
Abstract
Objective:
In the general population cannabis use is associated with better cardiometabolic outcomes. Patients with severe mental illness frequently use cannabis, but also present increased cardiometabolic risk factors. We explore the association between cannabis use and cardiometabolic risk factors in patients with severe mental illness.
Method:
A total of 3169 patients with severe mental illness from a Dutch cohort were included in the study. The association of cannabis use with body mass index, waist circumference, blood pressure, cholesterol, triglycerides, glucose, glycated hemoglobin and Positive and Negative Syndrome Scale was examined with separate univariate AN(C)OVA. Changes in metabolic risk factors and Positive and Negative Syndrome Scale were examined after a follow-up interval of 9–24 months, for patients who continued, discontinued, started or were never using cannabis between the two assessments.
Results:
Cannabis users at baseline had lower body mass index, smaller waist circumference, lower diastolic blood pressure, and more severe psychotic symptoms than non-users. Patients who discontinued their cannabis use after the first assessment had a greater increase in body mass index, waist circumference, diastolic blood pressure and triglyceride concentrations than other patients, and the severity of their psychotic symptoms had decreased more compared to continued users and non-users.
Conclusion:
Extra attention should be paid to the monitoring and treatment of metabolic parameters in patients who discontinue their cannabis use.
Introduction
Cardiovascular diseases are the main cause of premature mortality in people with severe mental illness (SMI), such as psychotic disorders, depression and bipolar disorder, and shorten their life-expectancy by 13–30 years (De Hert et al., 2011; Hennekens et al., 2005). Antipsychotic medication may have a negative impact on cardiometabolic risk factors. Patients using antipsychotic medication often experience an increase in waist circumference, dyslipidemia and hyperglycemia (Atmaca et al., 2003; Haupt and Newcomer, 2001; Suvisaari et al., 2007). Together with hypertension and hypertriglyceridemia, these symptoms constitute the metabolic syndrome (Grundy et al., 2005). Other factors contributing to the risk of developing cardiovascular diseases are unhealthy lifestyle habits, such as a poor diet, physical inactivity, smoking, excessive alcohol intake and substance abuse (Scott and Happell, 2011). The prevalence of cannabis use is twice as high among people with SMI compared to the general population (Green et al., 2005). Moreover, patients often have less access to physical health care, whereas the health care they do receive often is of poorer quality (De Hert et al., 2011).
Interestingly, there are indications of an inverse relation between cannabis use and cardiometabolic risk in the general population, but the findings of different studies are inconclusive (Le Strat and Le Foll, 2011; Penner et al., 2013; Rodondi et al., 2006; Smit and Crespo, 2001; Warren et al., 2005). Several large population studies found that current cannabis use was independently associated with lower body mass index (BMI), less obesity, lower concentrations of fasting insulin, higher concentrations of high-density lipoprotein cholesterol (HDL-C) and a smaller waist circumference, after correcting for confounders (Le Strat and Le Foll, 2011; Penner et al., 2013; Smit and Crespo, 2001; Warren et al., 2005). However, another large population study found that these associations were no longer significant after controlling for confounders, such as smoking, alcohol intake and physical activity (Rodondi et al., 2006).
The role of cannabis with regard to the increased cardiometabolic risk in people with SMI has not been clarified yet. Previous studies addressing cannabis use in people with psychotic disorders mostly focused on effects on psychotic symptoms (Green et al., 2005; Henquet et al., 2010). They showed that the use of cannabis can trigger psychoses and can lead to persistence of psychotic symptoms (Kuepper et al., 2013; Semple et al., 2005). Only one study reported on the effect of cannabis use on cardiometabolic risk factors in people with psychotic disorders, showing that patients using cannabis had significantly higher blood glucose levels than non-users as well as more severe psychotic symptoms (Isaac et al., 2005). Furthermore, patients admitted to a hospital who continued to use cannabis showed a greater increase in body weight and their psychotic symptoms were more persistent. The authors did not report other metabolic parameters, nor controlled for other lifestyle factors.
Aims of the study
We will explore the association between cannabis use and cardiometabolic risk factors in people with SMI, controlling for the potential confounding effects of smoking, alcohol intake and antipsychotic medication. After a follow-up interval of 9–24 months, we will examine whether changes in metabolic risk factors are different for continued cannabis users, discontinuers, starters and non-users. Furthermore, we will examine the association between cannabis use and the severity of psychotic symptoms in a subsample of patients with psychotic disorders, expecting that psychotic symptoms will be more severe in cannabis users compared to non-users.
