
Abstract
Background:
Cognitive deficits are prevalent in bipolar disorder during remission but effective cognition treatments are lacking due to insufficient insight into the neurobiological targets of cognitive improvement. Emerging data suggest that dorsal prefrontal cortex target engagement is a key neurocircuitry biomarker of pro-cognitive treatment effects.
Aims:
In this randomized controlled functional magnetic resonance imaging study, we test this hypothesis by investigating the effects of an ineffective cognitive remediation intervention on dorsal prefrontal response during strategic memory encoding and working memory engagement.
Methods:
Bipolar disorder patients in partial remission with subjective cognitive difficulties were randomized to receive 12-week group-based cognitive remediation (n = 13) or to continue their standard treatment (n = 14). The patients performed a strategic episodic picture encoding task and a spatial n-back working memory task under functional magnetic resonance imaging at baseline and following cognitive remediation or standard treatment.
Results:
The right dorsolateral prefrontal cortex was commonly activated by both strategic memory tasks across all patients. The task-related prefrontal engagement was not altered by cognitive remediation relative to standard treatment. The dorsolateral prefrontal cortex response was not significantly associated with recall accuracy or working memory performance.
Conclusions:
As hypothesized, no task-related change in prefrontal activity was observed in a negative cognitive remediation trial in remitted bipolar disorder patients. By complementing previous findings linking cognitive improvement with increased dorsolateral prefrontal cortex engagement, our negative findings provide additional validity evidence to the dorsal prefrontal target engagement biomarker model of cognitive improvement by strengthening the proposed causality between modulation of dorsolateral prefrontal cortex engagement and pro-cognitive effects.
Introduction
Cognitive impairments related to memory, attention and executive function are core features of bipolar disorder (BD) that often persist during remission (Cullen et al., 2016). Trait-related cognitive dysfunction in patients with BD is a key aspect of the disorder that impedes functional recovery as well as treatment response and prognosis (Gitlin and Miklowitz, 2017; Martino et al., 2008; Torrent et al., 2012). Addressing cognitive impairments may therefore play a pivotal role in a successful syndromal and functional recovery in BD as well as other psychiatric disorders such as unipolar disorder (UD) and schizophrenia, where cognitive dysfunctions have high prevalence (McGurk et al., 2007). Despite intense research efforts within the past decade, there are no effective clinical treatments of cognitive function for BD patients (Miskowiak et al., 2016a, 2016c). This may partially be due to the absence of a human neuroimaging biomarker model of cognitive improvement that would facilitate the selection among novel candidate cognition treatments prior to large-scale clinical phase III trials (Miskowiak et al., 2017b).
Cognitive remediation (CR) is a behavioural training-based intervention that aims to improve cognitive processes (attention, memory, executive function, social cognition and metacognition) to facilitate functional recovery. A meta-analysis across 40 CR studies in patients with schizophrenia showed that CR had a noticeable beneficial effect on several cognitive domains such as attention, verbal working memory, memory and learning, as well as functioning (Wykes et al., 2011). The effects of CR in mood disorders are less conclusive. In a recent naturalistic study, Veeh et al. (2017) found no cognitive benefits of 12 weeks of a group-based CR programme in BD patients (n = 26) compared with patients given standard treatment (ST) (n = 10), although post-hoc analyses of within-group change in the CR group suggested some cognitive improvements over time. In an open trial in BD patients (n = 18), 14 individual sessions of CR increased observer-based ratings of executive function (Deckersbach et al., 2010). In UD patients, 10-week cognitive remediation was shown to improve attention and processing speed and verbal memory in 17 CR vs. 16 waiting-list patients (Bowie et al., 2013). Improved learning and memory (but not attention, psychomotor speed and executive function) have also been reported in UD patients (n = 16) following 10 weeks of cognitive training using the Neuropsychological Educational Approach to Remediation (Naismith et al., 2010). It is worth noting that these studies included small patient samples, non-randomized treatment allocation and often lacked an a priori hierarchy between the cognition measures, which would guard against selective outcome reporting (Miskowiak et al., 2017a). In contrast, in a randomized controlled trial, we found no statistically significant cognitive improvements in a group of BD patients in remission treated with CR (n = 18) compared to the group given ST (n = 22) (Demant et al., 2015).
There is emerging evidence that cognitive dysfunctions in schizophrenia and affective disorders are underpinned by similar abnormalities in the function of dorsolateral prefrontal cortex (dlPFC). The dlPFC region has been suggested to play a critical superordinate role in regulating cognitive control being involved in various cognitive tasks where executive functions are recruited (Miller and Cohen, 2001). Different aspects of executive dysfunction have been examined in these neuropsychiatric illnesses, demonstrating aberrant dlPFC activity across a range of cognitive tasks including multiple facets of working memory, response inhibition, conflict processing and problem solving (Lee et al., 2014; Minzenberg et al., 2009). Both task-related hypo- and hyper-activity in dlPFC have been observed in schizophrenia (Minzenberg et al., 2009; Ragland et al., 2009) and replicated in the majority of studies in BD and UD (Dietsche et al., 2014; Fernández-Corcuera et al., 2013; Frangou et al., 2008; Hamilton et al., 2009; Monks et al., 2004; Townsend et al., 2010) although some studies in UD also found hyper-activity (Ebmeier et al., 2006; Harvey et al., 2005; Matsuo et al., 2007). Callicott et al. (2003b) suggested that abnormalities of PFC function in schizophrenia are reflected by a compromised neural strategy for handling information mediated by the dlPFC and reconciled evidence of both hypo- and hyper-dlPFC activity by proposing a model where patients’ activity increases, peaks and drops earlier as a function of task difficulty than it does in healthy control subjects. In addition, similar abnormal prefrontal activity has also been observed in healthy first-degree relatives of BD and schizophrenia patients (Allin et al., 2010; Callicott et al., 2003a; Drapier et al., 2008). Aberrant task-related dlPFC activity thus seems to be the most reproducible neural marker of cognitive dysfunction across neuropsychiatric and genetically predisposed individuals.
