
Abstract
The relationships between serotonin and fear and anxiety disorders have been much studied yet many important questions remain, despite selective serotonin reuptake inhibitors having been the primary treatments for these disorders for some time. In order to explore this issue we performed a pooled analysis of six of our studies in remitted patients with a fear/anxiety disorder who were exposed to syndrome-specific aversive stimulation under acute tryptophan depletion. We based our analysis on the hypothesis that the inconsistencies observed in the studies could be predicted by Deakin and Graeff’s theory about the dual role of serotonin in responses to threats, whereby serotonin is critical to prevent fear (panic) but not anxiety. In accordance with this view, our results give support to a dissociation of the disorders traditionally grouped under fear and anxiety-related disorders in terms of different roles of serotonin in modulation of responses to aversive stimulation. Implications for future studies and psychiatric nosology are discussed.
Introduction
The conceptualization of the boundaries of anxiety disorders is an ongoing issue that is yet to be resolved (Starcevic, 2014). In DSM-5, fear and anxiety disorders have been separated for the first time, with panic disorder and generalized anxiety disorder (GAD) in separate groups. Also, posttraumatic stress disorder (PTSD) and obsessive–compulsive disorder (OCD) have been removed from the anxiety disorders group. Moreover, the ICD11 draft document refers to “anxiety and fear-related disorders”, which suggests different, but related conditions (Starcevic, 2014). In spite of a clear current demand for pathophysiological-based psychiatric nosology (Insel, 2014; Insel et al., 2010; Sanislow et al., 2010), none of the major re-conceptualizations have enough neurobiological support.
One approach to this issue is to explore the neurochemical basis of each disorder to look for patterns of similarity and difference. Serotonin (5HT) has long been implicated in the modulation of aversive stimulation as well as anxiety and stress-related psychiatric disorders. One hypothesis is that 5HT acts in these disorders through modulation of stress (Davidson et al., 2005). Increased synaptic levels of 5HT may have a crucial role in this process (Charney, 2004). Animal models consistently give support to this view by demonstrating that brain 5HT systems are critically involved in the response to stressors as well as in fear and anxiety generation (Deakin, 2013; Deakin and Graeff, 1991).
In humans, most anxiety and fear disorders respond to some extent to drugs that increase 5HT function, and the selective serotonin reuptake inhibitors (SSRIs) are now generally accepted as the first-line pharmacological treatments for these (Baldwin et al., 2014). However, it is not clear if they work through the same mechanisms in each disorder. One approach to explore this issue is to use the acute tryptophan depletion (aTD) technique to transiently lower brain 5HT and see what effect this has on the disorder (Hood et al., 2005). Previous studies have reported that aTD undermines the therapeutic effect of SSRIs in depression (Delgado et al., 1990), and increases depressive symptoms (Smith et al., 1997) and stress responses in drug-free recovered patients (Harmer et al., 2003). On the other hand, aTD alone seems to be insufficient to cause spontaneous relapse in fear/anxiety disorders such as panic disorder (Goddard et al., 1994) and OCD (Kulz et al., 2008; Smeraldi et al., 1996), but has been shown to reverse the effects of SSRIs and so lead to transient relapse in some people under fear/anxiety provocation challenges in panic disorder (Bell et al., 2002), social anxiety disorder (SAnD) (Argyropoulos et al., 2004) and PTSD (Corchs et al., 2009). This effect was also observed to some extent in panic disorder treated with cognitive-behavior therapy (CBT) (Bell et al., 2011). On the other hand, no effect of aTD was observed in subjective or physiological measures in 5HT antidepressants-remitted GAD (Hood et al., 2010) and OCD (Hood, 2010).
The causes of this variation in the effects of aTD are still unknown. It is, however, consistent with an existing, well-supported theory (Deakin, 2013; Deakin and Graeff, 1991) which proposes that 5HT may have an apparently paradoxical dual role in aversive contingencies. Although it can inhibit periaqueductal gray matter (PAG)-mediated fight/flight responses from threats, 5HT can also facilitate amygdala-mediated anxiety responses. This latter mechanism has been demonstrated both in animals (Deakin, 2013; Deakin and Graeff, 1991) and humans (Blanchard et al., 2001; Feinstein et al., 2013; Mobbs et al., 2007). These different mechanisms may explain, at least in part, the different types of emotions (Mobbs et al., 2007) and fear/anxiety disorders (Deakin and Graeff, 1991; Gray and Mcnaughton, 2000) seen in humans. Reactions to imminent, PAG-mediated threats relate to the emotion named “fear” and, as proposed earlier (Gray and Mcnaughton, 2000; Mcnaughton and Corr, 2004), may be more closely related with phobic, escape-dominant behavioral syndromes, such as specific phobias, SAnD, and panic. Potential, amygdala-mediated threats seem to be linked to the emotion named “anxiety” and related disorders, such as GAD and OCD (Gray and Mcnaughton, 2000; Mcnaughton and Corr, 2004). PTSD was not initially included in these clusterings and, actually, may have a more complex categorization. However, the onset of PTSD is driven by the fearful memory of harm or threat of harm, and there is strong neurobiological evidence for the inclusion of PTSD, together with panic disorder, social phobia and specific phobias, in a cluster of disorders characterized by the major involvement of brain “fear circuitry”, related to the responses to threats or fearful stimuli (Andrews, 2009; Friedman et al., 2011), which was one of the many reasons to exclude PTSD from the anxiety disorders in the DSM-5. For these reasons, we included PTSD in the fear-related disorders group.
