
Abstract
Background:
Evidence suggests that anti-inflammatory medication may be effective in the treatment of depressive symptoms. In this study, we aimed to investigate whether minocycline added to treatment as usual (TAU) for 3 months in patients with treatment-resistant depression will lead to an improvement in depressive symptoms.
Methods:
Multi-site, 12-week, double-blind, placebo-controlled, pilot trial of minocycline added to TAU for patients suffering from DSM-5 major depressive disorder, whose current episode has failed to respond to at least two antidepressants. The primary outcome measure was mean change in Hamilton Depression Rating Scale (HAMD-17) scores from baseline to week 12. Secondary measures were the Clinical Global Impression scale (CGI), Patient Health Questionnaire-9 (PHQ-9), the Generalised Anxiety Disorder scale (GAD-7) and EuroQoL (EQ-5D) quality-of-life questionnaire. Side-effect checklists were also used. Minocycline was started at 100 mg once daily (OD) and increased to 200 mg after 2 weeks.
Results:
A total of 41 participants were randomised, with 21 in the minocycline group and 20 in the placebo group. A large decrease in HAMD scores was observed in the minocycline group compared to the placebo group (standardised effect size (ES) –1.21, p < 0.001). CGI scores in the minocycline group also showed a large improvement compared with placebo (odds ratio (OR): 17.6, p < 0.001). PHQ-9, GAD-7 and EQ-5D total showed more moderate improvements (ES ~ 0.4–0.5).
Conclusion:
The findings indicate that adjunctive minocycline leads to improvement in symptoms of treatment-resistant depression. However, our findings require replication in a larger sample.
Trial Registration:
ClinicalTrials.gov identifier: NCT02263872, registered October 2014.
Introduction
Depression is the leading cause of disability worldwide (World Health Organisation, 2017). Although depressive symptoms are amenable to antidepressant treatments, a high proportion of patients neither responds adequately nor achieves remission (Rush et al., 2006). For example, in the Sequenced Treatment Alternatives for the Relief of Depression (STAR*D) study, the response and remission rates with stage 1 treatment (citalopram) were 49% and 37%, respectively. The additional response rates decreased to 16% and 13%, respectively, over the subsequent next three treatment steps (Rush et al., 2006). A recent meta-analysis of current pharmacological treatments for depressive disorder in primary care showed only a relatively small effect size for antidepressant treatments when compared with placebo (Linde et al., 2015). Thus, there remains a clear need for more efficacious and novel treatment approaches.
Recently, there have been promising preclinical and clinical data implicating inflammatory processes in a range of psychiatric disorders including depression. The findings include: a meta-analysis showing that pro-inflammatory cytokines are increased in the blood of patients with major depressive disorder (O’Donovan et al., 2013); and that peripheral administration of a pro-inflammatory cytokine (IFN-α) induces a depressive syndrome in many patients receiving it as a treatment for hepatitis (Van Gool et al., 2003). Treatment with cytokine IFN-α corresponded with the development of depressive symptoms in up to 45% of patients with no previous history of depression (Capuron and Miller, 2011). Longitudinal studies have demonstrated that high plasma pro-inflammatory protein levels precede, and thus potentially cause depressive symptoms (Gimeno et al., 2009; Khandaker et al., 2014). The most convincing evidence for a close relationship between inflammation and depression is the very frequent comorbidity of depressive symptoms with virtually all chronic inflammatory or autoimmune disorders (Capuron and Miller, 2011). Large proportions (probably >50%) of patients with rheumatoid arthritis and systemic lupus erythematosus have depressive or other psychiatric symptoms. Inflammatory medical illnesses, both CNS and peripheral, are associated with greater rates of depression and in patients with Crohn’s disease and comorbid depression, bouts of physical disease activity tend to co-occur with depressive episodes (Mardini et al., 2004). Although less robust, evidence also suggests that inflammation when present is associated with more severe course of illness (Zalli et al., 2016), and more prominent in people who are resistant to monoaminergic drugs (Carvalho et al., 2013; Grosse et al., 2016). There is also some preliminary evidence that anti-cytokine treatment may have antidepressant properties (Kappelmann et al., 2016).
Current evidence suggests that the addition of an anti-inflammatory medication may be effective in the treatment of depressive illness. Muller et al. were the first to demonstrate a reduction in depressive symptoms when using celecoxib, a COX-2 selective non-steroidal anti-inflammatory drug, in addition to reboxetine for the treatment of major depressive disorder in a double-blind, randomised, placebo-controlled pilot study (Muller et al., 2006). A recent meta-analysis showed that augmentation with celecoxib is an effective add-on treatment for unipolar depressive patients (Faridhosseini et al., 2014). However, other studies have found that anti-inflammatories may have an antagonistic effect on the antidepressant actions of selective serotonin reuptake inhibitors (SSRIs) (Warner-Schmidt et al., 2011). Further work is needed in this area to clarify the role of inflammatory processes and anti-inflammatories in the treatment of depression.
The tetracycline antibiotic minocycline has been proposed for the treatment of depressive symptoms, as well as negative symptoms in schizophrenia (Chaudhry et al., 2012; Soczynska et al., 2012). Studies in animal models have shown that minocycline may induce antidepressant-like effects (Arakawa et al., 2012). Preliminary data from an open-label study of patients with psychotic unipolar depression suggested that minocycline augmentation of antidepressant treatment was effective and well tolerated (Miyaoka et al., 2012). Minocycline has many actions on a variety of systems implicated in depression, including anti-inflammatory, anti-oxidant, anti-apoptotic, and modulation of glutamate and monoamine neurotransmission (Hashimoto and Ishima, 2010; Soczynska et al., 2012). Despite these properties, there have been no published controlled clinical trials investigating the antidepressant effects of minocycline in individuals with treatment-resistant depression.
In this double blind, randomised, placebo-controlled pilot trial, we examined the efficacy of minocycline as an adjunct to treatment as usual (TAU) for 12 weeks in patients with treatment-resistant major depressive disorder. The inflammatory hypothesis of depression predicts that minocycline augmentation should lead to an improvement in depressive symptoms in the experimental group in comparison with the control group.
Methods and materials
Overview
This was a multi-site, 12-week, double blind, placebo-controlled, pilot trial of minocycline added to TAU for patients suffering from a DSM-5 major depressive episode that has failed to respond to at least two antidepressant treatments. The study was conducted in Karachi, Pakistan, and participants were recruited from outpatient psychiatric clinics at Abbasi Shaheed Hospital, Karwan-e-Hayat Hospital, Civil Hospital, and the Institute of Behavioural Sciences between October 2014 and March 2016.