Given the involvement of this dorsal PFC region in active working memory maintenance and manipulation and in strategic encoding processes, these functional deficits are thought to reflect problems with selection and maintenance of information in working memory and with tactical memory encoding (Ragland et al., 2009). Consistently, two recent meta-analyses of functional magnetic resonance imaging (fMRI) data from CR interventions in schizophrenia demonstrated increased activations in various brain regions, mainly prefrontal, but also in parietal, occipital, anterior cingulate regions during working memory and executive tasks (Isaac and Januel, 2016; Ramsay and Macdonald, 2015). In line with these findings, an fMRI study investigating working memory and recollection memory changes following a 10-week CR treatment in mood disorder patients, Meusel et al. (2013) found behavioral improvements on working memory tests, outcomes associated with increased task-related response in lateral and medial PFC. However, decreased working memory activations in mood disorder patients have also been reported following vortioxetine treatment, a multimodal drug for depression shown to improved cognitive function (Smith et al., 2017). In a double-blinded randomized phase II trial conducted in 43 BD patients, we previously showed that 8 weeks of recombinant human erythropoietin (EPO) administration vs. placebo improves certain cognitive functions such as attention and executive function (Miskowiak et al., 2014), and further showed that the EPO treatment improved picture recall and increased encoding-related activity in dlPFC and temporo-parietal regions (Miskowiak et al., 2016b), irrespective of changes in mood. Taken together, these findings highlight prefrontal target engagement as a promising biomarker for cognitive deficits and pro-cognitive effects of both pharmacological and cognitive treatments across distinct neuropsychiatric disorders. The validity of such a biomarker model may be confirmed by testing the model against five key validity criteria (Harmer et al., 2011): it must (i) be sensitive to treatment with pro-cognitive effects, (ii) produce similar effects in patients with cognitive dysfunction and healthy participants, (iii) be sensitive to effective treatments with different mechanisms, (iv) be unresponsive to ineffective treatments and (v) be sensitive to cognitive improvement and decline.
Here we aim to test the biomarker model of dorsal prefrontal target engagement according to criteria (iv) in a group of remitted patients with BD randomized to either 12 weeks of group-based CR treatment in addition to ST or ST alone. As previously reported, the CR treatment did not result in significant improvements in any of the tested cognitive domains (Demant et al., 2015). We therefore hypothesized non-significant changes in the engagement of prefrontal regions involved in strategic cognitive processes (strategic memory encoding and working memory) following the CR intervention compared to ST. Across all patients, we further expected that greater task-related dlPFC engagement (reflecting inefficient processing) would correlate with poorer task performance (Callicott et al., 2003b).
Methods
Study design and patients
Patients were recruited from community psychiatric centres and practicing psychiatrists in Copenhagen, Denmark. Eligible patients had an ICD-10 diagnosis of BD according to the Schedule for Clinical Assessment in Neuropsychiatry (Wing et al., 1990), had subjective cognitive difficulties according to the Massachusetts General Hospital Cognitive and Physical Functioning Questionnaire (Fava et al., 2006), (score >4 on >2 domains), and were in full or partial remission according to the 17-item Hamilton Depression Rating Scale (HDRS) (Hamilton, 1960) and the Young Mania Rating Scale (YMRS) (Young et al., 1978), (scores <14). Exclusion criteria were a diagnosis of schizophrenia or schizoaffective disorder, significant suicide risk, electroconvulsive therapy (ECT) treatment within the past three months and current substance or alcohol abuse. Patients were permitted to take drugs for depression, anxiety, psychosis and relapse prevention (lithium). Complete details related to study design and inclusion criteria can be found in Demant et al., 2013. In total, 40 patients aged 18 to 50 years were found to be eligible and included in the study investigating the effects of cognitive remediation therapy on verbal memory, sustained attention, executive and psychosocial function (Demant et al., 2015). Patients were randomized (1:1) to receive either 12-week add-on group-based CR or to maintain their current ST in an evaluator-blind, between-group design. A clinical and behavioural assessment and an fMRI investigation were performed immediately before and after the intervention. Out of the 40 originally included patients, the MRI investigation was cancelled for five (one missed the first fMRI session, two due to body metal and two due to claustrophobia) and seven dropped out after completing the first fMRI session. In addition, the fMRI dataset from one patient was not included due to poor quality. Thus, data from 27 (14 ST and 13 CR) patients were include in the current fMRI study. The study was approved by The Regional Committee on Biomedical Research Ethics (protocol number H-1-2010-039), the Danish Data Protection Agency (protocol number 2010-41-4710) and was registered at clinicaltrials.gov (identifier NCT01457235). Written informed consent was obtained from all patients.
Interventions
The randomization of patients was performed by Pharma Consulting Group (http://www.pharmaconsultinggroup.com) using stratification for age (<35 years) and years of education (<15 years). The investigators were blinded to treatment allocation. In cases when one of the investigators became aware of the treatment received by a patient, a different blinded evaluator carried out further assessments. Blinding was maintained throughout the study, including in data management and analysis.
Patients randomized to the CR group received CR in addition to ST. CR was conducted in a group setting in weekly sessions of 2 hours over 12 weeks followed by a booster session of 4 weeks after treatment completion. We opted for a group setting over individual treatment because being part of a group of people that experience similar cognitive difficulties tends to be a motivational factor for adherence to treatment. Also, group settings are more cost effective than individual treatment, thus enhancing the chances of potential clinical implementation of this treatment. Finally, short-term prolonged exposure therapy in a group setting has been shown to have beneficial effects in BD (Torrent et al., 2013). The rationale for choosing a short-term treatment of 12 weekly sessions was that CR treatment durations vary across studies and there are no indications that a longer duration will result in greater cognitive improvement. Therefore, it seemed reasonable to investigate the effects of a short-term treatment given its greater feasibility and cost effectiveness vs. a longer-term treatment. A more detailed description of the CR programme, including examples of compensatory and adaptive strategies, can be seen in the published study protocol (Demant et al., 2013). Patients randomized to ST continued their ST with no added CR treatment. The ST for all patients typically included combined psychopharmacological treatment and group-based psychoeducation at the Copenhagen Affective Disorder Clinic or at patients’ local community mental health centres (Kessing et al., 2013). Patients that received psychoeducation had all finished the psychoeducation course prior to the inclusion in the present trial.
Behavioural and clinical assessment
The patients performed a battery of cognitive and clinical tests at baseline and the follow-up investigation including the HDRS, YMRS the Rey Auditory Verbal Learning Test (RAVLT), (Rey, 1964), the Delayed Matching to Sample (DMS) from the Cambridge Neuropsychological Test Automated Battery and the Danish Adult Reading Test (DART), used as a measure of premorbid intelligence (Nelson and O’Connell, 1978). For details on all outcomes in the entire cohort of 40 subjects, please see Demant et al., 2015. Given our investigation of neuronal underpinnings of memory encoding in the current sample of 27 patients, we also report the scores from RAVLT (the primary outcome), the DMS test and the clinical ratings HDRS and YMRS in our current sample of 27 individuals investigated with fMRI. In addition, we report the accuracy scores of the episodic memory encoding and working memory tasks performed under fMRI (see below).
