
Abstract
Purpose:
This study aimed to investigate the efficacy and tolerability of aripiprazole, olanzapine and risperidone in first-episode schizophrenia (FES).
Methods:
The eight-week, open, randomised study was conducted in six Chinese medical centres. Altogether, 498 FES subjects were randomised to aripiprazole (n = 165), olanzapine (n = 168) or risperidone (n = 165). Efficacy was measured with the Positive and Negative Syndrome Scale (PANSS), tolerability with the Udvalg for Kliniske Undersogelser Side Effect Rating Scale (UKU) and functioning with the Personal and Social Performance Scale (PSP).
Results:
All three antipsychotics significantly improved the baseline to end-point PANSS total and each of the sub-scale scores (p < 0.001). Risperidone was superior to olanzapine and aripiprazole regarding PANSS total end-point scores (p < 0.05). Cumulative response (PANSS total score reduction ⩾30%) was similar between risperidone, olanzapine and aripiprazole (74.8%, 73.5% and 70.1%; p = 0.707), but risperidone was superior to aripiprazole regarding PANSS total score reduction ⩾50% (37.8% vs. 26.6%; p < 0.05). Olanzapine was associated with the largest weight gain at week 4 and 8 (p < 0.01), weight gain ⩾7% (olanzapine = 49.0% vs. risperidone = 32.5% vs. aripiprazole = 17.0%; p < 0.01), more psychic side effects at week 8 (p < 0.01 each) and more ‘other’ side effects at week 4 (p < 0.001) and week 8 (p < 0.05) but fewer neurological side effects at week 4 (p < 0.05) and week 8 (p < 0.01). PSP improved more with risperidone than with aripiprazole at week 4 and 8 (p < 0.05).
Conclusions:
For FES, risperidone might be a better choice than aripiprazole due to improved efficacy and functional improvement, without inferior tolerability. Aripiprazole is a better choice to avoid relevant short-term weight gain. Olanzapine could be chosen to avoid neurological adverse effects.
Introduction
Risperidone, olanzapine and aripiprazole are the three most widely used antipsychotics for patients with schizophrenia in both the USA and China (Liu et al., 2012; Robinson et al., 2015b; Zhang et al., 2012). Each have different pharmacological mechanisms and different safety profiles while differences in efficacy are less pronounced and clear (Leucht et al., 2013, 2017), especially in first-episode schizophrenia (FES; Zhang et al., 2013; Zhu et al., 2017a, 2017b).
Since medication choice is based on evidence and past treatment experiences and since FES patients lack past treatment experiences, evidence becomes even more important. Although expected to be better tolerated, aripiprazole had mixed efficacy results in chronic patients regarding total psychopathology compared to olanzapine and risperidone, being either inferior to olanzapine (Fleischhacker et al., 2009; Kane et al., 2009) or risperidone (Kishi et al., 2015; Leucht et al., 2013) or of comparable efficacy (Potkin et al., 2003). Additionally, two randomised controlled trials (RCTs) in FES suggested that aripiprazole might be superior to risperidone regarding negative symptoms (Liemburg et al., 2011; Robinson et al., 2015a). In patients with chronic schizophrenia (Leucht et al., 2009) and those with FES (McEvoy et al., 2007; Robinson et al., 2006), olanzapine and risperidone might have similar efficacy. However, in both chronic patients (Leucht et al., 2009) and FES (Zhu et al., 2017a), olanzapine had a particular liability for cardio-metabolic adverse effects, while risperidone was associated with prolactin elevation, and aripiprazole appeared relatively well tolerated.
A recent meta-analysis comparing antipsychotics in the acute treatment of FES found no differences between aripiprazole, olanzapine and risperidone. However, the authors acknowledged that the evidence was generally of low quality, and the number of patients for individual antipsychotics was small (Zhu et al., 2017a). Further, there is no RCT exploring the efficacy of the three most commonly used antipsychotics head-to-head. In order to provide additional, much-needed evidence for medication choice for FES, we conducted an open-label RCT comparing head-to-head risperidone, olanzapine and aripiprazole. Based on the literature summarised above, we hypothesised that risperidone and olanzapine would have comparable efficacy, and that both would be more efficacious than aripiprazole, which in turn would have some tolerability advantages, namely regarding body weight and prolactin.
Methods
Setting
The study design has been detailed elsewhere (Han et al., 2014). The study was conducted at six major psychiatric, not-for-profit hospitals in China.
Participants
Inclusion criteria were: (a) age 18–45 years; (b) current diagnosis of schizophrenia based on the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) Axis I Disorder, patient edition (SCID-I/P); (c) illness duration ⩽3 years; (d) continuous antipsychotic treatment <4 weeks and cumulative antipsychotic exposure <12 weeks; and (e) the ability to understand the content of the interview and provide written informed consent. Exclusion criteria included: (a) current major medical conditions; (b) lifetime history of or current alcohol/drug abuse or dependence; or (c) contraindication to olanzapine, aripiprazole or risperidone. Both outpatients and inpatients were recruited. There was not a cut-off score in the Positive and Negative Syndrome Scale (PANSS) score at baseline to be included in (or excluded from) the study.
The investigators invited eligible patients to participate. After a complete description of the study was given to the subjects, written informed consent was obtained. The trial complied with the Declaration of Helsinki and was approved by the ethics committees of the participating centres.
Treatment
Patients were randomised to risperidone (3–6 mg/day), olanzapine (10–25 mg/day) or aripiprazole (15–30 mg/day; Shu, 2007), using a stratified block randomisation on the basis of a pre-established scheme, stratified by study centre. The randomisation table and programme were generated with SAS v9.2 (SAS Institute, Cary, NC) by a clinical epidemiologist who was not involved in the trial. Oral benzhexol (2–6 mg/day) or promethazine (25–75 mg/day) was allowed, but neither was used preventively. Adjunctive lorazepam (0.5–1.5 mg/day) was allowed to be used sparsely if deemed necessary. Concomitant short-acting antipsychotic injections such as haloperidol or chlorpromazine were allowed within the first two weeks during titration of the assigned drugs in case of severe agitation, severe impulsiveness or suicide risk, although these were not encouraged. The total treatment of the study lasted 56 weeks. This paper focuses on the first, acute, eight-week treatment phase. Per protocol, switching between the study antipsychotics was allowed as early as week 4 according to the treating physician’s decision in case of non-response, defined as a PANSS (Kay et al., 1987) reduction <50%, symptom exacerbation, severe impulsiveness, agitation, suicidal risk or intolerability, including clinically relevant weight gain (Han et al., 2014). Although the switchers were followed up to week 8, only data prior to the switching were included in the primary analysis.