All patients provided written informed consent after reading the information provided. TAU comprised medications including antidepressants (selective serotonin reuptake inhibitors, tricyclics, monoamine oxidase inhibitors, noradrenergic and specific serotonin antagonists and serotonin noradrenaline reuptake inhibitors), mood stabilisers (with the exception of valproic acid) and antipsychotics, as well as psychotherapy and other psychosocial interventions.
The trial was registered with Clinicaltrials.gov in October 2014 (ClinicalTrials.gov identifier: NCT02263872).
Randomisation and masking
An independent statistician, unknown to study personnel, randomised participants using a web-based randomisation tool (allocation ratio 1:1) to receive either minocycline or placebo, in addition to TAU. There was no further stratification. The randomisation lists were held by a pharmacist who was not involved in the research project.
Tablets were dispensed by a single pharmacy and patients, their families, referring psychiatrists, the study statistician and the research assistants carrying out the assessments were blind to the study drug until the completion of the study. Reign Nutro Pharma and Jawed Traders (Pakistan) provided minocycline and placebo in identical tablet form, matched for shape, size, texture, colour and odour. Both companies hold International Organisation for Standardisation (ISO) certification.
Sample size
A total of 41 participants were recruited and randomised into two arms.
Power calculation
This was a pilot trial and so the main objective was to estimate effect sizes. The US Food and Drug Administration guidance on drug study design recommends that a minimum of 12 subjects per group is sufficient for pilot trials (US Food and Drug Administration, 2016). In the proposed study, we aimed to recruit 20 to each treatment group: minocycline and TAU. Assuming 20% loss to follow up, with an alpha of 5% for a two-tailed test, our trial had 0.8 power to detect an effect size (ES) of 1 for a differential reduction of Hamilton Depression scores (HAMD) (Hamilton, 1960) between minocycline and TAU.
Local research ethics committee approval
Approval was obtained from the ethics committee of the Karachi Medical and Dental College and Dow University of Health Sciences, Pakistan.
Inclusion criteria
Inclusion criteria were: (1) patients aged 18 to 65 years; (2) Current Diagnostic and Statistical Manual-5 (DSM-5) diagnosis of major depressive disorder; (3) capacity sufficient for consent to participate; (4) taking the current antidepressant medication for a minimum of 4 weeks (6 weeks for fluoxetine) prior to baseline; (5) the current episode of depression has failed to remit with at least two courses of antidepressant treatment (one of which is the current medication) at the adequate dose (according to British National Formulary and Maudsley Prescribing Guidelines); relapse while taking an antidepressant is also considered a treatment failure; (6) able to take oral medication and (7) if female, willing to use adequate contraceptive precautions and to have monthly pregnancy tests.
Exclusion criteria
Exclusion criteria were: (1) relevant medical illness (renal, hepatic, cardiac, serious dermatological disorders such as exfoliative dermatitis, systemic lupus erythematosus); (2) prior history of intolerance to any of the tetracyclines; (3) concomitant penicillin therapy; (4) concomitant anticoagulant therapy; (5) presence of a seizure disorder; (6) currently taking valproic acid; (7) any change of psychotropic medications within the previous 4 weeks; (8) diagnosis of substance-use disorder (except nicotine or caffeine) or dependence within the last 3 months according to DSM-5 criteria; (9) pregnant or breast-feeding or (10) presence of primary psychotic disorder.
The criteria for leaving the trial were: (1) patient’s request; (2) at the discretion of the responsible medical officer or investigator (for example, an adverse event or poor compliance) and (3) pregnancy.
Study procedure
Recruitment
In the first instance, the research clinician approached the clinical teams to inform them about the research study and the inclusion and exclusion criteria. If patients met the entry criteria, were clinically stable and the clinical team agreed that the patient could be a possible participant, they introduced the study to the patient. With the patient’s agreement, the research clinician then visited the patient to explain the research study verbally (in either Urdu or English) and to provide them with the participant information sheet (Urdu/English). The study was described to each potential participant with a witness (usually a caregiver) present. The patient had time to read and understand the patient information sheet (at least 24 hours). If they agreed to take part, a meeting (visit one) was set up with the patient in order to obtain signed informed consent for the study and also signed consent for the research team to have access to their medical notes. Literate participants signed the consent forms but, if the participant could not write their name, they placed a thumbprint on the consent form which was countersigned by the witness.
Screening visit
Confirmation of patient suitability was carried out at this point. Participants recruited to the trial underwent structured diagnostic interviews using the Mini International Neuropsychiatric Interview (MINI) to confirm a diagnosis of DSM-5 major depressive disorder (Sheehan et al., 1998). This tool has been validated for use in the local Urdu language and has been used in previous studies in Pakistan (Nisar et al., 2004). The Hamilton Depression Rating Scale (HAMD-17) (Hamilton, 1960) was used to measure severity and response and has also been used previously in Pakistan (Husain et al., 2014). Other inclusion/exclusion criteria were checked at this visit and confirmation of consent and pregnancy testing, if appropriate was carried out.
Follow up
Participants were randomised to receive minocycline or placebo added to TAU. Patients continued with their current treatment as prescribed by their psychiatrists. In order to keep the study design pragmatic and to test the efficacy of minocycline in routine clinical settings, participants were permitted to change medications during the study period if required. Minocycline added to TAU started at a dose of 100 mg daily and was increased after 2 weeks to 200 mg daily, taken as a single dose to encourage compliance.
The patients’ day-to-day care remained the responsibility of their usual consultant psychiatrist or other mental health professional. Research assistants maintained contact throughout the study in order to respond to any concerns or changes in circumstances or mental or physical health. Contacts were twice weekly for the duration of the study. Any study-related safety concerns were the responsibility of the co-investigators who could be contacted at any time through the research team.
Outcome measures
The primary clinical outcome measure was mean change from baseline to week 12 on the Hamilton Depression Scale scores (Hamilton, 1960). Response was defined as a reduction of 50% or more of the HAMD-17. Remission was defined as a score of ≤7 of the HAMD-17.
Ratings were made on the basis of a clinical interview using HAMD-17 at baseline, weeks 2, 4, 8 and 12.
The secondary clinical outcome measures were the Clinical Global Impression (CGI) scale, a 7-point overall measure of severity (Busner and Targum, 2007); the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001) a self-rated depression severity measure; the GAD-7 (Spitzer et al., 2006), a measure of generalised anxiety disorder, and the EuroQoL (EQ-5D) scale, a measure of health-related quality of life (Brooks, 1996). All assessment scales were translated for use in Urdu and have been used in previous clinical trials in Pakistan (Husain et al., 2014). Adverse effects were monitored using a rating scale that has been specifically designed for minocycline. This rating scale has been used by the authors in previous studies (Chaudhry et al., 2012).