Volume of interest
Our functional analysis was initially restricted to a volume of interest (VOI). The VOI included the dorsal regions of the PFC and the hippocampi and was defined on a standard Montreal Neurologic Institute (MNI) template provided in the FMRIB’s Software Library (FSL) package using FSLView 4.0.1. The dlPFC was delineated bilaterally to include the superior and medial frontal gyri and the superior portions of the anterior division of the cingulate gyrus and the frontal poles. We defied the ventral border of the dlPFC by the area separating the dorsal from the ventral regions of medial PFC (MNI z >5), according to Veit et al., 2010. The bilateral dlPFC subregions and the hippocampi were defined using cortical maps thresholded at 5% provided by the Harvard-Oxford cortical structural Atlas implemented in FSLView (Desikan et al., 2006) and added together to form the final VOI.
The picture-encoding task
Task description
The task is a modified version of the encoding task from Hariri et al., 2003. Patients were instructed to determine whether pictures showed indoor or outdoor scenes and to pay attention as they would be asked to recall the pictures. The present task thus involved a strategic memory encoding component. This was followed by a free recall test immediately after the scan (Miskowiak et al., 2016b). Pictures were matched for valence, arousal and complexity and were presented in a blocked paradigm to maximize sensitivity for hippocampal blood-oxygen-level-dependent (BOLD) signal change (Birn et al., 2002). Six picture blocks (24 s each) were preceded by an instruction screen (2 s) and interleaved with 24 s of fixation crosses, resulting in a task duration of 4 min 50 s. Blocks consisted of six pictures presented serially for 3 s interleaved with a 1-s fixation cross. Each block contained an equal number of pictures representing indoor and outdoor scenes. Alternate matched versions of the task were administered at baseline and follow up in a counterbalanced order to minimize effects of learning.
Statistical analysis of functional MRI data
Functional MRI data processing was performed with the FMRI Expert Analysis Tool (version 6.00) part of FSL (www.fmrib.ox.ac.uk/fsl). Pre-processing involved image realignment, non-brain removal, spatial normalization to an MNI template and spatial smoothing (Gaussian kernel, 5 mm full-width-half-maximum). The time series in each session were high pass-filtered (to max 0.008 Hz). At subject level, we modelled the picture-encoding task using a block design and convolved the blocks with a canonical hemodynamic response function (Boynton et al., 1996). For each subject, we also calculated a contrast image representing the change in BOLD response between baseline and follow-up measurements by subtracting the estimated baseline image from the follow-up image (longitudinal contrast).
At the group level, we first calculated task activations at baseline across all subjects by entering the picture encoding contrast at baseline in a one-sample t-test. Second, we estimated group-by-time interaction effects (treatment group: ST or CR), (time: baseline and follow-up scan) by entering the longitudinal contrasts in a two-sample t-test. As a post-hoc test, we verified that the findings were not dependent on baseline-task performance by constructing an analogue model that included a performance covariate. Third, we estimated non-specific treatment effects on picture encoding by entering the longitudinal contrasts of all subjects in a one-sample t-test. The three statistical models were estimated using nonparametric permutation-based inference (n = 5000) using the ‘randomize’ algorithm implemented in FSL (Winkler et al., 2014). The models were estimated twice, first restricting the search volume to the defined VOI and second at whole-brain level, otherwise using identical parameters. Significant clusters were identified using the Threshold-Free Cluster Enhancement (TFCE) method at corrected p < 0.05.
The n-back task
Task description
An n-back working memory task was employed because it is widely used to probe memory aspects of executive function (Wager and Smith, 2003). During fMRI, participants performed a visuo-spatial n-back working memory task that included a strategic aspect by requiring continuous updating of the stored memory items (Miskowiak et al., 2016d). The task consisted of blocks of three types of conditions that differed in terms of working memory load (0-back, 1-back and 2-back). In each condition, a yellow circle appeared in a sequence of 14 appearances at random locations in a 5 x 5 grid. The circle was displayed for 300 ms followed by an empty grid for 1200 ms. In 1-back and 2-back conditions, patients indicated with a button press when the circle appeared at the same location as one trial and two trials back, respectively. During the 0-back condition, patients pressed a button when the circle appeared in one of the four grid corners. The blocks had an average of three target trials and were presented successively five times (15 blocks in total) interleaved with 8 s fixation crosses. The total task length was 7 min 35 s.
Statistical analysis of functional MRI data
fMRI data from the n-back task was pre-processed following the same procedure as for the picture encoding task above. Three conditions, 1-back, 2-back and 0-back, were modelled at subject level as blocks convolved with a canonical hemodynamic response function and we computed the high-load specific working memory ‘2-back>1-back’ and the general working memory ‘2-back>0-back’ contrasts. For these two contrasts, we further calculated ‘longitudinal contrasts’ by subtracting the baseline image from the follow-up image for each subject.
At the group level, we first calculated task activations at baseline across all subjects by entering the baseline high-load specific and general working memory contrasts in one-sample t-tests. Second, we estimated group-by-time interaction effects (treatment group: ST or CR), (time: baseline and follow-up scan) by entering the two longitudinal contrasts in separate two-sample t-tests. As a post-hoc test, we verified that the findings were not dependent on baseline-task performance by constructing analogue models that included the d’ performance covariate (see below). Third, we estimated non-specific treatment effects on high-load specific and general working memory by entering the respective longitudinal contrasts in one-sample t -test across all subjects. The statistical models were estimated in the same way as for picture encoding task by using FSL ‘randomize’ algorithm, which was run twice, first restricting the search volume to the defined VOI and second at whole-brain level. Significant clusters were identified using the TFCE method at corrected p < 0.05. Behavioural data from three baseline and four follow-up n-back sessions were lost; we therefore verified the findings by rerunning the analyses including only subjects with complete baseline and follow-up behavioural data (nine ST and 11 CR).