Outcomes
All measurements of psychiatric efficacy, safety and tolerability were performed at baseline and at the end of week 4 and 8.
Efficacy
Efficacy regarding psychopathology was measured with the PANSS. The primary efficacy measure was the baseline to end-point change in PANSS total score. The secondary efficacy measure included the change in PANSS positive, negative and general psychopathological sub-scale scores, and the percentage of responders (PANSS total score decrease ⩾30%) and full responders (PANSS total score decrease ⩾50%). Functioning was evaluated with the Personal and Social Performance Scale (PSP; Si et al., 2011).
Safety and tolerability
Side effects were measured with the Udvalg for Kliniske Undersogelser Side Effect Rating Scale (UKU; Lingjaerde et al., 1987), which is a comprehensive rating scale for psychotropic drugs and is commonly used in RCT studies (Crespo-Facorro et al., 2013; Kahn et al., 2008). Selected items from the UKU were used to measure extrapyramidal symptoms (EPS), menstrual problems and sexual symptoms.
None of the raters were blind to the allocation status of the patients. They underwent formal training on the scales and reached a good inter-rater reliability (intra-class correlation coefficients or kappa values >0.75).
Statistical analysis
Assuming mean PANSS total score changes of 30, 36 and 36 with aripiprazole, olanzapine and risperidone, respectively, a standard deviation of 18 and an attrition rate of 25%, we needed 166 patients per treatment group (i.e. 498 patients in total) based on a two-tailed test with α = 0.05 and 1–β = 0.80 (Chan et al., 2007; Kahn et al., 2008).
Efficacy and tolerability analysis
We used a linear mixed-effects model for continuous data. For the analysis of the baseline to end-point change score, variance analysis was used to explore effects of treatment groups, time points and interaction terms. Baseline data were used as co-variables in the analysis of raw scores to explore effects of treatment groups, time points and interaction terms. The Scheffe method was used for multi-comparison between different groups (Slanger, 1996). The Cochran–Mantel–Haenszel test with central effect controlling was used for categorical data (Agresti, 1990).
The full analysis set (FAS) included all randomised patients who completed at least one post-baseline assessment. Mixed-model repeated-measures analysis was used to manage the missing data. All data were analysed with SAS v9.2. All tests were two-sided, with α = 0.05.
Results
Participants
The FAS sample included 498 participants (Figure 1). The three groups did not differ on any other baseline characteristics (Table 1).
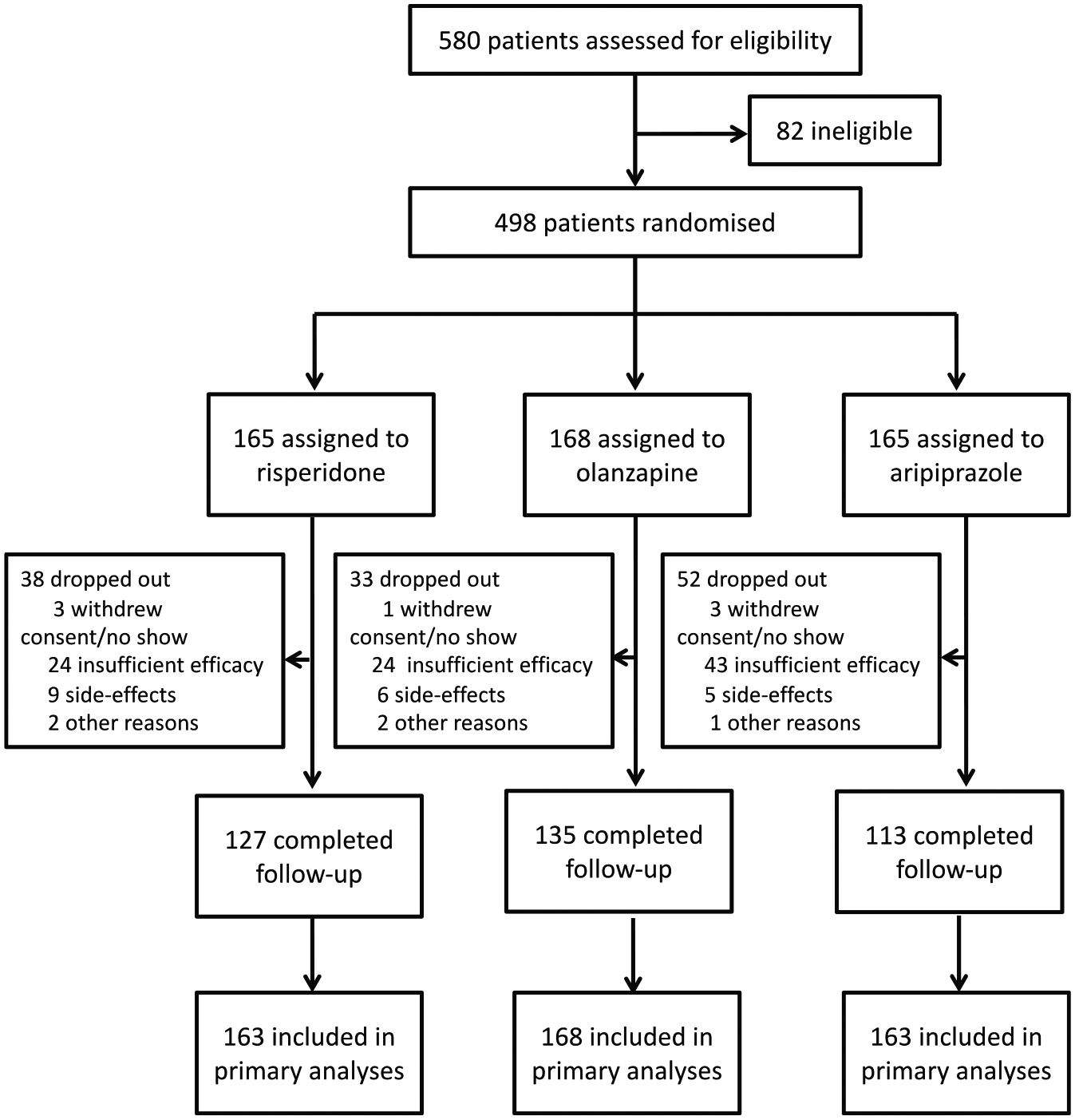
Trial profile.
