
Abstract
This study examined the overall psychological effects of inebriation facilitated by the naturally-occurring plant hallucinogen Salvia divinorum using a double-blind, randomized, placebo-controlled trial. Thirty healthy individuals self-administered Salvia divinorum via combustion and inhalation in a quiet, comfortable research setting. Experimental sessions, post-session interviews, and 8-week follow-up meetings were audio recorded and transcribed to provide the primary qualitative material analyzed here. Additionally, post-session responses to the Hallucinogen Rating Scale provided a quantitative groundwork for mixed-methods discussion. Qualitative data underwent thematic content analysis, being coded independently by three researchers before being collaboratively integrated to provide the final results. Three main themes and 10 subthemes of acute intoxication emerged, encompassing the qualities of the experience, perceptual alterations, and cognitive-affective shifts. The experience was described as having rapid onset and being intense and unique. Participants reported marked changes in auditory, visual, and interoceptive sensory input; losing normal awareness of themselves and their surroundings; and an assortment of delusional phenomena. Additionally, the abuse potential of Salvia divinorum was examined post hoc. These findings are discussed in light of previous research, and provide an initial framework for greater understanding of the subjective effects of Salvia divinorum, an emerging drug of abuse.
Keywords
Introduction
Salvia divinorum (SD) is a popular recreational hallucinogen amongst adolescent males. The plant, typically chewed or made into a water infusion, has been used by curanderos in Mexico for physical and spiritual healing for hundreds of years (Jenks et al., 2011). The principal psychoactive component in SD is salvinorin A (SA), a potent and selective non-nitrogenous kappa opioid receptor (KOR) agonist (Roth et al., 2002). Recreational use, in contrast, typically involves smoking an extract of SA, leading to quick onset and short duration of effects. Little is known about the subjective experience of SD inebriation, despite its ongoing recreational use.
Several surveys have revealed that nontraditional SD use tends to be sporadic, with most users reporting less than 20 lifetime uses (Baggott et al., 2010). Of Americans who had ever used SD as of 2012, only 2% had used in the past month and only 12% in the past year (SAMHSA, 2012). Self-reported reasons for using SD include “curiosity,” “interest in drug-induced states of consciousness,” and “spiritual purposes” (Sumnall et al., 2011). These data suggest few rewarding effects of SD at typical recreational doses. Nevertheless, chronic daily use of a commercial preparation purported to be SD has been reported (Travis et al., 2012). Further, conditioned place preference (Braida et al., 2008) as well as conditioned place aversion (Sufka et al., 2014) have been demonstrated in rats. These conflicting results may be species and/or dose specific.
SD is controlled in 20 US states (Drug Enforcement Administration, 2012) and is listed as a “drug of concern” by the US Drug Enforcement Administration (DEA) (Perron et al., 2012). SD is legally and commercially available in many states and countries, which likely contributes to its popularity (Khey et al., 2008). In 2012, 5.2 million individuals in the US (2% of the population) were estimated to have used SD in their lifetime, with highest use rate among young males (SAMHSA, 2012). In 2013, 3.4% of 12th graders in the US had used SD in the previous year, with highest use rate among males and Hispanics (Johnston et al., 2013). Use of SD is correlated with other hallucinogen use and with symptoms of depression and anxiety (Perron et al., 2012; Wu et al., 2011).
Several anecdotal reports have been published suggesting recreational use of SD can occasionally lead to psychotic symptoms requiring treatment by emergency care personnel (Bucheler et al., 2005; Przekop and Lee, 2009; Singh et al., 2007). However, prior personal and family psychiatric and drug use history, purity and potency of SD used, and long-term outcomes in these cases are under-reported. A review of the California Poison Control System (CPCS) found 37 cases where the CPCS had been contacted regarding patient exposure to SD in a 10-year period (Vohra et al., 2011). The most commonly reported symptoms were alteration in mental state (e.g. confusion, disorientation; n = 7) and hallucinations (n = 3). Such minimal reporting suggests little potential for toxic or fatal reactions to SD. The Drug Abuse Warning Network (DAWN) has tracked SD-related Emergency Department visits since 2004. However, they have been unable to estimate visits due to either overly large standard errors in their measurements or estimates of less than 30 cases per year (Drug Abuse Warning Network, 2013).
Retrospective surveys of repeat recreational SD users (Kelly, 2011; Nygård, 2007) report rapid onset and short duration of intense subjective effects as common themes. Twenty-five young adults (84% male, aged 18–29) reported a variety of subjective effects during SD inebriation, including perceptions of changes in bodily form, spatial relocation (e.g. revisiting places from childhood), altered time perception, visual hallucinations, confusion, and anxiety (Kelly, 2011). Thirteen repeat users (77% male) self-reported increased connection with others, creativity, and connection with nature, as well as a greater understanding of the nature of reality (Nygård, 2007). These findings are limited due to their retrospective nature, relatively small sample size, lack of objective characterization of substance and altered states, and potential recall bias.
