
Abstract
Aims:
The purpose of this study was to compare the effects of mephedrone and 3,4-methylenedioxy-methamphetamine (MDMA), as reported by young recreational polydrug users.
Methods:
152 MDMA users and 81 mephedrone users were recruited through snowballing on social network sites. They completed a standard online questionnaire for either mephedrone or MDMA. The questions covered the average amount taken per session, the longest duration of usage in the last 12-months, subjective effects while on-drug, and recovery effects in the days afterwards.
Results:
Mephedrone users reported a significantly longer maximum session of use than MDMA users. Mephedrone users also reported a significantly greater average amount used per session. The majority of on-drug subjective ratings did not differ between drugs, with similar increases in entactogenic effects. Although mephedrone users did report significantly more frequent issues with sleeping, anger and anxiety. In relation to recovery, mephedrone users reported more frequent craving, nasal irritation, paranoia, and relationship difficulties. Mephedrone users also rated general recovery effects as more severe over the seven-day period following use, taking more days to feel normal.
Conclusions:
The acute effects of MDMA and mephedrone were broadly similar. However, the recovery period for mephedrone was more enduring, possibly due to the longer duration of acute session usage.
Introduction
3,4-Methylenedioxy-methamphetamine (MDMA) is a synthetic phenethylamine and ring-substituted methamphetamine derivative, used recreationally for its stimulant and entactogenic effects (Boys et al., 2001; Vollenweider et al., 1998). MDMA is a potent indirect monoaminergic agonist and reuptake inhibitor, demonstrated through its actions on the serotonin and dopamine systems (Green et al., 2003). MDMA also affects the hypothalamic-pituitary-adrenal axis and neurohormonal system, causing pronounced increases in cortisol secretion (Mas et al., 1999; Harris et al., 2002). Since its first recreational usage during the 1980s (Shulgin, 1986), MDMA became the most favoured (Bean et al., 1997 cited in Smith et al., 2009), prevalent (Deehan and Saville, 2003), and purchased (Barratt et al., 2014) recreational stimulant in the 1990s and early 2000s. Recreational MDMA usage was initially characterized by intermittent single dosages (Davison and Parrott, 1997), although this evolved into more intensive patterns of usage (Kish et al., 2010; McCann et al., 1999).
Mephedrone is a substituted β-keto amphetamine (Green et al., 2014) and member of the cathinone class. It is another recreational stimulant with entactogenic properties (Kapitány-Fövény et al., 2013), and subjective experiences broadly comparable to those of MDMA (Carhart-Harris et al., 2011). Despite these self-reported similarities, Green et al. (2014) described many pharmacological differences between the two drugs. They included a lack of serotonergic neurotoxicity with mephedrone (Angoa-Pérez et al., 2011), which contrasted with MDMA’s neurotoxic potential (Ricaurte et al., 2000). Mephedrone is one of many novel psychoactive substances (NPS) that have been used for recreational purposes during the last decade (Corazza et al., 2013; European Monitoring Centre for Drugs and Drug Addiction, 2010; Winstock and Ramsey, 2010). However, amongst these many NPS, only mephedrone has become an ‘established part of the recreational drug scene’ (Wood et al., 2012: 959).
The core focus of the present study was to compare the patterns of usage and self-rated effects of mephedrone and MDMA, both on-drug and during the recovery period. Pharmacological research in animal models (Kehr et al., 2011; Shortall et al., 2013), drug market investigations (Brunt et al., 2011), and self-report studies of human users (Carhart-Harris et al., 2011; Kapitány-Fövény et al., 2013) indicate many parallels between the two substances. In a review of the acute subjective effects of MDMA, Baylen and Rosenberg (2006) reported a range of emotional effects on drug (euphoria, affection, sociability), accompanied by psychophysiological changes (bruxism, increased body temperature, greater energy). These effects are followed by a range of deleterious moods when recovering from MDMA (Parrott and Lasky, 1998; Parrott et al., 2008). Serotonin disturbance has been suggested as an underlying mechanism for these ‘mid-week’ recovery problems (Curran and Travill, 1997). The chronic use of MDMA has also been associated with significantly greater depression than in controls (Brière et al., 2012; McCardle et al., 2004), with serotonergic disruption again suggested as a potential causal mechanism. Similar neurochemical explanations are posited for the sleep disturbances found with recreational users (Allen et al., 1993; McCann and Ricaurte, 2007; Randall et al., 2009).
Turning to mephedrone, Winstock et al. (2011b: 1991) reported ‘typical stimulant-related subjective effects’, with feelings of euphoria, increased energy, and insomnia. Kapitány-Fövény et al. (2013) found that the subjective effects of mephedrone and MDMA were broadly similar, particularly regarding their entactogenic and psychostimulant properties. Freeman et al. (2012) also reported increases in stimulant-typical subjective effects, and noted that wanting more mephedrone was primed by its consumption. Indeed, the repeated compulsion to use mephedrone may be related to its dopaminergic actions (Hadlock et al., 2011). Literature related to the post-mephedrone recovery period is more ambiguous. Van Hout and Brennan (2011: 4) suggested a ‘lack of negative comedown symptomatology’. In contrast, McElrath and O’Neill (2011: 3) reported a case study of a male suffering ‘very negative comedown periods which continued for up to four days’.
