all our study procedures including MRI acquisition, treatment and follow-ups were conducted at only one site (the MEDVAMC/Baylor College of Medicine). The MRI acquisition was performed using a 3T Siemens Trio MR system (1 x 1 x 1 mm voxel, TR = 1200 ms, TE = 2.66 ms, flip angle = 12°, matrix size = 245 x 245, 192 1-mm slices). We performed the hippocampal volumetric segmentation as previously described (Abdallah et al., 2013). Briefly, we used the recon-all pipeline from the Freesurfer image analysis suite (http://surfer.nmr.mgh.harvard.edu/). This fully automated processing includes imaging segmentation and volumetric estimation of hippocampus and total brain segmentation volume (Fischl and Dale, 2000). Post-processing quality checking through visual inspection was carried out; however, no manual intervention was required. Previous studies show high agreement between FreeSurfer hippocampal segmentation and manual segmentation (Doring et al., 2011; Morey et al., 2009; Sanchez-Benavides et al., 2010). For a detailed description of the boundaries of FreeSurfer hippocampal segmentation, as compared to manual tracing, see Morey et al. (2009).
We used the IBM SPSS Statistics 19 (SPSS Inc.) program for our statistical analysis. Delta MADRS was computed by subtracting the baseline score from the 24-hour score. The adherence to the Gaussian distribution was tested prior to each analysis. Pearson’s product moment correlation was used to determine the relationship between pre-treatment hippocampal volume and the treatment outcome. In additional analyses, we used partial correlation to control for potential confounds, as detailed in the ‘Results’ section. All tests were 2-tailed, with the significance level set at p = 0.05. To reduce the number of comparisons, we restricted our analysis of clinical outcome to the parent trial’s primary outcome (i.e. MADRS at 24 hours post-treatment).
