
Abstract
Placebo response theory and set and setting theory are two fields which examine how non-biological factors shape the response to therapy. Both consider factors such as expectancy, preparation and beliefs to be crucial for understanding the extra-pharmacological processes which shape the response to drugs. Yet there are also fundamental differences between the two theories. Set and setting concerns itself with response to psychoactive drugs only; placebo theory relates to all therapeutic interventions. Placebo theory is aimed at medical professionals; set and setting theory is aimed at professionals and drug users alike. Placebo theory is primarily descriptive, describing how placebo acts; set and setting theory is primarily prescriptive, educating therapists and users on how to control and optimize the effects of drugs. This paper examines how placebo theory and set and setting theory can complement and benefit each other, broadening our understanding of how non-biological factors shape response to drugs and other treatment interventions.
Keywords
Introduction
Placebo response is one of the most studied, most contended phenomena in contemporary medicine. It concerns the ability of any type of treatment, including fake or inactive treatments such as a sugar pill, to lead to an improvement in a patient’s situation. This is due, in part, to expectation for improvement (Stewart-Williams, 2004). Set and setting is a largely overlooked concept which emerged in the 1960s within the field of psychedelic drug research. It posits that drug response is highly dependent on non-pharmacological factors such as expectation, preparation and intention (set), as well as physical and social environments (setting) (Hartogsohn, 2015a).
The common denominator linking placebo and set and setting research is that both study the impact of non-drug factors in therapy – effects that are not produced directly by a pharmacological or other material agent (such as surgery), but rather by some other psychosocial mechanisms. Both theories attribute a significant part of one’s response to various interventions to psychological factors related to cognition and meaning. This response is thus considered extra-or non-biological/pharmacological.
The literature on placebo effects shows that non-pharmacological factors are responsible for a significant part – sometimes the main part – of drugs’ effectiveness (Kirsch and Sapirstein, 1998; Walach et al., 2005). The literature on set and setting indicates that non-pharmacological factors modulate and shape the effects of drugs in many ways. As a review of 1950s and 1960s LSD research demonstrates, the same drug can create anxiety or relaxation, fear or joy, cognitive enhancement or retardation, suspiciousness or intimacy, depending on how it is used (Hartogsohn, 2015b).
Both placebo and set and setting theories have encountered resistance (Atwood, 2011; Hróbjartsson and Gøtzsche, 2001). Medicine, as a science, generally prefers dealing with the material and quantifiable, rather than with the less rigorously objective realms of culture. By invoking the role of non-material aspects in medicine, one thinks perhaps medicine might become less scientific. Yet integrating an awareness of psychosocial factors into medicine may actually enrich and consolidate it, bringing scientific rigor to areas which are still considered external to science.
Because of these shared concerns, it is worth considering placebo and set and setting theories together. By examining the commonalities and differences between them, we can better understand both, conceptualize them as two perspectives on a more general principle and advance the integration of non-biological factors into medicine. And yet a search of the literature did not locate any references to the ways in which the two theories are related. To address this need, I discuss herein the links between placebo phenomena and set and setting theory. In addition, I propose how the two may complement each other, theoretically as well as practically, empowering both patients and medical practitioners, and improving overall outcomes.
Placebo theory
The word ‘placebo’ originally appeared as the Latin translation of the Hebrew word ‘et-ha-lech’ (I shall walk), which appears in Psalm 116, erroneously translated as ‘placebo’ (I shall please). In medieval English the term evolved to refer to a flatterer or sycophant (Moerman, 2002), and by the 19th century it was assimilated into medicine as a name for ‘any medicine adapted more to please than benefit the patient’ (Moerman, 2002: 11).
Placebos were widely used in 19th century medicine, as well as in the first part of the 20th century, yet the concept of placebo held a very different meaning then from its meaning today. At that time, placebos were not considered beneficial or effective (Brown, 2012; Kaptchuk, 1998). Rather, they were regarded as harmless and fundamentally ineffective pills prescribed by doctors to put patients’ minds at ease in situations where little else could be done (Kaptchuk, 1998).