Material and methods
Study design
This study used data from the Pharmacotherapy Monitoring and Outcome Survey (PHAMOUS), an ongoing Dutch cohort study that started in 2006 in four mental health institutions in the northern Netherlands (Mulder et al., 2010). Patients with SMI were invited to participate in annual screenings for health evaluation purposes, where a trained nurse examined their mental and physical health. Assessments were carried out in accordance with the Declaration of Helsinki and patients participated on a voluntary basis. Of note, the comprehensive assessments included several interviews, measurements and questionnaires. Patients did not always complete each assessment, in which case we used pairwise exclusion. Patients were eligible for the current study when they: (a) were diagnosed with a psychotic disorder (i.e. schizophrenia, schizoaffective disorder, schizophreniform disorder, delusional disorder, substance induced psychosis or psychosis NOS) or mood disorder (i.e. depressive disorder, bipolar disorder); (b) had two consecutive assessments with an interval between 9 and 24 months. The intention of PHAMOUS is to screen patients every year, but the screenings are rarely exactly 12 months apart and therefore an interval between 9 and 24 months was chosen; (c) had disclosed whether or not they were currently using cannabis; (d) had a physical assessment and/or laboratory test data were available, more specific if information about at least one of the metabolic outcomes (i.e. BMI, waist circumference, blood pressure (BP), high-density lipoprotein cholesterol, HDL-C, low-density lipoprotein cholesterol (LDL-C), glucose or glycated hemoglobin [HbA1c]) was available.
Data of all eligible patients with SMI were used in the analyses for the associations between cannabis use and metabolic risk factors. For the association between cannabis use and the severity of psychotic disorders we used the subsample of the patients with psychotic disorders, meaning that patients with depressive and bipolar disorders (9.6% of the complete sample) were excluded from these analyses.
Outcome measurements
Psychiatric diagnoses and the year of first psychotic episode were provided by the patients and were verified by their psychiatrist, in the medical file record. Patients were asked about their daily consumption of regular meals, fruit and snacks, and about the amount of vegetable intake per week.
Cannabis, alcohol and cigarette use
Cannabis use was determined during an interview on health behaviors. Patients were asked whether they used cannabis and the current users were asked how much they used in number of joints per week. All patients were asked whether they smoked cigarettes and used alcohol. If applicable, their alcohol intake in glasses per week was assessed.
Physical assessment
To determine BMI (kg/m2), the patients’ height and body weight were measured. Waist circumference (cm) was measured exactly between the lower rib and the upper edge of the hip bone by using a flexible measuring tape. Patients were instructed to keep their feet flat on the ground, approximately 30 cm apart. The tape was read at the end of a regular exhalation.
Patients were seated for the determination of systolic and diastolic blood pressure (SBP and DBP; mm Hg). BP was measured after the patients had rested for several minutes. A second BP measurement took place after an interval of at least 15 seconds. The mean average of the two SBP and DBP measurements was used in this study.
Laboratory tests
Blood was taken from the patients to measure the concentrations of total cholesterol (mmol/L), HDL-C (mmol/L), LDL-C (mmol/L), triglycerides (mmol/L), glucose (mmol/L) and HbA1c (mmol/L). Participants were asked to fast for at least eight hours before their blood sample was taken.
Psychotic symptom severity
A shortened Positive and Negative Syndrome Scale (PANSS), based on the remission criteria according to Andreasen et al. (2005), was used to assess the severity of the psychotic symptoms (Andreasen et al., 2005; Kay et al., 1987). It consists of three items of the Positive Symptom Scale (i.e. delusions, conceptual disorganization and hallucinations), three items of the Negative Symptom Scale (i.e. blunted affect, social withdrawal and lack of spontaneity) and two items of the General Psychopathology Scale (i.e. mannerisms and posturing, and unusual thought content). Each item is scored on a 7-point Likert-scale: a score of 1 means the symptom is absent, whereas scores 2–7 indicate increasing symptom severity, with a score of 7 indicating extreme severity. Scores are calculated for the separate subscales, with a higher total score representing greater psychotic symptom severity.
Statistical analysis
Chi-square tests and independent sample t-tests were used to compare baseline differences between cannabis users and non-users.
Separate ANOVA models were fit with baseline BMI, waist circumference, SBP, DBP, total cholesterol, HDL-C, LDL-C, triglycerides, glucose, HbA1c and the PANSS (remission criteria) as continuous dependent variables, and cannabis status as independent variable. Next, separate univariate ANCOVA models were performed, adjusted for age, sex, type of prescribed antipsychotic drug (i.e. clozapine, olanzapine, risperidone, quetiapine, aripiprazole, haloperidol and other; each type of antipsychotic drugs was included as dichotomous variable), dosage antipsychotic drug (in chlorpromazine equivalents), smoking status (yes/no) and alcohol intake (yes/no), which were a priori selected as potential confounders. Patients with only depressive or bipolar disorder were excluded from all analyses with psychotic symptom severity as dependent outcome.
