
Abstract
Background:
Recent studies suggest that anti-inflammatory medication may play a role in the treatment of mood disorders.
Aims:
The purpose of this study was to determine the efficacy of anti-inflammatory drugs in patients with major depressive disorder and bipolar disorder.
Method:
The Cochrane Central Register of Controlled Trials, PubMed, EMBASE, PsychINFO and Clinicaltrials.gov were searched from inception until 15 April 2017 for completed and on-going randomized controlled trials of anti-inflammatory agents for major depressive disorder and bipolar disorder. Data from randomized controlled trials assessing the antidepressant and anti-manic effect of adjunctive mechanistically diverse anti-inflammatory agents were pooled to determine standard mean differences (SMDs) compared with placebo and/or treatment as usual.
Results:
Patients receiving anti-inflammatory agents showed lower post-treatment depressive symptom scores compared with those receiving placebo with a standard mean difference of −0.71 (six randomized controlled trials, n=214, 95% CI −1.24 to −0.17, p=0.009). Anti-inflammatory treatment was found to reduce post-treatment manic symptom scores with a standard mean difference of −0.72 (three randomized controlled trials, n=96, 95% CI −1.31 to −0.13, p=0.02). Anti-inflammatories did not show a statistically significant improvement in the secondary outcome measure (change in symptom scores from baseline to outcome).
Conclusions:
Further high quality trials are needed before making recommendations for the routine clinical use of anti-inflammatories in the treatment of mood disorders.
Introduction
Mood disorders are a leading cause of morbidity and mortality. Major depressive disorder (MDD) and bipolar disorder cause significant disability worldwide (Whiteford et al., 2013). These conditions are frequently chronic and debilitating, often with poor recovery between episodes (Malhi et al., 2007; Marotta et al., 2015). Despite advances in the treatment of mood disorders, current treatments are often not effective and may be poorly tolerated due to adverse effects (Geddes and Miklowitz, 2013; Linde et al., 2015; Rush et al., 2006; Vergunst et al., 2013). There remains a clear need for new treatment approaches. Recently promising data has indicated that inflammation may play an important role in mediating mood disorders. Multiple reviews have demonstrated that MDD and bipolar disorder are associated with abnormal pro- and anti-inflammatory immunological markers (Baumeister et al., 2014; Dowlati et al., 2010; Goldstein et al., 2009; Howren et al., 2009). The evidence that mood disorders (or some subgroups thereof) are inflammatory-related disorders derives from multiple sources including the observation that both MDD and bipolar disorder are associated with raised inflammatory markers in the absence of a physical illness (Baumeister et al., 2014; Dantzer et al., 2008; Munkholm et al., 2013; O’Donovan et al., 2013; Song et al., 1994). Recent evidence indicates that inflammatory changes with pharmacological treatment may differ based on clinical outcome: while interleukin (IL)-6 appears to reduce with pharmacological treatment, tumour necrosis factor (TNF)α levels may only decrease in treatment responders (Strawbridge et al., 2015). This is supported by a trial identifying improvements in clinical response to infliximab (a TNFα antagonist) in MDD patients with high levels of inflammatory markers (Raison et al., 2013).
Recent reviews and meta-analyses have suggested that anti-inflammatory medication may play an important role in the treatment of mood symptoms (Ayorech et al., 2015; Faridhosseini et al., 2014; Fond et al., 2014; Kohler et al., 2014; Rosenblat et al., 2016). However, meta-analyses have only evaluated the efficacy of these compounds for a specific disorder (e.g. bipolar disorder or MDD), and only for depressive symptoms (Kohler et al., 2014; Rosenblat et al., 2016). There has been significant research outputs from trials of anti-inflammatory agents in mood disorders since the literature search for the most recent meta-analyses was completed and in view of the on-going challenges posed by treatment resistance in mood disorders, (Geddes and Miklowitz, 2013; Linde et al., 2015; Rush et al., 2006; Vergunst et al., 2013), there remains a need to update the evidence-base for the use of novel treatments including anti-inflammatory medication. No meta-analyses have yet assessed anti-inflammatory treatments for mania. Furthermore, combining studies of both bipolar and unipolar depression may have the advantage of investigating inflammation as a trans-diagnostic target for multiple neuropsychiatric disorders; few studies have directly compared inflammation in unipolar and bipolar depression but there do not appear to be marked differences between these subpopulations (Goldsmith et al., 2016; Su et al., 2011) and increases in statistical power can be achieved by considering the two together.
The primary aim of this systematic review and meta-analysis is to determine the efficacy of anti-inflammatory drugs in improving both depressive and manic symptoms in patients with MDD and bipolar disorder. The review was registered on the PROSPERO database for systematic reviews and it is reported here following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Moher et al., 2015).
Method
Search strategy
We searched the Cochrane Central Register of Controlled Trials, PubMed, EMBASE, PsychINFO and the National Institute of Health website Clinicaltrials.gov from inception until 15 April 2017. Searches were not restricted by language. Citation lists of relevant studies and reviews were also checked for relevant trials. The authors of significant papers over the last five years and other experts in the field were also contacted and asked if they were aware of any additional studies.
The following search string was used: ((depression) OR (major depressive disorder) OR (depressive symptoms) OR (bipolar disorder) OR (mania) OR (manic symptoms)] AND [(anti-inflammatory) OR (NSAID) OR (acetylsalicylic acid) OR (cyclooxygenase 2 inhibitor) OR (COX-2) OR (antibiotics) OR (celecoxib) OR (infliximab) OR (etanercept) OR (minocycline) OR (N-acetyl cysteine) OR (NAC)] AND [(trial) OR (RCT) OR (treatment)).
Inclusion and exclusion criteria
Studies included were restricted to randomised controlled trials and crossover trials with male and female participants of all ages who met International Statistical Classification of Diseases and Related Health Problems 10th revision (ICD-10) (WHO, 1992) or Diagnostic and Statistical Manual of Mental Disorders 5th revision (DSM-5) (American Psychiatric Association, 2013) criteria for MDD or bipolar disorder. Trials with ICD 9 and DSM III/IIIR/IV/IVR diagnoses approximating to these codes were also included. All subtypes of major depressive and bipolar disorder were included. Dysthymia and cyclothymia were excluded. Clinical trials that measured depressive symptoms in patients with physical health comorbidities who did not meet criteria for MDD or bipolar disorder (i.e. not experiencing a current depressive, hypomanic or manic episode) at baseline were also excluded.
For the purposes of this review, anti-inflammatory treatments are defined as non-steroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase (COX)-2 inhibitors, pro-inflammatory cytokine inhibitors, N-acetyl cysteine (NAC) and minocycline hydrochloride. Minocycline has effects on multiple interacting systems (including inflammatory and oxidative pathways) that are thought to be involved in the pathophysiology of mood disorders (Soczynska et al., 2012). NAC has also been included as an anti-inflammatory treatment since recent evidence shows that it modulates pathophysiological processes including oxidative stress, neurogenesis and apoptosis, mitochondrial dysfunction and neuroinflammation (Dean et al., 2011).
