
Abstract
Despite the first reports concerning benzodiazepine dependence being published in the early 1960s literature, the risk of benzodiazepine addiction is still greatly debated. The severe discomfort and life threatening complications usually experienced by long-term benzodiazepine users who suddenly interrupt benzodiazepine intake have led to the development of several detoxification protocols. A successful strategy used by our Addiction Unit is abrupt benzodiazepine cessation by administering flumazenil slow subcutaneous infusion (FLU-SSI) with an elastomeric pump. Although some studies proved the efficacy of flumazenil infusion more than 20 years ago, only a few centres in the world offer this method to their patients. This paper reports the data related to 214 subjects addicted to high doses of benzodiazepine and treated with the FLU-SSI method between 2012 and 2014. This technique is less invasive and requires less nursing intervention than intravenous infusion. Our data support FLU-SSI as a possible efficient strategy for the treatment of patients with long-term, high-dose benzodiazepine addiction, and could become a routine therapy as long as the necessary further studies on dose, duration of infusion and safety issues are carried out.
Keywords
Introduction
Benzodiazepines are widely prescribed and useful for the clinical management of anxiety, panic disorders, insomnia, seizures, muscle spasms and alcohol withdrawal syndrome. However, the use of benzodiazepines may lead to abuse, tolerance and dependence on therapeutic doses as well as on high doses; the latter with a complete loss of control (Ashton, 2005; Lader, 2011; Nutt et al., 2010).
It is well known that benzodiazepines should be prescribed in selected clinical situations and only for short periods of time (Lader, 2014; López-Muñoz et al., 2011; Sirdifield et al., 2013). In case of long-term use, the risk of harmful effects and dependence should therefore be taken into consideration and the benefits of an alternative short or intermittent treatment should be assessed (Baldwin et al., 2013).
The most common definition of long-term benzodiazepine use is continuous use for at least six months (Kurko et al., 2015). Prevalence rates of long-term use vary around the world. Overall, it ranges from approximately 2.0% to 7.4% in the general population, whereas the estimated occurrence of long-term use among benzodiazepine users varies between 25% and 76% (Fang et al., 2009). An American investigation (Olfson et al., 2015) reported that in 2008 approximately 5.2% of US adults used to take benzodiazepines, with the proportion of long-term users increasing with age: from 14.7% (18–35 years) to 31.4% (65–80 years). In Italy, it is estimated that more than half of benzodiazepine users are chronic consumers, and 15–44% of these are addicted (Magrini et al., 1996).
Many epidemiological studies on benzodiazepine misuse are available in the literature, while less has been published about high-dose benzodiazepine consumers. Surveys from France, Germany, Italy and the UK, carried out during the 1990s, indicated that 3.2% of anxiolytic and 3.9% of hypnotic users utilised much higher doses than recommended (Ohayon and Lader, 2002). A cross-sectional study, performed on 520,000 patients in Switzerland (Petitjean et al., 2007), showed that approximately 6.6% of the Swiss adult population misused benzodiazepines, and about 1.6% had an intake even higher than twice the recommended daily dose. Another study (Holzbach, 2010) estimated that the percentage of misuse and dependency in Germany involved 5% of the overall population. Furthermore, a more recent study pointed out that the number of benzodiazepine-dependent patients in Germany ranged widely, from 128,000 to 1.6 million. This range is wide because most estimates exclude a large number of prescriptions such as those not reimbursed by the national health system or for elderly people (Janhsen et al., 2015).
An analysis of Taiwan national health insurance system database prescription data for the year 2007, which included 1.34 million benzodiazepine users, showed that 41.1% were long-term (>90 days) and 1.9% long-term high-dose (more than three defined daily doses; DDDs) users (Yu-Ping et al., 2014).
Long-term benzodiazepine use is associated with a risk of dependence, as confirmed by the occurrence of specific symptoms when the drug is abruptly withdrawn. Between 15% and 44% of chronic benzodiazepine users experience moderate to severe withdrawal syndrome, including extreme anxiety and signs of depression. In some cases, even life threatening complications such as seizures may occur (Albiero et al., 2011; Lader, 2011). The great discomfort experienced by patients suffering from benzodiazepine withdrawal syndrome has led to the development of therapeutic strategies, such as gradually tapering of the dosage or switching to an equivalent dose of another long half-life benzodiazepine before tapering (Ashton, 2005; Lader, 2011).
Of particular pharmacological interest is the alternative method of detoxification from benzodiazepines using flumazenil. Flumazenil is commonly employed in the treatment of benzodiazepine overdose, and is usually considered an antagonist with high affinity to benzodiazepine receptors. As a matter of fact, studies have shown that bolus infusion of flumazenil produced effects consistent with benzodiazepine withdrawal (Griffiths et al., 1993; Mintzer and Griffiths, 2005; Mintzer et al., 1999), whereas multiple slow bolus infusions of flumazenil reduce withdrawal symptoms (Gerra et al., 1996; Lader and Morton, 1992; Saxon et al., 1997), probably because flumazenil acts as a weak agonist on the benzodiazepine receptor, as shown in the animal or in vitro experimental setting (Gallager et al., 1986; Klein et al., 1994).