Baseline characteristics of the patients and concomitant treatments.
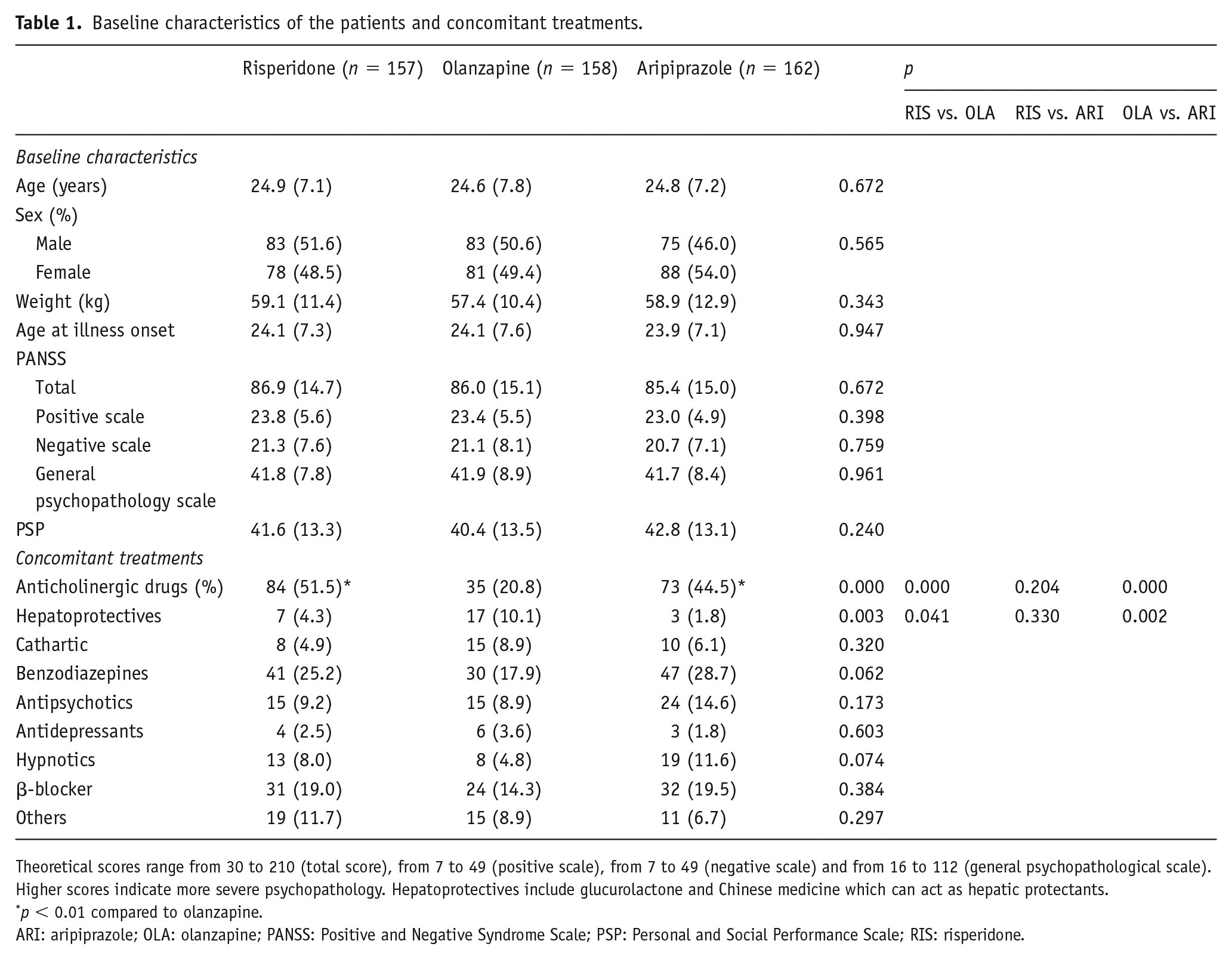
Theoretical scores range from 30 to 210 (total score), from 7 to 49 (positive scale), from 7 to 49 (negative scale) and from 16 to 112 (general psychopathological scale). Higher scores indicate more severe psychopathology. Hepatoprotectives include glucurolactone and Chinese medicine which can act as hepatic protectants.
p < 0.01 compared to olanzapine.
ARI: aripiprazole; OLA: olanzapine; PANSS: Positive and Negative Syndrome Scale; PSP: Personal and Social Performance Scale; RIS: risperidone.
Treatment and dose
The doses of risperidone, olanzapine and aripiprazole were 3.7 ± 1.2 mg, 16.0 ± 4.9 mg and 17.6 ± 5.2 mg, respectively. Patients on olanzapine were less likely to use concomitant drugs than patients on either risperidone or aripiprazole (p < 0.01; Table 1).
Efficacy
Primary efficacy outcome
Throughout the eight-week period, PANSS total scores reduced significantly in all three treatment groups (p < 0.001). PANSS total scores decreased by 39.0 (SD = 17.6) for risperidone, 36.1 (SD = 17.7) for olanzapine and 33.8 (SD = 16.6) for aripiprazole from baseline to the study end point. Risperidone was associated with a significantly greater reduction in PANSS total score than both aripiprazole and olanzapine at both week 4 (p < 0.01 and p < 0.05, respectively) and week 8 (both p < 0.05).