Winstock et al. (2011b) describe the difficulty in recruiting the hidden user populations of these emerging drug types and suggest the Internet as the most appropriate approach. Since the Internet played a pivotal role in the rise of mephedrone (Vardakou et al., 2011), it may also represent the ideal method of accessing these same hidden populations.
Green and Nutt (2014: 1) suggested: ‘Pharmacology should be at the center of all preclinical and clinical studies on new psychoactive substances’. However, they noted that many novel methodological procedures may need to be implemented. Hence, Internet surveys remain a useful approach for nascent NPS research.
In summary, the current research was designed to directly compare the subjective effects of each drug, as reported by two groups comprising predominantly-mephedrone users and predominantly-MDMA users. The effects of mephedrone and MDMA use appear broadly equivalent; a null hypothesis of similar effect ratings is therefore posited. However, due to a lack of previous direct comparisons, potential disparately rated effect frequencies will be of particular interest.
Method
This was an Internet-based cross-sectional survey approved by the Swansea University Ethics Committee. The survey was predominately delivered via the social networks of Facebook and Twitter during mid-2014. Participation was open to anyone over the age of 18 years, took approximately 30-40 min, and was anonymous. Participants were recruited via ‘snowball’ sampling (Solowij et al., 1992) and answered questions regarding their experiences with mephedrone or MDMA in the last 12 months (see Supplementary Material). A variety of substance misuse issues (e.g. functions of use, opinions on drug testing services) were addressed; however, only questions regarding demographics, consumption patterns and subjective effects are reported here. The inclusion criterion for the polydrug cohorts was the multiple uses of either mephedrone or MDMA. Participants gave informed consent and were asked which of the following statements best applied to themselves. The MDMA group reported that they had ‘used MDMA multiple times and had more experience with this substance’. The mephedrone group reported that they had ‘used mephedrone multiple times and had more experience with this substance’. Many individuals reported that they had ‘used neither of these drugs more than once’, and were excluded from this report. Options included statements indicating experience with one substance or use of ‘both substances multiple times’, and a decision to answer on one of the substances being compared due to having ‘more experience with this substance’. These statements allowed for allocation of participants to groups and identification of those who had used both substances.
Assessment measures
The University of East London Recreational Drug Usage Questionnaire (Parrott et al., 2001) was extended to cover the previous 12 months, and to include several NPS. Participants reported if they had ever taken a drug and, if so, how many times in the past 12 months. This was followed by a questionnaire concerning subjective effects experienced during, and recovering from, the use of either MDMA or mephedrone. This questionnaire was based on a combination of previous quantitative (Winstock et al., 2011b) and qualitative measures (Van Hout and Brennan, 2011). Participants also reported the age at which they first used the drug in question, their longest session of usage (in hours) in the past 12 months and the average amount consumed/session (in g).
The subjective effect questions were based on Winstock et al. (2011b), with the Likert-type scales extended from three to five points. Participants answered the question ‘Have you ever experienced any of the below while taking mephedrone/MDMA, if so, how often does this happen?’ using a five-point Likert-type scale (never, rarely, sometimes, most times, every-time; scored 0–4). Following the rating procedure, a comment box was used to collect any further effects of mephedrone use reported.
Participants were then presented with another list of subjective effects and asked ‘Have you experienced any of the below while RECOVERING from taking mephedrone/MDMA?’ Participants were next asked to ‘rate the intensity of these issues over the days after taking mephedrone/MDMA’. Participants rated the general recovery effect intensity each day for a 7-day period following use on a five-point Likert-type scale (feeling normal, a little worse than usual, fairly worse than usual, much worse than usual, the worst I have felt). These seven scores were combined to create the cumulative intensity measure. The ‘days before feeling normal measure’ was calculated by recording the day following drug use on which participants reported ‘feeling normal’.
Data analysis
Comparisons of gender across groups employed a chi-square test of independence. All other comparisons were carried out by independent samples t-test and SPSS (version 20; SPSS Inc.) was used for all analyses.
Results
A total of 81 participants indicated greater experience with mephedrone, while 152 participants indicated greater experience with MDMA. There were some missing individual data, however, the lowest number of respondents to a question was 94% of the total sample.
The 12-month drug frequency data, average amount consumed per session, longest session in 12-months and composite seven-day intensity were ranked in order to control for outliers. In all comparison tables, the unranked means are each displayed. Results of the Welch-Satterthwaite method are reported in cases in which a Levene’s test indicated heterogeneity of variance. This is indicated by (W) in tables and in the text.
Table 1 summarizes demographic data. The mean age of the MDMA group was 25.6 (standard deviation (SD)=6.3), and in the mephedrone group it was 25.4 (SD=6.9), independent t-tests revealed that the two groups did not differ significantly in age, t(231)=−0.233, p=0.816. A chi-square test for independence was conducted between group and gender. All expected cell frequencies were greater than five. There was no statistically significant association between group and gender, χ2(1)=0.56, p=0.453.
Group means (standard deviation (SD)) of demographic and descriptive drug use data.
