
Abstract
Patients receiving ketamine for refractory depression and anxiety report dissociative symptoms in the first 60 min post-dose. The most commonly used instrument to assess this is the Clinician-Administered Dissociative States Scale (CADSS), developed based on the assessment of patients with dissociative symptoms. Its psychometric properties for ketamine-induced dissociation have not been reported. We evaluated these from a study using 0.25–1 mg/kg ketamine and midazolam (as an active control) in 18 patients with treatment-resistant anxiety. Dissociation ratings were increased by ketamine in a dose-dependent manner. In contrast, midazolam showed no effect on ratings of dissociation. For individual CADSS items, the magnitude of change and the ketamine dose at which changes were observed were not homogenous. The Cronbach alpha for the total scale was high (0.937), with acceptable item-rest correlations for almost all individual items. Purposefully removing items to maximise alpha did not lead to meaningful improvements. Acceptable internal consistency was still observed after removing items which lacked evidence of responsiveness at lower doses. The high Cronbach alpha values identified in this study suggests that the CADSS is an internally consistent instrument for evaluating ketamine-induced dissociation in clinical trials in anxiety, although it does not capture symptoms such as thought disorder.
Introduction
Dissociation has been described as a disturbance to the continuity of conscious thought and emotion, disorganised memory processes, confusion about self-identity, self-perception and one’s surroundings (Spiegel et al., 2013). The Clinician-Administered Dissociative States Scale (CADSS) was developed by Bremner et al. (1998) as an instrument to evaluate dissociative symptoms, to assist in the diagnosis of dissociative disorders, and to monitor changes in symptom intensity over time. While the original CADSS contained both subjective and objective items, only the 19 subjective items are routinely used. These items are rated on an ordinal scale from 0 to 4 (representing ratings of ‘not at all’ to ‘extreme intensity’). The items comprise three subscales: depersonalisation (items 3–7), derealisation (items 1, 2, 8–13, 16–19) and amnesia (items 14 and 15). A recent review of the psychometric properties of the CADSS reported it to be a reliable and valid instrument with high internal consistency across all items, including finding a strong association between subjective items and total scores and a Cronbach alpha coefficient of 0.94 (Bremner, 2014), suggesting that the 19 subjective items are closely related as a group for assessing dissociation.
The initial report that a subanaesthetic (0.5 mg/kg) dose of ketamine provided rapid improvement in depression ratings in patients with treatment-resistant depression (TRD; Berman et al., 2000) has been confirmed in multiple subsequent studies (Xu et al., 2016). The same dose of ketamine had similar rapid effects on symptoms in patients with chronic post-traumatic stress disorder (PTSD; Feder et al., 2014) and obsessive-compulsive disorder (Rodriguez et al., 2013). We recently reported that ketamine doses ranging 0.25–1 mg/kg produced rapid dose-related improvements in anxiety ratings in patients with treatment-resistant generalised anxiety disorder (GAD) and/or social anxiety disorder (SAD; Glue et al., 2017).
In all of these studies, the characteristic early side effects reported by patients after ketamine administration are dissociative. Symptom onset is within 5–10 minutes of dosing, and is resolved within 1–2 hours after dosing (Xu et al., 2016). The magnitude of dissociation is related to ketamine dose (Lai et al., 2014; Loo et al., 2016), and is correlated with peak plasma ketamine concentrations (Loo et al., 2016). Healthy individuals given 0.51 mg/kg ketamine have similar dissociative experiences as those reported by patients (Hallak et al., 2011).
The CADSS was developed based on assessment of patients with dissociative symptoms (Bremner et al., 1998). Although the scale has been widely used in ketamine clinical trials to assess drug-induced dissociation, it is unclear whether dissociation as a clinical symptom is similar to ketamine-induced dissociation. In this pilot dose–response study of ketamine in patients with treatment-resistant anxiety, we assessed whether ketamine had a broad or more selective effect on CADSS items, and the effect of ketamine dose on magnitude of change in items ratings.
