
Abstract
Background/Aim:
The aim of the current study was to review drug harms as they occur in Australia using the Multi-criteria Decision Analysis (MCDA) methodology adopted in earlier studies in other jurisdictions.
Method:
A facilitated workshop with 25 experts from across Australia, was held to score 22 drugs on 16 criteria: 9 related to harms that a drug produces in the individual and 7 to harms to others. Participants were guided by facilitators through the methodology and principles of MCDA. In open discussion, each drug was scored on each criterion. The criteria were then weighted using a process of swing weighting. Scoring was captured in MCDA software tool.
Results:
MCDA modelling showed the most harmful substances to users were fentanyls (part score 50), heroin (part score 45) and crystal methamphetamine (part score 42). The most harmful substances to others were alcohol (part score 41), crystal methamphetamine (part score 24) and cigarettes/tobacco (part score 14). Overall, alcohol was the most harmful drug when harm to users and harm to others was combined. A supplementary analysis took into consideration the prevalence of each substance in Australia. Alcohol was again ranked the most harmful substance overall, followed by cigarettes, crystal methamphetamine, cannabis, heroin and pharmaceutical opioids.
Conclusions:
The results of this study make an important contribution to the emerging international picture of drug harms. They highlight the persistent and pervasive harms caused by alcohol. Policy implications and recommendations are discussed. Policies to reduce harm from alcohol and methamphetamine should be a priority.
Introduction
The international landscape in relation to drugs is constantly changing. There are concerns currently about the escalating availability of new psychoactive drugs, crystal methamphetamine and high potency opioids – particularly fentanyls – in Western countries and tramadol in Africa and Asia (World Drug Report, 2018). World drug markets are expanding, with supply higher than ever recorded and geographic spread into regions previously not affected. Not surprisingly, drug treatment services globally are unable to keep pace with need, and health care systems and law enforcement agencies are under strain.
If alcohol and drug policies are to be efficient and limit the burden of the increasing prevalence of drug use, they must focus on the drugs causing the greatest harm in the community. Assessing such harm has been approached in a variety of ways. Most commonly, harms incurred by an individual through drug use are examined, and include methodologies that focus on Margin of Exposure (MOE) (European Food Safety Authority, 2005, p. 282; Lachenmeier and Rehm, 2015), Burden of Disease (BOD) (Degenhardt et al., 2013; Griswold et al., 2018; World Bank, 1993), and dependence liability (Anthony et al., 1994; United Nations Office on Drugs and Crime, 1972, p. 4). An alternative approach has been to put a monetary value on the social and economic costs associated with the use of particular drugs, including costs related to judiciary and law enforcement, healthcare, loss of productivity, and road traffic accidents (Collins and Lapsley, 2008; Miller and Hendrie, 2008; Tait et al., 2018). While no single approach to assess harms related to drug use exists that encompasses both individual and societal costs, Multi Criteria Decision Analysis (MCDA), a decision support tool for consensus building and collaborative problem-solving, has been adopted to examine this issue in a number of countries, as it has been used successfully in a range of contexts beyond health or social harms. Examples include nuclear waste management in the United Kingdom, climate change by the United Nations, and in resource management in South America (Soma, 2003; Thokala et al., 2016; United Nations Framework for Climate Change, 2002). A major advantage of MCDA is that it brings together experts who contribute knowledge and understanding from a range of perspectives on a complex issue; especially where there are conflicting experiences or perspectives of stakeholders.
The aim of the current study was to review drug harms as they occur in Australia using similar MCDA methodology adopted in other jurisdictions, so as to ensure comparability of results. As such, the findings contribute to a series of investigations undertaken around the globe using MCDA to evaluate the harms associated with particular types of drug use. The initial study occurred in the United Kingdom (UK) in 2010 (Nutt et al., 2010), followed by others in Europe (Nutt et al., 2014; Van Amsterdam et al., 2010, 2015a). A study in South Africa focused on harms of nicotine based products (publication pending). We report on the results of this MCDA modelling for Australia as a contribution to the emerging international picture of drug harms across the world.
Methods
Study design
A facilitated workshop with 25 experts from across Australia, representing a range of professional domains, was held in April 2018, working together to input data and judgment into the MCDA model. The group was specifically convened to bring together not only research expertise, but also practice wisdom, and included a diverse range of sectors from across the community. Participants were selected to allow the broadest possible range of perspectives and opinions, reflected in their geographic spread across Australia and particular areas of expertise, encompassing treatment services, addiction medicine, psychiatry, pain medicine, academia and research, policy and planning, children and youth, aboriginal health, homeless services, judiciary, emergency services and police (Table 1). All participants provided independent perspectives and no conflicts of interest were declared. The process was facilitated by three independent, experienced individuals including the first author of the UK MCDA exercise (DN) and two specialists in MCDA (PS and PG) who ensured a consistent and rigorous process was followed and consensus was achieved. The facilitators did not take any part in the scoring.
Expert panel membership and organisational affiliation.
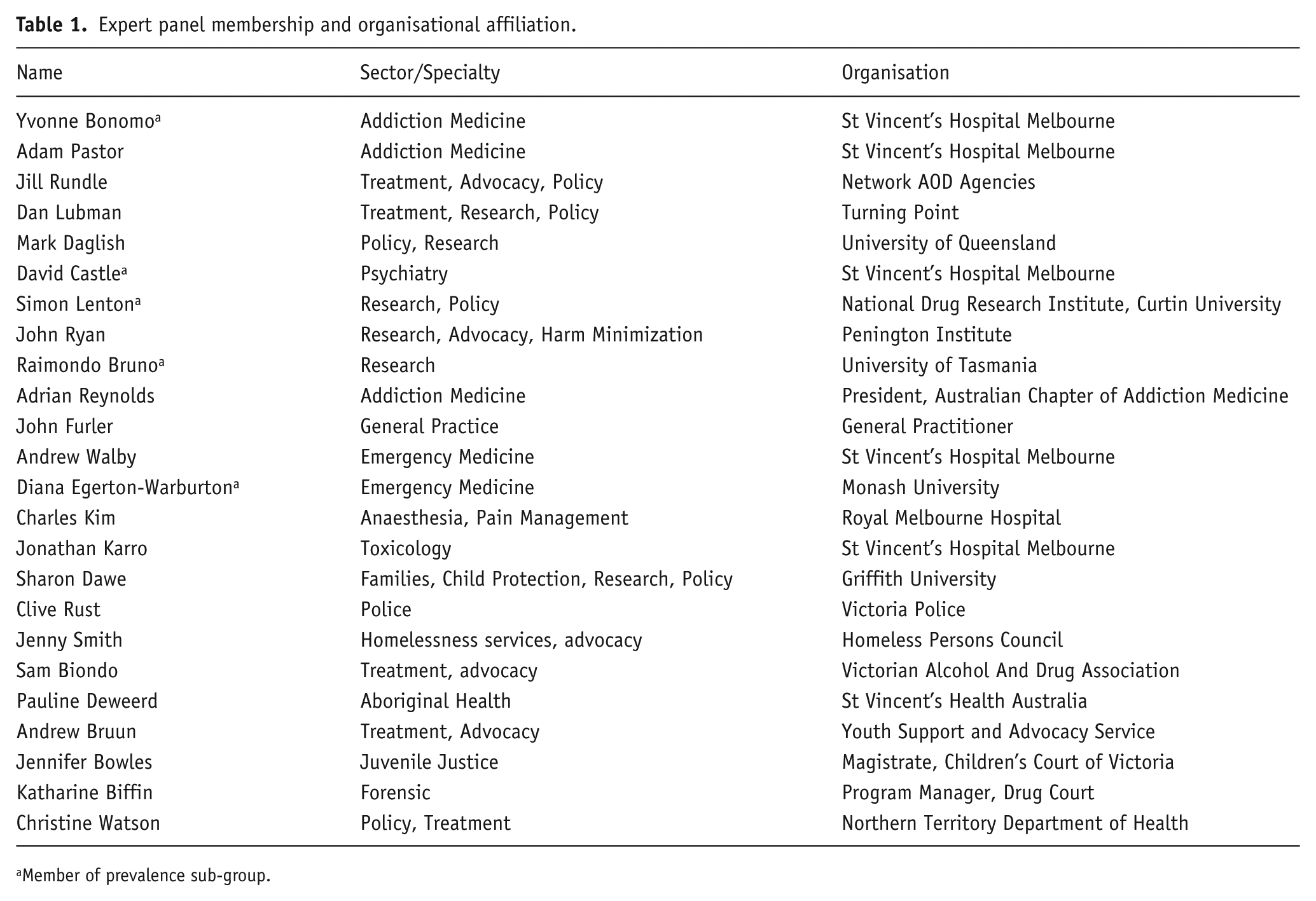
Member of prevalence sub-group.