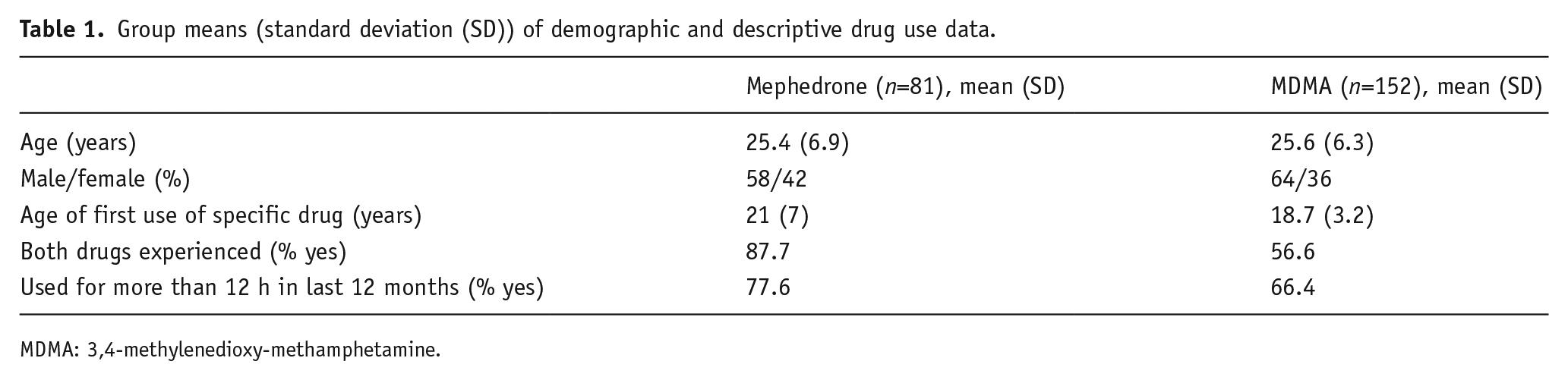
MDMA: 3,4-methylenedioxy-methamphetamine.
The only 12-month drug usage frequencies found to significantly differ were the frequencies relevant to the allocation of participants to groups. Those in the MDMA condition reported greater 12-month frequency of MDMA use and those in the mephedrone condition reported more frequent mephedrone use (Table 2). Independent t-tests indicated no significant differences between groups in terms of disparity between frequency of use of the drug being answered on and the comparison drug, t(W, 92.04)=−0.356, p=0.779. The groups did not differ in terms of total frequency of drug use other than the compared substances, t(231)=1.306, p=0.193.
Group means (standard deviation (SD)) and analysis of variance (ANOVA) comparisons of 12-month drug frequency data.
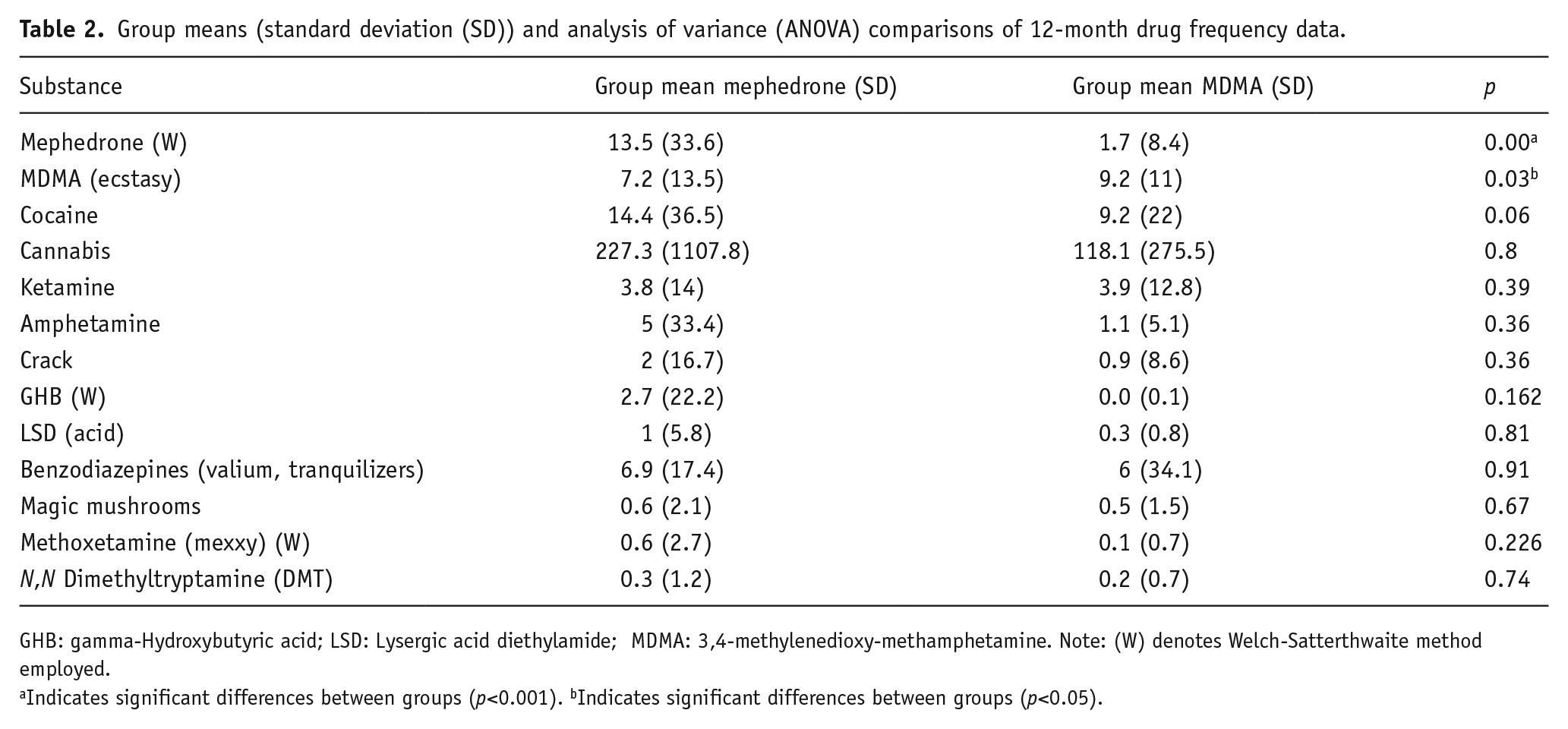
GHB: gamma-Hydroxybutyric acid; LSD: Lysergic acid diethylamide; MDMA: 3,4-methylenedioxy-methamphetamine. Note: (W) denotes Welch-Satterthwaite method employed.