Quantitative analyses of YouTube videos of individuals purportedly smoking SD have classified several observable behaviors during acute SD inebriation. Based on user behavior, facial expression, and dialogue, Casselman and Heinrich (2011) classified 100 YouTube videos as positive (65%), negative (12%), or neutral (23%). Similarly, Paterline and Albo (2013) classified 162 videos as either expansive (demonstrating euphoria, excitement, or discovery; 62% of videos) or constrictive (demonstrating fear or paranoia; 48% of videos). Lange et al. (2010) classified behavioral themes from 34 videos, noting the presence of expressions of emotions such as visible excitement or fear (94% of subjects), loss of coordination (88%), hyper-movement such as uncontrolled laughter or restlessness (84%), speech disruption such as disrupted diction or fluency (78%), and reported increases in body temperature (23%). However, such studies are limited due to unknown purity and potency of SD; other drugs potentially used concomitantly; and unknown subject characteristics, such as personal or family history of mental illness. Further, the subjective experience and the observable behavior have not been captured in the same sample of users.
Several controlled studies have been published recently describing behavioral, subjective, and physiological effects of SA (Addy, 2012; Johnson et al., 2011; MacLean et al., 2013; Mendelson et al., 2011; Pichini et al., 2005; Ranganathan et al., 2012; Siebert, 1994), none of which reported adverse events or sustained negative effects. Four of these studies (Addy, 2012; Johnson et al., 2011; MacLean et al., 2013; Ranganathan et al., 2012) employed the Hallucinogen Rating Scale (HRS) (Strassman et al., 1994), a quantitative assessment designed to characterize the subjective experience of intravenous administration of the serotonergic hallucinogen dimethyltryptamine (DMT). Although its generalizability to non-serotonergic hallucinogens has not been validated, the HRS has been used to describe alterationsin consciousness related to psychoactive substances of differing pharmacological classes and mechanisms of action includ-ing amphetamine, ayahuasca, dextromethorphan, ketamine, 3,4-methylenedioxymethamphetamine (MDMA), methylphenidate, psilocybin, and SA (Griffiths et al., 2006; Krupitsky et al., 2002; Reissig et al., 2012; Riba et al., 2001; Strassman et al., 1994; Tancer and Johanson, 2007).
While some authors have placed SD in the same category as psilocybin (Gonzalez et al., 2006), DMT (Coyle et al., 2012), and cannabis (Albertson and Grubbs, 2009), these may be inaccurate categorizations, likely due to the unique KOR agonist profile of SA (Roth et al., 2002). Recreational SD users report that SD inebriations differ from those of serotonin 2A receptor (5-HT2AR) agonist and N-Methyl-D-aspartate receptor (NMDAR) antagonist hallucinogens, for example by being less focused on visual distortions, more intense, and less enjoyable (Addy, 2012; Albertson and Grubbs, 2009; Baggott et al., 2010). Additionally, animal research has demonstrated that rodents and nonhuman primates trained to respond to SA do not generalize their response to delta or mu opioid receptor agonists, 5-HT2AR agonists, or NMDAR antagonists (Butelman et al., 2010). Further, SD is currently legal in the US and UK, compared to the highly restricted classification (US Schedule I, UK Class A and Class B) of psilocybin, DMT, and cannabis.
Basic and clinical research interests in the effects of KORs and SA are increasing (Butelman et al., 2012; Tejeda et al., 2012), however, adequate data on subjective effects in humans are lacking. No experimental research to date has incorporated mixed quantitative and qualitative methods toward understanding the subjective experience of SD inebriation. A qualitative examination of the subjective effects of acute SD inebriation may help to clarify several points, including: (a) abuse potential of SD; (b) psychotomimetic potential of SD; and (c) role of KOR system in consciousness.
Previously, we reported on the controlled self-administration of standardized extracts of SD in 30 healthy adult participants (Addy, 2012). Participants were rated as talking, laughing, and moving more often after inhaling 1017 mcg SA compared to a placebo dose of 100 mcg SA. Further, all six HRS cluster scores were elevated after active dose compared to placebo dose (see Table 1). No adverse events were reported after inhalation or at 8-week follow-up interview.
Participant ratings on Hallucinogen Rating Scale completed 1 h after drug self-administration.