The workshop followed standard decision conferencing processes, which have been previously reported (Nutt et al., 2010). In summary:
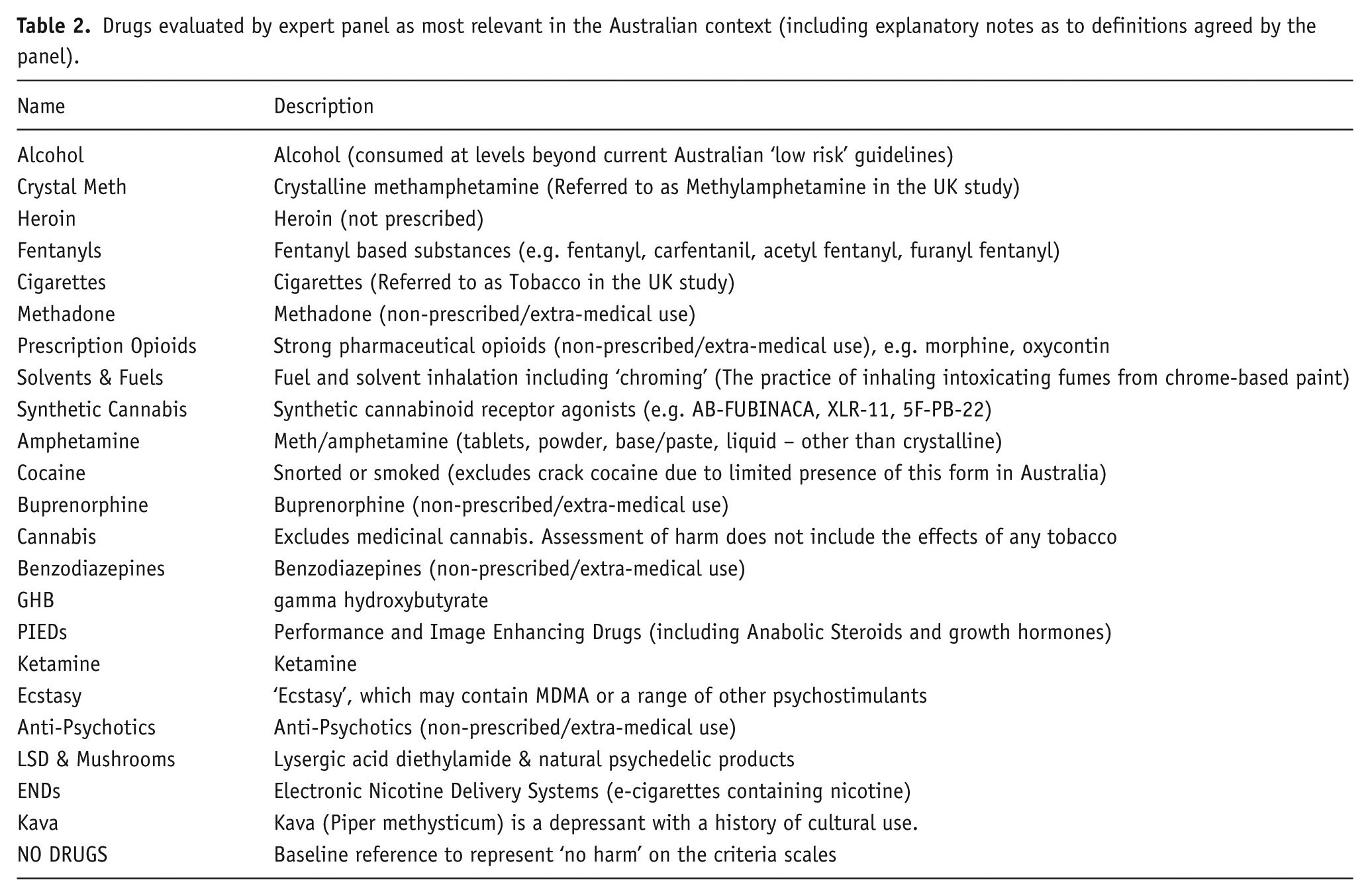
1. The substances to be evaluated were reviewed and confirmed by participants. The starting list was the same as that used in the UK study (Nutt et al., 2010) adapted to include substances most relevant to the current Australian context (Table 2);
Drugs evaluated by expert panel as most relevant in the Australian context (including explanatory notes as to definitions agreed by the panel).
2. The criteria for harm employed in the UK MCDA (Nutt et al., 2010) were reviewed and adopted as applicable to the Australian context. The criteria fall into two groups, namely:
Harm to Users – the effect of misuse of a given drug to the average user, considering the harm to a single user (i.e. not taking prevalence of use of the drug into account) and including the harms associated with the impact of mechanisms of control, such as policing, criminalisation, etc.;
Harm to Others – the effect of misuse of that drug on people other than the drug user themselves (such as their family, community, etc.). These criteria consider the total harm to others in Australia (physical/psychological and social) (Figure 1).