Results
The demographic and clinical characteristics of neuroimaging study participants are summarized in Table 1.
Demographic and clinical characteristics of pilot study subjects (n = 13).
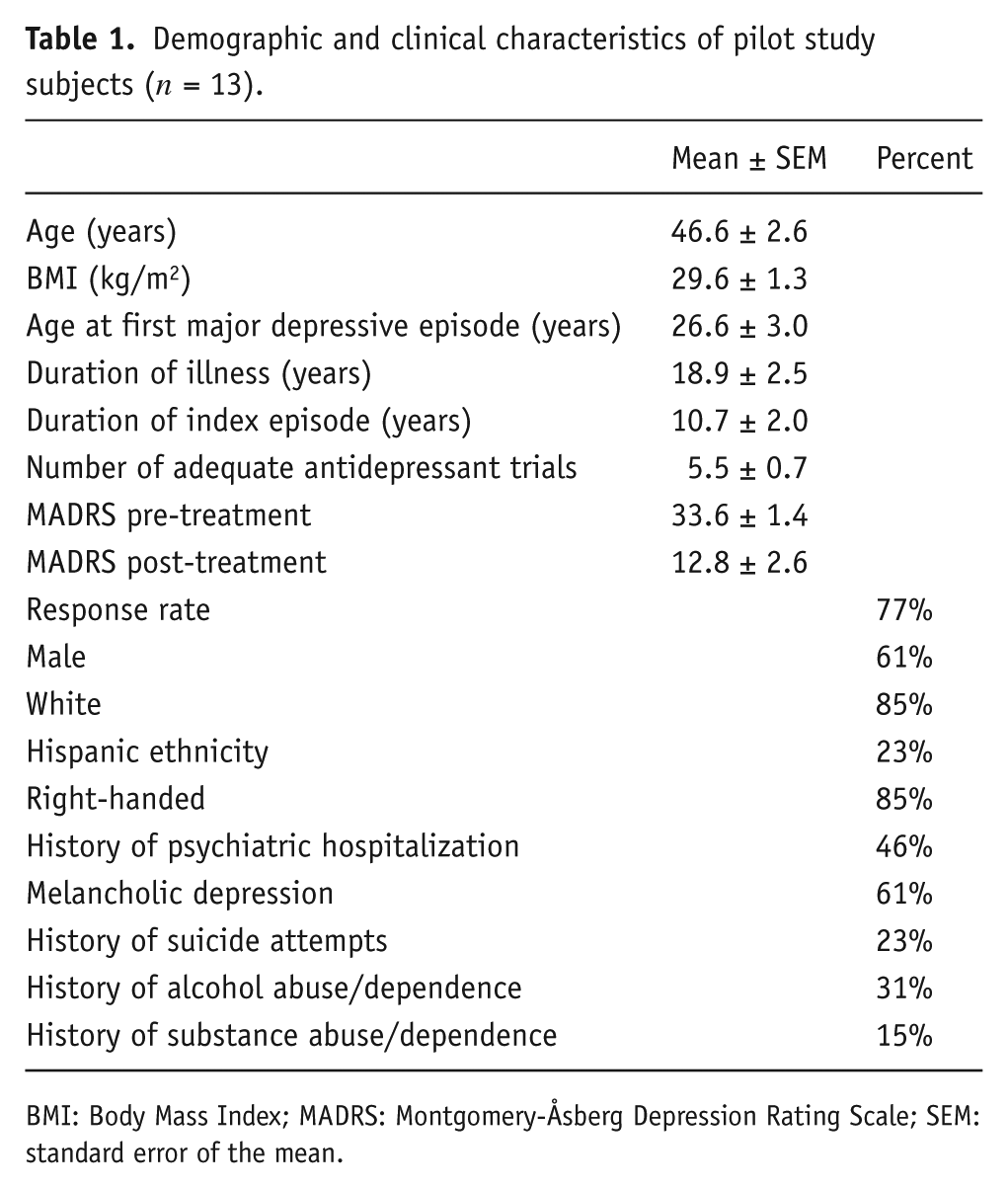
BMI: Body Mass Index; MADRS: Montgomery-Åsberg Depression Rating Scale; SEM: standard error of the mean.
We found a significant positive association between delta MADRS and the estimated volume of the left hippocampus at baseline (r = 0.66, p = 0.01; Figure 1); but there was no significant association between delta MADRS and the right hippocampal volume (r = 0.49, p = 0.09). The relationship between the left hippocampus and delta MADRS maintained significance following a conservative Bonferroni correction for multiple comparisons (p < 0.025). In addition, we also confirmed the positive relationship between hippocampal volume and delta MADRS using bootstrap analysis (see the online supplements). We conducted secondary analyses to examine the effects of potential moderating factors and confounders. We found that the association between left hippocampus and delta MADRS remained high (r > 0.6; df = 5; p = 0.13), after controlling for: total brain volume, handedness, age, gender, height and race. To provide preliminary data regarding the relationship between hippocampal volume and the antidepressant effects of the γ-aminobutyric acid (GABA)-modulating agent midazolam, we correlated hippocampal volume with MADRS scores changes. There was no significant correlation between delta MADRS (24 h post-treatment minus pre-treatment) and left (r = 0.73; n = 6; p = 0.10) or right hippocampal volume (r = 0.23; n = 6; p = 0.66).