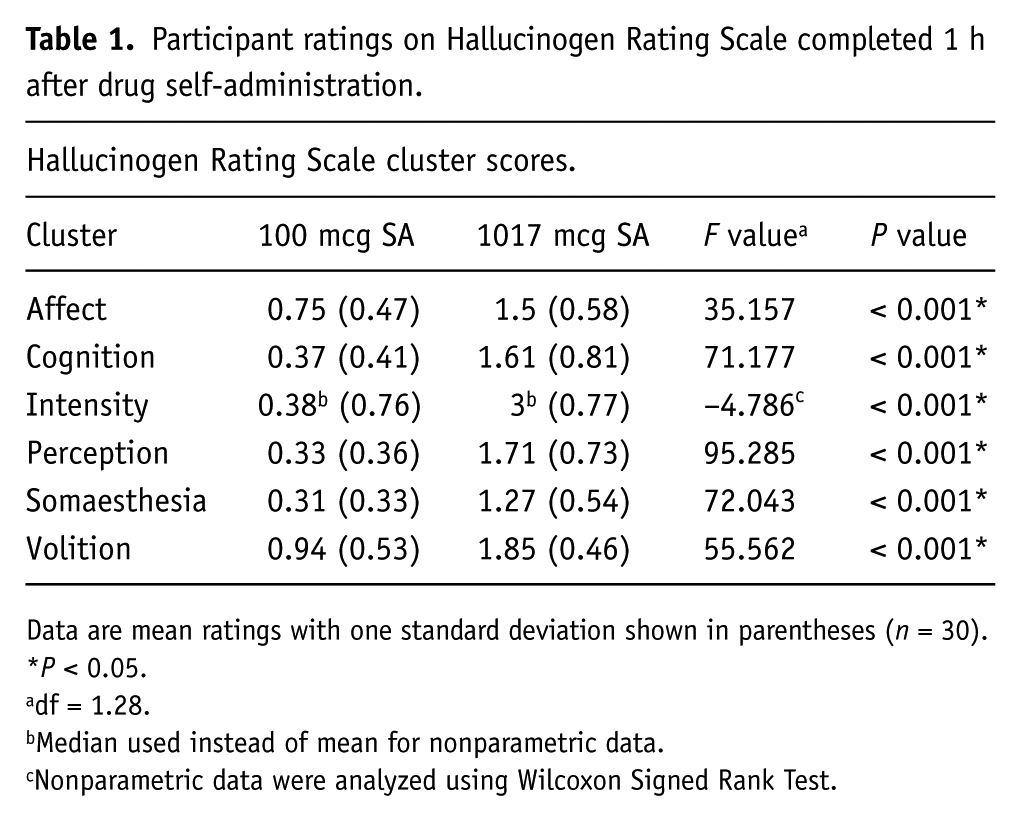
Data are mean ratings with one standard deviation shown in parentheses (n = 30).
P < 0.05.
df = 1.28.
Median used instead of mean for nonparametric data.
Nonparametric data were analyzed using Wilcoxon Signed Rank Test.
Methods and materials
Formal ethical approval was granted by the Research Ethics Committee of Sofia University (formerly the Institute of Transpersonal Psychology), Palo Alto, CA, and the study was carried out in accordance with the Helsinki Declaration of 1975. Study design, participant demographics, and quantitative results have been published previously (Addy, 2012).
Study design
This counterbalanced, double-blind, placebo-controlled, randomized, within-group study was conducted at the William James Center for Consciousness Studies (Sofia University, Palo Alto, CA).
Participants
Thirty-two participants were recruited locally through convenience sampling. Two individuals dropped out after screening and before test days, leaving 30 in the final sample.
Participants were medically and psychiatrically healthy adults based on self-report and completion of a structured clinical interview (SCID-I) administered and scored by a trained evaluator, fluent in English, aged 25–65. Volunteers without prior hallucinogen experience were excluded from participation. For this study, “prior experience” included ingestion of one of the following hallucinogens: psilocybin, LSD (d-lysergic acid diethylamide), mescaline, ayahuasca, or inhaled DMT. Participants were instructed to refrain from taking psychoactive substances, prescribed medication, and over-the-counter medication from screening through the second test day (mean duration 36.4 days). Abstinence was verified by self-report only, and did not include urine toxicology or Breathalyzer testing. Participants were not reimbursed for their time or travel.
Procedures
Participants completed four meetings with the research team: screening, two test days (average 14 days between test days), and an 8-week follow-up visit. Written informed consent was obtained during screening. On test days women underwent a urine pregnancy test, and all completed baseline ratings. In-study safety procedures were in place as described in a previous paper (Addy, 2012), including the presence of an Emergency Medical Technician (EMT) in an adjacent room at all times.
Test days
To maximize psychological and physical safety, and following published guidelines for ethical hallucinogen research (Johnson et al., 2008), the setting was designed to encourage relaxation and introspection. Participants had a brief conversation with the researcher and EMT to discuss their mindset and expectations for the day. Next, the researcher read a progressive muscle relaxation script and began playing classical music at low volume. Participants were encouraged to recline, close their eyes, and introspect. In the event of fear or anxiety, participants were encouraged to ask for assistance or put out their hand for the researcher to hold. Participants’ descriptions of their experiences during test sessions and post-session interviews were audio recorded, and all participants completed the 100-item HRS approximately one hour after SD administration.
Drugs
The SD was self-administered by the participant in order to increase generalizability to the non-traditional SD-using population. The Principal Investigator (PI) (PHA) placed 25 mg of plant material into a metal smoking pipe. The participant then ignited the material using a disposable butane lighter and inhaled the smoke. Participants were instructed to hold the smoke in their lungs for 15 s if possible. The doses were: an active dose of 1017 mcg SA dissolved onto 25 mg dried SD leaf and a presumed non-psychoactive dose of 25 mg un-enhanced dried SD leaf containing approximately 100 mcg SA.