To examine the longitudinal effects of cannabis use, the participants were divided into four groups: continuers (using cannabis at both assessments), discontinuers (using cannabis at the first, but not using cannabis at the second assessment), starters (not using cannabis at the first, but using cannabis at the second assessment) and non-users (not using cannabis at both assessments). With separate univariate AN(C)OVA models we examined whether the changes in BMI, waist circumference, SBP, DBP, total cholesterol, HDL-C, LDL-C, triglycerides, glucose, HbA1c and the PANSS (remission criteria) at the second assessment differed between these groups. In the ANCOVA models the associations were adjusted for the previously mentioned a priori selected confounders. Alcohol and smoking were included in the same manner as cannabis (continued smoking/drinking alcohol, discontinued smoking/drinking alcohol, started smoking/drinking alcohol, not smoking/drinking alcohol at either assessment). When the overall result was significant, simple and repeated contrast analyses were used for a detailed examination of the extent of the differences. Cohen’s d was calculated as measure of effect size (ES) (Thalheimer and Cooks, 2002). Patients with only depressive or bipolar disorder were excluded from all analyses with psychotic symptom severity as dependent outcome. Since we have no available outcome measures on the severity of depressive and bipolar symptoms, we are unable to describe how cannabis may influence the course of these specific symptoms. All data were analyzed using IBM SPSS Statistics version 22.0.
Post hoc analyses
Food intake was not reported for all patients. In post hoc ANCOVA analyses the number of meals per day and the amount of fruit and vegetable intake were included as additional covariates in the model. Because of missing data, multiple imputations were used to replace missing data for the amount of alcohol intake, the amount of cannabis intake and all of the metabolic outcomes. Fifteen imputed datasets were generated using predictive mean matching (Rubin, 2004). Post hoc AN(C)OVA analyses were performed with the pooled estimates of the imputed variables.
Results
Sample characteristics
Of the 6340 patients that participated in PHAMOUS, a total of 3169 patients fulfilled the inclusion criteria for the current study. Laboratory data were missing in 22–36% of the included patients and 23% of these patients had missing PANSS data. At baseline, 11.3% of the patients reported to use cannabis. Of these, 42.2% smoked less than one joint per day, 24.6% smoked one or more joints per day and 33.2% did not disclose the quantity of their cannabis use. The mean follow-up time between the two assessments was 14.0 months (SD = 4.50).
Several differences in baseline characteristics regarding demographics, medication and substance use were found between the cannabis users and the non-users (for an overview see Table 1). In addition, cannabis users reported to eat less regular meals per day (t = −7.70, P < 0.001), less fruit (t = −4.78, P < 0.001) and less vegetables (t = −4.67, P < 0.001) compared to non-users. There were no significant differences in the daily snacks consumption (t = 1.37, P = 0.180).
Baseline differences and characteristics between cannabis users and non-users.
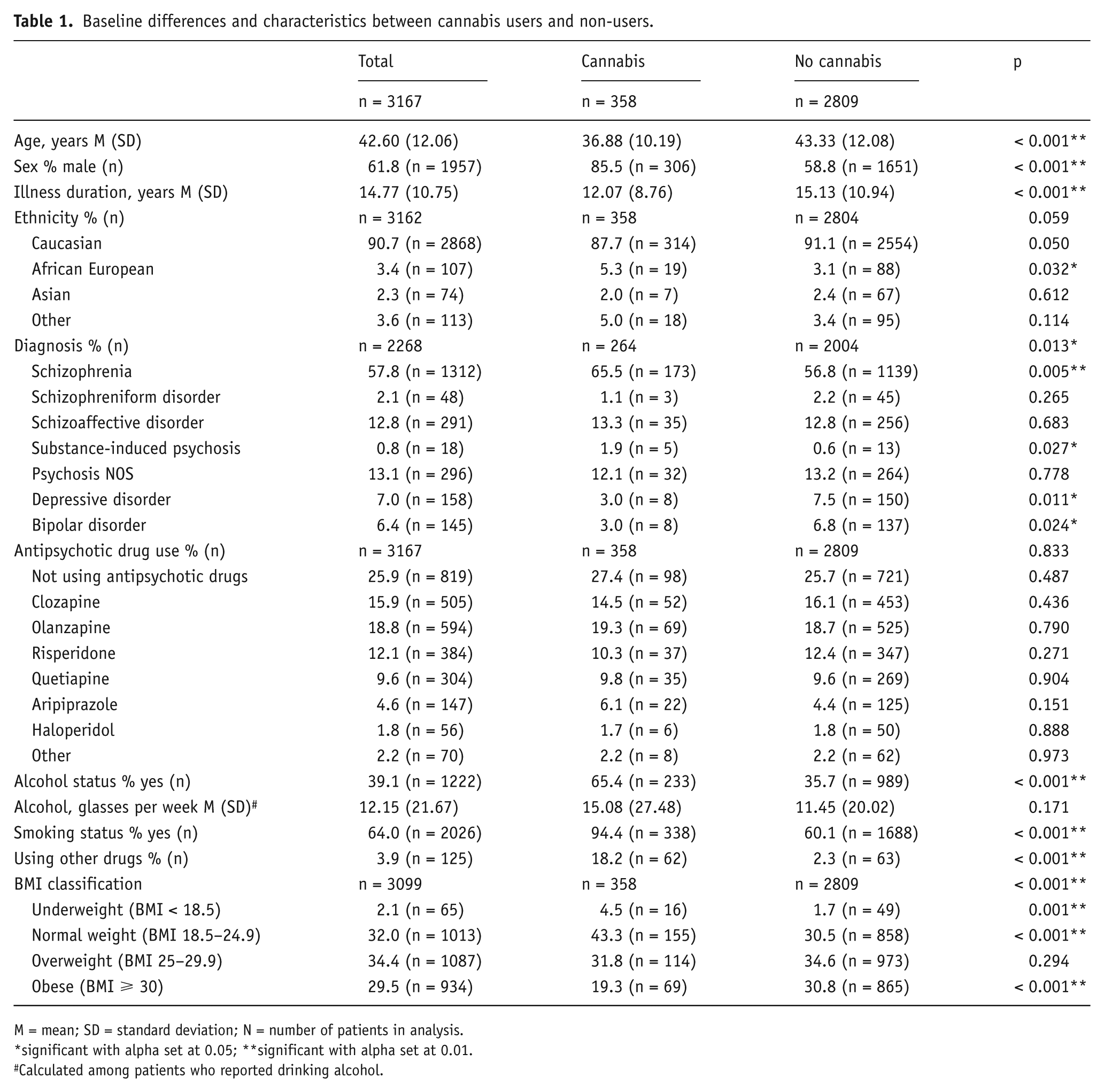
M = mean; SD = standard deviation; N = number of patients in analysis.
