
Abstract
Background:
Intravenous ketamine has been established as an efficacious and safe treatment, with transient effect, for treatment-resistant depression. However, the effectiveness of intravenous ketamine in non-research settings and with ultraresistant depression patients remains understudied.
Aims:
This study aims to measure the response and remission rates in ultraresistant depression patients in a clinical setting by means of a retrospective, open label, database study. Secondarily, the study will attempt to support previous findings of clinical predictors of effectiveness with intravenous ketamine treatment.
Methods:
Fifty patients with ultraresistant depression were treated between May 2015–December 2016, inclusive, in two community hospitals in Edmonton using six ketamine infusions of 0.5 mg/kg over 40 min over 2–3 weeks. Data were collected retrospectively from inpatient and outpatient charts. Statistical analysis to investigate clinical predictors of effectiveness included logistic regression analysis using a dependent variable of a 50% reduction in rating scale score at any point during treatment.
Results:
At baseline, the average treatment resistance was severe, with a Maudsley Staging Method score of 12.1 out of 15, 90.0% were resistant to electroconvulsive therapy, and the average Beck Depression Inventory score was 34.2. The response rate was 44% and remission rate was 16%. As a single predictor, moderate or severe anhedonia at baseline predicted a 55% increased likelihood of response. As a combined predictor, this level of anhedonia at baseline with a diagnosis of bipolar depression predicted a 73% increase in likelihood of response.
Conclusion:
In a clinical setting, intravenous ketamine showed effectiveness in a complex, severely treatment-resistant, depressed population on multiple medication profiles concurrently. This study gave support to anhedonia and bipolar depression as clinical predictors of effectiveness.
Introduction
An underserved and suboptimally treated population exists in depressed patients who have failed a comprehensive treatment regimen of antidepressants, augmentation strategies, psychotherapy, and electroconvulsive therapy (ECT) and can be described as ultraresistant depression (URD). These patients carry a large burden of illness (Kessler, 2012; Vos et al., 2015). When using the colloquial definition of an inadequate response to adequate trials of two or more antidepressants, it can be extrapolated from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial that over 35% of major depressive disorder (MDD) patients develop treatment-resistant depression (TRD), and of that population, 40% remain depressed after ECT which is considered the gold standard of treatment for TRD (Kennedy et al., 2016; Prudic et al., 1996; Trivedi et al., 2006). Further, the literature around the Maudsley Staging Method (MSM) for TRD demonstrates that a higher level of treatment resistance predicts poorer outcomes (Fekadu et al., 2009a, 2009b). Therefore, this is a population in which clinicians may consider the use of experimental treatments like intravenous (IV) ketamine (glutamatergic agent through N-methyl-D-aspartate (NMDA) receptor antagonism).
IV ketamine at subanesthetic doses has demonstrated effect sizes similar to ECT in TRD with a novel mechanism, for both unipolar and bipolar depression (Coyle and Laws, 2015; Zarate Jr et al., 2012). It has also yielded exciting anti-suicidal effects independent of anxiolytic and antidepressant effects (Ballard et al., 2014; Wilkinson et al., 2018). However, the effectiveness of IV ketamine in non-research settings and with URD patients remains understudied.
Given the current experimental nature of ketamine treatment, it would be ideal to collect biomarkers of response that would provide knowledge about which particular patients are more likely to respond. Until now, most of the biomarker research has been done in single infusion ketamine treatments. In search of symptoms of depression to stratify the depression phenotype that may respond to IV ketamine, evidence exists for anhedonia, anxiety/somatization, fatigue, and suicidal ideation (DiazGranados et al., 2010; Ionescu et al., 2014; Lally et al., 2014; Reinstatler and Youssef, 2015; Saligan et al., 2016). As for baseline sociodemographic variables, family history of an alcohol use disorder in a first degree relative (FHA) has been reported to be a clinical predictor of effectiveness, and this finding has been replicated (Luckenbaugh et al., 2012). In addition, a higher body mass index (BMI) and early response have been linked to initial and sustained response (Murrough et al., 2013b; Niciu et al., 2014). Alcoholism and higher BMI have been implicated in inflammation, which gives further support to ketamine’s theorized mechanism of action being anti-inflammatory and affecting synaptogenesis (Abdallah et al., 2016; Kadriu et al., 2017; Kiraly et al., 2017; Machado-Vleira et al., 2017; Shelton and Miller, 2011; Wang et al., 2010). The current literature requires further replication, and combining this information with other modalities may increase the predictive accuracy.
