
Abstract
Background:
Drug dependence is frequent in patients with attention deficit hyperactivity disorder (ADHD). Nevertheless, the efficacy and safety of pharmacological treatments in this population are unclear.
Methods:
A systematic review with meta-analysis was performed. Randomised placebo-controlled clinical trials investigating the efficacy of pharmacological treatment in patients with co-occurring ADHD and substance use disorder (SUD) were included. ADHD symptom severity, drug abstinence and all-cause treatment discontinuation were the primary study endpoints. The effects of patient-, intervention- and study-related covariates over the primary outcomes were investigated by means of meta-regression.
Results:
Thirteen studies were included, enrolling a total of 1,271 patients. A small to moderate reduction of ADHD symptoms was found. Meta-regression analysis identified the presence of a lead-in period as a covariate associated with reduced efficacy. Conversely, no beneficial effect was observed either on drug abstinence or treatment discontinuation. The efficacy on ADHD symptoms was smaller in studies with a lead-in period. A positive correlation between the efficacy for ADHD and that for SUD was found.
Conclusions:
The efficacy of pharmacological interventions for co-occurring ADHD and SUD has been little investigated. Mixed results were obtained: while pharmacological interventions improved ADHD symptoms, no beneficial effect on drug abstinence or on treatment discontinuation was noted. The strength of the recommendation of pharmacological treatment for co-occurring ADHD and SUD is therefore modest. The study was registered with the international prospective register of systematic reviews (PROSPERO): CRD 4212003414.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a chronic childhood-onset disorder that persists into adulthood with an estimated prevalence of 2–5% (Fayyad et al., 2007; Kessler et al., 2006; Simon et al., 2009). ADHD is considered a risk factor for the development of substance use disorders (SUDs) (Charach et al., 2011; Lee et al., 2011). Between 17–45% of ADHD patients have alcohol abuse or dependence and up to 30% have drug abuse or dependence (Wilens, 2004). The prevalence of ADHD in adolescents and adults with SUD has been estimated to be 23% (Van Emmerik-van Oortmerssen et al., 2012). Furthermore, ADHD may adversely affect the outcome of SUD. Individuals with both disorders are more frequently polydrug users and have an earlier onset of SUD, more intense drug craving, greater severity of substance use, and worse response to various addiction treatments than patients without ADHD (Kaye and Darke, 2012; Perez de los Cobos et al., 2012; Upadhyaya, 2007).
Two hypotheses that link ADHD with the subsequent development of SUD have been proposed. Firstly, ADHD patients may use drugs in order to alleviate symptoms associated with the disorder such as restlessness, inattention and impulsivity (Khantzian, 1985; Wilens et al., 2007). This is the so-called ‘self-medication hypothesis’. Secondly, ADHD patients may be more prone to drug use due to the impulsivity that is a typical feature of the disorder (Urcelay and Dalley, 2012). If there is a causal relationship between ADHD and SUD, treating the former could lead to an improvement of SUD outcomes in patients with co-existing ADHD and SUD. Nevertheless, there is some controversy about treating ADHD in patients with SUD because psychostimulants, which constitute the first-line pharmacological treatment for ADHD, have abuse potential (Wilens et al., 2008a). Furthermore, psychostimulants could also act as triggers and increase the use of the abused drug (Kaye and Darke, 2012). Safety concerns have also been raised, since therapeutic doses of methylphenidate and, perhaps, other psychostimulants drugs used to treat ADHD may increase the cardiovascular effects of abused drugs like cocaine (Collins et al., 2006).
Evidence of the efficacy of pharmacological treatment of co-occurring ADHD and SUD is inconclusive; some controlled clinical trials studies show a reduction of ADHD symptoms and SUD outcomes, while others show no benefit (Pérez de los Cobos et al., 2012). In the context of a systematic review, meta-analysis and meta-regression can be used to determine whether apparently discrepant results truly are, and, where there is heterogeneity, to identify the potential sources of between-study variability. This information can be useful when tailoring ADHD treatment to a patient’s characteristics.
This study firstly aimed to assess the risk-benefit relationship of pharmacological interventions for ADHD patients with comorbid SUD using ADHD symptom severity, drug abstinence and treatment discontinuation as primary study outcomes. Secondly, we analysed the influence of patient-, intervention- and study design-related covariates over these outcomes. Finally, we also investigated the correlation between the efficacy of the interventions studied upon ADHD symptoms and on SUD outcomes. If ADHD is an independent risk factor of SUD, a positive correlation between ADHD and SUD outcomes could be expected: that is to say, the higher the efficacy on ADHD symptoms the greater the abstinence achieved. To our knowledge, this is the first systematic review with meta-analysis (SRMA) to assess the efficacy and safety of pharmacological interventions for co-occurring ADHD.