Secondary efficacy outcome
All secondary efficacy parameters improved significantly throughout the study (p < 0.001). Risperidone was associated with greater improvements in PANSS positive sub-scores (p < 0.01) at week 8 and PANSS general psychopathological sub-scores at week 4 (p < 0.05) than aripiprazole (Figure 2), and greater reductions in PANSS negative sub-scores than both olanzapine and aripiprazole (p < 0.05 each), but only at week 4.
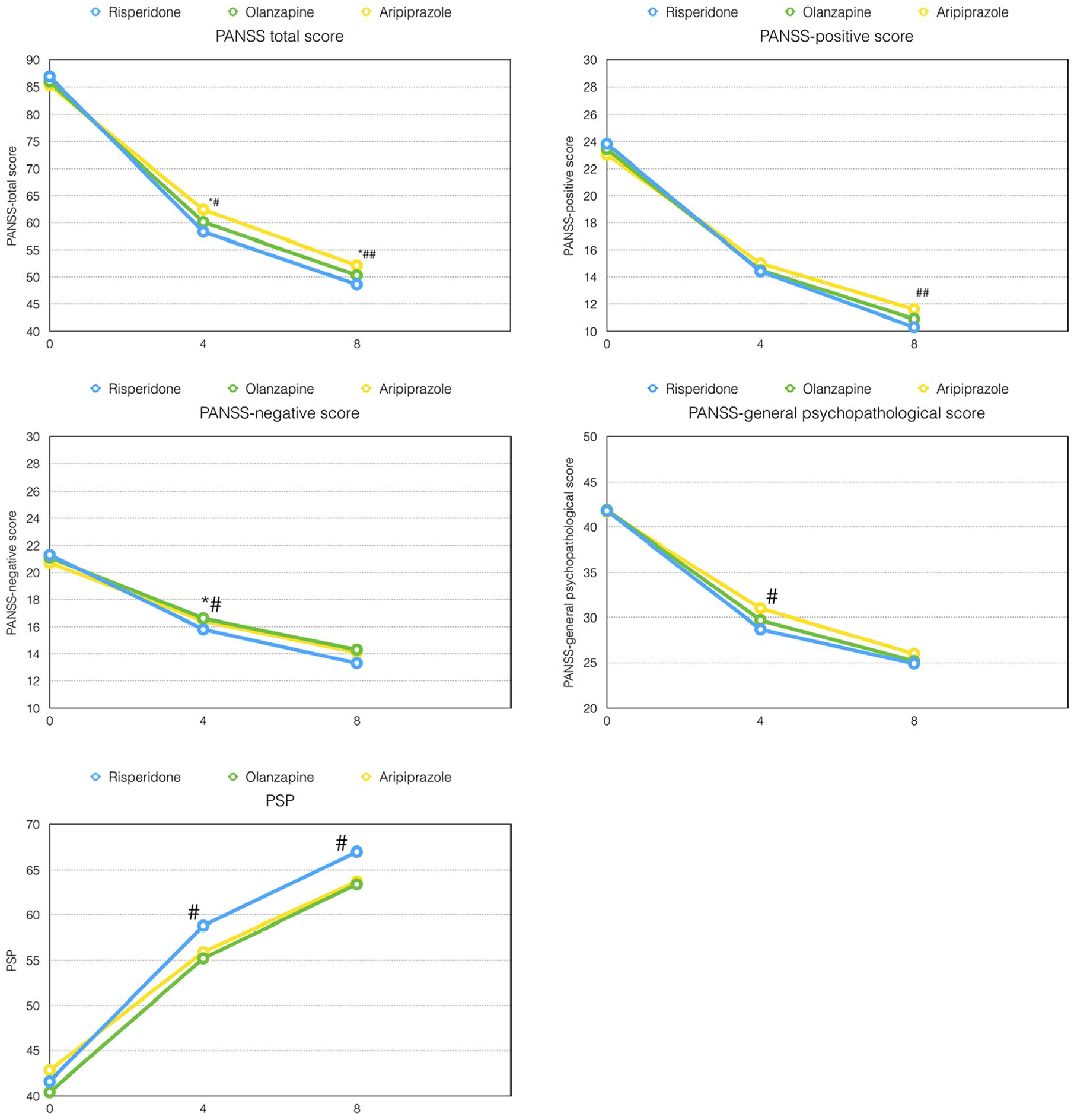
Outcome of efficacy mean changes of PANSS and PSP score from baseline.
Cumulative response rates (⩾30% PANSS total score reduction) did not differ between aripiprazole, olanzapine and risperidone (70.1%, 73.5% and 74.8%, respectively; p = 0.707), but risperidone was associated with a significantly more robust response (⩾50% PANSS total score reduction) than aripiprazole at both week 4 (18.4% vs. 9.2%, χ2 = 5.80, p < 0.05) and week 8 (37.8% vs. 26.6%; χ2 = 3.87, p < 0.05). There was a trend-level advantage with olanzapine versus aripiprazole at week 8 (36.4%; χ2 = 2.86, p = 0.091; see Supplemental Figure S1).
Social function
PSP improved significantly with each of the three treatments at both week 4 and week 8 (p < 0.001). Risperidone was associated with a significantly greater improvement than aripiprazole at both week 4 and week 8 (p < 0.05).
Safety and tolerability
Patients on risperidone (p < 0.05) and olanzapine (p < 0.01) experienced significant weight gain, while patients on aripiprazole did not (p = 0.94). Olanzapine was associated with the most weight gain (p < 0.01) and the highest incidence of ⩾7% weight gain (p < 0.001; Table 2).
Safety and tolerability.