Other agents such as polyunsaturated fatty acids (Appleton et al., 2010), statins (O’Neil et al., 2012), the antidiabetic drug pioglitazone (Kashani et al., 2013; Sepanjnia et al., 2012; Zeinoddini et al., 2015) and the nutritional supplement curcumin (Ng et al., 2017) have all been proposed as agents with supposed anti-inflammatory and antidepressant actions. However, as the anti-inflammatory effects of these agents are only considered to be putative, they were excluded from the present meta-analysis. In light of the evidence supporting their anti-inflammatory action, drugs included in this review were: ibuprofen, aspirin, diclofenac, naproxen sodium, celecoxib, anti-tumour necrosis factor (TNF)-α (etanercept, infliximab, adalimumab), ustekinumab, NAC and minocycline. We included studies where anti-inflammatories were administered in trials either as single or adjunctive therapy (in cross-over trials). The minimum length of therapy for inclusion was one day. Criteria for maximum length of therapy or length of follow-up were not stipulated. Anti-inflammatory treatments were compared with: placebo, antidepressant treatment, mood stabiliser treatment, combination treatment (e.g. antidepressant and mood stabiliser) and other treatments e.g. antipsychotic medication.
Outcome measures
The primary outcome measure was the effect of anti-inflammatory drugs in the treatment of acute mood symptoms. If more than one symptom measure was provided in a particular study, the primary outcome measure for the study was preferred to other measures.
For depressive episodes, treatment effects were measured by: severity of depressive symptoms at endpoint as measured by validated depressive symptoms rating scales (Beck’s Depression Inventory (BDI), Hamilton Depression Rating Scale (HAM-D), Montgomery-Asberg Depression Rating Scale (MADRS), Inventory of Depressive Symptomatology (IDS)). Secondary outcome was changes (from baseline to endpoint) in validated depressive symptom rating scales (BDI, HAM-D, MADRS and IDS).
For manic episodes, efficacy of treatment was measured by: severity of manic symptoms at endpoint as measured by validated manic symptom rating scales (Young Mania Rating Scale (YMRS), Altman Self-Rating Mania Scale (ASRM)). Secondary outcome was changes (from baseline to endpoint) in validated manic symptoms rating scales (YMRS, ASRM).
Data extraction
All studies generated from the systematic search were evaluated against the pre-defined inclusion criteria by one review author (MIH). Abstracts for these studies were screened and irrelevant studies excluded. Full texts for all studies that met the inclusion criteria were obtained. Any disparities were addressed by reaching consensus between review authors (RS, PRAS and AHY). Data extraction was conducted by two review authors (MIH, RS) and included description of participants, description of the intervention and control groups, psychometric data and outcomes. Two review authors (PRAS, AHY) undertook quality assessments. The bias risks of the randomised clinical trials included were addressed based on the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions using the Quality Assessment Tool for Quantitative Studies (Effective Public Health Practice Project, 1998; Higgins and Green, 2011). Study data quality was assessed in six domains: presence of selection bias, strength of study design, presence of confounders, blinding of outcome assessors, strength of data collection methods and reporting of withdrawals and drop-outs. Disagreements were resolved via further discussion with a third review author (RS).
Statistical analysis
Data was entered in to the Review Manager (Revman version 5.3) (Cochrane Collaboration, 2011) software program by one review author (MIH). Meta-analyses were conducted where data were available for ≥3 studies per main comparison. The main comparisons were anti-inflammatory treatment versus placebo or placebo added to treatment-as-usual (TAU). The primary outcome assessed was severity of mood symptoms at treatment endpoint measured using a pooled effect size of depressive/manic symptom scores between patients treated with adjunctive anti-inflammatory agents compared with those treated with adjunctive placebo and/or TAU.
Other outcomes included changes (from baseline to endpoint) in validated depressive and manic symptom rating scales. Sensitivity analyses comparing anti-inflammatories to placebo and/or TAU for unipolar depression and bipolar depression were undertaken.
Pooling of effect sizes and tests of heterogeneity were conducted using Review Manger 5.3 software. Cohen’s d effect sizes were calculated using continuous variables to determine the standardised mean difference (SMD) of change in depression scores for placebo-controlled trials. SMD was also calculated for post-treatment symptoms severity scores as a secondary outcome measure. A random effects model was used (DerSimonian and Laird, 1986). Heterogeneity of analyses was assessed using the I2 statistic which indicates the proportion of effect size variance likely due to study heterogeneity (Higgins et al., 2003). To further explore the sources of heterogeneity, meta-regressions were undertaken on the main comparisons to account for study quality, baseline symptom severity, and length of treatment. Meta-regressions utilised a restricted maximum likelihood (REML) method for estimating model parameters. The likelihood of publication bias was also assessed for the main comparisons using Egger’s test (Egger et al., 1997) in comparisons that contained at least 10 studies.
Results
Using our search criteria, 9053 records were identified. Following inspection of abstracts, 23 suitable papers were identified and the full-texts were assessed (see Figure 1). Nine of these papers were then excluded from the quantitative meta-analysis for the following reasons: (a) they reported outcomes (i.e. cognitive symptoms and suicidal ideation respectively) that did not pertain to overall mood symptom severity (Dean et al., 2012; Waterdrinker et al., 2015); (b) full results could not be obtained despite efforts to contact the authors (Berk et al., 2012, 2014; Halaris et al., 2014; Mousavi et al., 2017; Raghuvanshi et al., 2013); (c) they reported results of a secondary analysis of a primary study (Magalhães et al., 2011a); 4) they did not have a placebo/TAU arm (Mohammadinejad et al., 2015). A total of 14 studies were therefore included in the meta-analysis whilst the excluded studies were included in the qualitative analysis.