This state of affairs changed in 1955, with the publication of Beecher’s seminal paper ‘The powerful placebo’, which claimed that placebo response is responsible for 35% of drug effects (Beecher, 1955). Beecher’s 35% figure has since been invalidated due to a number of methodological errors in his research (Kienle and Kiene, 1997). However, his paper introduced the idea that placebo effects exerted a much greater effect than simply easing patients’ minds. Here was some mysterious but powerful intervention that actually impacted treatment outcomes.
It was with the rise of ‘randomized controlled trials’ (RCTs) that the placebo effect came into its own. The acknowledgement of the power of placebo, and the wish to separate placebo effects from material ones, led to the increasing integration of placebo control into research methodology. This trend intensified following the 1962 Kefauver–Harris amendments (Healy, 2013; Kaptchuk, 1998). The efficacy of treatment was now measured by its ability to achieve greater results than those achieved by placebo. Thus, placebo came to play a crucial role in the development of the RCT as the new gold standard of evidence-based clinical research. ‘The greater the placebo’s power the more necessity there was for the masked RCT itself’ (Kaptchuk, 1998: 1724).
Placebo response has been thoroughly studied in the decades since, providing us with an abundance of surprising data concerning placebo effects’ mechanisms. The literature has convincingly documented the profound nature of placebo response. For example, placebo effects were found to contribute twice as much as pharmacological effects to the therapeutic effects of anti-depressant medication (Kirsch and Sapirstein, 1998; Sapirstein, 1995; although see Horder et al., 2011), a ‘positive approach’ in general-practice consultation raises patient improvement rates by 25% (Thomas, 1987), and post-myocardial infarction patients who did not take their placebo medication regularly are twice as likely to die than patients who took it daily (Horwitz et al., 1990).
Placebo has served as an invaluable tool to assess the effectiveness of widely-employed medical procedures. It has led, for example, to the cessation of two decades of treating angina pectoris – chest pain resulting from acutely decreased blood flow to the heart – with bilateral internal mammary artery ligation (BIMAL) surgery. While BIMAL surgery previously had appeared successful in treating angina, newer data demonstrated that sham (placebo) surgery achieved similar results (Boissel et al., 1986; Cobb et al., 1959; Dimond et al., 1960). Similarly, sham surgery achieved similar results to those resulting from active neurosurgery for the treatment of Parkinson’s disease, and angioplasty for the treatment of multiple sclerosis, leading to a reevaluation of these interventions (Kim et al., 2005; Siddiqui et al, 2014).
Among the contributing factors to placebo response we find several variables that are also found in notions of set and setting, such as expectation, social interaction and cultural setting.
Expectations play a central role in inducing placebo response. Placebo improvement rates are dramatically decreased when patients are unaware that they are being treated (Benedetti, 1996; Vickers, 1996). Additionally, different colors, sizes and brands of pills can affect the placebo response (Blackwell et al., 1972; Branthwaite and Cooper, 1981; Buckalew and Ross, 1981; De Craen et al., 1996; Schapira et al., 1970), injections serve as more powerful placebos than pills (De Craen et al., 2000; Grenfell et al., 1961) and taking placebo twice a day is more effective than once (De Craen et al., 1999). These data reflect how perceptions of medical treatment shape expectations as well as clinical results. They are corroborated by studies that find that patient expectancies can change or even reverse the effects of active pharmaceutical agents (Flaten et al, 1999, Mitchell et al., 1996).
Social interaction alone may be sufficient to evoke a powerful placebo response. For example, a consultation conducted ‘in a positive manner’ increased the improvement rate for non-diagnosed complaints in a general practice by more than 50% (Thomas, 1987). In addition, doctors with different personalities achieve different results with standard treatments in patients with schizophrenia (Whitehorn and Betz, 1960). In a study of sham acupuncture, Kaptchuk found that prolonged interaction with the treatment provider improved treatment response rates from 44% to 62%, demonstrating that placebo effects can be graded in escalated doses (Kaptchuk et al., 2008a).
Physical setting may also affect placebo response. For example, patients who were recovering from surgery and assigned a room with a window view of a natural setting recuperated more quickly than patients whose rooms faced brick walls (Ulrich, 1984).