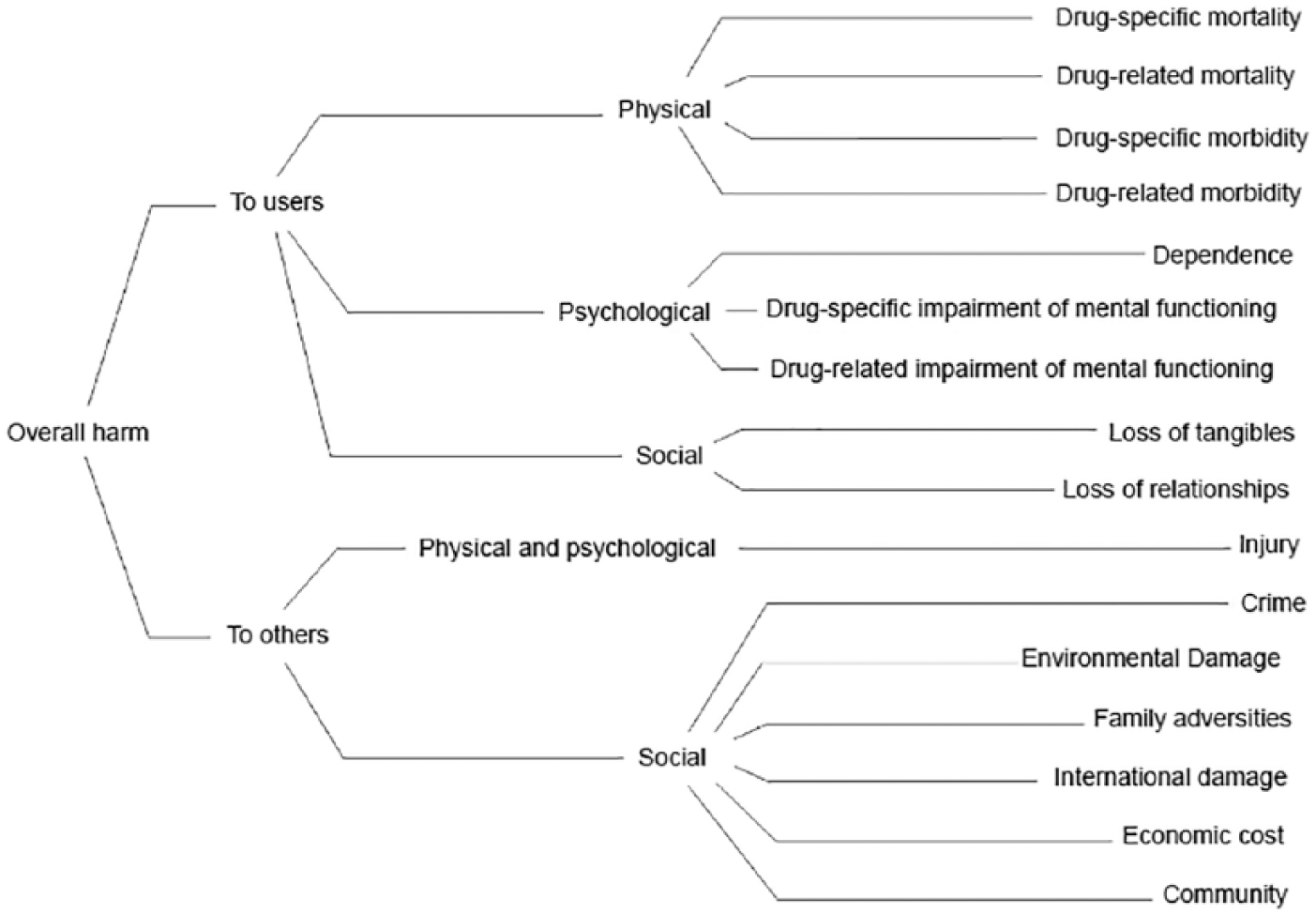
Evaluation criteria organised by harms to users and harms to others, and clustered under physical, psychological, and social effects.
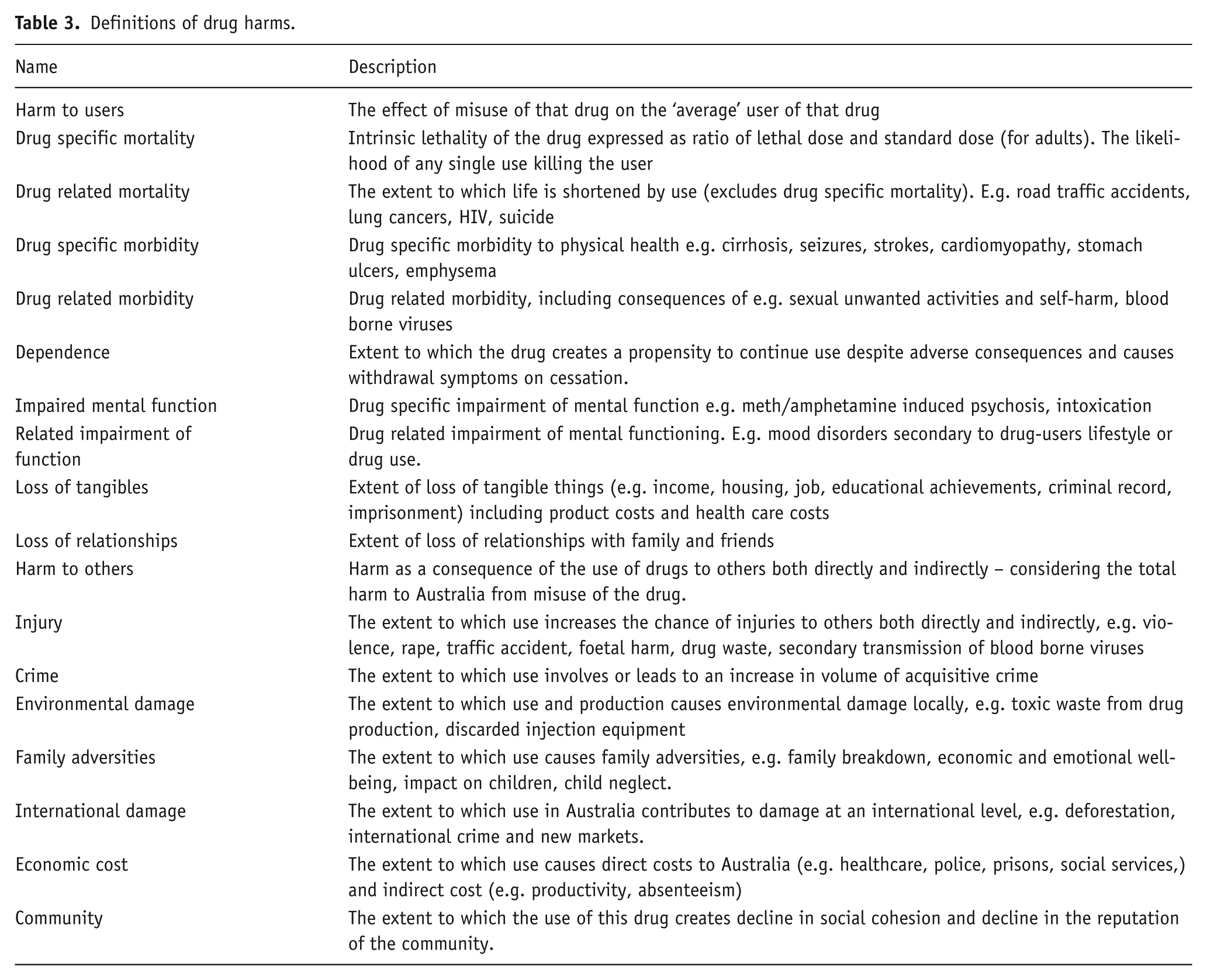
Definitions of harms are included in Table 3.
