
Abstract
Objective:
The purpose of this study was to identify the association between antipsychotics and mortality in Alzheimer’s disease patients.
Methods:
Using the Taiwan National Health Insurance Research Database, 735 newly diagnosed Alzheimer’s disease patients aged over 65 years and receiving antipsychotic treatments, and 735 age, sex, physical comorbidity, and entry year with propensity scores, matched control subjects were enrolled and followed for a 10-year period until the end of 2011. Multivariate Cox proportional hazards regression models were used for analysis.
Results:
The mortality rate was 56% in Alzheimer’s disease patients treated with antipsychotics, and 65% in Alzheimer’s disease patients not treated with antipsychotics during an average of 5.2 years of follow-up. The use of antipsychotics, typical antipsychotics, and atypical antipsychotics was found to be associated with lower mortality (adjusted hazard ratio=0.66, 95% confidence interval 0.58–0.75; 0.69, 0.60–0.79; 0.56, 0.44–0.71, respectively, all p<0.001). In addition, Alzheimer’s disease patients with higher cumulative dose and longer duration of exposure to antipsychotics showed a significantly reduced risk of mortality. Other variables associated with higher risk of mortality included age (adjusted hazard ratio=1.08, 95% confidence interval 1.07–1.09, p<0.001), male gender (1.27, 1.11–1.45, p<0.001), diabetes mellitus (1.30, 1.10–1.54, p<0.01), congestive heart failure (1.54, 1.11–2.12, p<0.01), and stroke (1.23, 1.05–1.44, p<0.01).
Conclusion:
The use of antipsychotics was found to be associated with lower mortality in Alzheimer’s disease patients. Moreover, dose and duration response effects were also identified.
Introduction
Dementia is a major neurocognitive disorder characterized by a host of impairments in brain functions, including memory and learning, executive function, perceptual motor function, complex attention, social cognition, and language (American Psychiatric Association, 2013). The increasing life expectancy of humans contributes to the increased dementia population, and its prevalence is estimated to be 5–7% among people aged over 60 years (Prince et al., 2015). A majority of Alzheimer’s disease (AD) patients have behavioral and psychological symptoms of dementia (BPSD), which include various non-cognitive manifestations such as aggression, psychotic disorder (hallucination and delusion), sleep disturbance, and wandering ( Benoit et al., 2006; Lopez et al., 2003; Lyketsos et al., 2002). In addition, patients with BPSD are known to have poor outcomes during institutionalization, they often become a care-burden on the family, and cause high medical costs for the community (Alexopoulos et al., 2005; Benoit et al., 2006).
Common medications for treating BPSD include both typical antipsychotics (TAPs) and atypical antipsychotics (AAPs) (Alexopoulos et al., 2005; Reus et al., 2016). Over the last two decades, the prescription of AAPs to patients with dementia has become increasingly popular compared to that for TAPs because of fewer side effects (e.g. sedation, extrapyramidal signs, and electrocardiogram (ECG) abnormalities) (Brodaty et al., 2003; Tariot et al., 2006). The US Food and Drug Administration (FDA) launched a black-box warning of increasing mortality risk among patients with dementia: for taking AAPs in 2005, and for taking TAPs in 2008. Despite this warning, both drugs are still used to treat neuropsychiatric symptoms due to lack of better alternatives (Maher et al., 2011).
The relationship between exposure to antipsychotics (APs) and mortality rate in patients with dementia remains debatable (Gill et al., 2007; Kales et al., 2012; Knol et al., 2008; Nonino et al., 2006; Pilotto et al., 2017; Raivio et al., 2007; Rochon et al., 2008; Rossom et al., 2010; Schneider et al., 2005; Suh and Shah, 2005; Wang et al., 2005). For example, a meta-analysis of 17 placebo controlled trials involving the use of AAPs for the treatment of BPSD conducted by the FDA showed elevated mortality (odds ratio=1.7) (FDA, 2005) and the result was further confirmed by Schneider et al. (Schneider et al., 2005). However, several issues need to be considered when drawing conclusions from these studies. First, most trials in the meta-analysis study were conducted over short periods (ranging from 10–12 weeks). The long-term effect of these drugs is therefore unclear. Second, the studied samples comprised institutionalized patients with other severe symptoms linked to cognitive or behavioral morbidity. Thus, APs could have been associated with higher mortality risk in this often frail population (Huybrechts et al., 2012). Third, drug safety profiles may be different among the TAPs and AAPs (Nasrallah et al., 2004; Wang et al., 2005). Finally, drug dosage may be another important determinant of the safety of APs, but the dose-effect remains unclear (Gerhard et al., 2014; Huybrechts et al., 2012; Wei et al., 2014). Given these concerns, our aim was to determine the effects of both TAPs and AAPs on mortality using a different study design. This involved the extraction of data from a nationwide population-based dataset in Taiwan.
Methods
Data source
Data were taken from the National Health Insurance Research Database (NHIRD) of Taiwan, which was launched in 1995. The database contains information on more than 99% of the country’s 21 m population. From the database we retrieved patient information such as age, sex, date of birth, place of birth, medical expenditure, and prescribed drugs.