After a randomised controlled clinical trial, in which Gerra et al. (2002) proposed flumazenil slow intravenous infusion as a detoxification protocol in high-dose benzodiazepine users, only a few studies on the topic have been published (Faccini et al., 2012; Hood et al., 2009, 2014; Lugoboni et al., 2011a; Quaglio et al., 2012).
Studies on the subcutaneous infusion of flumazenil in the treatment of benzodiazepine withdrawal in a hospitalised population show the high potential of this method, although actually this kind of administration is not common (Hulse et al., 2013; Luger et al., 1990). Following the clinical experience of Hulse et al. (2013), we recently used a new kind of flumazenil subcutaneous administration through an elastomeric infusion pump. In this paper, we report data on 214 high-dose benzodiazepine dependent subjects treated with this method.
Methods
Clinical setting
This observational study refers to patients hospitalised in the Addiction Unit of the Department of Internal Medicine of the University Hospital of Verona, Italy, from January 2012 to July 2014. The Addiction Unit is a public health facility, offering stay and therapies free of charge. The ward has four beds entirely dedicated to patients undergoing detoxification from therapeutic and illicit drugs (benzodiazepines, alcohol, opioids, cocaine, nicotine, etc.). Every year approximately 160 patients are admitted, pursuant to a referral made by a physician or after directly contacting the Addiction Unit, following information obtained from the web or other patients. In recent years detoxification from benzodiazepines has become our main activity, representing about 60% of total detoxification procedures.
Inclusion criteria
The inclusion criteria were: age ⩾18 years; ongoing use of benzodiazepines for at least six months at an equivalent dose of diazepam (EDD) of more than 50 mg/day. Patients who, alone or with their physician’s help, had tried to discontinue benzodiazepines, without success because of severe withdrawal syndrome, were also included in the study. Comorbid substance use disorder had to be successfully treated prior to the admission and, in cases of opioid abuse, an adequate replacement therapy had to be set up.
Exclusion criteria
Exclusion criteria included pregnancy or breast feeding, lack of written consent, severe illness causing physical and psychological impairment. Mental illnesses were not regarded as criteria of exclusion unless they affected the cognitive functions and the cooperation of the patient. In case of major depression or personality disorder a psychiatric consultation was performed, in order to be sure that the patient was stable and capable of undergoing the therapy. Patients with less severe dependence (daily intake of less than five times the DDD) were excluded, and directed to their general practitioner. Seizure or epilepsy were not criteria of exclusion, considering that all patients received low doses of clonazepam and anti-epileptic therapy (Albiero et al., 2011; Lugoboni et al., 2011b).
The procedure was explained to all patients, including the use of off-label flumazenil. A written consent was required in order to receive the treatment. This study was approved by the ethics committee for clinical trials of the provinces of Verona and Rovigo with approval number 683CESC.
Flumazenil slow subcutaneous infusion (FLU-SSI)
Patients were treated with a solution containing 7 mg of flumazenil, obtained by diluting fourteen commercial vials (0.5 mg/5 ml) in 190 ml of saline solution . The flumazenil final solution (260 ml, 27 µg/ml) was infused subcutaneously for 7 days through an elastomeric pump, a small and light disposable medical device releasing a constant flow (1.5 ml/hour). Although a little less precise than other pumps, the elastomeric pump is extremely easy to use and allows a greater mobility. The infuser’s internal pressure is constant and the drug is delivered through a filter. We used the Baxter 2C1087K device connected to a butterfly needle inserted subcutaneously into the patient’s anterior abdominal wall (see Figure 1). The pump, releasing about 1 mg of flumazenil every 24 hours, was then placed in a small bag, which could be carried attached to the belt or on the shoulder.

Elastomeric pump with Baxter device connected through a butterfly needle inserted into the anterior abdominal wall.
During the FLU-SSI we administered clonazepam by mouth, every day in the evening, at a dose decreasing from 5–6 mg on the first day to 0.5–2 mg on the last day of flumazenil treatment. Patients were discharged from hospital either without any treatment or with a clonazepam daily low dose (⩽2 mg) for up to two months. In the case of addiction to clonazepam, clobazam was designated as an alternative.
A treatment with anti-epileptic drugs (e.g. 1 g/day of valproic acid) had been prescribed to all patients starting from 10 days prior to the admission and throughout the hospital stay. The treatment with anti-epileptic drugs also went on for a further 20–40 days after discharge.
A phone follow-up was performed after two months from discharge.
Clinical assessment and data collection
All patient data, including toxicological history, psychiatric disorders, allergies to medications, previous illnesses and/or surgical interventions, were collected by the medical staff during a screening interview, performed approximately 20 days prior to the hospital admission. The severity of benzodiazepine addiction (e.g. use of high dose, years of abuse, severe withdrawal symptoms during previous attempts to reduce or stop the abuse) was assessed by the medical staff according to Diagnostic and Statistical Manual of Mental Disorders criteria (American Psychiatric Association, 2013). The severity of psychopathology was evaluated using the clinical global impression scale, a well established research rating tool applicable to all psychiatric disorders, which can easily be used in clinical practice (Busner and Targum, 2007).