Biomarkers
Participants were asked to provide two blood samples for research analysis. The provision of blood samples was optional and did not affect participation in the trial. These samples were collected at baseline and at week 12 and were collected to investigate the relationship of minocycline to inflammatory markers and if this relates to the subjective experience of symptom change. The biomarkers tested included erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). The selection of biomarkers was based on previous research that confirms the pro-inflammatory properties of these measures (Cameron and Kelvin, 2000). CRP was used as a direct marker of inflammation. Given the funding constraints for this pilot study, we were not able to measure levels of other inflammatory biomarkers (e.g. cytokines).
Research assistant training and inter-rater reliability
Although data on inter-rater reliability was not formally collected, all assessments were carried out by research assistants who are experienced Masters’ level clinical psychologists that were trained in clinical assessments and diagnostic interviews by two authors (IBC and NH).
Statistical analysis
The focus of this study was to estimate to ESs and 95% confidence intervals for treatment outcomes. All randomised participants were included in the analysis according to their treatment allocations at randomisation, according to the intention-to-treat (ITT) principle. All continuous measures, including the primary outcome HAMD were analysed with linear mixed models to account for the dependencies in the data from the repeated measures. CGI was an ordinal outcome and so a generalised linear mixed model (proportional odds) was used for this outcome. Hypotheses were two sided and tested at the p < 0.05 level. Standardised ESs for the treatment contrast were derived by dividing the group difference by the pooled standard deviation of the outcome scores.
Explanatory variables in the model were baseline outcome scores, treatment contrast (minocycline or placebo), time and interactions between time and treatment to allow treatment estimates to differ at 2, 4, 8 and 12 weeks. The primary outcome was mean group difference in HAMD scores at 12 weeks. The time point of interest for secondary outcomes was also 12 weeks. To deal with missing outcome data, we used the maximum likelihood (ML) approach: the main analysis used mixed effects models fit, using such models allow all available data to be included in the analysis, under the assumption that data is missing at random (MAR), that is, conditional on baseline predictors of missingness of outcomes being included in the model. To identify the latter, a binary indicator of missingness was generated for 12-week HAMD scores and predictors of missingness were sought using logistic regression and Fisher’s exact test. A criterion of p < 0.05 was used as with the small sample there is a risk of overfitting. There was a strong association between socio-economic status and missingness, p = 0.003, but no other predictors of missingness. Socio-economic status was therefore included in all the primary analysis models.
For the blood markers, there were further missing data for both baseline and 12-week outcomes. Analysis was descriptive and limited to calculating ES for impact of minocycline on inflammatory marker levels, and correlations between change in inflammatory markers and HAMD scores. Given the small number of observations, robust correlation coefficients and confidence intervals were calculated as appropriate. R 3.3 and STATA v14 IC (Stata corp., College Station, TX, USA) were used to perform the analysis.
Results
Initially, 87 potential study candidates were identified. However, 30 patients did not meet study inclusion criteria and 16 chose not to take part. Therefore, 41 participants were randomised, with 21 in the minocycline group and 20 in the placebo group (see Figure 1). No significant differences were identified in baseline demographic data, including age and sex between groups (see Table 1). A total of 34 participants completed the trial.
Demographic characteristics of participants.
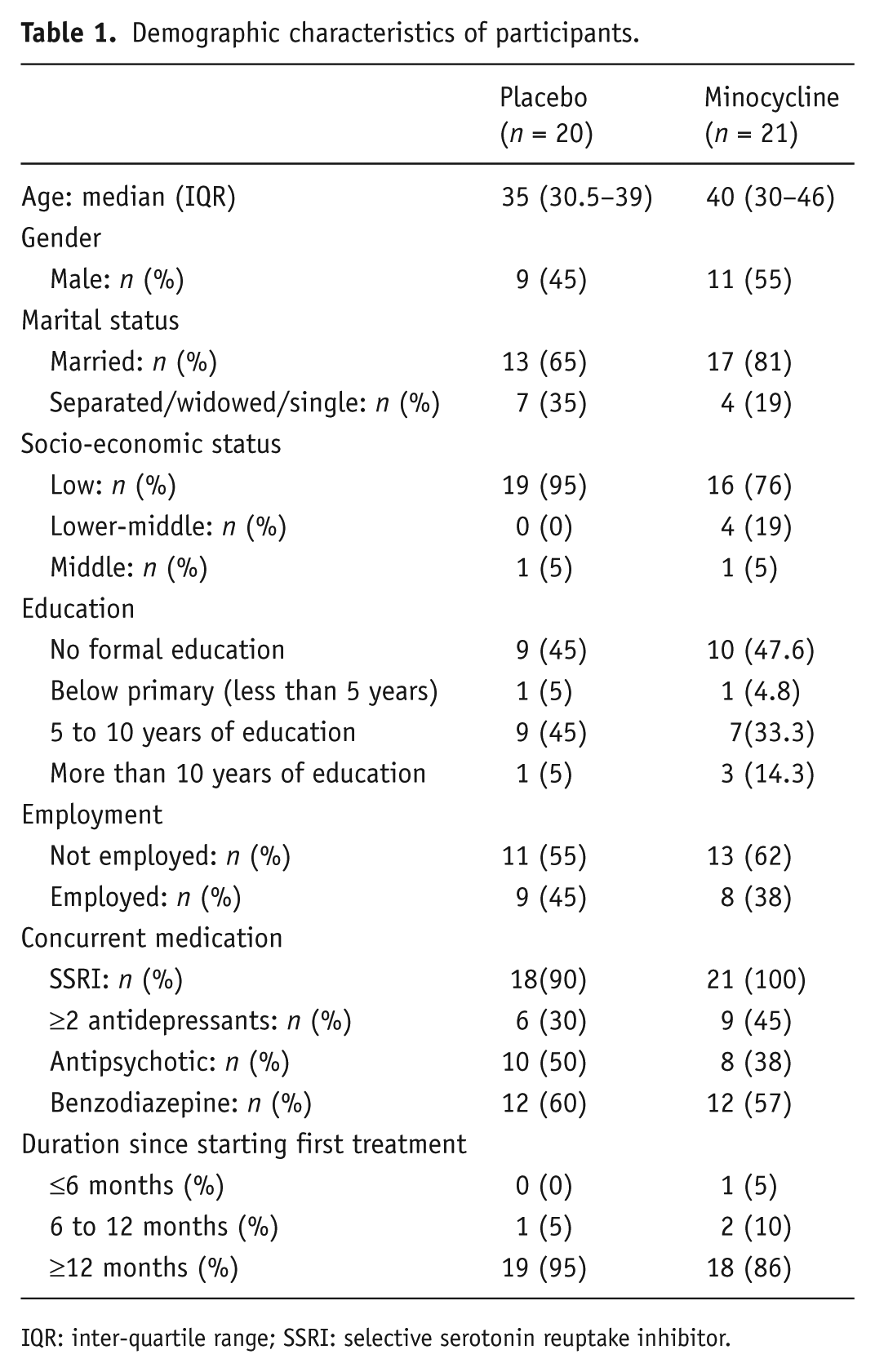
IQR: inter-quartile range; SSRI: selective serotonin reuptake inhibitor.
