
Abstract
The objective of this meta-analysis is to assess the efficacy and safety of partial and complete dopamine agonists in the treatment of acute mood disorder episodes. Randomized, double-blind and placebo-controlled trials of dopamine agonists in the treatment of acute mood disorder episodes were identified in the MEDLINE and PsycINFO databases and included in the meta-analysis. In monotherapy of mania, improved remission rates were found for cariprazine (odds ratio (OR): 2.08, P < 0.01) and for high-dose aripiprazole (OR: 3.00; P = 0.05), but not for low-dose aripiprazole. In bipolar depression, no improvement of remission and response rates was found for aripiprazole in monotherapy, whereas improved response rate (OR: 10.27, P < 0.01) was found for pramipexole only as an add-on to another mood stabilizer. In major depressive disorder, relatively similar improvements of remission rates were found for high-dose (OR: 1.96, p < 0.01) and low-dose aripiprazole (OR: 1.68, P = 0.01), as well as brexpiprazole (OR: 1.52, P = 0.05) as an add-on to antidepressant medication. Our meta-analysis shows that partial dopamine agonists at high doses are effective in treating acute mania. In major depressive disorder, which is resistant to classical antidepressants, low doses of partial dopamine agonists as adjunct therapy may represent a relatively safe and effective alternative.
Introduction
Mood disorders are frequent in the general population with an overall lifetime prevalence of 20.8% (Kessler et al., 2005). Specific lifetime prevalences are 16.6% for major depressive disorder (MDD) and 3.9% for bipolar disorder (Kessler et al., 2005). Mood disorders are often resistant to current treatments. A population of patients in routine primary care and psychiatric settings showed a response rate of 47% following treatment with a selective serotonin reuptake inhibitor; remission rates ranged between 28 and 33%. (Trivedi et al., 2006). To improve remission rates, it is important to explore alternative therapeutic strategies.
Some neurobiologists have hypothesized that dopamine may play a role in mood disorders (Ashok et al., 2017). Decreased dopamine levels have been observed in MDD (Belmaker and Wald, 1977) and increased levels during manic episodes (Gessa et al., 1995; Markou and Koob, 1991; Silverstone, 1985). Mesolimbic dopamine neurons that project into the nucleus accumbens have been linked to reward and motivation. Not only do they play a role in addictive disorders, they may also be implicated in mood disorder pathophysiology (Brown and Gershon, 1993; Fibiger, 1995; Kapur and Mann, 1992; Willner, 1997). In an animal model of stress, D3 receptor gene expression significantly increased following 21 days of treatment with imipraminic antidepressants. D3 receptor binding also increased after 42 days of amitriptyline and fluoxetine administration. (Lammers et al., 2000). Functional imaging studies in depressed patients have shown increased D2 receptor binding in the striatum (D’Haenen et al. 1994; Shah et al. 1997), leading to the hypothesis that dopamine function may be reduced in these patients.
Molecules such as pramipexole have a high in vitro affinity for D2 and D3 receptors (Mierau et al., 1995; Schneider and Mierau, 1987). Initially used in the treatment of Parkinson’s Disease, pramipexole has also been studied in the treatment of mood disorders (MDD and bipolar depression), both in monotherapy (Corrigan et al., 2000; Franco-Chaves et al., 2013) and as adjunctive therapy (Cusin et al., 2013; Franco-Chaves et al., 2013; Goldberg et al., 2004; Zarate et al., 2004).
Partial dopamine agonists including aripiprazole (Berman et al., 2009, 2007; El Mallakh et al., 2010; Fava et al., 2012; Findling et al., 2009; Kamijima et al., 2013; Kanba et al., 2014; Keck et al., 2003, 2009; Lenze et al., 2015; Lin et al., 2011; Marcus et al., 2008; Quante et al., 2010; Sachs et al., 2006; Thase et al., 2008; Vieta et al., 2008; Young et al., 2009), and more recently brexpiprazole (Thase et al., 2015a, 2015b) as well as cariprazine (Calabrese et al., 2015; Durgam et al., 2016a, 2016b, 2015; Sachs et al., 2015) have also been used to treat various mood disorders. Pharmacodynamic studies have determined that each of these treatments possess different binding affinities for human receptors; (Citrome, 2015) all have high to very high binding affinities for D2 and D3 dopamine receptors.
The objective of this systematic review and meta-analysis was to assess the efficacy and the safety of partial and complete dopamine agonists in the treatment of acute episodes of mood disorder using available randomized, placebo-controlled double-blind studies. Clinical remission rates and response were used to determine efficacy.
Method
Data sources and study selection process
We searched the MEDLINE and PsycINFO databases until June 2016 inclusive, without limits on publication year. In order to obtain additional data, an email alert was created after June 2016 in MEDLINE with the same keywords to detect putative publications of interest. We used the following keywords: dopaminergic agonist or dopaminergic partial agonist or aripiprazole or cariprazine or brexpiprazole or pramipexole and MDD or bipolar disorder. Studies were included if (a) they were published in English in a peer-reviewed journal, (b) they were randomized, double-blind and placebo-controlled trials of a partial or complete dopamine agonist, and (c) they included patients with a diagnosis of MDD or bipolar depression or mixed/mania episode based on Diagnostic and Statistical Manual of Mental Disorders III, IV or V criteria. Studies that did not fulfill all three criteria were systematically excluded from analyses.
Data extraction
We extracted all response and remission rates for each of the included studies. Any unavailable data in the article was completed through correspondence with the study’s authors (see Acknowledgements) or using information found in www.clinicaltrials.gov. Other clinical variables such as mean age, sex, diagnosis, current episode duration and mean treatment dose were also extracted to better define clinical samples. To assess treatment tolerance, we extracted rates for common adverse effects such as weight gain, dropouts due to adverse effects and serious adverse effects. Data extraction was performed by one author (BR) and verified by another (CM).
Data analyses
Data analyses were performed using RevMan, version 5.3 (Copenhagen, Denmark; the Nordic Cochrane Centre, Cochrane Collaboration). Treatment efficacy was calculated using odds ratios (ORs) and weight gain using standardized mean differences (SMDs). All analyses were performed using a random effects model, which considers both between-study and within-study variability (DerSimonian and Laird, 1986). An effect size was considered significant when the 95% confidence interval (95% CI) excluded 1 and the P-value was ≤ 0.05 for ORs, and when the 95% CI excluded 0 and the P-value was ≤ 0.05 for SMD. To assess the influence of aripiprazole dose on efficacy, we performed analyses according to dose. In mixed/mania treatment, low dose was defined as ≤ 15 mg/day and high dose as >15 mg/day. In MDD, low dose was ≤ 5 mg/day and high dose > 5 mg/day. Few studies of cariprazine and brexpiprazole were available, so all studies were pooled regardless of dose. ORs and SMDs were calculated when at least two studies were available. Single studies were included for discussion. To assess tolerance, we pooled all included studies for each molecule then analyzed them according to dose when possible.