As stated above, seizures and epilepsy were not exclusion criteria, although they caused modifications in the procedure, such as higher doses of anti-epileptic prophylaxis and the presence of a family member in the room. During hospitalisation patients were monitored on a daily basis (blood pressure, body temperature, heart rate, respiratory rate, presence/absence of pain) with frequent laboratory tests. For safety purposes (emergency procedures) a peripheral intravenous catheter was inserted in the patient’s forearm or wrist. Finally, every day each patient completed the benzodiazepine withdrawal scale (BWS; 33 items each with a score of 0–4), in order to assess their withdrawal symptoms subjectively (Mintzer et al., 1999; Quaglio et al. 2012).
Benzodiazepine dosage
The benzodiazepine dosage was converted into DDD (1 DDD is the therapeutic daily dose established by the World Health Organization for any drug) in order to assess the gap between its therapeutic and addiction use. Furthermore, the dosage of the various benzodiazepines was transformed into EDD using one of the most accepted conversion tables, in which 10 mg of diazepam is equal to 1 mg of lorazepam, 2 mg of lormetazepam, 0.5 mg of clonazepam, 0.25 mg of triazolam, 20 mg of zolpidem, 3 mg of delorazepam, 0.5 mg of alprazolam (Galanter and Kleber, 2008).
Statistical analysis
Means, percentages and their 95% confidence intervals (95% CI) were used to compare the sociodemographic characteristics of patients, their medical history and the current drug addiction in relation to gender. The Wilcoxon rank-sum test has been used to analyse non-parametric data. Statistical analysis was conducted using SPSS 11.5 statistical software (SPSS version 11.5, SPSS Inc, Chicago, IL, USA).
Results
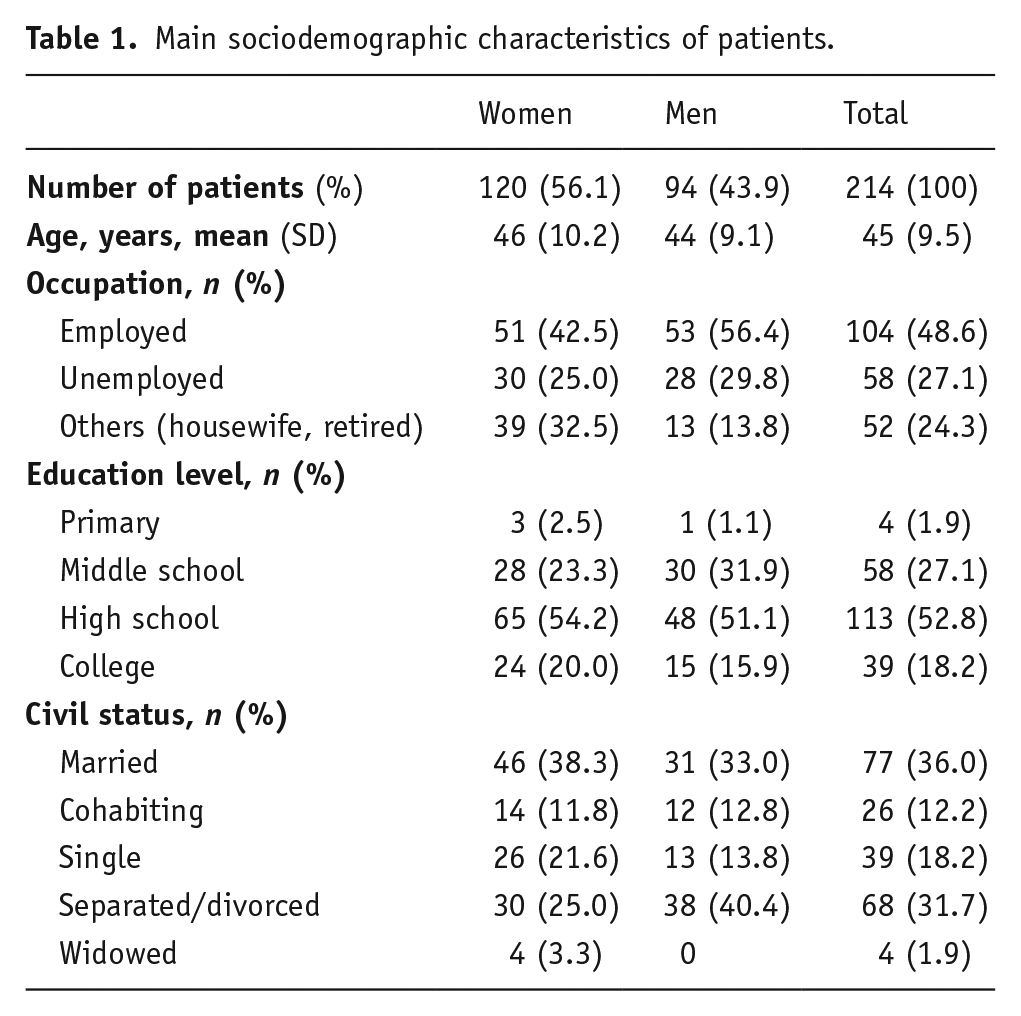
The main sociodemographic characteristics of the 214 patients treated with FLU-SSI, for addiction to high doses of benzodiazepines in the study period, are reported in Table 1. The mean age of the patients was 45 years, without significant difference related to sex. This is in line with the female/male ratio of the general Italian population for the corresponding age group (Italian National Institute of Statistics, 2011). The percentage of unemployed people was higher than the Italian population of the same age, while there were no differences concerning other characteristics. We noticed that 29 subjects (13%) were health professionals or had a degree in health care (eight doctors, six nurses, five psychologists, one pharmacist, nine others).
