
Abstract
The N-methyl-D-aspartate receptor antagonist ketamine has rapid onset activity in treatment-resistant depression, post-traumatic stress disorder and obsessive compulsive disorder. Due to similarities in brain network activity in depression and anxiety disorders, we hypothesized that ketamine might also be active in other refractory anxiety disorders. We evaluated the efficacy and safety of ketamine in 12 patients with refractory generalized anxiety disorder and/or social anxiety disorder who were not currently depressed, using an ascending single dose study design (0.25, 0.5, 1 mg/kg administered subcutaneously) at weekly intervals. Within 1 h of dosing, patients reported reduced anxiety, which persisted for up to seven days. A dose-response profile was noted for anxiolytic effects, dissociative side effects, and changes in blood pressure and heart rate, with minor changes at 0.25 mg/kg, and progressively greater and more durable changes at the higher doses. Ten of 12 patients were treatment responders at 0.5–1 mg/kg. Ketamine was safe and well tolerated in this population. Ketamine may be a potential therapeutic alternative for patients with refractory generalized anxiety disorder/social anxiety disorder. Along with its demonstrated effectiveness in patients with treatment-resistant depression, obsessive compulsive disorder and post-traumatic stress disorder, these data raise the intriguing possibility that ketamine may have broad efficacy in disorders characterized by negative emotional states, and that these disorders may share a common precipitating neurobiology.
Introduction
The initial report that low dose ketamine had rapidly acting antidepressant effects in treatment-resistant depression (TRD; Berman et al., 2000) has now been replicated in numerous randomized controlled trials (RCTs) and case series (Xu et al., 2016). Preliminary studies have reported rapid improvement in two disorders with prominent symptoms of anxiety: obsessive compulsive disorder (OCD; Rodriguez et al., 2013) and post-traumatic stress disorder (PTSD; Feder et al., 2014). To date there have been no data published on the effects of ketamine in treatment-resistant generalized anxiety disorder (GAD) or social anxiety disorder (SAD). We hypothesized that ketamine would improve anxiety ratings in GAD and SAD, based on overlapping alterations in brain network activity in depression and anxiety disorders (Pannekoek et al., 2015), similar regional changes in grey matter volume (van Tol et al., 2010), and alterations in glutamate signaling (Averill et al., 2016). The objective of this feasibility study was to evaluate the effect of ascending single doses of ketamine on anxiety ratings in patients with treatment-resistant GAD or SAD.
Methods
This study was approved by the Southern Health and Disabilities Ethics Committee (15/STH/86), and was registered prospectively with the Australian New Zealand Clinical Trial Registry (ACTRN 12615000617561). This was an ascending single-dose, uncontrolled, open label study in 12 patients with refractory Diagnostic and Statistical Manual of Mental Disorders, Volume IV (APA, 2000) GAD and/or SAD. Patient inclusion criteria included having a Hamilton Anxiety Scale (HAM-A; Hamilton, 1959) score of ≥20, and/or a Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987) score of ≥60 at screening, and being aged 18 years or older. Patients were excluded if there was evidence of severe acute or chronic medical disorders, if they were pregnant or lactating, if they were taking monoamine oxidase inhibitors, thyroxine, or stimulants, or had active suicidal ideation. To reduce the risk that changes in anxiety ratings were confounded by comorbid depression, patients with Montgomery-Asberg Depression Rating Scale (MADRS; Montgomery and Asberg, 1979) scores of ≥20 at screening were excluded. All subjects provided signed informed consent prior to enrolment, and were assessed as suitable to participate based on review of medical history, safety laboratory tests, and vital signs. Patients were permitted to remain on current medication regimens and to continue with ongoing psychotherapy. However, no new treatments were to be started or doses/visit schedules changed.