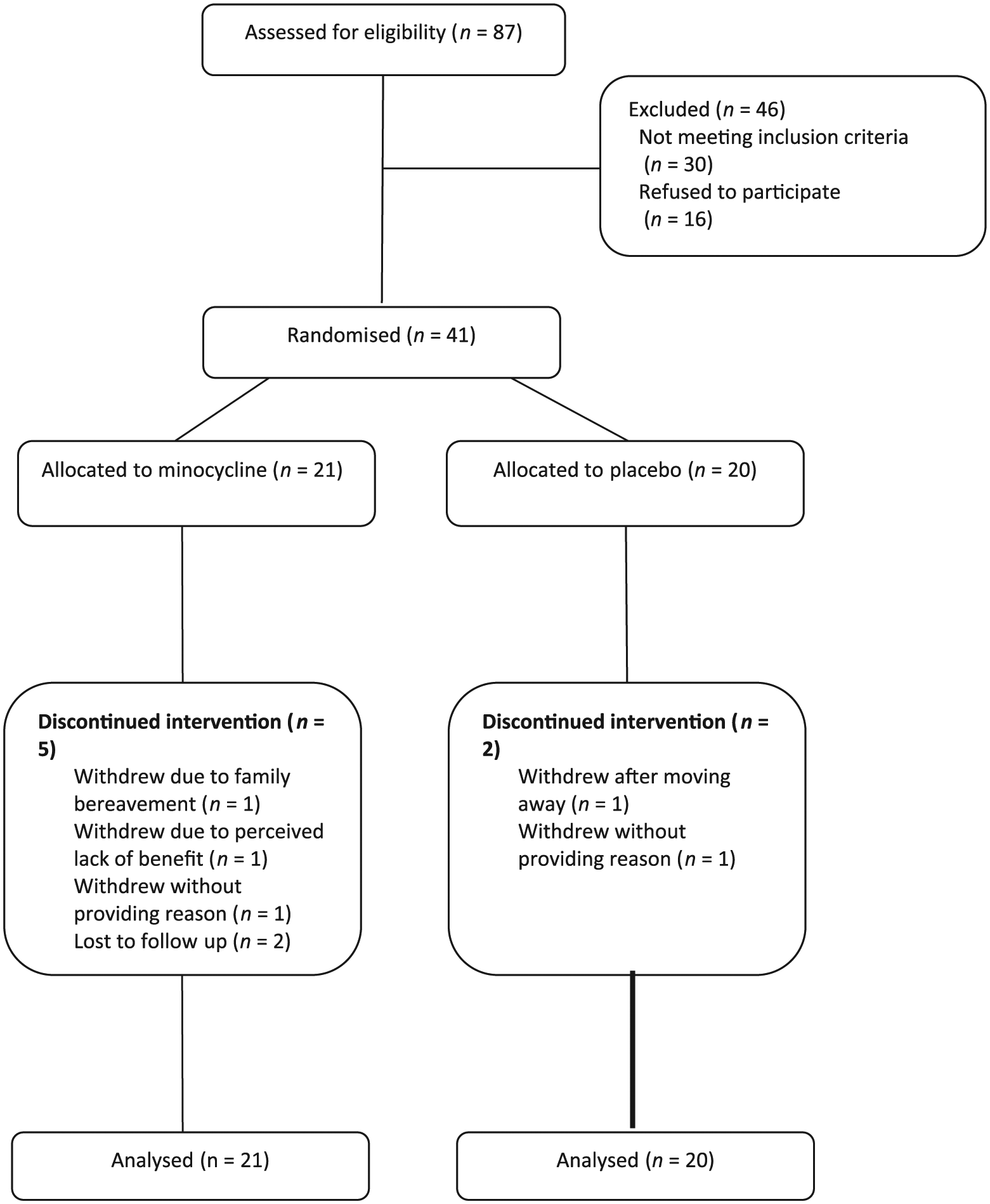
CONSORT flow diagram.
During the course of the 12-week trial, changes to TAU were made to patients in both the minocycline and placebo groups. Five participants in the minocycline group and seven participants in the placebo group were started on an augmentation treatment (i.e. an atypical antipsychotic or benzodiazepine). One participant in the minocycline group switched their antidepressant (from one SSRI to another), and one participant in the placebo group switched antidepressants (from a SSRI to mirtazapine).