Study participants
The study was based on the Longitudinal Health Insurance Database 2000 (LHID 2000), which contains original claim data for one million beneficiaries randomly sampled from the year 2000 Registry for Beneficiaries, amounting to approximately 5% of the total population in Taiwan. The LHID contains information about all medical procedures and prescriptions from January 1996–December 2011 (http://nhird.nhri.org.tw/date_01_en.html).
Study design
This retrospective case-control cohort study occurred between 1 January 2001–31 December 2011. The period of study subject inclusions was from 1 January 2001–31 December 2006 and the observation period was from 2000–2011. We enrolled subjects aged over 65 years who were newly diagnosed with AD according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM; WHO 1999) codes: 290.0–290.3, 294.1–294.2, 331.0. Previous studies have demonstrated that validity and accuracy of NHIRD claim data with respect to medical records are moderate to substantial (Kappa 0.55–0.95; positive predictive values between 0.5–1.0) (Chang, 2004; Cheng et al., 2011, 2014). To validate the accurate diagnosis of AD, only patients who had at least two outpatient visits or inpatient hospitalization records were included in the study. From these patients, we identified a new user of APs if the TAPs or AAPs were first dispensed following cohort entry (defined as index date). To reduce the potential for selection bias, we excluded patients who had received APs before the index date. In addition, we excluded the following groups of patients from the study: (a) patients diagnosed with schizophrenia, bipolar affective disorder, delusional disorder, Huntington’s disease, or Parkinsonism because APs are used differently in these medical illness; (b) patients diagnosed with cancer as of the index date since TAPs (chlorpromazine, haloperidol) could be used as antiemetics in some cancer patients, who are more likely to die within 180 days regardless of drug use (Schneeweiss et al., 2007); (c) patients who used longer-acting AP formulations; (d) patients who are being treated with both TAPs and AAPs; and (e) patients who switched between TAPs and AAPs during the follow-up period. From the remaining patients, we further selected elderly new users of APs from the date of AD diagnosis and up to 31 December 2011 (n=735).
For control patients not treated with APs, we again selected from the same cohort population. To minimize potential confounding and selection biases, we used the propensity score (PS) method, which is considered to be more effective than other statistical methods used in observational studies (Rosenbaum, 1983). A multivariate Cox regression model was used to predict the probability of receiving APs, given the following set of covariates: age, sex, physical conditions as measured using the Charlson Comorbidity Index (CCI), and entry year. Comorbidities which occurred 12 months before the diagnosis of AD were evaluated. Finally, a PS was assigned to each subject, and this was subsequently used to match the AP treatment group with the non-AP treatment group at a ratio of 1:1 (AP case group vs matched control group, both n=735). The endpoints of the follow-up were defined as the occurrence of death or the end of the study (31 December 2011).
Previous studies have shown that dose- and duration-responses of APs could affect mortality (Kales et al., 2012; Wang et al., 2016; Wei et al., 2014) Therefore, we applied two indices to validate the risk of APs on mortality, namely the cumulative AP dose and cumulative AP exposure period.
The cumulative AP dose is the cumulative number of the defined daily dose (DDD). Drugs were classified according to the Anatomical Therapeutic Chemical (ATC) classification system (WHO Collaborating Centre for Drug Statistic Methodology (2006). The daily dose is based on the international standard DDD (ATC/DDD Index 2009, http://www.whocc.no/atc_ddd_index/ (accessed 1 May 2009)). (WHO, 2009) The cumulative AP DDD was calculated by dividing the AP dosage during the study period by the DDD. Cumulative AP DDDs were classified into four subgroups: (a) no use, (b) <60 DDDs, (c) 60–180 DDDs, and (d) >180 DDDs. The cumulative AP exposure period is the sum of the number of days for which APs were prescribed for each subject. It was also divided into four subgroups: (a) no use, (b) <60 days, (c) 60–180 days, and (d) >180 days.
Clinical characteristics and outcomes
All causes of mortality and the date of death were recorded (based on the insurance status, outpatient care, and hospitalization claims of the National Health Insurance (NHI). The overall disease burden of various comorbidities was represented using the CCI. The other relevant psychiatric disease was depression (at least three records of ICD-9-CM codes 296.2, 296.3, 300.4, 311). In addition, the diagnosis of stroke was defined (by ICD-9-CM codes 430–438) in receiving related treatments in one inpatient or three outpatient visits during the study period. Comorbidities in the 12-month period prior to the diagnosis of AD, including diagnoses of diabetes mellitus (ICD-9-CM code: 250), hypertension (ICD-9-CM code: 401–405), hyperlipidemia (ICD-9-CM code: 272), and congestive heart failure (ICD-9-CM code: 428) were confirmed by having at least one inpatient or two outpatient visits listed in the NHI record.