There were three ascending ketamine dose levels (0.25, 0.5 and 1 mg/kg, given in that order), injected subcutaneously in the upper arm, with one week between doses. Subcutaneous dosing was selected as it is as effective as IV dosing, however with better tolerability (Loo et al., 2016). The lowest dose was chosen as it appears to be a threshold dose in patients with TRD, (Loo et al., 2016), and we have found the 1 mg/kg dose to have the greatest durability of response in patients with TRD (Glue et al., 2011). Patients were monitored in the clinic for 2 h post-dose, with vital signs obtained predose, and 15, 30, 45, 60, 90, and 120 min post-dosing. Anxiety assessments included the Fear Questionnaire (FQ; score range 0–136; Marks and Mathews, 1979) and the HAM-A (range 0–52; Hamilton, 1959) predose, at 1, 2, 24, 72, and 168 h post-dose. Tolerability assessments included reported adverse events throughout the study, and Clinician Administered Dissociative States Scale (CADSS; Bremner et al., 1998) predose, 30, and 60 min post-dose. Summary statistics were calculated and reported for demographic, vital signs, and rating scale data. Categorical variables were reported using counts and percentages. In order to accommodate the repeated measures on patients from both the multiple measurements over time within a given dose and from the three doses received by each participant in this ascending dose design, linear mixed models were used with random participant and participant-dose effects along with fixed effects for time, dose, and the time-by-dose interaction. Residual maximum likelihood estimates were used. Histograms and scatter plots of conditional residuals were inspected and, where appropriate, natural logarithm transformations investigated to see if this improved satisfaction of model assumptions. Statistical analyses were performed using Stata 14.1 and two-sided p<0.05 was considered statistically significant. As this was an exploratory study, and to avoid reducing power to detect both beneficial and adverse effects, no adjustments for multiple comparisons were made. A responder analysis was performed based on the proportion of participants with 50% or greater reduction in HAM-A or FQ total score after any dose.
Results
Seventeen patients were screened; 12 patients were enrolled and all completed the study. The participants comprised four females (33%) and eight males (67%). Mean age was 32 years (range 23–55), and duration of their anxiety disorders was 16.5 years (range 5–30). Ten subjects met the criteria for GAD (83%), and nine for SAD (75%). There was significant comorbidity, with five subjects also having panic disorder (42%; see Supplementary Material, Figure 1). All patients were currently taking antidepressants and had not responded to prior trials of antidepressants and group or individual psychotherapy, including CBT (individual patient details are tabulated in Supplementary Material, Table). Mean HAM-A at screening was 26 (indicative of severe anxiety), and mean LSAS at screening was 89 (threshold score for probable SAD is 60). Eleven subjects had had prior major depressive disorder (MDD) (92%), however none appeared to be currently depressed (mean screening MADRS=8.0, range= 5–12; threshold score for moderate depression is 20).
Changes in anxiety rating scales
Mean FQ rating-time profiles are shown in Figure 1(a). Dose responses were noted in terms of magnitude of initial decrease and duration of reduced ratings. The mixed model analysisidentified significant dose×time interaction (p=0.033). Mean HAM-A rating-time profiles are shown in Figure 1(b). Dose-responses were noted for magnitude of initial decrease, and duration of reduced scores. The mixed model analysis identified a non-significant tendency for a dose×time interaction (p=0.068). Overall 10 of 12 patients (83%) reported a >50% reduction in HAM-A and/or FQ scales after the 0.5 or 1 mg/kg doses.
