
Abstract
Statins have been shown to decrease depressive symptoms in certain groups of patients, an effect that is mostly attributed to their anti-inflammatory and neurotransmitter modulatory potentials. We aimed to investigate the antidepressant effects of simvastatin as an adjuvant therapy in patients with moderate to severe depression. In this double-blind placebo-controlled clinical trial, 48 patients were randomly allocated to receive simvastatin or placebo as an adjunct to fluoxetine for six weeks. Patients were evaluated with the Hamilton Depression Rating Scale (HDRS) at baseline and weeks 2, 4 and 6. Probable clinical and laboratory adverse events were also monitored and compared between the two groups. Simvastatin-treated patients experienced significantly more reductions in HDRS scores compared to the placebo group by the end of the trial (p=0.02). Early improvement and response rates were significantly greater in the simvastatin group than the placebo group (p=0.02 and p=0.01, respectively) but remission rate was not significantly different between the two groups (p=0.36). No serious adverse event was reported during this trial. In conclusion, simvastatin seems to be a safe and effective adjuvant therapy for patients suffering from major depressive disorder. However, more confirmatory studies are warranted.
Introduction
Major depressive disorder (MDD) is among the key causes of disability in adults worldwide (Kessler et al., 2003). Although there have been considerable advances in the pharmacotherapy of MDD in the last decade, around 30% of patients are refractory to the current antidepressant agents which highlights the need to develop new and more effective medications in this field (McIntyre et al., 2014; Stimpson et al., 2002). Among different strategies to address this issue, antidepressant augmentation with novel classes of medications has gained more popularity in the recent years. Indeed, investigating new compounds with different mechanisms of action is logical in light of various recent findings in pathophysiology of depressive symptoms. Multiple processes such as inflammation, oxidative stress, vascular abnormalities, and complex neurotransmitter interactions have been shown to be involved in the pathophysiology of MDD and thus might be investigated as novel therapeutic targets as well (Abbasi et al., 2012; Thuile et al., 2007).
Statins are a group of drugs which inhibit 3-hydroxy-3-methylglutaryl coenzyme-A (HMG-CoA) reductase, a rate-limiting enzyme in the biosynthesis of cholesterol. Beyond accumulating evidence which support benefits of statin use in cardiovascular diseases, the pleiotropic effects of statins have been also discussed in different fields. There are a growing number of trials showing the benefits of statins in different neuropsychiatric disorders including neurodegenerative and neuro-inflammatory diseases (Corrao et al., 2013; Willey and Elkind, 2010). Experimental studies have shown that statins are able to decrease production of β-amyloid protein in Alzheimer’s disease and improve the overall symptoms of multiple sclerosis (Koh, 2003; McIntyre et al., 2014). These promising effects are thought to be mainly attributed to the immunomodulatory potential of statins, particularly their impact on T lymphocytes and antigen-presenting cells (Stuve et al., 2003). In addition, a remarkable number of animal studies have demonstrated the inhibitory effects of statins on N-methyl-D-aspartate (NMDA) glutamate receptors, a well-known and widely explored therapeutic target in different psychiatric disorders including depression (Dang et al., 2014; Ludka et al., 2013).
The rationale behind the expected effects of statins on depressive symptoms can be justified from different aspects. From a cholesterol-lowering standpoint, the relationship between cholesterol levels and depressive symptoms has been a topic of controversy. Although older studies reported higher rates of depression and suicide in relation to low cholesterol levels (Fiedorowicz et al., 2007), more recent trials, in contrast, have found that cholesterol reducing strategies might be helpful in improving depressive symptoms (Weidner et al., 2009). In one study, high cholesterol levels were associated with higher prevalence of depression in Japanese men (Nakao and Yano, 2004). In another long-term survey of MDD patients, in the Netherlands, abnormal lipid patterns were significantly more common in depressed patients than the control group after adjustment for possible covariates such as body mass index (BMI), smoking, education and other life-style factors (Van Reedt Dortland et al., 2010). In an eight-week trial, high cholesterol levels were associated with significantly greater resistance to treatment with fluoxetine in MDD patients (Sonawalla et al., 2002). In addition to treating dyslipidemia, statins are also potent antioxidant and anti-inflammatory agents as they can reduce levels of C-reactive protein (CRP) and tumor necrosis factor-α (TNF-α) (Berthold-Losleben and Himmerich, 2008; Devaraj et al., 2007). There are several studies implicating inflammatory mechanisms in depression (Zunszain et al., 2013). Alterations in the cytokine system as well as higher levels of interleukin-6 (IL-6), TNF-α, CRP and cortisol have been shown in MDD patients (Karlovic et al., 2012). These data along with the mentioned anti-inflammatory potential of statins further support the probable benefits in treatment of depression.