This study aims to measure the response and remission rates of a six-infusion course of ketamine. Additionally, it aims to support previous findings of clinical predictors of effectiveness to IV ketamine in a clinical setting of URD patients.
Methods
Database collection
Data were collected from all patients who received ketamine at the Grey Nuns Community Hospital or Misericordia Community Hospital for depression from the inaugural patient on 13 May 2015–31 December 2016, retrospectively through pharmacy records. It was deemed a priori that 50 subjects were sufficient for the proposed statistical analysis. One patient had a significant response by clinician notes but did not complete rating scales, so was not included. Four patients had no response based on clinical notes and did not complete end rating scales, and were included in the study as non-responders. An electronic database was created and information from electronic outpatient charts, paper inpatient charts, and paper outpatient charts were input. All admission and discharge summaries in Edmonton have a standardized format, which allowed for extraction of past and present medical diagnoses, family history of addiction and mental illness, and history of substance use. Demographics, BMI, rating scales, and side effects from tracking sheets were extracted from nursing protocols before and during the infusions. Laboratory results, MSM scores, and past and present psychopharmacology use were extracted from a combination of all sources available. Personality and Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) diagnostic information were collected only if the words ‘disorder’ or ‘traits’ were ever documented in the ‘diagnoses’ section of any of the sources. Some patients underwent more than six treatments of ketamine, but no data were collected beyond the sixth post-ketamine rating scale. Ethical approval and a waiver of consent were provided by the University of Alberta Research Ethics Board and the Covenant Health Research Ethics Board.
Inclusion criteria
Inpatients or outpatients who satisfied three out of four criteria were permitted to be given IV ketamine and all were in this study. The criteria used were: (a) a diagnosis of a major depressive episode (unipolar or bipolar) determined by usual standard of care clinical opinion over years of observation, (b) refractory (defined by clinician) to pharmacological treatment by at least five psychotropic medications for treating a mood disorder, (c) refractory (underwent at least six ECT treatments without adequate response, defined by clinician) to, or not suitable for, ECT (not including refusal due to preference), and (d) acutely suicidal.
Exclusion criteria
The exclusion criteria used included patients with active psychosis, drug or alcohol abuse/dependence, dementia/delirium, a significant personality disorder believed to be the primary issue, a significant unstable medical condition, pregnancy, dissociative identity disorder, a history of allergic reaction to ketamine, or a history of any severe adverse reaction to ketamine. There were no suggestions to discontinue any medications through the study period and no specific medication classes were excluded. Further, substance use disorders that were in remission and past use of ketamine or phencyclidine were not excluded.
Administration of IV ketamine
A baseline assessment by a physician included a physical examination, blood work (complete blood count (CBC), electrolytes, aspartate transaminase (AST), alanine transaminase (ALT), gamma-glutamyl transpeptidase (GGT), thyroid-stimulating hormone (TSH)), an electrocardiogram, a urine drug screen 24 h before if deemed appropriate, and a medical consult when necessary. After written, informed consent was received, IV ketamine was administered in the inpatient unit or in the recovery room of the hospital by a nurse at a dose of 0.5 mg/kg over 40 min (Berman et al., 2000). A physician was on site during the procedure. Monitoring included measurement of oxygen saturation, blood pressure, and heart rate, with vital signs taken pre-, mid-, and immediately post-infusion, as well as pre-discharge. Infusions were repeated 2–3 times per week with a recommended maximum of six infusions. If side effects occurred during the infusion, the clinician had options to slow down the rate of the infusion, intervene with medications (low dose quetiapine and/or lorazepam), stop the infusion, or continue with close observation.
Rating scales
At baseline, one or more of the following scales were used: the Montgomery Asberg Depression Rating Scale (MADRS), the Beck Depression Inventory-I or –II (BDI-I or BDI-II), the Hamilton Rating Scale for Depression 17 or 21 (HRSD-17 or HRSD-21), and the Brief Psychiatric Rating Scale (BPRS). The MADRS and HRSD-17 were used as a self-rated scale so were only used for baseline symptomatology information. All other scales were used as recommended (Beck et al., 1961, 1996; Hamilton, 1960; Montgomery and Asberg, 1979; Overall and Gorham, 1962).
The frequency and type of rating scale administered was left to the clinician’s discretion, with a suggestion to administer rating scales at least at baseline, post-treatment one, post-treatment three, and on completion. When rating scales were given post treatment, the timing of administration was not standardized, but typically they were given at least four hours post-treatment, which extends past the half-life of IV ketamine.