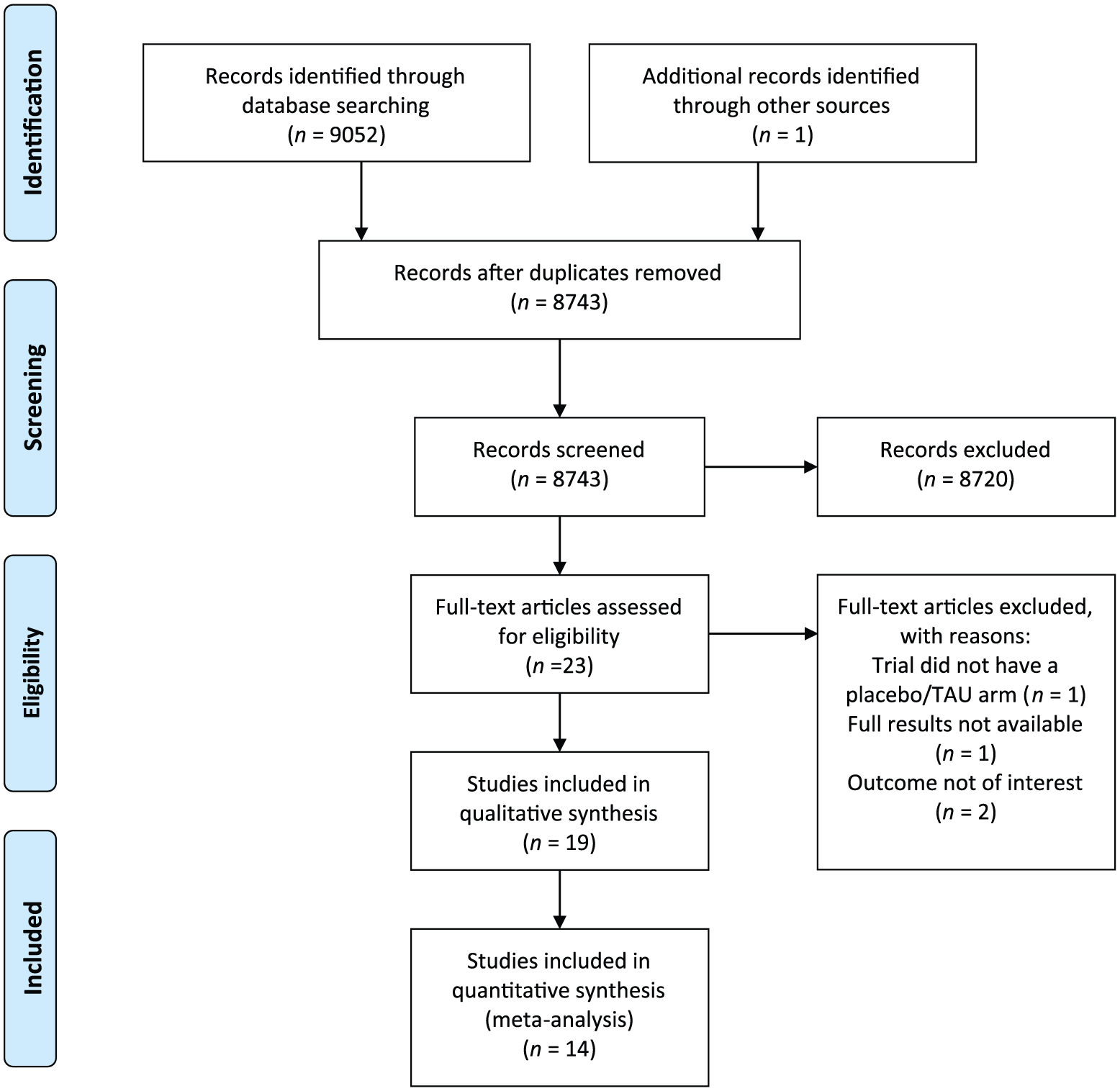
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram. TAU: treatment-as-usual.
Study characteristics
Tables 1 and 2 present study characteristics for each trial. Included studies randomised 847 participants ranging from 30–269 per study. Studies were conducted in the USA (Nery et al., 2008; Raison et al., 2013), Iran (Abbasi et al., 2012; Akhondzadeh et al., 2009; Arabzadeh et al., 2015; Emadi-Kouchak et al., 2016; Jafari et al., 2015; Kargar et al., 2015; Majid et al., 2015; Mousavi et al., 2017; Saroukhani et al., 2013), Germany (Müller et al., 2006) and Australia (Berk et al., 2008, 2012, 2014; Magalhães et al., 2011a,b, 2013). Seven RCTs investigated MDD, four RCTs investigated bipolar depression and three investigated manic/hypomanic symptoms. Only one RCT included patients under the age of 18 years (Mousavi et al., 2017).
Identified clinical trials investigating anti-inflammatory treatment in major depressive disorder.
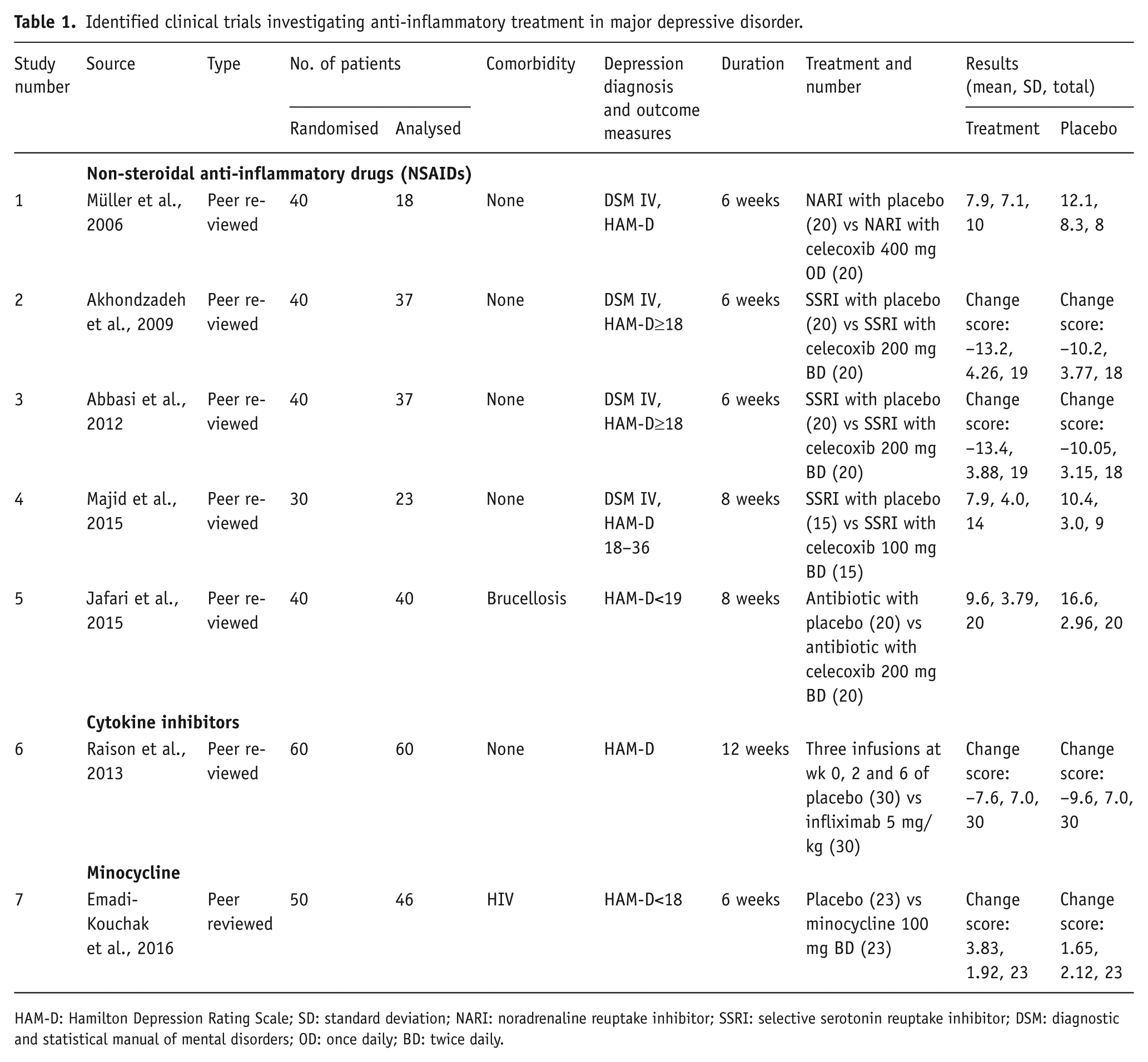
HAM-D: Hamilton Depression Rating Scale; SD: standard deviation; NARI: noradrenaline reuptake inhibitor; SSRI: selective serotonin reuptake inhibitor; DSM: diagnostic and statistical manual of mental disorders; OD: once daily; BD: twice daily.