Main sociodemographic characteristics of patients.
Thirty-five per cent of patients lived in Veneto, while the remaining 65% came from other Italian regions. Among the latter, 171 subjects (80%) were from the north, 22 subjects (10%) were from the south and the islands and 21 subjects (10%) were from central Italy.
Ninety-two per cent of patients had a psychiatric diagnosis of which 63% was pertaining to the anxious depressive sphere.
Characteristics of past and current patients’ addiction are described in Table 2. Out of 214 high-dose benzodiazepine users, 118 (55.1%) had a history of illicit drug use and/or alcohol-related problems, with a higher incidence among men (74.5%). Fifty-eight patients with a positive history of addiction used only one substance (mainly alcohol), while 60 used more than one among the following: cannabis (46 cases), alcohol (45 cases), cocaine (43 cases) and opioids (38 cases, of which 21 were on opioid substitution therapy with methadone or buprenorphine).
History of addiction and clinical evaluation of patients admitted to detoxification.
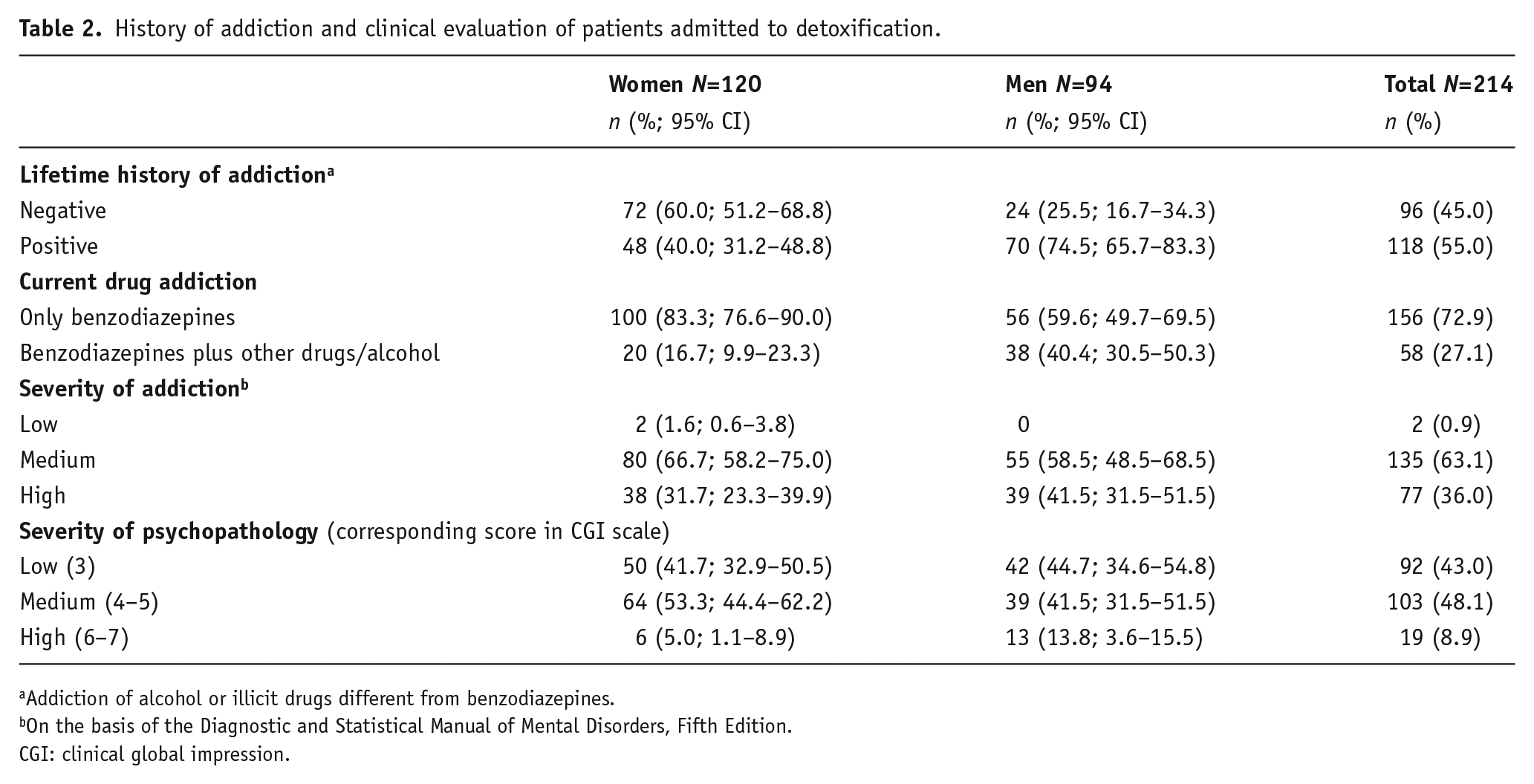
Addiction of alcohol or illicit drugs different from benzodiazepines.