Study heterogeneity was estimated using the Q statistic and was considered significant when P < 0.10. When heterogeneity was significant, the I² index was used to estimate the variance due to heterogeneity rather than chance. I² values of 25, 50 and 75 were indicative of mild, moderate and high heterogeneity between trials, respectively.
Selection, performance, detection, attrition, reporting and other biases were investigated using the Cochrane Collaboration’s Tool for Assessing Risk of Bias (Higgins et al., 2011). Funnel plots were drawn when at least five individual studies contributed to an overall result, and their asymmetry analyzed to assess the possible influence of publication and location biases (Green and Higgins, 2006).
Results
Article identification process
The article selection process is shown in Figure 1 and Table S1. A total of 30 articles were included in this study. Of the studies, 12 included patients with mixed or mania episode (Calabrese et al., 2015; Durgam et al., 2015; El Mallakh et al., 2010; Findling et al., 2009; Kanba et al., 2014; Keck et al., 2003, 2009; Sachs et al., 2006; Smith et al., 1980; Vieta et al., 2008; Young et al., 2009), 5 included patients with bipolar depression (Durgam et al., 2016b; Goldberg et al., 2004; Quante et al., 2010; Thase et al., 2008; Zarate et al., 2004) and 13 included patients with MDD (Berman et al., 2009, 2007; Corrigan et al., 2000; Cusin et al., 2013; Durgam et al., 2016a; Fava et al., 2012; Franco-Chaves et al., 2013; Kamijima et al., 2013; Lenze et al., 2015; Lin et al., 2011; Marcus et al., 2008; Thase et al., 2015a, 2015b). The main characteristics of each included study and their primary results are described in Tables 1, 2 and 3. Study quality was assessed using the Cochrane Collaboration’s Tool for Assessing Risk of Bias (Higgins et al., 2011) (Table S2).
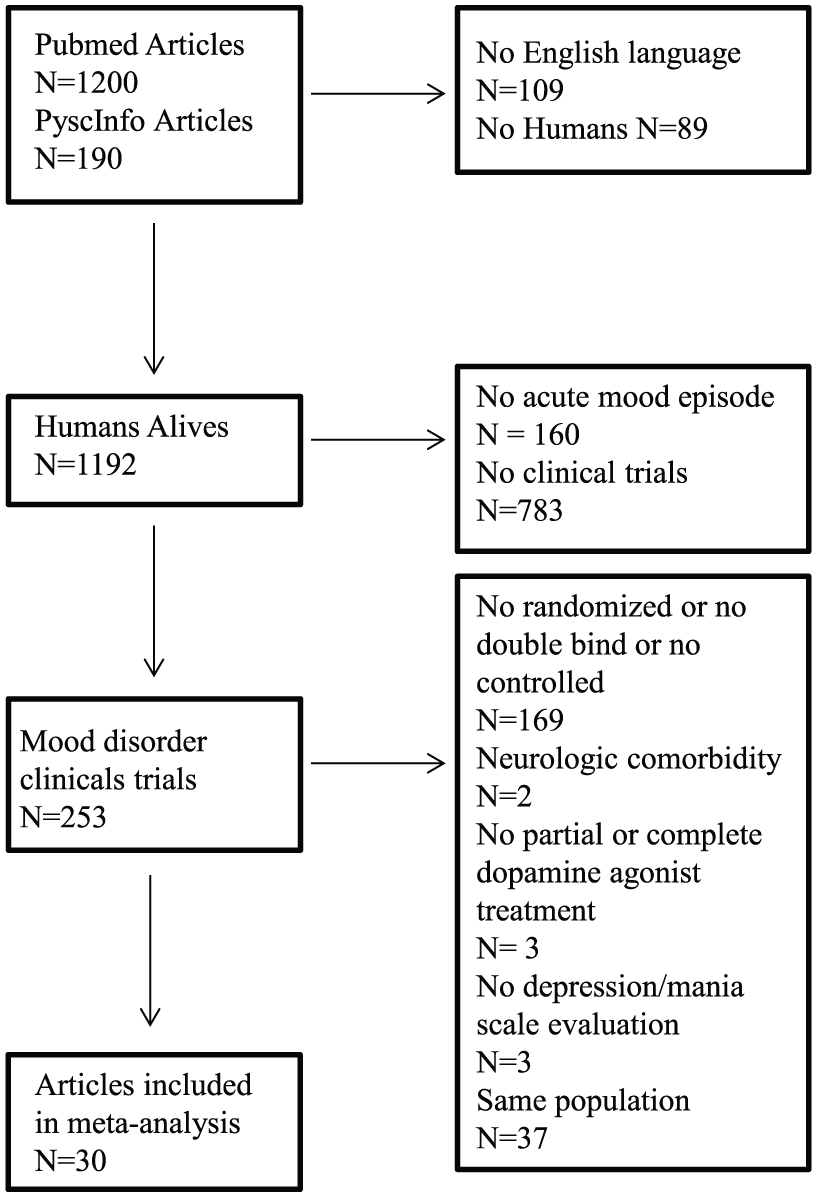
Flow diagram of randomized, double-blind and placebo-controlled trials.
Mixed/mania studies.
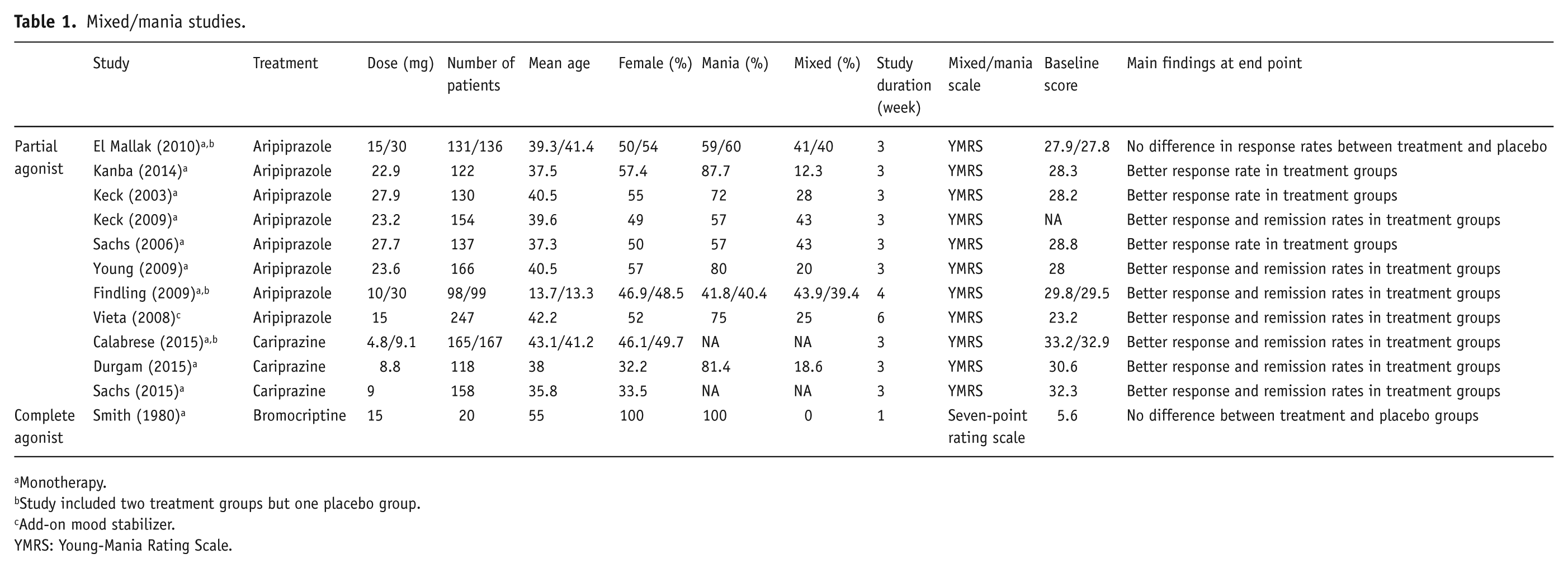
Monotherapy.