In line with our hypothesis, some recent studies have yielded promising results regarding the antidepressant effects of statins in certain groups of patients. Stafford et al. investigated the efficacy of statin therapy in improving depression after cardiac intervention and showed significant reduction in depressive symptoms (Stafford and Berk, 2011). In addition, a population-based cohort study of older adults revealed an inverse relation between statin use and depressive symptoms (Feng et al., 2008). Recently, a six-week trial conducted by Ganizadeh and Hedayati (2013) reported that augmentation of fluoxetine with lovastatin in patients with severe MDD significantly reduces depressive symptoms. Inspired by the above-mentioned reasons and studies, the purpose of the present investigation was to assess the efficacy of simvastatin as an adjuvant in treatment of major depression in a six-week, double-blind, placebo-controlled trial. Indeed, simvastatin passes the blood brain barrier better than all other statins currently in use (Vuletic et al., 2006).
Method
Trial design
This trial, with registration number IRCT201205131556N43 at the Iranian Registry of Clinical Trials, was designed as a six-week, parallel-group, double-blind, placebo-controlled, clinical trial in patients suffering from MDD. The study was conducted in compliance with principles of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Tehran University of Medical Sciences (TUMS). All participants in this study provided a written informed consent and were instructed about possible adverse events (AEs) and their right to withdraw anytime during the study without any consequence to their clinical benefits.
Participants
Inclusion criteria
Patients aged 20−70 years, irrespective of their gender who fulfilled the diagnostic criteria of MDD based upon the Diagnostic and statistical manual of mental disorders, Fourth edition, text revision (American Psychiatric Association, 2000) were considered for participation in this study. Inclusion criteria of participants were narrowed to those who scored ⩾22 at the screening visit according to the 17-item Hamilton Depression Rating Scale (HDRS).
Exclusion criteria
Patients who were suffering from any diagnosis other than MDD on the DSM-IV-TR axis I or II were consider ineligible to take part in the trial. Presence of any psychotic features or being on any psychotropic medications could also exclude the subject. Additionally, patients who had received any antidepressant medication in the last month or electroconvulsive therapy (ECT) in the last two months prior to enrollment were considered ineligible to participate. Patients with a serum low-density lipoprotein (LDL) level of <80 mg/dL at baseline were also excluded from the study. Other conditions which were defined as exclusion criteria included: history of hypothyroidism, cardiovascular disorders, hepatic diseases, myopathies, use of any other lipid-lowering agent, hypersensitivity to statins, high levels of liver aminotransferases, any present life-threatening condition or neurological disorder, and pregnancy or breast feeding.
Study setting
This trial was carried out from June 2012−March 2014 in an outpatient setting. The visits and evaluations were all conducted at Roozbeh Hospital and Baharloo Hospital, two large academic centers affiliated with TUMS. In addition to the first baseline/screening visit, participants were evaluated three more times at weeks 2, 4, and 6 as follow-up visits.
Interventions
The trial participants were randomized to receive fluoxetine plus either simvastatin or placebo through the course of this study. Simvastatin (Shahre Darou Co., Tehran, Iran; 20 mg tablets) was administered with a fixed dose of 20 mg/day (one tablet) in this trial. All patients received 20 mg/day of fluoxetine (Jalinous Co., Tehran, Iran; 20 mg capsules) for the first two weeks followed by 40 mg/day (two capsules) for the subsequent four weeks of the study. Patients were not allowed to take any other antidepressant or lipid-lowering agent, or any form of behavioral or diet therapy, during the course of this trial. Medication adherence was measured using weekly tablets counts justified against participant reports of medication intake to calculate the proportion of dispensed medication doses that were actually ingested.
Outcomes
The primary outcome measure was HDRS score change from baseline to week 6 in the simvastatin versus the placebo group. This scale refers to a widely used measure which includes seventeen three-point and five-point questions addressing the severity of depressive symptoms. This scale has been applied in many clinical trials in Iran exploring depression therapeutic strategies (Akhondzadeh et al., 2009; Khajavi et al., 2012; Sepanjnia et al., 2012; Shahmansouri et al., 2013). In addition to primary scoring prior to initiation of medications at the baseline visit, all participants were evaluated by HDRS at weeks 2, 4 and 6. Two psychiatrists with previous experience in this field conducted all assessments and the inter-rater reliability between the two raters was >90%. The primary outcome of this trial was defined as the difference between the two study groups (simvastatin vs placebo) regarding of HDRS scores change from baseline (week 0) to the study endpoint (week 6). Early improvement (⩾20% reduction in HDRS score by the end of the second week), response rate (⩾50% decrease in the HDRS score), and remission rate (HDRS score ⩽7) were also compared between the two groups (Frank et al., 1991; Szegedi et al., 2009).