On the basis of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
CGI: clinical global impression.
Without considering smoking, at the time of hospitalisation 156 subjects (72.9%) were addicted only to benzodiazepines, while the remaining 58 patients were addicted to more than one substance. The majority of women were hospitalised only for the benzodiazepine dependence (see Table 2). With regard to alcohol consumption, 124 patients (58%) had never had drinking problems, 54 (25%) had an addiction already in remission, while it was still active for 36 subjects (17%). Furthermore, 65% of subjects were smokers (72 women and 67 men), while 9% were ex-smokers. At the beginning of the detoxification programme, the severity of addiction was medium/high for almost patients, while only a minority of subjects presented with a form of severe psychopathology (8.9%).
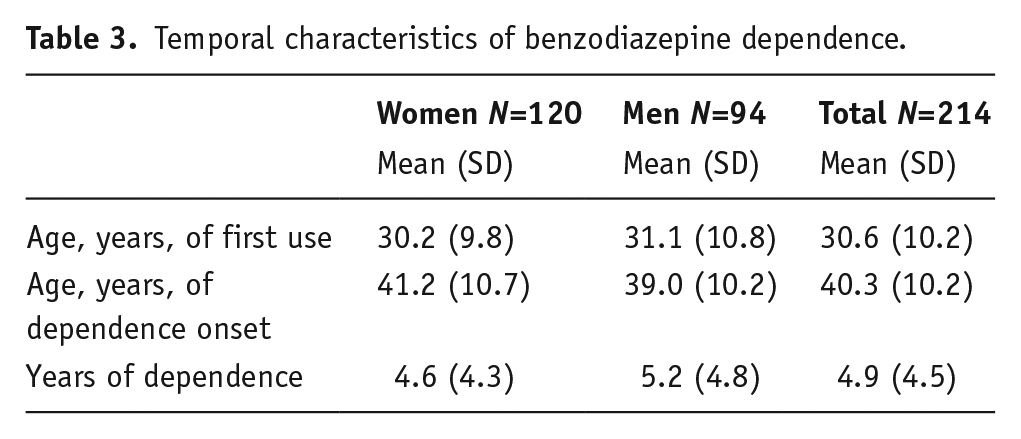
All patients were long-term benzodiazepine daily users, as shown in Table 3. In general, benzodiazepines had been used for the first time 10 years before the onset of the abuse. The mean duration of the abuse was 4.9 years, slightly higher for men than women. In about a quarter of our cases the benzodiazepine use started as a behavioural addiction, while the remaining 75% of patients started on medically prescribed benzodiazepines and had subsequently escalated the dosage. Almost all patients (96%) reported previous unsuccessful attempts to reduce or discontinue the benzodiazepines. For 60% of them the withdrawal symptoms were mild/medium, for the remaining 40% they were severe, and a subset of 22 subjects (10%) had also experienced seizures.
Temporal characteristics of benzodiazepine dependence.
At the time of hospitalisation, 155 patients (72.4%) were taking one benzodiazepine, 45 (21.1%) two benzodiazepines and 14 (6.5%) three or more. The most used benzodiazepine pharmaceutical formulation was the oral drops solution (149 patients, 69.9%), followed by capsules (48 patients, 22.4%). Sixteen patients (7.5%) used oral drops and capsules in association, whereas only one patient used an intravenous formulation.
