
Abstract
Clinical observations indicate no cataractogenic potential for quetiapine, in contrast to studies in laboratory animals. This randomized, non-inferiority study compared changes in lens opacity during long-term treatment with quetiapine versus risperidone. Patients with schizophrenia or schizoaffective disorder participated in the 2-year, randomized, multicentre, open-label, ophthalmologist-masked, flexible-dose, parallel-group study. Two ophthalmologists examined each patient 6-monthly for presence of nuclear opalescence (N) and cortical (C) or posterior subcapsular opacification (P), according to the lens opacities classification system II. 1098 patients were randomized to treatment. Mean doses were 386.3 mg/day quetiapine and 3.2 mg/day risperidone. Estimated absolute risk differences in cataractogenic events for quetiapine versus risperidone over 2 years were −0.035 (C), −0.012 (N) and −0.017 (P), with upper margins of confidence intervals within the non-inferiority margin of 10%. In post hoc analysis, risk of any lens opacification event was significantly lower for quetiapine than risperidone (6 and 16 events, respectively; risk difference: −0.058; P = 0.035). Efficacy and other safety assessments were in agreement with known profiles of these medications. Quetiapine was non-inferior to risperidone for changes in lens opacity grade in patients with schizophrenia or schizoaffective disorder, indicating that quetiapine does not have clinically significant cataractogenic potential during long-term treatment.
Introduction
Patients with schizophrenia are at elevated risk of developing cataract when compared with the general population (McCarty et al., 1999; Smith et al., 1997). Risk factors for the development of cataract include poor general health, smoking, alcoholism, a high-fat diet, and comorbidities such as diabetes and hypertension. These diseases and environmental and behavioural factors are common in patients with schizophrenia (Sartorius, 2007). Selected antipsychotic medications used in the treatment of schizophrenia, such as chlorpromazine, thioridazine, molindone and carbamazepine, have also been associated with increased risk of cataract (Greiner and Berry, 1964; McCarty et al., 1999; Richa and Yazbek, 2010; Ruigómez et al., 2000; Siddall, 1965; Siddall, 1968). While the pathophysiology of lens opacification in such cases is complex and poorly understood, the risk of cataract consistently increases with the dose and duration of pharmacologic treatment (Barsa et al., 1965; Forrest et al., 1966; Garner et al., 1974; Satanove, 1965; Siddall, 1965).
Atypical antipsychotics were developed with the aim of providing efficacy in the reduction of psychotic symptoms, while reducing the incidence and severity of adverse effects, such as extrapyramidal disorders, associated with phenothiazine derivatives in the treatment of schizophrenia and other psychiatric disorders (Friedman, 2004). Preclinical and clinical evidence on the cataractogenic potential of atypical antipsychotics is relatively limited (Ruigómez et al., 2000; Shahzad et al., 2002; Souza et al., 2008; Ucok and Gaebel, 2008).
Preclinical investigations of quetiapine identified an increased risk of cataract in beagle dogs following exposure for 6–12 months at a dose of 100 mg/kg (i.e. four times the recommended human dose). Cataracts have not been associated with quetiapine exposure in other species. However, a striated appearance of the anterior lens surface was noted in two of seven non-human primates exposed to quetiapine for 1 year at a dose of 225 mg/kg (i.e. 5.5 times the recommended maximum human dose) (AstraZeneca Pharmaceuticals, 2013).
The clinical development program for quetiapine has identified no consistent pattern of lens changes. A survey of 620,000 patients exposed to quetiapine for 32 months reported 34 patients with lens opacities, most of whom had established risk factors for lens opacity, including exposure to other medications, ocular trauma, hypertension and diabetes (Laties et al., 2000). The authors concluded that cataractogenesis secondary to quetiapine was unlikely based on the lens changes observed. Furthermore, there was no relationship between quetiapine dose or treatment duration and development of lens opacities observed in the study. An independent review of 34 case reports of cataract in patients treated with standard-dose quetiapine for a mean of 9 months reached a similar conclusion that cataractogenesis secondary to quetiapine was unlikely (Fraunfelder, 2004).
As the possibility cannot be excluded from current evidence that lenticular changes may occur during long-term treatment with quetiapine, the current prescribing information for quetiapine recommends lens examination for cataract formation at the initiation of treatment and at 6-month intervals (AstraZeneca Pharmaceuticals, 2013).
This 2-year, open-label study in patients with schizophrenia or schizoaffective disorder was designed with input from the US Food and Drug Administration (US FDA) to evaluate the cataractogenic potential of quetiapine with the lens opacities classification system II (LOCS II). The study used a non-inferiority design in which risperidone was selected as the comparator because of the absence of evidence that this atypical antipsychotic has cataractogenic potential (Shahzad et al., 2002). Secondary objectives for the study included a comparison of the efficacy, safety and quality of life effects of quetiapine and risperidone in the treatment of these patients.
Methods
Study design
The primary objective of this study was to determine the relative cataractogenic potential of quetiapine versus risperidone based on eye examinations performed every 6 months. This 2-year, randomized, multicentre, open-label, ophthalmologist-masked, flexible-dose, parallel-group study recruited outpatients with schizophrenia or schizoaffective disorder from 82 centres in the United States between September 2003 and October 2008 (Study 5077IL/0089; ClinicalTrials.gov Identifier: NCT00206102).
After a screening period of up to 30 days, patients were randomly assigned to treatment with quetiapine or risperidone and followed with LOCS II. An overview of the study design is included in Figure 1.
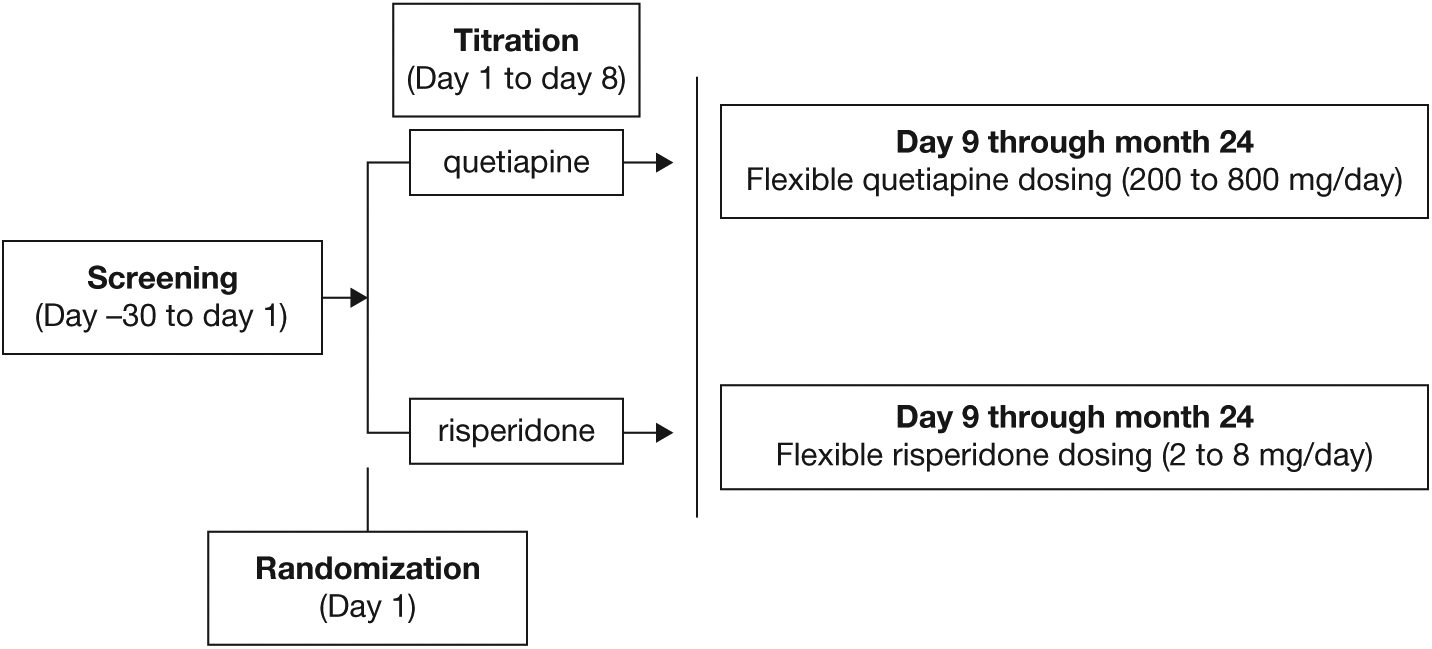
Study design.
Patients
Men or women aged 18–65 years with a diagnosis of schizophrenia (catatonic, disorganized, paranoid, undifferentiated or residual) or schizoaffective disorder, based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV), were eligible for inclusion (American Psychiatric Association, 1994).