Planned follow-up fMRI analyses
To test our hypothesis, we isolated brain activity specifically related to strategic cognitive processes independent of task specifics by identifying regions commonly activated by both strategic tasks. We explored whether the BOLD response to each task in the identified dlPFC regions correlated with associated task performance or the DMS scores. For this we computed an image containing the region activated at baseline during both strategic memory encoding and working memory (2-back>0-back) and extracted the mean percent BOLD signal change from this region for both contrasts. We first tested for significant linear correlations between task-related dlPFC BOLD response at baseline and task performance (see below) and DMS scores. We then tested whether baseline to follow-up changes in dlPFC BOLD response and changes in task performance scores correlated across all subjects. The correlation analyses were performed using Statistical Package for the Social Sciences (SPSS) v20 with p < 0.05 as significance threshold.
MRI acquisition protocol
MRI data were acquired with a Siemens Trio MR scanner (Siemens Trio, Erlangen, Germany) using an eight-channel head array coil. We collected BOLD-sensitive fMRI using a T2*-weighted gradient echo-planar imaging sequence. Acquisition parameters for the sequences used for both the picture encoding and n-back tasks: echo time (TE) 30 ms, repetition time (TR) 2.49 ms, flip angle 90°. Each brain volume consisted of 42 slices with a slice thickness of 3 mm and a field of view (FOV) of 192 × 192 mm with a 64 × 64 grid. Overall, 117 brain volumes were acquired for the picture-encoding task and 184 brain volumes for the n-back task.
High-resolution, three-dimensional structural T1-weighted spin echo images were also obtained using the following acquisition parameters: TI = 800, TE = 3.93, TR = 1540 ms, flip angle 9°, 256 × 256 FOV and 192 slices. The protocols used for baseline and follow-up investigation were identical.
Statistical analysis of behavioural and clinical variables
The CR and ST groups were compared for demographic variables and changes in behavioural and clinical characteristics with SPSS v20 (IBM, Armonk, New York, United States). The performance on the picture-encoding task was calculated as the number of correctly recalled pictures assessed following the fMRI session. The performance of the n-back task (1-back and 2-back) was calculated as d’ response accuracy (correct hits) corrected for response tendency (commission errors) using the signal detection theory (Grier, 1971). Continuous data (demographic: age and education, cognitive scores: RAVLT, DMS, picture encoding and n-back performance, and the depression ratings: HDRS and YMRS) were checked for deviation from the normal distribution using the Shapiro-Wilk test. In the case of significant deviations from normality, group differences were assessed using non-parametric Mann-Whitney U tests. The Pearson chi-square test was used to evaluate whether the distribution of the two sexes was even among the treatment groups.
Longitudinal changes in the cognitive measures of interest (RAVLT, DMS, picture encoding and n-back performance) were evaluated in repeated measures analysis of covariance (ANCOVA) models using the treatment group (CR and ST) as within-subject factor and time of investigation (baseline and follow up) as between-subject factor. The ANCOVA model used to test for changes in working memory further included a load factor (2-back and 1-back). We controlled for differences in mood symptoms by including the changes in HDRS as covariate in the model. Longitudinal changes in the HDRS and YMRS scores were assessed in analogue ANCOVA models with the stratification variables as covariates (age and years of education).
Using two-sample t-tests we also checked for any differences in baseline cognitive and clinical measures and baseline to follow-up changes in these tests between the group of 27 patients included in the fMRI analysis and the group of 13 patients from the Demant et al. study (2015) not included.
Results
Demographic and behavioural data
The CR and ST groups were comparable for age and years of education and baseline (Table 1). There was no significant difference in the change in picture recall accuracy or in the change in estimated working memory performance between the ST and CR groups (e.g. no significant group-by-time interaction effects).
Demographic behavioural, and clinical data.
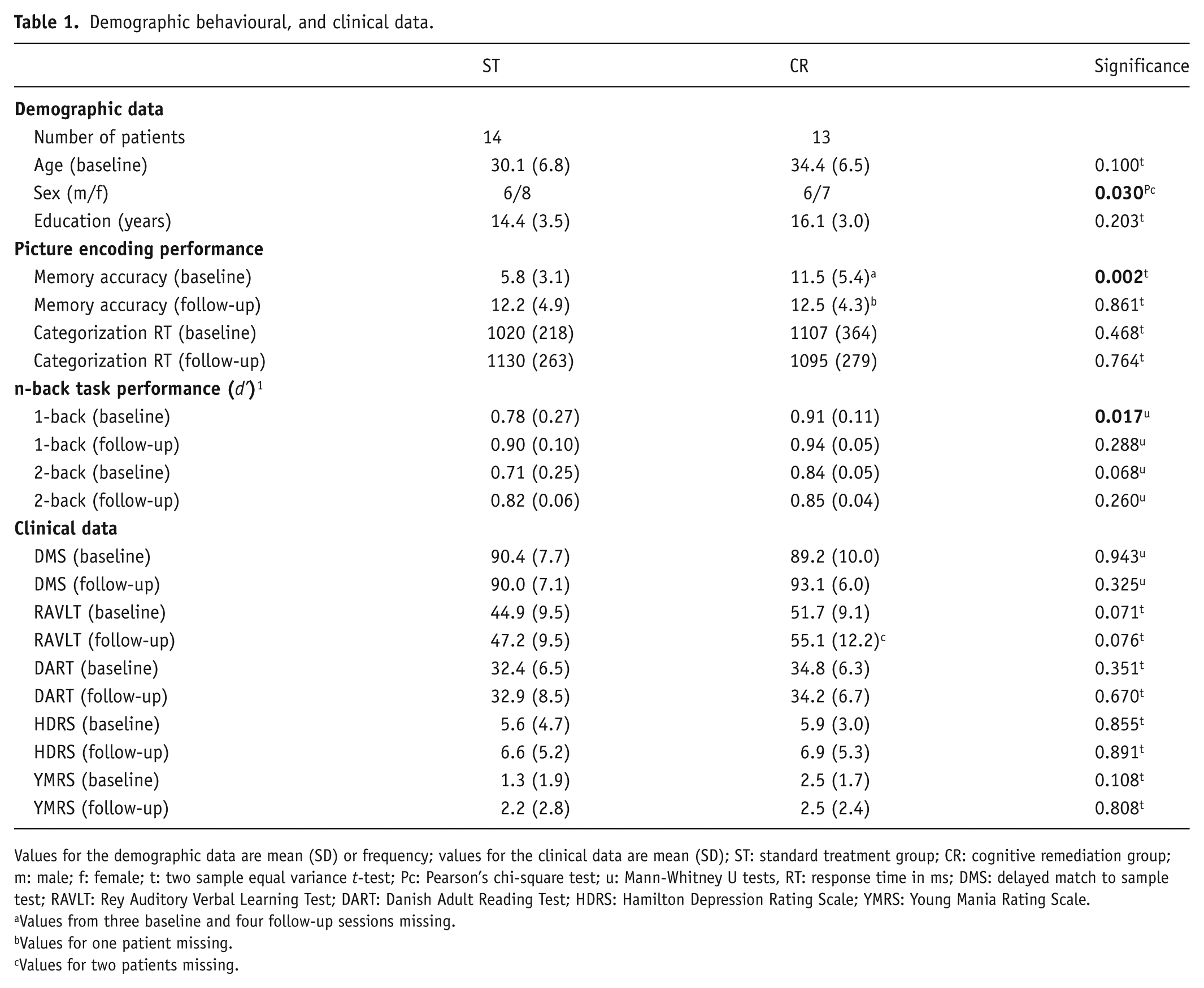
Values for the demographic data are mean (SD) or frequency; values for the clinical data are mean (SD); ST: standard treatment group; CR: cognitive remediation group; m: male; f: female; t: two sample equal variance t-test; Pc: Pearson’s chi-square test; u: Mann-Whitney U tests, RT: response time in ms; DMS: delayed match to sample test; RAVLT: Rey Auditory Verbal Learning Test; DART: Danish Adult Reading Test; HDRS: Hamilton Depression Rating Scale; YMRS: Young Mania Rating Scale.