Identified clinical trials investigating anti-inflammatory treatment in bipolar disorder.
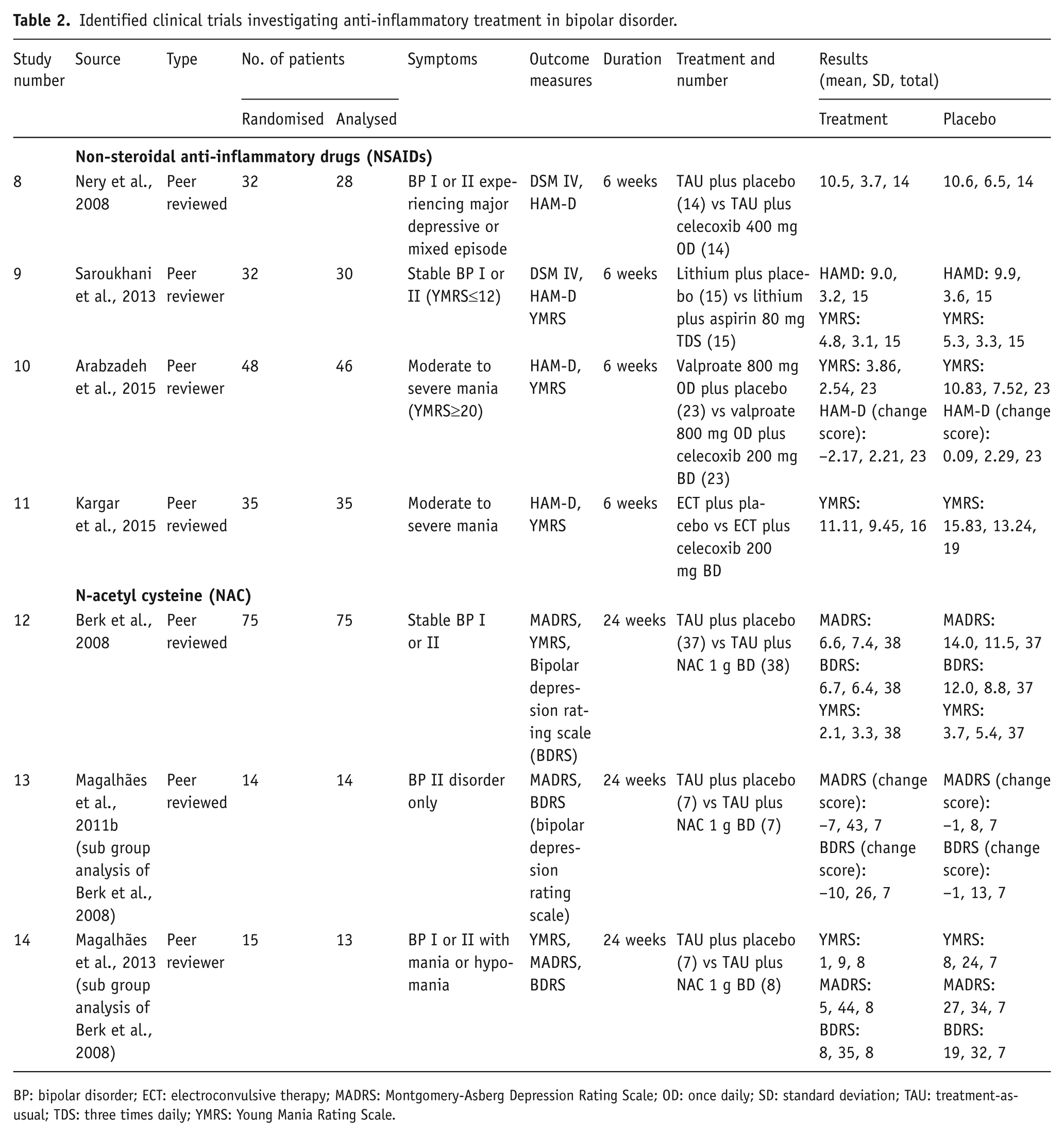
BP: bipolar disorder; ECT: electroconvulsive therapy; MADRS: Montgomery-Asberg Depression Rating Scale; OD: once daily; SD: standard deviation; TAU: treatment-as-usual; TDS: three times daily; YMRS: Young Mania Rating Scale.
Eleven studies investigated the COX-2 selective non-steroidal anti-inflammatory drug, celecoxib (Abbasi et al., 2012; Akhondzadeh et al., 2009; Arabzadeh et al., 2015; Halaris et al., 2014; Jafari et al., 2015; Kargar et al., 2015; Majid et al., 2015; Mohammadinejad et al., 2015; Mousavi et al., 2017; Müller et al., 2006; Nery et al., 2008) and three studies investigated N-acetyl cysteine (Berk et al., 2008, 2012, 2014), although there were several secondary analyses published based on one of these original trials (Dean et al., 2012; Magalhães et al., 2011a,b, 2013; Waterdrinker et al., 2015). We included one study investigating the cytokine inhibitor infliximab (Raison et al., 2013), one investigating aspirin (Saroukhani et al., 2013) and one investigating minocycline (Emadi-Kouchak et al., 2016). Length of treatment varied from 6–24 weeks (mean 10.57, standard deviation (SD) 7.46). Two studies included patients with physical health comorbidity (brucellosis and human immunodeficiency virus (HIV) (Emadi-Kouchak et al., 2016; Jafari et al., 2015).