Study included two treatment groups but one placebo group.
Add-on mood stabilizer.
YMRS: Young-Mania Rating Scale.
Bipolar depression studies.
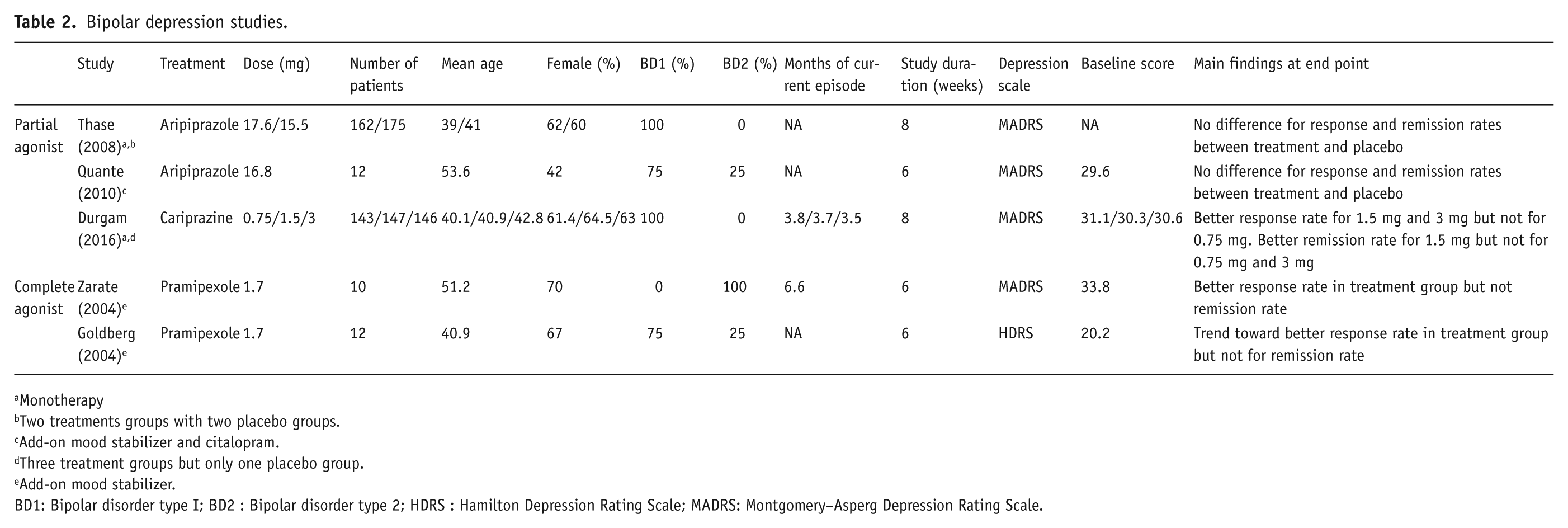
Monotherapy
Two treatments groups with two placebo groups.
Add-on mood stabilizer and citalopram.
Three treatment groups but only one placebo group.
Add-on mood stabilizer.
BD1: Bipolar disorder type I; BD2 : Bipolar disorder type 2; HDRS : Hamilton Depression Rating Scale; MADRS: Montgomery–Asperg Depression Rating Scale.
MDD studies.
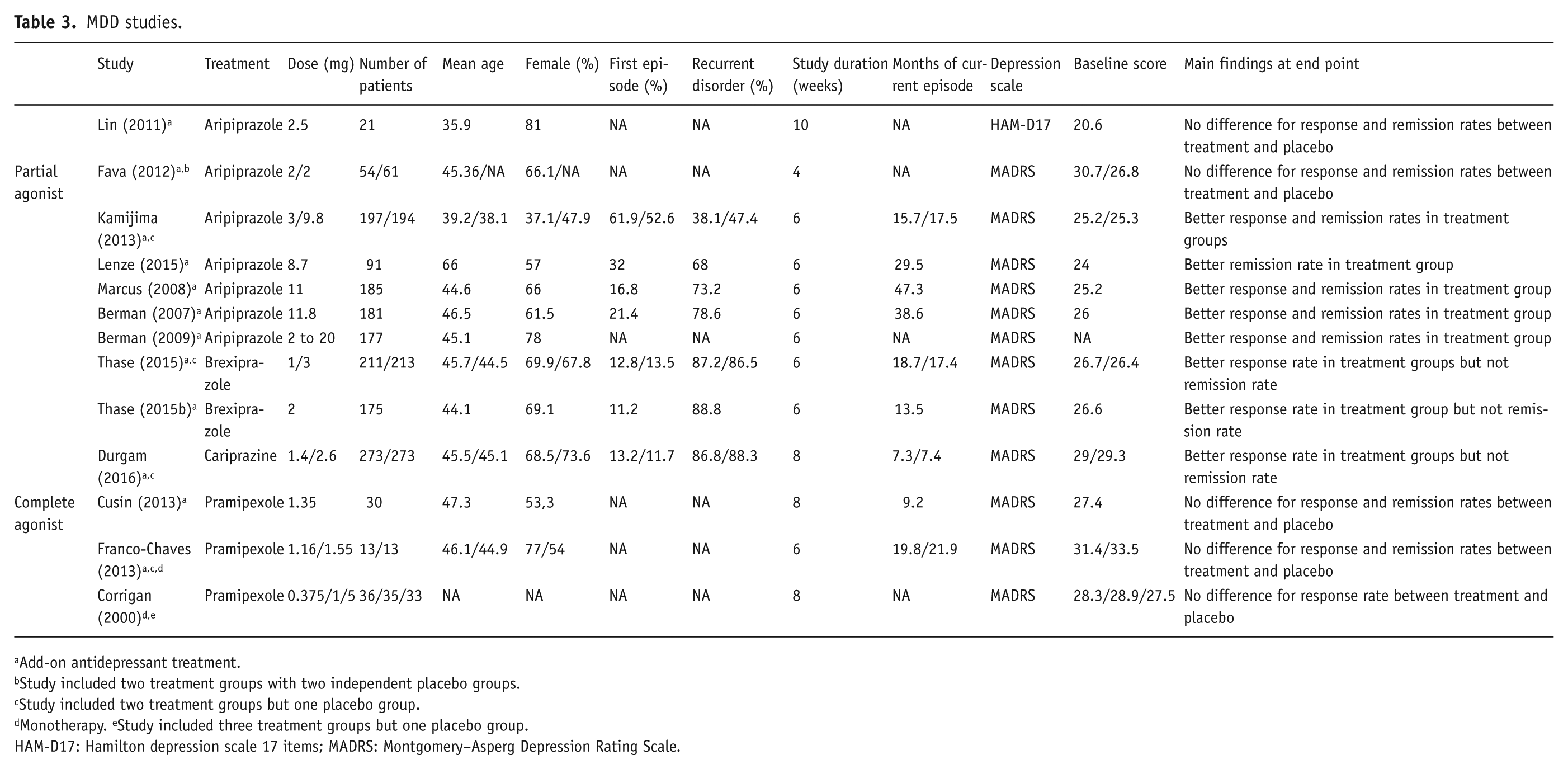
Add-on antidepressant treatment.