The aTD plus challenge studies quoted above focused on each disorder specifically by measuring their specific symptoms. In the present study we focus on the category of responses to aversive stimuli rather than specific symptoms, in a pooled sample. Our main hypothesis is that differences in challenge-provoked responses under aTD and non-depleted conditions can be explained in terms of the cluster of fear versus anxiety-related conditions.
Methods
Participants
Data from 66 subjects from six different studies were included in the analysis (see Table 1). The sample was divided based on the hypothesis: fear disorders (PTSD, panic disorder and SAnD; n = 47); and anxiety disorders (GAD and OCD; n = 19). According to this grouping, the sample has the characteristics described in Table 2. In all studies, diagnoses were based on the Mini-International Neuropsychiatric Interview (MINI) (Sheehan et al., 1998) and remission was considered if the subject had “good improvement” or “very good improvement” (scores 2 or 1) on the clinical global impression improvement scale (CGI-I) (Guy, 1976) for at least 3 months before the tests.
Summary of participant and study details included in the pooled analysis presented here.
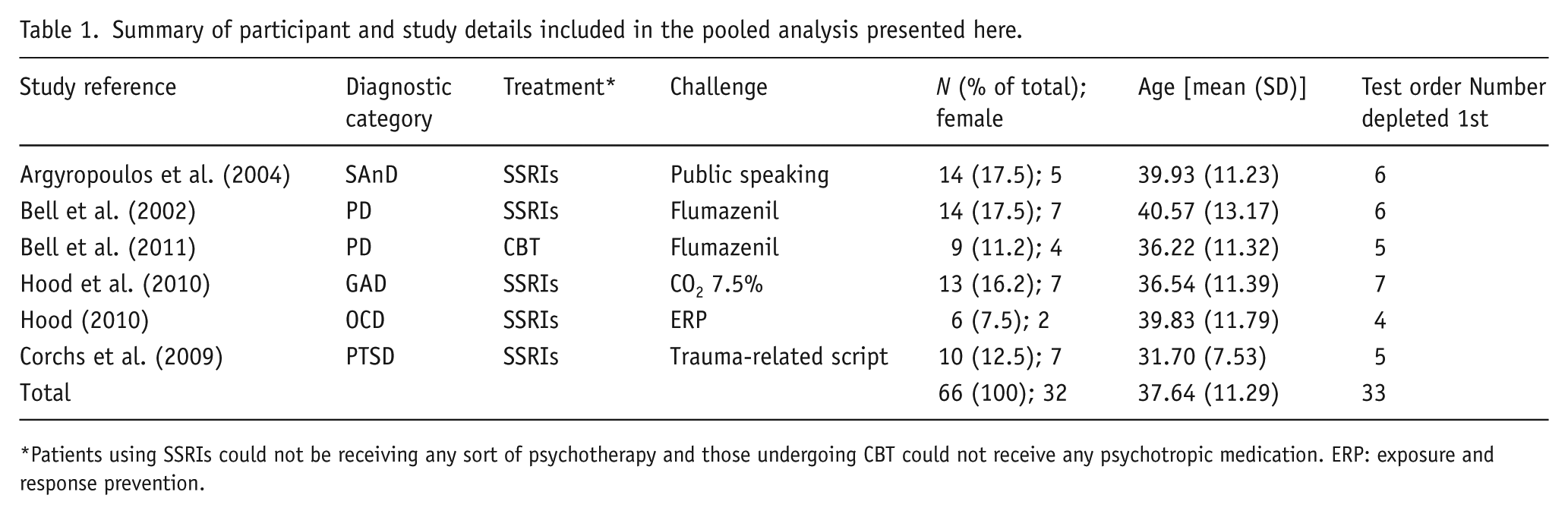
Patients using SSRIs could not be receiving any sort of psychotherapy and those undergoing CBT could not receive any psychotropic medication. ERP: exposure and response prevention.
Demographic and baseline data for fear and anxiety disorder groups.
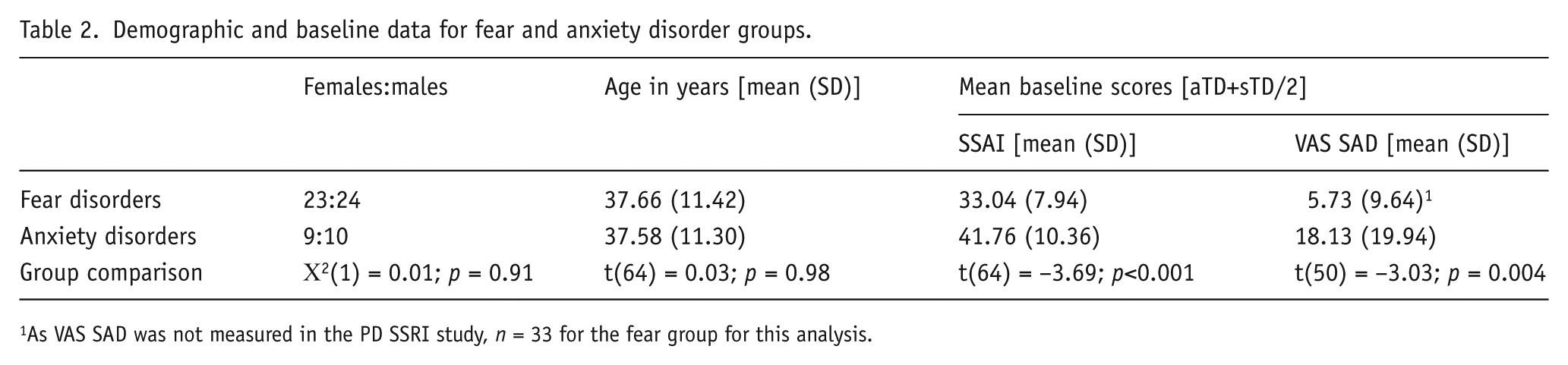
As VAS SAD was not measured in the PD SSRI study, n = 33 for the fear group for this analysis.