A side effect tracking scale was uniquely created for this patient population based on known short term side effects at the initiation of the treatment (see Supplementary Material Table 1) (Serafini et al., 2014). Nursing staff were instructed to fill out the tracking sheet at least three times between initiation and the end of the recovery period. Notes were made if the patient experienced any side effects (categorized as ‘mild’), side effects requiring decreasing the rate of infusion or requiring intervention (categorized as ‘moderate’), or side effects requiring premature stoppage of the infusion (categorized as ‘severe’).
Statistical analysis
Clinical and demographic characteristics at baseline were compared between responder and non-responder groups using independent t-tests. Response was defined as a 50% reduction in BDI-I, BDI-II, or HRSD-21 between baseline and any time-point during treatment. Remission was defined by accepted criteria for each scale (Beck et al., 1961, 1996; Hamilton, 1960).
Logistic regression analyses all involved a dependent variable of response and were repeated with remission as the dependent variable. Three separate logistic regression calculations were done to mitigate type 2 errors.
Categorical independent variables of age (>50 and ⩽50), gender, FHA, suicidality (zero on any scale or other), anxiety (zero or one versus two or three on any scale), unipolar versus bipolar depression, and anhedonia (zero or one versus two or three on any scale).
Continuous data independent variables of BMI, age, and MSM.
Categorical independent variables of patients on lamotrigine (glutamate release inhibitor and voltage-gated sodium channel blocker), benzodiazepines, and antipsychotics (first, second or third generation) during ketamine treatments.