Methods and materials
Procedures and study design
An SRMA of randomized controlled clinical trials was carried out. Randomised placebo-controlled clinical trials (RPCCTs) comparing the efficacy of pharmacological interventions for ADHD with placebo in patients with ADHD and comorbid SUD were included. No language restrictions were applied. The following databases were searched (the last search was performed on 11 November 2013): Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, psycINFO, www.clinicaltrialsregister.eu, and www.clinicaltrials.gov (see Supplementary Material, Table 1 for search strategies). Abstracts of potentially relevant studies were inspected and the full articles of those studies deemed suitable were acquired. The reference list of retrieved studies and of relevant review articles (Faraone et al., 2004; Koesters et al., 2009; Perez de los Cobos et al., 2012; Peterson et al., 2008; Schubiner, 2005) and guidelines (Canadian Attention Deficit Hyperactivity Disorder Resource Alliance (CAADRA), 2010; Kleber et al., 2007, Kooij et al., 2010; National Institute for Health and Clinical Excellence (NICE), 2008; Nutt et al., 2007; Pliszka, 2007) were examined to identify any further studies.
Data extraction was performed independently by two investigators (RC, XC). Since the results of RPCCTs are often posted on clinicaltrials.gov, this database was also inspected for non-published information. Where relevant information was not available, study authors were e-mailed and missing information was requested.
The primary study outcomes were: (a) ADHD symptom severity, which included both self- and clinician-rated scores; (b) drug abstinence, including both objective and subjective measures; and (c) all-cause treatment discontinuation, defined as the proportion of randomised patients that did not complete the study for any reason. When change scores, endpoint scores and response rates of the same outcome (e.g. clinician-rated ADHD efficacy using the ADHD rating scale IV) were reported in the same study, we preferred change scores to endpoint ones and the latter to response rates. Secondary outcomes were: (a) proportion of patients who discontinued due to lack of efficacy (LOE); and (b) proportion of patients who discontinued due to adverse events (AEs). Intention to treat data was preferred to per protocol.
The following covariates were collected: gender (% men), age, baseline ADHD severity (expressed as a percentage of scale maximum), type of SUD, type of pharmacological intervention, administration of concomitant psychosocial interventions, treatment duration, recruitment of patients by advertisement, and presence of a lead-in phase.
The risk of bias was ascertained with the Cochrane Collaboration instrument (Higgins and Green, 2011a), which is based on the description and suitability of seven domains, namely: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and other sources of bias. Most domains are assessed at study level, except for blinding and incomplete outcome data, which are assessed at outcome level. This tool involves assigning a judgement relating to the risk of bias for each entry in terms of ‘low’, ‘high’, or ‘unclear’ risk.
Statistical analysis
Effect sizes were calculated as follows: odds ratios (ORs) were calculated for dichotomous outcomes, and standardised mean differences (SMDs) for continuous ones. SMDs were subsequently re-expressed as OR to allow further combination of continuous and dichotomous outcomes (Higgins and Green, 2011b). Elbourne’s recommendations were applied to calculate SMDs and ORs from cross-over studies (Elbourne et al., 2002); when this was not possible only the results of the first period of the study were used (Higgins 2011c). In studies with multiple and correlated comparisons, e.g. a three-group study comparing two different pharmacological interventions against one placebo group, we analysed the two pharmacological interventions separately but, to avoid over-counting the placebo group, the number of patients in this group was divided by two (Higgins and Green, 2011b). Change scores, endpoint scores and response rates were all used, since combining change and endpoint scores has been shown to be valid (Da Costa et al., 2013), as has the combination of continuous and binary data (Higgins and Green, 2011b). Where one study reported multiple outcomes of ADHD symptom severity (e.g. clinician- and self-rated ADHD symptom severity) or of drug abstinence (e.g. self-reported and objective abstinence) we calculated the effect size for each and averaged them, taking into account the correlation coefficient between the two outcomes where available, and assuming r=1 where it was not (Borenstein et al., 2009). This method allows the incorporation of all the information about the efficacy on, for example, drug abstinence available from one study in the same analysis in an accurate manner because it avoids double-counting and overweighting the study.
The study-specific estimates were pooled using both fixed and random effects models (DerSimonian and Laird, 1986) by means of the inverse variance method. Between-study heterogeneity was assessed using Cochran’s Q-test for homogeneity (Cochran, 1954) jointly with the I2 index (Higgins et al., 2003), which establishes the percentage of variation in the combined estimate attributable to between-study heterogeneity. Publication bias was evaluated using the funnel plot along with Begg’s test (Begg and Mazumdar, 1994).