In all studies, patients were excluded if they had active major depressive disorder, alcohol or substance use disorder, bipolar or a primary psychotic disorder, or any physical condition that could make tests biased or risky to the patient. Each study was approved by the research ethics committee of the site where it took place. Two of the authors of this paper (SDH, DJN) were also authors of all of the studies pooled.
Tryptophan depletion procedure
The experimental phase of the studies was designed in a double-blind, placebo-controlled crossover fashion. Following a standard procedure (Young et al., 1985) subjects took part in two similar test days, 1 week apart, in which they consumed a 100 g mixture containing 15 large neutral amino acids. This drink contained 2.3 g of tryptophan on the sham tryptophan depletion (sTD) day and not on the acute tryptophan depletion (aTD) day. The presence or absence of tryptophan in the amino acid formula ingested was the only programmed difference between test days. This determined acute tryptophan depletion effect (aTD day), with the sTD day acting as a control condition to allow comparison with acute tryptophan depletion. Subjects were instructed to have a low tryptophan diet the day before each test and fast from midnight, as well as to take all medications they might be using as usual on the test days. The order of aTD and sTD condition was random and counterbalanced within each study, and presented in a double-blind fashion. Female subjects took only 80% of the total amount because of their lower body weight. Further details about experimental procedures can be found in the original papers and in Hood et al. (2005).
Aversive exposure challenge
Each study involved a specific challenge that represented a well-established symptom provocation procedure, related to the anxiety disorder under study (Table 1).
Challenges were performed between 4.5 and 7 h after the drink, as this was estimated to be the peak time of aTD that could be managed within the daily protocol of each study.
Psychological measures
As the aTD effects could have become obvious to the examiner during the tests, the psychological effects of these procedures were measured exclusively by self-rating scales.
During testing, the main assessment was of anxiety, measured by the Spielberger State Anxiety Inventory (SSAI) (Spielberger et al., 1970). Mood was assessed by a visual analog scale (VAS) anchored to the term “sad” that followed standard practice for theses scales (Bond and Lader, 1974). Subjects from the SSRI-remitted panic disorder study (Bell et al., 2002) were not assessed for mood using the same instrument (VAS) so could not be included in the overall mood analysis.
These instruments were applied at baseline (before ingestion of the amino acid formula), immediately before the challenges, and during/immediately after the challenge, when subjects were given the rating scales and instructed to fill them in to reflect the peak intensity of symptoms they felt during the challenge. The Beck Depression Inventory and the Spielberger Trait Anxiety Inventory (Spielberger et al., 1970) were applied only at baseline.
Cardiovascular measures
Cardiovascular data (n fear:anxiety groups = total; systolic blood pressure (SBP) 36:19 = 55, diastolic blood pressure (DBP) 31:19 = 50, heart rate (HR) 37:19 = 56) were obtained and analyzed here. Missing data were due to random recording failure.
Blood pressure was measured 1–2 min after the stress test (time of peak subjective anxiety) and was compared with that immediately before the stress test. Further details on the methods of SBP ascertainment can be obtained in our earlier publication which included patients with panic disorder and SAnD (Davies et al., 2006).
Plasma tryptophan levels
Blood samples for the measurement of total tryptophan were taken before the amino acid drink and after the challenge, but before re-feeding. Three subjects from the GAD study did not have plasma tryptophan data at the time this paper was prepared and were not included in the analysis.
Statistical analysis
The main analysis used a repeated measures analysis of variance (ANOVA; sphericity assumed) with depletion condition (sTD vs. aTD) and time (baseline, pre-challenge and peak post-challenge) as within-subjects factors. Disorder group (fear vs. anxiety disorders) and the depletion order were included as between-subjects variables. In order to be conservative with the analysis, although the pair-wise comparisons made were planned a priori, we used Bonferroni corrected pair-wise t-tests to assess differences of importance to the hypothesis following significant or trend significant interactions. All tests were 2-tailed with alpha = 5% and beta = 20%. We used the statistical package SPSS v. 22 (SPSS Inc, Chicago, IL).
Results
Plasma tryptophan levels
Analysis of total plasma tryptophan levels revealed a main effect of depletion condition (F(1,58) = 148.4; p < 0.001), and a significant depletion condition by time interaction (F(1,58) = 173.6; p < 0.001). Tryptophan levels did not differ at baseline, that is, prior to the drink (mean difference = 0.19, 95% CI –1.96–6.50, p = 0.74) but were significantly lower at peak time of depletion in the aTD compared with the sTD condition (mean difference = 20.0, 95% CI 17.1–23.0, p < 0.001). As shown in Table 3, tryptophan levels decreased across the depletion condition (79.7% reduction) but increased on the sham depletion day (99.9% increase). Disorder group did not significantly interact with the within-subjects effects (p > 0.05). Order of depletion, however, was involved in a significant interaction with depletion condition and time (F(1,58) = 4.158, p = 0.046). This was a consequence of mean tryptophan level under the sTD condition being 5.7 µg/mL lower (95% CI 0.03–11.5, p = 0.049) at peak time in the group depleted on day 2 compared with those depleted on day 1, although the results were in the same direction for both depletion orders. Mean tryptophan levels were not different between the two orders of depletion at any other time point under either aTD or sTD conditions (all p > 0.68).
Effects of tryptophan (TRP)-depleted and control mixtures on plasma total tryptophan.