Indicates significant differences between groups (p<0.001). bIndicates significant differences between groups (p<0.05).
Mephedrone users reported a greater mean frequency of the majority of substances probed, indicating a broader experience of illicit drug use. For example, a trend for greater frequency of cocaine use was found in the mephedrone group. However, these trends did not reach significance. Although there were no significant differences in specific drug frequency, there was a trend for greater frequency of use in mephedrone users (Table 3). Mephedrone users reported a significantly older age of first use of the drug specifically being reported on, t(W, 96.12)=2.72, p=0.008. Mephedrone users also reported a significantly greater longest session of use in the previous 12 months and a greater average amount used per session (Table 3).
Group means and standard deviation (SD) of drug usage and recovery intensity data.
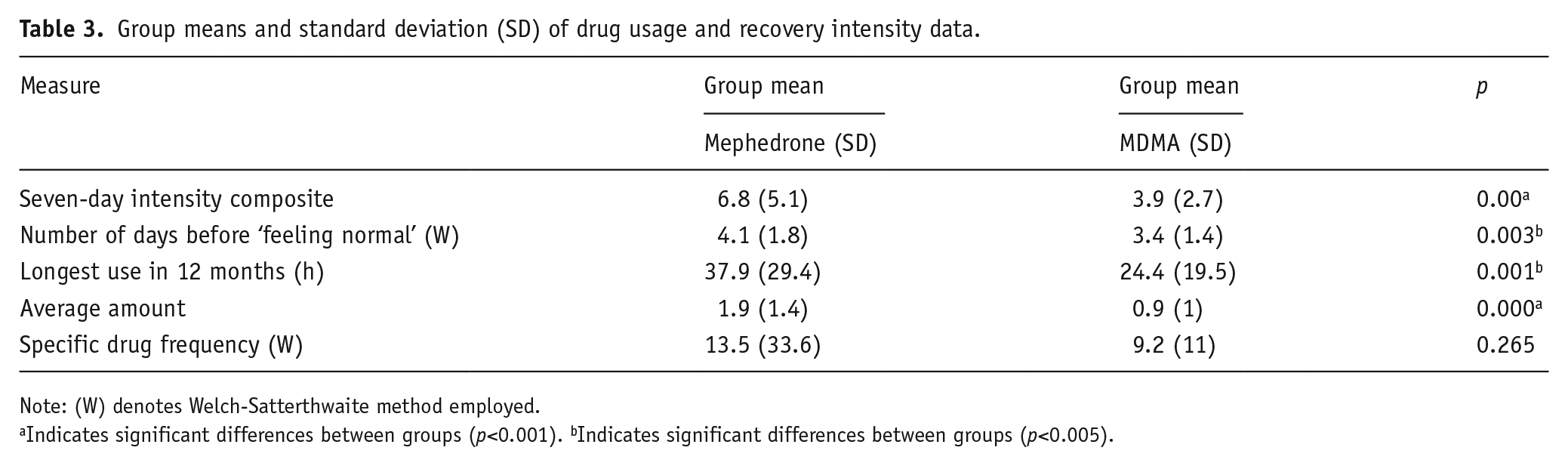
Note: (W) denotes Welch-Satterthwaite method employed.
Indicates significant differences between groups (p<0.001). bIndicates significant differences between groups (p<0.005).
Table 4 details the comparisons of on-drug frequencies; the large majority of on-drug effects did not significantly differ between groups. However, mephedrone users reported a significantly greater frequency of issues with sleep, anger, and anxiety. In relation to recovery, mephedrone users rated a significantly greater frequency of craving for more drug, paranoia, nasal irritation, and ‘difficulties with relationships resulting from the weekend’s mephedrone use’ (Table 5). Mephedrone users reported a significantly longer period before ‘feeling normal’ after drug use and rated the cumulative seven-day intensity of the recovery effects as significantly greater than MDMA users (Table 3). The group mean intensity scores across the seven-day period are displayed in Figure 1; mephedrone users rated a greater intensity of recovery effects on each of the seven days following drug use. Mephedrone users reported that mephedrone continued to provide an effective hit throughout a drug use session in a comment box that followed rating effects.
Group means (standard deviation) and t-test data of on-drug effects.