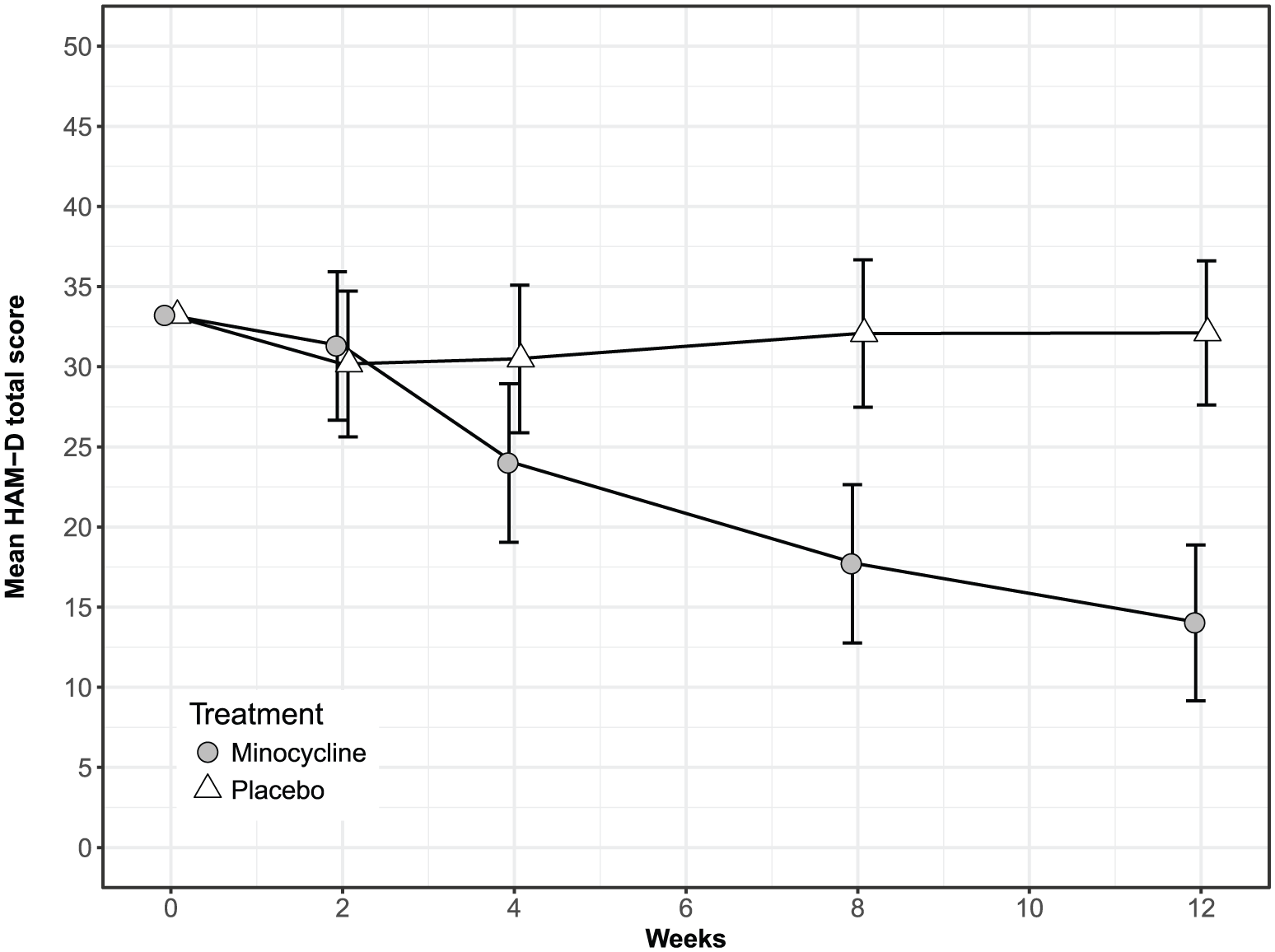
Table 2 shows descriptive statistics (mean and standard deviation (SD)) for the clinical outcome measures at baseline and 12 weeks, together with the change from baseline. Table 3 shows the parameter estimates for the generalised linear mixed model analysis, giving the baseline-adjusted mean difference between treatment groups at 12 weeks, together with the standardised regression coefficient. A strong association between treatment group and HAMD depressive symptoms at 12 weeks (ES = −1.21, p < 0.001) was observed in the minocycline group compared with the placebo group. The course of the HAMD scores is shown in Figure 2, with treatment differences appearing at week 4 and no overall change in the placebo group. According to the HAMD definitions of treatment response (response > 50%), 63% of the minocycline group responded to treatment compared with 22% of the placebo group (OR: 5.5, p = 0.035). There were also a greater proportion of participants that showed remission (HAMD < 7) in the minocycline group versus the placebo group (odds ratio (OR) 7.3, p = 0.078). Similarly, the minocycline group showed a strong response in terms of CGI relative to placebo (OR: 17.6, p < 0.001). In addition, the minocycline group showed greater improvement in PHQ-9 scores, GAD-7 and EQ-5D total and visual analogue scores (VAS) although the ESs in these cases were more moderate (~0.4–0.5, see Table 3).
Descriptive statistics: mean clinical outcome measures (with SD) at baseline and 12 weeks with change scores for placebo and minocycline groups.
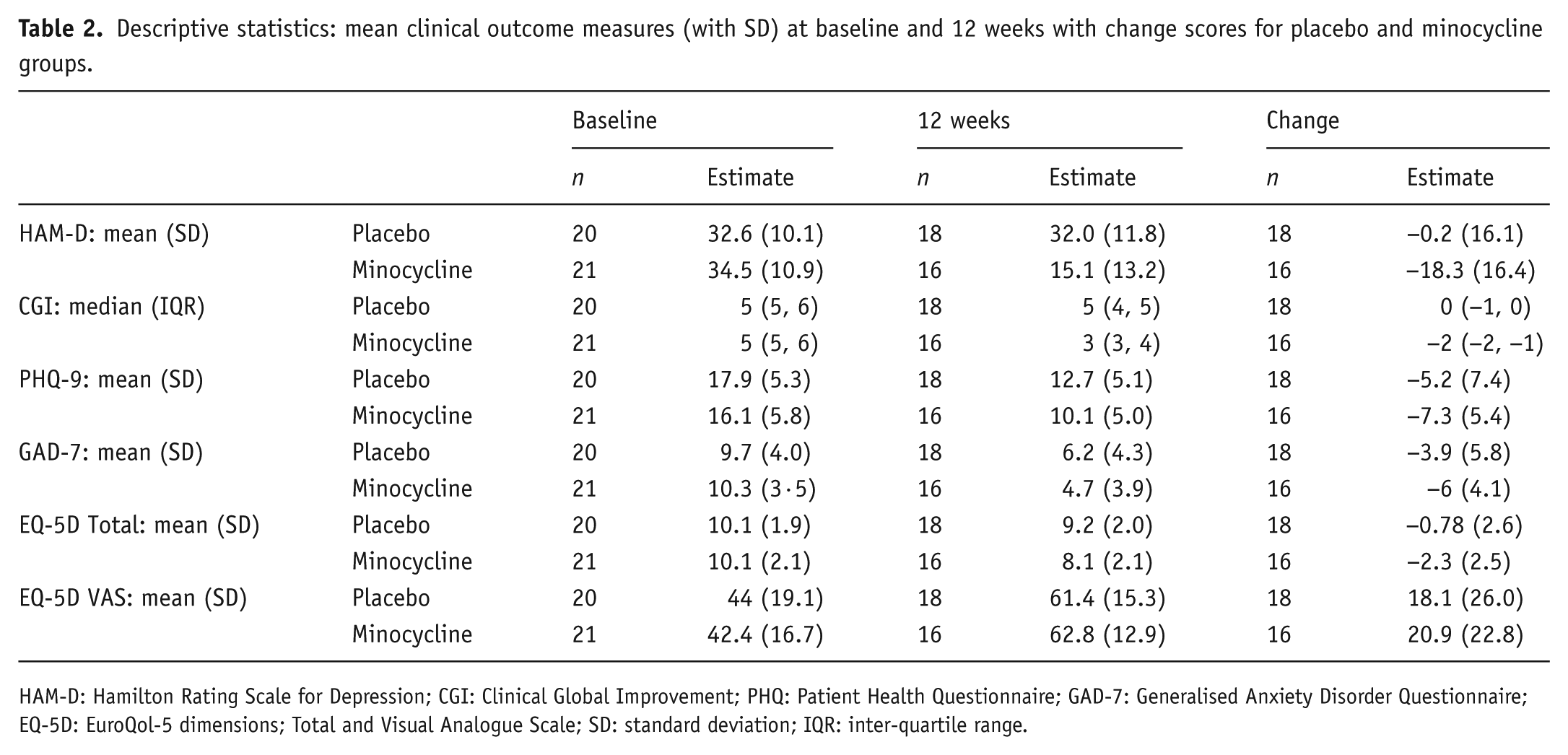
HAM-D: Hamilton Rating Scale for Depression; CGI: Clinical Global Improvement; PHQ: Patient Health Questionnaire; GAD-7: Generalised Anxiety Disorder Questionnaire; EQ-5D: EuroQol-5 dimensions; Total and Visual Analogue Scale; SD: standard deviation; IQR: inter-quartile range.