Covariate analyses for the primary outcomes were performed for the following characteristics: gender (% men), age, baseline ADHD severity (expressed as percentage of scale maximum), type of SUD, type of pharmacological intervention, administration of concomitant psychosocial interventions, treatment duration, recruitment of patients by advertisement and presence of a lead-in phase. Specific-stratum ORs for each covariate were calculated and comparison between each subgroup was performed using random-effects meta-regression (Berkey et al., 1995). The relationship between the efficacy of study medication on ADHD symptoms and drug abstinence was investigated by means of a regression analysis.
Sensitivity analyses of the primary outcomes were performed by: (a) excluding those studies for which at least one domain that could affect any primary outcome was rated as having ‘high risk of bias’ by means of the Cochrane instrument; and (b) excluding cross-over studies. Statistical analyses were performed using Stata statistical software (StataCorp, 2011) by using the metan (Harris et al., 2008) and metareg commands (Harbord and Higgins, 2008).
Results
Description of studies
Thirteen studies were included (see Supplementary Material, Figure 1 for flow diagram) (Carpentier et al., 2005; Kollins et al., 2014; Konstenius et al., 2010; Levin et al., 2006, 2007; McRae-Clark et al., 2010; Riggs et al., 2004, 2011; Schubiner et al., 2002; Szobot et al., 2008; Thurstone et al., 2010; Wilens et al., 2008b; Winhusen et al., 2010), which enrolled 1271 patients (see Supplementary Material, Table 2 for a description of the studies’ characteristics). One study provided two drugs (methylphenidate and bupropion) vs placebo comparisons (Levin et al., 2006). Patients had a mean age of 28.9 years, most were men (74%) and had combined-type ADHD (69.5%). ADHD diagnosis was performed using the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association, 1994) or 4th edition, text revision (DSM-IV-TR) (American Psychiatric Association, 2000) diagnostic criteria in all of the studies (one did not refer the criteria used) and five of them required a minimum symptom severity (Levin et al., 2006, 2007; Thurstone et al., 2010; Wilens et al., 2008b; Winhusen et al., 2010). SUD diagnosis was performed using DSM-IV/DSM-IV TR criteria in 10 studies, DSM-IIIR (American Psychiatric Association, 1987) criteria in one (Riggs et al., 2004) and two did not specify which diagnostic criteria were applied (Kollins et al., 2014; Winhusen et al., 2010). The comorbid SUDs investigated were nicotine dependence (Kollins et al., 2014; Winhusen et al., 2010), cocaine dependence (Levin et al., 2007; Schubiner et al., 2002), alcohol abuse/dependence (Wilens et al., 2008b), opiate dependence (Levin, 2006), cannabis dependence (McRae-Clark et al., 2010), amphetamine dependence (Konstenius et al., 2010) and four studies enrolled patients with any SUD other than nicotine dependence (Carpentier et al., 2005; Riggs et al., 2004, 2011; Szobot et al., 2008; Thurstone et al., 2010). Three studies required patients to be abstinent to be included (Carpentier et al., 2005; Konstenius et al., 2010; Wilens et al., 2008b).
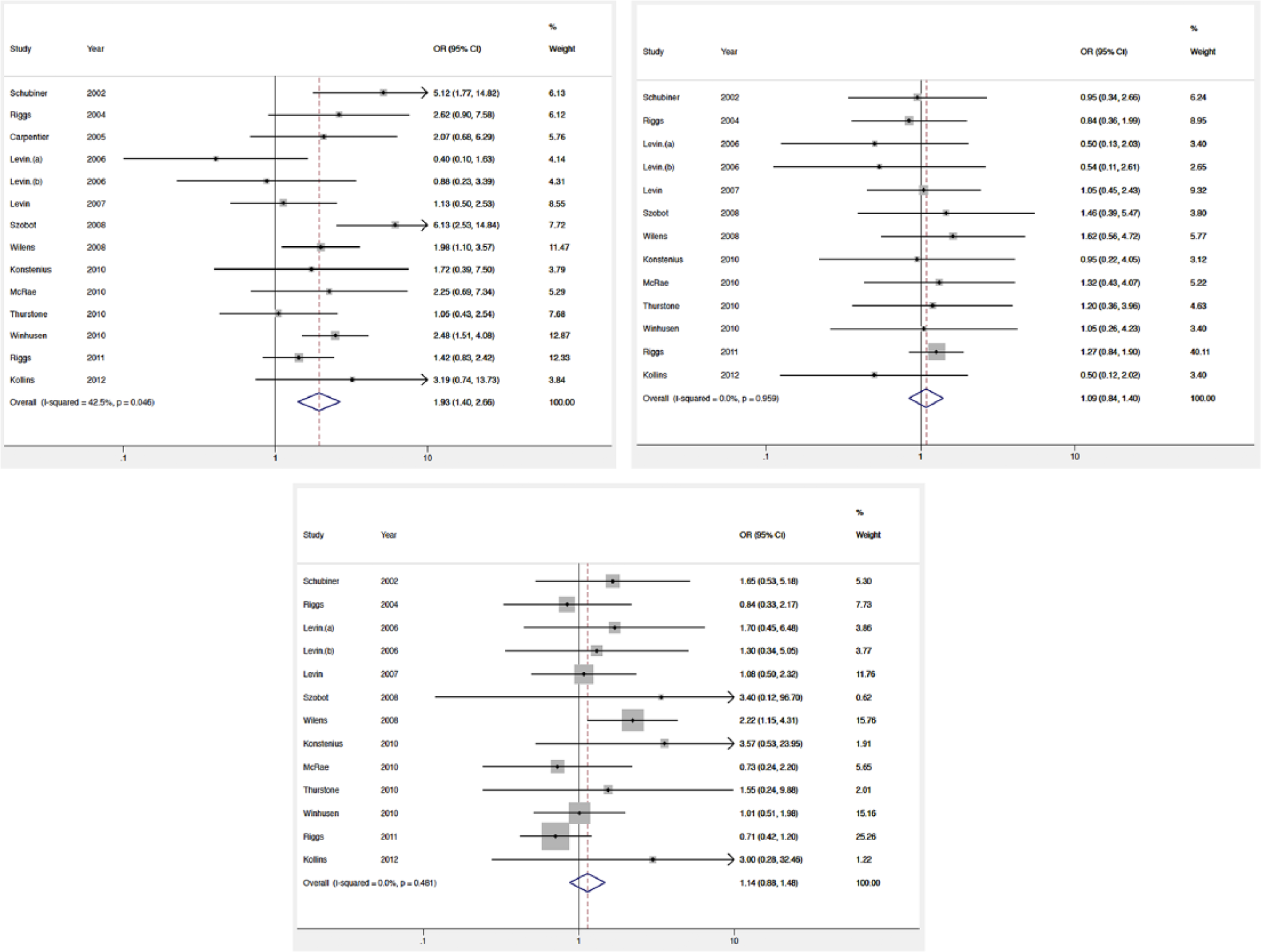
Forest plots of the comparison of pharmacological interventions vs placebo for the primary outcomes: efficacy on attention deficit hyperactivity disorder (ADHD) symptom severity (top-left), efficacy on global drug abstinence (top-right) and all-cause treatment discontinuation (bottom). CI: confidence interval; OR: odds ratio.
Five pharmacological interventions were investigated: methylphenidate (eight studies, 875 patients, mean dose=62.2 mg/d) (Konstenius et al., 2010; Levin et al., 2006, 2007; Riggs et al., 2011; Schubiner et al., 2002; Szobot et al., 2008; Winhusen et al., 2010), atomoxetine (three studies, 295 patients, mean dose=89.5 mg/d) (McRae-Clark 2010, Thurstone et al., 2010, Wilens et al., 2008b), pemoline (one study, 69 patients, mean dose=105.2 mg/d) (Riggs et al., 2004), bupropion (one study, 98 patients, study dose=200-400 mg/d) (Levin et al., 2006), and lisdexamphetamine (one study, 32 patients, study dose=up to 70 mg/d) (Kollins et al., 2014). The average treatment duration was 12.2 weeks, ranging from 3–16 weeks. Additional psychotherapy was reported to have been provided in eight studies, with cognitive behaviour therapy (CBT) being the most widely used approach. Psychotherapy addressed SUD in six studies (Levin et al., 2006, 2007; McRae-Clark et al., 2010; Riggs et al., 2011; Thurstone et al., 2010; Winhusen et al., 2010) and both SUD and ADHD in two (Konstenius et al., 2010; Schubiner et al., 2002). Only three studies permitted specific pharmacological treatment for SUD during the double blind phase of the study (Kollins et al., 2014; Levin et al., 2006; Winhusen et al., 2010).
All studies but two (Carpentier et al., 2005; Szobot et al., 2008) had a parallel-group design. Two studies used a pre-randomization placebo lead-in phase (Levin et al., 2006, 2007). All studies but three were carried out in the USA, one of them with additional participation from Canada (Wilens et al., 2008b). The other studies took place in Sweden (Konstenius et al., 2010), the Netherlands (Carpentier et al., 2005) and Brazil (Szobot et al., 2008). All studies were publicly funded except one (Kollins et al., 2014) which was sponsored by a pharmaceutical company (Kollins et al., 2014). Another study received additional pharmaceutical economic support (Wilens et al., 2008b).