Missing data were dealt with by excluding the patient from that analysis rather than using the mean.
Results
Baseline characteristics of the population demonstrated an average MSM TRD level of severe with low variance at 12.1 out of 15, in addition to being 90% ECT resistant and 86% psychotherapy resistant. All the patients except one were concomitantly on medication while receiving the treatment course. Diagnoses of Cluster B and C personality traits were given to a patient by clinician documentation in 44% and 48% of the population, respectively, and 64% of the population had a documented DSM-5 diagnosis of an anxiety disorder at least once in their lifetime.
Baseline characteristics of responders and non-responders were compared with independent t tests and z tests. Only ‘concurrent use of lamotrigine’ (p=0.015) was found to be statistically different between responders and non-responders at p<0.05, and bipolarity (p=0.080) was the only factor that was statistically different at p<0.1 (Table 1). A full list of medications and the total number of patients concurrently and previously taking the medications is included in Supplementary Material Table 2.
Baseline demographic and clinical data of patients receiving intravenous ketamine, separated by total, responders and non-responders.
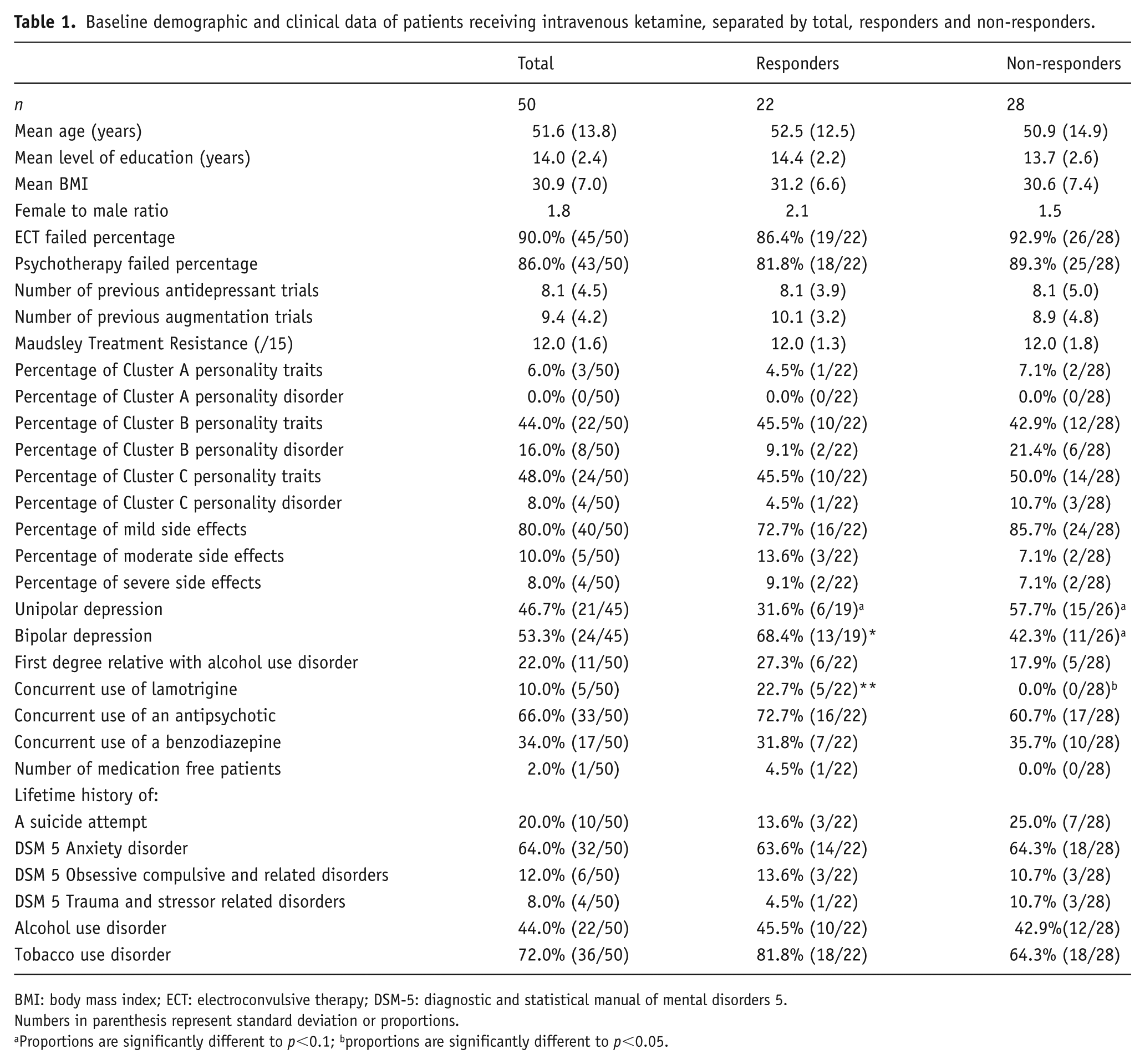
BMI: body mass index; ECT: electroconvulsive therapy; DSM-5: diagnostic and statistical manual of mental disorders 5.
Numbers in parenthesis represent standard deviation or proportions.
Proportions are significantly different to p<0.1; bproportions are significantly different to p<0.05.
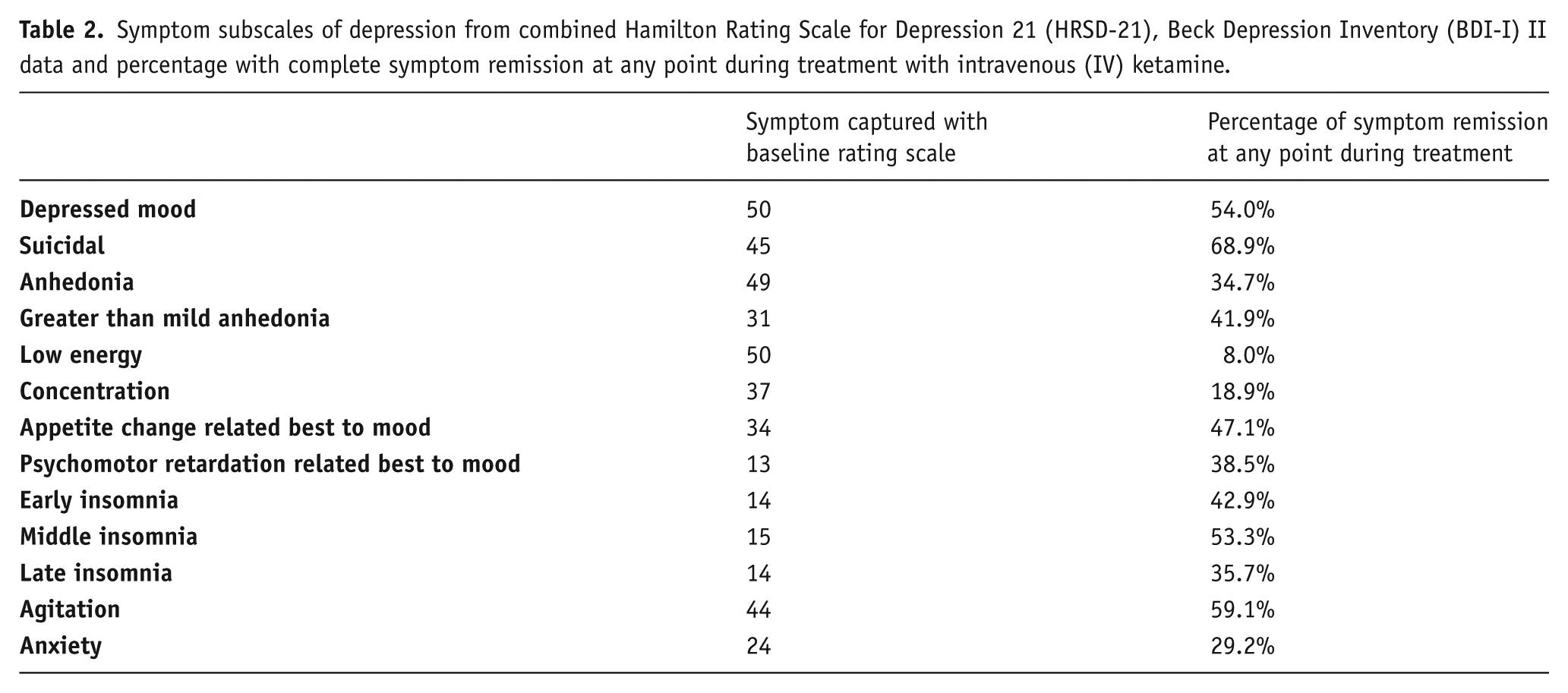