Definitions of drug harms.
3. In open discussion the drugs were ‘scored’ against the criteria – working through one criterion at a time, in the order of the list above. A process of ‘relative preference scoring’ was used: For each criterion, the participants debated and ranked all the drugs on the list in order of most harm to least harm (with ‘NO DRUGS’ being consistently assessed as least harm); The participants then debated the relative harm of each of the drugs, and ranked them on a scale from 0 to 100, where 0 represented ‘no harm’ and 100 represented ‘most harm’ against that criterion. For example, a drug which was assessed as half as harmful as the drug assessed as most harmful, would score 50; Scores were frequently re-visited and reviewed by the group with the facilitator to ensure consistency.
4. Criteria were then weighted using a process of ‘swing weighting’, and a ‘bottom up’ approach: First, all the ‘harm to users’ criteria were weighted against each other (swing weighting); Then, all the ‘harm to others’ criteria were weighted against each other (swing weighting); Finally, the highest weighted ‘to users’ criterion was weighted against the highest weighted ‘to others’ criterion (‘bottom up’). The result of attributing these weights was that the units of harm for each substance were equated. A final normalisation preserved the ratios of all weights but ensured that the weights on the criteria summed to 1.0. The weighting process enabled harm scores to be combined for each substance by adding their weighted scores.
5. All scores and weights were captured in the MCDA software tool used for other MCDA analyses – Catalyze Hiview 3® (http://www.catalyzeconsulting.com/software/hiview3/ accessed 12 October 2018).
During the Decision Conference, the participants noted these points of rationale and/or assumptions about specific drugs that impacted the assessment of harms:
Fentanyls – these are currently low prevalence in Australia, but it is expected they may become more prevalent; hence, they were included in the exercise;
Inhaled fuels – these are a particular issue in indigenous communities [for example sniffing of Avgas (aircraft fuel)];
Tobacco was considered only as ‘cigarettes’, with ENDs (electronic nicotine devices or ‘e-cigarettes’) being rated separately (note that ENDs were not legal at the time of the decision conference);
Cocaine – the ‘average user’ in Australia is generally of higher socio-economic status than the average user of other illicit substances, and most ‘average users’ do not inject the drug;
Prescription medications such as benzodiazepines, buprenorphine, methadone and antipsychotics referred to diverted drugs for ‘street’ use;
Each substance was assessed as if the user was using the substance alone, even when in practice it was acknowledged that multiple substances are frequently used together;
Possible transition (‘gateway’) effects were not considered.
A supplementary analysis incorporating the prevalence of use of each substance in the assessment of harm to users was also undertaken as this had been a criticism of previous studies (Caulkins et al., 2011). The National Drug Strategy Household Survey 2016 (NDSHS) (Claydon et al., 2017) covers most, but not all, of the substances considered. Where there was no NDSHS data, the group referenced other data to determine prevalence, using the NDSHS as starting points (Table 4). Scores on each of the ‘harm to individual users’ criteria were multiplied by prevalence. Results were then normalised to a 0–100 scale for each criterion. Because the combining of the scores on the individual criteria was achieved through a swing weighting process, the weights on these criteria also needed to be scaled to account for the impact of prevalence.
Prevalence data based on National Drug Strategy Household Survey.
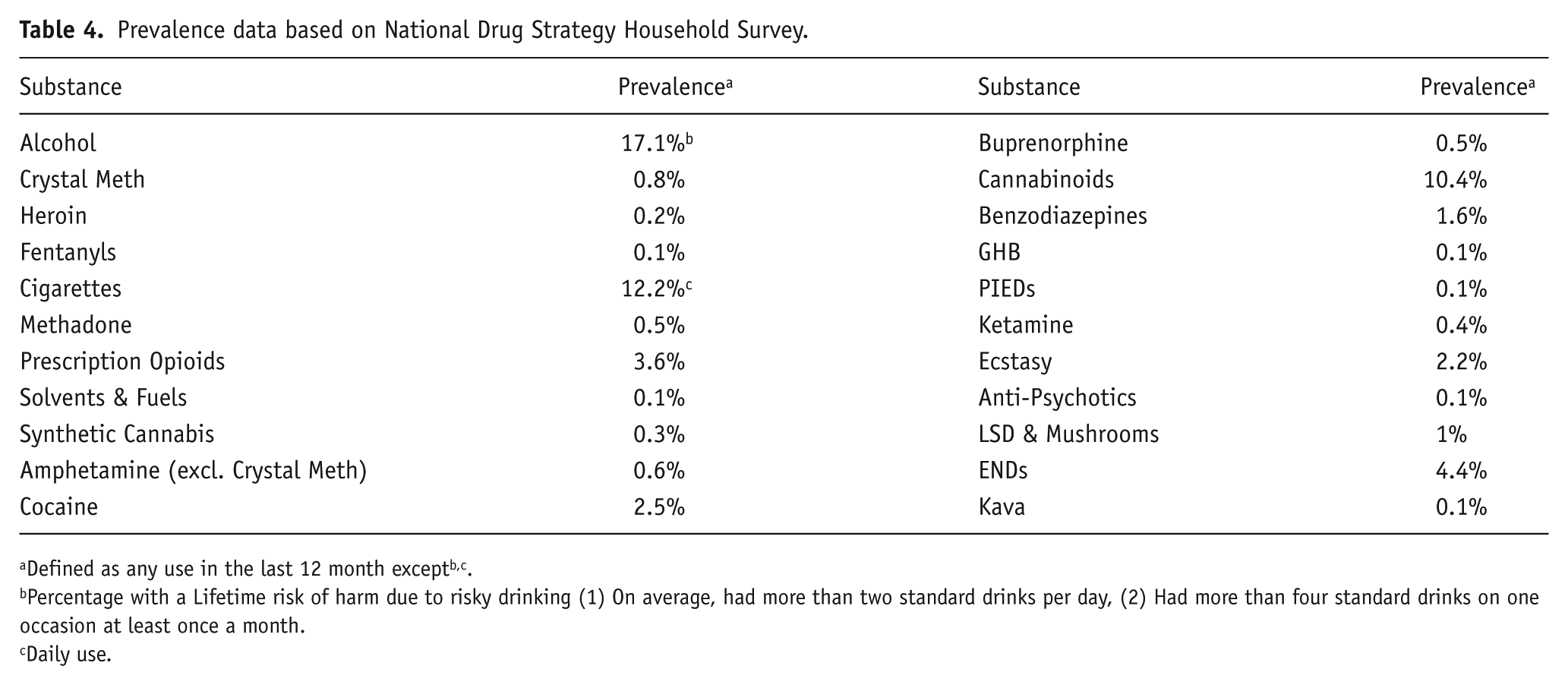
Defined as any use in the last 12 month exceptb,c.