Exclusion criteria included a history of, or clinical evidence of, narrow-angle glaucoma or eye disease potentially requiring treatment during the study; previous history of intraocular surgery; or a baseline lens rating of >0 for posterior subcapsular opacification, >1 for cortical opacification or >2 for nuclear opalescence. Additional exclusion criteria included more than three hospitalizations for psychiatric illness in the previous 12 months; evidence of previous noncompliance with medication; history of substance use or abuse; clinically significant deviations in laboratory test results; and a history of known non-responsiveness or intolerance to quetiapine or risperidone. Patients who received continuous systemic steroids for >3 months or had a medical illness likely to require corticosteroid treatment, patients with unstable or inadequately treated diabetes mellitus, and those with clinically significant electrocardiogram results were also excluded.
The study was performed in accordance with the ethical principles of the Declaration of Helsinki and was consistent with the International Conference on Harmonization (ICH)/Good Clinical Practice (GCP) (http://www.ich.org/; http://www.fda.gov/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacco/OfficeofScienceandHealthCoordination/ucm2018191.htm). The study protocol was approved by the institutional review board for each study site. All patients provided written, informed consent before study entry. Patients could withdraw from the study at any time by their own choice or at the discretion of the investigator. Patients who experienced a cataractogenic event, as determined by an ophthalmologist, were withdrawn. An independent Data and Safety Monitoring Board, including three ophthalmologists with an interest in cataractogenesis, reviewed data during the study for unusual or unexpected trends in the number or type of events that may have required study termination.
Use of concomitant medications or drugs known to cause cataracts, such as psoralens and allopurinol, was prohibited during the study. Treatments that were considered necessary for the patient’s safety and well-being, including antidepressants or mood stabilizers, were administered at the investigator’s discretion.
Doses and treatment regimens
Patients were randomly assigned to receive oral, flexibly-dosed quetiapine or risperidone (in immediate-release formulations) based on a central stratified randomization schedule, with stratification of groups by age at entry (<40 years and ≥40 years) and by previous exposure to study treatments (i.e. previous exposure to quetiapine only, risperidone only, neither medication, or both). Each eligible patient was assigned a randomization number based within a stratum based on the central randomization schedule. The randomization schedule was prepared by the Quantitative Decision Science Group of AstraZeneca. In a protocol amendment made after 800 patients had been enrolled, randomization to study treatments was changed from an initial ratio of 1:1 to 2:1 in favour of quetiapine due to a higher early withdrawal rate in the quetiapine group. This amendment ensured a balance of approximately 170 patients per treatment arm at 2-year evaluation.
The doses of quetiapine and risperidone administered during the study were in accordance with current prescribing information for schizophrenia. Patients who entered the study while receiving quetiapine or risperidone, and who were randomized to the same medication during study, were allowed to continue at the same dose, unless the quetiapine dose was less than 600 mg/day or the risperidone dose was less than 4 mg/day previously. For other patients randomized to quetiapine, the dose was increased from 50 mg on Day 1, 100 mg on Day 2, 200 mg on Day 3, 300 mg on Day 4, 400 mg on Days 5 through 7, to 600 mg on Day 8; thereafter, the dose was adjusted for efficacy and tolerability within the range of 200–800 mg/day. For other patients randomized to risperidone, the dose was increased from 2 mg on Days 1 through 5, 3 mg on Days 6 and 7, to 4 mg on Day 8; thereafter, the dose was adjusted within the range of 2–8 mg/day. Study drugs were administered twice daily during dose escalation. From Day 8 onward, quetiapine could be administered two or three times daily and risperidone once or twice daily. Quetiapine or risperidone treatment was planned to be continued for a minimum of 21 months or until an increase in lens opacity was identified.
Assessments
Eye assessments using slit lamp examination were performed at baseline and every 6 months by two masked ophthalmologists, working independently, for the presence of nuclear opalescence (N) and cortical (C) or posterior subcapsular opacification (P), according to LOCS II (Chylack, Jr. et al., 1989). Assessments were provided by two ophthalmologists to increase the robustness of the LOCS II analyses. Any disagreement between the ophthalmologists in LOCS II assessment required a repeat eye assessment. Only ophthalmologist agreements at either the first or second assessment were included in the primary analysis. LOCS II is a validated technique for assessment of cataract incidence and cataractogenic potential (Chylack, Jr. et al., 1993; Leske et al., 1997a; Leske et al., 1997b; Magno et al., 1993; The Italian-American Cataract Study Group, 1994). Initially Dr Chylack or a designated colleague provided certification in the use of LOCS II scale to the study investigators; this was later replaced by web-based training and testing.
The efficacy evaluations included Positive and Negative Syndrome Scale (PANSS) and Clinical Global Impression-Severity of Illness and Global Improvement (CGI-S and CGI-I) scores (Guy and Bonato, 1970; Kay et al., 1987). The time to first relapse and the number of relapses of schizophrenia or schizoaffective disorder during the study were also recorded. Relapse was defined as a hospitalization for psychiatric symptoms or an increase in two units on the CGI-S scale. Efficacy evaluations were performed at Day 1 and once monthly (CGI) or every 3 months (PANSS), with final assessment at study end.
Patient-reported outcomes included changes in the Quality of Life Enjoyment and Satisfaction Questionnaire – Short Form (Q-LES-Q SF) and Personal Evaluation of Transitions in Treatment (PETiT) scores (Endicott et al., 1993; Voruganti and Awad, 2002). Patient-reported outcomes were assessed at Day 1 and every 3 months until study end.
Safety evaluations included the incidence, severity and causality of adverse events (AEs) and withdrawals due to AEs, as recorded by the investigator. Changes in weight, clinical laboratory assessments, vital signs and physical evaluations were also recorded. Treatment-emergent metabolic risk factors were defined as changes in body mass index (shift to ≥30 kg/m2), blood pressure (shift to ≥130 mmHg systolic or ≥85 mmHg diastolic), triglycerides (shift to ≥1.7 mmol/L), high-density lipoprotein cholesterol (shift to <1.04 mmol/L in men, <1.3 mmol/L in women), and fasting glucose (shift to ≥5.56 mmol/L). AEs, weight and vital signs were reported at screening, Days 1, 7, 14 and 30, and then monthly until study end. Laboratory assessments were performed at screening and every 3 months until study end.
Extrapyramidal symptom-related scales for assessment of movement disorders included the Simpson-Angus Scale (SAS), Barnes Akathisia Rating Scale (BARS; including Global Assessment of Akathisia), Abnormal Involuntary Movement Scale (AIMS), and the seven-item AIMS (AIMS-7) (Barnes, 1989; Guy, 1976; Simpson and Angus, 1970). Extrapyramidal symptom-related scale assessments were performed at Day 1 and every 3 months until study end.
Compliance with study drugs was assessed using returned tablet counts. Patients who took less than 80% of their prescribed drug at two consecutive visits were considered noncompliant.
Statistical analyses
The primary study analysis tested the null hypothesis that the difference in cataractogenic event rate between quetiapine and ris-peridone was ≥10%, in favour of the alternative that the difference was <10% for each event (N, C or P). The Mantel–Haenszel test, which allows comparison of two groups on a categorical response (Mantel and Haenszel, 1959), was performed with 95% confidence intervals (CIs) to evaluate the difference in the proportions of patients with each type of cataractogenic event between the quetiapine and risperidone groups. If none of the three upper 95% CIs for the difference in the proportions of patients exceeded the predefined non-inferiority limit (10%), this indicated that the criterion for non-inferiority was met.
Kaplan–Meier survival analyses were performed for the proportion of patients versus time to a lens opacification event (any of N, C or P) and the time to first relapse of schizophrenia or schizoaffective disorder. A Cox proportional hazards model assessed differences in the time to a cataractogenic event and to first relapse of schizophrenia or schizoaffective disorder for quetiapine versus risperidone. A generalized estimating equation model compared SAS, AIMS and BARS scores between quetiapine and risperidone groups. Other secondary efficacy, safety and tolerability variables were analysed by descriptive statistics.
The primary analysis was performed on the ‘2-year per protocol for eye evaluations’ (E2PP) set, which included all randomized patients who reached the endpoint of either: study drug administered for at least 21 months with no major protocol deviations or an identified increase in lens opacity. Supportive analysis for the primary analysis was performed on the ‘ITT for eye evaluations’ (EITT) set, which included all randomized patients who received at least one dose of study medication and had at least one valid post-baseline LOCS II evaluation. Other analysis sets included the ‘2-year intent-to-treat for eye evaluations’ (E2ITT) set, the ‘intent-to-treat for psychiatric assessments’ (ITTP) set, and the safety analysis set. The safety analysis set included all patients who received at least one dose of study drug, the E2ITT set included patients who received at least one dose of study drug and reached the study endpoint, and the ITTP set included patients who additionally had at least one post-baseline assessment of PANSS score. Assuming 170 evaluable patients per treatment group, the power of the study was estimated to be at least 86%, supposing a conservative event rate of 7% for each of the cataractogenic events.