Safety
Before starting the trial, all participants were notified regarding the possibility of AEs during this study and were asked to inform the research team about any change in their health status. Patients were visited in person, at weeks 2, 4, and 6, and given thorough physical examinations and were also questioned about probable AEs through a 25-item checklist covering a broad range of somatic symptoms. In addition, all participants were asked about any unexpected symptom just one week after start of medications by a phone call. A rater, different from those scoring the HDRS scale, was in charge of performing the safety assessments. Furthermore, laboratory parameters including total serum cholesterol, LDL, high-density lipoprotein (HDL), triglyceride, aspartate transaminase (AST), and alanine transaminase (ALT) were measured at baseline (week 0) and endpoint (week 6) in order to detect any change.
Randomization
Generation of randomization code was performed by the permuted randomization block method using Excel software by an independent party (allocation ratio 1:1, blocks of four).
This procedure was handled with the aid of Microsoft Excel software. A computer-generated code was allocated to each patient and the person who ran the randomization was not involved elsewhere in the project. Assignments were kept in sequentially numbered, sealed, opaque envelopes and were opened sequentially only after participant details were written on the envelope.
Blinding
All investigators were provided with drugs in sealed envelopes on which randomization codes were written. The selected placebo was identical to simvastatin in shape, size, texture, color, and smell. The study drugs were dispensed by an investigational drug pharmacist and all members of the research team as well as the patients and their family were blind to the treatment group assignments. At the end of the study, we asked patients and raters whether they thought they were in the active treatment or the placebo group.
Sample size and statistical methods
Based upon previous trials, the sample size was calculated with the following assumptions: given the lowest detectable score difference of 3.5 on the HDRS with a standard deviation (SD) of 3.5, a power of 90%, a two-sided significance level of 5%, and an attrition rate of 20%, a total sample size of 48 was calculated. In order to analyze the data, we took advantage of IBM SPSS 20 software. Continuous variables were described as mean (SD), while categorical ones were reported as number with percent in each group. General linear model repeated measures was our main analysis to detect the effect of time × treatment interaction in which the placebo vs. simvastatin group was considered as the between-subject factor and HDRS score at the four study time-points (weeks 0, 2, 4, and 6) as the within-subject factor. Whenever Mauchly’s test of sphericity was significant, Greenhouse-Geisser correction was used. Independent sample t-test was also used to compare the HDRS score changes from baseline to each of the study time-points between two groups. The frequency of AEs as well as early improvement, response, and remission rates were compared between the two trial groups using the chi-square test. In all steps, statistical significance was defined as a p value of <0.05.
Results
Participants
As illustrated in Figure 1, 65 patients were screened for the eligibility criteria and a total number of 44 patients (simvastatin=22, placebo=22) completed the trial. No significant difference was detected between the two groups in the basic characteristics of the participants as summarized in Table 1. Similarly, baseline HDRS scores were not significantly different between the two groups (MD (95% CI)=1.45 (1.33−4.44), t(42)=1.05, p=0.29).