Assessment of bias
The quality of the included clinical trials was assessed systematically via evaluation of bias in accordance with the Cochrane Handbook for Systematic Review of Interventions (Higgins and Green, 2011). The results are summarised in Supplementary Material, Table 1. Three studies had a high risk for bias for inadequate reporting of withdrawals and drop-outs (Abbasi et al., 2012; Magalhães et al., 2013; Müller et al., 2006). One study was found to have a high risk of bias in several categories for inadequate reporting of participant selection, concealment, control of confounders and data collection methods (Majid et al., 2015). Publication bias was assessed using a funnel plot, as shown in Supplementary Material, Figures 1 and 2. An Egger’s test could not be conducted as a minimum of 10 studies is required for sufficient power of this test to distinguish chance from real asymmetry in the funnel plots.
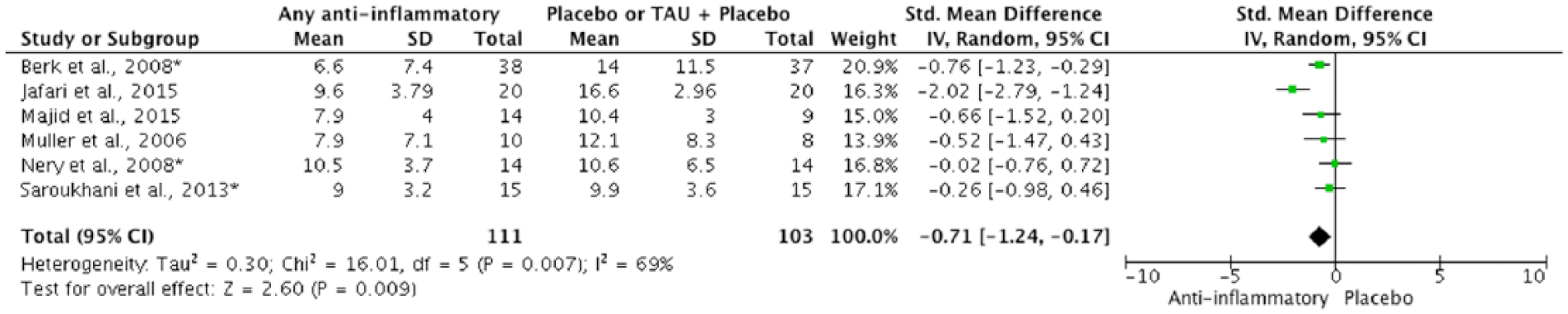
Depression symptoms scores (post-treatment) (pooled effect size).
Outcomes
Anti-depressant effect of anti-inflammatory agents
With regards to the primary outcome, six trials (n=214 patients) showed lower post-treatment depressive symptoms scores following treatment with anti-inflammatory interventions when compared to TAU or placebo with an overall effect size of −0.71 (95% confidence interval (CI) −1.24 to −0.17, p=0.009; I2= 69%, p=0.007) (Figure 2). These studies did not report change in depressive symptoms scores and only provided data on post-treatment severity, thus they are analysed separately.
Five of the 12 available studies investigating MDD and bipolar depression reported mean change in depressive symptoms scores at the end of treatment. From the results of these studies, anti-inflammatory treatment did not yield a statistically significant antidepressant effect (i.e. change in depressive symptom scores from baseline to outcome) with a pooled effect size (SMD) of −0.52 (95% CI −1.01 to 0.05, p=0.07) (Figure 3). This effect estimate was based on a total of 194 participants and was associated with substantial heterogeneity; I2=72% (p<0.001).

Change in depressive symptom scores.
Anti-manic effect of anti-inflammatory agents
Three studies investigated the effect of anti-inflammatory treatment in a total of 96 patients. Overall, anti-inflammatory treatment reduced manic symptom scores with an overall effect size of −0.72 (95% CI −1.31 to −0.13, p=0.02, I2= 46%, p=0.16) (Figure 4). The studies included in this analysis only reported post-treatment severity and not change in manic symptoms scores.

Manic symptoms scores (post-treatment).
Subgroup analyses
We conducted sub-analyses on the main comparisons in studies of sufficient size and found that of the seven studies using adjunctive NSAIDs for depressive symptoms, six were RCTs of celecoxib. Celecoxib showed a trend of superiority over placebo and/or TAU when comparing post-treatment depressive symptom scores however this was not statistically significant (four RCTs, n=109; SMD −0.81, 95% CI −1.71 to 0.09, p=0.08; I2=79%, p=0.003). Two RCTs (Abbasi et al., 2012; Arabzadeh et al., 2015) were excluded from this subgroup analyses because they did not report post-treatment symptom severity scores.
To determine the influence of a placebo-only comparator versus placebo added to TAU we conducted a sub-analysis excluding studies that used a placebo-only control group. Only one such study was identified (Emadi-Kouchak et al., 2016), which was included in the original meta-analysis of the secondary outcome measure. The sub-analysis revealed that anti-inflammatories still did not yield a statistically significant antidepressant effect when considering the secondary outcome of change in depressive symptoms (four RCTs, n=148, SMD=−0.38, 95% CI −1.01 to 0.25, p= 0.24, I2=70%, p=0.02). A sub-analysis of trials recruiting patients with bipolar depression indicated that anti-inflammatory treatments showed a trend towards an antidepressant action in this group, although this was not statistically significant (three RCTs, n=133, SMD=−0.42, 95% CI −0.88 to 0.04, p= 0.07, I2=38%, p=0.2).
Further sub-analyses indicated that anti-inflammatory treatments had an antidepressant action when considering the primary outcome of post-treatment symptom severity (five RCTs, n=174, SMD=−0.51, 95% CI −0.81 to −0.20, p=0.001, I2=0%, p=0.50) irrespective of the presence of a co-morbid physical health condition. However the secondary outcome measure of change in depressive symptoms from baseline to endpoint were not statistically significant when studies of patients with physical health comorbidities were excluded (four RCTs, n=148, SMD=–0.38, 95% CI −1.01 to 0.25, p=0.24, I2=70%, p=0.02),
Meta-regression analyses were completed to determine the association of study quality, baseline symptom severity and duration of treatment with antidepressant effects of anti-inflammatory agents. None of the three variables significantly affected the SMD for the effect of anti-inflammatory agents on post-treatment depressive symptom severity. Conversely, all three variables showed a significant linear relationship for the secondary outcome of effect of anti-inflammatory agents on change in depressive symptom scores: studies with a poorer quality score (p=0.004), more severe baseline depression severity (p = 0.003) or longer duration of symptoms (p=0.005) yielded a greater anti-inflammatory treatment benefit.
Qualitative analysis
Given the variable profile of each anti-inflammatory compound, the qualitative analysis of results will be divided by agent.
Celecoxib
We identified 11 RCTs of celecoxib in mood disorders. Six of these trials included patients with a diagnosis of MDD (Abbasi et al., 2012; Akhondzadeh et al., 2009; Jafari et al., 2015; Majid et al., 2015; Mohammadinejad et al., 2015; Müller et al., 2006).