Values of plasma are means (SD) in µg/mL.
Obs: N=62.
Psychological ratings
Spielberger State Anxiety Inventory
The mean SSAI scores for the anxiety and fear disorder groups under sTD and aTD conditions are displayed in Figure 1. Repeated measures ANOVA revealed a near significant depletion by time by disorder group interaction (F(2,124) = 2.95, p = 0.056), a significant depletion by disorder group interaction (F(1,62) = 7.35, p = 0.009), and a main effect of time (F(2,124) = 46.21, p < 0.001), depletion (F(1,62) = 7.88, p = 0.007) and disorder group (F(1,62) = 18.69, p < 0.001). Depletion order did not reach significance as a main effect or in any interaction in this analysis (all p > 0.179). To explore the source of the three-way interaction, both disorder groups were subjected to repeated measures ANOVA separately. The fear group displayed a significant depletion condition by time interaction (F(2,90) = 7.35, p = 0.001) with significantly higher SSAI scores observed in the aTD condition at pre-challenge (mean difference = 3.89, 95% CI 1.28–6.50, p = 0.004) and challenge (mean difference = 8.77, 95% CI 4.77–12.76, p < 0.001), but not at baseline (p = 0.47; see Figure 1). In the anxiety group, both the depletion condition by time interaction (F(2,34) = 0.53, p = 0.66) and the main effect of depletion condition (F(1,17) = 0.007, p = 0.93) were not significant.
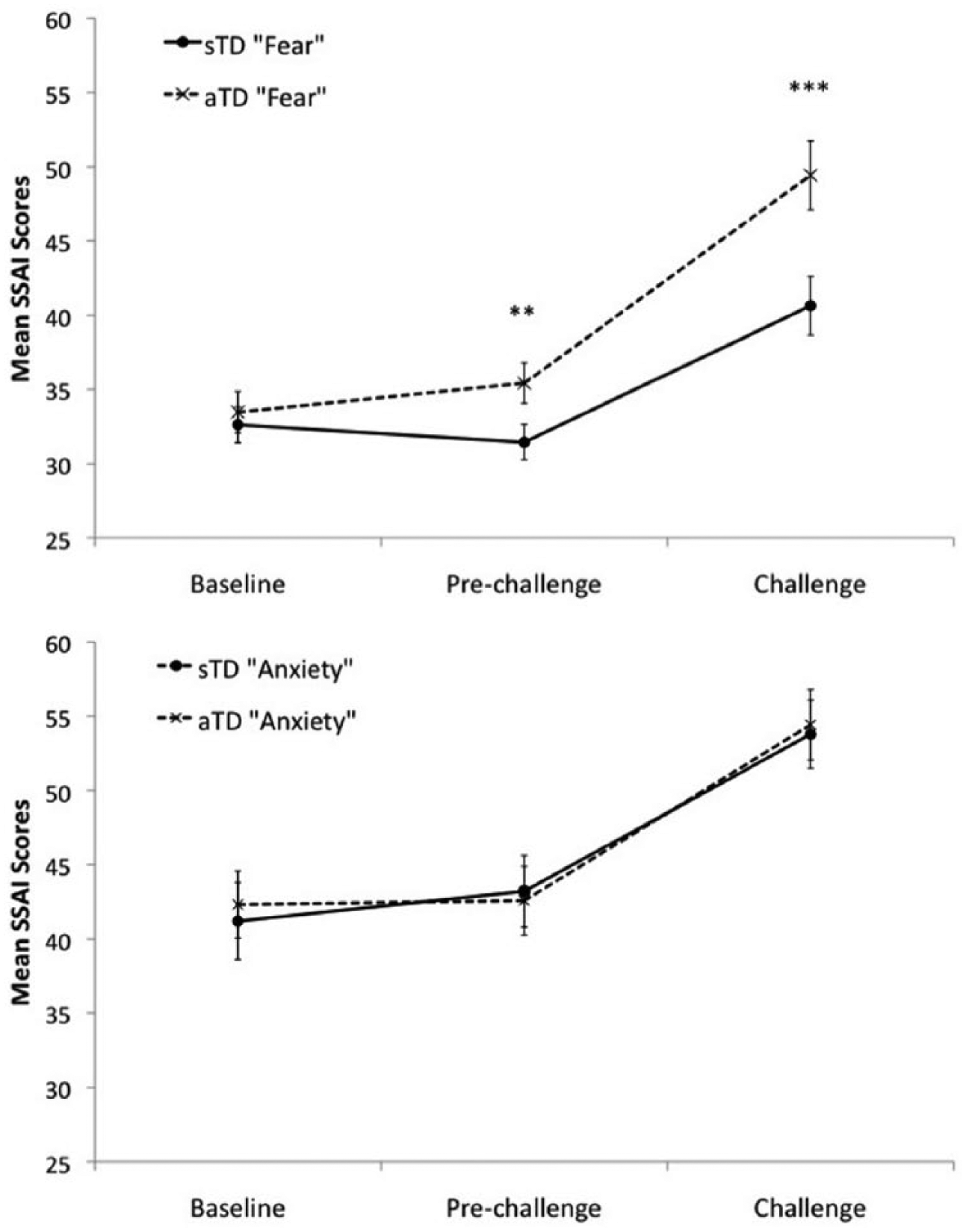
Mean Spielberger State Anxiety Inventory (SSAI) scores on the acute tryptophan depletion (aTD) and sham depletion (sTD) days (top: fear disorders; bottom: anxiety disorders. **p < 0.01; ***p < 0.001). Error bars represent the standard error of the mean.