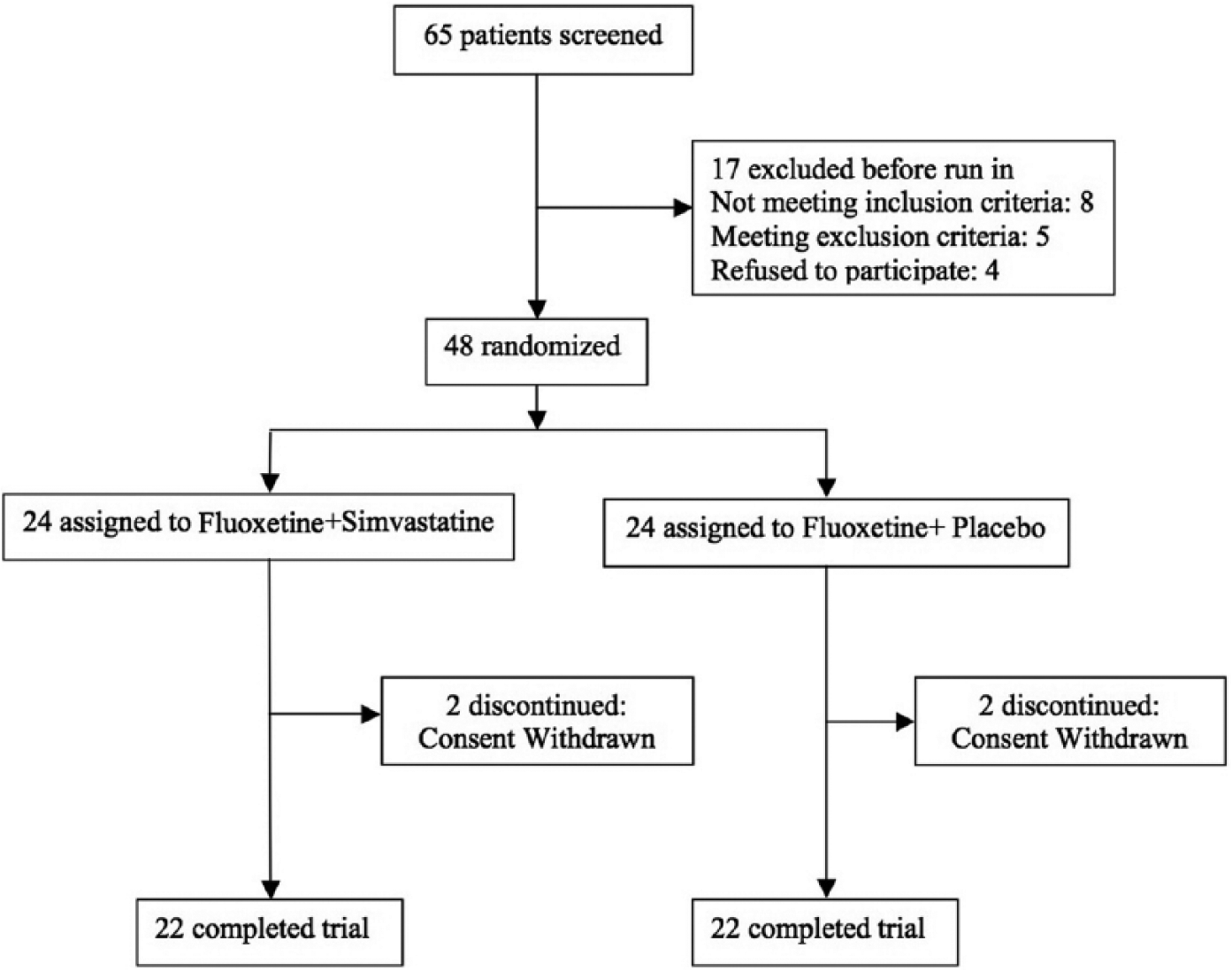
Flow diagram of the trial.
Baseline characteristics of the participants.
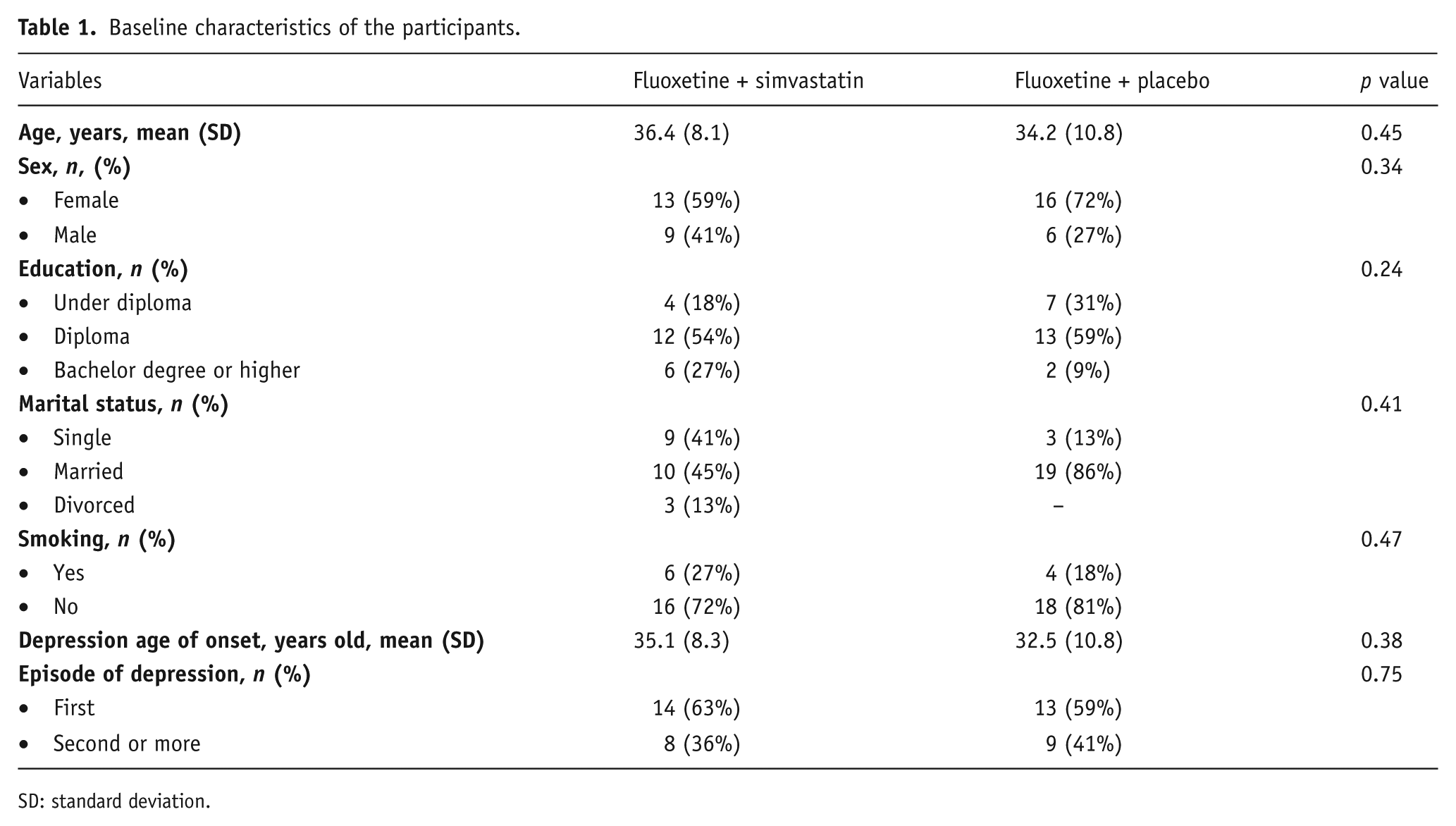
SD: standard deviation.
Outcomes
A significant effect was detected for time×treatment interaction (F(1.88,78.94)=3.78, p=0.02) in HDRS scores indicating a significant difference in behavior of the two groups throughout this study (Figure 2) (Cohen’s d at week 6: 0.61). Analyzing with the independent t-test, the difference between the