Study included two treatment groups with two independent placebo groups.
Study included two treatment groups but one placebo group.
Monotherapy. eStudy included three treatment groups but one placebo group.
HAM-D17: Hamilton depression scale 17 items; MADRS: Montgomery–Asperg Depression Rating Scale.
Efficacy
Mania/mixed episode
Partial dopamine agonists
Aripiprazole
Clinical response for low-dose aripiprazole monotherapy showed a pooled OR of 1.58 (95% CI: 0.8–3.13) (Table 4 and Figure 2(a)). No clinical remission data were available for analysis. One study (Vieta et al., 2008) investigated aripiprazole add-on to valproate or lithium, which showed greater response and remission rates at 6 weeks in thearipiprazole group versus placebo.
Summary of main findings.
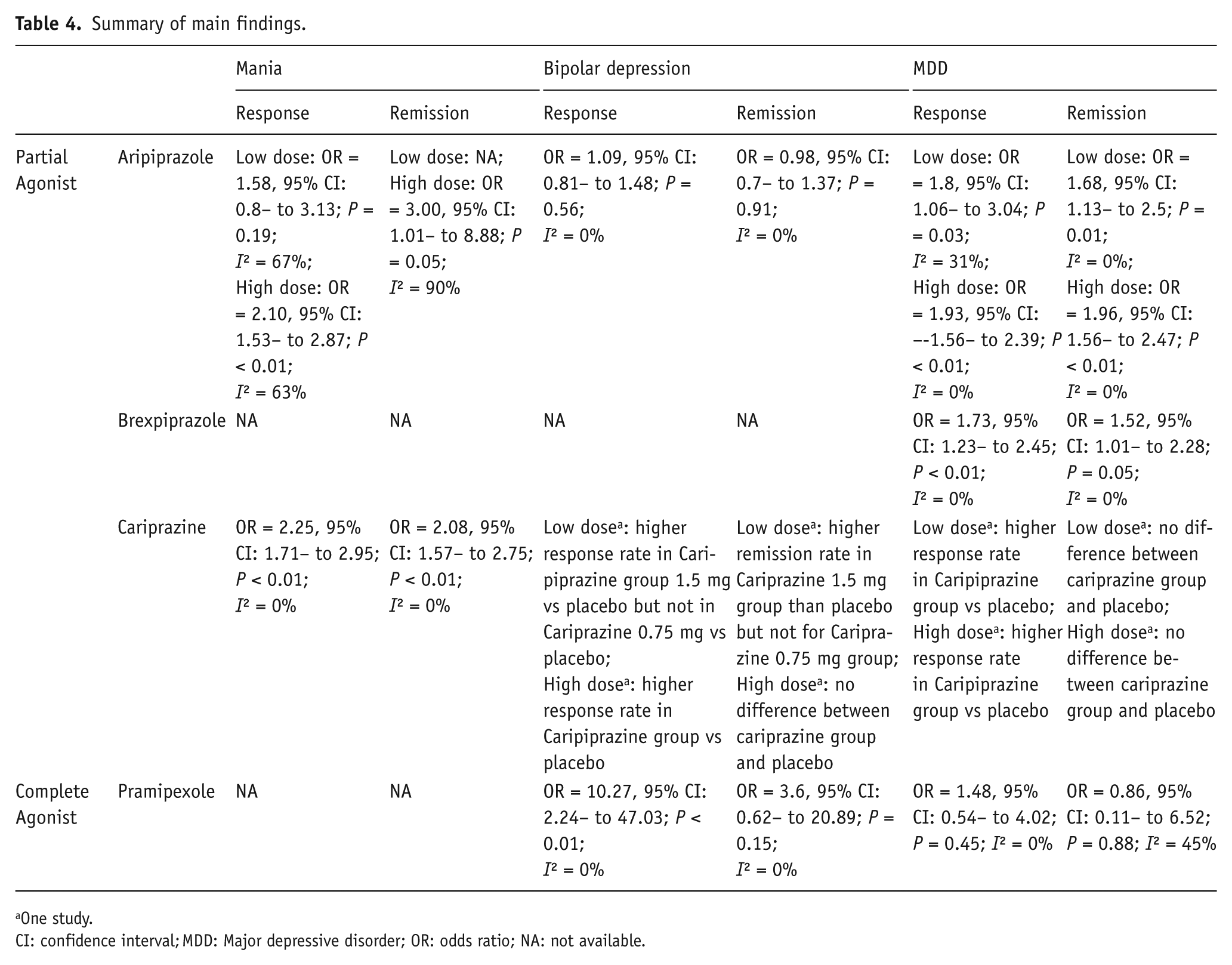
One study.
CI: confidence interval; MDD: Major depressive disorder; OR: odds ratio; NA: not available.