Cultural elements also play a significant role in placebo response. For example, the contribution of placebo to a single drug’s effects may vary from 10% to 60% between countries (Lambert et al., 1977; Salgado et al., 1981). An analysis of 117 drug trials demonstrated that the average placebo response for ulcer medication in Germany was twice that seen in the rest of the world, and almost three times higher than in Germany’s closest neighbors, the Netherlands and Denmark (Moerman, 2002).
Cultural effects also affect the ‘nocebo’ response. Nocebo is the negative counterpart of the placebo effect, in that negative expectations of illness outcome worsen those outcomes. The life expectancy of Chinese-Americans with a combination of disease and ‘astrologically inauspicious’ birth year is lower than that of Whites with the same disease–birth year combination. In a study of over 28,000 Chinese-American patients, and almost half a million Whites, Chinese-Americans with ‘inauspicious combinations’ died several years earlier than those who had the same disease but without ill-fated birth years. No such effects were observed in White Americans with the same disease who shared the same birth year with their Chinese counterparts (Phillips et al., 1993).
In addition to being modified by a variety of psychological, social and cultural parameters, the placebo response also exerts measurable effects on the nervous system. For example, placebo activates endogenous dopamine release in the striatum and affects single neurons in the subthalamic nucleus in Parkinson’s disease (Benedetti et al., 2004; de la Fuente-Fernández et al., 2001). Placebo also changes brain metabolism in depression (Leuchter et al., 2002) and modifies the activity of rostral anterior cingulate and lateral orbitofrontal cortices in anxiety (Petrovic et al., 2005). When placebo blocks pain, it does so by activating the endogenous opioid system. This relief is inhibited by naloxone, an opioid antagonist (Sauro and Greenberg, 2005).
The placebo effect is not limited to placebo pills only. It is integral to conventional medical treatment, a therapeutic element which is extraordinarily difficult to separate from actual medical interventions. This is seen in the finding that older medications appear to lose efficacy after the introduction of newer medications for the same condition. For example, the percentage of patients helped by cimetidine fell from 72% in 1975 to 64% in 1981 after the introduction of a newer drug (ranitidine). In this case, it may be suggested that what changed was not the molecular action of the medicine, but the halo of efficacy projected upon it by doctor enthusiasm (Moerman, 2000).
Since active drug and placebo effects are so difficult to separate, some researchers suggest that active drug effects consist of a combination of the two. For example, Claridge proposed the concept of total drug effects, which adds a variety of factors to the drug’s pharmacology. These include (1) drug (e.g. form, color, size, shape, brand and price); (2) prescriber (attitude, self-confidence and status); (3) recipient (personality, suggestibility and psychological state); and (4) the physical setting in which the drug is administered (Claridge, 1970). Total drug effects are thus understood as pharmacological effects combined with a variety of extra-pharmacological variables, a model which has since gained acceptance by others (Finnis et al., 2010).
Set and setting theory
The field of set and setting research is less well-developed than that of placebo. Set and setting was all but forgotten after the prohibition of clinical psychedelic drug research at the end of 1960s, although the term remained in use within certain drug-using subcultures. With the recent resurgence of clinical psychedelic research, it has reemerged within the academic context as well.
The idea that non-pharmacological elements shape the response to hallucinogens was studied by several mid-twentieth century LSD researchers including Rinkel, Dimasico, Klerman, Lasagna and Von Felsinger (Dimascio and Klerman, 1960; Dimascio and Rinkel, 1963; Dimascio et al., 1961; Lasgana, 1963, Von Felsinger et al., 1955). Some of the most fascinating research on the subject was performed by Hyde, who modified his study design over three years, changing staff behavior from normal, to friendly, to cold and impersonal. Hyde found that the severity of negative effects of LSD changed accordingly from 3.4 to 2.8 to 4. Moreover, patients who took the drug by themselves experienced more negative reactions than those who did so in groups. Patients who were expected to perform specific tasks or undergo tests suffered more negative effects, while those who were allowed to choose their own setting and activities had more positive experiences. Hyde conceptualized the non-pharmacological factors that shaped the response to LSD using a number of dimensions such as ‘rigidity–flexibility of goals; familiarity–unfamiliarity of environment; attitudes of acceptance–nonacceptance of the subject’s behavior and feelings; and presence or absence of others with a common culture’ (Hyde, 1960: 306).