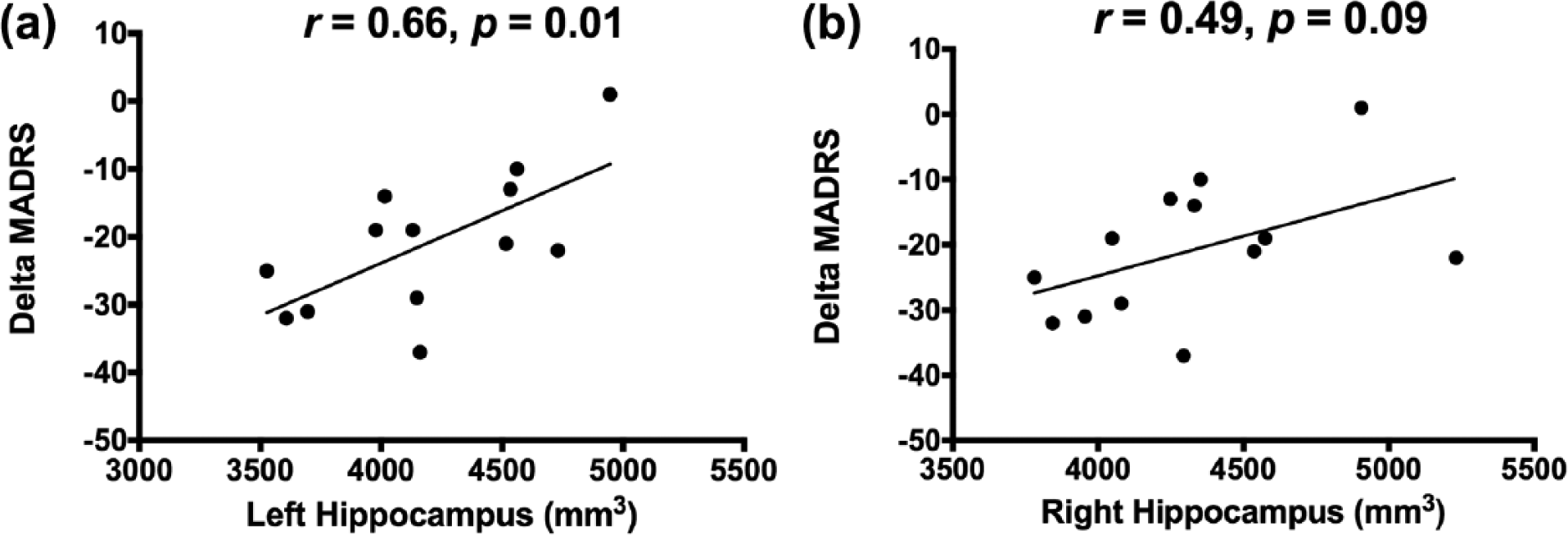
Correlation between response to ketamine and the left (a) or right (b) estimates of hippocampal volume.
Discussion
This pilot study was designed to determine the relationship between hippocampal volume and the rapid antidepressant effects of ketamine in patients with TRD. We found a significant association between left hippocampal volume and rapid improvement in depression severity, such that patients with a relatively smaller left hippocampus had a greater reduction in depression scores 24 hours following ketamine infusion. No statistically significant associations were found between baseline right hippocampal volume and the patients’ response to ketamine.
A major focus of MDD research is to understand the mechanisms underlying the rapid-acting antidepressant effects of ketamine (Duman and Aghajanian, 2012). Investigating the relationship between ketamine treatment and the volumetric deficits observed in treatment-resistant mood disorders could provide insight into mechanisms underlying ketamine’s antidepressant effects. Animal studies show that repeated stress impairs the tripartite glutamate synapse, leading to increased extracellular glutamate and excitotoxicity (Sanacora et al., 2011). The excitotoxicity results in structural deficits (i.e. reduction of spine density and dendritic shrinkage), precipitating an overall synaptic depression. A single injection of ketamine rapidly reverses these structural deficits within 24 hours of its administration in rodents, leading to an overall normalization of synaptic strength (Duman and Aghajanian, 2012). Ketamine is also found to rapidly (within 30 minutes) increase hippocampal Brain-Derived Neurotrophic Factor (BDNF) protein levels (Autry et al., 2011). The structural deficits observed when using MRI in depressed patients (e.g. smaller hippocampus) are believed to reflect the microstructural changes of neuronal remodeling observed in animal models of depression (Drevets et al., 2008). Strongly supporting this hypothesis, recent preclinical work by Kassem et al. (2013) related the stress-induced anterior cingulate and hippocampal volume deficits, as estimated by MRI, to the reduction of spine density and dendritic length in the same brain regions. Thus, we hypothesized that the rapid effects of ketamine on neurotrophic factors and synaptic plasticity would render the drug particularly effective in patients with relatively greater structural deficits, as evidenced by their smaller hippocampal volumes.