Statistical analyses
Chi-square tests and Student t-tests were performed to compare categorical and continuous variables including demographic and clinical characteristics between case and control groups. Multivariate Cox proportional hazards regression models were used to determine the relationship between exposure to APs and the risk of mortality after controlling for potential confounding factors. To correct for survival bias, Cox regression analysis was repeated with APs as time-dependent covariates, the value of which was allowed to change with the time component of the regression model. Potential factors that might confound the association were identified and examined initially in univariate models. Different relevant covariates which might confound the medication-death association were selected to examine the potential dose and duration response effects. For example, delirium itself is an independent risk factor for mortality, and it occurs frequently among elderly patients with AD. At the same time, APs are often prescribed for delirium (Adamis et al., 2006; Kales et al., 2007). Thus, we included the presence of delirium diagnosis at the time the APs were prescribed, as a covariate in our analyses. Furthermore, in order to address the potential for confounding effects of different classes of APs, we first divided patients into subgroups according to treatment with TAPs or AAPs, and then performed subgroup analysis. Kaplan–Meier curves were constructed to illustrate the cumulative rate of mortality between the groups during the follow-up period. The log-rank test was performed. All statistical tests were two-sided. Statistical significance was set at a p-value of 0.05, with a 95% confidence interval (CI). All statistical analyses were performed using SAS statistical software package version 9.2 (SAS Institute. Inc., Cary, North Carolina, USA).
Results
Baseline characteristics
From 14,924 patients in the database diagnosed with AD, 5898 were diagnosed within the study period (from January 2001–December 2006). The number of eligible patients after applying the exclusion criteria was 2169. From this number, we selected 735 AD patients who had received APs, and 735 AD patients who were not treated with APs as the comparison group (matched on age, sex, CCI, and entry year) (Figure 1). The mean age of patients who had received APs was 78.3±6.6 years, and that for the comparison group was 78.3±6.8 years. The demographic characteristics, usage of medication (APs and Acetylcholinesterase inhibitors [AchEIs]), rate of comorbid medical and psychiatric disorders, and death, are shown in Table 1. No significant difference was found between both groups, except usage of AchEIs, hyperlipidemia and death (p<0.05). During the entire observation period, 55.8% of AD patients receiving APs died, compared to 65.4% in the comparison group.
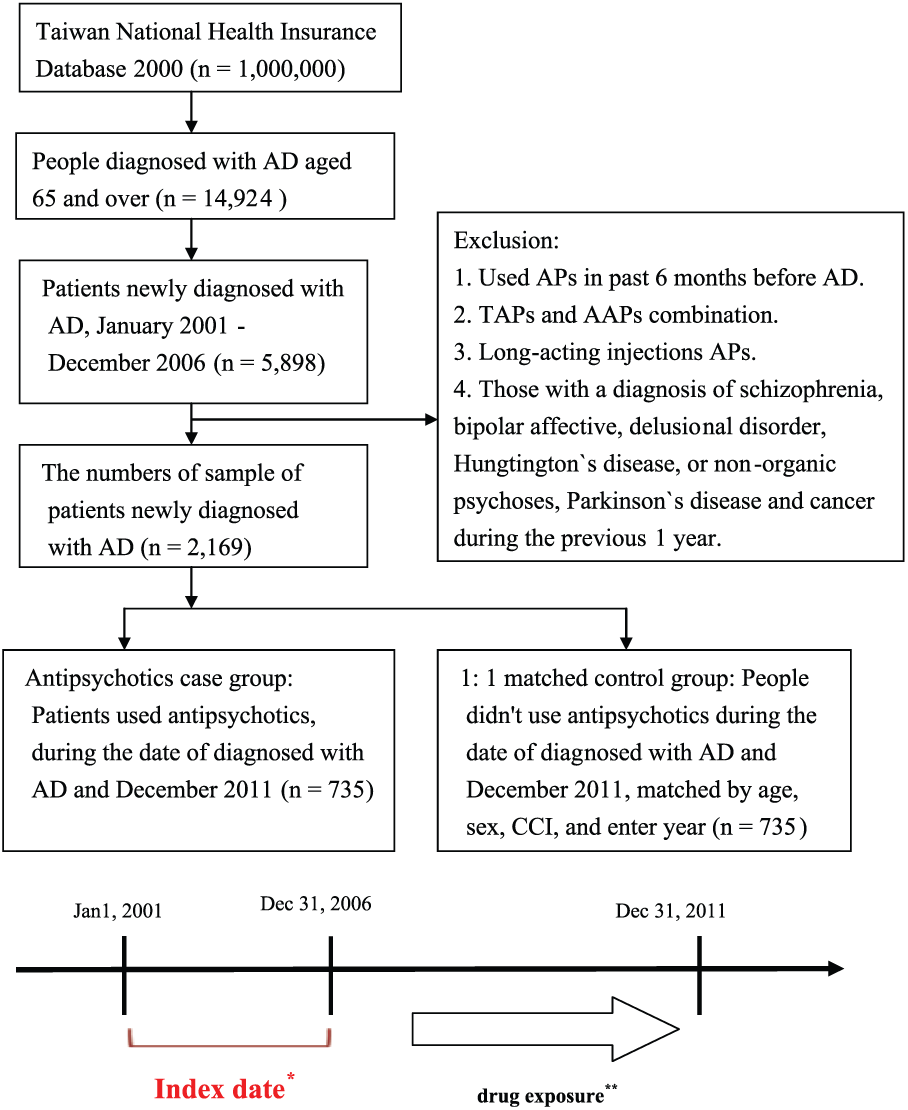
Flow-chart.