two groups in HDRS score reduction from baseline was also significant by the end of weeks 2, 4, and 6 (Table 2). Early improvement was detected in 81.8% of patients in the simvastatin group, while 50% of patients in the placebo group showed such improvement (p=0.02). At the end of this trial, 90% of patients in the simvastatin group and 59% of patients in the placebo group experienced a response to treatment, a difference which was statistically significant (p=0.01). However, remission rate in the simvastatin and placebo groups were 59% and 45% respectively, and the difference between the two groups was not statistically significant (p=0.36).
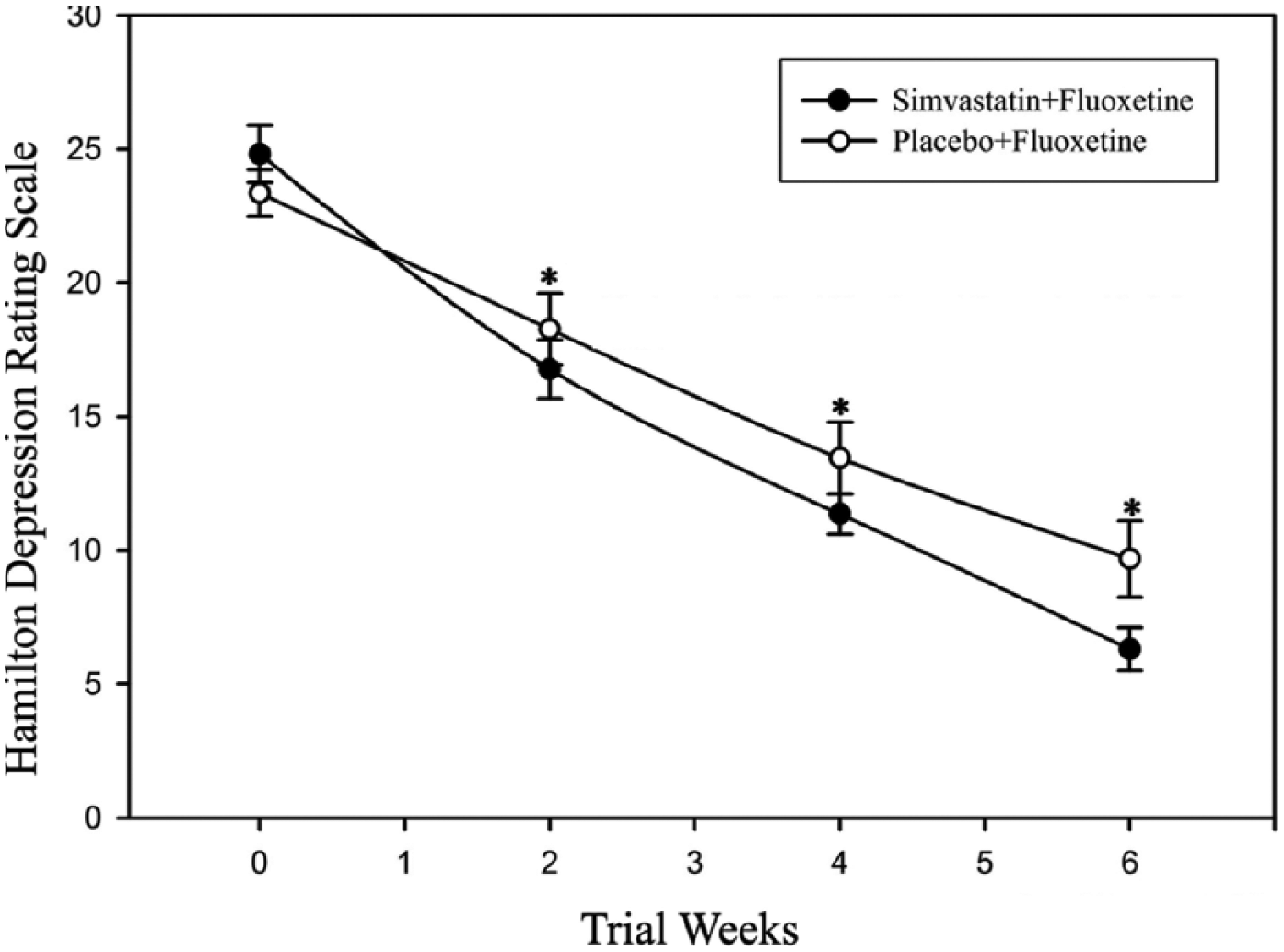
Comparing the mean±standard error (SE) of Hamilton Depression Rating Scale scores between two study arms at each time-point, *p value<0.05.
Hamilton Depression Rating Scale (HDRS) score reduction from baseline to each time-point.
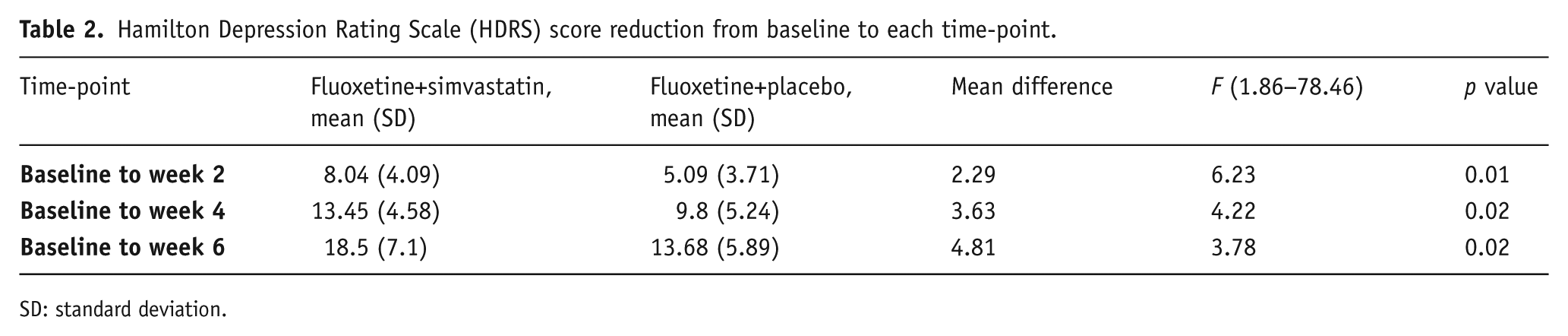
SD: standard deviation.