No study was considered free of bias in all domains of the Cochrane tool (Supplementary Material, Figure 2), mainly because the treatment discontinuation rate was rather high, yielding the possibility of attrition bias for most study outcomes except for ‘all-cause treatment discontinuation’, which is not affected by this bias. Additionally, the possibility of performance and detection bias was judged to be likely since the interventions investigated have been associated with behavioural effects (Heil et al., 2002; Jasinski et al., 2008) that may yield to blinding failure and, hence, to revealing the assigned intervention. The exception was ‘objective drug abstinence’, which we deemed unlikely to be affected by detection bias due to its objective nature. Two studies (Schubiner et al., 2002; Thurstone et al., 2010) scored ‘high risk of bias’ in the so-called ‘other biases’ domain: one because patients’ characteristics were unbalanced at baseline (Thurstone et al., 2010), and the other because one study group was removed when the clinical trial was already on-going (Schubiner et al., 2002). Studies with high risk of bias were withdrawn in one sensitivity analysis.
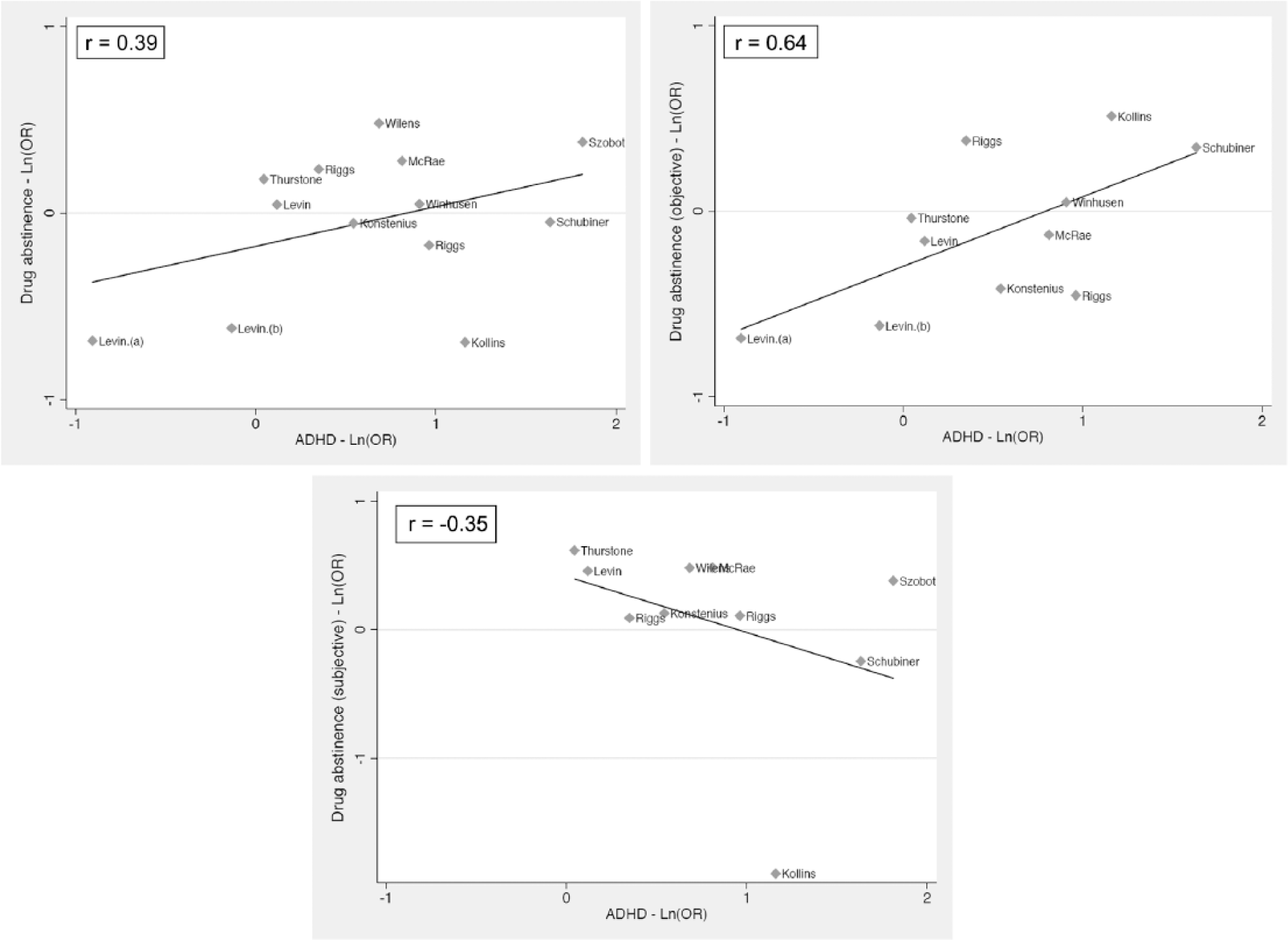
Correlation between the efficacy of pharmacological interventions on attention deficit hyperactivity disorder (ADHD) symptom severity and efficacy on global drug abstinence (top-left), objective drug abstinence (top-right), subjective drug abstinence (bottom). OR: odds ratio.