The current dosage of 1017 mcg was chosen for its known ability to reliably produce psychoactive effects without significant adverse reactions. In contrast, a recent study used a high dose of 21 mcg/kg, or approximately 1391 mcg, of pure inhaled SA (MacLean et al., 2013). The active doses of SD were purchased as “Extra-Strength Standardized salvinorin A Enhanced Leaf” (Salvia divinorum Research and Information Center (SDRIC), Malibu, CA) (Siebert, 2014). SA was extracted from SD and purified using a process of solvent partitioning followed by repeated recrystallization. HPLC analysis indicated 98% purity, with the main impurity being salvinorin B. One gram of 98% pure SA was dissolved in methylene chloride and mixed with 25.6 g dried SD leaves containing 0.4% SA (by weight), resulting in 26.6 g plant material containing 1082.4 mcg SA. This mixture was divided into 1064 units, each theoretically containing 25 mg SD leaf and 1017 mcg SA. This final potency was calculated from initial conditions; it was not measured after production. Mr. Siebert states that, “it is safe to say that the dosage is accurate within a plus or minus 2% margin” (D. Siebert, personal communication, 24 February 2011).
Unaltered SD leaf was also purchased from the SDRIC as “Sierra Mazateca Prime Harvest Dried Salvia divinorum Leaves,” which the PI then ground, measured, and packaged into identical 25 mg doses. These placebo doses theoretically contained approximately 0.4% SA, or 100 mcg per 25 mg dose (D. Siebert, personal communication, 24 February 2011). Previous analysis revealed no subjective or behavioral effects of the placebo dose (Addy, 2012). Un-adulterated SD leaves were chosen as the comparator in order to maintain the blind. Both doses looked identical, and participants remarked that they smelled and tasted identical.
Analyses
Qualitative data related to the active dose condition were analyzed, including anything the participant said during the experience, post-session interview, and follow-up, as well as open-ended responses from the HRS. Audio data were transcribed by professional third parties and the PI (PHA), and transcripts checked against the recordings for accuracy. Quantitative results from HRS questions were also considered in the following exploratory mixed-methods analysis to supplement qualitative reports.
Qualitative data were subjected to thematic analysis, which is defined as “a method for identifying, analyzing, and reporting patterns within [qualitative] data [that are] … essentially independent of theory and epistemology” (Braun and Clarke, 2006: 79). This approach emphasizes an inductive “bottom-up” identification of patterns in which themes are generated directly from the data rather than theoretical orientations or specific questions asked during the interview.
Coding was carried out independently by three authors (PHA, AGR, MM) to reduce bias, using MaxQDA v9.5 (VERBI Software, Marburg, Germany) and Dedoose (SocioCultural Research Consultants, Los Angeles, CA). Adhering to the methodology of Braun and Clarke (2006), any feature of the data that appeared salient to the researcher was identified and coded. Codes were then collated into overarching themes, using all relevant coding excerpts to generate an initial thematic map. The researchers then collectively examined all themes, checking for both internal homogeneity (that codes within a theme were consistent) and external heterogeneity (that themes were distinct from each other). Themes were co-analyzed, labeled, and given specific operational definitions. Finally, vivid representative quotations were selected to illustrate the relationship of themes to the research question for inclusion in this report.
Results
Participants
The study sample consisted of 30 participants (mean age = 39; 47% female), with 37% reporting previous SD use. Demo-graphics and participant characteristics have been reported previously (Addy, 2012). During statistical analyses and theme generation, no differences were noted based on gender or previous substance use.
Themes
Thematic analysis identified three major themes and 10 subthemes. Major themes included: (a) qualities of the experience; (b) perceptual alterations; and (c) cognitive-affective shifts. Themes were organized according to common elements of human experience (e.g. perception, cognition), and the effects observed under the influence of SD within these basic psychological domains. They are presented here in a bottom-up fashion, beginning with the essential qualities of the experience, and continuing to effects on increasingly higher order systems from sensation and perception, to affect, cognition, and self-awareness. In addition to bottom-up theme generation, one a priori theme was created to explore the abuse potential of SD determined by perceived desire to use SD at the end of the test day and actual use of SD within eight weeks of the test days. Participant quotes are denoted by participant ID (1–16) and gender (F or M).
Theme one: Qualities of the experience
This theme encompasses three basic subjective effects attributed to acute administration of SD rapid onset, intensity, and uniqueness. These qualities seemed to be inextricably linked, having some bearing on one another and on the global assessment of the drug effect.
Rapid onset
The rapid onset subtheme referred to the suddenness, abruptness, and brevity of the drug experience: “It was so quick and unexpected” (10M); “The transition between states was abrupt, very abrupt and that was a little unpleasant” (7M). Twenty-six participants (87%) described a “rush,” experienced as a marked shift out of normal waking consciousness, and highlighting a sense of disorientation that was also commonly reported: “I got completely in it and completely lost my orientation of where I was” (10F); “It all just happened really fast, but there was some information going on” (7F). Eighteen individuals (60%) described feelings of disorientation, and nine (30%) attributed this to the rapid onset and brevity of the experience. On the HRS, the mean score for the item “amount of time between when the drug was administered and feeling an effect” was 0–5 seconds.
Intensity
Another key feature of SD inebriation was the high degree of intensity with which the drug effects were felt. Participants were asked to rate the intensity of their experiences in both active and placebo conditions on a scale from 0, “not at all intense,” to 4, “extremely intense.” In the active dose condition participants overall considered the experience to be very much to extremely intense (M = 3.1 active vs. 0.5 placebo). One participant emphasized, “The sudden intensity and the short duration” (6M) as standing out. On the HRS, mean ratings for both “intensity” and “high” were “very much,” or 3 on a 0–4 Likert scale.