Adverse events
A total number of nine AEs were reported in patients during this trial based on the checklist, including myalgia, increased appetite, decreased appetite, nausea, vomiting, headache, constipation, insomnia, and abdominal pain. No significant difference was detected between simvastatin and placebo groups in any of the AEs. No serious or life-threatening event occurred in this study. The laboratory values were not significantly different between the two groups at the beginning of the trial. No significant change was reported during the course of the study in this regard as well (Table 3).
Laboratory tests at baseline and the trial endpoint.
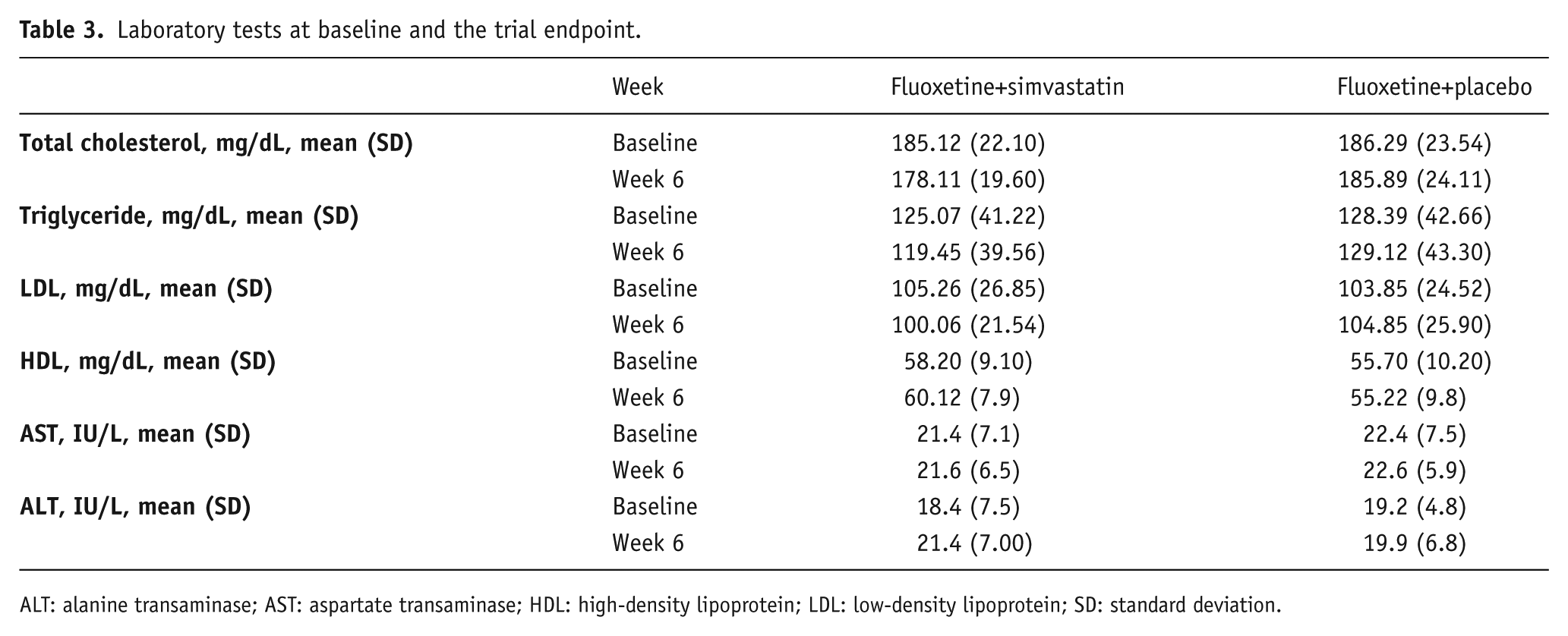
ALT: alanine transaminase; AST: aspartate transaminase; HDL: high-density lipoprotein; LDL: low-density lipoprotein; SD: standard deviation.
Discussion
During the course of this trial, patients who took simvastatin as an augmentative therapy to fluoxetine showed significantly greater improvement in depressive symptoms than the placebo group. Significant reduction in depressive symptoms was also achieved by weeks 2 and 4, suggesting a probable fast-acting property for simvastatin in antidepressant regimen augmentation. Treatment parameters such as early improvement, response to treatment, and remission are considered as important measures of efficacy in clinical trials. In the current study, simvastatin-treated patients improved significantly earlier than the placebo group. According to studies with longer follow-up periods, early improvement is positively associated with higher rates of stable remission and response after ten weeks (Tadic et al., 2010). This trial showed the same pattern because the response rate was significantly higher in the simvastatin group than the placebo group by the endpoint. In terms of remission rates, 59% of participants in the simvastatin arm experienced remission in this trial, but this was not significantly different from the placebo group. This finding may be due, in part, to the short follow-up period in this study. However, more studies with longer follow-up periods are needed to unmask different aspects of simvastatin therapy in patients with MDD.