Efficacy, safety and treatment discontinuation
Figure 1 shows the effect of the interventions studied on ADHD symptoms, drug abstinence and all-cause treatment discontinuation. Pharmacological treatment reduced ADHD symptoms in dual patients compared with placebo. The pooled OR was 1.93 and statistical heterogeneity was moderate (I2=42.5%). This result was similar irrespective of whether the rater was the patient (OR=1.98) or the clinician (OR=1.62) (Supplementary Material, Figure 3). The results, stratified by type of medication and type of SUD, are shown in Supplementary Material, Table 3. Atomoxetine and methylphenidate were efficacious for reducing ADHD symptoms. In contrast, not one of bupropion, lisdexamfetamine, and pemoline were different from placebo at a statistically significant level. Regarding the type of drug dependence, pharmacological treatment was efficacious in reducing ADHD symptoms in alcohol and nicotine dependent patients as well as in those classified as ‘unspecific’, but no differences were found in patients with comorbid psychostimulant or opiate dependence.
No pharmacological intervention was efficacious in improving drug abstinence (OR=1.09), (Figure 1) whether stratifying the analysis for pharmacological interventions, or for SUD type (Supplementary Material, Table 3). These results were consistent between objective and subjective drug abstinence (OR=1.08 and 1.23, respectively) (Supplementary Material, Figure 4).
The number of patients that dropped out due to lack of efficacy was only available in four studies, which reported two patients dropping out for this reason with the active intervention and none with placebo (OR=5.35, p=0.28). Twenty-two patients discontinued due to AEs and no statistically significant differences were found between groups (OR=1.19, p=0.58). Similarly, no differences were observed in all-cause treatment discontinuation (OR=1.14) (Figure 1). These results were consistent across interventions studied and type of SUD (Supplementary Material, Table 3).
Covariate and regression analyses
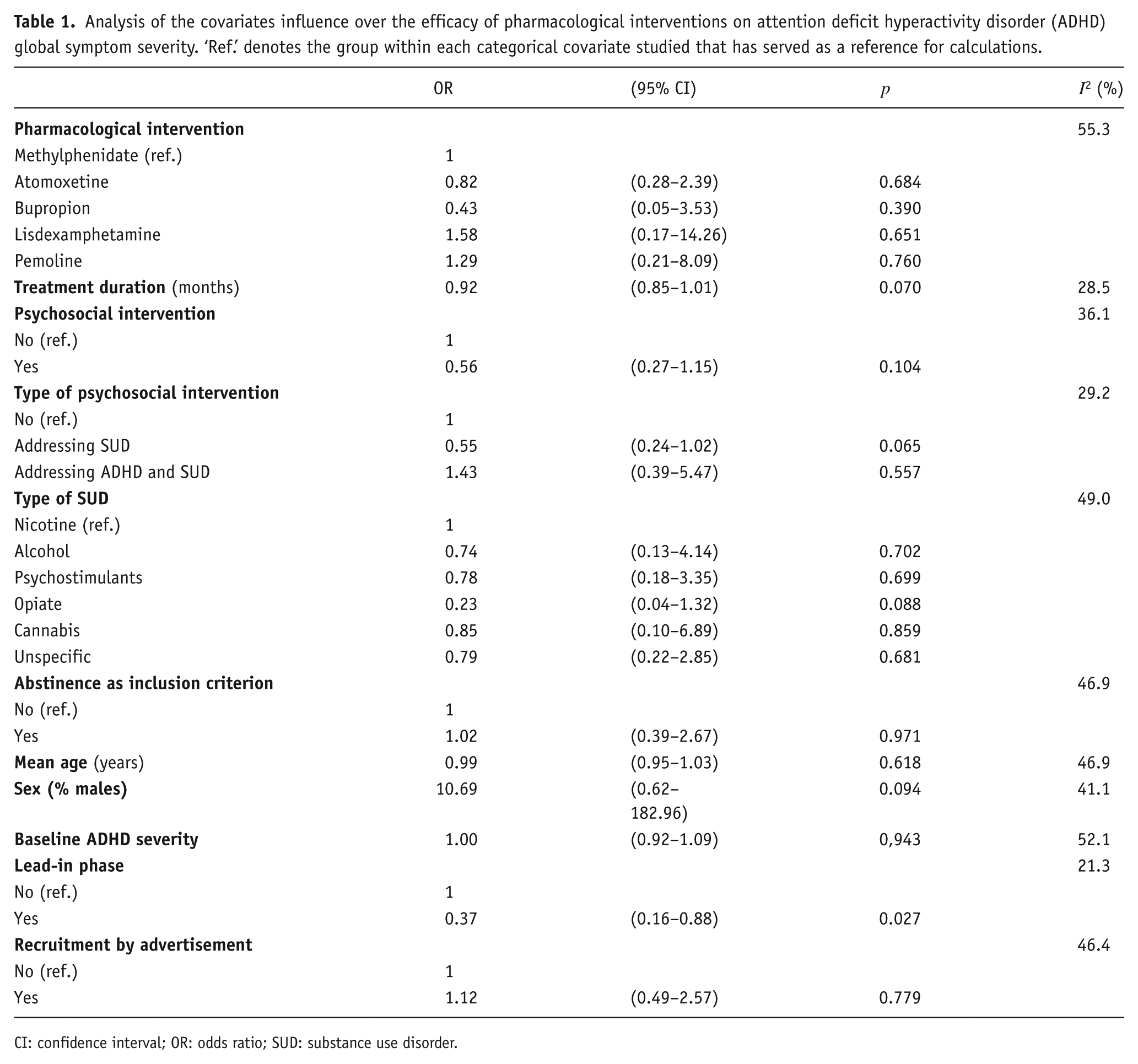
Sources of heterogeneity were investigated only for ADHD symptom severity, because for SUD outcomes and treatment discontinuation no statistical heterogeneity was observed. Table 1 shows the effect of patient-, intervention- and study design-related covariates. This analysis showed that RPCCTs with a placebo lead-in period had lower efficacy than those without. This covariate accounted for a large amount of the total statistical heterogeneity. A post hoc analysis excluding the two studies with a lead-in period resulted in an OR for ADHD efficacy of 2.26 (p<0.00001) with no statistically significant heterogeneity (I2=27%, p=0.17). No other covariate was found to modify the effect of the studied interventions on ADHD symptoms.
Analysis of the covariates influence over the efficacy of pharmacological interventions on attention deficit hyperactivity disorder (ADHD) global symptom severity. ‘Ref.’ denotes the group within each categorical covariate studied that has served as a reference for calculations.
CI: confidence interval; OR: odds ratio; SUD: substance use disorder.