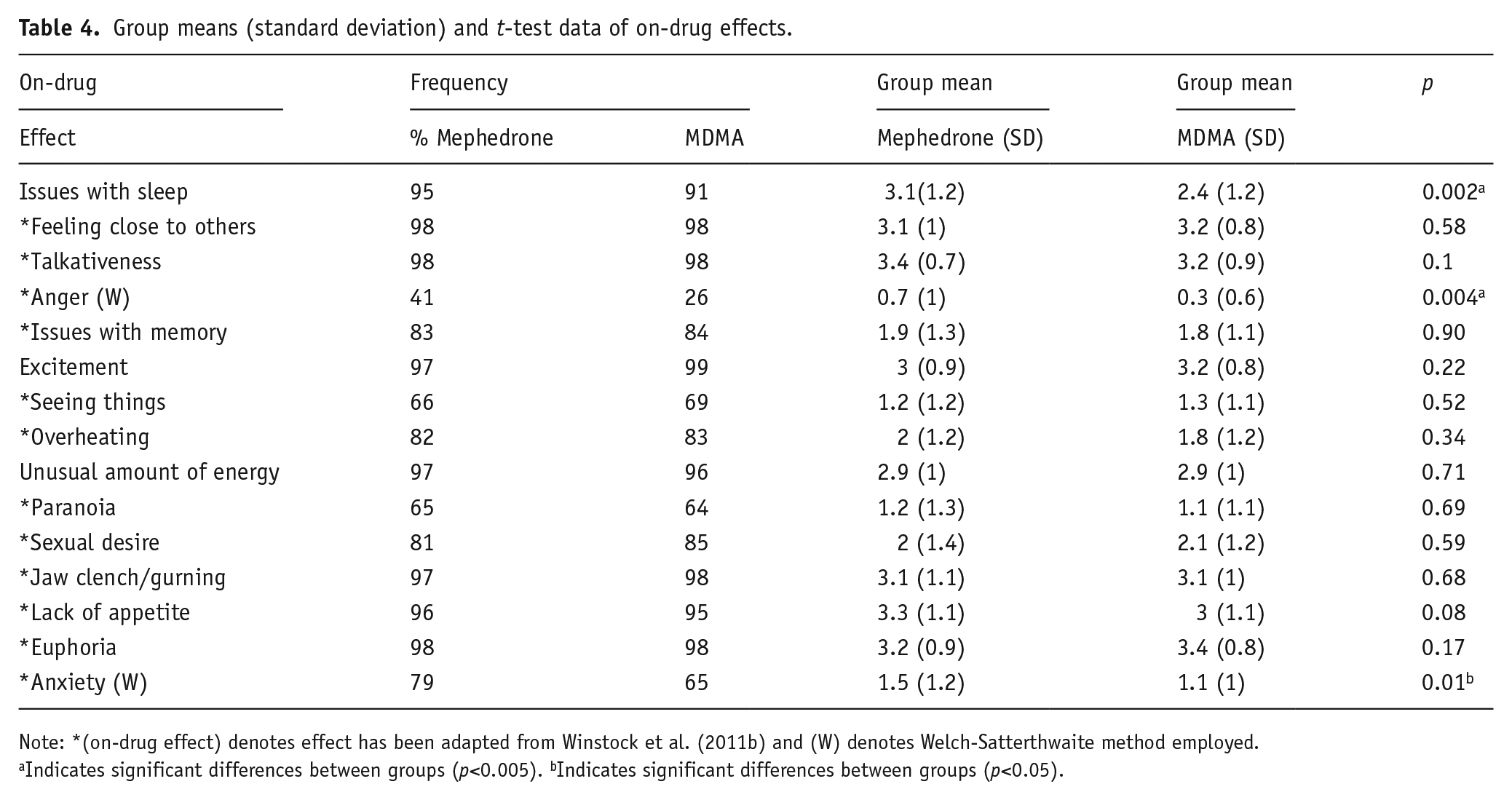
Note: *(on-drug effect) denotes effect has been adapted from Winstock et al. (2011b) and (W) denotes Welch-Satterthwaite method employed.
Indicates significant differences between groups (p<0.005). bIndicates significant differences between groups (p<0.05).
Group means (standard deviation) and t-test data of recovery effects.
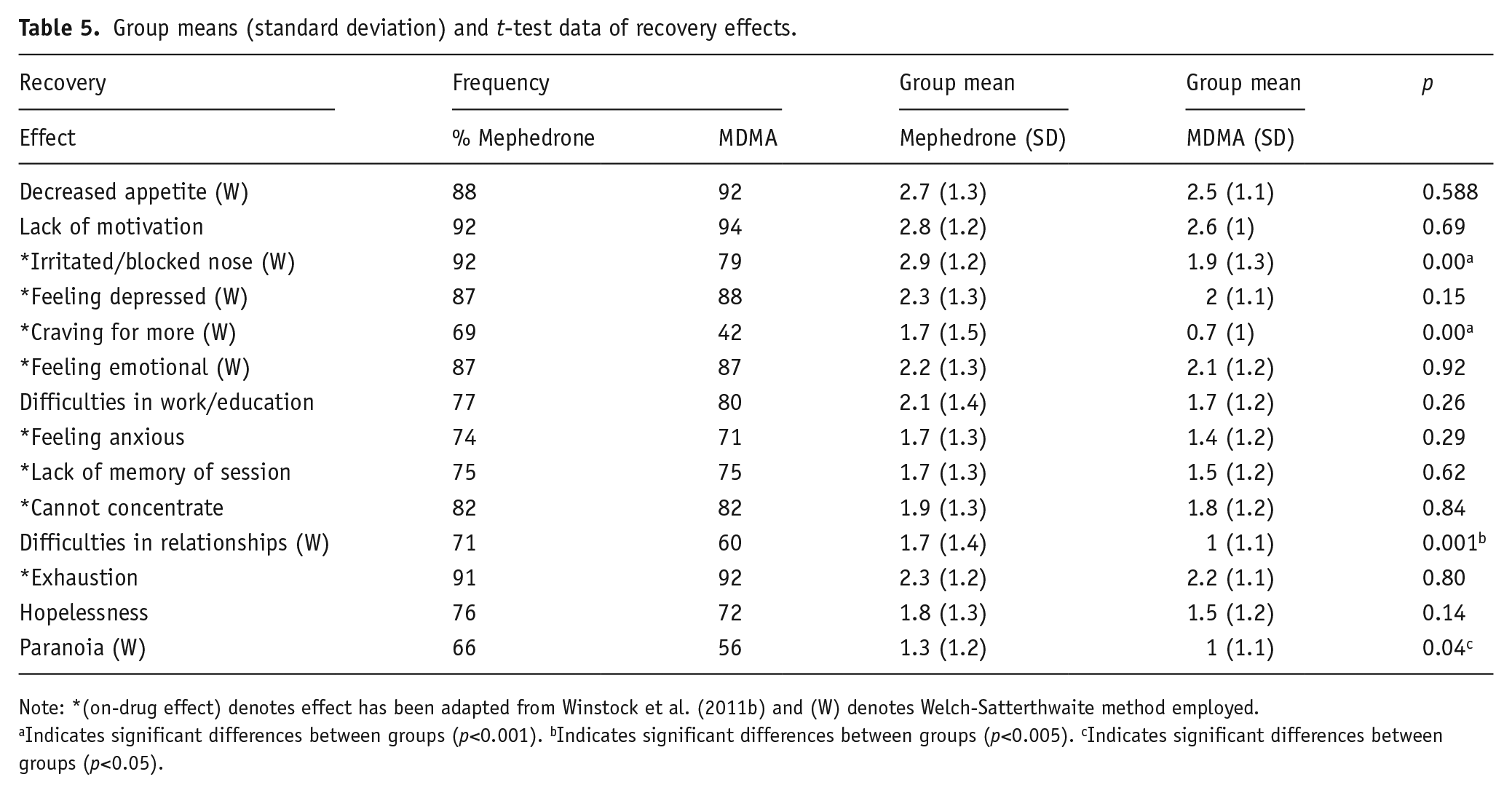
Note: *(on-drug effect) denotes effect has been adapted from Winstock et al. (2011b) and (W) denotes Welch-Satterthwaite method employed.
Indicates significant differences between groups (p<0.001). bIndicates significant differences between groups (p<0.005). cIndicates significant differences between groups (p<0.05).
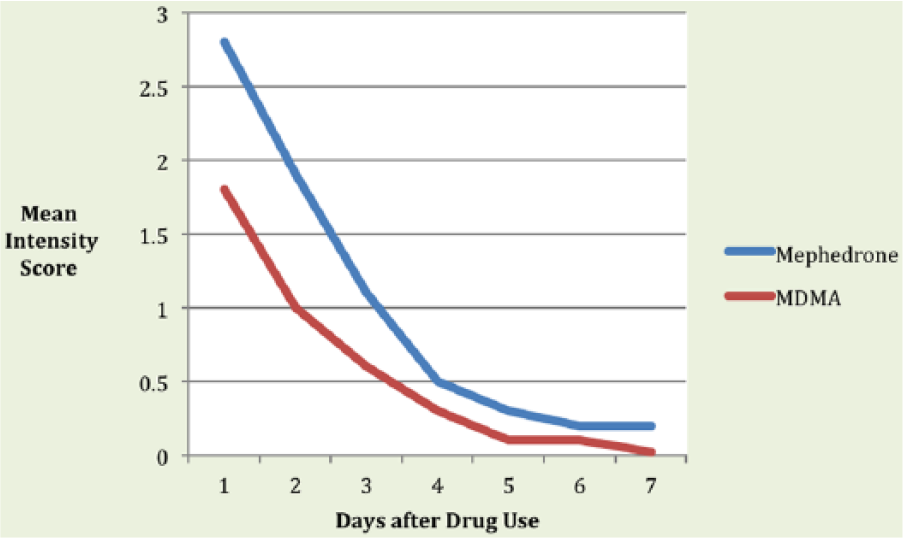
Graph to show group mean recovery intensity scores at each of the seven days following drug use. These groups also differed significantly in terms of amount of drug consumed on average per session and longest session of use in last 12 months. MDMA: 3,4-methylenedioxy-methamphetamine.
Discussion
The entactogenic and stimulant effects of mephedrone and MDMA, as described by the two groups of recreational users, were broadly similar. In particular, feeling close to others, greater talkativeness, increased feelings of energy, and feelings of excitement, were given very similar on-drug frequency ratings by each user group (Table 4). We believe this is the first study to directly compare the effects of each recreational substance, although the findings agree closely with previous reports. For instance, Kapitány-Fövény et al. (2013) found mephedrone users reported substantial similarities between mephedrone and MDMA. Carhart-Harris et al. (2011) also found 49% of a mephedrone-using sample reported that MDMA was the substance with subjective effects most similar to mephedrone. The similarly rated effects of these substances are congruent with past parallels indicated by animal research (Shortall et al., 2013). The current findings also agree with previous summaries of the acute mood effects of each individual drug, for both MDMA (Baylen and Rosenberg, 2006; Parrott et al., 2001), and mephedrone (Schifano et al., 2011; Wood et al., 2010a). Winstock et al. (2011b) similarly noted that the subjective effects of mephedrone were comparable to the typical effects of all recreational stimulants, a conclusion also reached in the psychobiological review by Parrott (2015). Furthermore, Winstock et al. (2011b), and the current study, each found that mephedrone users reported frequent experiences of euphoria, bruxism, overheating, and a lack of appetite when on-drug.