The response rate in this population was 44% and the remittance rate was 16%. There were no instances where a patient responded during the treatment and did not sustain their response when followed to the end of treatment, which was substantiated by clinical notes throughout the study period. Specific subscales followed for remission over the course of treatment found that 54.0% and 68.9% of patients who were at least mildly depressed or suicidal at baseline scored a zero on depressed mood and suicidality subscales, respectively, during treatment. Complete symptom remission percentages in other subscales are listed in Table 2.
Symptom subscales of depression from combined Hamilton Rating Scale for Depression 21 (HRSD-21), Beck Depression Inventory (BDI-I) II data and percentage with complete symptom remission at any point during treatment with intravenous (IV) ketamine.
Logistic regression on categorical data of age, gender, anxiety, anhedonia, bipolarity, FHA, and suicidality were investigated and at least moderate anhedonia at baseline and bipolar depression were seen as predictors in this regression model. The finding was more significant when the two factors were combined. When investigated alone, patients with at least moderate anhedonia at baseline were found to be 55% more likely to respond to IV ketamine (p=0.072, odds ratio (OR)=1.21) and the presence of bipolar depression was found to be 54% more likely to respond (p=0.087, OR=1.18). Together, patients with a diagnosis of bipolar depression and at least moderate anhedonia at baseline were 73% more likely to respond to IV ketamine (p=0.035, OR=3.03). (Table 3)
Results of logistic regression calculations versus the dependent variable of response to intravenous ketamine treatment. (a) Categorical independent variable calculations; (b) single predictor logistic regression for anhedonia; (c) single predictor logistic regression for polarity of depression; (d) two predictor logistic regression for polarity of depression and anhedonia.