Two studies included patients with bipolar depression (Halaris et al., 2015; Nery et al., 2008). The RCT by Nery et al. showed that patients experiencing acute bipolar depression experienced a rapid but short-lived antidepressant effect with celecoxib; this was not maintained at the study end-point (Nery et al., 2008). The other RCT was not included in our meta-analysis as full results were not available although the authors’ interim analysis showed that participants receiving celecoxib as an adjunct to escitalopram had a reduction in HAM-D mean scores compared to placebo (Halaris et al., 2015).
Three RCTs have investigated celecoxib in the treatment of moderate to severe mania (Arabzadeh et al., 2015; Kargar et al., 2015; Mousavi et al., 2017). One of these studies investigated celecoxib as an add-on to sodium valproate and found a significant difference in the change in YMRS scores at the six-week endpoint compared to baseline in the two groups with an effect size of 1.16 for celecoxib (Arabzadeh et al., 2015). Another study investigated celecoxib as an adjunct to electroconvulsive therapy but did not find that the addition of celecoxib had any significant effect on treatment response (Kargar et al., 2015). More recently Mousavi and colleagues (2017) have completed a RCT of celecoxib 200 mg daily added to lithium and risperidone in 42 adolescent patients with bipolar mania. The authors report significantly greater improvement in YMRS scores in the celecoxib group compared with the placebo group from baseline YMRS score at week 8 (p=0.04). There were no serious adverse events reported. The results from this study could not be included in our quantitative synthesis as the study remains unpublished at the time of writing and authors did not respond to our requests to access for their data.
Overall current evidence indicates that celecoxib may be associated with antidepressant effects in patients with MDD without an increased risk of adverse effects. However there are insufficient trials to assess the efficacy of celecoxib in bipolar depression or mania; larger-scale RCTs are required to support this claim.
Cytokine inhibitors
Although previous studies have investigated the effect of cytokine inhibitors on depressive symptoms in patients with physical health comorbidities, we were able to identify only one study in which examined the effect of cytokine inhibitors in primary mood disorders (Raison et al., 2013). This was an RCT investigating the TNFα antagonist, infliximab, for use in treatment-resistant depression. The authors did not find a significant difference in change in depressive symptom scores between treatment groups, but an exploratory analyses focusing on patients with a baseline C-reactive protein (CRP) concentration greater than 5 mg/L revealed a treatment response (50% reduction in HAM-D score) of 62% in infliximab-treated patients versus 33% in placebo-treated patients (Raison et al., 2013). Conversely the authors found that in patients with CRP<5mg/L, treatment response was 41% for the infliximab group and 57% for the placebo group. Thus cytokine inhibitors may have antidepressant effects in patients with high baseline inflammatory markers, although further studies are required to confirm this.
NAC
We identified six studies, all by the same research group, investigating the use of NAC. The same dose of NAC (2 g) was used in all studies. We only included three of these studies (Berk et al., 2008; Magalhães et al., 2011b, 2013) in our quantitative analysis, as others either did not report change in symptoms scores or symptom severity (Dean et al., 2012; Waterdrinker et al., 2015) or because there was incomplete reporting of results (Berk et al., 2012, 2014). The three studies included all reported separate findings of the same RCT (Berk et al., 2008): two investigated change in depressive symptoms as their primary outcome measure (Berk et al., 2008; Magalhães et al., 2011a) and one study investigated the effect on manic symptoms (Magalhães et al., 2013). All three studies supported the use of NAC as an adjunctive treatment for both depressive and manic symptoms without any serious adverse effects reported. Study size varied from 15–75 participants and study duration was 24 weeks.
A study excluded from the current meta-analysis examined the use of NAC as a maintenance treatment for bipolar disorder (Berk et al., 2012). This study (n=149) was an eight-week open-label trial of adjunctive NAC prior to a 24-week RCT. Results showed a decrease in symptoms in the open-label phase, but no significant change in outcome measures were found between the NAC and placebo groups at the end of the RCT phase, which the authors argue could be due to a ceiling effect, with participants responding to eight weeks’ treatment with NAC In the open-label phase.
The same group has also investigated the use of NAC as an adjunctive treatment for 12 weeks in 252 participants with unipolar depression (Berk et al., 2014). The authors did not find any significant difference in MADRS scores between groups at the end of the treatment phase. We were unable to include either of these studies in our analysis as the authors did not report outcomes that met our inclusion criteria, and did not respond to requests for access to full results.
In summary, the evidence from one RCT and its subsequent secondary analyses (Berk et al., 2008; Magalhães et al., 2011b, 2013) may support the hypothesis that adjunctive NAC may ameliorate depressive and possibly manic symptoms in patients with bipolar disorder. However a more recent study with a larger sample size did not find any significant improvement in symptoms following treatment with NAC in MDD (Berk et al., 2014). Further well-designed, larger controlled trials are required before NAC use can be recommended for routine clinical use in both bipolar disorder and MDD.
Aspirin
Only one RCT of aspirin use as an adjunct to lithium in the treatment of bipolar disorder was identified (Saroukhani et al., 2013). The primary outcomes in this study were symptoms of sexual (erectile) dysfunction in euthymic patients with bipolar disorder. By the end of the six-week study period, there was no significant difference in either depressive or manic symptoms scores between the treatment and control groups. Although further studies are underway investigating the use of aspirin in mood disorders (Savitz et al., 2012), at present there is insufficient evidence to support its use, although there is evidence to support the safety and tolerability of concomitant aspirin and lithium use (Saroukhani et al., 2013).
Minocycline
We were able to find only one RCT of minocycline for the treatment of depressive symptoms (Emadi-Kouchak et al., 2016). This was a six-week study of 46 patients diagnosed with HIV+, presenting with mild to moderate depressive symptoms (HAMD score≤18). Participants received minocycline monotherapy or placebo without any other pharmacological or psychological treatment for MDD. The authors found significantly greater improvements in HAMD scores in patients in the minocycline group compared to those in the placebo group. There were also more partial responders in the minocycline group compared to the placebo group. There was only one participant in the study who made a full response (≥50% reduction in HAMD score), and they were in the minocycline group. The authors did not find any significant difference in the frequency of adverse effects between groups. The only other study investigating the use of minocycline for the treatment of mood disorders that was identified is an open label study of patients with psychotic unipolar depression (Miyaoka et al., 2012). The results indicate that minocycline augmentation of antidepressant treatment was effective in improving depressive symptoms and was well tolerated. Despite a lack of further studies of minocycline for the treatment of mood disorders, our search indicated multiple studies currently underway investigating the use of minocycline for both MDD and bipolar disorder (Dean et al., 2014; Husain et al., 2015, 2016; Savitz et al., 2012). The results of these trials will add to the current evidence base for the efficacy and safety of minocycline in the treatment of mood disorder.