Values from three baseline and four follow-up sessions missing.
Values for one patient missing.
Values for two patients missing.
The picture recall accuracy analysis showed a significant main effect of time (F1,22 = 19.886, p < 0.001) denoting a general improvement in task performance and a significant group-by-time interaction (F1,22 = 6.169, p = 0.021). Post-hoc tests revealed the ST group had a lower performance at baseline compared to the CR group (two-sample t-test, p = 0.002), which improved significantly at follow up (paired t-test p < 0.001), Figure 1A. The CR group did not show a significant change between the baseline and follow-up measurements (p > 0.239). The working memory performance was similar between the groups at both the baseline and follow-up measurements (Figure 1B). As expected, there was a main effect of working memory load across both groups and times of investigation with lower performance for the 2-back vs. 1-back task (F1,18 = 18.442, p < 0.001).
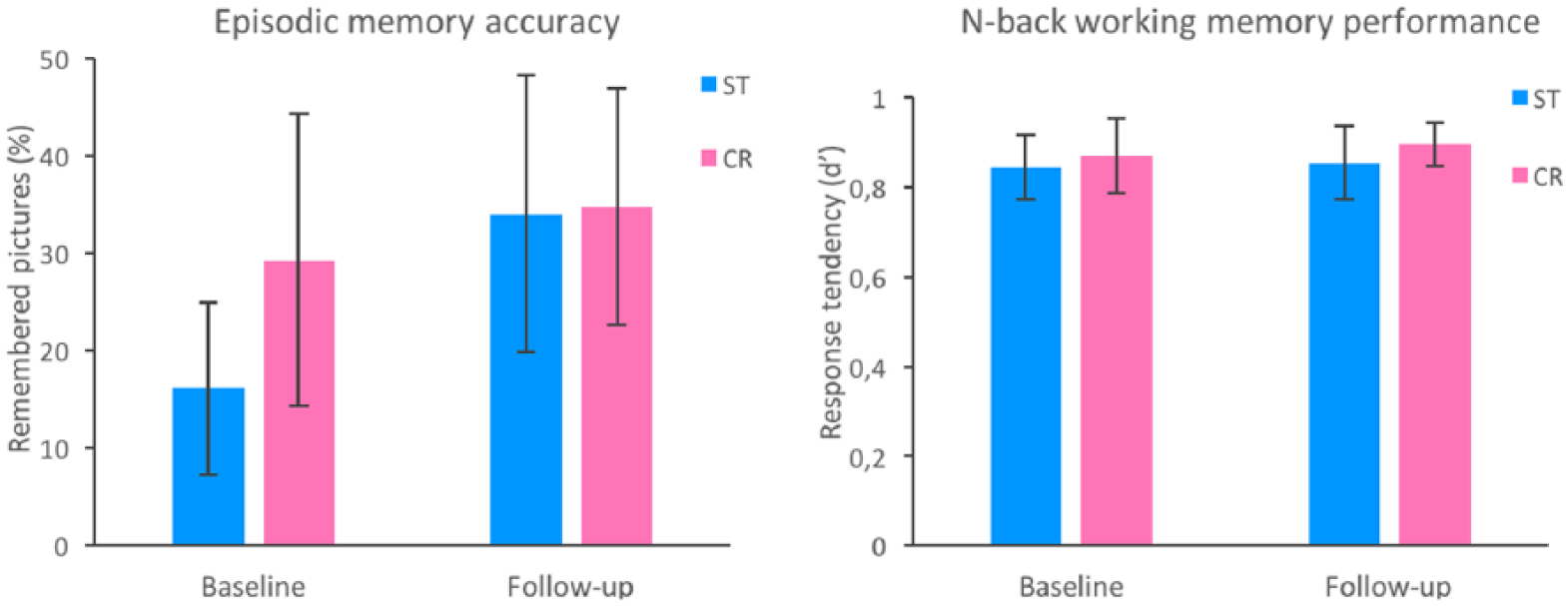
Comparison of the effect of standard treatment (ST, n = 14) and cognitive remediation therapy (CR, n = 13) on episodic memory accuracy (left panel) and working memory performance (right panel) in patients with bipolar disorder. The episodic memory accuracy was calculated as the correctly recalled number of pictures following the magnetic resonance imaging session in the picture-encoding task. The working memory performance scores represent the average response accuracy (d’) for the 1-back and 2-back tasks. The ST group showed a lower episodic memory recall accuracy compared to the CR group at baseline and a significant improvement at follow up compared to baseline. The error bars show standard deviation.
There was no differential change in the DART, RAVLT and DMS cognitive scores between the CR and ST groups over time (p > 0.868 and p > 0.265, respectively). We also found no differential chance between the two treatment groups in mood symptoms (p > 0.402 and p > 0.412, for HDRS and YMRS respectively). However, there was a significant increase in depression symptoms over time across both groups (F1,23 = 6.040, p = 0.022).