VAS SAD
The mean VAS SAD scores for the anxiety and fear disorder groups under sTD and aTD conditions are displayed in Figure 2. This measure was not recorded for the panic disorder SSRI study, therefore n = 33 for the fear group in this analysis. Repeated measures ANOVA revealed a significant depletion by time by disorder group interaction (F(2,96) = 6.08, p = 0.003), a significant time by disorder group interaction (F(2,96) = 6.70, p = 0.002), a significant depletion condition by time interaction (F(2,96) = 4.31, p = 0.02), a main effect of time (F(2,96) = 9.35, p < 0.001), and a main effect of depletion condition (F(1,48) = 5.11, p = 0.028). Depletion order did not reach significance as a main effect or in any interaction in this analysis (all p > 0.217). To explore the source of the three-way interaction, both disorder groups were subjected to repeated measures ANOVA separately. The fear group displayed a significant depletion condition by time interaction (F(2,62) = 8.95, p < 0.001) with significantly higher VAS SAD ratings observed under the aTD condition following the challenge (mean difference = 14.05, 95% CI 4.55–23.55, p = 0.005), but no difference noted at baseline (p = 0.16) or pre-challenge time points (p = 0.68, see Figure 2). A significant depletion by time interaction was also revealed for the anxiety group (F(2,34) = 2.81, p = 0.039). Pair-wise comparisons revealed significantly greater mean VAS SAD scores on the aTD day compared with nTD at only the pre-challenge time point (mean difference = 5.74, 95% CI 0.88–10.61, p = 0.023).
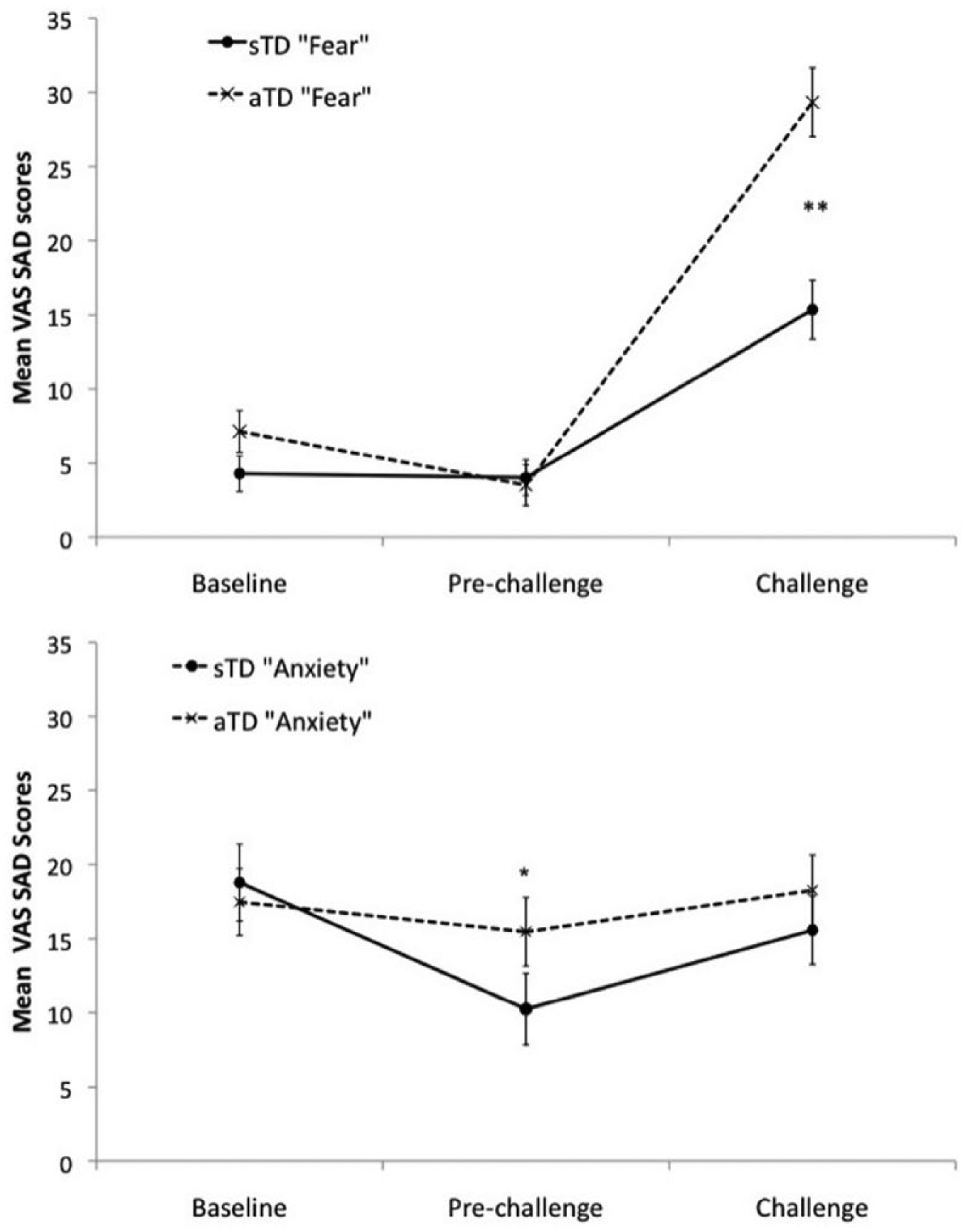
Mean visual analog scale scores anchored to the term “sad” (VAS SAD) I on the acute tryptophan depletion (aTD) and sham depletion (sTD) days (top: fear disorders; bottom: anxiety disorders. *p < 0.05, **p < 0.01). Error bars represent the standard error of the mean.