significant with alpha set at 0.05; **significant with alpha set at 0.01.
Calculated among patients who reported drinking alcohol.
Associations with metabolic risk
Cannabis users had significantly lower BMI, smaller waist circumference and lower DBP (see Table 2). When adjusting the models for age, sex, type of prescribed antipsychotic drug, dosage antipsychotic drug, smoking and alcohol, the associations between cannabis use and BMI (F(1,3045) = 8.30, P = 0.004), waist circumference (F(1,2810) = 13.83, P < 0.001) and DBP (F(1,3049) = 5.20, P = 0.023) remained statistically significant.
Unadjusted ANOVA models for baseline cardiovascular risk factors and psychotic symptom severity.
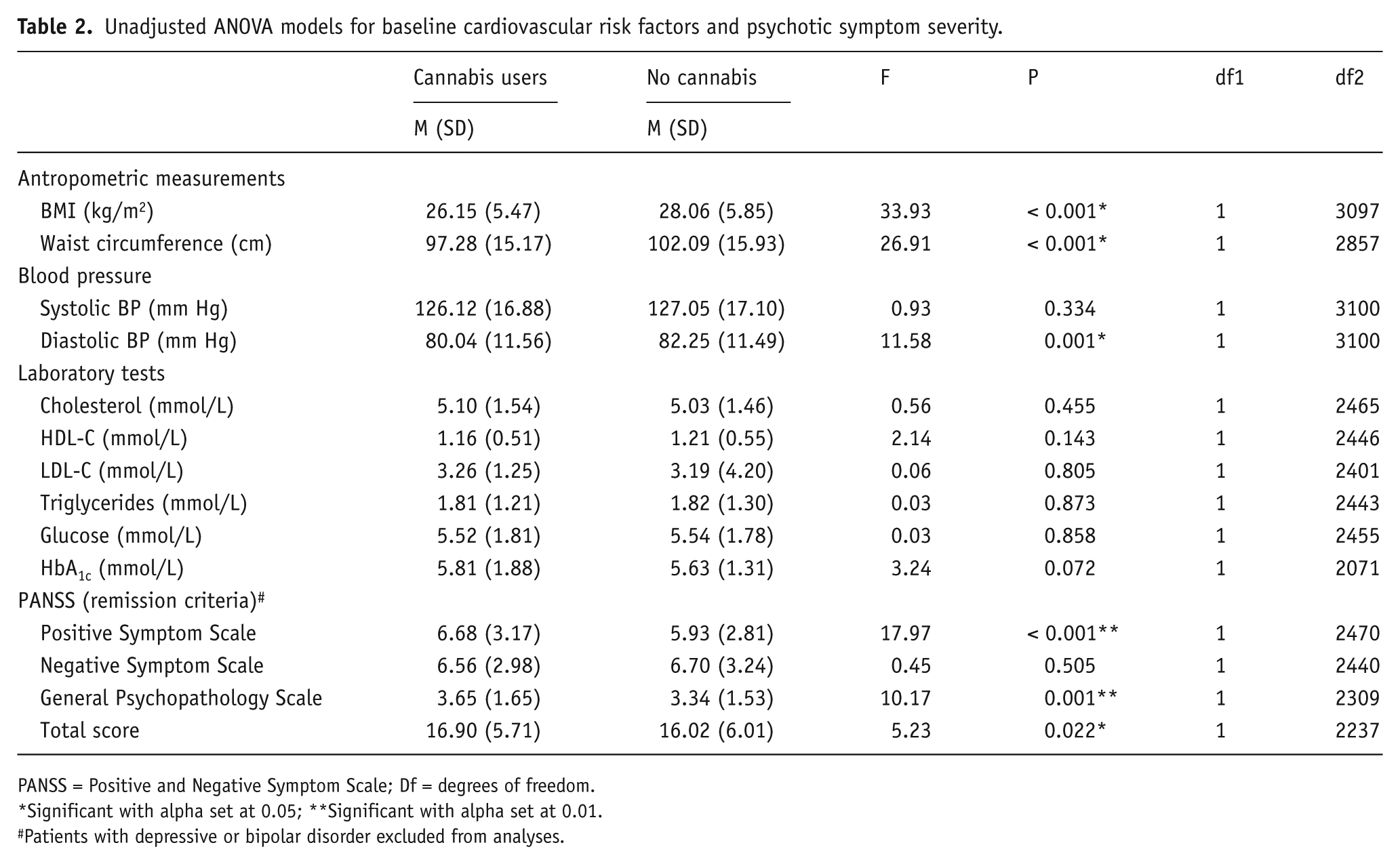
PANSS = Positive and Negative Symptom Scale; Df = degrees of freedom.