There exists relative inconsistency in the literature on the effects of statins on depressive symptoms. On the one hand, some trials failed to show any significant antidepressant effect for statins. In the Long-term Intervention with Pravastatin in Ischemic Disease (LIPID) study, the impact of pravastatin was investigated on depression, anxiety, impulsiveness, and anger in 1222 stable cardiovascular patients (Stewart et al., 2000). Although the outcomes rejected any negative effect on mental health for pravastatin, no significant positive results were reported in patients treated with pravastatin. In another clinical trial assessing the effects of lovastatin on psychosocial well-being parameters in patients with hyperlipidemia, the difference between two groups was not significant and lovastatin failed to show any positive or negative effect on depressive symptoms (Muldoon et al., 2000). In spite of appropriate sample size and extended follow-up time, both studies were conducted in only cardiovascular and hyperlipidemic patients, making it hard to generalize the results to all patients suffering from MDD. On the other hand, and in line with our hypothesis, a cohort study in a large number of patients with coronary artery disease showed that statin use was associated with 38% decrease in incidence of depression after six years of follow-up (Otte et al., 2012). In another trial, statins were administered to individuals after discharge from cardiac service and patients were followed for nine months to observe development of new depressive symptoms. Surprisingly, a 79% decrease in likelihood of depression occurrence was reported in that study (Stafford and Berk, 2011). In a recent clinical trial, lovastatin added to fluoxetine showed to be effective in reducing depressive symptoms in just two weeks after administration (Ghanizadeh and Hedayati, 2013). This fact coupled with the results of our trial may support the claim that adjuvant therapy with statins might decrease the lag-time in treatment with antidepressants.
The exact mechanisms of action through which statins exert antidepressant properties are not completely understood. Dysregulation in glutamate balance and subsequent glutamate-induced excitotoxicity is thought to play a key role in the pathophysiology of depression (Sanacora et al., 2012). Interestingly, it has been shown that statins are able to increase glutamate uptake in different brain regions (Tramontina et al., 2011). In addition, in vitro studies have demonstrated that statins could protect neurons from the glutamate-induced increase of intracellular calcium (Domoki et al., 2010) and this effect is independent of HMG-CoA enzyme inhibition (Bosel et al., 2005). There is a growing body of evidence introducing a central role for NMDA receptors, as a subtype of glutamate receptors, in pathophysiology and treatment of depression (Dang et al., 2014). NMDA antagonism (e.g. ketamine) is a promising strategy to achieve rapid antidepressant effects (Li et al., 2010). Interestingly, simvastatin and other statin analogues were found to prevent NMDA-induced cell death in brain neurons and retinal ganglion cells (Nakazawa et al., 2007; Ponce et al., 2008), a mechanism that might justify the rapid antidepressant effects of simvastatin in the present study. In addition to neurotransmitter pathways, statins might modulate some of the vital neurotrophic factors. Fabiana et al. reported decreased expression of brain-derived neurotrophic factor (BDNF) in hippocampal neurons of mice after acute treatment with atorvastatin (Ludka et al., 2013). Alterations in BDNF levels have been reported in patients with MDD (Lee et al., 2007) and monitoring of this factor has been suggested to be used as a marker of response to antidepressant treatment (Martinowich et al., 2007).
The present study had different limitations which should be considered. Given the long-term nature of depressive symptoms and high rate of relapse, the short course of follow-up in this study may decrease the value of our results for estimating the long-term impact of simvastatin on depression. In addition, our relatively small sample size did not allow separate data analysis based on different patient characteristics such as severity of depression. More studies are warranted to specifically address simvastatin safety and its probable AEs in long-term use in patients with moderate to severe major depression.
In conclusion, simvastatin was significantly more efficient than placebo in terms of overall antidepressant effects and lag-time reduction in response to fluoxetine in the present trial. Further studies with longer follow-up and larger sample size are warranted to reveal the exact antidepressant properties of simvastatin in patients suffering from MDD.
Footnotes
Acknowledgements
This study was based on the Medical Doctor (MD) thesis of Nahid Zareh-Mohammadi and Samira Raheb under supervision of Shahin Akhondzadeh for MD degree.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Tehran University of Medical Sciences (grant no: 17218) to Shahin Akhondzadeh.