Inferential statistics for mean treatment group differences at 12 weeks adjusted for baseline outcome scores and time (weeks 2, 4 and 8) together with standardised effect size (standardised by the outcome score standard deviation).
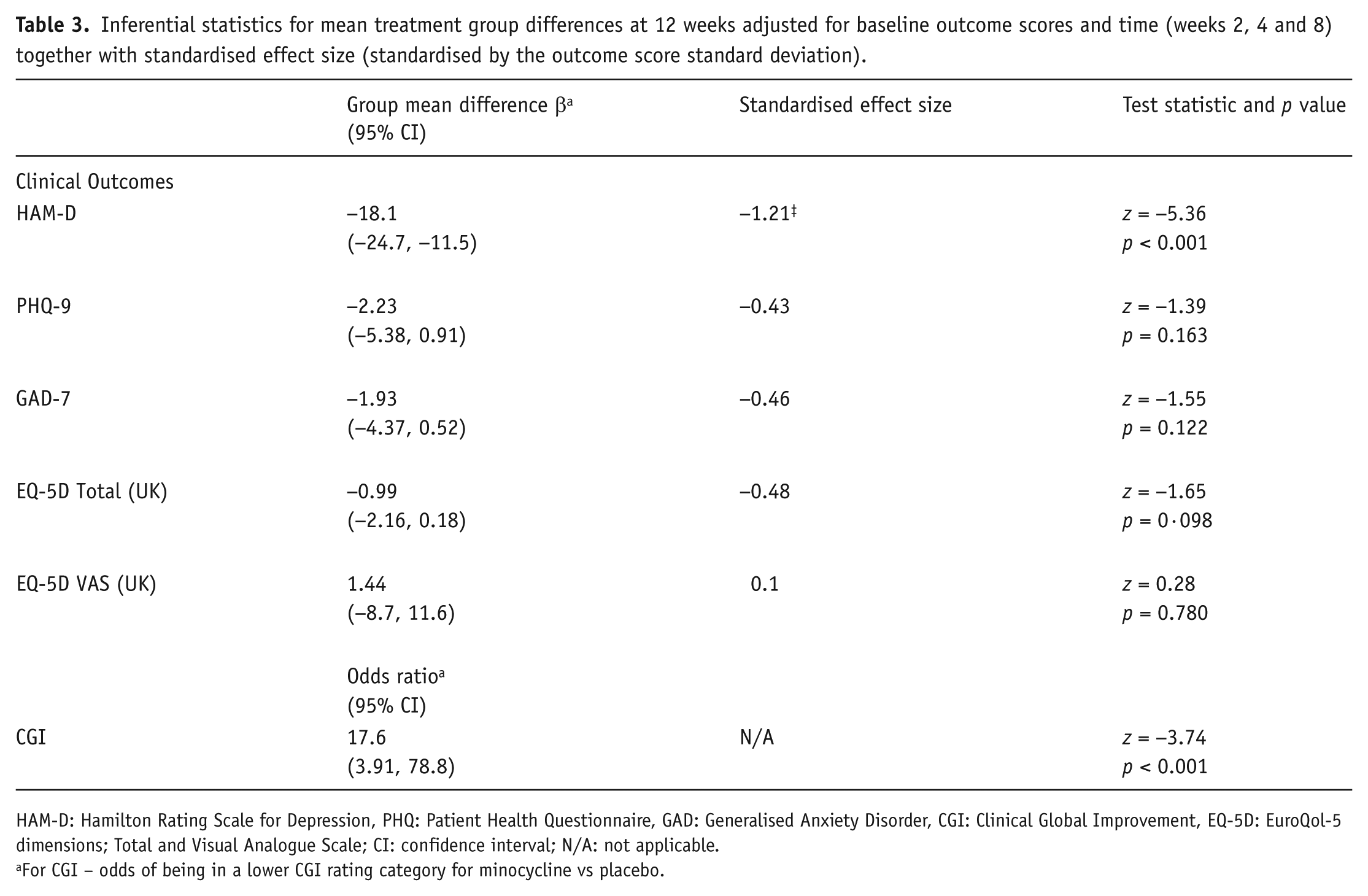
HAM-D: Hamilton Rating Scale for Depression, PHQ: Patient Health Questionnaire, GAD: Generalised Anxiety Disorder, CGI: Clinical Global Improvement, EQ-5D: EuroQol-5 dimensions; Total and Visual Analogue Scale; CI: confidence interval; N/A: not applicable.
For CGI – odds of being in a lower CGI rating category for minocycline vs placebo.
Predicted means and 95% confidence intervals for Hamilton Rating Scale total scores by treatment group and week for lower socio-economic status class participants (most frequent class).
With regards to inflammatory biomarker results, several participants refused to consent to the provision of blood samples. Baseline biomarker levels were only available for a sub-sample of approximately 17 participants (see Table 4) and we present a descriptive analysis of HAMD means in subgroups defined by CRP > 5. Only six patients had CRP levels less than 5 (two in minocycline and four in placebo). For the subgroup with CRP > 5, group difference was 17.6 (minocycline – HAMD = 15.7, placebo – HAMD = 33.3) and for CRP ≤ 5, the group difference was 1.8 points lower at 15.8 (minocycline – HAMD = 10.5, placebo – HAMD = 26.3).
Descriptive statistics for blood inflammatory markers at baseline and 12 weeks for minocycline and placebo.