Percentage with a Lifetime risk of harm due to risky drinking (1) On average, had more than two standard drinks per day, (2) Had more than four standard drinks on one occasion at least once a month.
Daily use.
Results
Figure 2 shows the total harm score for all the drugs and the part-score contributions to the total from the subgroups ‘harms to users’ and ‘harms to others’. The most harmful substances to users were fentanyls (part score 50), heroin (part score 45) and crystal methamphetamine (part score 42). The most harmful substances to others were alcohol (part score 41), crystal methamphetamine (part score 24) and cigarettes/tobacco (part score 14). When the two part-scores were combined, alcohol and crystal methamphetamine were the two most harmful substances followed by heroin, fentanyls and cigarettes/tobacco. The least harmful drugs were kava, ENDS, LSD and mushrooms, antipsychotics and ecstasy. Overall, alcohol was ranked the most harmful drug, with a combined score of 77.
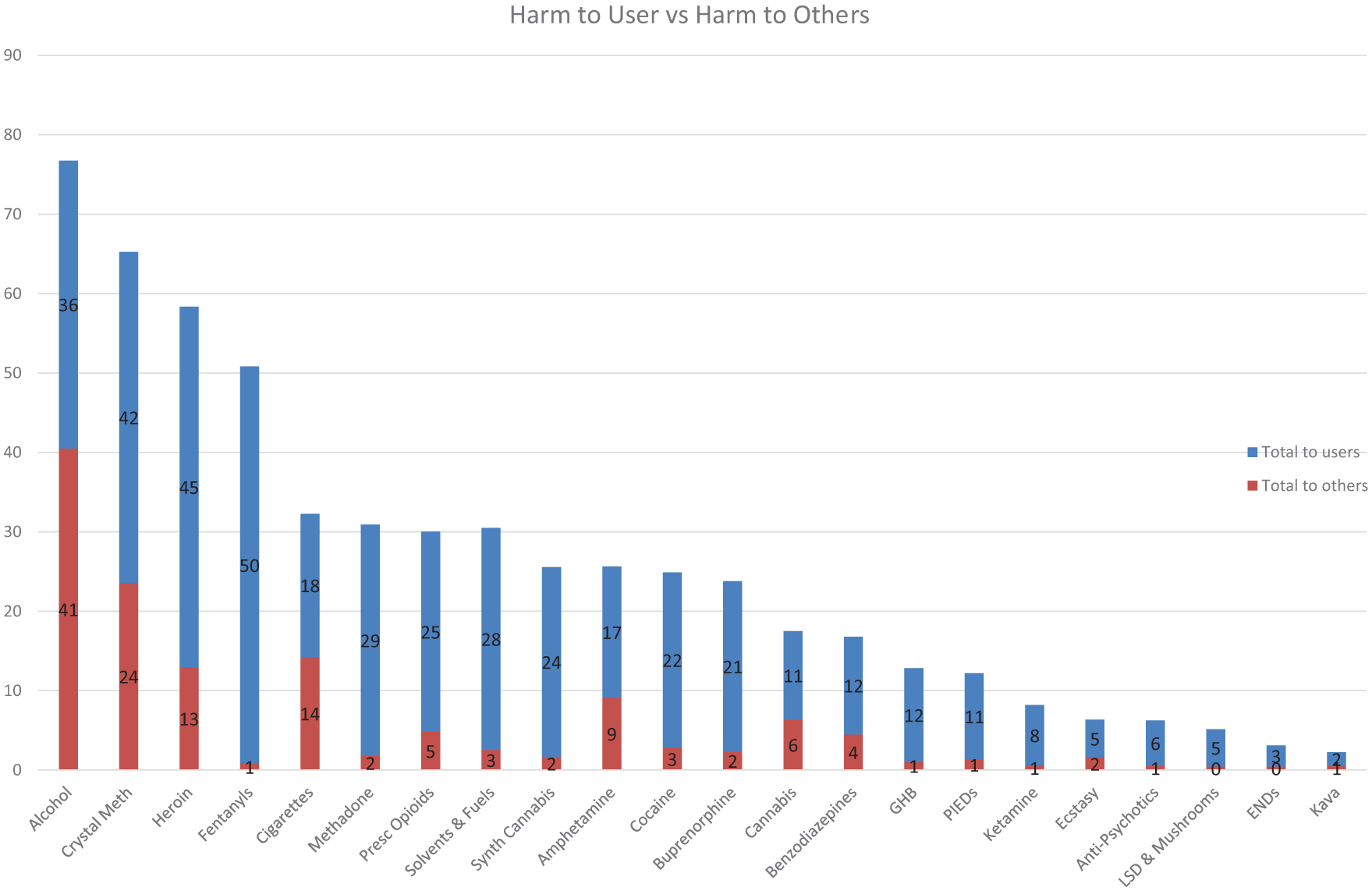
Contribution of harm to user and harm to others to overall harm.
Figure 3 shows the contributions that the part scores for each criterion made to the total score for each drug. Alcohol, the substance judged to be the most harmful overall with a score of 77, scored highly on economic costs, family adversity, injury, drug related morbidity and drug specific morbidity. The major contributors to the overall harm score of crystal methamphetamine were crime, injury, loss of relationships, loss of tangibles, drug specific morbidity and drug related morbidity. Tobacco was rated the fifth most harmful substance, scoring highly on economic costs and drug related morbidity and drug-related mortality. Drug-specific mortality contributed substantially to the overall harm score of heroin and fentanyls while economic cost contributed heavily to the overall harm score of cigarettes and alcohol.