Reported uniqueness
The SD experience was often referred to in terms of its uniqueness or apparent difference from other previously experienced states. Participants referred to the experience as a whole as different from other experiences in the participants’ own personal repertoire. Fifteen (50%) described their experiences as unique, novel, or strange: “It’s a very unique psychedelic, and I’ve never had anything else that induces that same [or] even somewhat similar state” (6M). Similarly, six (20%) described their experiences as “crazy” in nature. “That’s crazy. I’ve never felt anything like that … It was like a crazy dramatic river scene” (8M).
Theme two: Perceptual alterations
This theme is characterized by marked changes in sensory processing and perceptual integration. A wide range of such effects was observed during SD inebriation. These were divided by general modality into three subthemes: auditory, visual, and interoceptive phenomena. Although some minor olfactory and gustatory effects were noted (smell of bacon, taste of “battery” and water) these were limited to only three participants, and therefore did not warrant their own subthemes. In all, 17 participants (57%) described two or more sensory channels mixing (i.e. synesthesia). These have been classified in the following sections according to the dominant sensory modality.
Auditory phenomena
Participants reported changes in usual hearing function. To mask potentially distracting sounds from the research setting (e.g. people in adjacent areas, air conditioning) a classical music CD (Gorecki, 1976) was played during the drug administration session. However, six participants (20%) reported not hearing anything: “The deafening sound of quiet. I didn’t really hear a noise for some reason” (1M).
Furthermore, five participants (17%) described hearing sounds the researcher did not hear, ranging from frank auditory hallucinations (e.g. “a voice telling us all to come along and leave the door open” (2M)) to less well-defined auditory sensations (e.g. “Not physical sounds, but the sense of a lot going on around me, sense of sound” (7F)).
Visual phenomena
Visual phenomena were widely reported after SD inhalation, including visual distortions, illusions, and hallucinations. Twenty-five participants (83%) reported closed eye visual imagery, ranging from elementary geometric patterns, lights, and colors to complex scenic hallucinations: “What had been a bit of light entering through the bottoms of the eye mask became two voluminous hills or waves, and then they were supplemented by others that extended outwards into a horizon” (6M). On the HRS, “dimensionality of images/visions/hallucinations” was given a mean rating of 3, or “multidimensional,” and the item “movement within visions/hallucinations” was scored “very much.”
Visual imagery was often described as swirling, spiraling, or kaleidoscopic in nature: “garden images morphing into spirals” (2M); “a whole bunch of little diamond shapes in this whole kaleidoscope that was the world” (12M). In addition, six (20%) reported a “kaleidoscopic” synesthesia, referring to some combination of sensory modalities: “It was a kaleidoscopic visual thing going on; a general body buzz” (13M). Furthermore, seven (23%) experienced a mixture of visual and tactile sensations: “I think it looks the same way that it felt” (9F).
Interestingly, five people (17%) specifically described seeing carnival scenes: “It took me in a different place altogether, some sort of carnival tent” (6F). In contrast to such complex scenic hallucinations, several participants reported less defined visual distortions: “It was beautiful and it was expanded. It was light filled. It was peaceful. It was beautiful, but it didn’t have any form, like nothing I recognize” (12F).
Interoceptive phenomena
Participants experienced both tactile and kinesthetic hallucinations. Tactile hallucinations are defined as bodily sensations in the absence of correspondent sensory stimuli, while kinesthetic hallucinations are characterized by illusory sensations of bodily movement (Blom and Sommer, 2012).
Twelve participants (40%) described physical sensations moving up the body toward the head: “Beginning in abdomen rising on left side peaking in the face and gently falling down to right” (9M). Eight (27%) expressed an abnormal sense of touch or being touched: “There’s some kind of strange thing going on in my mouth, as though there was a tongue depressor in there” (15F). Six people (20%) described their bodies being pulled, as well as a sense that their bodies moved pliably with the pulling. Six people (20%) described their bodies as twisting or spinning. Four people (13%) mentioned their bodies tingling: “An inward musculature tingling in every muscle that can move” (6M). Furthermore, four people (13%) described visual-tactile synesthesia consisting of visual imagery of objects being “folded” and simultaneously feeling that their bodies were being folded: “The field was solid, but I was falling through the field and then there was a diamond shaped pattern. I was falling through the pattern, and it was all folding in, and it was falling away from me” (12M).
Some individuals experienced changes in temperature after inhaling SD. Seven (23%) became cold: “Oh, I’m so cold. I’m cold. Can I get a blanket?” (4F). Seven people (23%) became hot: “The region around my face right here was burning like it was hot” (8F). Four people (13%) described sweating during the experience: “cycling in waves: hot sweaty to cold” (10M), and three (10%) reported clammy hands.
Other, more general somatic phenomena were also described. Three people (10%) reported a sense of bodily pleasure: “At the peak of it, my body felt wonderful. Really a beautiful body sensation … pure relaxed bodily pleasure” (5F). Additionally, three participants (10%) expressed feeling tired or sleepy: “The body feels a little tired, like you just went through something. It has a little bit of fatigue” (1M).