Significant with alpha set at 0.05; **Significant with alpha set at 0.01.
Patients with depressive or bipolar disorder excluded from analyses.
At the second assessment, significant differences between the four patient groups were observed in changes in BMI, waist circumference, DBP and triglyceride concentrations (see Table 3 and Figure 1a–d). After adjusting for covariates the differences in BMI (F(3,2940) = 2.46, P = 0.050), waist circumference (F(3,2599) = 2.85, P = 0.036), DBP (F(3,2953) = 2.85, P = 0.036) and triglyceride concentrations (F(3,1961) = 3.27, P = 0.020) remained statistically significant. More specifically: discontinuers showed a greater increase in BMI compared to non-users (ES = 0.27, 95% CI 0.07–0.46) and starters (ES = 0.29, 95% CI −0.01–0.59), as well as a greater increase in waist circumference compared to continuers (ES = 0.30, 95% CI 0.06–0.54), non-users (ES = 0.28, 95% CI 0.08–0.48) and starters (ES = 0.25, 95% CI −0.05–0.55). Discontinuers also had a greater increase in DBP than starters (ES = 0.36, 95% CI 0.06–0.66). Triglycerides concentrations had increased less in non-users compared to continuers (ES = −0.18, 95% CI −0.64–0.21).
Unadjusted ANOVA changes in BMI, cardiometabolic risk factors and PANSS (remission criteria) from first to second assessment.
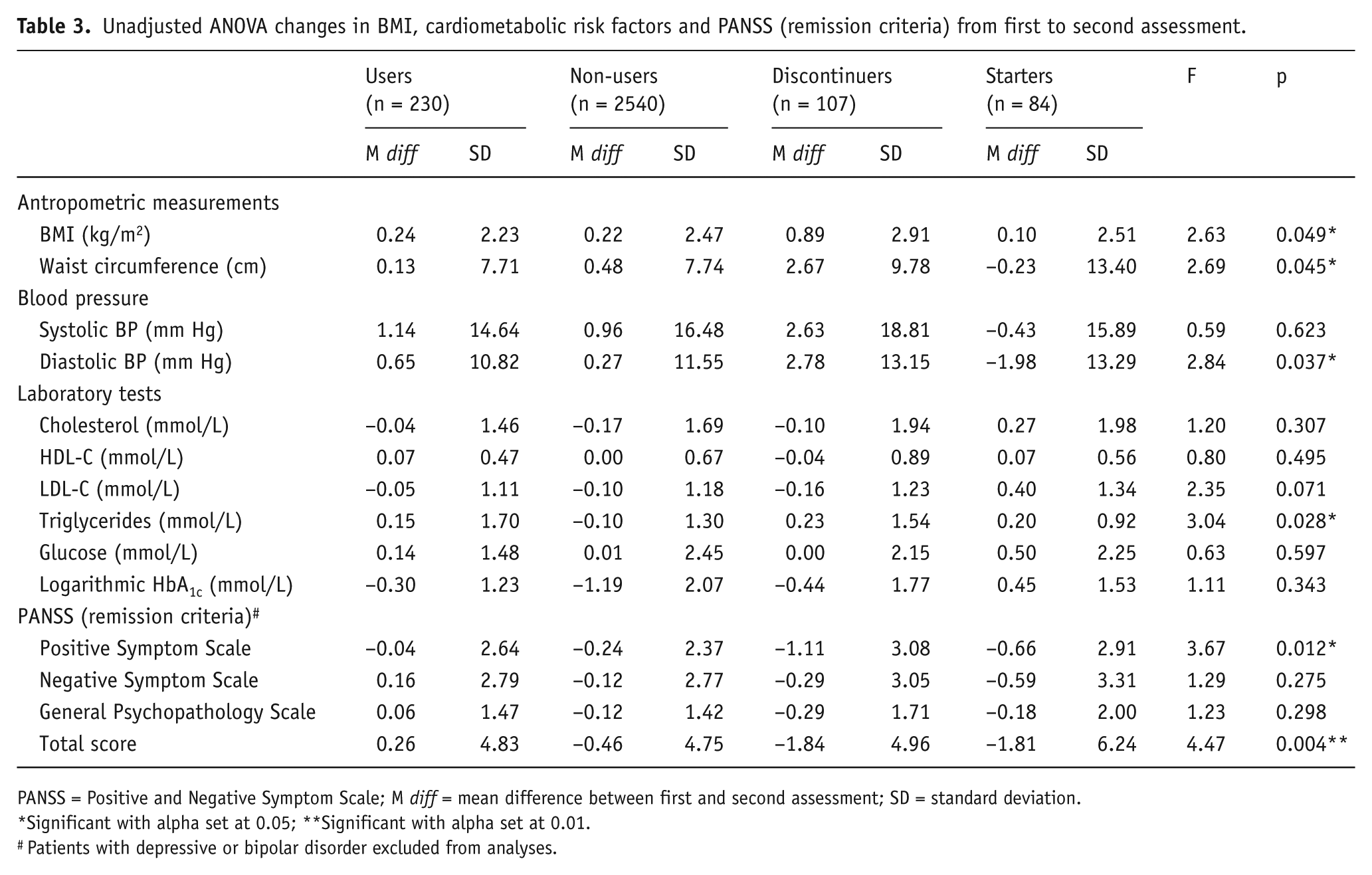
PANSS = Positive and Negative Symptom Scale; M diff = mean difference between first and second assessment; SD = standard deviation.