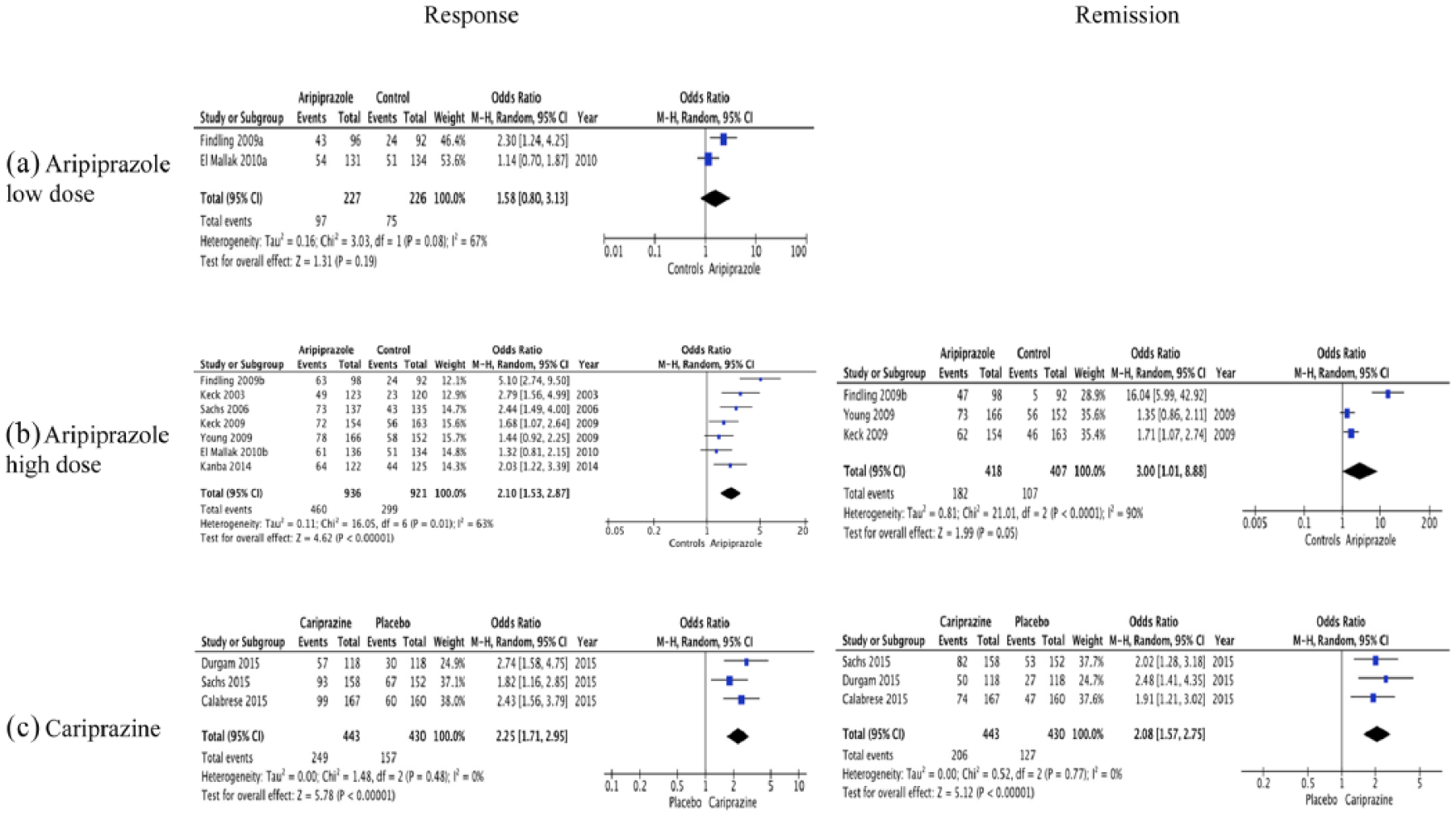
Forest plot for Mania and mixed episodes.
Clinical remission for high-dose aripiprazole monotherapy showed a pooled OR of 3.00 (95% CI: 1.01–8.88), and for clinical response a pooled OR of 2.10 (95% CI: 1.53–2.87), thus indicating a significant difference in outcome favoring aripiprazole (Table 4 and Figure 2(b)). On excluding the only study in children (Findling et al., 2009), heterogeneity was not significant for clinical remission (I² = 0%, P = 0.47) or clinical response (I² = 23%, P = 0.26), and no change in treatment efficacy was observed (Figures S2 and S3).
Cariprazine
Clinical remission for cariprazine monotherapy showed a pooled OR of 2.08 (95% CI: 1.57–2.75), and for clinical response a pooled OR of 2.25 (95% CI: 1.71–2.95) (Table 4 and Figure 2(c)). This indicates a significant difference in outcome favouring cariprazine.
Complete dopamine agonists
Bromocriptine
We found only one study using bromocriptine in the treatment of mania in bipolar disorder (Smith et al., 1980), which showed no efficacy.
Bipolar depression
Partial dopamine agonists
Aripiprazole
Clinical remission for high-dose aripiprazole monotherapy showed a pooled OR of 0.98 (95% CI 0.7–1.37), and for clinical response a pooled OR of 1.09 (95% CI 0.81–1.48) (Table 4 and Figure 3(a)), thus indicating no significant difference between aripiprazole and placebo. Only one study investigated add-on aripiprazole in bipolar depression (Quante et al., 2010) with no significant differences in remission and response rates versus placebo.
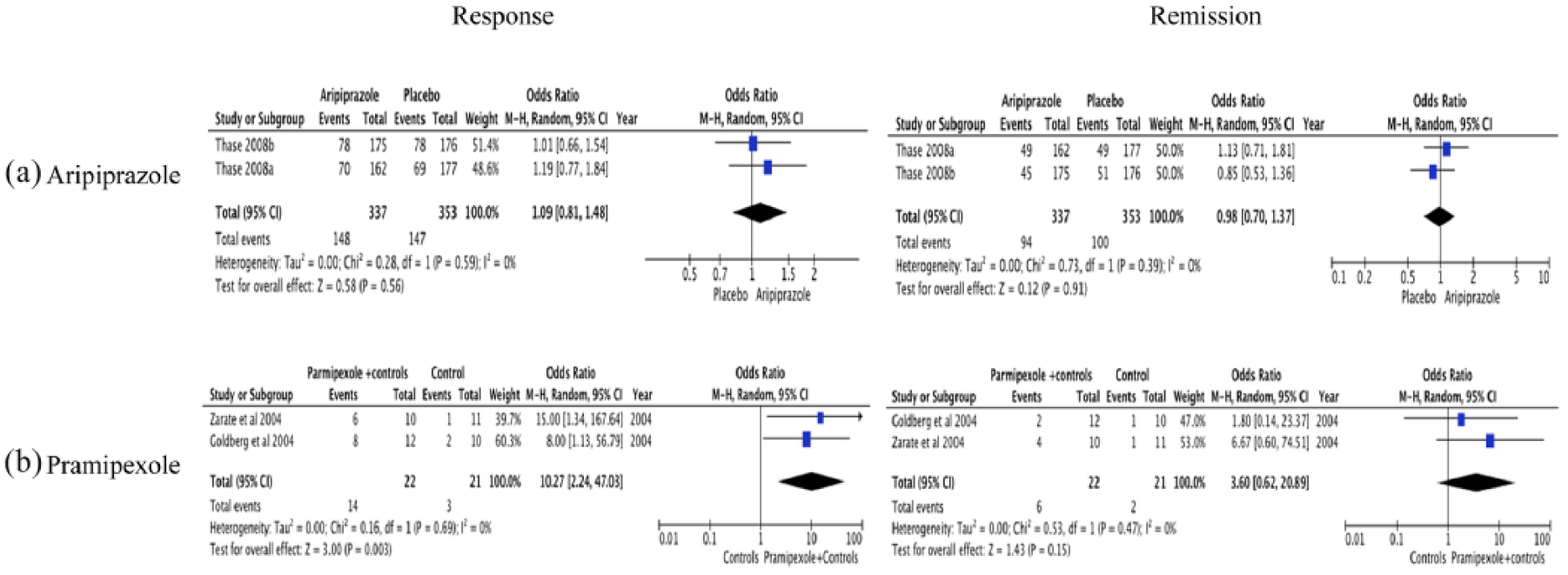
Forest plot for bipolar depression.