At the same time, LSD therapists such as Osmond and Eisner began to explore the many possibilities of set and setting, influenced by Hubbard, who was the first to attempt the optimization the LSD experience using external stimuli. Techniques included the use of music, pictures, flowers and candlelight to enhance the physical setting and charge it with positive cues, as well as thorough preparation which enhanced expectation and intention. They also involved a therapeutic approach that was accepting and non-intrusive (Chwelos et al., 1959; Eisner and Cohen, 1958).
The term set and setting was introduced by Harvard psychologist Timothy Leary (Leary et al., 1963). Leary’s set and setting hypothesis argued that psychedelic drugs acted as a magnifying glass to consciousness, augmenting whatever already existed in one’s mind. He defined set as including the psychological factors of personality, preparation, expectation and intention; and setting as including the environmental factors of the physical, social and cultural surroundings in which the experience occurred.
The set and setting hypothesis has been used to explain the striking rise and fall in the rate of adverse reactions to LSD in the late 1960s (Bunce, 1979). It can also help us understand why 1950s literature on LSD is filled with many contradictory accounts that perplexed researchers at the time. Some claimed that LSD was primarily an anxiety-provoking agent (Hoch, 1957), while others believed it imbued a sense of wholeness (Eisner and Cohen, 1958). Some claimed that LSD invoked psychosis (Rinkel, 1958), while others that it was a harbinger of a ‘new sanity’ (Janiger, 1959). Some said it caused retardation of thought (Deshon et al., 1952), while others presented it as a cognitive enhancer (Harman and Fadiman, 1970). Finally, some maintained that no one who had the LSD experience wanted to repeat it, while others claimed those who had the LSD experience wish to repeat it regularly (Abramson, 1960). Such striking contradictions can be resolved by considering the divergent types of sets and settings used by different research groups which utilized a variety of research perspectives to concentrate alternatively on the potential of hallucinogens to induce psychosis, assist in psychotherapy, augment creativity or enhance spirituality (Hartogsohn, 2015b). These differences in perspectives can be appreciated by considering the many names suggested for these agents, such as hallucinogens (producing hallucinations), psychotomimetics (mimicking psychosis), mysticomimetics (mimicking mystical states), psychedelics (mind manifesting), psychodysleptics (mind-disruptive) or oneirogens (producing dreams) (Strassman, 1984, 2010).
While Leary would later attain notoriety for popularizing the extra-medical use of psychedelics, his lasting contribution to the field was his work on set and setting, a notion that still possesses practical and theoretical value (Dalgarno and Shewan, 2005; McElrath and McEvoy, 2002; Shewan et al., 2000; Zinberg, 1984). The principles of set and setting are discussed (not always under this term) in many contemporary books and websites dedicated to educating drug users who are interested in optimizing their drug experiences (Biebrman, 2014; Fadiman, 2011; Kilham, 2014; Oak et al., 2015). They are also used as the basis for the work of psychedelic support organizations which provide ‘psychedelic first aid’ to individuals in psychedelic emergency situations in the context of psytrance festivals (Carvalho et al., 2014; Ruane, 2015).
The concept of set and setting has also been used in research with non-psychedelic substances, such as heroin, alcohol, cocaine, crack-cocaine, methamphetamine and methylphenidate (Ritalin) (Cohen, 1990; Ditman et al., 1969; Dwyer and Moore, 2013; Hart, 2013; Zinberg, 1984). It helps explain the exceptionally high rates of spontaneous discontinuation of heroin use by soldiers who returned to the USA from the Vietnam war. As suggested by Robins et al. (2010), Zinberg (1984) and Courtwright (2001), rampant heroin use and dependence among enlisted men during the Vietnam war was a result of stressful conditions and the inexorable ennui and boredom that were part of soldiers’ everyday reality, so that when war veterans returned home to a different setting which did not include such incentives to use, an exceptional number of 88% of those who were dependent on heroin gave up the habit spontaneously and seemingly without effort. Similar support for the relevance of the set and setting to the shaping of drug use patterns can be found in Alexander’s rat park experiment, which found that physical environment drastically alters the degree of morphine addiction in laboratory animals (Alexander et al., 1978), a finding which has since been corroborated by similar research on cocaine and methamphetamine (Chauvet et al., 2012; Stairs et al., 2006).