Theme three: Cognitive-affective shifts
In describing their experiences under the influence of SD participants reported noteworthy shifts in their emotional and thinking processes.
Changes in affect
Fourteen participants reported marked alterations in their emotional state during the course of drug action, to which they attributed positive valence (e.g. happiness, euphoria; n = 10, 33%) or negative valence (e.g. fear, anxiety, panic; n = 4, 13%). Descriptions of positive emotions included: “It was nice emotionally. I felt like I was connecting with something that I missed and I forgot about and was happy to be reconnecting with” (7F); “It’s so funny … I feel so good and happy” (4F). Negative emotions included: “feelings of guilt and selfishness” (15M), and “I felt frightened” (8F). Furthermore, three people (10%) described a change in emotional closeness with the researcher: “I already feel close. Now, closer” (4F); “Like I was alone” (15F).
On the HRS, the highest mean scores for affective items were for “self-accepting” and “awe, amazement” (mean 2.3 out of 4, corresponding to “moderately”), and the lowest mean scores were for the items “despair” and “sad” (mean 0.2 and 0.3, respectively, corresponding to “not at all”). Self-reports indicated that changes in affect had resolved by the end of the test day. Additionally, during the 8-week follow-up 9% of participants (n = 2) reported lasting negative affective shifts, including feeling “unsure of things” and “ready to cry,” and 17% (n = 5) reported lasting positive affective shifts, including feeling “aligned,” “wholesome,” and “calm.”
Depersonalization
Depersonalization is defined as a sense of detachment from one’s mind and body, as well as a feeling of dreamlike strangeness or unreality of the external world (Sierra and Berrios, 1998). Eleven participants (37%) reported experiencing such subjective alterations in their self-awareness: “[SD] made me feel like outside of who I normally am, but still me” (4F). Another feature of depersonalization is a sense of diminished volition or control over one’s thoughts and actions (American Psychiatric Association, 2013). Thirteen participants (43%) felt out of control for part of their experience. Participants’ attitudes toward losing control were split dichotomously between a stance of resistance or rejection on one hand, and acceptance or surrender on the other. Eight people (27%) described holding onto their sense of self and resisting the altered state experience: “I didn’t feel like it was under my control, which I guess was also kind of scary” (3F). In contrast, five people (17%) described surrendering into the experience: “There’s something delightful about not being in control. I actually really enjoy that experience of just being witness to my own mental experience” (1F).
Distorted body-ownership
Body-ownership “tells us that our body belongs to us, and other bodies do not” (Walsh et al., 2011: 3009). During SD inebriation, body-ownership and body identity showed dramatic alterations for some participants. Six people (20%) reported feeling disconnected from their bodies, e.g. “Disconnected from body, only ‘head’ awareness” (4F). Three participants (10%) noted an alteration in the perceived shape or makeup of their body: “I was blended in with the air around me” (9F); “I couldn’t tell if I was part of the carpet, or you’re part of the chair” (10M). Furthermore, three people (10%) felt paralyzed or unable to move for a portion of the experience.
Altered reality monitoring
Reality monitoring is the meta-cognitive ability to discriminate between real and imaginary events (Buda et al., 2011). Participants reported disturbed reality monitoring, such as an inability to track what was happening in consensus reality during inebriation and a profound immersion in drug-induced experiences. Twenty-two participants (73%) referred to consensus reality while describing the SD state: “The room was beginning to become movable” (5M). Twelve people (40%) reminded themselves of being in a research setting: “I maintained lucid awareness of my place in the room, and the intentions of the study and my thoughts” (6M). Nine participants (30%) described a total loss of awareness of the experimental session: “I didn’t have a sense of being in a position to observe myself. There was no third-person observation point” (5M); “I was so much a part of it there was no part of a person that had been” (10F). On the HRS, the item “able to remind yourself of being in a research room” was given a mean rating of “moderately.”
Twelve people (40%) specifically mentioned an awareness of the researcher. For 10 of those the researcher’s presence was deemed calming or reassuring: “you’re [the researcher] very grounded and stable” (7F). For the other two, the researcher’s presence brought suspicion or was perceived as distant: “I thought that you couldn’t hear me” (3F). Three people (10%) remarked upon having physical contact with the researcher: “No. I didn’t feel that [holding hands]. I was so busy, so intense and sweating … that I didn’t notice” (1M).
In addition to the researcher and participant, no other individuals were present during acute drug effects. However, 11 participants (37%) sensed other people or beings during their experiences: “I got the impression that other people could hear me and they were around. Almost like people were saying ‘It’s okay.’ It wasn’t you saying it; it was other people saying ‘It’s okay.’” (6F).
Theme four: Abuse potential
Immediately post-session all participants were asked to rate, “How soon you would like to repeat the experience” as part of the HRS (possible responses: “Never again,” “Within a year,” “Within a month,” “Within a week,” and “As soon as possible”). The mean and median responses were “within a week.” Mean ratings for “euphoria” and “desire for the experience regularly” were both “slightly,” or 1.4 and 1.2 out of 4, respectively.