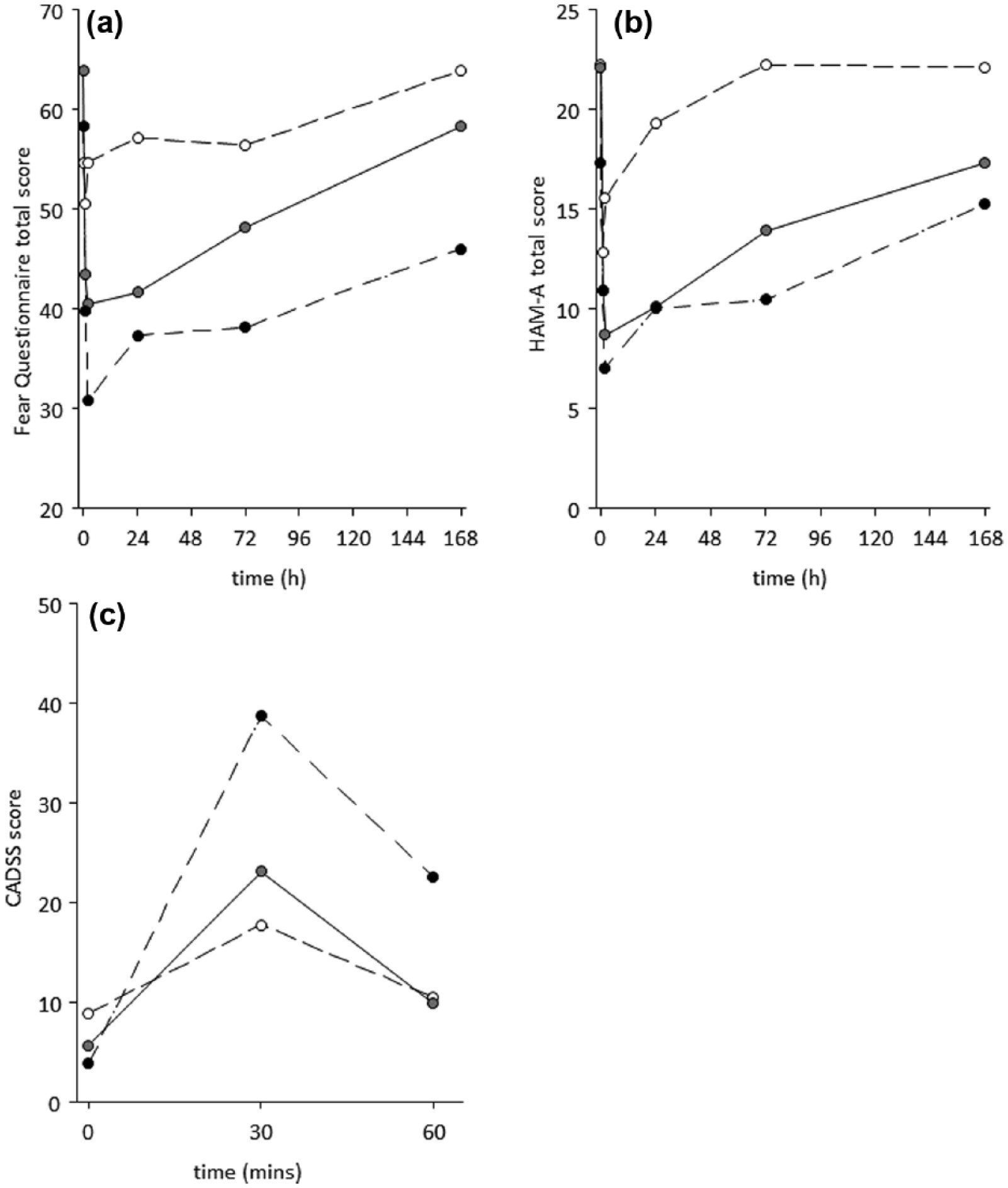
Effects of ketamine dose on mean anxiety scale ratings, predose to 168 h post-dose: (a) Fear Questionnaire; (b) Hamilton Anxiety Scale (HAM-A); (c) effects of ketamine dose on mean Clinician Administered Dissociative States Scale (CADSS) scores, predose to 60 min post-dose. Open symbols: 0.25 mg/kg; grey symbols 0.5 mg/kg; black symbols: 1 mg/kg.
Safety and tolerability
All subjects reported dissociative symptoms, starting approximately 5 min after each injection, with peak intensity around 20–30 min. CADSS scores showed dose-dependent increases at 30 min and were returning towards baseline by 60 min (Figure 1(c)). The mixed model analysis identified a significant dose×time interaction (p=0.008). After the 1 mg/kg dose, two subjects rated these experiences as very intense, feeling out of control. Two subjects also reported transient nausea at 30 min post dose. Dose-related increases in systolic and diastolic blood pressure were observed at 30 min, with mean change from baseline of 9.4 and 7.5 mm Hg after 1 mg/kg dosing. Heart rate increased by 4.5 beats/min at 15 min after 1 mg/kg dosing.