There were, however, a number of differences between the two drugs. In particular, different ratings emerged for the questions regarding sleep, anger, and anxiety (Table 4). Acute sleep issues have been previously reported with both substances. Randall et al. (2009: 1513) have demonstrated acute sleep disturbances in MDMA use, with MDMA users exhibiting ‘hyperarousal and impaired REM function’. McCann and Ricaurte (2007) reviewed animal studies and human evidence, indicating that MDMA could lead to sleep disturbance. Turning to mephedrone, ‘insomnia at end of session’ was the second most prevalent withdrawal-related effect in a previous survey of mephedrone users (Winstock et al., 2011b). In the current study, acute difficulties with sleep were more pronounced within mephedrone users than MDMA users, as indicated by higher frequency ratings. Furthermore, the mephedrone cohort also indicated a relatively greater frequency of anxiety. Heightened anxiety in abstinent MDMA users has been indicated through greater scores on the anxiety sub-scale of the Symptom Checklist-90 (SCL-90; Parrott et al., 2000). Corroborative findings are provided by research reporting heightened levels of the stress hormone cortisol in MDMA users (Gerra et al., 1998; Parrott et al. 2008, 2014). In regards to mephedrone, Wood et al. (2010b) describe anxiety symptoms when detailing a case study of mephedrone use and Wood et al. (2010a) found agitation to be the most common symptom observed within mephedrone-related presentations to emergency departments.
There have been previous reports of an association between recreational MDMA use and anger, with significantly elevated SCL-90 ‘hostility’ levels in abstinent MDMA users (Parrott et al., 2001). Curran et al. (2004) also observed an angry cognitive bias in the days following MDMA use, while Reid et al. (2007) reported a higher incidence of aggressive behaviour in those with a higher lifetime usage of MDMA. In relation to mephedrone and anger, aggression was the most common clinical feature enquired about when healthcare professionals contacted the National Poisons Information Service regarding this substance (James et al., 2011). Mephedrone users in the current study reported anger at a comparably greater frequency, although replication of these findings is certainly required.
In relation to the post-drug recovery effects, the majority (71%) of those investigated were similar for the two cohorts. Hence, the two drug user cohorts provided similar ratings for decreased appetite, lack of motivation, exhaustion, feeling emotional, feeling depressed, and other effects. Depressed mood and sadness in the post-MDMA recovery period has been previously reported (Curran and Travill, 1997; Parrott and Lasky, 1998). In support of this, 88% of the MDMA cohort reported depression in the recovery period. Mephedrone and MDMA users reported a similar frequency of depression and hopelessness in recovery. Several recovery effects were, however, rated differently by users of these substances (Table 5): the physical problem of an irritated nose, the psychological problem of drug cravings, the psychiatric issue of paranoia and the psychosocial problem of ‘difficulties with relationships resulting from the weekend’s mephedrone use’. In each case these were rated as more frequent in mephedrone use. In an early mephedrone survey (Winstock et al., 2011b), a congested nose was among the most frequent and intense withdrawal symptoms reported. An irritated nose was among the recovery effects currently rated at a greater frequency by mephedrone users, an effect caused by rapid re-dosing via nasal insufflation. MDMA is typically consumed orally (Smith et al., 2002; Topp et al., 1999) and mephedrone is typically consumed via nasal insufflation (Carhart-Harris et al., 2011; Winstock et al., 2011a), these differing administration routes may underlie the disparate nasal irritation ratings. However, research describing the corrosive nature of mephedrone cutting agents and synthesis by-products (Walker, 2011) highlights mephedrone as particularly damaging to the nose.
Paranoia has been previously reported within the on-drug mephedrone experience (Centers for Disease Control and Prevention, 2001; Kelly, 2011; Winstock et al., 2011b). In relation to MDMA, greater levels of paranoid-ideation have been found within abstinent users when measured using the SCL-90 (Parrott et al., 2001). Potential for paranoia to occur at a comparably greater frequency when recovering from mephedrone use is evidenced by current findings. Unsociability in the recovery period following MDMA use has also been previously reported (Parrott and Lasky, 1998). No past literature has directly investigated sociability in the recovery period of mephedrone. However, Winstock et al. (2011b) report that 64% of their sample experienced ‘irritability’ in mephedrone withdrawal. Current data suggests relatively more frequent social issues are associated with mephedrone recovery. This finding may reflect the psychosocial impact of a more intense and enduring recovery period caused by long periods of intense mephedrone usage.
Bingeing on MDMA was initially rare (Winstock, 1991) and intermittent single dosages formed the typical pattern of use (Davison and Parrott, 1997). However, later surveys identified a rise in MDMA bingeing (Winstock et al., 2001). In contrast, the considerable abuse liability of mephedrone has been widely described in the early literature (Brunt et al., 2011; Winstock et al., 2011b; Wood et al., 2010b). Winstock et al. (2011b: 1995) describe how mephedrone ‘induces a strong and repeated compulsion to use’. More recent findings also identify mephedrone use as associated with a greater ‘urge to use more’ than MDMA (Uosukainen et al., 2015). In concordance with this literature, users reported a relatively greater frequency of ‘cravings for more drug’ when recovering from using mephedrone. Past implication of dopamine in drug cravings (Volkow et al., 2006) and disparate action of the compared substances on dopamine (Kehr et al., 2011) suggest this neurochemical as a likely mediator.