Results
Patient characteristics
Of 1837 patients enrolled for screening, 1098 were randomized to treatment (n = 596, quetiapine; n = 502, risperidone group). The most common reasons for screen failure were a positive urine drug screen for illicit substances (15.4%), a non-qualifying LOCS II assessment (14.6%), clinically significant deviations from the reference range in laboratory tests (12.6%) and a baseline or screening rating >0 for P, >1 for C or >2 for N (9.1%). Patient flow through the study and the numbers of patients per analysis set are shown in Figure 2.
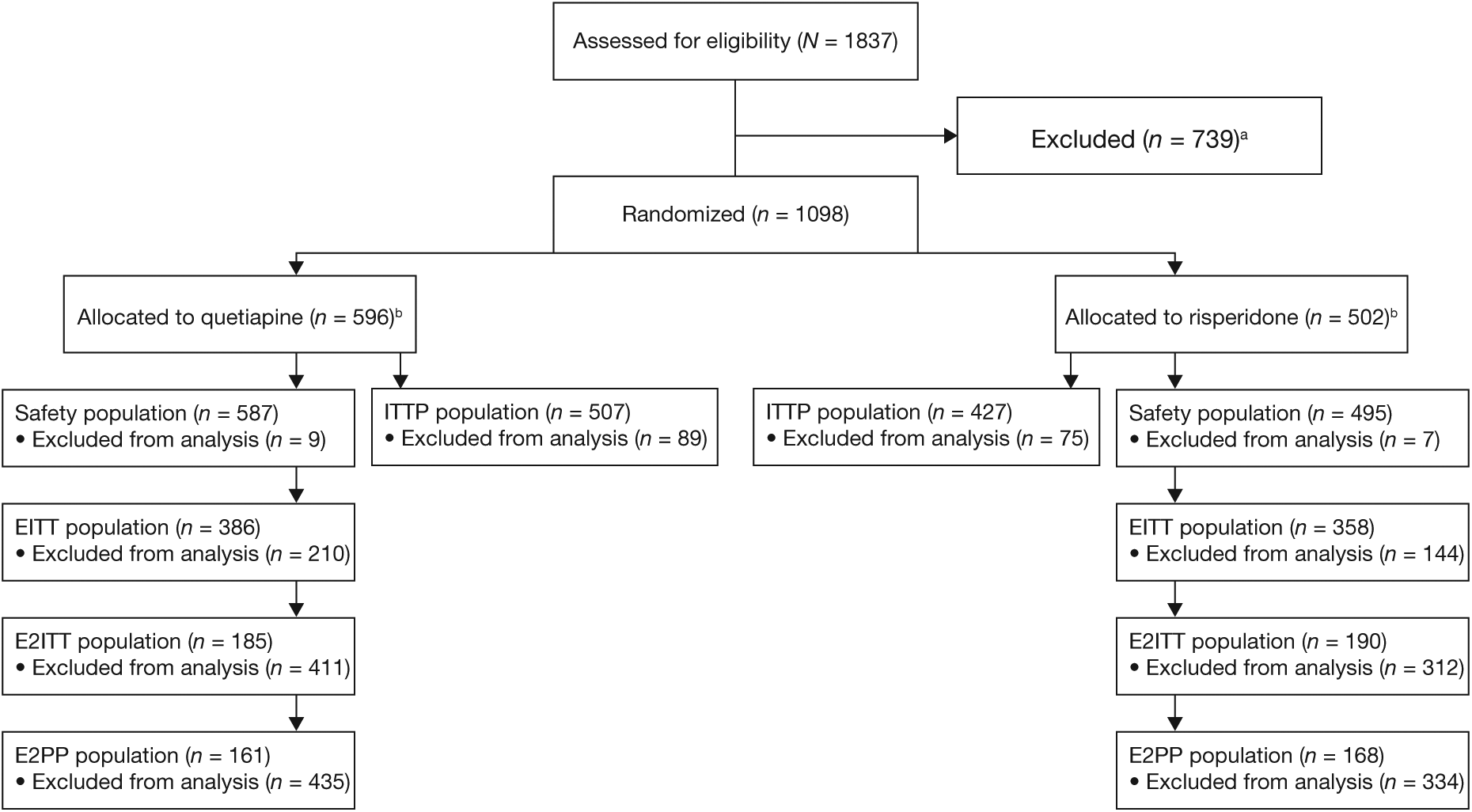
Patient flow during study. aOf the 739 patients who did not qualify, the most common reasons (>5% of patients) for screen failure were positive urine drug screen for illicit substances (15.4%), a qualifying LOCS II assessment (14.6%), clinically significant deviations from the reference range in screening laboratory tests (12.6%), baseline or screening >0 for P, >1 for C or >2 for N by either eye grader (9.1%). bOne patient was randomized to quetiapine but was administered risperidone. This patient’s data were analysed in the safety, EITT, E2ITT and ITTP analysis sets by actual treatment taken. EITT, intent-to-treat for eye evaluations analysis set; E2ITT, 2-year intent-to-treat for eye evaluations analysis set; E2PP, 2-year per protocol eye evaluation analysis set; ITTP, intent-to-treat population for psychiatric assessments.
Baseline characteristics, including psychiatric disease and incidence of cataract risk factors, were balanced between the groups receiving quetiapine or risperidone (Table 1). More than 90% of patients reported taking prior medication at baseline. Risperidone was a prior medication in 32.6% of all randomized subjects who were treated with quetiapine and in 32.9% who were treated with risperidone during the study. Quetiapine was a prior medication in 26.3% of subjects who were treated with quetiapine and in 25.1% who were treated with risperidone.
Patient characteristics at baseline (all randomized patients).
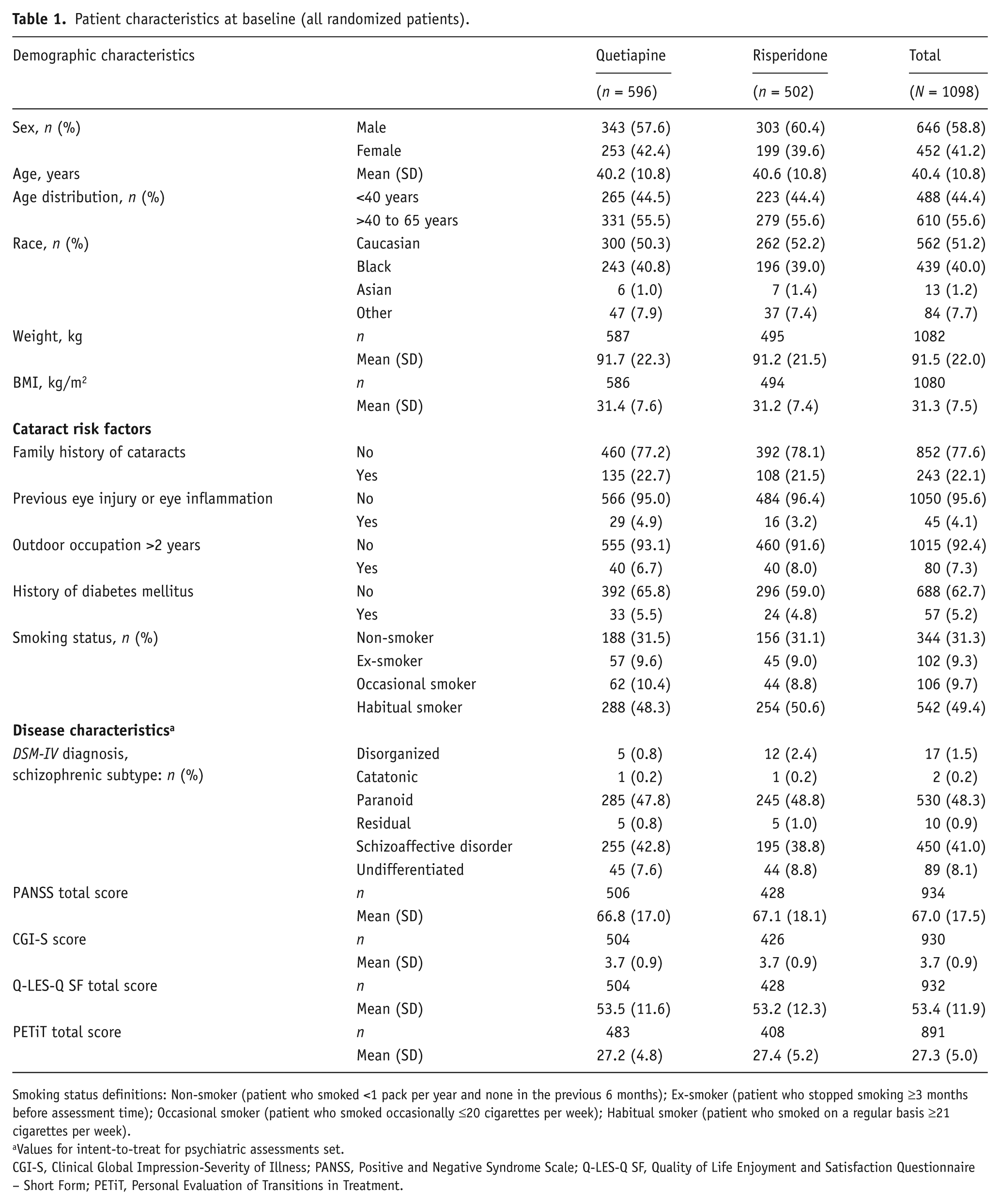
Smoking status definitions: Non-smoker (patient who smoked <1 pack per year and none in the previous 6 months); Ex-smoker (patient who stopped smoking ≥3 months before assessment time); Occasional smoker (patient who smoked occasionally ≤20 cigarettes per week); Habitual smoker (patient who smoked on a regular basis ≥21 cigarettes per week).