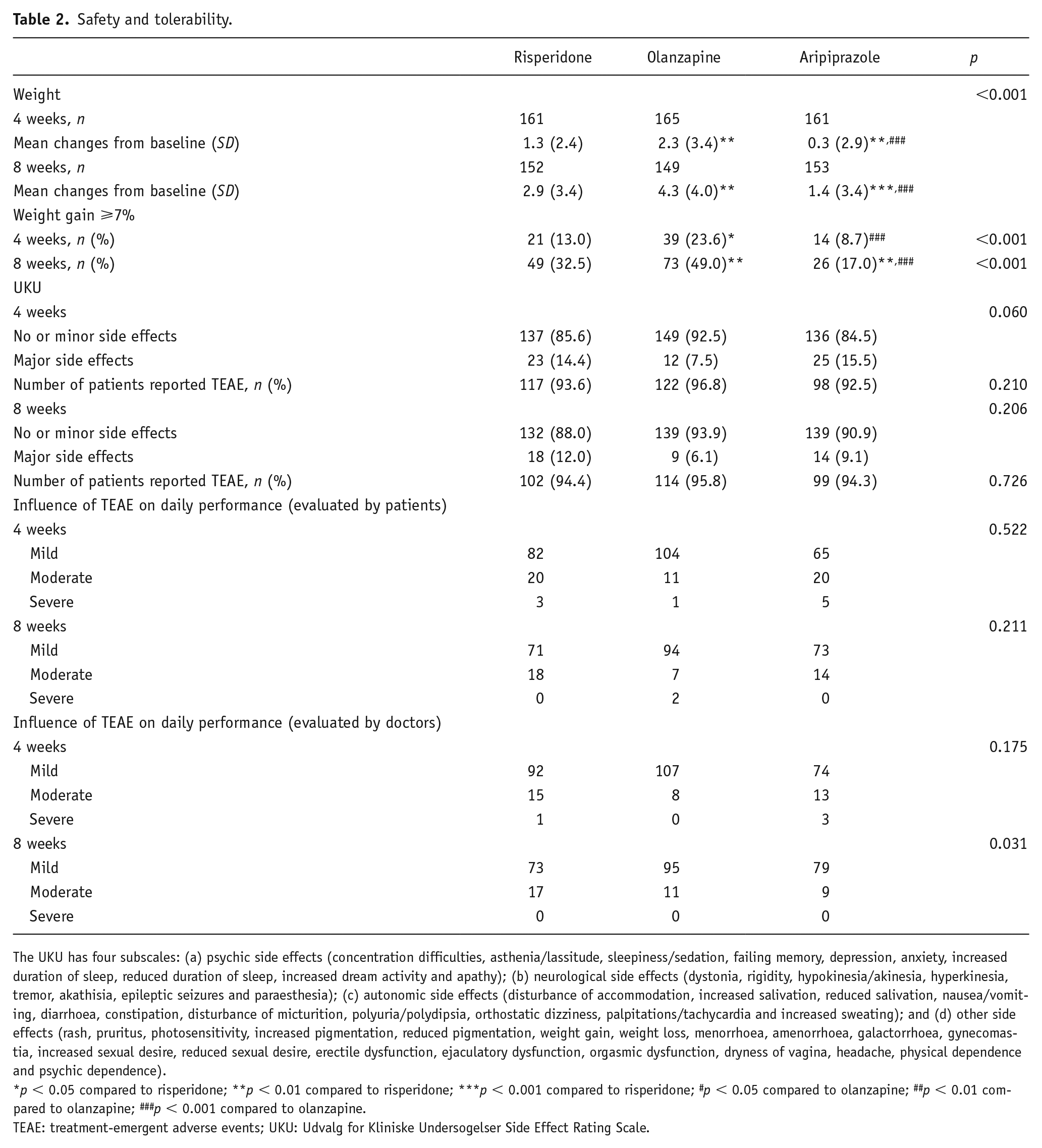
The UKU has four subscales: (a) psychic side effects (concentration difficulties, asthenia/lassitude, sleepiness/sedation, failing memory, depression, anxiety, increased duration of sleep, reduced duration of sleep, increased dream activity and apathy); (b) neurological side effects (dystonia, rigidity, hypokinesia/akinesia, hyperkinesia, tremor, akathisia, epileptic seizures and paraesthesia); (c) autonomic side effects (disturbance of accommodation, increased salivation, reduced salivation, nausea/vomiting, diarrhoea, constipation, disturbance of micturition, polyuria/polydipsia, orthostatic dizziness, palpitations/tachycardia and increased sweating); and (d) other side effects (rash, pruritus, photosensitivity, increased pigmentation, reduced pigmentation, weight gain, weight loss, menorrhoea, amenorrhoea, galactorrhoea, gynecomastia, increased sexual desire, reduced sexual desire, erectile dysfunction, ejaculatory dysfunction, orgasmic dysfunction, dryness of vagina, headache, physical dependence and psychic dependence).
p < 0.05 compared to risperidone; **p < 0.01 compared to risperidone; ***p < 0.001 compared to risperidone; #p < 0.05 compared to olanzapine; ##p < 0.01 compared to olanzapine; ###p < 0.001 compared to olanzapine.
TEAE: treatment-emergent adverse events; UKU: Udvalg for Kliniske Undersogelser Side Effect Rating Scale.
Neither the proportion of patients reporting treatment-emergent adverse side effects (TEAEs) on the UKU nor the severity evaluated by clinicians or patients differed between the three groups (Table 2). Similarly, the three groups did not differ regarding autonomic side effects (Table 3). However, patients on olanzapine experienced more psychic side effects at week 8 (p < 0.01), more ‘other’ side effects at both week 4 (p < 0.001) and week 8 (p < 0.05) and fewer neurological side effects at both week 4 (p < 0.05) and week 8 (p < 0.01) (Table 3). Olanzapine was associated with fewer EPS than both risperidone and aripiprazole at both week 4 (p < 0.01 each) and week 8 (p < 0.05 and p < 0.001, respectively). Patients on risperidone suffered more from menstrual problems than aripiprazole at week 4 (p < 0.01) and week 8 (p < 0.001) and than olanzapine at week 8 (p < 0.05; Table 3). The proportion of sexual side effects in males did not differ between the three groups.
Comparison between the three groups in four subscales of the UKU, EPS, menstrual problems and sexual symptoms (male).