Significant with alpha set at 0.05; **Significant with alpha set at 0.01.
Patients with depressive or bipolar disorder excluded from analyses.
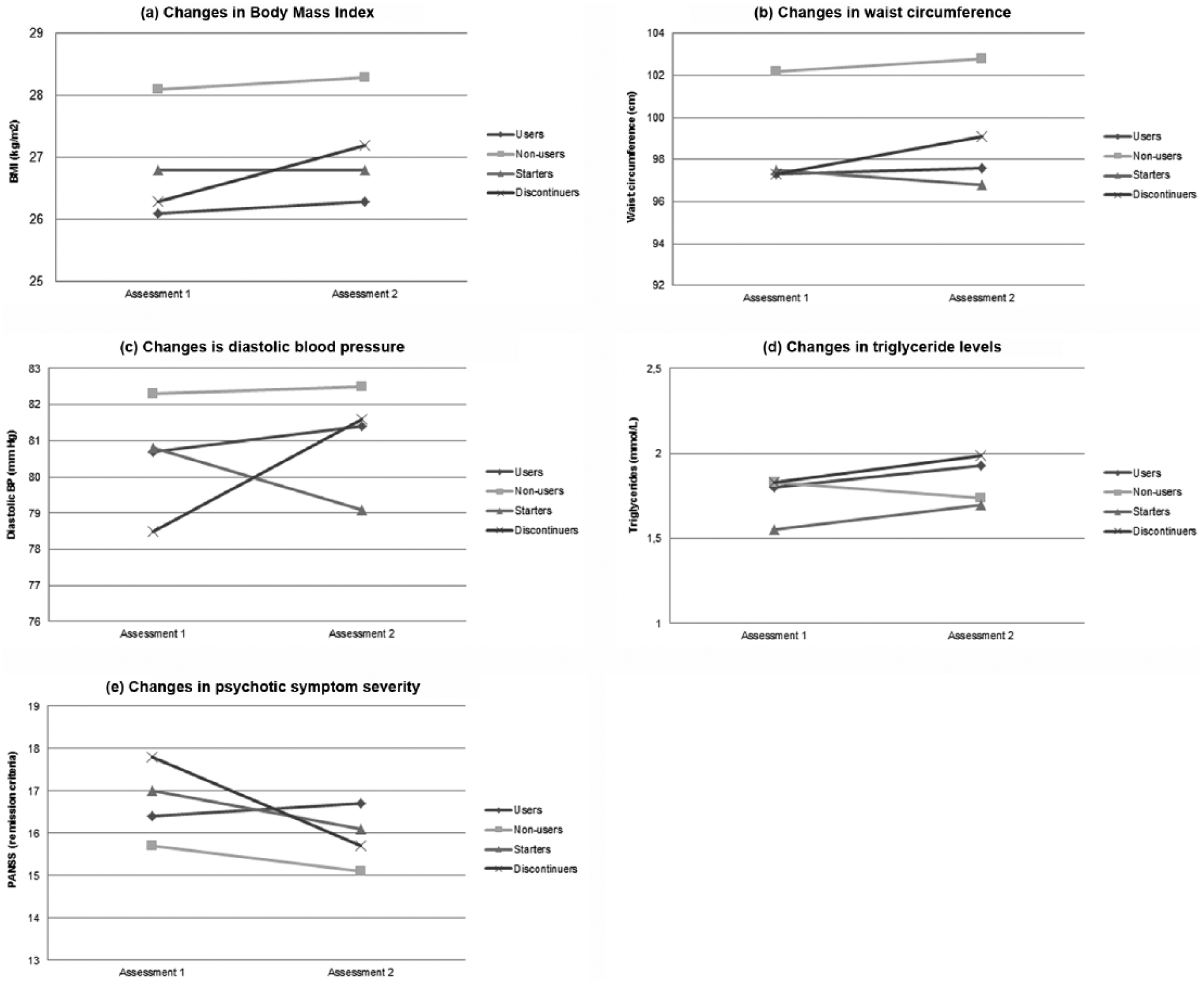
Changes in severity of BMI, cardiometabolic risk factors and psychotic symptoms from the first to second assessment.