With the resurgence of clinical psychedelic research and discussions of drug policy reform (which emphasizes strategies for harm reduction), the concept of set and setting is once again relevant for psychedelic study designs as well as for informational public campaigns to minimize drug harms and maximize beneficial outcomes.
Relating placebo and set and setting
Placebo theory and set and setting theory both address extra-pharmacological factors in response to drugs and other clinical interventions. Both propose that factors such as expectancy, preparation, social interaction and belief shape the effects of drugs and other interventions, and both attempt to explore how this occurs.
However, there are also a number of differences in how the two theories have been conceptualized. Placebo research measures the non-drug factors that shape response to pharmaceutical agents and non-pharmaceutical interventions. Set and setting, on the other hand, traditionally dealt specifically with psychoactive substances, and particularly with psychedelics. Placebo research typically measures effects on specific health indices such as improvement or symptom reduction, whereas set and setting has been traditionally treated as multi-dimensional and includes a diverse array of disparate phenomena which include not just severity of symptoms but also psychological insights, outbursts in creativity and peak spiritual experiences. While placebo theory is aimed at healthcare professionals only, set and setting theory is also aimed at the general population of drug users. This also betrays another difference in how the two have been usually understood. While placebo theory has been primarily investigatory, studying the different factors which enhance placebo response – there have been few scholarly papers or university courses instructing doctors on how to use placebo – set and setting theory has been primarily practical, engaging therapists and users about controlling and optimizing the factors which shape drug effects. In addition set and setting theory lays special stress on specific factors which play a significant role in psychedelic drug experiences, such as music, space arrangement or communication strategies, which are given only marginal attention in placebo literature. Finally, while placebo response assumed critical significance with the rise of RCTs, set and setting theory has been marginalized and abandoned following the rise of RCTs, whose standardized research protocols seemed incompatible with the principles of set and setting, posing difficulties to mid-20th century psychedelic research (Dyck, 2008; Langlitz, 2012).
Daniel Moerman’s ‘meaning response’ may help bridge the gap between placebo and set and setting theories (Moerman and Jonas, 2002). As Moerman points out, it is not the placebo itself which exerts ‘placebo effect’. Placebos, after all, are biologically inert by definition. Rather, it is the meaning we attach to pills, injections, doctors and the various symbols of medical treatment that is responsible for placebo response. Instead of talking about placebo, Moerman suggests that we talk about meaning response, a broader concept which includes the many ways in which symbolic elements exert positive or negative effects on health in a variety of contexts.
Meaning response relates to how humans understand illness, healing, ritual and symbols of therapy. The medical profession, after all, was not always averse to including extra-pharmacological elements in treatment. Traditional healers commonly employ suggestive elements in their work including a variety of ritual symbols. The setting for a traditional healer’s work might be located in a shrine, temple, sacred place of pilgrimage or special room in the healer’s home. The healer may use incense, blow smoke, chant, sing, produce extraordinary sounds, assume special bodily postures, dance, or move in a specific way. They may be dressed in a ceremonial fashion. Ritual objects may include holy texts, idols, icons, stones and pipes (Helman, 2001). As noted by Turner, each of these objects represents something grander, a significance which goes beyond its utilitarian use and corresponds to essential elements of the society’s worldview (Turner, 1981). ‘To understand the placebo effect fully’, writes Helman, ‘is to understand the society in which it occurs. This is because the symbols that help sustain it are both derived from, and validated by, the wider sociocultural milieu (or “macrocontext”) and help to validate it in turn’ (Helman, 2001: 7).