There were no statistically significant differences between the group of 27 patients included in the fMRI analysis and the group of 13 patients from the Demant et al. study (2015) not included regarding baseline cognitive and clinical measures or changes in these tests from baseline to follow up.
Functional MRI analyses
Picture-encoding task
There were no significant group-by-time interaction effects in the brain response to picture encoding at a whole-brain level or within the dlPFC and hippocampus VOI. The negative finding remained after controlling for baseline task performance. Across all patients at baseline, the right dlPFC was significantly activated to picture encoding at a whole-brain level and within the VOI (Table 2, Figure 2). The hippocampi were, however, not significantly activated by the task. There were no differences between the baseline and follow-up task activations, i.e. there were no significant non-specific treatment effects.
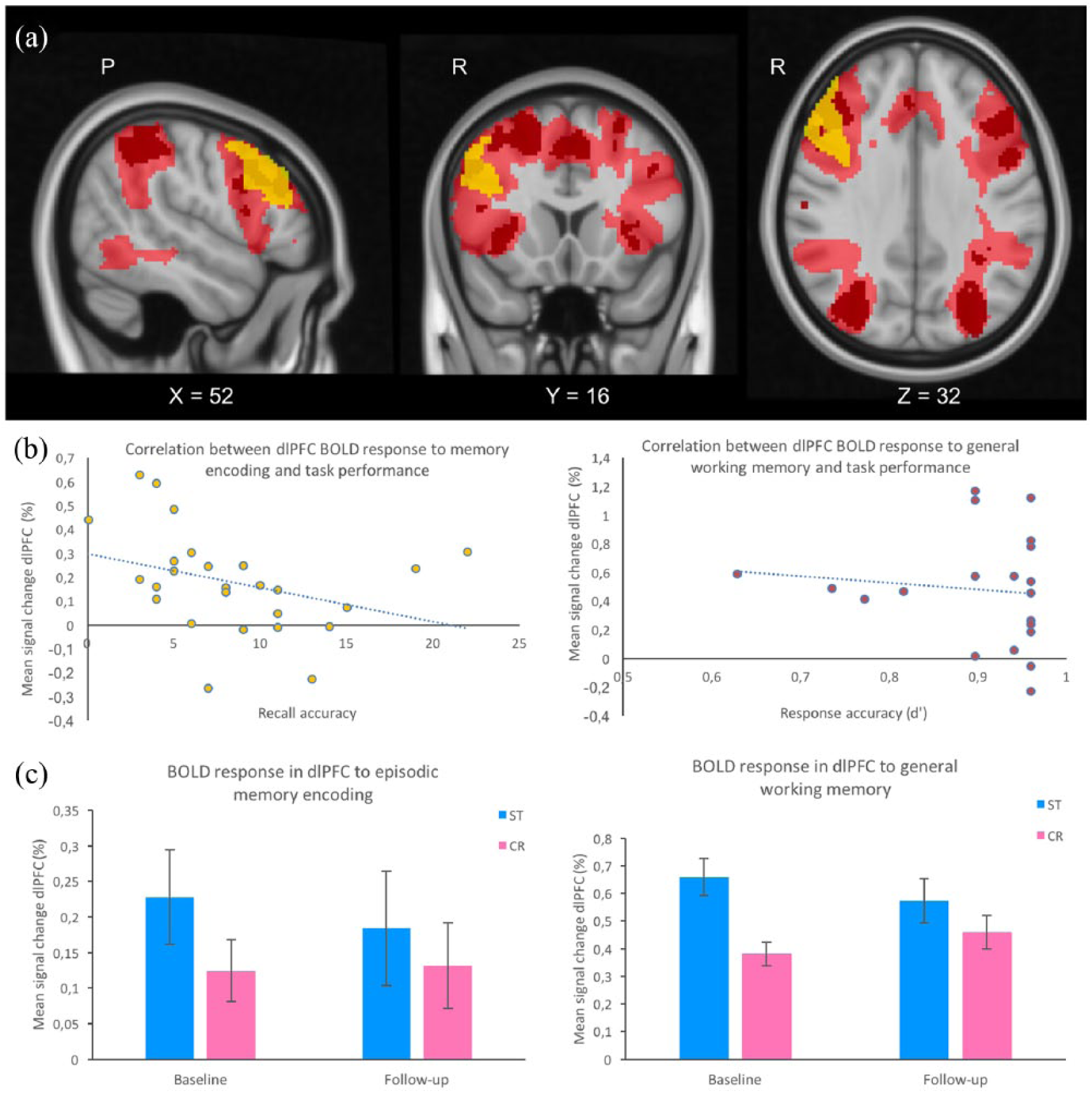
Task-related blood-oxygen-level-dependent (BOLD) responses to the strategic picture encoding and working memory tasks in 27 patients with bipolar disorder. a) Statistical map showing significantly increased BOLD response to strategic picture encoding (yellow) and general working memory (2-back>0-back) at the baseline investigation. b) Baseline correlations between the task related BOLD response in the dorsolateral prefrontal cortex (dlPFC) region commonly activated by the picture-encoding (left panel) and working memory (right panel) tasks and the associated task performance. The statistical analyses showed non-significant negative correlations between BOLD response and performance in both functional magnetic resonance imaging tasks. c) Graphs show BOLD response in the dlPFC region commonly activated by both the memory-encoding and working memory tasks presented by treatment group (standard treatment, n = 14 and cognitive remediation, n = 13) and time of investigation (baseline and follow up). There was no significant effect of time or group-by-time interactions in either of the two tasks. Error bars show SEM.
Significant clusters for the picture encoding and the n–back task. Cluster peak and local maxima of more than 20mm apart are represented with x, y, z MNI coordinates and Threshold–Free Cluster Enhancement corrected p values.