Associations with psychotic symptoms
Psychotic symptoms were more severe in cannabis users compared to non-users (see Table 2). The effects remained statistically significant after adjusting the models for age, sex, type of prescribed antipsychotic drug, dosage antipsychotic drug, smoking and alcohol (F(1,2195) = 7.31, P = 0.007). Cannabis use was related to both positive symptoms (F(1,2424) = 17.39, P < 0.001) and general psychopathology (F(1,2266) = 13.81, P < 0.001), but not to negative symptoms (F(1,2440) = 0.45, P = 0.505, unadjusted).
Changes in psychotic symptom severity from the first to the second assessment differed significantly between the four patient groups (see Table 3 and Figure 1e). The differences in total PANSS scores remained statistically significant after adjusting for age, sex, type of prescribed antipsychotic drug, dosage antipsychotic drug, smoking and alcohol (F(3,1777) = 4.29, P = 0.005). Cannabis discontinuers showed a greater decrease of psychotic symptom severity (ES = −0.43, 95% CI −0.64–0.22), and specifically in positive symptoms (ES = −0.38, 95% CI −0.60–0.17), compared to continuers. Cannabis discontinuers also showed a greater decrease of psychotic symptom severity (ES = −0.29, 95% CI −0.48–0.10), and specifically in positive symptoms (ES = −0.36, 95% CI −0.55–0.17), compared to non-users.
Post hoc analyses
Including the amount of regular meals and fruit and vegetables intake as additional covariates besides the a priori selected confounders, did not change the implications of the results (see Table S1). Replacing alcohol (yes/no) with the pooled estimate of the imputed number of glasses alcohol intake per week as continuous covariate did not change the implications of the results (see Table S2), neither did using the amount of cannabis intake (number of joints per week) as independent variable by categorizing the patients into three groups: no joints, ⩽ 1 joint per day and > 1 joints per day (see Table S3).
Discussion
In this study we found that patients using cannabis had a lower BMI, a smaller waist circumference and a lower DBP, but that their psychotic symptoms were more severe than in non-users. Patients using cannabis were more often of normal weight or underweight, whereas non-users were more often obese. Patients who had discontinued their cannabis use after the first assessment showed a greater increase in BMI, waist circumference, DBP and triglyceride concentrations than other patients, and a greater reduction of psychotic symptom severity compared to continued users and non-users. The effects were small to moderate and the associations remained significant after controlling for age, sex, type of prescribed antipsychotic drug, smoking status and alcohol intake. Although discontinuers of cannabis showed the greatest increase in metabolic risk, the non-users still had the greatest overall metabolic risk at the second assessment.
These findings are in line with studies in the general population, in which cannabis users have a lower BMI, a smaller waist circumference and suffer from obesity less often than non-users (Le Strat and Le Foll, 2011; Penner et al., 2013; Smit and Crespo, 2001; Warren et al., 2005). These findings are substantiated by our follow-up analyses, showing a greater increase in metabolic risk in discontinuers compared to continuers, starters and non-users. Interestingly, Rodondi et al. (2006) found no relation between cannabis use and cardiometabolic risk, despite an increased caloric intake and greater alcohol consumption in cannabis users (Rodondi et al., 2006).
The prevalence of cannabis use in the last month of the Dutch population between the ages of 15 and 64 is 4.2% (European Monitoring Centre for Drugs and Drug Addiction – EMCDDA, 2012). Given the fact that cannabis use in people with psychotic disorders is twice as high compared to the general population (Green et al., 2005), a prevalence of 11.3% patients currently using cannabis was to be expected. Another Dutch study found a slightly higher prevalence with 16.3% of their patients with psychotic disorders currently using cannabis, but this sample was much younger with a mean age of 27 years (Meijer et al., 2012). Cannabis users in this study were more often diagnosed with schizophrenia than non-users. This is consistent with previous studies that suggest there is a stronger association between cannabis use and schizophrenia than between cannabis use and other psychotic disorders (Manrique-Garcia et al., 2012).