Cardiovascular measures
Two CBT participants with panic disorder had no cardiovascular data recorded. Heart rate and blood pressure data were not available pre-challenge on either sTD or aTD days for eight participants with social anxiety. Both SBP and DBP were not available on the sTD day at challenge for one PTSD participant, and DBP was not available at challenge on the aTD day for another PTSD participant. DBP was also not available at baseline or pre-challenge on the aTD day for a further four SAnD participants. Therefore, the following analyses are based on n = 36 (SBP), n = 31(DBP) and n = 37 (HR) for the fear group. No data were missing in the anxiety group. Supplementary analyses which included only baseline and challenge time points, thereby including the eight SAnD participants without pre-challenge scores, returned similar results to that reported below (data not shown).
Blood pressure
Mean SBP (mmHg) and DBP (mmHg) for the anxiety and fear disorder groups under sTD and aTD conditions are displayed in Figure 3. For SBP, although inspection of Figure 3 suggests that the fear disorder group under the sTD condition is the only disorder group/depletion condition combination not to show an increase in SBP following challenge, the repeated measures ANOVA failed to find the three-way interaction significant (p = 0.159). ANOVA did reveal a significant effect of time (F(2,102) = 9.32, p < 0.001), reflecting the significantly lower SBP pre-challenge in comparison with baseline (mean difference = 5.4, 95% CI 1.89–8.86, p = 0.001) and challenge (mean difference = 8.42, 95% CI 2.92–13.91, p = 0.001) when the means were collapsed across all other conditions (see Figure 3). ANOVA also returned a significant disorder group by depletion condition interaction (F(1,51) = 10.73, p = 0.002), because when collapsed across time, SBP was significantly lower under aTD in the anxiety group (mean difference = 6.04, 95% CI 1.53–10.55, p = 0.010), but the 3 mmHg mean increase in SBP under aTD condition in the fear group was not significant (p = 0.067).
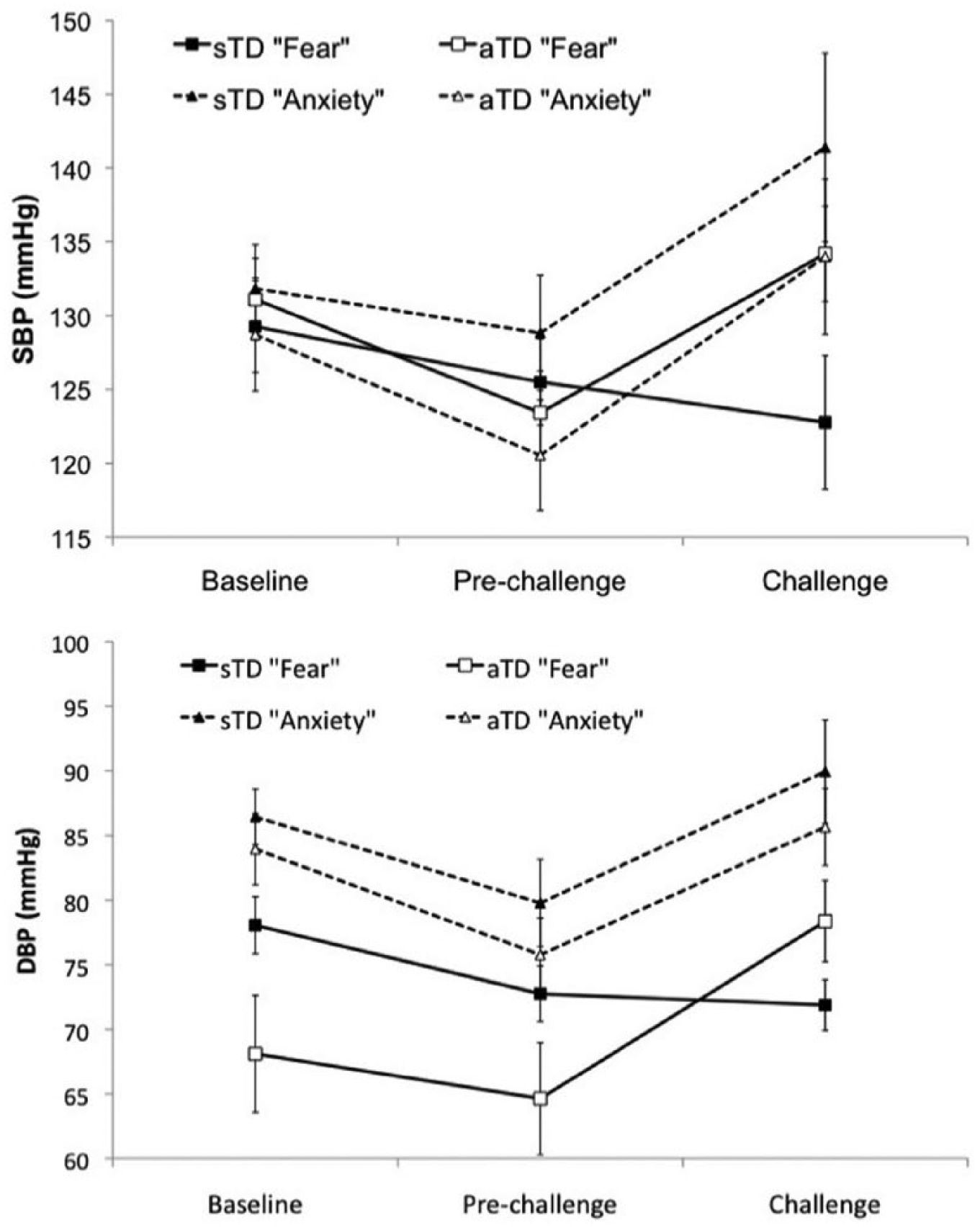
Mean systolic blood pressure (SBP; top) and diastolic blood pressure (DBP, bottom) on the acute tryptophan depletion (aTD) and sham depletion (sTD) days for the fear and anxiety disorder groups. Error bars represent the standard error of the mean.