Values for intent-to-treat for psychiatric assessments set.
CGI-S, Clinical Global Impression-Severity of Illness; PANSS, Positive and Negative Syndrome Scale; Q-LES-Q SF, Quality of Life Enjoyment and Satisfaction Questionnaire – Short Form; PETiT, Personal Evaluation of Transitions in Treatment.
In total, 375 patients (34.2%) completed the planned 2-year study period (188 patients (31.5%) in the quetiapine and 187 (37.3%) in the risperidone group). The most common reasons for study discontinuation were ‘patient unwilling to continue’ (n = 118, quetiapine; n = 101, risperidone), ‘patient lost to follow-up’ (n = 95, quetiapine; n = 66, risperidone), AEs (n = 119, quetiapine; n = 82, risperidone) and development of study-specific discontinuation criteria (including inability to comply with protocol, noncompliance with study medication, and continued use of corticosteroid; n = 18, quetiapine; n = 17, risperidone). In the quetiapine treatment group, withdrawal rates were 8.6%, 18.2%, 15.8% and 8.8%, respectively, for patients previously treated with quetiapine, risperidone, both medications or neither. In the risperidone treatment group, the discontinuation rates were 6.7%, 18.1%, 15.3% and 7.8%, respectively.
Compliance with treatment was 95.7% in the quetiapine group and 93.5% in the risperidone group (E2PP analysis set). Mean doses were 386.3 mg/day for quetiapine (range of mean doses, 25–821 mg/day) and 3.2 mg/day for risperidone (range of mean doses, 1.2–8 mg/day). Mean durations of exposure were 345.1 days in the quetiapine group and 399.3 days in the risperidone group, while median durations of exposure were 267 and 374 days, respectively.
A total of 38 patients (3.5%) discontinued study medication but continued in the study for 24-month eye assessment, including 24 (4.0%) in the quetiapine and 14 (2.8%) in the risperidone group.
Primary study variable: Cataractogenic potential
Quetiapine was non-inferior to risperidone for changes in lens opacity grade in patients with schizophrenia or schizoaffective disorder. The estimated absolute risk differences in cataractogenic events for quetiapine versus risperidone over the 2-year period were −0.035 (C), −0.012 (N) and −0.017 (P), with upper margins of CIs within the non-inferiority margin of 10% in all cases (Table 2; E2PP analysis set). In a post hoc analysis, the risk of any lens opacification event (i.e. C, N or P) was lower for quetiapine than risperidone, with the upper margin of the CI below 0% (n = 6 (3.73%) and 16 (9.52%) events, respectively; risk difference: −0.058; P = 0.035; Table 2). Of the 22 patients reporting any type of cataractogenic event during the study, 19 patients were aged ≥40 years. The incidence of cataractogenic events (C, N and P) assessed by LOCS II in the quetiapine and risperidone groups categorized by age group is shown in Table 3 (E2ITT analysis set). A plot of the absolute risk reduction for lens opacity grade events (C, N, P and ‘any’) in the quetiapine versus risperidone group is presented in Figure 3.
Risk differences between quetiapine and risperidone for cataractogenic events (2-year per protocol for eye evaluations (E2PP) analysis set).
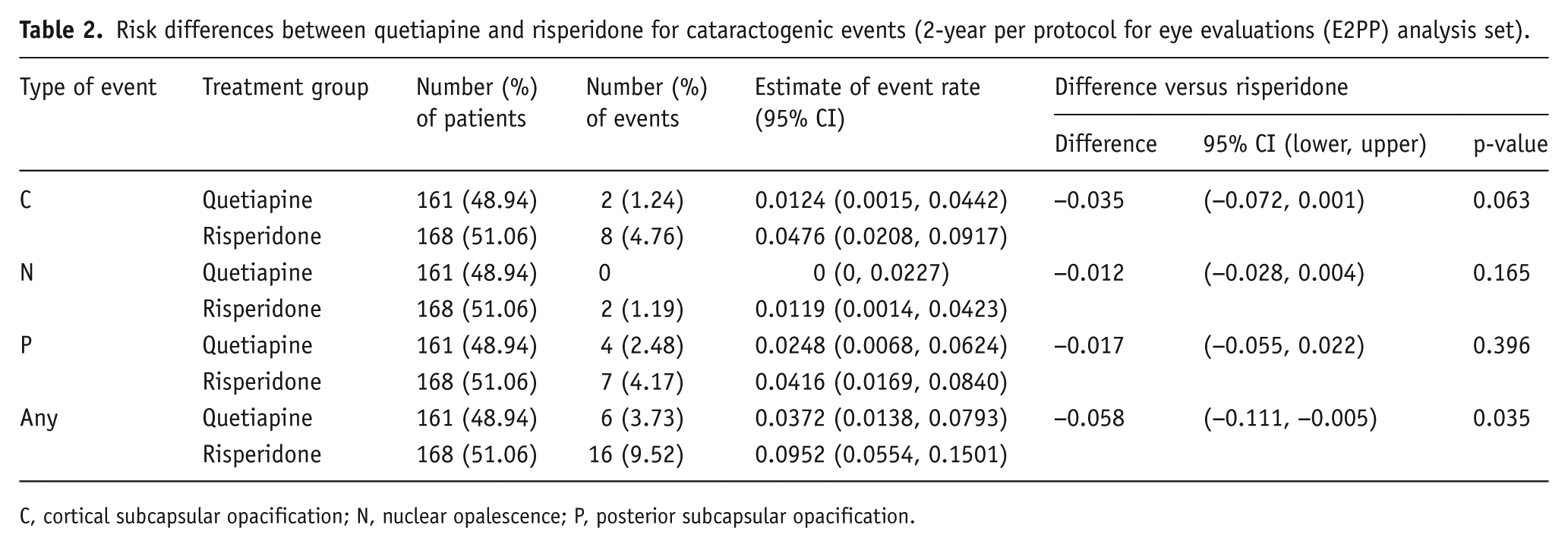
C, cortical subcapsular opacification; N, nuclear opalescence; P, posterior subcapsular opacification.
Cataractogenic events (C, N and P) by age group, assessed by LOCS II (2-year intent-to-treat for eye evaluations (E2ITT) analysis set).