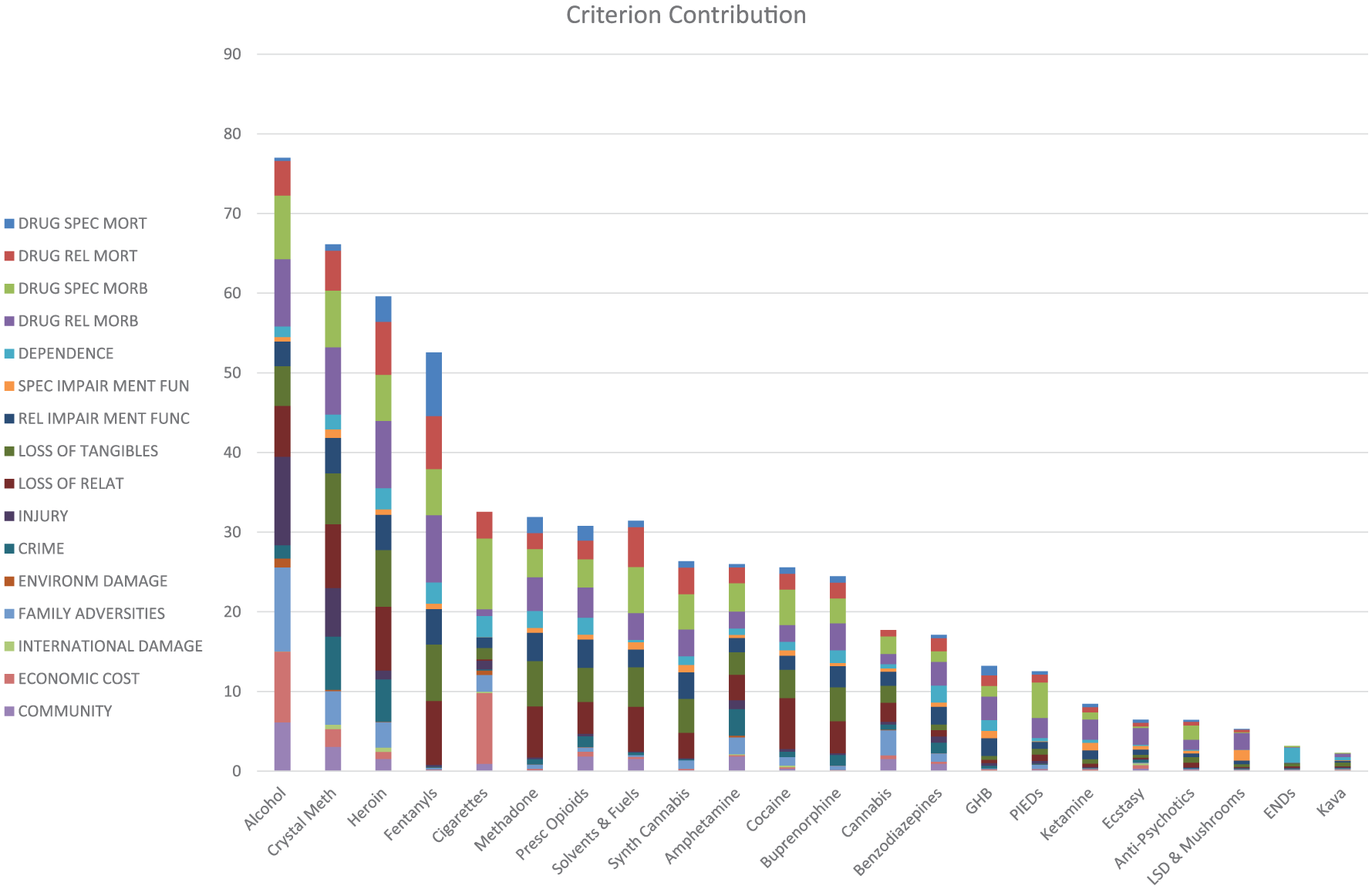
Contribution of criterion scores to overall harm.
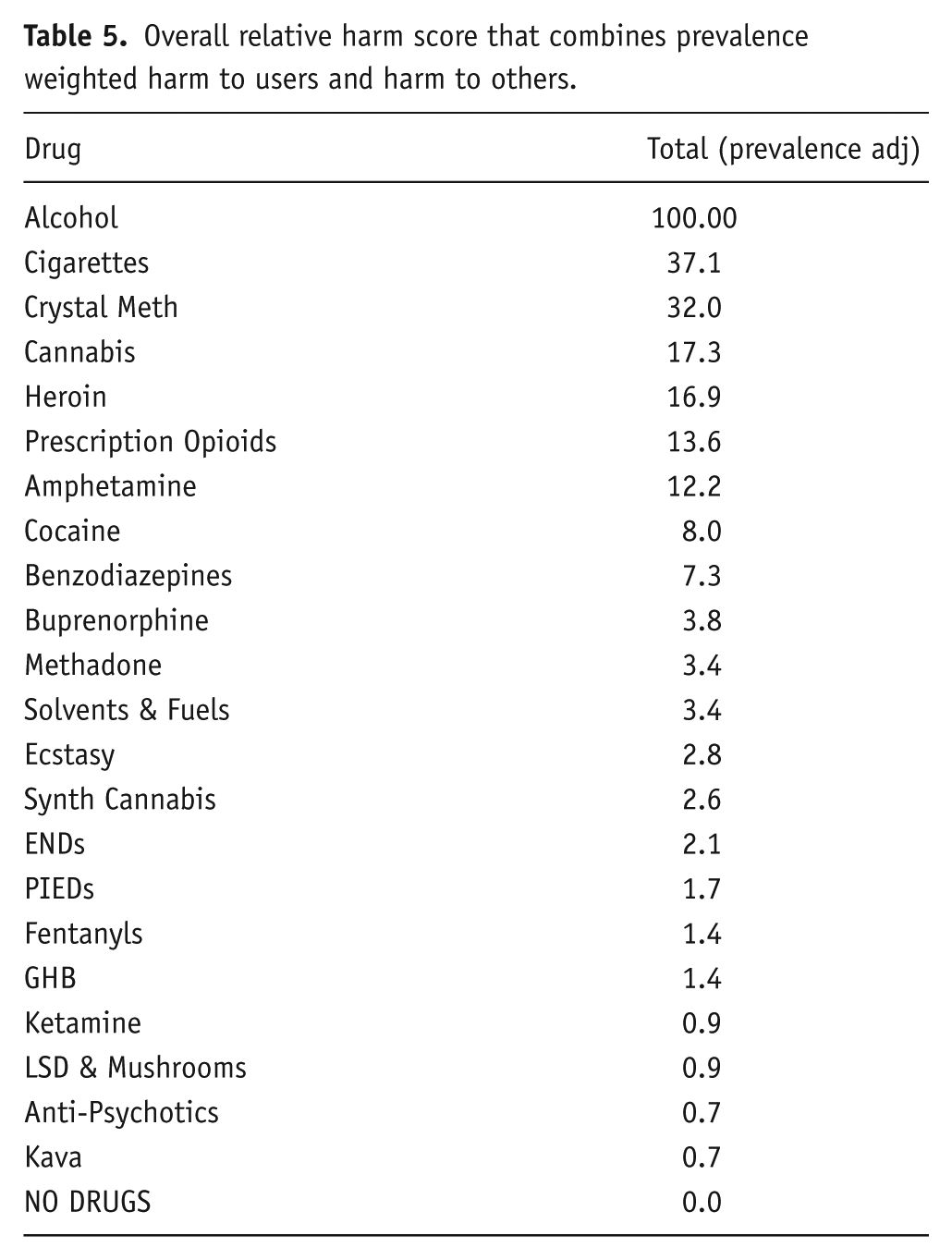
The scores from the supplementary analyses encompassing prevalence weighted harm to users, are shown in Table 5, normalised to 0 to 100 and sorted in decreasing harm. The top five most harmful drugs overall, considering prevalence-adjusted harm to users and harm to others, were (in rank order) alcohol, cigarettes, crystal methamphetamine, cannabis and heroin. This result is driven by the high prevalence of heavy alcohol consumption in Australia; the similar (high) weights of the first four ‘to users’ criteria (Drug-specific- and Drug-related mortality and Drug-specific and Drug-related morbidity); and the consistently high scoring for alcohol across all measures.