Demographic and clinical characteristics of patients with Alzheimer’s disease.
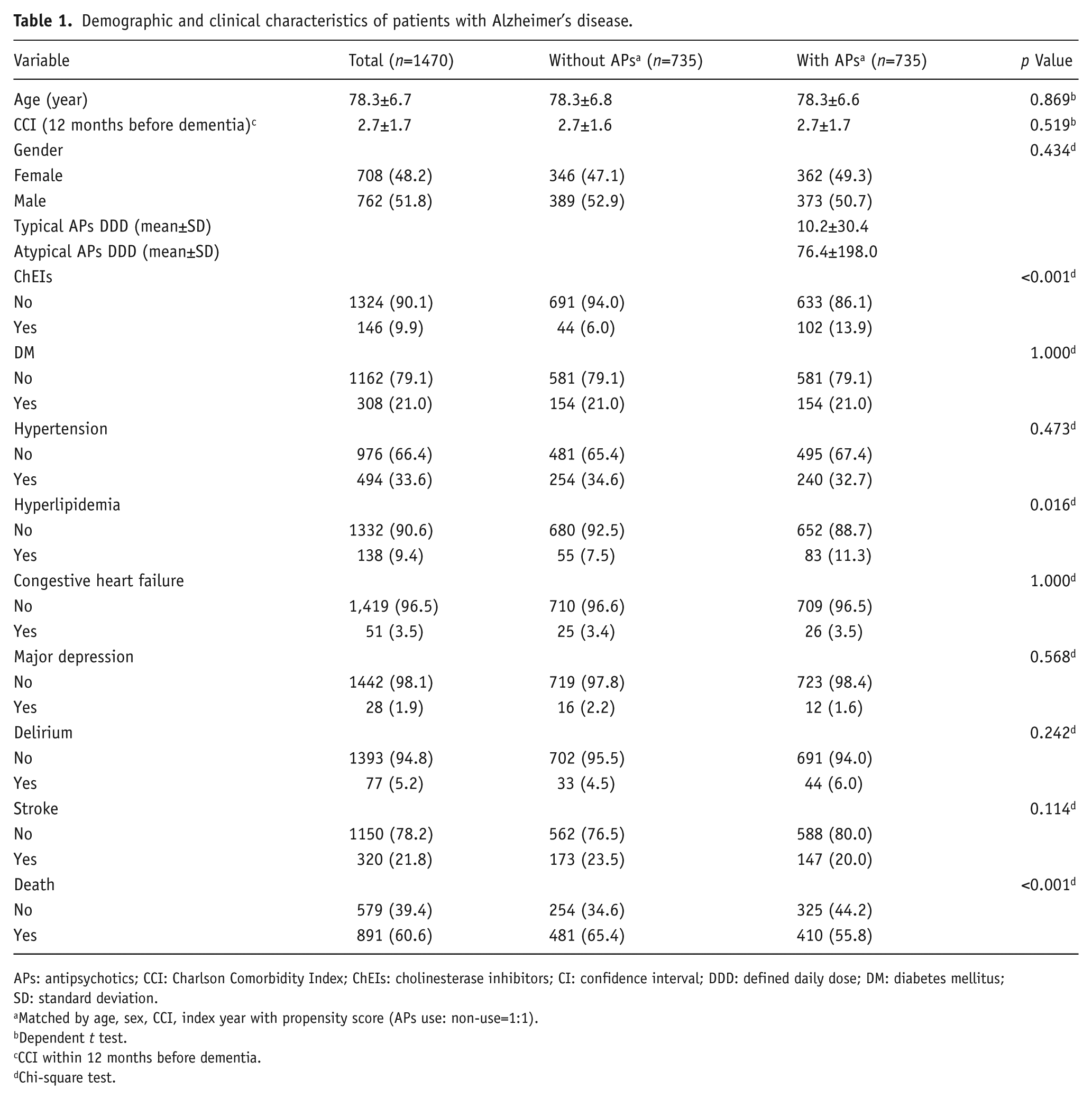
APs: antipsychotics; CCI: Charlson Comorbidity Index; ChEIs: cholinesterase inhibitors; CI: confidence interval; DDD: defined daily dose; DM: diabetes mellitus; SD: standard deviation.
Matched by age, sex, CCI, index year with propensity score (APs use: non-use=1:1).
Dependent t test.
CCI within 12 months before dementia.
Chi-square test.