Similarly, in the 19th century, when many Western medical practitioners became disenchanted with the effectiveness of widely-used medications, they would prescribe placebo. Prestigious medical journals such as The Lancet and The American Journal of Medicine published advice on how to best utilize placebos as late as the 1950s (Carter, 1953; Leslie, 1954).
While the use of explicitly inactive drugs has moved to the margins of modern medical practice (Brown, 2012; Schattner, 2011), placebo response (or meaning response) is integral to any medical treatment. As Helman notes, a visit to a Western doctor’s office involves many symbols of professionalism, success and expertise which enhance meaning response, even when they are not directly involved in treatment. Examples include walls covered with diplomas, a library with rows of impressive books, a section of neatly displayed medical instruments, commercial leaflets by medical companies, uniformed helpers such as nurses and receptionists and the highly symbolic white doctor’s coat. Combined with other factors such as grooming, professional confidence, or even the cost of an appointment, these elements ‘transmit to the patient a message about the healing powers of medical science, and of this particular representative of it’ (Helman, 2001:9). The fact that the different placebo interventions (e.g. pills vs. injections) vary in the level of placebo response they elicit indicates how integral symbolical elements are to everyday medical practice.
Thus, both placebo and set and setting effects meet in meaning response, whether the context is a doctor’s office or a shamanic ritual. The web of significance in which any medical treatment is enmeshed could be considered as the set and setting of that particular treatment. A set and setting which serve to determine the degree of placebo response.
How the fields of placebo and set and setting could benefit each other
Examining placebo and set and setting theories together suggests two ways in which the two may synergize. First, attention to set and setting can help enrich our understanding of placebo, because of how it relates to the factors shaping placebo response. The concept of set and setting has been traditionally considered fundamental to psychedelic therapy and thought. Contemporary psychedelic therapy commonly lays emphasis on the methodic construction of positive sets and settings including preparation, music, flowers, pictures as well as strategies for interaction between patient and therapist (e.g. Mithoefer, 2013). Non-medical users of psychedelics also often place great importance on creating optimal set and setting conditions, a practice to which various books and websites are dedicated (Biebrman, 2014; Fadiman, 2011; Kilham, 2014; Oak et al., 2015). Religious groups which ritually use hallucinogens, such as the Native American Church, União de Vegetal, or the Santo Daime, also make elaborate use of techniques aimed at directing the drug experience towards a positive outcome (Groisman, 1999; Labate and Jungaberle, 2011; Shanon, 2002).
Such cases are of interest for placebo theory. Placebo research has been long looking to move out of the laboratory and get back to the clinic, from which it was eliminated in the 1950s, when giving placebos came to be regarded as unethical. Set and setting theory can provide a model for the introduction of non-pharmacological elements to enhance meaning response in medical treatment. For example, a medical practitioner treating a patient with anti-depression medication might invest time in preparing and priming him for positive expectations and developing a therapeutic intention.
At the same time, the placebo response may help clarify some of the mechanisms by which psychedelics exert their effects. Psychedelics have often been described as amplifiers or magnifiers of consciousness (Grof, 2008; Lee and Shlain, 1992; Metzner, 2011). They also increase suggestibility (Carhart-Harris, 2014; Middlefell, 1967; Sjoberg and Hollister, 1965). If placebo response is understood as meaning response, and if psychedelics magnify the perception of meaning (Savage et al., 1966), it may be that psychedelics augment meaning response.