Overall relative harm score that combines prevalence weighted harm to users and harm to others.
Discussion
This study highlights the persistent and pervasive harms of the most frequently used psychoactive substances in the Australian community. As in previous studies in other jurisdictions, alcohol was the drug ranked as causing the greatest overall harm. Alcohol had by far the highest score on harm to others (a score of 41 compared with the next highest score of 24 for crystal methamphetamine), reflecting its widespread negative impacts on broad sectors of our community. In contrast to other countries, crystal methamphetamine was found to be the next most harmful drug to the Australian community, with high scores in both harm to the user and harm to others. Notwithstanding this latter finding, there is striking consistency between the results of the studies undertaken at different time points (the first study in the UK took place in 2010) and in different jurisdictions.
Alcohol consistently dominates harms in the MCDAs performed across the world (Nutt et al., 2010; Van Amsterdam et al., 2010, 2015a) and the most recent burden of disease study concluded that the level of alcohol consumption that minimises health loss is zero (Griswold et al., 2018). The harms associated with alcohol consumption cannot be ignored, and are particularly relevant to areas where per capita consumption is increasing, including South East Asia and the Western Pacific regions (World Health Organization, 2015). Recent data indicate per capita alcohol consumption in Australia has been declining. However, figures for alcohol-attributable deaths, alcohol-attributable hospitalisations (Lensvelt et al., 2018) and emergency department presentations (Lensvelt et al., 2015) have not followed this trend. The harm to others attributable to alcohol, is less easily quantified, but its pervasiveness is reflected in this study in that over 50% of alcohol’s total harm score was contributed by harm to others. A 2011 study, the first to comprehensively examine the harms to Australians caused by the drinking of others (Laslett et al., 2011), found that 73% of respondents had been negatively impacted by someone else’s drinking in the previous 12 months; women were more likely to be impacted by family members or intimate partners, while men were more affected by strangers, friends and co-workers. Of concern, young adults were the most negatively affected across a wide range of harms. This is reflected in the relatively high contribution of ‘family adversities’ and ‘injury’ to the overall harm ranking of alcohol in this MCDA. In Australia, the cost of the harms caused by the drinking of others was estimated to be approximately AUD $6.8 billion in 2010 (Laslett et al., 2011). Yet, initiatives aimed at limiting alcohol harms, such as restrictions on the alcohol content of beverages at sporting events, despite their effectiveness (Egerton-Warburton, 2018), draw complaints about the imposition of a ‘nanny state’ (http://www.abc.net.au/news/2017-11-26/is-ban-on-full-strength-beer-at-perth-stadium-nanny-state-move/9190292, accessed 12 August 2018). These data consistently and unequivocally indicate that alcohol and drug policies must prioritise investment in effective alcohol policies not only for the sake of the drinker but also the community. To this end, the WHO recommends quantifying the effects of alcohol on others in similar fashion to the effects of passive smoking (World Health Organization, 2015).
In this study, crystal methamphetamine scored next highest in terms of overall harm. This contrasts with the UK and European Union (EU) where heroin was the next most harmful substance after alcohol (Nutt et al., 2010; Van Amsterdam et al., 2015a). The costs of methamphetamine to the Australian community are estimated at AUD $5 billion annually, excluding the costs of Federal policing, Federal courts, and border protection (Tait et al., 2018). Methamphetamine death rates have doubled in Australia from 2009 to 2015, with direct toxicity being the most frequent cause but acceleration of natural disease, suicide and accidental death also feature highly (Darke et al., 2017). Regional and rural areas and younger drug users are disproportionately affected (Clayden et al., 2017). Globally, Australia is reported to have the highest prevalence of use of methamphetamine (O’Brien et al., 2017). In North America in 2016, methamphetamine was reported to be the second greatest drug threat after heroin (World Drug Report, 2018). In Europe, however, methamphetamine use is historically low, fairly stable and specific to the Czech Republic and Slovakia (European Monitoring Centre for Drugs and Drug Addiction, 2018).
A unique aspect of our study was the supplementary analysis, which took into account prevalence data to scale harm to user scores. Such analysis reflects that drug harms are not independent of prevalence of use. In this Australian MCDA, cannabis ranked 13th in harms prior to taking into account its prevalence of use. This contrasts with the UK and EU where it scored eighth position. However, once prevalence of use was taken into account, cannabis moved to the fourth rank. This is an important finding given the current debate in Australia and internationally regarding the legalization of recreational cannabis. The harms associated with cannabis use are lower than other substances, but cannabis is not ‘harmless’ and this study indicates that an increase in use will be likely to result in an increase in cannabis-related harm to some individuals and the wider community. From a public health and policy perspective sensible approaches to access cannabis under one of a number of potential non-prohibition models (Kilmer, 2017) will reduce cannabis related health and economic burden.
There are public health concerns about the move to full commercial cannabis legalisation schemes being implemented in North America. In Colorado, for example, the emerging evidence suggests: impacts on rates of cannabis use is mixed, the black market continues; providing a product free of pesticides and other chemicals and of known purity is challenging; product diversity increases particularly in very high potency preparations; and the marijuana industry has strongly resisted regulations which might affect their profits and continues to target high frequency users which they see as the backbone of their industry (Parnes et al., 2018; Subritzky et al., 2016) Against this there is increased attention being focussed on ‘mid-range’ non-commercial models such as Cannabis Social Clubs, which are seen as more attractive from a public health perspective (Decorte, 2018).