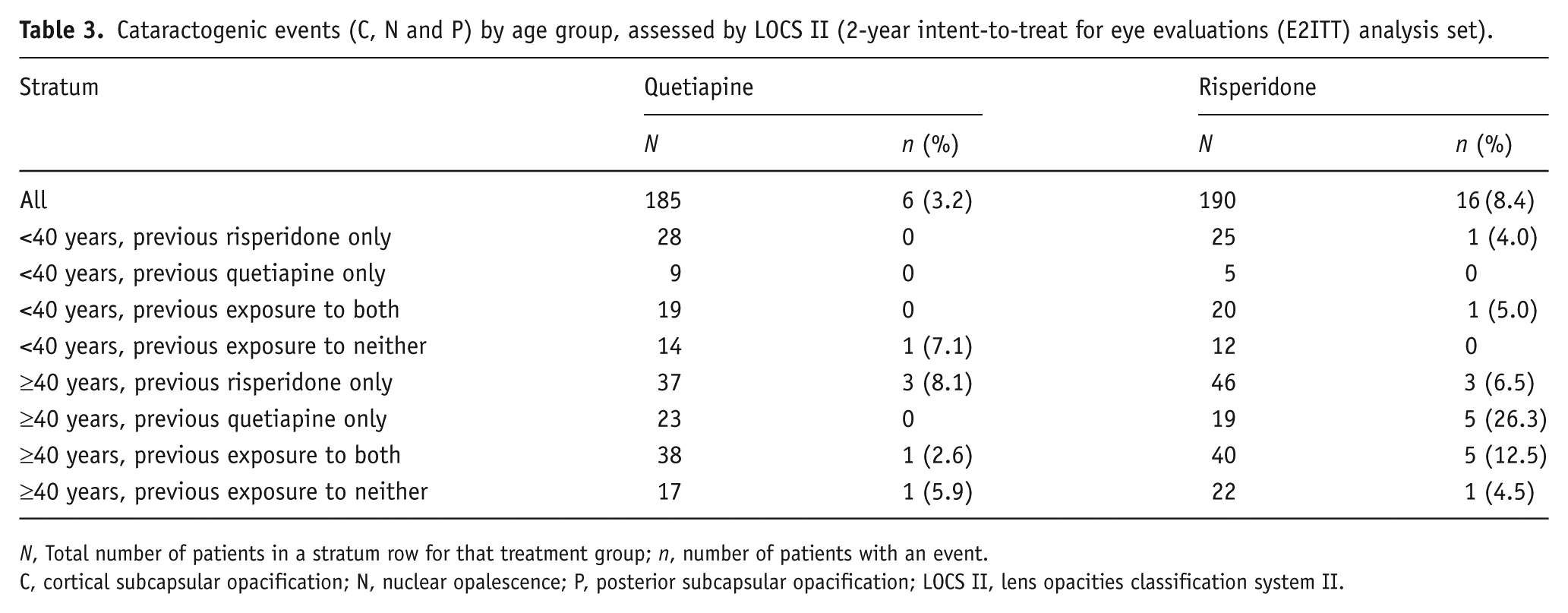
N, Total number of patients in a stratum row for that treatment group; n, number of patients with an event.
C, cortical subcapsular opacification; N, nuclear opalescence; P, posterior subcapsular opacification; LOCS II, lens opacities classification system II.
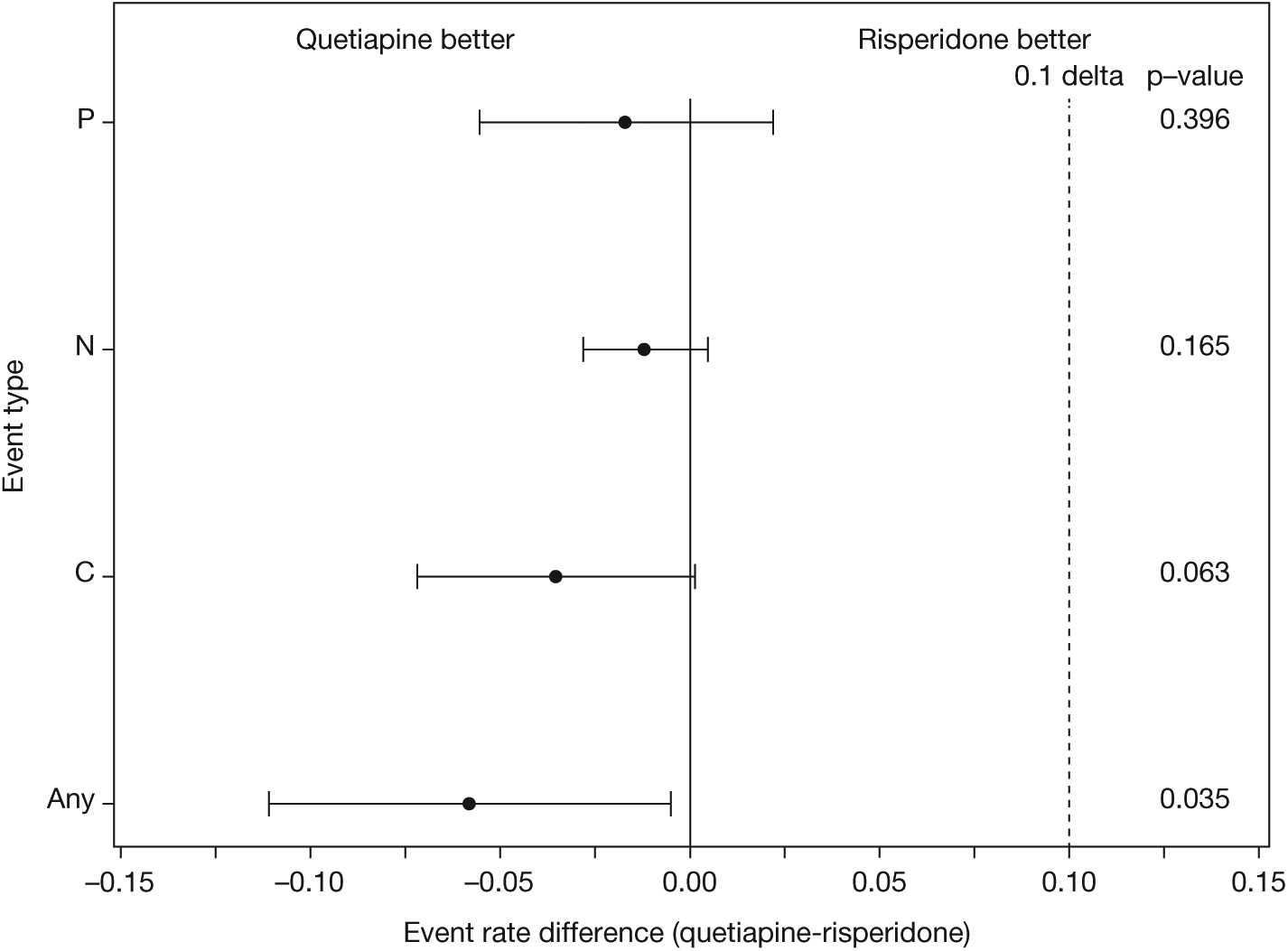
Plot of absolute risk reduction for lens opacity grade events for quetiapine versus risperidone (E2PP analysis set).
Supportive analysis on the EITT set provided results similar to the E2PP analysis set: the estimated absolute risk differences in cataractogenic events for quetiapine versus risperidone over the 2-year period were −0.017 (C), −0.006 (N), and −0.009 (P), with upper margins of CIs within the non-inferiority margin of 10% in all cases, with overall a lower risk of any lens opacification event in the quetiapine than risperidone group (n = 6 (1.56%) events, quetiapine group and n = 16 (4.46%) events, risperidone group; risk difference: −0.029; P = 0.019). There were no statistical differences in the evaluations by the two ophthalmologists in either E2PP or EITT sets.
In the EITT set, there were similar rates of prior use of quetiapine (47.5% versus 43.3%) and mean duration of prior quetiapine use (14.5 versus 14.4 months) between subjects treated with quetiapine and risperidone during the study. Similarly, rates of prior use of risperidone (65.7% versus 69.0%) and mean duration of prior risperidone use (21.4 versus 22.8 months) were similar between subjects treated with quetiapine and risperidone during the study. Prior quetiapine doses were 400.5 mg/day (SD 235.9) and 352.4 mg/day (219.6) in patients treated with quetiapine and risperidone, respectively, while prior risperidone doses were 4.0 mg/day (5.0) and 3.9 mg/day (4.0), respectively.
Supportive analyses of the time to first clinically meaningful increase in lens opacity grade (any of C, N or P) using Kaplan–Meier estimation are shown in Figure 4. A log-rank test with P-value of 0.036 supported the statistical significance of the Mantel-Haenszel estimate of between-group difference for any cataractogenic event. Separation in the number of any cataractogenic events between the quetiapine and risperidone groups began by the 6-month assessment and continued through the 2-year study period.