The finding that metabolic risk factors are less severe in cannabis users compared to non-users could be explained by the interaction of cannabis with the endocannabinoid system via the cannabinoid type 1 (CB1) and cannabinoid type 2 (CB2) receptor. Over-activity of the endocannabinoid system is associated with an increased risk of developing abdominal obesity, hyperglycemia and dyslipidemia (Juan et al., 2015; Matias and Di Marzo, 2007). The main psychoactive constituent of cannabis (−)-trans-Δ9-tetrahydrocannabinol (THC) is a CB1 receptor agonist, which increases appetite and food intake and stimulates the storage of body fat (Di Marzo and Matias, 2005; Hillig and Mahlberg, 2004). However, cannabis is a mixture of compounds, with a variety of effects. Naturally occurring CB1 receptor antagonists, such as cannabidiol and tetrahydrocannabivarin are also present in cannabis (Hillig and Mahlberg, 2004). These CB1 receptor antagonistic properties could diminish appetite and food intake and therefore lead to metabolic improvements (Christopoulou and Kiortsis, 2011). Randomized controlled trials with rimonabant, a selective CB1 receptor antagonist, advocate this theory: rimonabant was shown to reduce waist circumference, fasting glucose, HbA1c and triglyceride concentrations, and to increase HDL-C (Curioni and Charles, 2006; Waterlow and Chrisp, 2008). The presence of both CB1 receptor agonists and antagonists in the natural cannabis used by patients could explain, at least in part, why cannabis use can both increase and decrease cardiometabolic risk. The endocannabinoid system may also be associated with dopamine events: cannabis use increases dopamine release, whereas rimonabant appears to decrease cannabis-induced dopamine release by disrupting endocannabinoid signaling (Oleson and Cheer, 2012). A greater experienced pleasure of eating has been associated with increased dopamine release as well (Small et al., 2003). Patients discontinuing cannabis use may attempt to mimic the feeling of cannabis-induced dopamine release by overeating or by eating unhealthy ‘comfort food’, which can cause weight gain and increase their metabolic risk. In this study, eating behavior was reported only globally and not assessed by standardized food diaries or food frequency questionnaires. However, our finding that patients using cannabis eat less healthy food, such as fruits and vegetables, than non-users does seem to support this possible explanation.
An important finding is that the use of cannabis in patients with psychotic disorders was associated with more severe psychotic symptoms, which is in accordance with a wide body of literature (Foti et al., 2010; Henquet et al., 2010; Kuepper et al., 2013; Negrete et al., 1986; Peralta and Cuesta, 1992). Notably, patients who discontinued the use of cannabis showed greater reductions of psychotic symptoms than continuers and non-users, particularly positive symptoms such as hallucinations and delusions. Thus, discontinuation of cannabis use remains an important treatment goal as this will presumably reduce the severity of psychotic symptoms. At the same time, physicians should be aware of possibly increasing metabolic risk. Special attention should be paid to the monitoring and treatment of metabolic risk factors in patients who discontinue cannabis use, in order to prevent the development of cardiovascular diseases and premature cardiovascular mortality.
Limitations
Cannabis use was determined in an interview, where patients were only asked about the number of joints they would smoke on a weekly basis. No information was available about the size of the joints, the amount of cannabis in grams, or the compound of the cannabis plants.
At the second assessment information cannabis use was again determined in an interview, but no information was available about the duration of cannabis use when patients had started using between the assessments, or the duration of abstinence in case patients had discontinued using cannabis.
Physical inactivity could have influenced the relation between cannabis use and cardiometabolic risk (Brown et al., 1999), because physical activity is negatively associated with both cardiometabolic risk and cannabis use (Henchoz et al., 2014). Unfortunately, information about the patients’ physical activity was not obtained at the first assessment.
Socioeconomic status could also be of importance, because both poor socioeconomic circumstances during childhood and adolescence and own educational level are associated with an increased chance of cannabis use (Daniel et al., 2009; Lee et al., 2015), as well as an increased risk of obesity and the metabolic syndrome (Drewnowski et al., 2013; Kim et al., 2013). However, we had no available information on patients’ educational level nor on their socioeconomic circumstances while growing up.
It has been shown that cannabis users have lower levels of fasting insulin and insulin resistance than non-users (Penner et al., 2013). These are important outcome measures, given the high prevalence of diabetes type 2 in people with a psychotic disorder (Schoepf et al., 2012), but insulin levels were not assessed in this study.
Future studies on cannabis use and cardiometabolic risk factors in people with psychotic disorders should examine the influence of physical activity and socioeconomic circumstances on this association, and include levels of THC and cannabinoids. Measures of insulin and insulin resistance could be valuable additional outcome variables of cardiometabolic risk. Regarding psychotic symptom severity, future studies may focus on the effects of cannabis use on volumetric or shape measurements of subcortical structures of the brain (Weiland et al., 2015), since this was found to be associated with increased psychotic symptom severity (Padmanabhan et al., 2015).
Conclusion
Cannabis use is associated with a lower BMI, a smaller waist circumference and a lower DBP in people with SMI. Although non-users of cannabis present the greatest overall metabolic risk, the greatest increase in BMI, waist circumference, DBP and triglyceride concentrations was shown in patients who discontinued their cannabis use. However, although some patients mention they use cannabis as a form of self-medication (Gómez Pérez et al., 2014), cannabis use appears to have a negative impact on psychotic symptoms. Therefore, encouraging patients to discontinue the use of cannabis is still an important treatment goal as it will reduce the severity of psychotic symptoms. Nonetheless, the effects of discontinuing cannabis use on patients’ physical health should not be underestimated and physicians should be aware of the increased metabolic risk this discontinuation may entail.
Footnotes
Acknowledgements
The authors are grateful to all the staff members of the different institutions for collecting the data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: his work was supported by the Rob Giel Research Center at the University Center for Psychiatry of the University Medical Center Groningen, Friesland Mental Health Services, GGZ Drenthe and Lentis Mental Health Organization.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.