Association between AP use and the risk of mortality
In model 1 of Table 2, we found a lower risk of mortality with the use of AchEIs (adjusted HR, aHR=0.57, 95% CI 0.44–0.75, p<0.001), hyperlipidemia (adjusted hazard ratio (aHR)=0.71, 95% CI 0.54–0.94, p<0.05), and AP (adjusted HR, aHR=0.66, 95% CI 0.58–0.75, p<0.001) after adjusting for age, sex, AchEIs, hyperlipidemia, CCI, major depression, and delirium (using the multivariate Cox proportional hazards regression model). In model 2 of Table 2, a higher risk of mortality was also associated with age (aHR=1.08, 95% CI 1.07–1.09, p<0.001), male gender (aHR=1.28, 95% CI 1.12–1.46, p<0.001), diabetes mellitus (aHR=1.31, 95% CI 1.11–1.54, p<0.01), congestive heart failure (aHR=1.54, 95% CI 1.11–2.12, p<0.01), and stroke (aHR=1.23, 95% CI 1.05–1.44, p<0.01). Compared to the AD patients who were not treated with APs, both users of TAPs (aHR=0.69, 95% CI 0.60–0.79, p<0.001) and AAPs (aHR=0.56, 95% CI 0.44–0.71, p<0.001) showed a significantly reduced risk of mortality. Model 3 of Table 2 shows the risk of mortality associated with different levels of exposure to APs. Compared to the control group, a significantly reduced risk of mortality was found in the following subgroups with a cumulative AP dose either less than 60 DDDs (aHR=0.68, 95% CI 0.59–0.77, p<0.001), 60–180 DDDs (aHR=0.58, 95% CI 0.37–0.93, p<0.05), or greater than 180 DDDs (aHR=0.37, 95% CI 0.20–0.68, p<0.01). In model 4 of Table 2, we found the reduced risk of mortality to be more pronounced in the subgroup of patients with the highest cumulative AP DDDs. The duration-response effect between exposure to APs and mortality was further revealed in the adjusted models. A significantly reduced risk of mortality was found in the subgroup with a period of cumulative AP use for less than 60 days (aHR=0.68, 95% CI 0.58–0.78, p<0.001), 60–180 days (aHR=0.67, 95% CI 0.53–0.85, p<0.001), and longer than 180 days (aHR=0.57, 95% CI 0.43–0.75, p<0.001).
Results of the Cox regression model examining the association between antipsychotics (APs) and mortality risk in Alzheimer’s disease (AD) patients (n=1470).
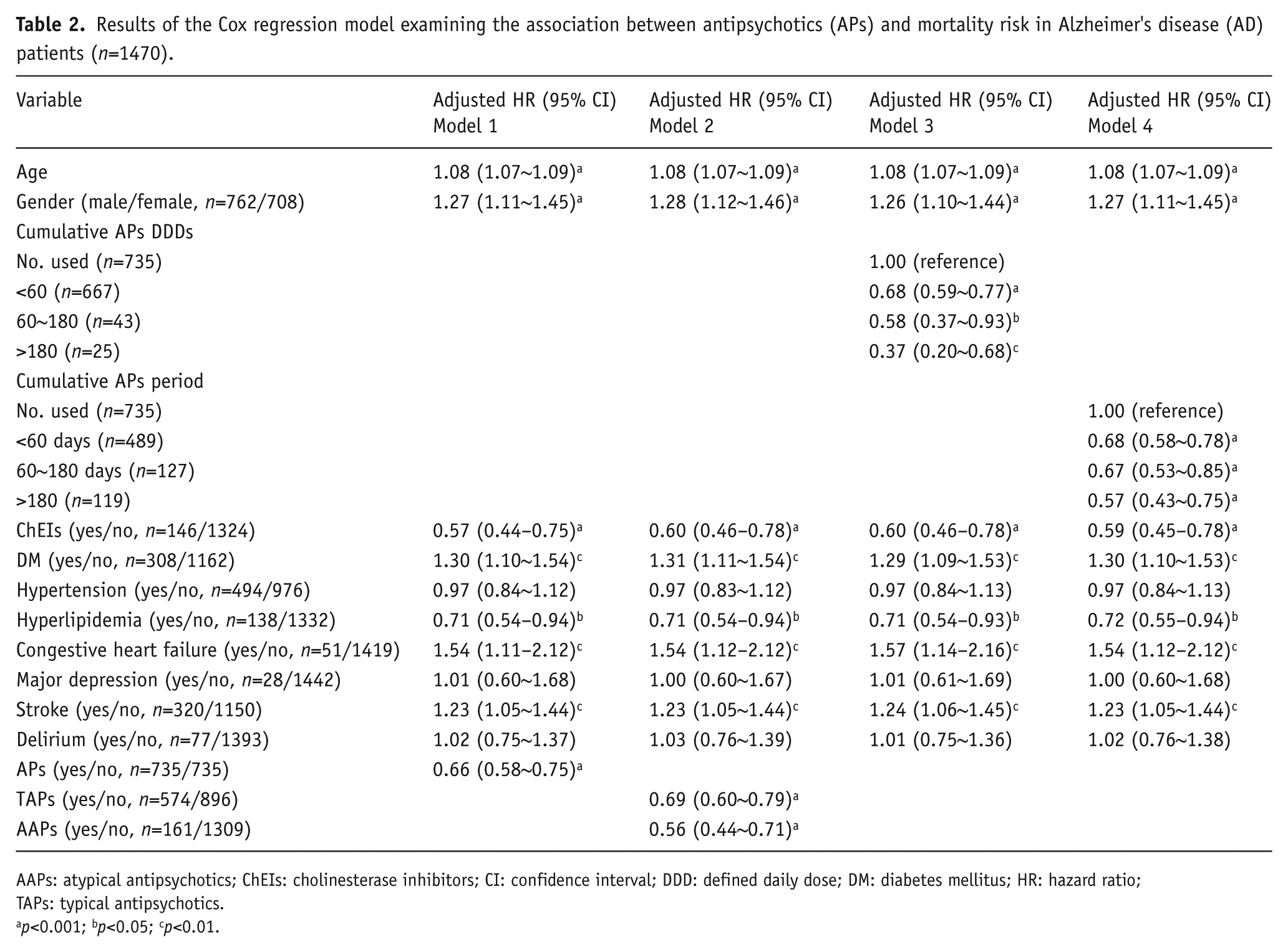
AAPs: atypical antipsychotics; ChEIs: cholinesterase inhibitors; CI: confidence interval; DDD: defined daily dose; DM: diabetes mellitus; HR: hazard ratio; TAPs: typical antipsychotics.
p<0.001; bp<0.05; cp<0.01.