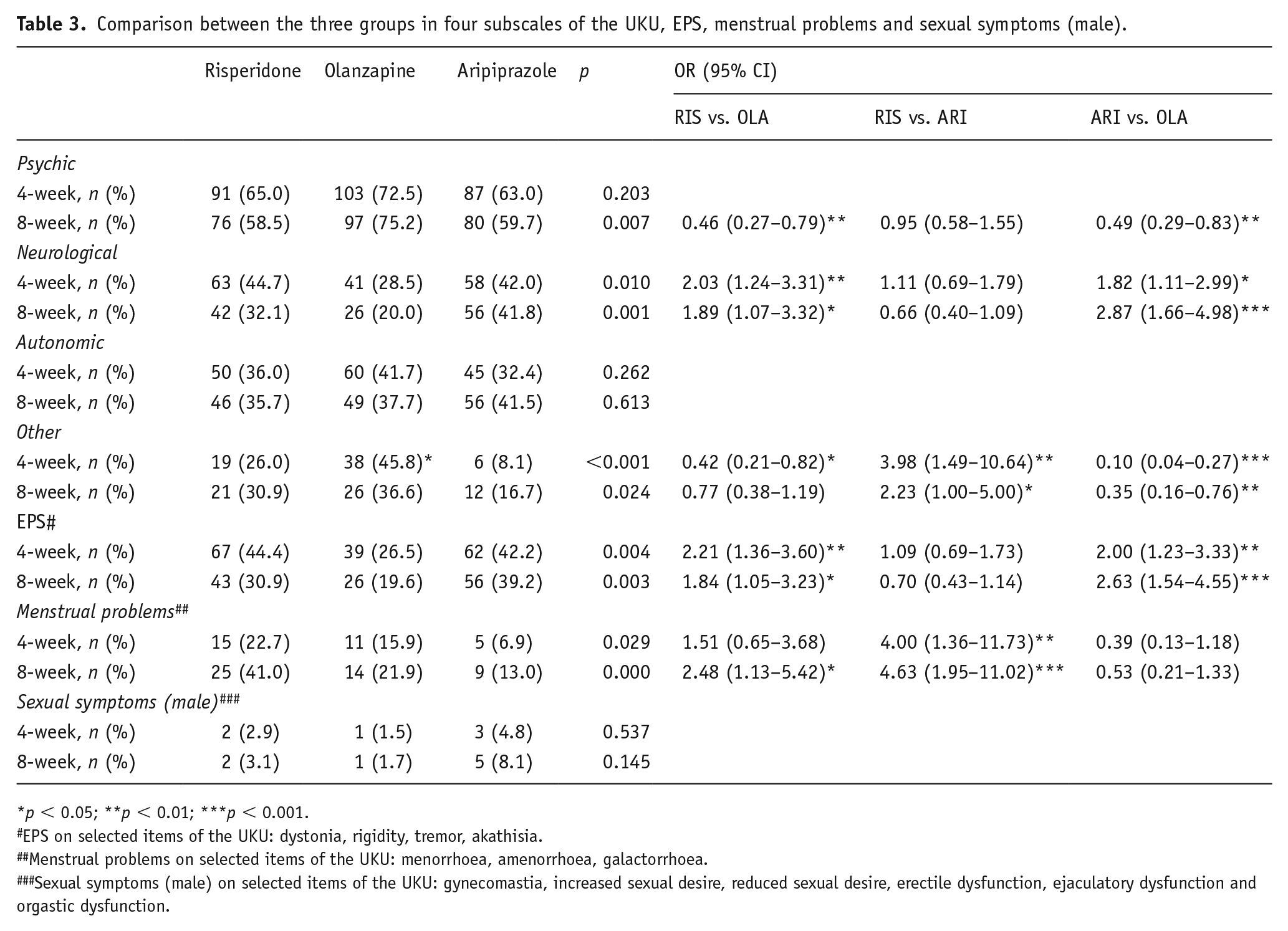
p < 0.05; **p < 0.01; ***p < 0.001.
EPS on selected items of the UKU: dystonia, rigidity, tremor, akathisia.
Menstrual problems on selected items of the UKU: menorrhoea, amenorrhoea, galactorrhoea.
Sexual symptoms (male) on selected items of the UKU: gynecomastia, increased sexual desire, reduced sexual desire, erectile dysfunction, ejaculatory dysfunction and orgastic dysfunction.
Discussion
To our knowledge, this is the first randomised, head-to-head trial comparing risperidone, olanzapine and aripiprazole for the acute treatment of FES patients. Results suggest that all three antipsychotics can effectively relieve the acute symptoms in FES patients. However, risperidone was superior to both olanzapine and aripiprazole regarding total symptoms and superior to aripiprazole regarding positive symptoms. Eight-week response rates were nearly 75% and were similar between the three medications, which is consistent with most previous studies in FES (Robinson et al., 2015a). However, an eight-week robust response occurred in only little more than one third of patients on risperidone and olanzapine, as well as little more than one quarter of patients on aripiprazole, with a significant advantage for risperidone and near-significant advantage for olanzapine.
Robinson et al. (2015a) found no differences between aripiprazole and risperidone in global symptom efficacy in FES evaluated with the BPRS. A recent meta-analysis comparing antipsychotics in the acute treatment in FES similarly found no differences between aripiprazole and risperidone in symptom reduction, but with limited studies and sample sizes (Zhu et al., 2017a). However, consistent with our findings, Zhang and Dai (2012) found paliperidone to reduce PANSS total scores more than aripiprazole in Chinese FES. A network meta-analysis of acute trials in multi-episode patients found better efficacy for improvement in global symptoms with risperidone compared to aripiprazole (Leucht et al., 2013). Although response rates were similar between risperidone and aripiprazole, however, risperidone was superior to aripiprazole regarding total symptoms, positive symptoms and robust response rates in our trial. Thus, patients with risperidone might response more fully than patients with aripiprazole. Although olanzapine also outperformed aripiprazole in chronic patients (Fleischhacker et al., 2009; Kane et al., 2009; Leucht et al., 2013), and generally performed similarly as risperidone (Conley and Mahmoud, 2001; Sacchetti et al., 2008), including in the network meta-analysis (Leucht et al., 2013), in our trial, olanzapine and aripiprazole were not different regarding any psychopathology outcome. In fact, in our study, risperidone was superior even to olanzapine at the eight-week study end point – a difference that was not found in another head-to-head FES trial at week 16 (Robinson et al., 2006). However, there were no differences in response rates and robust response rates between olanzapine and risperidone. Thus, there was hardly any clinically meaningful difference between risperidone and olanzapine in symptom reduction in FES patients.