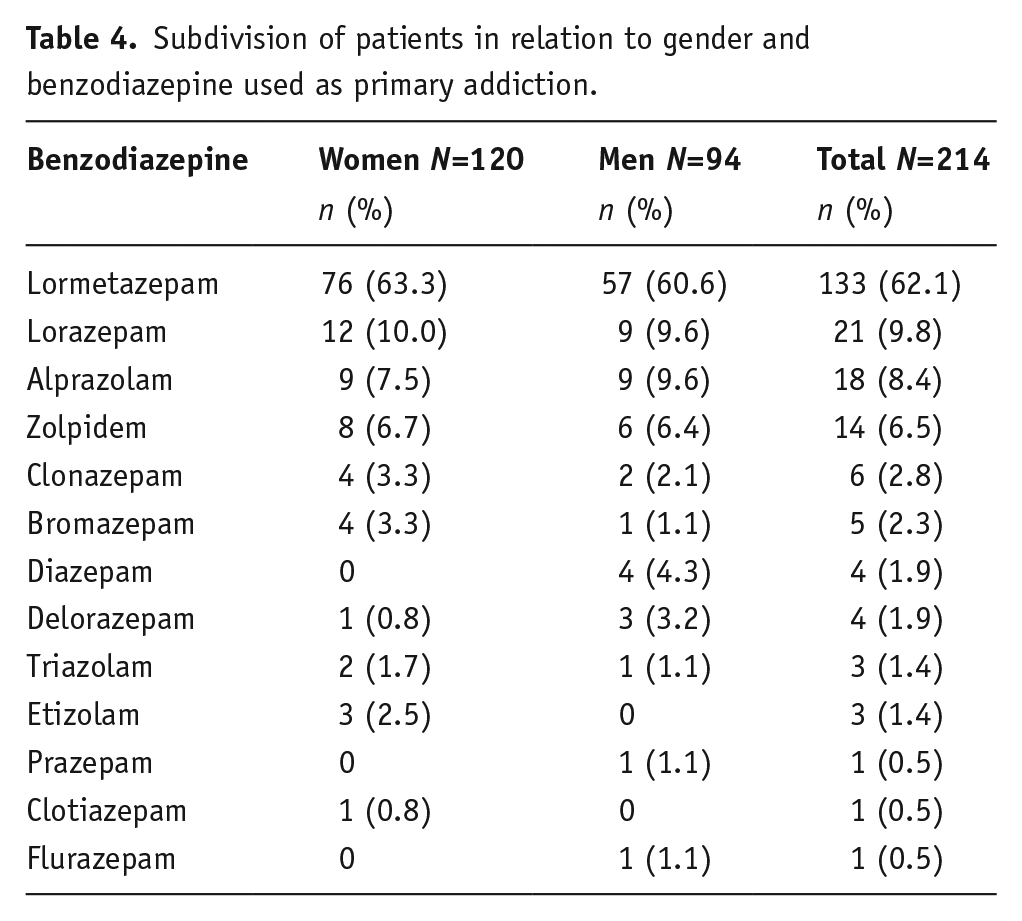
As shown in Table 4, most patients (62.1%) had lormetazepam as the primary addiction followed by lorazepam (9.8%) and alprazolam (8.4%), with no significant gender differences. Surprisingly, very commonly used benzodiazepines, such as diazepam, were not particularly relevant in our cases of severe addiction. No correlation between the use of lormetazepam and other considered variables, such as age, gender, comorbid substance use disorder, presence of mental illness or region of provenance was found (data not shown).
Subdivision of patients in relation to gender and benzodiazepine used as primary addiction.
The benzodiazepine dosage is reported in Table 5: lormetazepam (considering DDD) and lorazepam (considering EDD) were the benzodiazepines used at the highest dosage. The average EDD in the entire sample, considering also the association of more benzodiazepines, was 389 mg.
Benzodiazepine dosage used by patients. The benzodiazepines taken by at least 10 patients are reported.
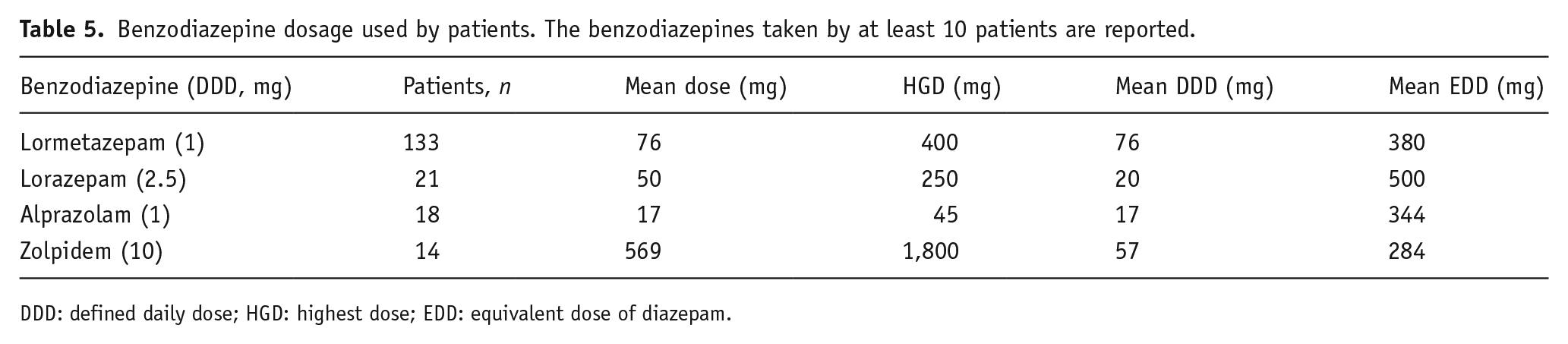
DDD: defined daily dose; HGD: highest dose; EDD: equivalent dose of diazepam.