Methods
This study was approved by the Southern Health and Disabilities Ethics Committee (15/STH/86), and was registered prospectively with the Australian New Zealand Clinical Trial Registry (ACTRN 12615000617561). Patients with refractory DSM-IV GAD and/or SAD (APA, 2000) were recruited from local psychiatric community services and general practices. Patient inclusion criteria included having a Hamilton Anxiety Scale (HAMA; Hamilton, 1959) score of >20, and/or a Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987) score of >60 at screening, and being aged 18 years or older. Patients were excluded if there was evidence of severe acute or chronic medical disorders, if they were pregnant or lactating, if they were taking monoamine oxidase inhibitors, thyroxine or stimulants, or had active suicidal ideation. All subjects provided signed informed consent prior to enrolment, and were assessed as suitable to participate based on review of medical history, safety laboratory tests, and vital signs. Patients were permitted to remain on current medication regimens and to continue with ongoing psychotherapy. However, no new treatments were to be started or doses/visit schedules changed.
Patients received either three ascending open-label ketamine dose levels (0.25, 0.5 and 1 mg/kg, given in that order), with 1 week between doses (n = 12), or three ascending double-blind ketamine dose levels (0.25, 0.5 and 1 mg/kg, given in that order) with a dose of midazolam 0.01 mg/kg randomly inserted into this sequence (n = 6). All medications were injected subcutaneously in the upper arm. The lowest ketamine dose was chosen as it appears to be a threshold dose in patients with TRD, (Loo et al., 2016), and we have found the 1 mg/kg dose to have the greatest durability of response in patients with TRD (Glue et al., 2011). All patients were monitored in the clinic for 2 h post-dose, with vital signs obtained pre-dose to 2 h post-dose, and anxiety ratings obtained pre-dose to 168 h post-dose (details of these data are in Glue et al., 2017). The 19 item CADSS was administered pre-dose and at 30 and 60 min after each dose of drug.
This study was a secondary analysis of the CADSS individual items, subscales and total scores for the three ketamine doses (n = 18/dose level) and the active control midazolam (n = 6). Summary statistics were calculated for these data. Inspection of the ketamine dose–response data from patients dosed open-label (n = 12) and double-blind (n = 6) showed these to be similar and thus data were combined for further analysis.
Cronbach alpha (Cronbach, 1951) was calculated for the CADSS at each time point for each dose group, including pre-dose baselines, to determine the degree of consistency between items at these times. Item-rest correlations were also calculated at these times to identify any particular items that were not consistent with the remainder of the scale. Shortened versions of CADSS were examined by pooling multiple times and/or doses with items removed on the basis that this could improve Cronbach alpha values, the items did not show statistically significant evidence of responsiveness from pre- to post-administration, or the items did not show statistically significant evidence of between-dose differences in responsiveness from pre- to post-administration. A priori, alpha values of 0.7 or above were considered acceptable. In order to detect differences prior to dosing baseline values of the CADSS and its subscales were compared between escalating doses (including midazolam) using linear mixed models with a random participant effect (to accommodate the multiple doses received by each participant). Scale and subscale responsiveness (changes from baseline to subsequent time points) was then assessed using linear mixed models with an interaction between dose (including midazolam) and time, and random effects for participant (to accommodate the multiple doses received by each participant) and participant-dose (to accommodate the multiple time points within doses). Wald tests were used to assess evidence for changes from baseline to any subsequent time (30 or 60 minutes) and to assess the interaction between dose and time (whether any such changes differed between doses). Model residuals were checked for approximate normality and homoscedasticity using histograms and scatter plots. Finally, mixed ordinal logistic regression models were used to assess responsiveness of individual items in each dose group following administration. This required combining responses of items 2, 3, and 4 into a single category in order to provide sufficient numbers at each level so that proportionality could be assessed using a generalised ordinal logistic regression model with robust clustered standard errors based on Froot’s extension to Huber–White’s sandwich estimator (Froot, 1989). The relationship between change in anxiety scores at 60 min and dissociation scores at 60 mins was evaluated using Spearman’s rank correlation. Statistical analyses were performed using Stata 14.2 and two-sided p < 0.05 was considered statistically significant.
Results
Mean CADSS total and subscale ratings for all dose arms pre-dose and 30 and 60 min post-dose are shown in Figure 1. Baseline ratings were clinically similar prior to each dose (between 3.8 and 7.3 for the total score). However, despite these small numerical differences, baseline values of CADSS did statistically significantly vary between the four interventions (Wald p < 0.001) with significantly lower values in the midazolam, 0.5 mg, and 1 mg exposures compared with 0.25 mg (all p ≤ 0.013). This effect was not significant for the amnesia (Wald p = 0.077) or depersonalisation subscales (Wald p = 0.069), although the direction of differences was similar with lower values after the initial (0.25 mg) administration, but was significant for derealisation (Wald p = 0.003) with the same pattern of pairwise comparisons (all p ≤ 0.030).