Olanzapine and risperidone were associated with significant weight gain, while this was not the case for aripiprazole. The latter finding is not consistent with other studies where aripiprazole has also been associated with significant weight gain in FES patients (Crespo-Facorro et al., 2013; Pérez-Iglesias et al., 2014; Robinson et al., 2015a) or antipsychotic-naïve patients (Correll et al., 2009). The overall non-significant weight gain with aripiprazole in our study might be due to differences between Western and Chinese populations. Zhang and Dai (2012) found that aripiprazole increased the weight at 3.3 kg within 13 weeks in FES, which was much lower than 5.04 kg in the 12-week study by Robinson et al. (2015a). Nevertheless, 17.0% of patients still experienced ⩾7% weight gain at week 8 in the aripiprazole group, although this was lower than in the risperidone group (32.5%) and the olanzapine group (49.0%). These data suggest a lower weight impact of aripiprazole than olanzapine and risperidone in Chinese FES, at least in the short term, as weight gain ⩾7% occurred in 45% of Spanish FES patients at week 12 (Crespo-Facorro et al., 2013) and 77% and 63% after only 6 weeks of treatment with olanzapine and risperidone, respectively (Saddichha et al., 2008). Because of this problematic side effect, olanzapine was not recommended as the first-line medication in patients with FES in updates of several guidelines (Buchanan et al., 2010). However, as weight gain with antipsychotics was a highly variable phenomenon, standard deviations of weight gain were almost always larger than the means. More studies were needed to identify which group of patients were more likely to gain weight with antipsychotics. An alternative explanation, however, could also be that in our study patients could have had up to 12 weeks of cumulative lifetime antipsychotic exposure, during which some degree of weight gain could have occurred. Nevertheless, ⩾7% weight gain risk in FES patients is higher than in multi-episode patients in whom weight gain has already occurred to variable degrees, being 37–40.3% with olanzapine and 14–16.4% with aripiprazole after 26–28 weeks of treatment (Kane et al., 2009; McQuade et al., 2004). Although switching from olanzapine or risperidone to aripiprazole was successful in multi-episode patients in reducing body weight and metabolic abnormalities (Stroup et al., 2011; Wani et al., 2015), aripiprazole can also cause cardio-metabolic effects, especially in subgroups of FES and antipsychotic-naïve patients.
The three antipsychotics did not differ regarding overall adverse effects. Thus, different from our hypothesis, aripiprazole failed to demonstrated better global safety and tolerability than risperidone or olanzapine in FES. When we explored results on the four UKU sub-scales in more detail, we found no group differences regarding autonomic side effects, but olanzapine increased the risk of ‘psychic’ and ‘other’ side effects compared to both risperidone and aripiprazole. In contrast, patients on risperidone or aripiprazole suffered more ‘neurological’ side effects. Robinson et al. found that parkinsonism and EPS did not differ significantly between risperidone and olanzapine (Robinson et al., 2006) or between aripiprazole and risperidone (Robinson et al., 2015a). This finding is largely consistent with our data showing that risperidone and aripiprazole did not differ regarding EPS. However, both risperidone and aripiprazole were associated with more EPS than olanzapine. The proportion of patients requiring anticholinergic drugs was also higher with risperidone and aripiprazole than with olanzapine. Similar to our data, a one-year study conducted in FES suggested that olanzapine was associated with fewer EPS than risperidone (Crespo-Facorro et al., 2011). The meta-analysis comparing tolerability of 15 antipsychotics in multi-episode patients also suggested that olanzapine was associated with fewer EPS than both risperidone and aripiprazole. Our data showed that this advantage of olanzapine over risperidone and aripiprazole also seems to exist in the FES population – a finding for which too few FES data were available in the recent meta-analysis of antipsychotics in FES (Zhu et al., 2017a). In that meta-analysis of FES, only use of antiparkinsonian medications was meta-analysed, and olanzapine was only superior to risperidone but not aripiprazole, which was likely due to insufficient power. Our data showed that aripiprazole had the least risk of the ‘other’ UKU side effect sub-scale, which mainly includes weight gain and sexual symptoms, than risperidone and olanzapine. Further analyses revealed that there were no significant differences between the three antipsychotics regarding male sexual symptoms. However, aripiprazole caused fewer menstrual problems than risperidone at both the four- and eight-week time points, and than olanzapine only at the eight-week time point. Although prolactin levels are often measured, relatively few RCTs have reported on sexual symptoms in patients with schizophrenia. RCTs of multi-episode patients consistently showed that risperidone-treated patients reported more sexual dysfunction than olanzapine-treated patients (Ciudad et al., 2007; Knegtering et al., 2006; Potkin et al., 2017). Our data suggested that at least when measuring symptoms with the UKU, these differences did not appear to be this large in the FES population. The ‘autonomic’ side effects, which include disturbance of accommodation and constipation, were rarely reported in the studies of FES. Our data showed that the three drugs did not differ in this area. There were few data of ‘psychic’ side effects in previous FES studies.
All three antipsychotics improved functioning, measured by the PSP. However, there was a significant advantage with risperidone versus aripiprazole. To our knowledge, to date, no RCT in acute FES has reported on differences in social and personal functioning. Maat et al. (2014) found an improvement in social functioning (evaluated by the Social Functioning Scale and Quality of Life Scale) with both risperidone and aripiprazole during eight weeks of treatment without differences between the two drugs. Gureje et al. found that olanzapine was superior to risperidone in improving social functioning (evaluated by QLS and SF-36) during 30 weeks of treatment (Gureje et al., 2003). Therefore, it is currently unclear which antipsychotic may yield greater social and personal functioning in FES patients, and this therefore requires further study.