Association between both TAPs and AAPs and risk of mortality in AD patients
Figure 2(a) shows the Kaplan–Meier analysis of the survival of AD patients treated with APs and those not treated with APs during the follow-up period (X2=39.47, degree of freedom (df)=1, p<0.0001, Log-rank test). Similarly, Figure 2(b) demonstrates that there is no significant difference in mortality risk in AD patients treated with either TAPs or AAPs (X2=1.296, df=1, p=0.255, Log-rank test).
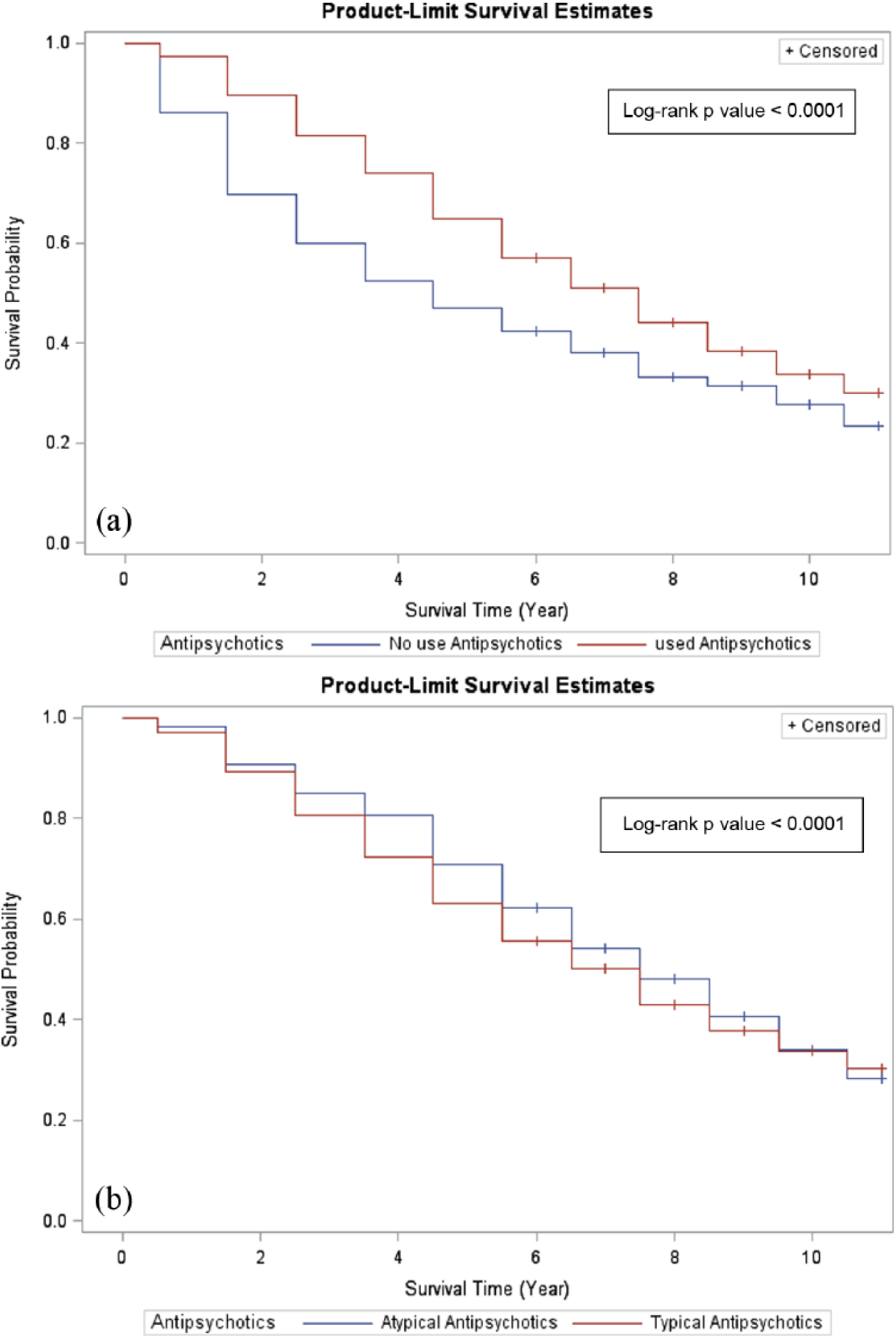
(a) Survival curves according to the antipsychotic (AP) treatment (yes/no) in Alzheimer’s disease (AD) patients. (b) Survival curves according to the typical AP (TAP) and atypical AP (AAP) treatment in AD patients.