Cariprazine
One study investigated three cariprazine doses (0.75 mg/day; 1.5 mg/day and 3.0 mg/day) in treating bipolar depression (Durgam et al., 2016b). A significant difference between cariprazine and placebo was found only for the 1.5 mg/day dose in terms of clinical response and remission. There was no significant difference between the other two groups.
Complete dopamine agonists
Pramipexole
Clinical remission for pramipexole add-on to a mood stabilizer showed a pooled OR of 3.6 (95% CI 0.62–20.89), and for clinical response a pooled OR of 10.27 (95% CI 2.24–47.03) (Table 4 and Figure 3(b)). This indicates a significantly more favorable outcome with pramipexole in terms of clinical response but not clinical remission.
Major depressive disorder
Partial dopamine agonists
Aripiprazole
Clinical remission for low-dose aripiprazole add-on to antidepressant treatment showed a pooled OR of 1.68 (95% CI 1.13–2.5), and for clinical response a pooled OR of 1.8 (95% CI 1.06–3.04) (Table 4 and Figure 4(a)), thus indicating a significant difference favoring low-dose aripiprazole.
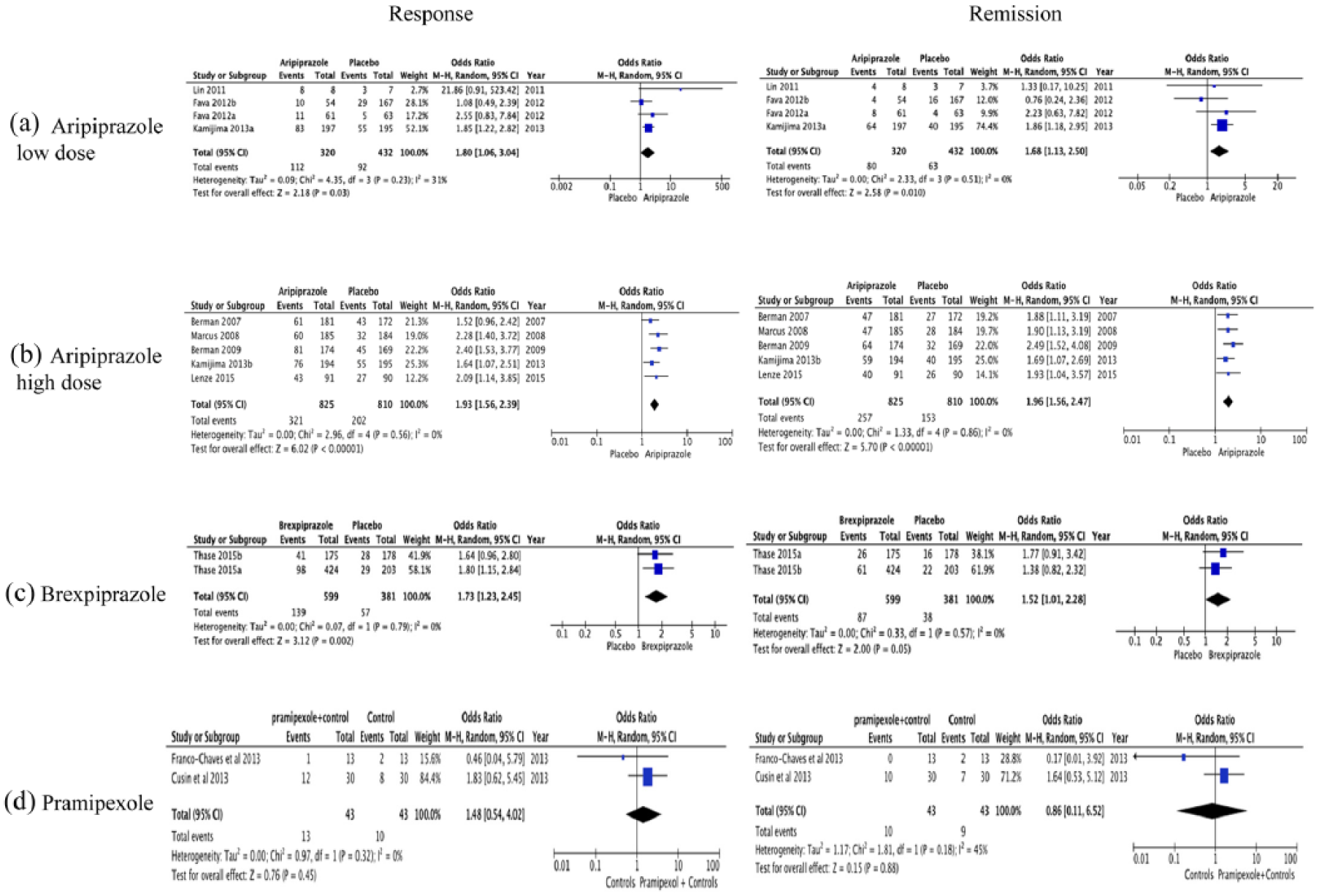
Forest plot for major depressive disorder.
Clinical remission for high dose aripiprazole add-on to antidepressant treatment showed a pooled OR of 1.96 (95% CI 1.56–2.47), and for clinical response a pooled OR of 1.93 (95% CI 1.56–2.39) (Table 4 and Figure 4(b)). This indicates outcomes in favour of high-dose aripiprazole.
Brexpiprazole
Clinical remission for brexpiprazole add-on to antidepressant treatment showed a pooled OR of 1.52 (95% CI 1.01–2.28), and for clinical response a pooled OR of 1.73 (95% CI 1.23-2.45) (Table 4 and Figure 4(c)), thus indicating a significantly more favorable outcome with brexpiprazole versus placebo.