Order of depletion did impact on the results for SBP. The depletion condition by depletion order interaction (F(1,51) = 5.41, p = 0.024) reflected the lack of depletion effect for those depleted on the first day (mean difference = 1.70, 95% CI –2.01–5.41) in comparison with higher SBP when not depleted for those depleted on the second test day (mean difference = 4.73, 95% CI 0.61–8.85, p = 0.025). In addition, ANOVA also found a significant disorder group by depletion order interaction (F(1,51) = 5.31, p = 0.025). When collapsed across all other factors, SBP in the anxiety group was substantially lower in those depleted on the second day, but not significantly so (mean difference = 9.19, 95% CI –3.96–22.33, p = 0.167). However, for the fear group, SBP was almost significantly higher in those participants depleted on the second day (mean difference = 9.38, 95% CI –0.05–18.81, p = 0.051).
For DBP, the pattern of means was very similar to that observed for SBP. Repeated measures ANOVA revealed a significant main effect of time (F(2,92) = 12.03, p < 0.001) and disorder group by depletion condition interaction (F(1,46) = 9.86, p = 0.003). Again, inspection of Figure 3 suggests that the fear disorder group under the sTD condition is the only disorder group/depletion condition combination not to show an increase in SBP following challenge, but the repeated measures ANOVA failed to find the three-way interaction significant (p = 0.182). The disorder group by time interaction (F(2,92) = 3.23, p = 0.044) reflected the observation at DBP was significantly higher in the anxiety group compared with the fear group at baseline (mean difference = 7.54, 95% CI 1.95–13.13, p = 0.009), and challenge (mean difference = 11.88, 95% CI 4.07–19.68, p = 0.004) but not at pre-challenge (p = 0.106). ANOVA for DBP also found a main effect of disorder group (F(1,46) = 7.77, p = 0.008).
ANOVA also found a significant disorder group by depletion order interaction (F(1,46) = 5.06, p < 0.029). When collapsed across all other factors, DBP in the anxiety group did not vary with respect to order of depletion (mean difference = 2.84, 95% CI –6.58–12.25, p = 0.547). However, for the fear group, DBP was significantly higher in those participants depleted on the second day (mean difference = 10.46, 95% CI 3.18–17.74, p = 0.006).
Heart rate
Disorder group and depletion condition had no impact on HR, as repeated measures ANOVA found no main effect or interaction involving these factors significant (all p > 0.08). ANOVA did return a main effect of time (F(2,104) = 8.90, p < 0.001) reflecting significantly higher HR at challenge compared with baseline (mean difference = 4.73, 95% CI 1.45–8.01, p = 0.002) and pre-challenge (mean difference = 3.64, 95% CI 0.4–6.89, p = 0.023) means.
Discussion
Our results give support to what is being proposed for the revision of the ICD11, that the group of disorders traditionally called “anxiety disorders” can be divided up into two distinct but related groups (Starcevic, 2014). We showed that decreasing the function of the 5HT system in patients in clinical remission leads to psychological and physiological exacerbation in response to stressors in the fear disorders (PTSD, panic and SAnD) though not in the anxiety disorders (GAD and OCD). Specific phobias were not tested. Importantly, these differences could not be explained by differences in the degree of depletion achieved in the different disorder groups.
These data are in concordance with previous theories and their predictions (Deakin and Graeff, 1991; Graeff and Zangrossi, 2010; Gray and Mcnaughton, 2000). According to these theories, fear disorders would be related to aversive contingencies in which the organism needs to move away from the threat and in which 5HT acutely modulates sensitivity to fear-related stimuli. Once undermined by aTD, a relapse occurs.
In contrast to the fear disorders, these theories also predict that anxiety disorders would be related to aversive contingencies in which the organism has to approach the threat (Mcnaughton and Corr, 2004). In these cases, 5HT-mediated therapeutic effects seem to happen through chronic enhancement (through SSRIs, for example) and consequent long-lasting neural changes – acute 5HT depletion causes no effects (Graeff and Zangrossi, 2010).
Epidemiological studies have also proposed similar re-formulation of the traditional group of “anxiety disorders” (see, for example, Andrews et al., 2008; Krueger, 1999). However, rethinking psychiatric classification based on different patterns of neurobiological and behavioral functioning rather than on clinical observation and clustering of symptoms is proposed to be the best way to overcome the fragilities recognized in the current nosologies, such as proposed by the Research Domain Criteria (RDoC) project, initiated by the National Institute of Mental health (NIMH) (Insel, 2014; Insel et al., 2010; Sanislow et al., 2010). In this sense, the present study gives evidence to a neurochemical dissociation of what has previously been clustered in a single group named “anxiety disorders”.
One explanation for our findings is that response to challenge under aTD conditions does not depend on the disorder in question, but on the nature of the stimuli used in the challenge: that is, fear-provoking stimuli versus anxiety-provoking stimuli. Rather, as proposed in the original theory, it is possible that individual differences in a subject’s sensitivity to each of these sorts of stimulations could relate to the specific type of clinical anxiety disorder being experienced (Gray and Mcnaughton, 2000). In spite of being a solid theory derived from many studies with animals, this view has little and only indirect support in humans. Taken as a whole, emotional reactions to aversive contingencies seem to be the result of a complex interaction between the different sorts of aversive contingencies and individual variability in sensitivity to each. The participation of 5HT in response inhibition in each case seems to be dependent on those variables rather than on diagnostic criteria. It must be noted that in panic disorder, panic attacks frequently occur in the absence of identifiable relevant environmental stimuli. With respect to the theories herein assumed (Deakin and Graeff, 1991; Gray and Mcnaughton, 2000; Mcnaughton and Corr, 2004), panic attacks would be expected to occur in response to imminent, inescapable threats, and spontaneous activation of the organic-related systems could account for the unexpected attacks seen in the disorder.