Discussion
We did not find an association between APs and elevated mortality risk in AD patients but even protective effect. The results of our study showed that (a) AD patients taking either TAPs or AAPs had a lower risk of mortality compared to those not treated with APs; (b) a dose-response effect was observed in the subgroups treated with APs after adjusting for confounding factors. Moreover, a duration-response effect was found in the subgroups treated with APs; (c) AD patients receiving AChEIs had a significant lower risk of mortality compared to those not received with AchEIs.
Several studies have examined the association between APs and risk of mortality in AD patients, but the results are inconsistent (Gill et al., 2007; Kales et al., 2012; Knol et al., 2008; Nonino et al., 2006; Raivio et al., 2007; Rochon et al., 2008; Rossom et al., 2010; Schneider et al., 2005; Suh and Shah, 2005; Wang et al., 2005). Some studies reported higher mortality in AD patients treated with APs, (Gill et al., 2007; Kales et al., 2012; Knol et al., 2008; Rochon et al., 2008; Rossom et al., 2010; Schneider et al., 2005; Wang et al., 2005) while others described no risks of mortality, (Barak et al., 2007; Nonino et al., 2006) or even protective effects among AD patients (Raivio et al., 2007; Suh and Shah, 2005; Wei et al., 2014). For example, in a population-based, retrospective cohort study of patients with dementia, the use of TAPs and AAPs was associated with higher risk of mortality (Gill et al., 2007). On the contrary, in a study involving institutional geriatric patients with dementia from Finland using APs, the use of AAPs (risperidone, olanzapine) showed lower two-year mortality risk compared with that observed for non-users (Raivio et al., 2007). Additionally, Kales et al. found that quetiapine conferred a lower risk of mortality compared to other APs in dementia patients (Kales et al., 2012). In the present study, we did not examine what kinds of APs were mostly used. However, one study conducted by Chiu et al in 2017 (Chiu et al., 2017) used the NHIRD in Taiwan, as we used in the present study, and found that quetiapine and risperidone were the two most common APs prescribed for dementia. Therefore, the pattern of AP prescribed in Taiwanese dementia patients could provide some explanations of lower risk of mortality. Finally, to validate our finding, we conducted Cox proportional hazards regression analysis to account for several possible confounders, and we still could not find increased mortality risk with the use of APs. Rather, the use of APs seemed to have a somewhat protective effect. We also used the simple random sampling method to validate our findings using another statistical model, and the results were still the same.
Studies which reported the association of APs with mortality were short term studies, with mostly shorter than six-month follow-up periods (Kales et al., 2012; Knol et al., 2008; Rochon et al., 2008; Rossom et al., 2010; Schneider et al., 2005; Wang et al., 2005) Some of these studies found the risk of mortality being strongest shortly after the start of treatment. This risk of mortality reduced thereafter, indicating that the associated risk could be due to an uncontrolled acute disease rather than the AP itself (Kales et al., 2012; Wang et al., 2016; Wei et al., 2014). In the present study, we used Cox regression analysis to correct for survival bias and found that a larger protective effect of APs existed among AD patients who received treatment with APs for a longer period (>180 days). Short-term APs are prescribed for patients exhibiting acute behavioral and psychotic symptoms, which are predictors of mortality among patients with dementia (Craig et al., 2005; Wilson et al., 2005). Similarly, one study reported that psychiatric symptoms were strongly associated with mortality, instead of APs, in patients with probable AD who manifested psychiatric symptoms (Lopez et al., 2013). Except mortality, one recent study found AD patients with BPSD showed lower neuropsychiatric symptoms relapse in AP continuous treatment group (up to one year) compared with discontinuation of APs (Patel et al., 2016). Taken together, we might bear a fair view when prescribing APs for patients without problematic side effects and well-response to psychiatric symptoms.
The use of APs is associated with different mortality risks among patients with AD or other dementia (vascular/mixed dementia) (Liperoti et al., 2009; Suh and Shah, 2005). For example, APs are associated with a lower risk of mortality in AD patients but not in patients with vascular/mixed dementia (Suh and Shah, 2005). In a meta-analysis study of 15 placebo-controlled clinical trials which involved patients with AD or vascular/mixed dementia, AAPs were shown to be associated with a small increase in mortality risk (Schneider et al., 2005). However, proper controlling for confounding factors, especially cardiovascular risk factors, was not performed in that study (Schneider et al., 2005). Patients with vascular/mixed dementia were more likely to have comorbid vascular risk factors, such as cardiovascular disease and hypertension, when compared to AD patients. These comorbidities make AD patients vulnerable to cerebrovascular accidents, one of the commonest adverse events leading to death (Schneider et al., 2006). The sample population in the present study comprised only AD patients who exhibited less cardiovascular disease burden. We also used the propensity score matching method to select control cases. Therefore, the association between APs and mortality was minimally affected by the underlying comorbidities of patients, especially vascular risk factors, apart from selection bias.