Our study has several limitations. First, the acute and controlled portion of our open-label RCT lasted only eight weeks. Although, we followed patients up to 52 weeks in the overall study design, clinicians were allowed to switch the assigned treatment as early as four weeks but were discouraged to do so until week 8, which is why we can only report on the formal efficacy part of this RCT until week 8, as afterwards too many treatment crossovers and switches occurred (Cheng et al., 2019). Second, the study employed an open-label design to improve the trial’s acceptability for patients because the three-phase design of the whole trial aimed to keep the patients on antipsychotic treatment for as long as possible and to maximise the possibility of completing the follow-up. An open-label design could have introduced a bias. However, lack of blinding increases external validity, as in clinical care, the patients and treating clinicians know which medication they are using and dose adjustments are made knowing what to expect from certain dose increments with a specific medication. Open randomised trials will arguably provide a better indication of the true value of the three drugs in clinical practice than double-blind trials will (Kahn et al., 2008), which are still needed to provide information without biases from subjective factors. Third, we employed the targeted dose range of antipsychotics for general schizophrenia patients according to the Chinese guideline, although patients with FES might respond to a relatively low dose of antipsychotics. However, the titration rate was not fixed in our study, as we wanted to enhance the generalisability of the findings to clinical care where dose adjustments are made based on efficacy and tolerability signals in individual patients, but we recorded the prescribed doses. It was very interesting that the mean dose in both the risperidone and aripiprazole groups was 12 mg/day in olanzapine equivalent (Gardner et al., 2010), which was comparable with other RCTs (Zhu et al., 2017a) but lower than the mean dose in the olanzapine group (16 mg per day) in this study. In another RCT study with a flexible dose design, the mean dose (16.7 mg per day) in the olanzapine group was also higher than in the aripiprazole group (12.9 mg/day; Kahn et al., 2008). However, the relatively high dose of olanzapine failed to demonstrate any advantage in effectiveness at both symptom and function level over risperidone or aripiprazole. Additionally, some patients might need 30 mg of olanzapine to achieve an optimal treatment response, which was beyond the usual recommended dose range for FES patients. However, efficacy and safety of olanzapine with a high daily dose (25–30 mg) was beyond our trial. Fourth, we did not collect laboratory information or conduct an electrocardiogram on patients for research purposes. However, we assessed adverse effects from a patient and clinician perspective using the UKU, which provides a picture of clinically relevant adverse events. Fifth, pharmacokinetic data in this study were not collected. Thus, medication adherence could not be ensured for outpatients. Finally, several important factors related to the management of schizophrenia, such as cognition and quality of life, were not evaluated in the eight-week trial.
Despite these limitations, together with one five-arm study in FES (Kahn et al., 2008), this is the largest randomised, head-to-head-trial in FES and the largest comparing the three most used antipsychotics in FES: risperidone, olanzapine and aripiprazole. Results indicated that risperidone seemed to have some advantages in total psychopathology versus both olanzapine and aripiprazole, and regarding positive symptoms and PSP compared to aripiprazole. There was no difference in overall side effects between the three drugs. Conversely, there were significant advantages of aripiprazole over risperidone and of both agents over olanzapine regarding body weight gain, of aripiprazole over both risperidone and olanzapine regarding menstrual problems, of both risperidone and aripiprazole over olanzapine regarding psychic side effects, and of olanzapine over risperidone and aripiprazole regarding EPS and anticholinergic use. Nevertheless, the clinical meaningfulness and relevance of these results for certain patient subgroups remains unclear (Heres et al., 2006), and additional studies are needed to shed light on the comparative efficacy and effectiveness of antipsychotics in FES – an area where still too few large studies exist (Zhu et al., 2017a).
Supplemental Material
figure_3-only_online-4.11-revised – Supplemental material for An open-label randomised comparison of aripiprazole, olanzapine and risperidone for the acute treatment of first-episode schizophrenia: Eight-week outcomes
Supplemental material, figure_3-only_online-4.11-revised for An open-label randomised comparison of aripiprazole, olanzapine and risperidone for the acute treatment of first-episode schizophrenia: Eight-week outcomes by Zhang Cheng, Yanbo Yuan, Xue Han, Lei Yang, Shangli Cai, Fude Yang, Zheng Lu, Chuanyue Wang, Hong Deng, Jingping Zhao, Yutao Xiang, Christoph U Correll and Xin Yu in Journal of Psychopharmacology
Footnotes
Acknowledgements
We thank the participating patients and their families, as well as the site investigators, without whom this study would not have been possible. We thank Yangfeng Wu for his help with data analysis. Dr Xin Yu had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Christoph U. Correll has been a consultant and/or adviser to or has received honoraria from: Alkermes, Allergan, Bristol-Myers Squibb, Gerson Lehrman Group, IntraCellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, Medavante, Medscape, Neurocrine, Otsuka, Pfizer, Rovi, Sunovion, Takeda and Teva. He has provided expert testimony for Bristol-Myers Squibb, Janssen and Otsuka. He served on a Data Safety Monitoring Board for Lundbeck and Pfizer. He received grant support from Janssen and Takeda. Dr Xin Yu has been an adviser or in speaker’s bureau to or has received honoraria from: Eli Lilly China, Xian Janssen, Lundbeck, Pfizer China, Eisai China, Novartis China and Sanofi China. The remaining authors report no competing interests related to the topic of this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this study was supported by National Key Project of Scientific and Technical Supporting Programs funded by Ministry of Science and Technology of China (no. 2007BAI17B04). CNFEST received study drugs from Eli Lily, Janssen & Janssen and Kanghong Pharmaceutical Co. Ltd. The funding agency of the study as well as the pharmaceutical companies providing the study medications in kind had no role in study design, data collection, data analysis, data interpretation, writing of the report or decision of where to publish the results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.