If psychedelics are understood as meaning-response magnifiers or as hyper-active placebo catalysts, which set the stage for particularly powerful placebo response, this may help explain the anecdotal yet frequent reports of healing associated with their use in ritualistic settings and other meaningful settings. Such reports include conditions such as cancer (Schenberg, 2013), substance abuse (Thomas et al., 2013), stuttering (Isaacson, 2009), allergies (Weil, n.d.) and frigidity (Ling and Buckman, 2007), among others. 1 Though these reports are purely anecdotal in nature, and should no doubt be viewed critically and taken with a grain of salt, they might point to veritable phenomena which occur on the nexus which joins therapeutic outcomes and meaning response. Meaning response appears to have real effects on health, and psychedelics, as shown above, appear to enhance meaning perception. These reports of healing may relate to a specific mechanism which has been proposed as a key to understanding the benefits of placebo – emotional change placebo – which activates the body’s natural immune system following experiences of profound emotional change and reductions in anxiety and depression (Lundh, 1987; Stewart-Williams, 2004;). Psychedelics are showing promising results in the treatment of depression and anxiety (Carhart-Harris et al., 2016; Gasser et al., 2014; Grob et al., 2011, 2013; Osório et al., 2015). In addition, participants in psychedelic experiments habitually rate the experience to be among the most meaningful and spiritually significant experiences in their lives, if not the most meaningful (Griffiths et al., 2006; Leary et al., 1963). Such deeply felt cathartic experiences which reportedly reduce depression and anxiety can arguably lead to an augmented emotional type placebo response of the type described in the literature.
A placebo related conception of psychedelic reactions might change how we think and conceptualize psychedelic therapy. Science journalist John Horgan once asked if ‘peyote is just a hyperactive placebo’ (Horgan, 2010). Such a proclamation might be understood to mean that peyote, which contains the psychedelic agent mescaline, lacks any real power, or it can construed to mean that indeed it holds a formidable power to unlock one of the most significant, least understood, mechanisms of human health.
Placebo theory and set and setting theory seem to corroborate each other’s findings. Integrating the two may have clinical relevance. Both set and setting and placebo empower patients by allowing them to take a more active role in the process of healing. They also empower practitioners by providing additional tools to enhance their practice. At a time when many patients are seeking a more active role in treatment (Bardes, 2012), the judicious use of placebo and set and setting principles may prove especially useful.
As clinical psychedelic research returns to the scene, it is imperative to examine not just the clinical opportunities such agents offer, but also how their effects relate to conditions of set and setting. Furthermore, research into the complex relation between psychedelic effects and placebo response is warranted. One possible way to examine the relationship between psychedelics and placebo would be to conduct studies which will investigate whether LSD can increase placebo response in the treatment of pain and other conditions, and whether an increased LSD-induced placebo response corresponds to the parameters of emotional change placebo. Another way would be to examine the way in which psychedelic agents alter the activity of brain centers known to be involved in placebo response. Thus, for example, researchers have found that placebo-induced expectations of decreased pain activated the rostral anterior cingulate cortex as well as the posterior cerebellum (Petrovic et al., 2005; Ploghaus et al., 2003). In the 1960s, LSD was demonstrated to be effective in the alleviation of pain (Kast et al., 1964; Kast, 1967). Might some of the above-mentioned placebo-induced brain-function modifications which are involved in the decrease of pain perception be enhanced under the effects of psychedelics? 2 Similarly, might other neurological markers involved in placebo (see, for instance, those indicated in the aforementioned studies by Benedetti et al. (2004), de la Fuente-Fernández et al. (2001) and Petrovic et al. (2005)) be enhanced by psychedelics? Finally, Hall and Kaptchuk (2013) point to the existence of genetic biomarkers such as the COMT Val158Met genetic variant which predict the degree of placebo response in patients. Might such genetic variants also predict response to set and setting? Future studies might examine such questions to establish the link between placebo, set and setting and psychedelics.