Adverse effects
Adverse effects from each RCT included are summarised in Table 3. Conventional NSAIDs are known to be associated with gastrointestinal (GI) side effects such as upper GI bleeding (Wolfe et al., 1999). Selective COX-2 inhibitors such as celecoxib are thought to be associated with cardiovascular adverse events such as atherosclerosis and myocardial infarction due to possible increased pro-thrombotic activity (Mukherjee et al., 2001). The tetracycline antibiotic minocycline has been associated with GI side effects, dizziness, skin pigmentation and lupus (Garner et al., 2012). None of the trials reported a serious adverse event and no incident of GI bleed or cardiovascular side effect was reported.
Adverse effects (AEs) of anti-inflammatory agents.
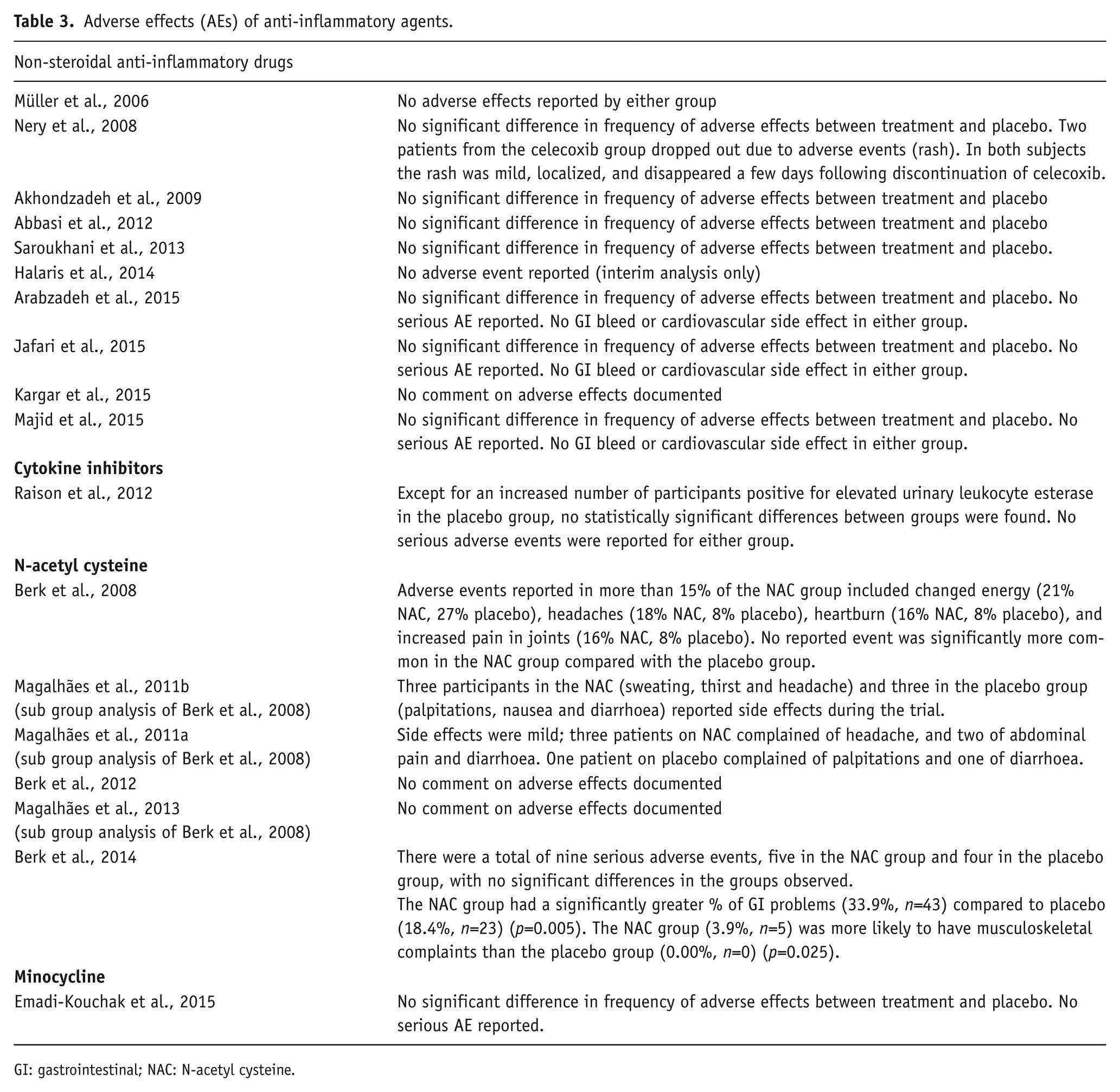
GI: gastrointestinal; NAC: N-acetyl cysteine.
Trials of cytokine inhibitors did not report a significant association with increased likelihood of infections.
An RCT of NAC in depression reported that the treatment group had a significantly greater incidence of GI adverse effects compared to placebo (p=0.005). The NAC group was also more likely to experience musculoskeletal adverse effects than the placebo group (p=0.025) (Berk et al., 2014). An earlier trial of NAC in bipolar disorders by the same authors did not show any significant difference in the frequency of adverse effects between treatment and placebo groups (Berk et al., 2008).
Discussion
This meta-analysis suggests that anti-inflammatory treatments may have a beneficial effect on both depressive and manic symptoms. When assessing the primary outcome measure of post-treatment symptom severity, the quantitative analysis of six anti-inflammatory RCTs (n=214 participants with either MDD or bipolar depression) demonstrated a significant moderate antidepressant effect (SMD=−0.71). This is comparable with effect sizes reported in clinical trials of antidepressants, where an effect size of 0.40 or higher is considered a clinically significant response criterion (Faries et al., 2000). A sub-analysis of three trials in patients with bipolar depression showed that anti-inflammatory agents may have antidepressant actions in this group, although the overall effect (SMD −0.42) was not statistically significant and included substantial heterogeneity. With regards to the anti-manic effects of anti-inflammatory agents, there were only three studies of 96 patients evaluated and thus the pooled effect size of −0.72 for these studies must be treated with caution, making it impossible to base any clinical recommendations on this evidence.
Meta-regression analyses of included trials indicated that study quality, baseline symptom severity and duration of treatment with antidepressants did not influence the effect of anti-inflammatory treatments on the primary outcome measure of post-treatment symptom severity scores. However all three of these variables showed a significant linear relationship for the effect of anti-inflammatory agents on the secondary outcome of change in depressive symptom scores; there was a negative correlation between study quality and anti-inflammatory treatment effect, whereas baseline symptom severity and duration of depressive symptoms were positively correlated to a treatment effect.