During FLU-SSI treatment, 155 subjects (72.4%) completed the BWS, with individual daily scores ranging from 0 to 132. As shown in Figure 2, the initial mean score of women (n=85) was higher, although not statistically significant, than men (n=70), but the scores of both gender groups constantly decreased, from the first to the seventh day. During hospitalisation, 60 patients (38.7% of those who completed the BSW) had at least one daily score greater than 30, but among them only 13 (8.4%) always had a daily score over 30. For 22 subjects (14.2%) the treatment could be considered asymptomatic (daily score <5), while the remaining 73 subjects (47.1%) had a score between five and 30.
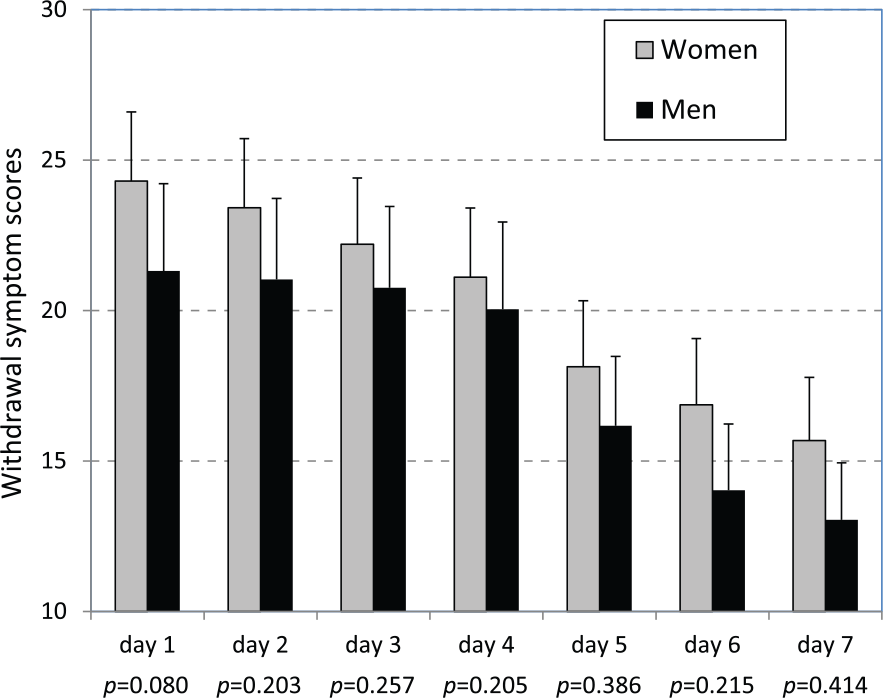
Scores of withdrawal symptoms measured, during the period of hospital detoxification, in 85 women and 70 men benzodiazepine users. Values are expressed as the mean score per day with standard error. On the x-axis, the P value of the Wilcoxon rank-sum test for the difference in the score distribution between the two groups is reported for each day.
The medical staff considered the withdrawal symptoms experienced by 64 subjects (29.9%) relevant, including two convulsive-like crises, which was quite consistent with the subjective evaluation of the patients. The detoxification procedure was interrupted only in two cases (0.9%): one on the third day for craving (polydrug abuser taking lormetazepam intravenously), the other on the second day for feeling uncomfortable in the hospital environment. Despite the fact that all patients had been given anti-epileptic drugs as prophylaxis, two patients experienced convulsions during the days following discharge (one patient had a positive medical history, while the other had a completely silent anamnesis).
As regarding the subcutaneous procedure, repositioning was required in only a few occasions, following accidental removal of the needle. No adverse reactions due to flumazenil were observed during the treatment.
The FLU-SSI treatment allowed 99% of patients to be detoxified from high doses of benzodiazepines. Twenty-six subjects (12.1%) achieved complete withdrawal from benzodiazepines, whereas 186 (86.9%) patients were discharged with a prescription of clonazepam at a low dose. We contacted by phone 149 out of the 214 patients (70%). At the time of the interview, 30 patients (20%) had relapsed to a high-dose benzodiazepine dependence, 49 patients (33%) continued to use clonazepam at a low dose two months after discharge and 70 (47%) did not used benzodiazepines any longer. We did not find any significant differences between women and men, as well as between mono and poly-drug abusers.
Discussion
Over the past few years, the use of partial agonists such as buprenorphine and varenicline in the treatment of opioid and smoking dependencies has increased significantly, whereas the use of flumazenil in the treatment of benzodiazepine dependence is spreading at a much slower rate.
Benzodiazepine addiction differs from other kinds of addiction, because many patients have no other substance use disorder in their medical histories and its relapse rate is much lower.
The intravenous administration of flumazenil with available pharmaceutical preparations has long been proved efficient in the treatment of benzodiazepine withdrawal syndrome (Gerra et al., 1996, 2002; Lader and Morton, 1992), and now its use is supported by several experts (Lader, 2011; Lader et al., 2009). Unfortunately, the use of such a procedure is not widespread, although our group has been applying it successfully on high-dose benzodiazepine users for about 10 years (Faccini et al., 2012; Lugoboni et al., 2011b; Quaglio et al., 2012).