Conclusions
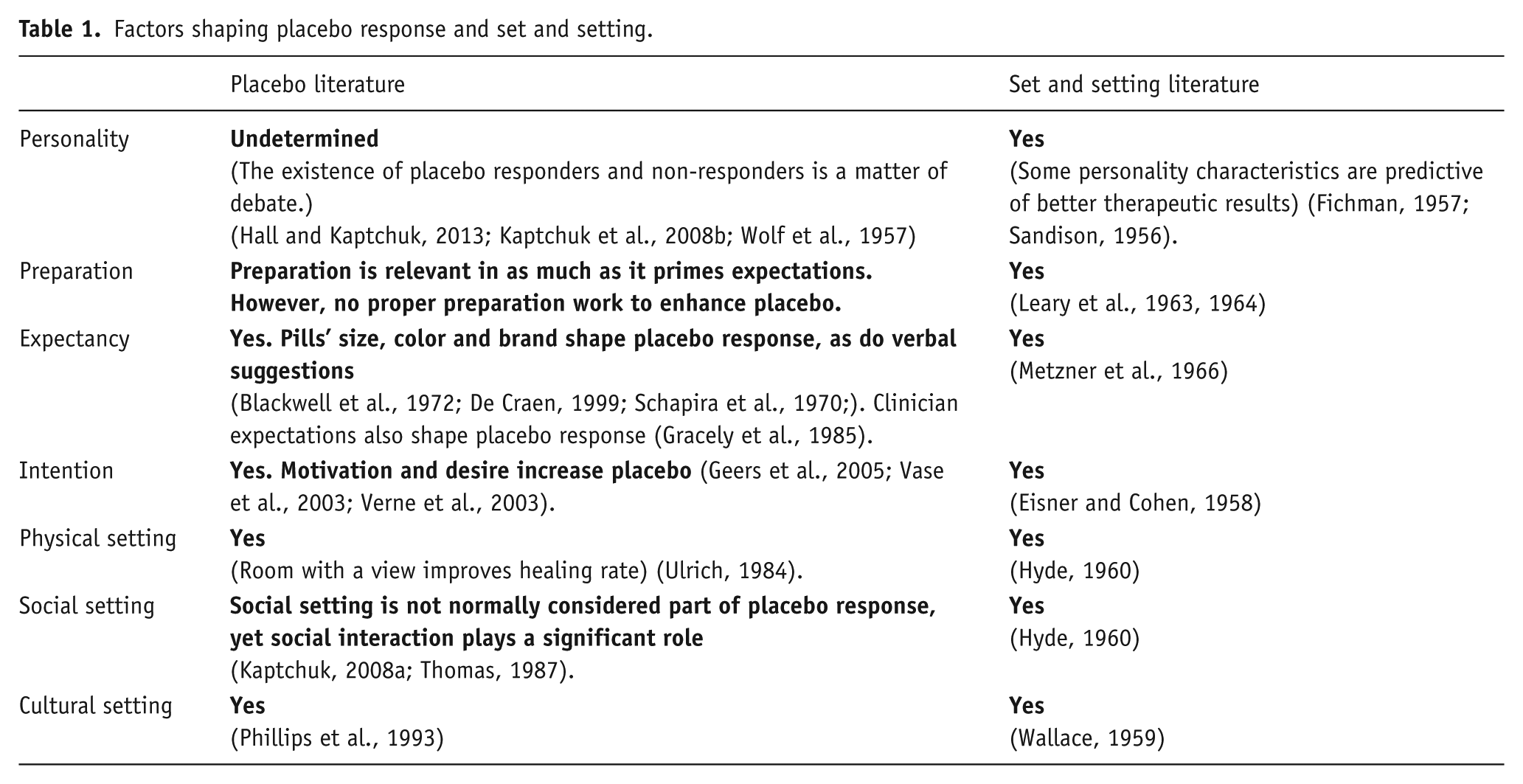
Placebo response and set and setting might be viewed as two different expressions for a single meaning-response related process by which desired treatment outcomes may be made more likely. Up until now, they have been considered separately because of set and setting’s association with psychedelic drugs and their effects. However, when examined carefully, it becomes clear that these are two closely related perspectives on an identical phenomenon: the influence of non-drug/material factors on psychological and medical outcomes effected by material interventions (see Table 1). While the exact ways in which these two perspectives interrelate demands further clarification, considered in conjunction the mutual benefits of their joint consideration become evident: set and setting theory offers a model for the reintegration and optimization of placebo response in clinical practice, whereas placebo theory, in turn, points to how psychedelics, as suggestibility-enhancing, meaning-magnifying drugs, might serve to enhance placebo response.
Factors shaping placebo response and set and setting.
Footnotes
Acknowledgements
The writer wishes to thank the following individuals for their input during the revision stages of text: Prof. Rick Strassman, Dr., and would like to thank Rick Strassman, MD, Matt Johnson, PhD, Galia Tanay, PhD and Leor Roseman for their help in discussing and editing parts of this manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.