(a)
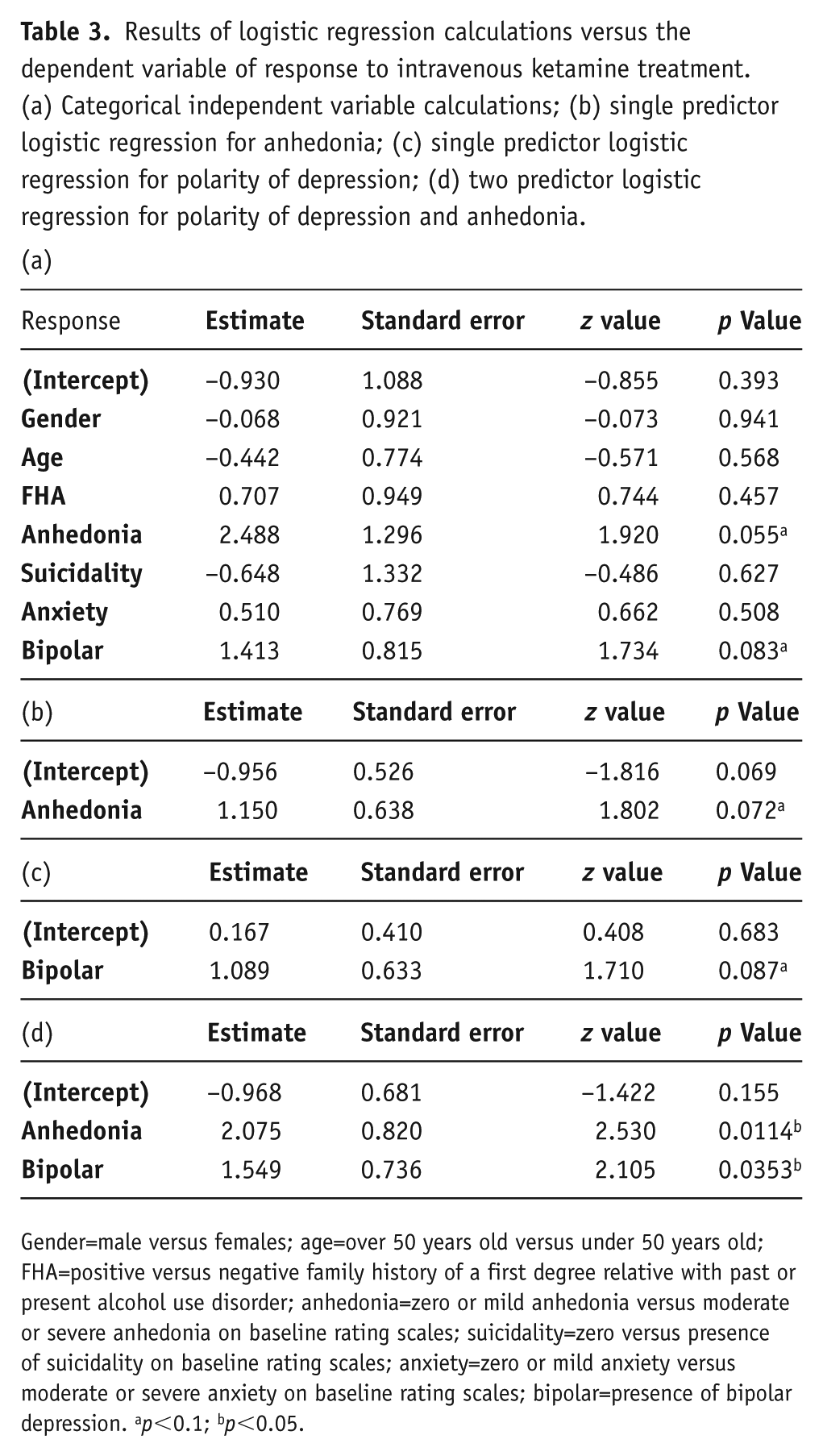
Gender=male versus females; age=over 50 years old versus under 50 years old; FHA=positive versus negative family history of a first degree relative with past or present alcohol use disorder; anhedonia=zero or mild anhedonia versus moderate or severe anhedonia on baseline rating scales; suicidality=zero versus presence of suicidality on baseline rating scales; anxiety=zero or mild anxiety versus moderate or severe anxiety on baseline rating scales; bipolar=presence of bipolar depression. ap<0.1; bp<0.05.
Logistic regression was done to investigate clinical predictors of effectiveness for continuous variables of BMI, MSM, and age as well as with presence or absence of benzodiazepines and antipsychotics during treatment, and no statistical significance was found (Supplementary Material Table 3). All logistic regression calculations were repeated with remission as the dependent variable and no statistical significant clinical predictors of remission were found (Supplementary Material Table 4).
Discussion
This retrospective, database study in a clinical setting with 50 patients represents the highest level of TRD that has been studied for IV ketamine. In this population, 90% have failed ECT, which is one of the most effective treatments for TRD (UK ECT Review Group, 2003). When considering the growing number of IV ketamine clinics for TRD in North America, information on this population adds applicability to the literature (Yan, 2016). The heterogeneity and complexity of these patients make them difficult to study in clinical research settings, as was seen in our population with a high proportion of comorbid personality traits, comorbid anxiety disorders, and a mixture of unipolar and bipolar depressed patients.