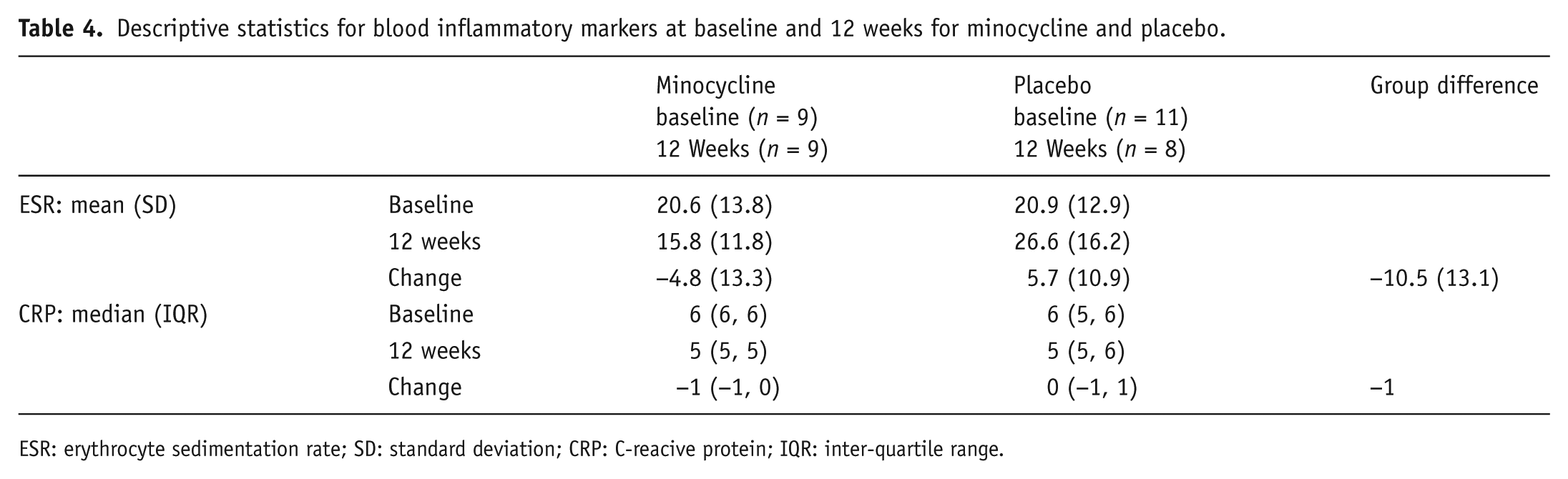
ESR: erythrocyte sedimentation rate; SD: standard deviation; CRP: C-reacive protein; IQR: inter-quartile range.
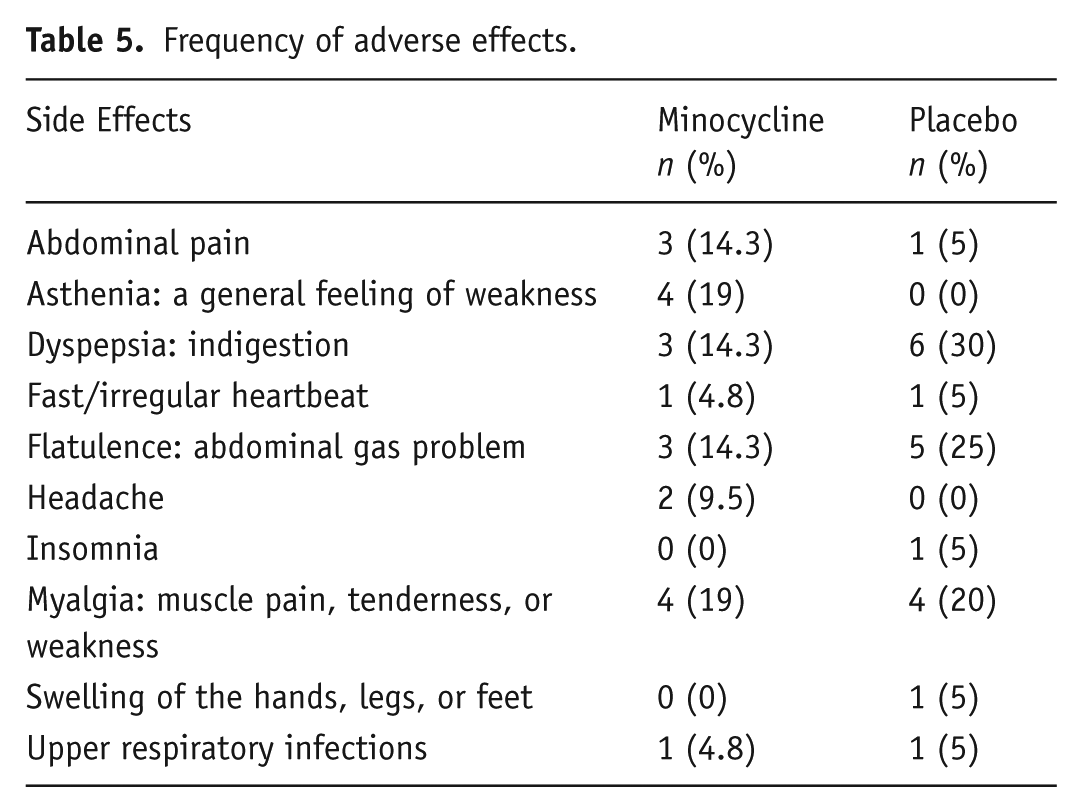
There was no significant difference in the frequency of reported adverse effects between groups. Table 5 summarises all side effects reported by participants.
Frequency of adverse effects.
Discussion
To our knowledge, this is the first randomised control trial (RCT) of minocycline in patients with treatment-resistant depressive symptoms. Our findings show that minocycline may be effective as an adjunct to TAU in patients with treatment-resistant depressive symptoms. The majority of participants in both the minocycline and placebo groups were receiving a SSRI antidepressant as part of their usual treatment. Most participants were also using an augmenting agent (either a second antidepressant or an antipsychotic). The duration since starting their first treatment for depression was over 1year for the majority of participants, which suggests that their symptoms were indeed significantly treatment refractory.
Participants randomised to minocycline showed a significant response, and the estimated mean reduction in HAMD scores was 18 points. The standardised effect size of 1.21 is large; an effect size of 0.40 or higher is considered a clinically significant response criterion in previous clinical trials of antidepressant treatments (Faries et al., 2000). The intervention was also well tolerated in comparison with placebo and there was no significant difference between groups in terms of frequency of adverse events. The absence of a response as measured by HAMD scores in the placebo group may reflect the chronicity and initial severity of the sample. A total of 95% of the participants receiving either treatment had been receiving treatment for major depressive disorder for at least 12 months. Studies have indicated that the natural history of illness and specifically, longer duration of current illness can reduce the placebo response (Rutherford and Roose, 2013). Secondly, it has been found that placebo response decreases with increasing severity of baseline depression scores, with a recent study finding that placebo response significantly declined as baseline HAMD increased (particularly as it exceeded a score of 25) (Fournier et al., 2010). The mean baseline HAMD score in the placebo group in the current study was 32.6, with only three participants scoring less than 25. It is worth noting that participants in the placebo group did show a response on the patient-rated PHQ-9 measure but not on the clinician-rated HAMD-17 and CGI measures. Lack of correlation between clinician and patient-rated outcomes are not uncommon and previous larger trials of antidepressant treatments have also reported similar discrepancies (Targum et al., 2013). The reasons for the discrepancy in the current study are unclear, although participant motivation to be involved in the trial, a heightened awareness of symptoms at baseline, and the experimental environment itself (i.e. expectancy biases) may have affected the patients’ perception of depressive symptoms and influenced self-rating during the study.