The regression analysis between the improvement of ADHD and that of objective drug abstinence showed a high positive relationship (r=0.64), while it was low between ADHD efficacy and both global drug abstinence and subjective drug abstinence (Figure 2).
Sensitivity and publication bias analyses
Supplementary Material, Table 4 shows the results of sensitivity analyses. No relevant effect on any primary outcome was identified after excluding either cross-over trials or studies with high risk of bias from the analysis.
No evidence of publication bias was found, as shown by funnel plots and Berg tests (Supplementary Material, Figure 5).
Discussion
This is the first SRMA of RPCCTs that has assessed the efficacy and safety of pharmacological treatment of patients with dual ADHD. Despite SUD being a well-recognised common comorbid disorder in patients with ADHD (Wilens, 2004), and being associated with numerous negative consequences, the efficacy of pharmacological interventions has been infrequently investigated in this population. Furthermore, we found that in these patients pharmacological interventions primarily targeting ADHD symptoms showed mixed results. While ADHD symptoms improved compared to placebo, no benefit was observed on substance use outcomes nor on all-cause treatment discontinuation.
Pharmacological treatment reduced ADHD symptom severity in patients with concurrent ADHD and SUD and only modest statistical heterogeneity was found. The effect size was small, as shown by an OR=1.93, which roughly corresponds to a SMD=0.30 (Higgins and Green, 2011b). This effect size is smaller than that observed in other studies in which SUD was not an inclusion criterion (Castells et al., 2011, 2013; Cunill et al., 2013; Koesters et al., 2009). Nevertheless, it is likely that the effect size is slightly larger because ADHD symptoms may overlap with those of SUD, hampering both ADHD diagnosis and the assessment of the change in its severity (Dakwar et al., 2012). Covariate analysis identified one clinical trial design characteristic – the presence of a placebo lead-in period before randomization – to be associated with a lower effect size. Two studies (Levin et al., 2006, 2007) included a placebo lead-in period. Only those patients that completed this period were randomised. It is likely that this procedure selected the most motivated patients, which may explain why the placebo response in these studies was large (Levin et al., 2006, 2007). Therefore, any room for further improvement was slight, as was the effect of the interventions investigated in these studies. The exclusion of these studies yielded a slightly larger effect size (OR=2.26), which corresponds to an SMD of 0.45 with no statistically significant heterogeneity. This effect size is modest and falls between those of two approved medications for adult ADHD, methylphenidate and atomoxetine (Castells et al., 2013; Cunill et al., 2013). It must be noted that the effect of a placebo lead-in is likely to be the opposite of the one seen in this study when the lead-in period is intended to exclude patients who improve with placebo. Doing so is expected to yield a small placebo-response during the double-blind phase and, thus, a higher effect size.