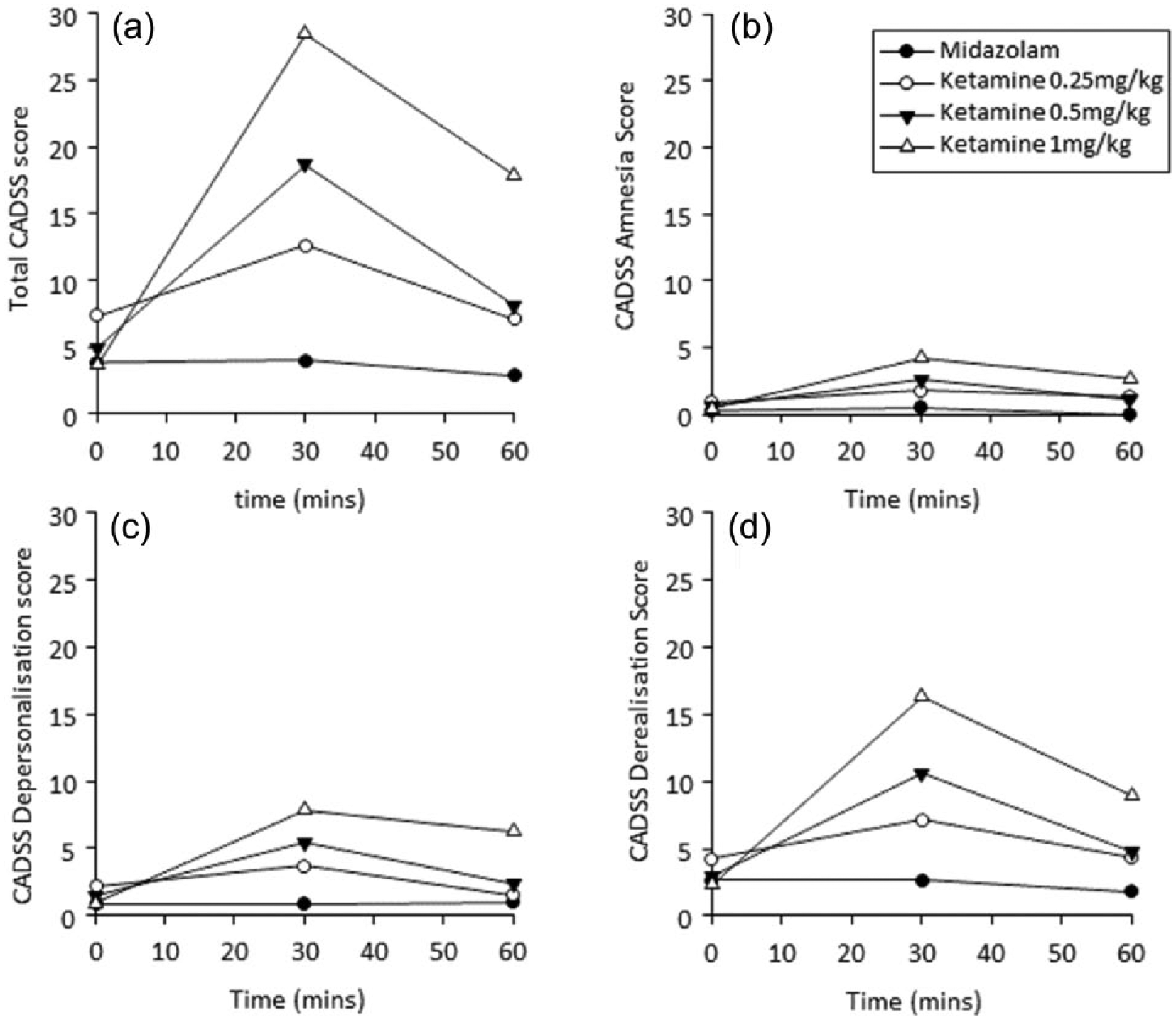
Mean CADSS total (a) and subscale ratings (b–d) for three doses of ketamine (0.25, 0.5, 1 mg/kg; n = 18) and midazolam (0.01 mg/kg; n = 6) at pre-dose, 30 and 60 min post-dose.