Of note, there was a positive, yet statistically non-significant, association between the left hippocampal volume and the antidepressant effects of the GABAergic agent midazolam. While the reader should interpret these preliminary data with extreme caution, it is an intriguing observation that, if confirmed in larger samples, would raise an important question regarding the specificity of the ketamine finding and whether a smaller hippocampal volume would predict enhanced antidepressant effects, regardless of the treatment modality (i.e. glutamatergic, GABAergic, monoaminergic, or even placebo). We are not aware of studies reporting the relationship between hippocampal volume and placebo antidepressant effects; however, there is relatively consistent literature associating smaller hippocampal volume with poor response to monoaminergic and traditional antidepressants (Frodl et al., 2004, 2008; Hsieh et al., 2002; Kronmuller et al., 2008; MacQueen et al., 2008; Sheline et al., 2012; Vakili et al., 2000). In contrast, smaller hippocampal volume predicted enhanced response to ketamine (the current report) and riluzole (Abdallah et al., 2013). As predicted, given the tight coupling between glutamate and GABA activities, both ketamine and riluzole have profound GABAergic effects (Banasr et al., 2010; Chowdhury et al., 2012). Thus, it is plausible that patients with smaller hippocampal volumes are more likely to benefit from glutamate-/GABA-modulating agents, while those with larger hippocampal volumes are better treated with monoaminergic antidepressants.
A limitation of this study was the small sample size, which may have constrained our ability to detect a significant association between treatment effects and right hippocampal volume; however, if the observed hemispheric laterality was to be confirmed in larger future studies, it would be consistent with our prior work in non-human primates, associating rearing stress with left, but not right, hippocampal deficits (Coplan et al., 2010; Jackowski et al., 2011). Another limitation was the lack of a healthy control group; thus, it is unknown whether the relatively smaller hippocampus in the current sample is abnormally small compared to the general healthy population. The strengths of this study include its relevance to the understanding of the neurobiology of TRD and its relevance to the development of response biomarkers for patient stratification and drug discovery. The use of fully automated segmentation methods further facilitates the implementation of these response biomarkers, if they prove to be of clinical value in larger future studies.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CGA received research funding or consultation fees from NARSAD, APF and Genentech.
SJM received research funding or salary support over the last 3 years from the Banner Family Fund, NARSAD, The Brown Foundation, Inc., Bristol-Myers Squibb (BMS), US Department of Veterans Affairs, Evotec, Johnson and Johnson, and the National Institute of Mental Health (NIMH). He received consulting fees or honoraria from: Allergan, AstraZeneca, Cephalon, Corcept, Noven, Roche and Takeda. He received a medication from Sanofi-Aventis for a NIMH-sponsored study. SJM is named as an inventor on a use-patent of ketamine for the treatment of depression. SJM has relinquished his claim to any royalties and will not benefit financially, if ketamine is approved for this use.
JDC received grant support from NIMH, New York State Stem Cell Science (NYSTEM), GlaxoSmithKline (GSK), Pfizer and Alexza Pharmaceuticals. He is on the Pfizer advisory board and gives talks for BMS, AstraZeneca, GSK, and Pfizer.
Authors RS, AJ, PB and JRS declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The funding sources had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; nor in the decision to submit the paper for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Clinical Neuroscience Division of the Veteran’s Administration (VA) National Center for PTSD (grant numbers K23 MH-101498, R01 MH-081870), American Psychiatric Foundation (APF Early Academic Career Award (for CGA)), The Brain and Behavior Research Foundation (NARSAD Independent Investigator and NARSAD New Investigator Awards), The Brown Foundation and the Michael E Debakey VA Medical Center (resources and facilities for SJM).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.