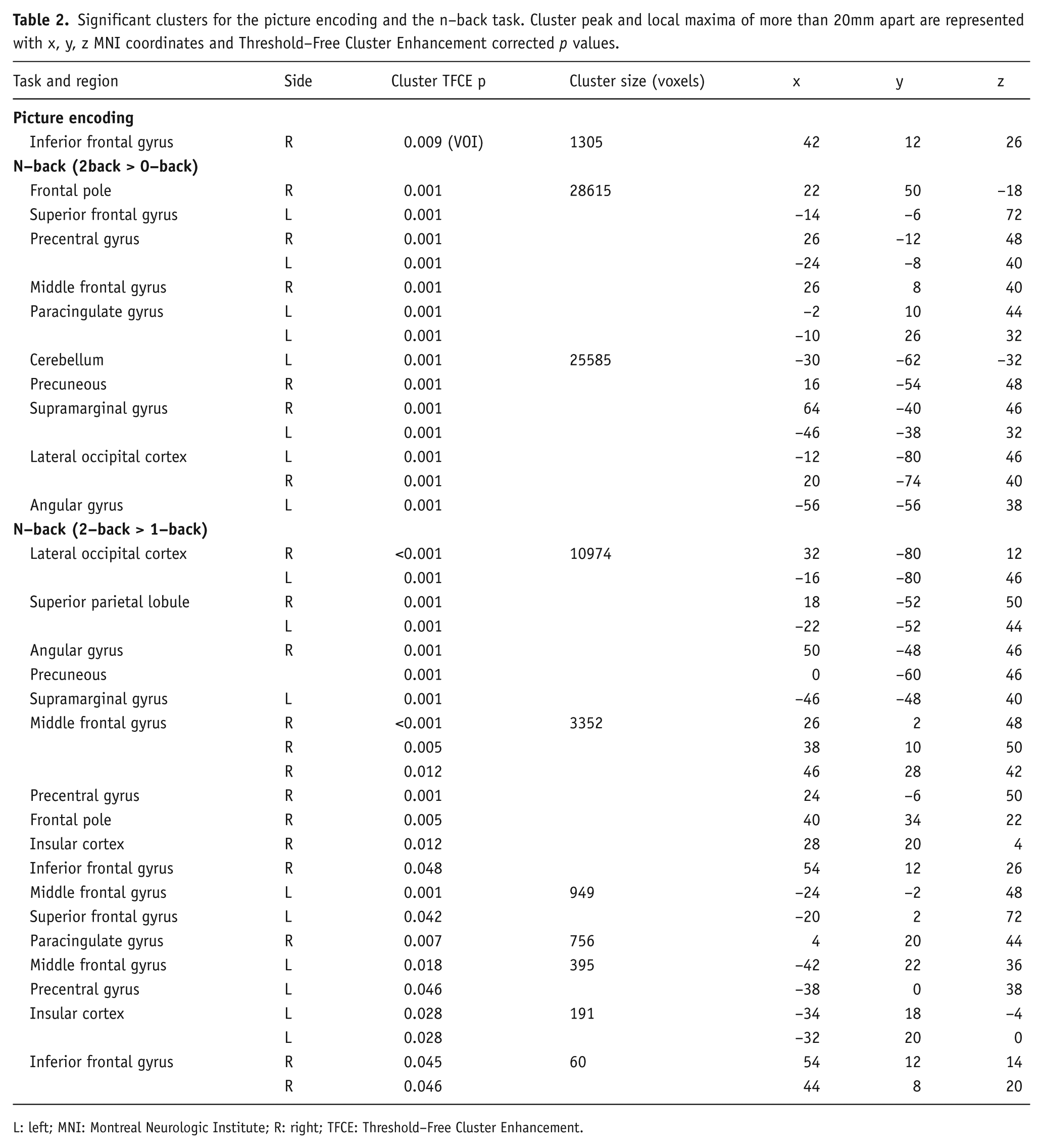
L: left; MNI: Montreal Neurologic Institute; R: right; TFCE: Threshold–Free Cluster Enhancement.
N-back task
There were no significant group-by-time interaction effects in the brain response to 2-back>0-back or to 2-back>1-back responses at a whole-brain level or within the VOI. Controlling for baseline task performance or excluding the subjects with missing behavioural data did not reveal any significant findings. Across all patients at baseline, the 2-back>0-back and 2-back>1-back significantly activated a widespread working memory related fronto-parietal network (Table 2, Figure 2). There were no significant differences between the baseline and follow-up working memory-related responses across all patients.
Planned follow-up analyses
Across all subjects at baseline, the task-related BOLD response in the strategy-related dlPFC region commonly engaged by the picture encoding and general working memory (see above) showed a non-significant negative correlation with associated performance in the fMRI tasks (Pearson c = -0.34, p = 0.089 and Pearson c = -0.045, p = 0.835 for the picture encoding and n-back task respectively, Figure 2B). The baseline to follow-up change in BOLD response to picture encoding and general working memory did not correlate with longitudinal changes in respective task performance. The analogue correlation analyses between DMS scores and task-related dlPFC BOLD response yielded no significant findings in either of the two fMRI tasks.
Discussion
In this randomized controlled fMRI study in BD patients, we tested the hypothesis that dorsal prefrontal target engagement is a key neurocircuitry biomarker of pro-cognitive treatment effects. We investigated the outcome of a 12-week group CR intervention compared to ST on dorsal prefrontal response during strategic memory encoding and working memory engagement. This was a negative trial in terms of lack of statistically significant pro-cognitive effects of CR compared with ST on cognitive function as previously reported (Demant et al., 2015). As hypothesized, we found no significant effect of cognitive remediation therapy compared to ST in the neural response to either strategic picture encoding or working memory performance within the dorsal PFC and hippocampus VOI or when exploring across the entire brain. The BD patients engaged the dlPFC during strategic memory encoding and working memory to a similar degree at the baseline and follow-up measurements. The response in the right dlPFC region commonly activated by both tasks did not correlate significantly with performance scores in either of the two tasks. Behaviourally, the CR vs. ST group comparison showed no CR-related improvement in picture recollection after fMRI, in n-back working memory performance or in verbal or spatial memory measured with the RAVLT and DMS. These findings support our initial hypothesis that an ineffective treatment would not alter prefrontal target engagement in strategic cognitive processes, thus confirming one of the proposed validity criteria for biomarker models (see Introduction).