The mechanisms underlying the protective effect of APs from mortality in AD patients are still unclear. The present finding is supported by studies showing a lower risk of mortality in patients with dementia taking AAPs (mainly quetiapine) (Huybrechts et al., 2012; Kales et al., 2012; Rossom et al., 2010). AAPs have been identified as having anti-oxidative properties, which are one of the pathophysiological etiologies of AD (Al-Chalabi et al., 2009; Rinaldi et al., 2003; Zhang et al., 2012). Most importantly, the APs could reduce the levels of agitation, anxiety, and aggression, leading to these vulnerable patients easier to control and subsequently to receive proper care and reduced further complication.
Another interesting finding of the present study is that patients with AD who received AchEIs demonstrated significant lower risks of mortality in all models compared with those who did not receive AchEIs. Our findings are consistent with recent study conducted by Pilotto et al. (Pilotto et al., 2017), reporting community-dwelling patients treated with anti-dementia drugs had a significant lower risk of death than untreated patients, although another study showed no effect of AchEIs on life expectancy (Lopez et al., 2002). The inconsistency between these studies might be related to patient characteristics (all-cause dementia or AD), different setting (community-based or nursing home), or dose- and duration-effect (Gasper et al., 2005; Lopez et al., 2002; Pilotto et al., 2017; Wattmo et al., 2014). We did not investigate risk of mortality of individual anti-dementia drugs and if there is any dose- and duration- dependent effects among patients with AD. The contribution of these effects is beyond the scope of the present study and further studies are warranted.
Study strengths and limitations
The present study has some noteworthy strengths. First, we conducted a nation-wide population-based study with wide population coverage. Therefore, our sample was more representative of the general population and of patients with AD. Second, dose- and duration-dependent effects of APs were assessed more critically using the cumulative dose and cumulative dose duration, instead of using less comprehensive evaluations such as prescription counts or continuous duration of AP therapy. Third, we restricted the outcome only to patients with AD (excluding vascular/mixed dementia). Such homogeneity in the selected populations aided in avoiding possible confounding effects of vascular risk factors, one main contributor to mortality in AD patients.
The present study has several limitations, which should be addressed. First, information related to diagnostic decisions including dementia severity, specific neuropsychological assessments for dementia (e.g. Mini-Mental State Examination, Mini-Cog Test, Clinical Dementia Rating, and Cognitive Assessment Screening Instrument), brain imaging and laboratory data (e.g. electrolyte imbalance results) could not be obtained from the database. Nevertheless, all insurance claims of the NHI program were scrutinized by medical reimbursement specialists and peer reviews. The institutions will be penalized and no reimbursement will be made if coding of diseases or treatments is incorrect, as such, coding errors have been minimized. Second, information on adherence to the prescribed medication is unavailable in the database. Non-adherence to the prescribed medication can lead to the misclassification of exposure and the underestimation of the protective effect of APs. Third, several potential confounding factors such as malnutrition and substance use (such as cigarette smoking and alcohol consumption) were unavailable in the database. Therefore, residual confounding due to unmeasured covariates could not be ruled out. Fourth, as most subjects from our study are ethnic Chinese, the extent to which our findings can be generalized to other ethnic populations remains to be determined. Finally, we could not look into the exact causes of death in the individuals because morality data in the NHIRD could not be linked to the death certification records. Therefore, we identified the codes of inpatient diagnosis one month before among those patients who expired during the hospitalization as proxy as cause of death. The most common reason for death is pneumonia (detailed in Supplementary Material Table 1), which is line with previous similar studies (Brunnstrom and Englund, 2009). We think this finding is reliable, as previous study has reported the accuracy of death records in the NHIRD was high and valid (Cheng et al., 2015).
Conclusion
In summary, both TAPs and AAPs were found to be associated with lower mortality in AD patients. Moreover, an association between dose and duration of APs, and reduced mortality was found in AD patients. Although the current study demonstrated protective effects of APs on mortality in AD patients, especially in the long-term, we suggest that clinicians should also take into account the benefit-to-risk ratio of APs in AD patients.
Supplemental Material
JOP780016_Supplementary_Tables – Supplemental material for The use of antipsychotics is associated with lower mortality in patients with Alzheimer’s disease: A nationwide population-based nested case-control study in Taiwan
Supplemental material, JOP780016_Supplementary_Tables for The use of antipsychotics is associated with lower mortality in patients with Alzheimer’s disease: A nationwide population-based nested case-control study in Taiwan by Che-Sheng Chu, Wan-Rung Li, Kuan-Lun Huang, Pei-Yu Su, Ching-Heng Lin and Tsuo-Hung Lan in Journal of Psychopharmacology
Footnotes
Acknowledgements
This study is based in part on data from the NHIRD provided by the National Health Insurance Administration, Ministry of Health and Welfare and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of National Health Insurance Administration, Ministry of Health and Welfare or National Health Research Institutes. This work was supported by grants from the Ministry of Health and Welfare, Taiwan (MOHW107-TDU-B-212-123004). The authors would like to thank the Healthcare Service Research Center (HSRC) of Taichung Veterans General Hospital for statistical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study is supported in part by the Taichung Veterans General Hospital (TCVGHAGE-99B10), the Ministry of Health and Welfare, Taiwan (MOHW107-TDU-B-212-123004). The funders had no role in study design, data collection, and analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.