Our findings add to the growing evidence that minocycline may have antidepressant properties. As mentioned previously, open-label studies of minocycline augmentation for unipolar depression have supported this claim (Miyaoka et al., 2012). A more recent RCT of minocycline monotherapy in patients with an HIV diagnosis and mild-to-moderate depression (HAMD < 18) found significantly greater improvements in HAMD scores in patients in the minocycline group compared with those in the placebo group. There were also more partial responders in the minocycline group compared with the placebo group (Emadi-Kouchak et al., 2016). Minocycline has already shown to have beneficial effects in schizophrenia, particularly in the treatment of negative symptoms (Chaudhry et al., 2012, Oya et al., 2014). The effects of minocycline in depression may indicate that similar pathogenic mechanisms play a role in schizophrenia and in mood disorders.
Numerous mechanisms have been proposed to explain the association between inflammation and depression, ranging from disturbed neurotransmission, to disturbances in the biological mediators of stress (i.e. cortisol levels) and the release of neurotoxic metabolites. We hypothesise that minocycline acts on several of these mechanisms to produce an antidepressant effect. Biological mediators of stress (e.g. glucocorticoids) and peripheral inflammation have been found to activate neuroinflammatory processes, of which microglia exert a central role (Frank et al., 2015). Minocycline is an inhibitor of microglial activation (Soczynska et al., 2012) and has been shown to decrease depressive and anxiety symptoms in mice whist reducing pro-inflammatory cytokines (i.e. tumour necrosis factor (TNF) and interleukin (IL)-1B) and glucocorticoids (Majidi et al., 2016). The kynurenine pathway is another inflammatory pathway that is believed to be involved in depression, and has shown to be modulated by minocycline. Pro-inflammatory cytokines can activate the enzyme indoleamine 2,3-dioxygenase (IDO). Increased IDO activity decreases synthesis of serotonin from tryptophan, leading to the production of pro-depressant and neurotoxic metabolites (Grosse et al., 2016). In animal models, minocycline has been shown to block the pro-inflammatory cytokine TNFα, which activates IDO (Liu et al., 2015; O’Connor et al., 2009).
Although an altered inflammatory status may underlie a sub-group of depressive disorders, recent evidence indicates that inflammatory changes with pharmacological treatment may differ, based on clinical outcome. For instance, IL-6 appears to reduce with treatment, while TNFα may reduce alongside treatment in people who show a good clinical response but remain elevated in non-responders (Strawbridge et al., 2015). This is supported by a trial identifying a greater level of clinical response to infliximab (a TNFα antagonist) in depressed patients with high levels of TNFα (Raison et al., 2013).
In the current study, we attempted to measure ESR and CRP levels at baseline and at the end of treatment, however, many participants refused to consent to the provision of blood samples. We have included analysis of the biomarker data but given the small sample size and amount of missing data, drawing further inference would be unwise. The missing data are due in part to the limited funding for the study, which did not allow for assertive follow up of participants to ensure bloods were drawn at both baseline and end-point. We will try and address this in the replication study, which we hope will have more substantial funding. Future studies of minocycline should also include measurement of inflammatory cytokines such as IL-6 and TNFα, amongst others, to determine the association between changes in inflammatory biomarkers and improvement in depressive symptoms.
Another important consideration when examining minocycline’s putative antidepressant action is its pharmacokinetic properties and possible interactions with antidepressant drugs. There are limited data on the metabolism of minocycline (Nelis and De Leenheer, 1982) but it is plausible that it is mediated by cytochrome P450 enzymes, which are involved in the metabolism of many commonly used antidepressants. Further, recent in vitro studies indicate that minocycline may exert local inhibition of cytochrome p450 enzyme activity in neuronal cells (Regen et al., 2016). If minocycline does inhibit one or more cytochrome p450 enzymes either by competition for metabolism or a direct mechanistic effect, it may also be contributing to enhanced antidepressant activity by increasing the plasma or local concentration of antidepressant drugs.
The results of our study indicate that minocycline has a potential role as an augmentation strategy in patients with treatment-resistant depression. It is a readily available, inexpensive, off-patent drug that has low propensity to produce antibiotic resistance (Soczynska et al., 2012). It could be a cost-effective treatment option, particularly in settings with diminishing resources, such as low- and middle-income countries and other state-funded healthcare services. However, our findings should be interpreted in the light of certain limitations before minocycline can be recommended for routine clinical use. Firstly, as participants were followed up for a relatively short period of time, we are unable to comment on the long-term efficacy and safety of minocycline. Furthermore, as this was a pilot study with a small sample size, it requires replication in a larger sample. Our objective was to inform the study design in terms of recruitment, randomisation, intervention implementation, biomarker collection, blinded assessment procedures and retention for a larger scale hypothesis-testing study. We were able to achieve these aims, whilst also showing that minocycline may be a safe and effective treatment option for those with persistent depressive symptoms. Of note, we found a very strong clinical effect, which was generally supported by secondary outcome measures. In summary, minocycline 200 mg daily added to TAU for 12 weeks was well tolerated and efficacious in improving depressive symptoms in patients with treatment-resistant major depressive episodes. Future studies with larger sample sizes and longer follow-up periods are required to confirm our findings.
Footnotes
Acknowledgements
The authors would like to thank Dr Livia Carvalho for her comments on the manuscript.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MIH, ABK, JH and IQ have no conflict of interests and disclosures to declare. IBC, JFWD and NH have given lectures and advice to Eli Lilly, Bristol Myers Squibb, Lundbeck, Astra Zeneca and Janssen pharmaceuticals, for which they or their employing institution have been reimbursed. RR and MMH have received educational grants and support for academic meetings from Pfizer, Roche, Novartis and Nabiqasim. AHY has been commissioned to provide lectures and advice to all major pharmaceutical companies with drugs used in affective and related disorders. AHY has undertaken investigator-initiated studies from Astra Zeneca, Eli Lilly, Lundbeck and Wyeth. None of the companies have a financial interest in this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been funded by the Pakistan Institute of Living and Learning (PILL). It represents independent research partly funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London, and Maudsley NHS Foundation Trust and King’s College, London. The views expressed are those of the authors and not necessarily those of the National Health Service (NHS), the NIHR, nor the Department of Health.