Yet, according to Deakin and Graeff’s theory (1991), the anti-fear effect of SSRIs is mediated by chronically increased synaptic 5HT and thus was reversed by aTD. In contrast, anti-anxiety effects of SSRIs involve down-regulation of 5HT transmission in the amygdala, putatively mediated by their well-known ability to down-regulate 5HT2c function. Thus aTD had little further effect on SSRI-treated anxiety disorders, since the SSRIs had already reduced 5HT function.
It should also be noted that definitions based on subjective emotional states may have led to some of the conceptual problems psychiatry has been facing (Ledoux, 2012, 2014). The present study is an initial step that may help contribute to a longer journey towards a better, more objective psychiatric nosology. Yet, it is still based on the formal and current diagnostic criteria. Future studies that categorize a clinical population based on individual sensitivity and pattern of behavioral responses to each type of aversive contingency and related neurobiology, rather than on subjective descriptions, are needed.
Some additional points deserve attention. Firstly, in spite of active major depressive disorder being an exclusion criterion, residual and/or overlapping depressive symptoms may have influenced the results. In depression, aTD alone suffices to produce mood changes (Delgado et al., 1990; Smith et al., 1997). In the present paper, it is clear from the results that mood and anxiety actually have distinct patterns of response to aTD. Differently from VAS SAD, significant differences in anxiety levels between aTD and sTD conditions were observed only after the challenge, allowing the distinction between aTD effects alone from aTD + challenge effects.
Secondly, the reader should be aware that, with the exception of one study examined here (Bell et al., 2011), all patients were treated with serotonergic antidepressants. It is possible that the differential response of the clinical groups to aTD could reflect different mechanisms of 5HT drugs in these disorders. We have no indication, however, that the non-SSRI-treated group (who had been treated with CBT instead) differed in any significant manner from the SSRI-treated cohort.
Finally, it must be noted that our data suggest some level of influence of depletion order over plasma tryptophan and cardiovascular results. This is not a usual finding in tryptophan depletion studies. Exclusion of one outlying participant from the plasma tryptophan analysis (the only participant out of the whole dataset who did not show lower plasma tryptophan under the depletion condition) removed the order effect, suggesting this was a spurious finding. The observed effect in the cardiovascular data is more difficult to explain, as there were no obvious outliers in this dataset. It is possible that there is a “real” interaction between order of depletion and BP responses, perhaps as a consequence of altering serotonergic activity within a learning or habituation context. At this stage, however, this and other potential reasons are highly speculative but worthy of further consideration. Importantly, depletion order did not influence our primary measures, viz SSAI and VAS SAD, and the order effects observed do not undermine the arguments presented here.
Given the importance of 5HT in fear/anxiety-related disorders, and the evidence presented herein, it is proposed that the monoamine system might be a major focus of investigation in this sense.
Footnotes
Acknowledgements
Caroline J. Bell, Ann S. Rich, Spilios V. Argyropoulos, Sam Forshall, Mariona Adrover, Jon Nash, John Potokar, Neil C. Rich, Harry J. Witchel
Declaration of Conflicting Interests
Dr. Corchs, Davies, Bernik and Hince declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Hood declares unrestricted educational grants – Servier, Pfizer, Wyeth; Speaker’s Fees / Honoraria – Astra-Zeneca, Boehringer, Bristol-Myers-Squibb, Cephalon, Eli-Lilly, Janssen-Cillag, Lundbeck, Pfizer, Sanofi-Aventis, Servier, Wyeth; Advisory Board – GSK (Aropax), Eli-Lilly (Cymbalta), Pfizer (Pristiq – Chair), Lundbeck (Vortioxetine); Travel Support –Astra-Zeneca, Boehringer, Bristol-Myers-Squibb, Cephalon, Eli-Lilly, Janssen-Cillag, Lundbeck, Pfizer, Sanofi-Aventis, Servier, Wyeth; Clinical trials support – Park-Davis, Pfizer, Raine Foundation, Sanofi-Aventis, Servier, University of Western Australia, Wyeth, Wellcome Trust (UK) Prof. Nutt declares Consultancies – Pfizer (W-L), GSK (SKB), MSD, BMS, Esteve, Novartis, Asahi, Organon, Cypress, Lilly, Janssen, Takeda, Phamacia, Therasci, Passion for Life, Hythiam, Servier, Roche, Sanofi-Aventis, Actelion, Lundbeck, Wyeth; Speaking honoraria (in addition to above) – Reckitt-Benkiser, Cephalon; Grants or clinical trial payments – MSD, GSK, Novartis, Servier, Janssen, Yamanouchi, Lundbeck, Pfizer, Wyeth, Organon, AZ, Cephalon, P1vital, MoDefence, NHS; Worked for the UK Government’s Committee on Safety of Medicines; Advisory Council on the Misuse of Drugs, British National Formulary.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fundação de Amparo à Pesquisa do Estado de São Paulo (State of São Paulo Research Foundation; Grant Nos. 2008/04122-5 and 99/ 00170-4 for the support of the PTSD study (![]() ).
).