Cariprazine
In one study examining cariprazine as an add-on to antidepressant treatment, Durgam et al. (2016a) observed significantly better response rates at each dose (1–2 mg/day and 2–4.5 mg/day) versus placebo. No significant differences in remission rates were observed.
Complete dopamine agonists
Pramipexole
Clinical remission for pramipexole as an add-on to antidepressant showed a pooled OR of 0.86 (95% CI 0.11–6.52), and for clinical response a pooled OR of 1.48 (95% CI 0.54–4.02) (Table 4 and Figure 4(d)), thus indicating no significant difference between pramipexole add-on antidepressant and placebo.
In monotherapy in MDD, pooled OR was 0.95 (n = 2 studies, 95% CI 0.28–3.27, P = 0.94, test for heterogeneity: χ² = 1.56, I² = 36%, P = 0.21) for clinical response, indicating no significant difference between pramipexole and placebo. Corrigan et al. (2000) investigated other doses (0.375 mg and 5 mg). No significant differences were observed in 8-week response rates, regardless of the dose. Franco-Chaves et al. (2013) found no significant difference in 6-week remission rates between pramipexole monotherapy and escitalopram.
Safety and tolerance
Partial dopamine agonist
Aripiprazole
Significantly more patients experienced at least one adverse effect in the aripiprazole group both < 5 mg/day (OR = 1.4, 95% CI 1.04–1.89) and 5–15 mg/day (OR = 2.12, 95% CI 1.69–2.65) versus the placebo group. Significantly more patients receiving aripiprazole 5–15 mg/day (OR = 2.21, 95% CI 1.43–3.41) withdrew from trials due to adverse effects versus placebo. No significant differences were observed at < 5 mg/day or ≥ 15 mg. No significant differences were observed in terms of serious side effects for patients receiving aripiprazole 5–15 mg/day (OR = 1.05, 95% CI 0.61–1.82), 15–25 mg/day (OR = 1.3, 95% CI 0.63–2.70) and > 25 mg/day (OR = 0.92, 95% CI 0.54–1.59) versus placebo. Details concerning side effects are listed in Table S3.
Cariprazine
Significantly more patients had at least one adverse effect in the cariprazine versus placebo group at < 2.5 mg/day (OR = 1.42, 95% CI 1.09–1.85), at 2.5–5 mg/day (OR = 2.07, 95% CI 1.48–2.91) and at > 5 mg/day (OR = 2.02, 95% CI 1.48–2.75). No significant differences were observed in terms of withdrawal due to side effects at < 2.5 mg/day (OR = 1.3, 95% CI 0.47–3.64), at 2.5–5 mg/day (OR = 2.27, 95% CI 0.85–6.08) and at > 5 mg/day (OR = 1.62, 95% CI 0.80–3.27) versus placebo. No significant differences were observed in terms of serious side effects at < 2.5 mg/day (OR = 0.3, 95% CI 0.08–1.13), at 2.5 to 5 mg/day (OR = 1.2, 95% CI 0.37–3.86) and at > 5 mg/day (OR = 0.87, 95% CI 0.31–2.47) versus placebo. Details concerning side effects are listed in Table S4.
Brexpiprazole
Significantly more patients had at least one adverse effect in the brexpiprazole versus placebo group (OR = 1.65, 95% CI 1.28–2.12). No significant differences were observed in terms of withdrawal due to side effects (OR = 3.32, 95% CI 0.5–22.07) or to serious adverse effects (OR = 1.32, 95% CI 0.25–6.87) versus placebo. Details concerning side effects are listed in Table S5.
Complete dopamine agonist
Pramipexole
No significant differences in terms of withdrawal due to adverse effects were observed between pramipexole versus placebo (OR = 1.69, 95% CI 0.61–4.66). Details concerning side effects are listed in Table S6.
Discussion
In routine primary and psychiatric care settings, approximately one in two patients has an incomplete response to available serotoninergic antidepressant treatments and less than one in three achieve clinical remission. (Trivedi et al., 2006) To improve clinical outcomes, it is important to explore other therapeutic strategies. One possibility is the use of partial or complete dopaminergic agonists as a second line or add-on treatment. Using an exhaustive review and meta-analysis of the current available literature, we found that certain dopamine agonists, both partial and complete, may be useful in treating mood disorders. Specifically, in mania or mixed episodes, high-dose aripiprazole monotherapy (> 15 mg/day), but not low-dose aripiprazole or cariprazine, improved remission and response rates. In bipolar depression, aripiprazole does not seem to improve remission or response rates in monotherapy or as an add-on to another mood stabilizer. Add-on pramipexole to mood stabilizer improved response but not remission rates. In MDD, both low- and high-dose aripiprazole, as well as brexpiprazole add-ons to antidepressant treatment, improved response and remission rates. Pramipexole as an add-on antidepressant treatment was not associated with improved response or remission rates. The main findings from our study are summarized in Table 4.
One of the most striking results from this meta-analysis is that high-dose aripiprazole improved clinical remission and response in mania, which was contrary to that for low-dose aripiprazole. This distinction between high- and low-dose aripiprazole may also explain the lesser efficacy of aripiprazole compared to other antipsychotics, such as risperidone or olanzapine, found in a meta-analysis by Yildiz et al. (2011). Other studies have shown that aripiprazole has an efficacy comparable to molecules such as lithium and haloperidol in treating mania (Brown et al., 2013; Keck et al., 2009; Vieta et al., 2005; Young et al., 2009). One possible explanation is that contrary to higher doses, low-dose aripiprazole would be insufficient to counter increased dopamine levels observed in mania (Gessa et al., 1995; Markou and Koob, 1991; Silverstone, 1985).
This result may also have significant implications for prescriptions in clinical practice. Aripiprazole is currently a recommended first-line treatment for acute mania (Goodwin et al., 2016) with practitioners determining aripiprazole dose according to clinical response. Our results show that it may be important to initially use high aripiprazole doses in order to obtain a rapid response. Our results also show that, in the short term, this approach is not associated with a significant risk of adverse effects. Cariprazine may represent a potential alternative. Our analysis shows that it is effective in treating manic or mixed episodes. Results between high-dose aripiprazole and cariprazine in adult patients were fairly comparable, thus indicating that either could eventually be used in treating mania.
In bipolar depression, our results were more contrasted and inconclusive as to the benefits for prescribing partial or complete dopamine agonists. We found no efficacy when aripiprazole was used as an add-on to another mood stabilizer or in monotherapy. Pramipexole showed only a relative efficacy in bipolar depression with improved clinical response. However, we did not observe significant results in terms of remission. These results should be interpreted with caution due to the few studies that were included. A single clinical trial in bipolar depression showed that cariprazine also seemed to be effective, notably at 1.5 mg/day, similar to other antipsychotics such as quetiapine (Calabrese et al., 2005), olanzapine (Tohen et al., 2012) or lurasidone (Loebel et al., 2014). These results must be replicated in order for conclusions to be drawn and for them to be recommended in current clinical practice. One potential benefit for cariprazine treatment in comparison with quetiapine or olanzapine was the absence of weight gain at doses of < 2.5 mg/day.