At the 8-week follow-up, only two participants (9%) reported interim SD use. In contrast, 87% of participants had used other psychoactive drugs since the previous meeting: alcohol (61%), cannabis (39%), ayahuasca (9%), psilocybin mushrooms (9%), SD, and “ecstasy” (4%). During this follow-up meeting 20 (87%) said they would like to use SD again.
Discussion
We present the most detailed systematic analysis of the subjective effects of SD utilizing the largest sample to date. Our main findings indicate that smoked SD facilitates an intense altered state of consciousness consisting of marked changes in affect, cognition, interoception, and sense of reality. The experience itself was described as having rapid onset and being intense and unique. Individuals often lost normal awareness of themselves and their surroundings, as well as reporting an assortment of delusional phenomena. While these effects are sought by recreational users of SD and other hallucinogens (Sumnall et al., 2011), this sample did not report subsequently abusing SD according to DSM-IV-TR definitions, despite its legality and easy access.
Other qualitative research on SD has focused on data that may be more ecologically valid (e.g. online surveys, experience reports, YouTube videos), but cannot be effectively verified regarding key variables such as substance and dose, and has consequently been limited in its generalizability. However, rigorous qualitative analysis of placebo-controlled SD administration had heretofore not been published to the authors’ knowledge. Hence, this study together with previous studies helps us to understand what is happening within a substantially altered state of consciousness evoked by SD, and represents a significant contribution to the literature on the subjective effects of SD, specifically relating to: (a) abuse potential of SD; (b) psychotomimetic potential of SD; and (c) role of KOR system in consciousness.
Comparison to previous SD research
Portions of our findings have been reported anecdotally elsewhere (Gonzalez et al., 2006; MacLean et al., 2013; Ranganathan et al., 2012), indicating some reliability of participant accounts and objective measures of SA/SD effects. These results are congruent with previously published work. The typical course of effects for inhaled SA is less than 20 minutes, with peak subjective effects achieved approximately two minutes after inhalation (Johnson et al., 2011). The subthemes of rapid onset and intensity reported here confirm prior accounts detailing the abrupt, sometimes overpowering subjective effects of SA/SD (Gonzalez et al., 2006; MacLean et al., 2013), highlighting these as reliable, reproducible features of SA inebriation. Intensity of SD is likely related to route of administration and pharmacodynamic availability of SA. Auditory hallucinations and the sensed presence of other entities in the room have also been observed in other human SA laboratory research (MacLean et al., 2013). In keeping with our findings, KOR agonists have been shown to exhibit dose-dependent effects upon thermoregulation in animal models (Baker and Meert, 2002). However, no significant difference in body temperature was observed between placebo and active dose SD sessions in this study (Addy, 2012). Also congruent with our results, survey data on recreational SD use found feelings of relaxation and physical tiredness to be among the most commonly reported pleasant and unpleasant subjective effects of SD respectively (Gonzalez et al., 2006).
Comparison to other recreational drugs
SD produces visual-tactile synesthesia. According to a recent systematic review (Luke and Terhune, 2013), substance-induced synesthesia is usually visual-auditory in nature. Other than SD there are three reports of mescaline-induced visual-tactile synesthesia. However, these three reports are older (1934–1966) and with limited subject samples (4–5 each). The exact mechanism by which synesthesia occurs is currently unknown. Synesthesia is thought to be related to 5-HT2AR-mediated excitation of pyramidal neurons (Brogaard, 2013). Exploring synesthesia induced through the activation of alternative neurotransmitter pathways may provide key data in the ongoing effort to understand synesthesia and higher order perceptual integration.
Our results suggest moderate overlap between HRS items and themes related to SD inebriation. HRS scores from our group are roughly comparable to those obtained by Johnson and MacLean (Johnson et al., 2011; MacLean et al., 2013), and somewhat higher than those obtained by Ranganathan et al. (2012). In comparison to other pharmacology challenge studies, the HRS changes induced by SA are most similar to those induced by ayahuasca (e.g. Barbanoj et al., 2008; Dos Santos et al., 2012; Riba et al., 2006). However, this scale has not been quantitatively validated with regard to non-serotonergic hallucinogens such as SA, and may therefore be neglecting key features of SA subjective effects. Seventy-one items compose the six HRS cluster scores, yet the HRS is composed of 100 items. Future research could benefit from an exploratory factor analysis on all 100 items in order to determine more accurate and inclusive cluster scores. This will serve to increase validity of the HRS and help quantitatively compare and contrast altered states of consciousness.
The DSM-5 (American Psychiatric Association, 2013: 524) defines hallucinogens as “a diverse group of substances [that] produce similar alterations of perception, mood, and cognition in users.” Hallucinogens include phenylalkylamines, indoleamines, ergolines, and “miscellaneous other ethnobotanical compounds” including SD. However, cannabis is excluded from the hallucinogen group due to “significant differences in their psychological and behavioral effects.” Our results indicate both similar alterations and significant differences in effects between SD and other hallucinogenic substances. Given the rapid proliferation of newly synthesized hallucinogenic compounds, careful consideration of pharmacology and subjective effects is warranted in the classification of novel drugs of abuse (Vandrey et al., 2012).