The right dlPFC region commonly engaged in both fMRI tasks has been suggested to play a critical role in supervisory attentional control independent of task specifics by monitoring the relevant task set and exciting goal-relevant processing areas (Cieslik et al., 2015). In a previous study in mood disorder patients we observed improved picture recall following eight weekly EPO (40 000 IU) infusions vs. saline, an effect associated with increased response to picture encoding in an overlapping dlPFC region (Miskowiak et al., 2016b). The ability of different interventions to impact response sensitivity in this region may therefore be predictive of pro-cognitive effects. In support of this hypothesis, studies across distinct neuropsychiatric disorders with cognitive dysfunctions where cognitive improvement can be observed following pharmacological or cognitive treatments typically show increased prefrontal task-related activations (Isaac and Januel, 2016; Meusel et al., 2013; Miskowiak et al., 2016b; Ramsay and Macdonald, 2015). For instance, a 10-week CR treatment in mood disorder patients was shown to improve performance in working memory and recollection as well as improve working memory-related activations in latera and medial PFC and lateral parietal regions (Meusel et al., 2013) and preliminary findings in UD by Siegle et al. (2007) showed that an intensive 2-week CR intervention targeting the brain correlates of depression was associated with increased dlPFC response to high-effort cognitive tasks while decreasing depression severity. A recent meta-analysis of fMRI data from CR interventions in schizophrenia revealed robust treatment-associated reversal of task-related dorsal and medial hypo-activity (Ramsay and Macdonald, 2015). In contrast, although administration of the multimodal drug for depression vortioxetine resulted in improved subjective cognitive function in UD patients, Smith et al. (2017) showed decreased dlPFC and hippocampus response during an n-back working memory task following 14 days of active treatment vs. placebo. Notably, although hippocampal hypo-activity has been reported during memory encoding and retrieval in both UD and BD and linked to the observed memory deficits in these patients (Fairhall et al., 2010; Glahn et al., 2010; Kelley et al., 2013; Milne et al., 2012), treatment studies have not reported consistent changes in task-related hippocampal activity, which is in line with our negative findings in this region. Interestingly, the association between memory performance and related hippocampal response was only found to be significant in healthy but not in UD individuals (Dietsche et al., 2014), suggesting a deficient hippocampal engagement to memory encoding and recall in mood disorders.
While the neurobiological mechanisms associated with cognitive impairments remain unclear, neuroanatomical studies in neuropsychiatric disorders demonstrate structural abnormalities in various brain regions subserving cognitive function such as the dlPFC and medial PFC, anterior cingulate cortex and hippocampus (Bora et al., 2012). Critically, pharmacological and cognitive intervention that demonstrate improved cognitive function are associated with neuroplastic structural changes. We previously showed that 8 weeks of EPO treatment in treatment-resistant UD and BD patients improved memory recall and increased grey matter volume in the left hippocampus (Miskowiak et al., 2015). Following a 2-month memory training intervention, individuals with subjective memory impairment exhibited improved recall and grey matter volume increases in frontal, temporal and parietal brain regions involved in episodic memory (Engvig et al., 2014). Although there was no significant group change in the hippocampus, individual differences in hippocampal change were related to greater memory improvement following treatment. In addition, schizophrenic patients followed for two years while receiving cognitive enhancement therapy showed greater preservation of grey matter volume in the left hippocampus, parahippocampal gyrus and fusiform gyrus, and greater grey matter increases in the left amygdala, compared with a control group receiving supportive illness management therapy (Eack et al., 2010). Overall, these findings present compelling evidence that the beneficial effect of pro-cognitive treatment is at least partially mediated by grey matter changes in regions subserving cognitive function. A successful cognitive intervention may therefore be conditional on structural neuroplastic changes independent of the therapeutic approach.
The strengths of the current study include a high completion rate and the use of a randomized control design accounting for learning effects. However, there are also limitations. First, the employed CR protocol might not have been long or intensive enough (one session per week for 12 weeks) to stimulate significant neuroplastic changes. For instance, the beneficial effect of CR in schizophrenia are often observed after longer-term (average 16.7 weeks), more frequent sessions (2.2 per week) and mainly in individualized CR treatments (Wykes et al., 2011). Second, at screening, we did not use an objective measurement of the patients’ cognitive deficits. In particular, we are unware of how our patient groups compare with healthy controls in the memory domain. The baseline cognitive performance of the larger group (n = 40) used for participant inclusion in the present study (Demant et al., 2015) was comparable with international normative data, showing that despite the subjective cognitive complaints, there were no significant objective cognitive dysfunctions in executive function or sustained attention at group level. The absence of objective cognitive deficits in many of the included patients may have limited the detection of treatment effects on cognitive function and neural engagement at the group level due to ceiling effects. Consistently, neuropsychological impairment in BD before treatment was found to predict the improvement in psychological functioning in response to CR treatment (Deckersbach et al., 2010; Miskowiak et al., 2017a). Notably, the ST group showed lower memory recall performance at baseline compared with the CR group, which improved at follow up. This improvement was, however, not associated with a change in dlPFC engagement and may reflect a general task repetition or learning effect observed in both groups, but more evident in the ST group due to their lower baseline task performance. Third, a relatively small sample of patients may have resulted in decreased statistical power and impeded the detection of more subtle treatment-related changes. Caution should therefore be applied when interpreting the negative findings. Nevertheless, our data provide hypothesis-generating evidence because the majority of the CR studies in schizophrenia included in the Ramsay and Macdonald, (2015) meta-analysis of fMRI data were based on similar or smaller sample sizes, yet still demonstrate significant treatment effects on cognitive function and related neural responses. Finally, there might also be differences in the psychopharmacological and/or psychoeducational treatments performed by the CR and ST groups as part of their standard illness management. However, none of the included patients received targeted treatment to improve cognition. Possible differences in the received ST are therefore not likely to account for the lack of significant group differences in memory performance.
In conclusion, this randomized controlled fMRI study revealed that a 12-week group-based CR in fully or partially remitted patients with BD had no significant effect on picture recall or working memory performance and related neural processes in the dlPFC. The dlPFC region commonly engaged by both fMRI tasks seems to be involved in strategic cognitive processes across several tasks and was previously associated with pro-cognitive effects. We suggest that the failure of the CR intervention to increase strategy-related dlPFC activity constitutes the neurobiological underpinning of its lack of efficacy on cognition. These findings bring further support to the prefrontal target engagement biomarker model of pro-cognitive improvement. Additional studies are underway to further examine this model.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JM and KMD report no biomedical financial interests or potential conflicts of interest. Within the past three years, MV reports being a consultant for Lundbeck and Astra Zeneca, LVK reports having been a consultant for Lundbeck, AstraZeneca and Sunovion, HRS discloses honoraria as journal editor from Elsevier Publishers and book editor from Springer Publishing as well as honoraria as speaker from Genzyme and MerckSerono and grant support from Biogen-idec and KWM reports having received consultancy fees from Lundbeck and Allergan.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the TRYG foundation (grant number 7-09-0159), received by KWM.