Several studies have shown that the dopamine system may play a role in bipolar disorder (Ashok et al., 2017). D3 receptors in the nucleus accumbens have been found to be downregulated in stressed rats and administration of an antidepressant restored this expression (Lammers et al., 2000). Furthermore, these receptors are highly present in certain brain structures implicated in mood disorders (Zarate et al., 2004). Pramipexole (Piercey, 1998; Piercey et al., 1996) and cariprazine (Stahl, 2016) are both specific D3 dopamine agonists. Black et al. (2002) showed that pramipexole administration in primates causes decreased cerebral blood flow in regions such as the orbitofrontal cortex and the subgenual anterior cingulate. Studies such as these may help to explain the efficacy of dopamine agonists.
In MDD, we found similar results between low- and high-dose aripiprazole as an add-on to an antidepressant. This result is in contrast to a recent meta-analysis by Zhou et al. (2015), which showed no difference in efficacy between low-dose antipsychotics (i.e., aripiprazole or olanzapine associated with fluoxetine) versus placebo when using a depressive symptoms score. However, they did observe a significant difference in terms of response and remission rates. Our analysis included two additional studies (Lin; 2011; Lenze, 2015), which probably improved our statistical power, thus explaining our positive result.
As previously stated, we found similar efficacy between low- (≤ 5 mg/day) and high-dose aripiprazole (> 5 mg/day) as an add-on to antidepressant medication. One study by Han et al. (2015) has shown that add-on aripiprazole may also be more effective than switching to another antidepressant. Mischoulon et al. (2012) investigated the benefits of increasing aripiprazole from 2 to 5 mg/day in patients who had not responded at 2 mg/day. They found no significant difference in response rates between increasing aripiprazole to 5 mg/day and placebo (response rates were 12.8 and 7.9%, respectively) in patients who had not responded at 2 mg/day. In a previous study (Yoshimura et al., 2013), the efficacy of aripiprazole add-on to paroxetine was similar to add-on lithium or olanzapine with response rates of 40, 40 and 30% respectively. Our results indicate that the prescription of low-dose aripiprazole (≤ 5 mg/day) may be sufficient as an add-on treatment to antidepressants and may also limit the risk of adverse effects in long-term treatment.
We also found that brexpiprazole add-on to antidepressant treatment may represent an alternative in treating major depressive episodes in MDD. Response and remission rates were similar to those with aripiprazole.
Only one study investigating cariprazine showed improved response rates, but not remission rates. Pramipexole does not seem to be effective in monotherapy or as an add-on to antidepressant treatment in our analysis. This is an interesting result, since both of these molecules showed possible efficacy in treating bipolar depression. This difference may inform future research as to the separate pathophysiological implications of the D3 dopamine receptor in MDD and bipolar disorder.
Our analysis did not show any significant differences in terms of serious sides effects between treatment groups and placebo for all partial dopamine agonists. However, significantly greater numbers of patients in treatments groups (cariprazine, brexpiprazole and aripiprazole) experience at least one adverse effect. Upon discontinuing, no significant differences in adverse effects were found for brexpiprazole and cariprazine. Lao et al. (2016) showed a similar result in their meta-analysis of all known cariprazine trials. Significantly greater adverse effects were observed upon discontinuing aripiprazole at 5–15 mg/day doses but not at other doses. Contrary to other atypical antipsychotics, such as olanzapine and quetiapine, aripiprazole was not associated with significant weight gain. (Domecq et al., 2015). Mean observed weight gain was 0.54 kg at < 5 mg/day and 0.46 kg between 5–15mg/day. No significant differences were observed between aripiprazole and placebo in terms of weight gain prevalence (> 7%). Most studies were over a brief period (maximum 10 weeks), which may be insufficient to determine long-term outcomes for weight gain. Future research should prolong weight monitoring in patients treated with atypical antipsychotics (Cipriani et al., 2008)
The primary limitation of this analysis is the limited number of randomized controlled trials that prevented us from performing certain analyses. One example is the lack of data on the efficacy of different brexpiprazole doses. This was also the case for cariprazine in bipolar depression. It is also important to note that the majority of the MDD studies were in the context of resistant depressive episodes. Thus, these results cannot be generalized to the context of all major depressive episodes.
In conclusion, our meta-analysis shows that partial dopamine agonists at high doses may represent a safe and effective alternative in treating acute mania. In treating resistant MDD, low doses would seem to be just as effective as high doses as an add-on to antidepressant medication. At this time, the benefits of partial or complete dopamine agonists in the treatment of bipolar depression are not clear. Future research should better elucidate and differentiate the mechanisms of D3 dopamine receptors in bipolar and MDD. Molecules such as cariprazine and pramipexole may yet prove to be effective in these indications. Our results show that dopamine agonists have their place in treating mood disorders. Their doses must be carefully adapted according to the clinical diagnosis of the patient in order to optimize their efficacy and minimize the risk of adverse effects.
Supplemental Material
JOP760661_Supplementary_Material – Supplemental material for Meta-analysis and review of dopamine agonists in acute episodes of mood disorder: Efficacy and safety
Supplemental material, JOP760661_Supplementary_Material for Meta-analysis and review of dopamine agonists in acute episodes of mood disorder: Efficacy and safety by Bruno Romeo, Lisa Blecha, Katia Locatelli, Amine Benyamina and Catherine Martelli in Journal of Psychopharmacology
Footnotes
Acknowledgements
We thank the following authors for their kind collaboration: Lenze Eric (Washington University School of Medicine, St Louis, MO, USA); Reynolds Charles (University of Pittsburgh School of Medicine, University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA, USA); Stewart Anderson (University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA,USA); Salem Bensasi (University of Pittsburgh School of Medicine, Pittsburgh, PA, USA); Toshihide Kuroki (Kyushu University Graduate School of Human-Environment Studies; Kyushu; Japan); Sakiko Yamada (Abilify science manager Otsuka Pharmaceutical); Clement Parel (Otsuka Pharmaceutical Europ); Francesca Page (Otsuka Pharmaceutical Europ); Durgam Suresh (Clinical Development, Forest Research Institute); and Philip D. Ross (External Scientific Communications Group Allergan Jersey City, NJ, USA).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bruno Romeo, Lisa Blecha, Katia Locatelli and Catherine Martelli have no conflict of interest.
Amine Benyamina has been an invited speaker for Lundbeck, Mylan, Merck-Serono and Bristol-Myers Squibb, and is a member of the board for Indivior.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.