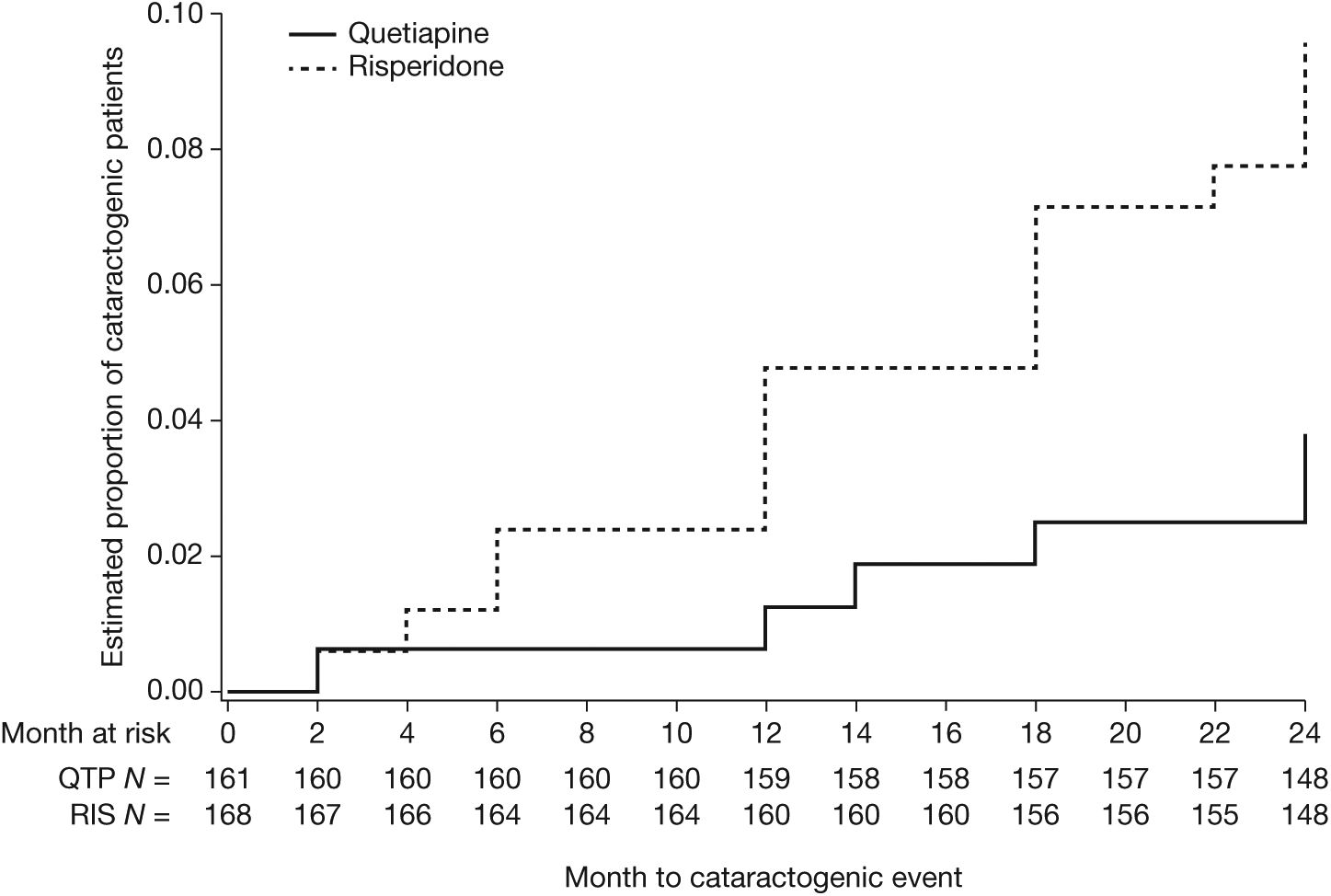
Kaplan–Meier estimation of time to first increase in LOCS II lens opacity grade (N, C or P; E2PP analysis set).
Sensitivity analyses performed on the E2ITT analysis set confirmed that quetiapine was non-inferior to risperidone in lens opacity grades. By the Cox proportional hazard model, quetiapine was associated with a significantly longer cataractogenic event-free survival than risperidone (hazard ratio = 0.32, 95% CI 0.11, 0.91; P = 0.033; E2PP analysis set).
Efficacy variables
Mean PANSS total scores at baseline were similar in the quetiapine and risperidone groups (66.8 and 67.1, respectively; Table 1). At 2-year assessment, mean PANSS total score decreased to 55.6 in the quetiapine group and 57.1 in the risperidone group (Figure 5). Mean PANSS positive, negative and psychopathology subscale scores at baseline in the quetiapine and risperidone groups were 16.5 and 16.4, 17.1 and 17.1, and 33.2 and 33.5, respectively. At 2 years, mean PANSS positive, negative and psychopathology subscale scores were 13.2 versus 12.9, 14.8 versus 15.7, and 27.7 versus 28.5 in the quetiapine and risperidone groups, respectively.
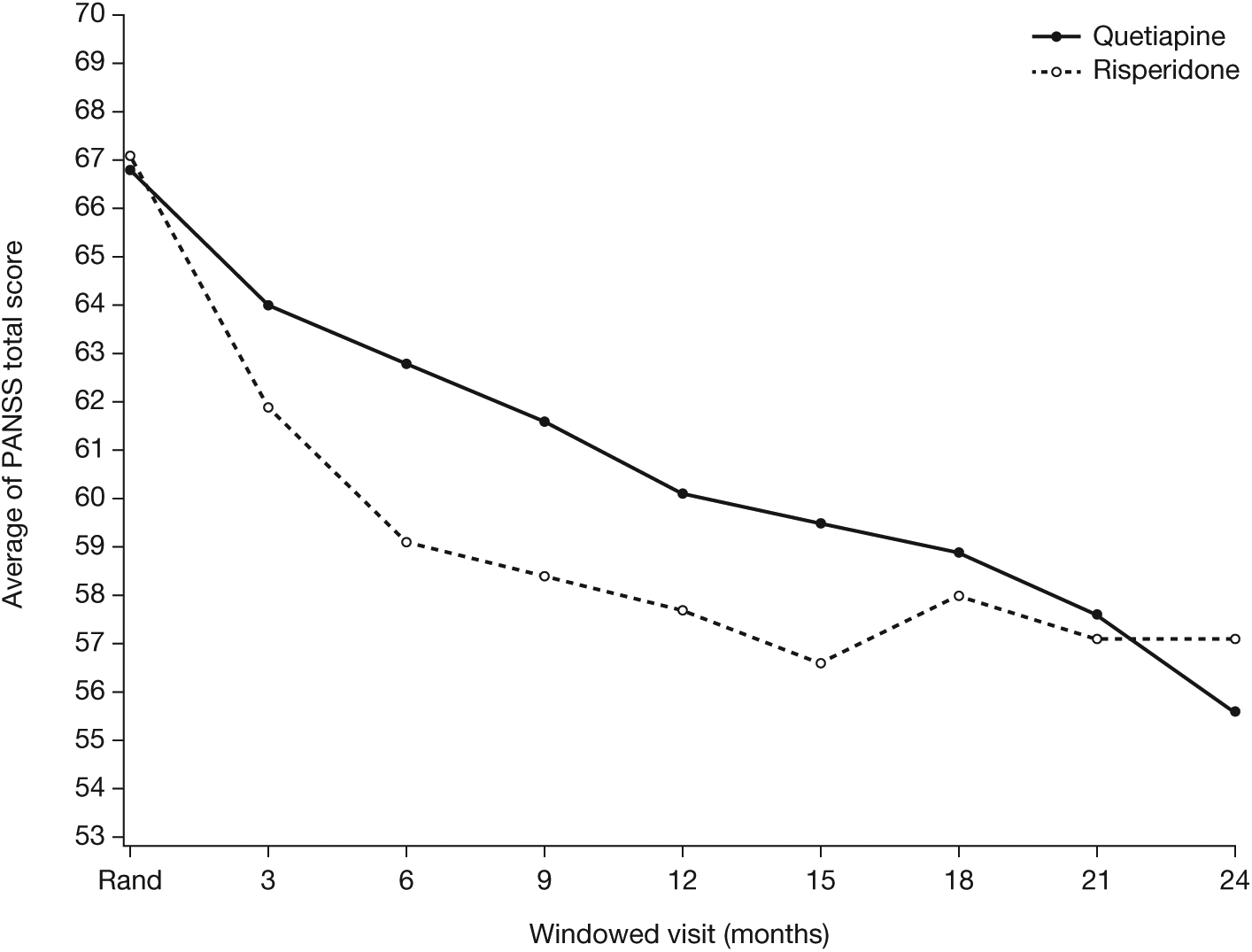
Plot of mean PANSS total score by visit and treatment (observed cases, ITTP analysis set).
Mean CGI-S scores decreased from 3.7 at baseline in both groups to 2.9 in the quetiapine group and 3.1 in the risperidone group at 2 years. Based on mean CGI-I scores, 18.3% of patients were very much improved, 36.0% were much improved and 25.6% were minimally improved in the quetiapine group at 2 years. In the risperidone group, 11.9% of patients were very much improved, 35.6% were much improved and 24.9% were minimally improved.
There was no significant difference between the quetiapine and risperidone groups in the time to first relapse of schizophrenia or schizoaffective disorder by Kaplan–Meier estimation (p-value of log-rank test 0.123; Figure 6). Cox proportional hazard modelling supported the non-significant results of Kaplan–Meier analysis for the difference between the quetiapine and risperidone groups in time to first relapse, with a hazard ratio of 1.24 (95% CI 0.93, 1.65; P = 0.137).