For ketamine, the highest total and subscale ratings occurred at 30 min, and the magnitude of this increase was dose-related. Ratings at 60 min were still elevated compared with baseline but were trending towards pre-dose values. There were no changes from baseline noted at any time for the midazolam arm. Table 1 presents p-values for changes over time from the linear mixed models of total and subscale ratings to assess responsiveness to study treatments. Evidence of responses were observed for all ketamine doses, with the smallest p-values after the two higher ketamine doses. There was no evidence of change after midazolam dosing (all p ≥ 0.856; Table 1).
Analysis of total scale and subscale changes over time to evaluate responsiveness to administered treatments (data are p-values).
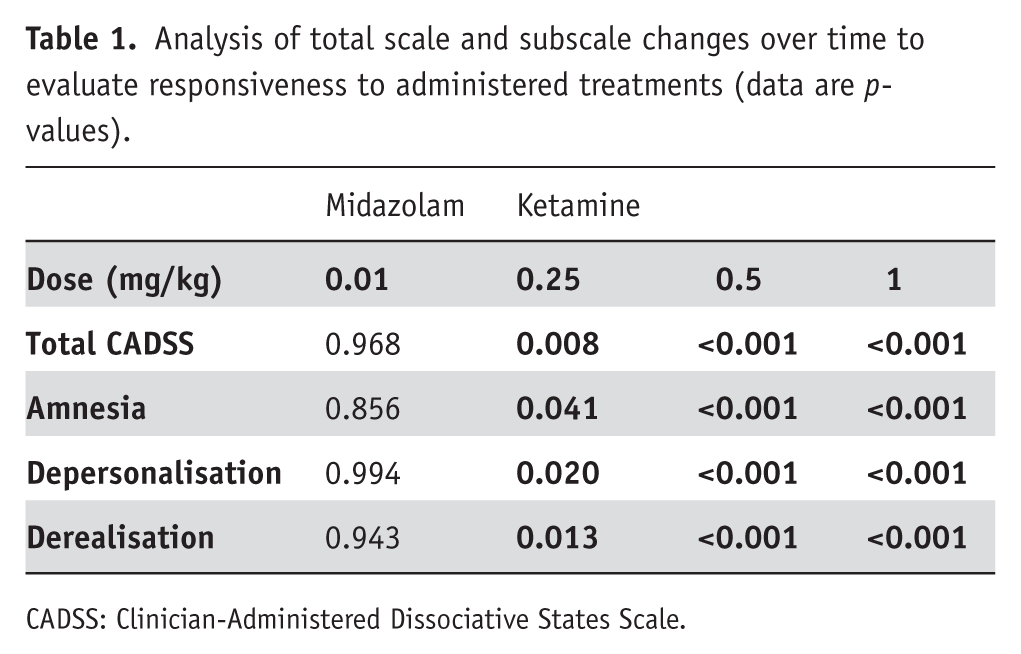
CADSS: Clinician-Administered Dissociative States Scale.
Individual item ratings
Although ratings for all scale items increased after ketamine dosing, the magnitude of change and the dose at which changes were observed were not homogenous. Figure 2 shows mean ratings for individual items at 30 min post-dose, at which time the greatest changes occurred after ketamine dosing. Larger increases were noted for some items (e.g. 2, 15 and 16) but not others (e.g. 8, 17 and 19). Minimal changes occurred in any items after midazolam dosing. Table 1 in Supplementary Material shows an analysis of changes over time for individual items by treatment arm, presented as p-values from mixed ordinal logistic regression models using responses for individual items (combining responses of items 2, 3, and 4 due to small frequencies). Statistically significant changes were observed for all ketamine doses for items 1, 2, 6, 7, 15–17, whereas significant changes were noted only at the highest ketamine dose for items 3, 5, 8, 10, 12, 13, 18 and 19.