Two possible explanations of the differences found in both on-drug and recovery effects are suggested. Firstly, it may be potential differences in the respective psychopharmacology of these substances (Green et al., 2014; Kehr et al., 2011); or, it may be due to differing patterns of drug usage. 12-Month drug use frequency of the substance being specifically reported on did not significantly differ between groups (Table 3), indicating a similar number of recent drug use sessions. However, in support of the latter explanation, mephedrone users reported using the drug in a significantly more intensive pattern of use within sessions. Mephedrone users reported a significantly greater average amount consumed per session and a significantly greater longest session of use (Table 3). The average amount consumed per session reported by the mephedrone cohort (1.9 g) was substantially higher than averages reported in earlier work, in which 65% of users reported using 0.5 g or less per session (Carhart-Harris et al., 2011). The mephedrone cohort employed within this study may represent users with particularly intense usage; in lighter users of mephedrone, the reported effects may be more similar to MDMA. This degree of mephedrone consumption may underlie the greater frequency of recovery effects and more severe recovery period associated with the use of mephedrone.
A comparably more intense and enduring recovery period is associated with mephedrone when compared to MDMA. Current findings support the long recovery periods reported by McElrath and O’Neill (2011) and conflict with reports of a lesser mephedrone comedown experience (Van Hout and Brennan, 2011, 2012). The suggestion that users perceive greater harms associated with mephedrone use than MDMA use (Carhart-Harris et al., 2011) is also corroborated. The greater severity of the mephedrone recovery period is likely related to longer sessions in which users consume larger amounts. Mephedrone users commented that after successive doses the use of mephedrone continued to generate an effective hit. This suggests that mephedrone was not leading to acute pharmacodynamic tolerance. This may help explain why in this study the users reported using mephedrone over extended periods of time. These authors are not aware that this has been previously reported. Hence, this needs to be further empirically studied. The strong compulsion to use mephedrone, and the apparent lack of acute pharmacodynamic tolerance, may underlie its more frequent and intense recovery effects. Greater consumption may also underlie the more frequent on-drug effects reported by mephedrone users. However, there may also be a pharmacological explanation for its more intense usage. The role of dopamine in reward systems and drug addiction has been widely described in the past literature (Childress et al., 1999; Di Chiara et al., 2004). Rapid and fleeting action on dopamine and a shorter half-life associated with mephedrone (Green et al., 2014; Kehr et al., 2011) may underlie differing consumption patterns (Farré et al., 2015), and in turn mediate the more frequent subjective effects and more severe recovery period reported by mephedrone users.
Herzig et al. (2013) concluded that the decline in cognitive functioning found across the pre and post mephedrone clubbing experience was primarily due to prior polydrug use. Of the drugs currently probed, only mephedrone and MDMA were found to significantly differ, suggesting largely uniform polydrug use across groups. A lack of differences between relative frequency of compared substances use, and between total frequency of other substance use, further substantiates similar polydrug use patterns. However, the current study does not account for polydrug use prior to the 12-month period before testing and the potential for associated depression likely to influence cognition.
Various limitations need to be considered when interpreting this work. Recall bias and polydrug contamination of subjective effect responses are characteristic issues of survey methodology relevant to current findings. A heavy reliance on self-nomination and self-report also represent current limitations. However, a self-report approach employing samples from an appropriate sentinel population is an adequate means of accruing data concerning NPS trends (Topp et al., 2004). More specifically to this work, the current cohorts are smaller than that of studies that have employed forum staff to formally aid recruitment.
Past surveys regarding mephedrone largely relied upon drug discussion boards for recruitment of large samples (Carhart-Harris et al., 2011; Winstock et al., 2011a). It could be argued that these means are further biased to a particular subgroup of experienced users (i.e. those liable to regularly document and report their use). The current smaller sample could be argued to be more naturalistic and representative of average stimulant drug users.
Future naturalistic studies should build on current findings and specifically investigate the subjective effects highlighted as more frequent in mephedrone users, especially those related to craving. Future emphasis on potential dopaminergic actions and psychobiological effects found to be more prevalent in the mephedrone using cohort will negate problematic multiple comparisons currently found. Naturalistic investigation focused on relevant effects and involving measurement of dopamine would represent consideration of the role of a suggested neurochemical mechanism within a more advantageous design.
Mephedrone’s effects on dopamine have been likened to amphetamine (Kehr et al., 2011); therefore, the need for future comparisons of mephedrone with other stimulants is highlighted. The greater variety of drugs experienced by users of the NPS mephedrone, and the longer periods of drug use they report, should also be investigated in future research.
In conclusion, the first direct comparisons of mephedrone and MDMA indicate that many effects are experienced at a broadly similar frequency. Stimulant and euphoriant properties were approximately equivalent, while each drug was associated with a similar frequency of most recovery issues. There were some indications of more intense effects with mephedrone use. For example, a subset of recovery effects of greater frequency and weeklong intensity were found within mephedrone use. However, this may be related to a more intensive pattern of usage. Reports of an apparent lack of acute pharmacodynamic tolerance with mephedrone use represent one of several novel findings that require future assessment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.