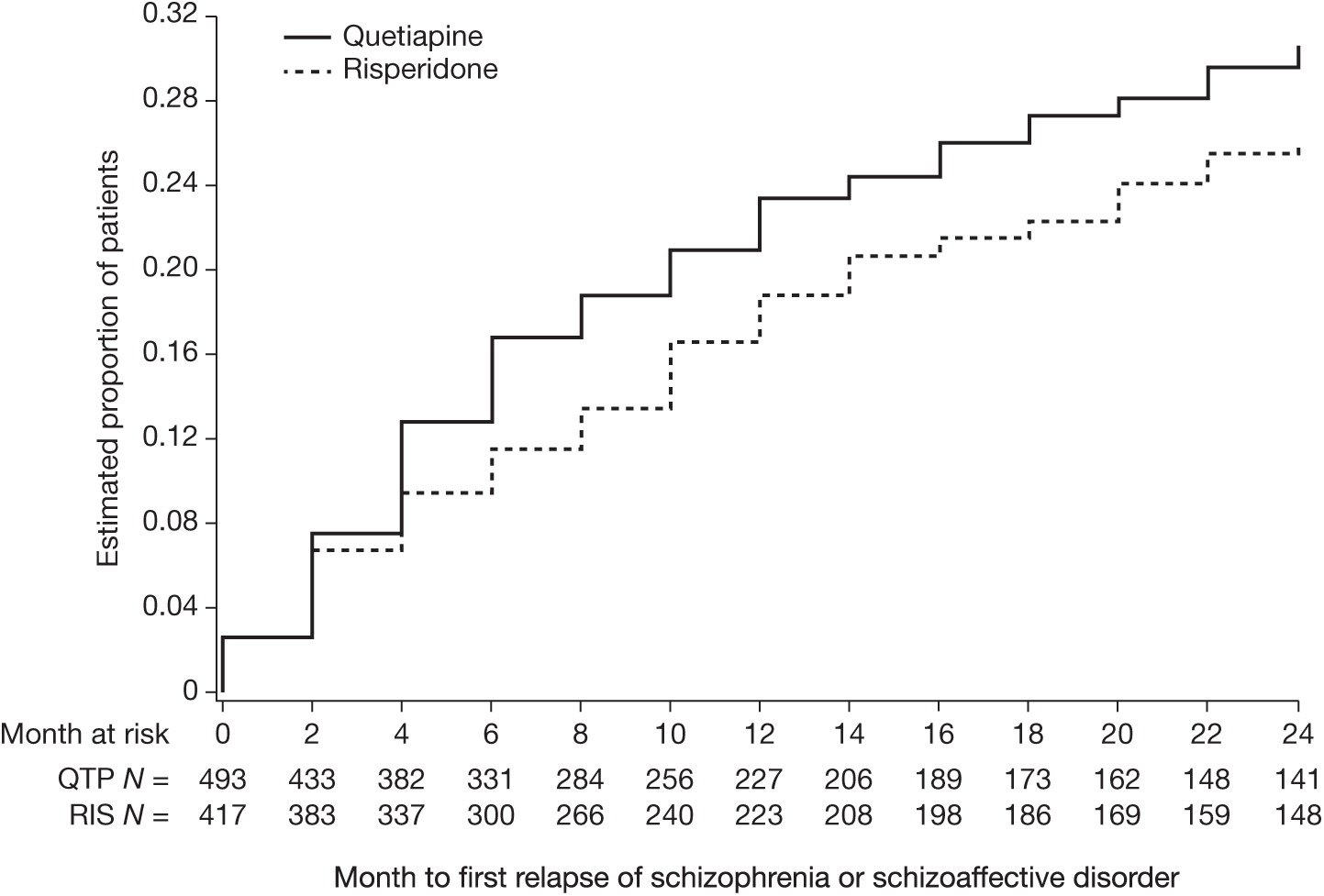
Kaplan–Meier estimation of time to first relapse of schizophrenia or schizoaffective disorder (ITTP analysis set).
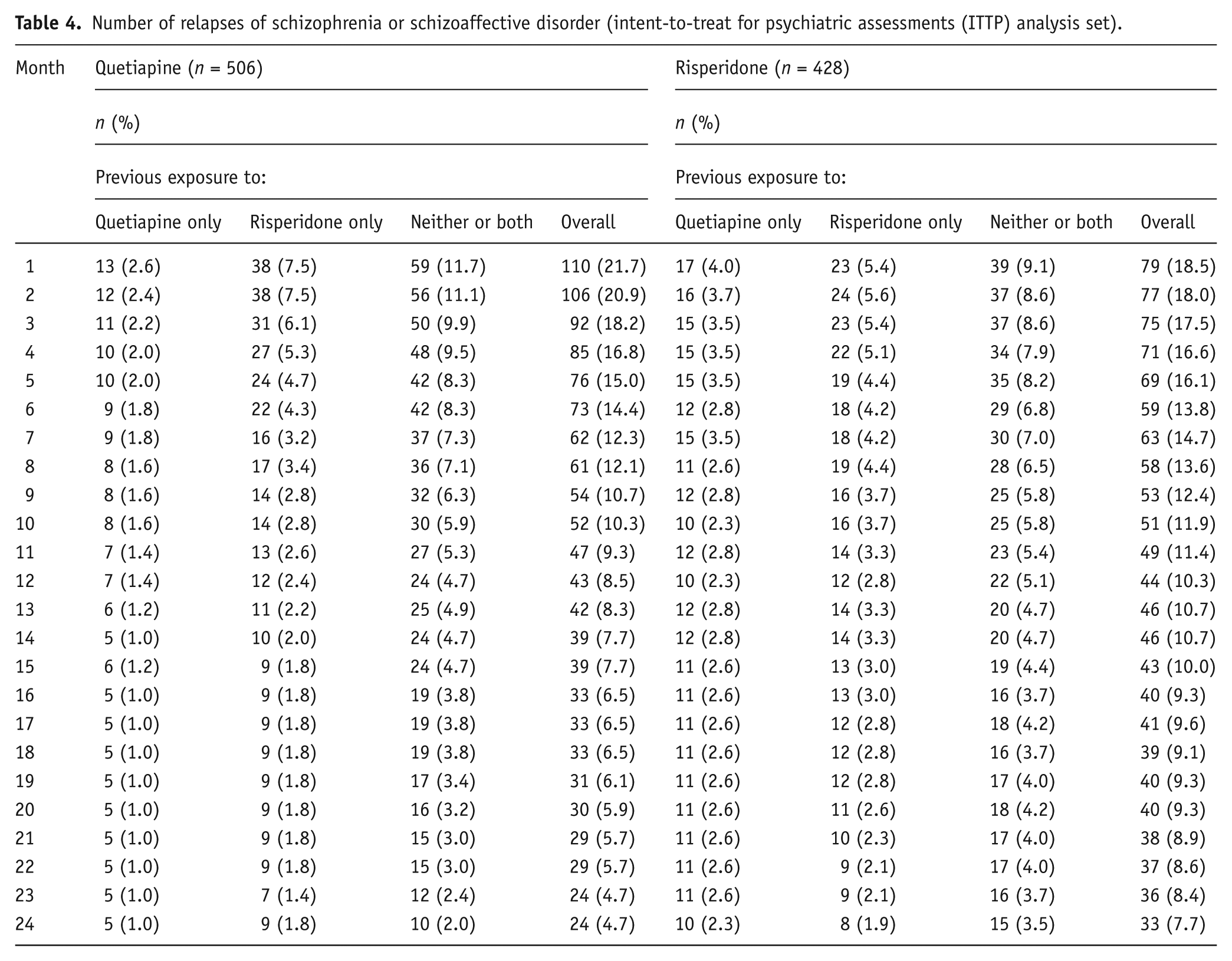
The number of relapses, including patients with multiple relapses, was similar between the two treatment groups, with no evident differences on the basis of prior quetiapine or risperidone treatment (Table 4).
Number of relapses of schizophrenia or schizoaffective disorder (intent-to-treat for psychiatric assessments (ITTP) analysis set).
Patient-reported outcomes
Mean Q-LES-Q SF total scores at baseline in the ITTP analysis set were similar in the quetiapine and risperidone groups (53.5 and 53.2, respectively) and showed similar improvements at the 2-year visit (56.4 and 55.4, respectively). Mean PETiT total scores were similar between the quetiapine and risperidone groups both at baseline (27.2 and 27.4) and at 2 years (28.2 and 28.0).