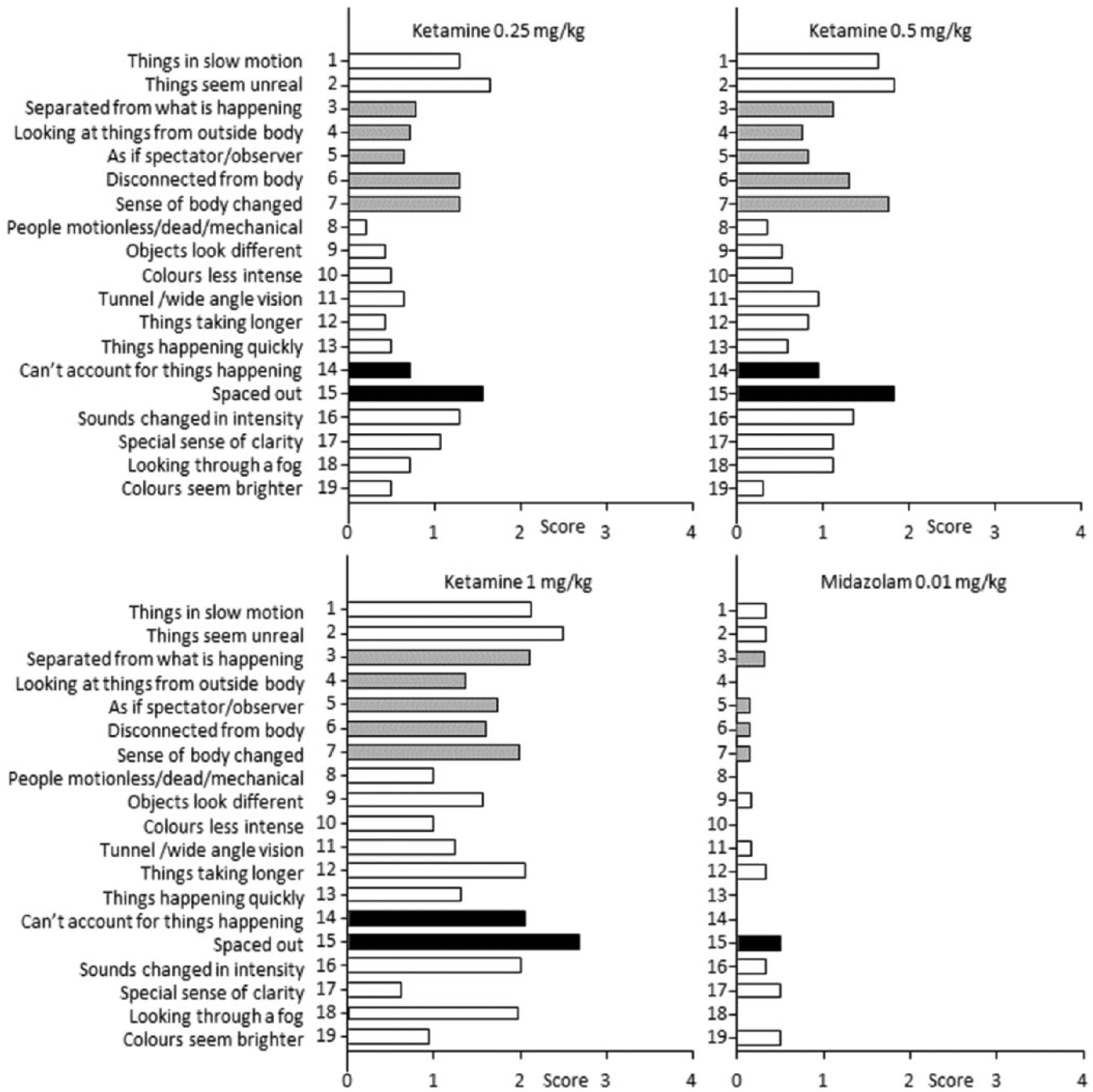
Mean individual CADSS item scores at 30 min post-dose, by treatment arm. CADSS subscales items are identified (: amnesia; : depersonalisation; : derealisation; ketamine n = 18; midazolam n = 6).
Cronbach alphas for the different treatment arms at the three timepoints are shown in Table 2. With the exception of midazolam at 60 min, all Cronbach alphas were 0.8 or greater (‘good’ internal consistency), well above our threshold of 0.7 for acceptable internal consistency, and the majority were above 0.9 (‘excellent’ internal consistency). As noted by Streiner (2003), high values of alpha (>0.9) suggest unnecessary redundancy in the scale. Supplementary Material Table 2 shows item-rest correlations for individual items (these are correlations of each item with the summed index with that item excluded). The majority of these were >0.5.
Item consistency table, including shortened scales.