Pharmaceutical opioids ranked sixth overall in the prevalence weighted rankings. This reflects the rapid increase in prevalence in Australia and internationally and the concomitant diversion for illicit use. The expansion of world drug markets and the continuing emergence of new drugs is reflected in the absence of fentanyls in the original MCDA analysis on drug harms in 2010 in the UK (Nutt et al., 2010), but its presence by 2015 in the EU MCDA (Van Amsterdam et al., 2015a) and in the UK opioid MCDA (Van Amsterdam et al., 2015b). In 2016, in the United States, there was a 21% increase in overdose deaths from the previous year largely due to a rise in deaths associated with pharmaceutical and synthetic opioids including analogues of fentanyl such as carfentanil (World Drug Report, 2018). Currently, the recreational use of fentanyls is far less prevalent in Australia than in North America, and cases of fentanyl contamination of street heroin deals are extremely rare. Consequently fentanyls are positioned at 17th in the prevalence weighted rankings (compared with 3rd in the primary analysis). It should be noted, however, that between 2002 and 2012, rates of fentanyl related deaths in Australia increased on average 40% per year (Roxburgh et al., 2017). Given their extremely high potency, and consequent high risk of harm to the user, and drug market trends in the United States and Canada, public health measures are needed in anticipation of any increase in the prevalence of misuse of fentanyls in Australia. These measures should include: sentinel site monitoring of potential fentanyl contamination of street heroin samples; access to supervised injecting facilities, education for injecting drug users; and ready access to the opioid antagonist naloxone.
In this study, the harms of GHB ranked relatively low when compared with similar studies in the UK (Nutt et al., 2010) and the Netherlands (Van Amsterdam et al., 2010, 2015a, 2015b). GHB use in Australia seems to have stabilised, with less than 1% of Australians aged over 14 years having used GHB at some stage in their life and 0.1% having used it in the previous 12 months (Claydon et al., 2017). Emergency department presentations continue, especially on weekends and public holidays in inner city hospitals, with patients presenting mostly with varying levels of altered conscious state including coma (Dietze et al., 2014; Munir et al., 2008) but the rapid increase in presentations in the early 2000s has not been sustained. As well as the acute harms, there is emerging evidence of more chronic problems with memory and information processing in those users who experience recurrent episodes of coma (Raposo et al., 2018a, b) and delirium in acute withdrawal. As GHB use continues, the greater harms associated with GHB use will become apparent with time.
Limitations to the MCDA approach to assessing the drug harms have been discussed in previous publications (Nutt et al., 2010; Van Amsterdam, 2015a, 2015b). For example, some of the harms assessed in MCDA are unequivocally influenced by their legal status in the community, and it could be argued that the MCDA would be more accurate if only the harms resulting directly from the use of the drug – notwithstanding its legal status – were addressed. However, it was decided not to change these so that the findings could be compared with other international studies. In addition, rankings reflect only the current state of knowledge; for example, the harm status of ENDS in certain contexts remains to be determined, fentanyls or the more potent carfentanil may present greater risks if their prevalence, increases. Purity of crystal methamphetamine on the other hand may decrease, which may lower levels of harm over time (Scott et al., 2015). Also needing acknowledgement is that this exercise focused on the Australian population in general, and rankings within sub-populations of Australia would be different. Regional and rural communities, for example, have higher rates of use of methamphetamine and less access to treatment services, resulting in greater harms. Some remote indigenous Australian communities also have specific and significant problems with the recreational use of solvents and fuels. Another potential limitation is that the panel did not specifically include persons with a lived experience. It was deemed, however, that the diversity of our panel both in terms of extensive practice experience, skills, background and geography redressed these limitations.
International comparison of drug-related harms is essential. Comparing and contrasting trends between countries and regions to understand the most effective approach to a global problem, is a necessary step in understanding the impact of these drugs. Multi-criteria decision analysis is a useful approach to issues of concern for which there is no simple answer; using mathematical modelling to assess harms related to substance use that extend well beyond the traditional measures of drug-related morbidity and mortality, and that include assessment of harms that extend beyond the user to community. Application of this broad but detailed technique in different global regions enables useful international comparisons of trends in drug use and associated harms and hence informed debate by which to arrive at effective drug policy.
Footnotes
Acknowledgements
The authors would like to thank all participants in the MCDA workshop process for their valuable input and contribution to the study outcomes. All participants have given permission for their involvement in the study to be acknowledged. The authors would also like to thank Patrick Sharry from People+Decisions, and Paul Gordon from Catalyze for facilitating the workshop and analysing the data.
Authors contributions
Yvonne Bonomo: literature search, study design, data interpretation, manuscript writing, expert panel member; David Castle: study design, data interpretation, writing, expert panel member; David Nutt: study design, data interpretation, writing; Amanda Norman: literature search, data interpretation, writing; Adam Pastor: data interpretation, writing, expert panel member; Simon Lenton: data interpretation, writing, expert panel member; Raimondo Bruno: data interpretation, writing, expert panel member; Dan Lubman: data interpretation, writing, expert panel member; Sharon Dawe: data interpretation, writing, expert panel member; Diana Egerton-Warburton: data interpretation, writing, expert panel member; Mark Daglish: data interpretation, writing, expert panel member; Sam Biondo: data interpretation, writing, expert panel member; John Ryan: data interpretation, writing, expert panel member; Jonathan Karro: data interpretation, writing, expert panel member; Charles Kim: data interpretation, writing, expert panel member; Jill Rundle: data interpretation, writing, expert panel member. Patrick Sharry and Paul Gordon: study methodology, workshop facilitation, preparation of initial report.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YB has received honoraria as an Advisory Board Member to Indivior. AN has nothing to disclose. SB has nothing to disclose. RB has received grants from Indivior, outside the submitted work. SD has nothing to disclose. MD has received honoraria for talks and consultancy from Indivior, Janssen Cilag, Lundbeck, Servier; and is a current Advisory Board Member for Sublocade: Indivior. DEW has nothing to disclose. JK has nothing to disclose. CK has nothing to disclose. SL has nothing to disclose. DL has received speaking honoraria from AstraZeneca, Indivior, Janssen, Servier, Shire and Lundbeck and has provided consultancy advice to Lundbeck and Indivior. AP has nothing to disclose. DN has nothing to disclose. DC has received grant monies for research from Eli Lilly, Janssen Cilag, Roche, Allergen, Bristol-Myers Squibb, Pfizer, Lundbeck, Astra Zeneca, Hospira; Travel Support and Honoraria for Talks and Consultancy from Eli Lilly, Bristol-Myers Squibb, Astra Zeneca, Lundbeck, Janssen Cilag, Pfizer, Organon, Sanofi-Aventis, Wyeth, Hospira, Servier; and is a current Advisory Board Member for Lu AA21004: Lundbeck; Varenicline: Pfizer; Asenapine: Lundbeck; Aripiprazole LAI: Lundbeck; Lisdexamfetamine: Shire; Lurasidone: Servier; Brexpiprazole: Lundbeck; Treatment Resistant Depression: LivaNova. He does not knowingly have stocks or shares in any pharmaceutical company. Travel and accommodation costs for all workshop participants were provided by the Inclusive Health Fund, St Vincent’s Health Australia. PS and PG were paid a consulting fee by SVHA to conduct the study and analyze the data. PS has received a consultancy fees from Pfizer.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funds for this project were provided by the Inclusive Health Fund, St Vincent’s Health Australia.
The funding body had no role in the design or execution of the project.