Discussion
This is the first demonstration of anxiolytic effects of ketamine in patients with severe treatment–resistant GAD and/or SAD who were not currently depressed. The pattern of improvement was similar to that seen in patients with TRD, in that there was a rapid onset of anxiolytic effects, and that these effects wore off over 3–7 days. A dose-response profile was noted for anxiolytic effects and dissociative side effects. Ketamine was safe and well tolerated.
Treatment-resistant anxiety disorders are a major clinical problem. Between 40–60% of patients with anxiety disorders may fail to respond to conventional drug or psychological treatments (Bandelow et al., 2008). Evidence to support specific treatment strategies for treatment-resistant anxiety is limited (Ammar et al., 2015), and patients may remain functionally impaired (Kroenke et al., 2007). We have identified that ketamine has broad anxiolytic effects with GAD and/or SAD, with improvements in cognitive, emotional, and physical symptoms of anxiety, irrespective of diagnosis.
We identified a dose response for ketamine in this patient group. 0.25 mg/kg appeared to be a threshold dose, associated with a brief reduction in anxiety ratings at 1 h post dose, which did not persist. The maximum reduction in anxiety appeared to be greater for 0.5–1 mg/kg, and the duration of anxiolytic effects appeared to be greatest at 1 mg/kg. There are limited dose-response data for ketamine in TRD. We have recently showed in an individual dose-titration study that 0.2–0.3 mg/kg is a threshold dose for reducing severity of depression in patients with TRD, and that higher doses (up to 0.5 mg/kg) appear to have more robust antidepressant effects (Loo et al., 2016). The efficacy of doses >0.5 mg/kg has not been systematically studied in TRD.
There a number of limitations with the current study, including diagnostic comorbidity, use of concomitant medication, and the open-label study design. Seven patients met criteria for comorbid GAD and SAD, six had current or previous panic disorder, and two had PTSD (see Supplementary Table, online). Comorbidity of anxiety disorders is not uncommon in patients with treatment-resistant anxiety (Kroenke et al., 2007), and this cohort represents a real-world patient population. Almost all patients had had prior MDD. While none were depressed at the time of testing, it is possible that a history of prior MDD could represent a clinical phenotype responsive to ketamine. Also potentially of relevance is the finding that TRD patients with high baseline anxiety levels may be more responsive to ketamine than nonanxious TRD patients (Ionescu et al., 2014). This could be explored in future treatment trials in anxious patients with and without prior MDD. Although patients were not responding to ongoing antidepressant therapies, we decided not to change these prior to ketamine treatment, consistent with our earlier study in TRD (Loo et al., 2016). The study design involved open-label ascending doses of ketamine, where both patients and investigators knew they were receiving ketamine, which potentially introduced reporting and measurement bias issues. Subject numbers were small. Since this was the first study to evaluate the efficacy and safety of ketamine in this patient population, we believe that this design was fit for purpose.
In conclusion, this study provides the first evidence that ketamine improves symptoms of anxiety in patients with treatment refractory GAD and SAD who are not currently depressed, and is safe and well tolerated. Ketamine has the potential to provide a therapeutic alternative for this patient group with few treatment alternatives. Along with its demonstrated effectiveness in patients with TRD, OCD, and PTSD, these data raise the intriguing possibility that ketamine may have broad efficacy in disorders characterized by negative emotional states, and that these disorders may share a common precipitating neurobiology.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P Glue and N Medlicott have a contract with Douglas Pharmaceuticals to develop novel ketamine formulations. Within the last three years P Glue has received research funding from DemeRx Inc. and participated in an advisory board for Janssen Pharma. Dr McNaughton has a confidential disclosure agreement with Janssen Research & Development, LLC. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.