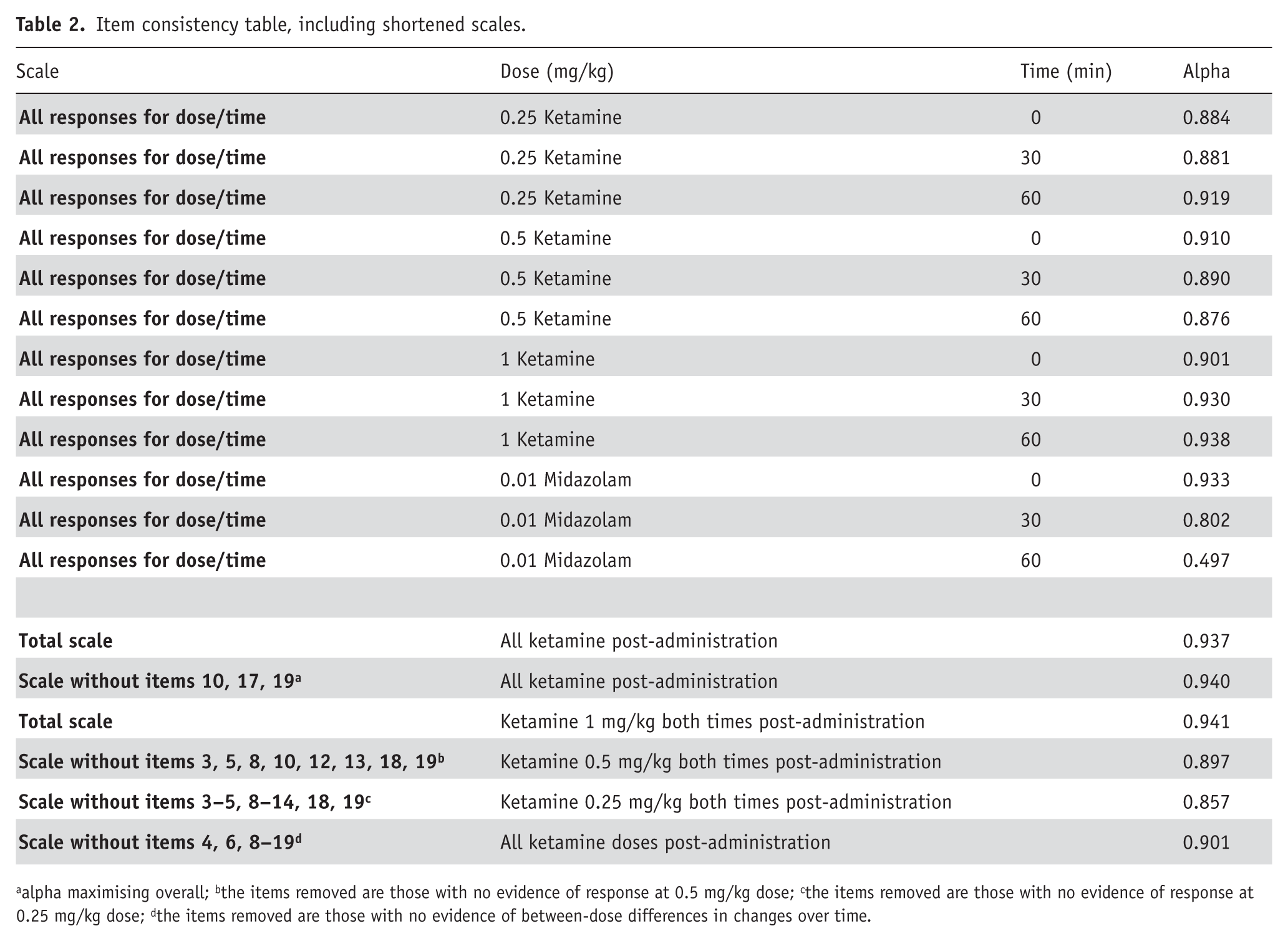
aalpha maximising overall; bthe items removed are those with no evidence of response at 0.5 mg/kg dose; cthe items removed are those with no evidence of response at 0.25 mg/kg dose; dthe items removed are those with no evidence of between-dose differences in changes over time.