A higher level of treatment resistance infers a poor prognosis (Fekadu et al., 2009a, 2009b; Trivedi et al., 2006). The response and remittance rates that were achieved are therefore very encouraging to a population that is underserved. As expected with a higher level of treatment resistance, the remission rate of 16% was lower than the Serafini et al. (2014) systemic review findings of 26–67%. The response rate of 44% is also consistent with the lower end of the Coyle and Laws (2015) meta-analysis results of a 40–90% response rate. In terms of suicidality, this population responded to ketamine at a rate superior to the Price et al. (2014) study. When measuring the percentage of the population that scored a zero on a suicidality rating subscale, Price et al. (2014) reported 53%, whereas this study yielded a 68% remission at any point in treatment. Further, 55% of the population remitted in the depressed mood subscale of a rating scale at some point in the study, and this correlates with the positive clinical opinion of ketamine effectiveness. Also, this rate is much higher than the remission rate. This brings up the possibility that IV ketamine has a differential effect on different subscales of depression. Ballard et al. (2018) attempted to address the heterogeneity of depression and the treatment response to ketamine by way of an exploratory factor analysis on 119 patients involved in ketamine clinical trials. Their results supported the contention that a differential symptom response may exist and that measuring specific factors found across rating scales may be more accurate in identifying ketamine treatment response than conventional rating scales.
Given the heterogeneity in the study population and the lack of biomarkers, it could be hypothesized that the sensitivity of the study to find clinical predictors of effectiveness to ketamine would be low. Due to the sample size, the percentage of some of the predictors present were of low frequency, and this limits the ability to assess many of the predictors with sufficient power. Nevertheless, there was evidence for at least moderate anhedonia as a single clinical predictor of effectiveness. This is especially encouraging as treatment for anhedonia is an unmet need in psychiatry. It is known that anhedonia is a negative prognostic factor for depression, as standard antidepressants do little to treat anhedonia and anhedonia is a major risk factor for suicide (Fawcett et al., 1990; McMakin et al., 2012; Nutt et al., 2007; Spijker et al., 2001; Uher et al., 2012). Growing evidence is supporting the role of anhedonia as a potential clinical predictor of effectiveness to ketamine. Lally et al. (2014) demonstrated, in a randomized, placebo-controlled, double-blind trial of single infusion ketamine to 36 patients with bipolar depression, that ketamine had anti-anhedonic effects and that these effects were related to action at the anterior cingulate cortex. Anhedonia has been localized to the anterior cingulate cortex in resting state functional magnetic resonance imaging (fMRI), electroencephalography and deep brain stimulation studies as well (Mayberg et al., 1997; McInerney et al., 2017; Wacker et al., 2009). Among other roles, the anterior cingulate cortex functions in error detection, task shifting, conflict monitoring and reward based learning (Bush et al., 2000, 2002). In terms of clinical predictors of effectiveness, this was also seen in fMRI studies showing that fearful face stimuli elicit responses in the anterior cingulate cortex. Dysfunction in the anterior cingulate cortex at baseline significantly predicted patient response to single infusions of ketamine four hours post-treatment (Salvadore et al., 2009).
The exact mechanism of action of ketamine’s anti-anhedonic effects remains unknown. The current hypothesis of ketamine’s antidepressive mechanism of action is that of synaptogenesis through the glutamate pathway (Duman, 2014; Li et al., 2010). Anhedonia is in part related to pathology in the reward system, motivation, rumination and distraction, leading to a difficulty in managing negative thoughts and feelings (Cohen et al., 2012; Lally et al., 2014; Lehmann et al., 2016; Wacker et al., 2009). The negative, self-referential, ruminative aspect of MDD has been related to an increased resting state functional activity and a decreased reactivity in the default mode network (Hamilton et al., 2011). Lehmann et al. (2016) demonstrated with fMRI responsive to negative face stimuli and treatment with single infusion ketamine, that ketamine was effective and had action in the anterior cingulate cortex, perhaps normalizing neuronal connection. Further, they found patients with less ability to distract from negative experiences at baseline had more pronounced findings in the anterior cingulate cortex.
An interesting yet underpowered finding of this study was that of the five patients on lamotrigine throughout treatment, all responded to IV ketamine. Theoretically, lamotrigine functions to inhibit the release of glutamate which is opposed to the proposed mechanism of action of ketamine (Doyle et al., 2013; Duman, 2014). Anand et al. (2000) found that lamotrigine attenuated dissociation and increased immediate mood elevating properties. However, Mathew et al. (2010) administered lamotrigine 300 mg versus a placebo two hours prior to IV ketamine 0.5 mg/kg over 40 min and discovered no significant difference in side effects or antidepressant effect. Our study did not quantify dissociation, but the effect seen gives support to lamotrigine as a possible adjunct to IV ketamine.