Implications for abuse, psychosis, and consciousness
The current study lends support to the view that SD, like synthetic KOR agonists, has a low potential for abuse. Subjects did not report experiencing euphoria or craving to use, and did not seek out SD subsequent to experimental exposure. Animal models suggest some potential therapeutic applications of SA and other KOR agonists in the treatment of addiction (Freeman et al., 2014; Morani et al., 2009; Walker et al., 2012). To date there are no published studies or case series discussing the therapeutic use of SD for addiction. However, a series of cases has been published describing SD use as an antidepressant (Hanes, 2001, 2003). Further investigation is warranted on the effects of SA on reward behavior and mood in humans.
Results indicate a potential role for use of SA in probing neural substrates of psychotic symptoms such as auditory hallucinations and impaired reality testing (White and Roth, 2012). Studies of KOR distribution in animal models have found that these receptor sites are widely dispersed throughout the brain and are present in visual processing areas, such as the superior colliculi and periventricular hypothalamic nuclei (DePaoli et al., 1994; Mansour et al., 1995), which play a role in the occurrence of hallucinations in particular clinical syndromes (e.g. peduncular hallucinosis) (Manford and Andermann, 1998; Mocellin et al., 2006). However, the precise mechanisms by which SA may mediate such perceptual alterations are still uncertain, and remain a topic of interest for future research. Furthermore, the specificity of particular hallucinatory content, such as carnival imagery, suggests another area for future study.
The role of the KOR system in the generation and maintenance of conscious experience is currently underexplored. We hypothesize that the effects of salvinorin A on consciousness may be mediated by disruption of activity in the claustrum and the insular cortex, two brain regions located between the basal ganglia and the cortex with widespread connectivity to the cortex (Mathur, 2014).
The claustrum contains the highest density of KOR receptors in the entire brain (Peckys and Landwehrmeyer, 1999). The morphology and function of the claustrum remain to be elucidated. Theories suggest the claustrum may act to bind and integrate multisensory information, or else to encode sensory stimuli as salient or nonsalient (Mathur, 2014). One theory suggests the claustrum harmonizes and coordinates activity in various parts of the cortex, leading to the seamless integrated nature of subjective conscious experience (Crick and Koch, 2005; Stiefel et al., 2014). Disrupting claustral activity may lead to conscious experiences of disintegrated or unusually bound sensory information, perhaps including synesthesia. Such theories are in part corroborated by the fact that SA, which functions almost exclusively on the KOR system, can cause consciousness to be decoupled from external sensory input, leading to experiencing other environments and locations, perceiving other “beings” besides those actually in the room, and forgetting oneself and one’s body in the experience.
Additionally, synthetic KOR agonists bind to the human insula with high affinity (Izenwasser et al., 1999). The insular cortex is thought to play a role in interoception and self-awareness, and has been considered as a potential neural correlate of consciousness (Craig, 2009). Participants in this study reported a variety of interoceptive distortions and hallucinations, as well as distortions in self-awareness such as “forgetting” that they had a physical body. Previous studies have shown vaporized salvinorin A to produce mystical-type experiences in healthy volunteers (Johnson et al., 2011; MacLean et al., 2013). In an fMRI study examining the neural correlates of recall of mystical union with God in a sample of Carmelite nuns, joint activation of the anterior insular cortex and the anterior cingulate cortex was observed (Beauregard and Paquette, 2006).Thus, one aspect of such drastic alterations in consciousness could be related to disruption of the insular cortex and/or disruption of the connection between the anterior insular cortex and the anterior cingulate cortex.
Imaging studies documenting the neural correlates of acute SA inebriation in healthy adults would do much to shed light on the role of the KOR system in consciousness, mental illness, and addiction. However, there are difficulties inherent in this task. The close proximity of the claustrum and the insular cortex renders them impossible to distinguish via PET (Mathur, 2014). More generally, the subjective effects of smoking or vaporizing SA last approximately 10 minutes, while neuroimaging scans require several times that length to complete. Exploring alternative routes of administration will be important for future research.
Limitations
Ecological validity was sought through participant self-administration of a standardized extract of SA-enhanced SD leaf, the most common method of consumption in the general population (Baggott et al., 2010). However, there are inherent limitations to the generalizability and replicability of this method, including idiosyncratic smoking behavior and differences in lung capacity. Our sample was older (mean age 39) and included more females than the typical SD using population aged 18–25, according to the 2012 NSDUH (SAMHSA, 2012). Further, subjects were not tested for recent drug use during screening or test days. Subjects could theoretically have been under the acute or post-acute influence of recreational drugs during their SD inhalation. As with any qualitative research, the researcher’s own biases and expectations may have influenced the analysis. To help reduce such bias, two raters not involved with the experimental procedures independently coded the transcripts. Further, the combined quantitative and qualitative approach was designed to minimize the weaknesses of each.
Footnotes
Acknowledgements
We thank Daniel Siebert for providing the Salvia divinorum; Anne Huffman and David Lane for providing their time as EMTs; and Dr. Swapnil Gupta for comments on this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Portions of this research were funded by a grant from the Multi-disciplinary Association for Psychedelic Studies (MAPS). MAPS had no input or influence on study design or outcomes. Support for Dr. Garcia-Romeu was provided by the NIDA (grant number T32DA07209).