We investigated several shortened scales to see if removal of individual items could improve alpha, or if removing items not showing consistent responsiveness was viable. Removal of items 10, 17 and 19 (which incrementally increased the alpha because of their low item-rest correlations) produced only a small increase in alpha (0.937 to 0.940; Table 2). Removing items with no evidence of response at ketamine doses of 0.25 or 0.5 mg/kg (all items were responsive at the 1.0 mg/kg dose in Supplementary Table 1), or items that did not show evidence of between-dose differences in changes over time produced slightly lower alpha values compared with the total scale alpha (Table 2, bottom rows). In all cases, alpha values were still >0.8.The 60 min FQ/CADSS correlation was r = −0.14, p = 0.31, and the HAMA/CADSS correlation was r = −0.15, p = 0.29.
Discussion
This analysis of changes in dissociation ratings after ketamine and midazolam dosing in patients with treatment-resistant anxiety has identified a number of key findings. Dissociation ratings are increased by ketamine in a dose-dependent manner. In contrast, midazolam, a psychoactive control in this study, has no effect on ratings of dissociation. For individual scale items, the magnitude of change and the dose at which changes were observed were not homogenous. Cronbach alpha for the total CADSS scale after ketamine dosing was high (0.937), with acceptable item-rest correlations for almost all individual items. Exploratory analyses in which specific items were removed did not meaningfully improve alpha, but neither did they worsen it to unacceptable levels. Dissociation scores at 60 min were not correlated with changes in anxiety ratings.
The finding that dissociation ratings were increased by ketamine in a dose-dependent manner is consistent with earlier reports for ketamine in patients with TRD by Lai et al. (2014) and Loo et al. (2016) over a lower ketamine dose range (0.1–0.5 mg/kg), and with esketamine 0.2–0.4 mg/kg (Singh et al., 2016). In contrast, midazolam, the psychoactive control in this study, had no effect on ratings of dissociation. Benzodiazepines appear to have minimal effects on dissociation ratings (e.g. lorazepam in healthy volunteers (Krystal et al., 1998)) and a range of midazolam doses in patients with PTSD (0.045 mg/kg; Feder et al., 2014), TRD (0.01 mg/kg; Loo et al., 2016; 0.045 mg/kg; Murrough et al., 2013) and cocaine dependence (0.025 mg/kg; Dakwar et al., 2017).
The Cronbach alpha for the total CADSS scale after ketamine dosing was high (0.937), very similar to that reported by Bremner et al. (1998) (0.94), with acceptable item-rest correlations for almost all individual items. Sensitivity analyses, in which specific items were removed, did not meaningfully improve alpha. Potentially, shortened versions of the CADSS could be developed with acceptable internal consistency, if some less responsive items were removed (Table 2). However, the scale is quick to complete and development of a shorter version may be of limited value.
It is possible that additional items could usefully be added to the scale to enhance its content validity for ketamine-induced dissociation. For example, the CADSS does not have an item rating alterations in thought. At least half of the patients in this study reported the experience of having difficulty expressing themselves (turning thoughts into speech), or felt their thoughts were rambling. A single dose study of ketamine in healthy volunteers (Pomarol-Clotet et al., 2006) reported in detail on the phenomenology of ketamine-induced thought disorder, and highlighted a number of differences between this and thought disorder in schizophrenia. This study and Adler et al. (1998) identified poverty of content of speech and circumstantiality as the main observed abnormalities after ketamine, in contrast to other changes noted in patients with schizophrenia.
There are a number of shortcomings in this analysis that should be acknowledged. This was a post-hoc analysis of a relatively small data set, and any findings will require replication. Patients in this study had treatment-resistant anxiety, but were not currently depressed. Although we anticipate that psychometric analysis of CADSS data in depressed patients treated with ketamine will show similar results to those reported here, this requires confirmation. We did not directly compare ketamine-induced dissociation with dissociation as a clinical symptom in patients, however we note that our total scale alpha (0.937) was similar to that reported by Bremner et al. (1998) (0.94), based on assessment of patients with dissociative symptoms.
In conclusion, the high Cronbach alpha identified in this study suggests that the CADSS is a valid instrument for evaluating ketamine-induced dissociation in clinical trials in anxiety, and that the scale is sensitive to identifying dose-related changes in dissociation.
Footnotes
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Glue has a contract with Douglas Pharmaceuticals to develop novel ketamine formulations. Within the last 3 years Dr Glue has received research funding from DemeRx Inc and has participated in an advisory board for Janssen Pharma. No other authors have disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.