Two key points in the management of substance-abusing ADHD patients are the type of pharmacological treatment and the timing of its initiation in relation to detoxification or other interventions to reduce substance use. This study found no differences between the interventions examined. Regarding the best time to begin pharmacological treatment, arguments for and against immediate pharmacological treatment of ADHD have been proposed, but no consensus exists (Kleber et al., 2007; Mariani and Levin 2007; Nutt et al., 2007; Perez de los Cobos et al., 2012). We found that the efficacy of pharmacological treatment for ADHD did not differ between RPCCTs for which drug abstinence was an inclusion criterion and those for which it was not. Decisions about the type of pharmacological intervention to be made and the time to begin treatment should, therefore, be based on safety rather than efficacy. For instance, a number of hazardous pharmacokinetic and pharmacodynamics interactions between drugs of abuse and medications to treat ADHD have been described (Collins et al., 2006, Delavenne et al., 2013, Patrick et al., 2007, Tirado et al., 2008). For safety reasons, it may be, therefore, advisable to delay the initiation of pharmacological treatment for ADHD until abstinence is achieved.
Inasmuch as ADHD is associated with SUD – possibly due to the impulsivity that is a feature of ADHD, or because patients ‘self-medicate’ with drugs – it was expected that alleviating ADHD symptoms in patients with coexisting ADHD and SUD would lead to drug use reduction. Nevertheless, we found that pharmacological treatment, despite reducing ADHD symptom severity, did not improve SUD outcomes. This finding showed no statistical heterogeneity and this was consistent across all the analyses performed. These results may be added to recently published studies showing that pharmacological treatment of ADHD patients does not protect them from the development of future SUD (Humphreys et al., 2013; Molina et al., 2013). While pharmacological treatment did not increase drug abstinence, we found that the efficacy over ADHD was positively correlated with drug abstinence in some analyses, suggesting that the larger the efficacy for ADHD, the greater the drug abstinence. Together, these findings may indicate that the treatment of ADHD in patients with comorbid SUD could have a positive effect on drug abstinence if the effect size on ADHD symptoms was larger. In patients with major depressive disorder and comorbid SUD it was found that antidepressant treatment achieved drug use reduction when the effect size on depressive symptoms was above an SMD of 0.5, this is when the antidepressant efficacy was modest to high (Nunes and Levin, 2004). Nevertheless, this interpretation is rather speculative and should be confirmed in the future.
Few patients dropped out due to AEs. This contrasts with previous studies showing a higher rate of AE-induced treatment discontinuation in patients receiving pharmacological treatment for ADHD (Castells et al., 2013; Cunill et al., 2013). This lower AE-induced dropout rate could be a consequence of the fact that the study population consisted of drug-dependent patients who may be accustomed to certain drug-induced behavioural AEs such as drowsiness or insomnia, which are common causes of treatment discontinuation in non-dual ADHD patients. Overall, no differences were found in all-cause treatment discontinuation. This is consistent with the findings that pharmacological treatment had modest efficacy and that it was well tolerated.
Study limitations include those of the RPCCTs included along with those typical of a SRMA. Biased RPCCTs lead to a biased SRMA. No study was found free of bias and some of them scored high for risk of bias. It seems that these studies did not unduly influence our findings because their exclusion from the main analyses yielded similar results. Publication bias must also be borne in mind. However, this bias appears unlikely in this study, as shown by the fact that Begg’s test provided no evidence of small study effects. Besides this, the funnel plots were symmetrical. It must be stressed that the external validity of this study may be compromised by the short study duration of most RPCCTs included. Unlike meta-analysis, co-variable analysis provides indirect evidence with a high risk of selection bias. Furthermore, no adjustment for multiple comparisons was made, and the risk of false positive associations must be taken into account. Furthermore, the possibility that some study co-variables confound each other cannot be ruled out. Confounding could be controlled by means of multi-variable meta-regression. Nevertheless, this type of analysis could not be performed due to the small number of RPCCT that exist. Finally, the precision of the effects calculated is limited by the reduced number of RPCCT, most of which had a small sample size. This limitation is particularly relevant in the subgroup and meta-regression analyses because some categories included a low number of studies; therefore, the statistical power of these analyses is small.
Conclusions
This study found mixed results of the efficacy of pharmacological treatment for patients with ADHD and comorbid drug dependence. While small to moderate reduction of ADHD symptoms was achieved, no improvement in drug abstinence or treatment discontinuation was found. A moderate reduction of attention and hyperactivity/impulsivity that is not accompanied with an increase of drug abstinence in patients with ADHD and comorbid SUD is of limited clinical interest. This, along with the fact that few short-term RPCCTs have been carried out, provides modest evidence to support pharmacological treatment in patients with ADHD and comorbid drug dependence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.