Limitations
The majority of studies included in our review had small sample sizes and had only small to medium effect sizes with high heterogeneity. For the meta-analysis we were unable to pool SMDs from all studies in unipolar and bipolar depression because not all of them used the same symptom rating scales and not all of them reported post-treatment symptom severity as an outcome measure; instead they provided data on change in symptom scores. The Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green, 2011) suggests only pooling change in symptoms scores with post-symptom severity measures into one mean difference analysis if the same rating scale is used in all studies. Therefore the pooled SMDs reported in this meta-analysis may not be indicative of the true effect size of anti-inflammatory agents in the treatment of bipolar and unipolar depression.
Although we found no evidence of publication bias, this was not assessed statistically due to small numbers and sizes of studies included. Furthermore, treatment durations tended to be short, mostly ranging from 6–12 weeks, meaning that we were unable to inspect the long-term adverse effects, tolerability and efficacy of anti-inflammatory treatment. Although we made efforts to summarise adverse effects of the anti-inflammatory interventions, not all studies reported these, limiting a full evaluation of the safety and tolerability of these interventions. It is also important to note that the antidepressant effect of the interventions may be mediated via their effects on somatic comorbidities, although we have only included three studies in which patients recruited were diagnosed with somatic comorbidity. Finally, the generalizability of nine studies’ findings included in this systematic review is potentially questionable since these trials were all conducted in Iran and trials in high-income countries may yield different results.
Implications and direction for future research
The current evidence for the use of anti-inflammatories as treatments for mood disorders remains inconsistent. Current studies are limited by small sample sizes, short durations, differing baseline symptomatology and poorly defined illness durations, which makes it impossible to provide recommendations on the routine clinical use of these agents in the treatment of mood disorders. The most investigated anti-inflammatory treatment is celecoxib, with many studies reporting antidepressant effects when used as an adjunct or as monotherapy (Abbasi et al., 2012; Akhondzadeh et al., 2009; Jafari et al., 2015; Majid et al., 2015; Müller et al., 2006). There are also indications that celecoxib may have anti-manic properties, although this assumption is based on a small study not evaluating long-term effects on response and remission (Arabzadeh et al., 2015). Although it has been reported that NSAIDs carry an increased risk of gastrointestinal (Wolfe et al., 1999) and cardiovascular (Mukherjee et al., 2001) adverse effects, this has not been supported by our analysis. However, it is important to note that three studies did not provide any comment on adverse effects (Berk et al., 2012; Kargar et al., 2015; Magalhães et al., 2013). Furthermore, given the short study period for many of the trials, it is possible that adverse effects were not identified in the study timeframe. Given these important caveats we would suggest that it is important to proceed cautiously before implementing celecoxib in routine clinical practice, and the potential therapeutic benefits in mood disorder must be balanced against the risk of adverse effects. More large-scale clinical trials of celecoxib for patients with depression (both unipolar and bipolar) and mania are warranted. Such trials will assess longer-term safety and tolerability as well as effects on response and remission rates in both MDD and bipolar disorder.
Given the small number of studies that have investigated cytokine inhibitors, NAC and minocycline for the treatment of mood disorders, we would encourage further high-quality controlled clinical trials to contribute to the current body of evidence. More studies are required, particularly investigating whether these anti-inflammatory drugs are effective in the treatment of mania.
Numerous mechanisms have been proposed to explain the association between inflammation and mood disorders, ranging from disturbed neurotransmission, to disturbances in the biological mediators of stress (i.e. cortisol levels) and the release of neurotoxic metabolites. It is possible that anti-inflammatory agents act on several of these mechanisms to produce an antidepressant and possibly an antimanic effect. Biological mediators of stress (e.g. glucocorticoids) and peripheral inflammation have been found to activate neuroinflammatory processes, which could lead to the onset of mood symptoms (Miller and Raison, 2016). In particular, the kynurenine pathway is an inflammatory pathway that is believed to be involved in mood disorders, and has shown to be modulated by anti-inflammatory agents. Pro-inflammatory cytokines can activate the enzyme indoleamine 2,3-dioxygenase (IDO). Increased IDO activity decreases synthesis of serotonin from tryptophan, leading to the production of pro-depressant and neurotoxic metabolites (Grosse et al., 2016). Anti-inflammatories have been shown to block pro-inflammatory cytokines, which activate IDO.
We would suggest that future treatment trials should also include the measurement of biomarkers in order to identify whether the clinical benefits of anti-inflammatory medications occur alongside a change in inflammatory activity, or in only a biological sub-group of patients experiencing a mood disorder. Studies have already found that patients with both depression and bipolar disorder may have abnormal levels of circulating inflammatory markers (Dowlati et al., 2010; Goldstein et al., 2009; Howren et al., 2009). A recent meta-analysis has found that in MDD, these levels may normalise with treatment and the authors identified TNFα as a potential marker for treatment-resistant depression (Strawbridge et al., 2015). However, plasma cytokines are strongly affected by environmental factors (e.g. age, gender, exercise, obesity, insulin resistance, smoking), and by the heterogeneity of mood disorder itself, and so exhibit high inter-individual variance. Instead it has been suggested that measuring the pro-inflammatory state of monocytes, the main cytokine producers, via gene expression may be a more sensitive way to detect inflammation (Carvalho et al., 2014; Grosse et al., 2015). Future RCTs of anti-inflammatory medications should attempt to incorporate these putative biomarkers in order to determine whether the mechanism of any antidepressant action is due to the inhibition of inflammatory processes. The results of such studies may provide clinicians with clear guidelines on when to implement anti-inflammatory treatment for patients with treatment-resistant symptoms.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MIH has been awarded research grants from the Stanley Medical Research Institute (USA). PRAS has received support for research, expenses to attend conferences and fees for lecturing and consultancy work (including attending an advisory board) from life sciences companies including Corcept Therapeutics, Indivior and Liva Nova. PRAS is a consultant psychiatrist within a tertiary level specialist service and a specialist consultant advisor in mood disorders to the UK Civil Aviation Authority. AHY has been commissioned to give lectures and is on advisory boards for all major pharmaceutical companies with drugs used in affective and related disorders. AHY is the lead Investigator for Embolden Study (AZ), BCI Neuroplasticity study and Aripiprazole Mania Study. AHY has been involved in investigator-initiated studies of AZ, Eli Lilly, Lundbeck and Wyeth. AHY has been awarded research grants from: National Institute of Mental Health (USA); Canadian Institute of Health Research (Canada); National Association for Research on Schizophrenia And Depression (USA); Stanley Medical Research Institute (USA); Medical Research Council (UK); Wellcome Trust (UK); Royal College of Physicians (Edinburgh, UK); British Medical Association (UK); University of British Columbia-Vancouver General Hospital Foundation (Canada); Western Economic Diversification Canada (Canada); CCS Depression Research Fund (Canada); Michael Smith Foundation for Health Research (Canada); National Institute for Health Research (UK).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study presents independent research part-funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the National Health Service (NHS), the NIHR or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.