Adverse events
At least one AE was reported by 985 patients in the safety analysis set (91.0% overall; 93.0% in the quetiapine and 88.7% in the risperidone group) and at least one treatment-related AE was reported by 657 patients (60.7% overall; 63.1% in the quetiapine and 57.9% in the risperidone group). Supplemental Table 1 describes those AEs that occurred at an incidence ≥5% in either group.
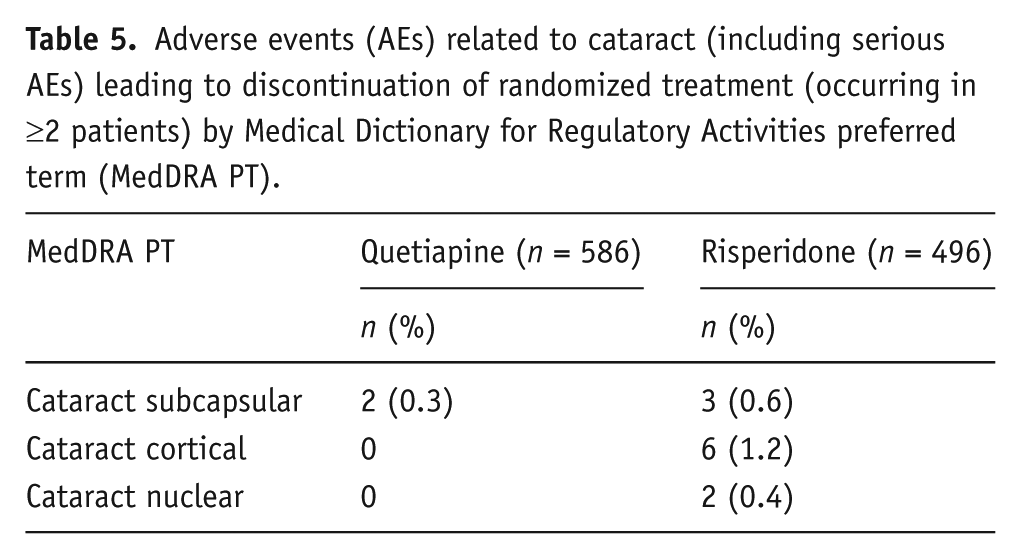
AEs led to discontinuation in 195 patients (18.0% overall; 20.0% in the quetiapine and 15.7% in the risperidone group) (see supplemental Table 2). Discontinuation was related to six cases (1.2%) of cortical cataract and two cases (0.4%) of nuclear cataract in the risperidone group, versus no cases of cataract in the quetiapine group. Subcapsular cataract led to discontinuation in two cases (0.3%) in the quetiapine and in three cases (0.6%) in the risperidone group (Table 5). Serious AEs were reported in 265 patients (24.5% overall; 25.8% in the quetiapine and 23.0% in the risperidone group). Nine deaths occurred during the study (seven (1.2%) in the quetiapine and two (0.4%) in the risperidone group). None of the deaths were treatment-related as assessed by investigators. The deaths in the quetiapine group were attributed to accidental overdose (n = 1), arteriosclerosis (n = 1), completed suicide (n = 2), metastases to the liver (n = 1), pneumonia (n = 1) and respiratory fume inhalation disorder and thermal burn (n = 1). The deaths in the risperidone treatment group were from completed suicide (n = 1) and illicit drug toxicity (n = 1).
Adverse events (AEs) related to cataract (including serious AEs) leading to discontinuation of randomized treatment (occurring in ≥2 patients) by Medical Dictionary for Regulatory Activities preferred term (MedDRA PT).
Clinical laboratory evaluations and physical findings
Mean changes from baseline to final visit and incidence of shifts in clinical chemistry, haematology, vital signs, and electrocardiogram parameters to abnormal values were consistent with the known safety profiles of the study compounds (see supplemental Tables 3–5). Mean (SD) increases in body weight by the end of treatment visit were 1.4 (8.7) kg in the quetiapine group and 0.8 (8.3) kg in the risperidone group, while incidences of ≥7% weight gain were 21.9% and 20.7%, respectively. The proportion of patients with ≥3 metabolic treatment-emergent risk factors was comparable in the quetiapine (12.9%) and risperidone (12.7%) groups.
Extrapyramidal symptom-related scales
Mean SAS total score changes between baseline and 2-year visit were −0.7 in the quetiapine group and −0.4 in the risperidone group. Mean BARS global assessment, AIMS total and AIMS-7 scores were unchanged in both groups. At 2 years, 13 events of worsening extrapyramidal symptoms were recorded in quetiapine-treated patients (7.8%) versus 33 events in risperidone-treated patients (18.2%), based on analysis of categorical changes in SAS score. Incidences of worsening symptoms based on BARS global assessment and AIMS total scores were similarly lower in the quetiapine-treated than risperidone-treated patients.
Discussion
The current randomized, open-label study was designed with input from the US FDA and is one of the most rigorous studies of cataractogenic potential performed on any antipsychotic to date. The study demonstrated that quetiapine is clearly non-inferior to risperidone, the comparator medication, for change in lens opacity grade during 2-year treatment in patients with schizophrenia or schizoaffective disorder.
An assumption made when designing the study was that risperidone is non-cataractogenic. The trial was designed as a non-inferiority study due to the expectation of a similar low rate for each of the three types of potential cataractogenic event (nuclear opalescence, cortical, or posterior subcapsular opacification) among patients treated with quetiapine or risperidone. Low rates of each type of event at 2 years were apparent in both treatment groups, while post hoc analysis indicated the overall rate of any lens opacification event (combined nuclear opalescence, cortical, and posterior subcapsular opacification) was significantly lower in the quetiapine than risperidone group (3.73% and 9.52%, respectively; P = 0.035; E2PP analysis set). Sensitivity analysis on the EITT analysis set, which included all patients with at least one post-baseline evaluation, confirmed the results of the E2PP analysis set, with overall rates of any lens opacification event of 1.56% in the quetiapine and 4.46% in the risperidone group (P = 0.019). Analysis of the E2PP analysis set showed similar rates and durations of prior quetiapine or prior risperidone use between subjects treated with quetiapine and risperidone during the study, indicating that prior treatment was unlikely to have influenced cataractogenic rates.
A number of explanations may be considered for the apparent divergence between the current clinical study in humans and the preclinical study reported in beagle dogs for the cataractogenic potential of quetiapine. Potential explanations include differences between these studies in the methodologies for assessment, differences in the study drug dose and likely species-specific divergence in susceptibility to cataract formation. In support of a species-specific divergence in susceptibility is the observation that statins are associated with cataract formation in beagle dogs, but this association has not been replicated in man (Schlienger et al., 2001; Tan et al., 2007). Follow-up studies would be required to elucidate the underlying explanation for the divergent outcomes.
The efficacy results reported here show similar changes for mean PANSS and CGI scores and similar relapse rates in the two treatment groups. These long-term treatment effects are consis-tent with reports of the long-term efficacy of quetiapine and risperidone in other studies (e.g. Lieberman et al. (Lieberman et al., 2005)). Patient satisfaction during long-term treatment, measured by Q-LES-Q SF and PETiT scores, was also similar for quetiapine and risperidone. The safety assessments showed that both quetiapine and risperidone were generally well tolerated during the study, and the findings were consistent with the known long-term safety profiles of these medications. No new safety signals were identified in this clinical trial.
Limitations of the study include the open-label study design with lack of patient masking, the lack of exclusion of patients who had prior exposure to study medications, the high rates of discontinuation in both treatment groups and the absence of a placebo arm for ethical reasons. However, the large numbers of patients investigated, the use of validated assessments and the exclusion of medications with known cataractogenic potential during the study support the validity of the study outcomes, while the rates of discontinuation are consistent with previous studies (Lieberman et al., 2005). The similarity in efficacy and quality of life outcomes between the two groups supports that quetiapine and risperidone were investigated at equivalent, clinically relevant doses.
In conclusion, this study indicates that 2 years of quetiapine treatment is not associated with a clinically significant increase in cataractogenic potential when compared with the comparator treatment, risperidone. More specifically, quetiapine at a mean dose of 386 mg/day (range, 25–821 mg/day) was non-inferior to risperidone at a mean dose of 3.2 mg/day (range, 1.2–8 mg/day) over treatment durations of 345 and 399 days, respectively, for changes in lens opacity grade in patients with schizophrenia or schizoaffective disorder.
Footnotes
Acknowledgements
AstraZeneca provided support in the design and conduct of the study; the collection, management and analysis of the data; review of the manuscript; and decision to submit the paper for publication. The authors thank Bill Wolvey from PAREXEL, who provided medical writing support funded by AstraZeneca.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. AML: none declared. AJF: none declared. The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IB is a full-time employee of AstraZeneca. IR, WE and SP were full-time employees of AstraZeneca at the time the study was performed.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by AstraZeneca Pharmaceuticals LP.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.