This study gave evidence for bipolarity as a predictive factor to response, which has not been previously described (Pennybaker et al., 2017; Rong et al., 2018). However, it is in keeping with consistent evidence that IV ketamine has a robust effect on bipolar depression and bipolar depression suicidality, which is encouraging as it is a patient population with few available treatments options and often a large burden of illness (Coyle and Laws, 2015; Grunebaum et al., 2017; Kennedy et al., 2016; Zarate et al., 2012). A meta-analysis by Coyle and Laws (2015) investigated polarity and treatment effect and found that effect sizes were not significantly different four hours post-treatment, but IV ketamine effect sizes on bipolar depression were larger after seven days. This extended effect may have been captured and may have been seen as an additive effect in the multiple doses given over 2–3 weeks in this study. A limitation to this finding is that the diagnosis was based on a standard of care diagnosis by a clinician and not by a standardized diagnostic tool. However, the standard of care diagnosis in this real-world population has increased accuracy due to lengthy longitudinal relationships with clinicians through many previous treatment failures. Further, given the sample size, a specific study of polarity of depression as a clinical predictor of response is warranted to confirm these findings.
This study has also added to the majority of evidence that ketamine is a well-tolerated treatment in the short term. Patients often described a pleasant but abnormal sensation (82% with mild side effects) that did not require treatment. Only four out of 50 patients suffered side effects that resulted in aborted treatment. This is comparable to the Wan et al. (2015) study which reported a dropout rate of 1.9–3.0%.
Despite this study’s strength in its applicability, there are limitations due to its design. Confounders are an issue for post-hoc analysis without controls. Although the response rate and effect size previously achieved in the literature are robust, a large active placebo effect still exists, with one study documenting a 28% response rate with midazolam (Murrough et al., 2013a). The clinical setting allowed for different medication combinations and for many different concomitant psychosocial interventions that may have confounded the study. The placebo effect is mitigated in this sample to some extent as most of the other interventions were continuations of previous interventions that the patient had responded to minimally, if at all, over many years.
The findings reported here should be replicated with larger clinical sample sizes, and this could be accomplished with similar logistic regression techniques through national and international data registries (Malhi et al., 2016). As biomarker research continues to progress, clinical indicators could be combined with biomarkers to make composite clinical decision making tools (Kessler, 2018). For example, the advancements of fMRI techniques have produced exciting findings that may be able to stratify depression phenotypes with the goal of giving more appropriate treatments sooner. Drysdale et al. (2017) studied over 1000 depressed patients with fMRI and were able to subdivide patients into four ‘biotypes’ of depression. They also found that one biotype was more responsive to repetitive transcranial magnetic stimulation (rTMS) than the others. Further, Abdallah et al. (2017) demonstrated that MDD patients had a distinctly dysfunctional global brain connectivity with global signal regression parameters shown through fMRI techniques in the prefrontal cortex, posterior cingulate, precuneus, lingual gyrus, and cerebellum. This pattern normalized with ketamine treatment. With a connection to more feasible clinical measures, this is a step towards personalized medicine and could prevent the many years of functionally disabling depression we see in the treatment resistant depression population (Kessler, 2012).
Conclusion
In a clinical setting, a course of six infusions of ketamine showed effectiveness in a complex, severely treatment-resistant, depressed population on multiple concurrent medications. Given the large unmet need of this patient population, the response rate seen in ketamine is encouraging. An international registry of all patients undergoing IV ketamine has been advocated for by the American Psychiatric Association Council Research Task Force on Novel Biomarkers and Treatments. Such a registry would certainly build on this study and further the applicability and effectiveness data of IV ketamine for the treatment of URD (Sanacora et al., 2017). This study gives support to previous findings that depression with at least moderate anhedonia is a clinical predictor of effectiveness for IV ketamine. Continued study is warranted regarding clinical predictors of effectiveness to ketamine treatment and feasible clinical decision-making tools to avoid years of disability and failed antidepressant trials, and enhance the quality of life for these patients.
Supplemental Material
JOP793104_Supplementary_Material – Supplemental material for Rapid effectiveness of intravenous ketamine for ultraresistant depression in a clinical setting and evidence for baseline anhedonia and bipolarity as clinical predictors of effectiveness
Supplemental material, JOP793104_Supplementary_Material for Rapid effectiveness of intravenous ketamine for ultraresistant depression in a clinical setting and evidence for baseline anhedonia and bipolarity as clinical predictors of effectiveness by Rejish K Thomas, Glen Baker, John Lind and Serdar Dursun in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funds were provided by the University of Alberta.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.