The remark regarding the need for future research on the tolerability and effectiveness of the subcutaneous administration of flumazenil, which was stated in the only study published so far on the matter (Hulse et al., 2013), triggered the idea for this study. Both the Australian team’s and our results show the effectiveness of the subcutaneous infusion, which is a convenient alternative to intravenous administration. Even if we change the method of infusion, the symptoms of highly addicted patients are well controlled, grading from mild to moderate.
This is the largest case series ever reported of high-dose benzodiazepine users receiving FLU-SSI. The EDD usually taken by the patients of our study was significantly higher than the EDD in the research by Hulse et al. (2013) (389 mg vs. 169 mg). In part, this might be because it is so easy to buy benzodiazepines in Italy, although these drugs should not be dispensed by pharmacists without prescription. Many of our patients had bought benzodiazepines from complacent pharmacists, without the necessary prescription.
Our study shows that the benzodiazepine detoxification with FLU-SSI, even if not always achieving immediate benzodiazepine withdrawal (because of psychiatric conditions, high epileptic risk, sleeplessness, severe withdrawal symptoms), allows a quick transition (within 7 days) from very high to therapeutic doses of benzodiazepines, with an equally rapid disappearance of the craving. Furthermore, the follow-up data show that about 80% of the treated patients do not relapse to high doses of benzodiazepines (although admittedly this result is not necessarily linked to our procedure). FLU-SSI is likely to be accepted and performed by physicians who, although interested in the procedure, are afraid that administering flumazenil intravenously might trigger significant withdrawal symptoms, including convulsions. Furthermore, subcutaneous administration with an elastomeric pump allows an improved continuity of the infusion and avoids alarms ringing for the frequent variations in infusion speed, mostly caused by arm movements during night sleep.
In the research by Hulse et al. (2013), flumazenil was added to a neutral solution in order to reduce the risk of local skin irritation. In our study, flumazenil was diluted in a saline solution, inside the elastomeric pump, and no skin irritation was noticed around the insertion of the needle area. Unlike Hulse’s study, we used normal elastomeric infusers, which are cheap and easy to find on the market, factors worth considering in order to avoid what might hinder the use of this procedure.
Moreover, because elastomeric infusers are very light and compact, patients appreciated the greater mobility they allowed and rated them as painless, safe and comfortable, with no bound to the pump and respecting privacy about the therapy, whereas nurses acknowledged they required less time to manage.
The appraisal of nurses, who had previously administered flumazenil both intravenously and subcutaneously for at least one year, was assessed through an anonymous test. The nurses appreciated the subcutaneous infusion because it was easier to apply, it generated a smaller risk of professional accident, it solved the problem of difficult peripheral venous access, it only needed one single preparation at the beginning and the infusion was continuous, without any technical interruption. On the other hand, they remarked on a few weak points such as the scarce visibility of the inserting point of the needle, the partial limits to patients’ hygiene and the difficulty in appraising the exact duration of the infusion.
The standard dose of FLU-SSI used by Hulse’s team was significantly lower than what we used in our clinical practice during the last four years (1 mg/day for 7 days vs. 4 mg/day for 4 days). The choice of this dose of flumazenil, based on our eight years of previous flumazenil dose testing, was made to limit the risk of convulsions, therefore allowing the treatment of patients who are more prone to seizures. However, before applying FLU-SSI as a routine therapy more research about dosage and duration is needed and the safety of outpatient treatment has to be tested further, in particular to evaluate the convulsive risk.
According to our clinical expertise, another factor that needs to be considered is the patient’s body mass index. In the case of severe obesity, we suppose that a longer duration of the infusion might be more efficient than a higher dose and we would suggest investigating the matter further. Furthermore, as we believe flumazenil might play a role in the treatment of protracted withdrawal symptoms, we are waiting for a formulation suitable for use at home.
The present case series has some limits. First of all, the FLU-SSI method has not been directly compared with other detoxification methods. Secondly, our follow-up data are scarce, because some patients have only recently been discharged, whereas others have been followed for two years. In any case, to our knowledge no negative events directly linked to the procedure occurred. Furthermore, a number of aspects concerning this therapeutic approach need to be clarified, and some questions are still to be answered: for example, what is the minimum diazepam-like benzodiazepine dosage threshold and what is the minimum duration of the continuous use of benzodiazepines for recommending FLU-SSI treatment? As regarding the procedure, given the potential side effects and the difficulties concerning dosage, studies comparing intravenous and subcutaneous administration need to be carried out. The risk of seizure is a matter of concern, which could prevent a more extensive use and the appropriateness of an adjunctive therapy should be taken into consideration.
In conclusion, our data support FLU-SSI as a possible efficient strategy for detoxification of patients with long-term high-dose benzodiazepine addiction, and could become a routine treatment as long as the necessary further studies on dose, duration of infusion and safety issues are carried out (Lugoboni and Leone, 2012).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.