
Abstract
Background:
Major depressive disorder is characterized by the presence of at least five of nine specific symptoms that contribute to clinically significant functional impairment. This analysis examined the effect of desvenlafaxine (50 or 100 mg) versus placebo on symptom cluster scores and the association between early improvement in symptom clusters and symptomatic or functional remission at week 8.
Methods:
Using data from nine double-blind, placebo-controlled studies of desvenlafaxine for the treatment of major depressive disorder (N=4317), the effect of desvenlafaxine 50 or 100 mg versus placebo on scores for symptom clusters based on 17-item Hamilton Rating Scale for Depression items was assessed using analysis of covariance. Association between early improvement in symptom clusters (⩾20% improvement from baseline at week 2) and symptomatic and functional remission (17-item Hamilton Rating Scale for Depression total score ⩽7; Sheehan Disability Scale score <7) at week 8 was analyzed using logistic regression. Symptom clusters based on Montgomery–Åsberg Depression Rating Scale were also examined.
Results:
Desvenlafaxine 50 or 100 mg was associated with significant improvement from baseline compared to placebo for all symptom clusters (p<0.001), except a sleep cluster for desvenlafaxine 100 mg. For all symptom clusters, early improvement was significantly associated with achievement of symptomatic and functional remission at week 8 for all treatment groups (p⩽0.0254).
Conclusion:
Early improvement in symptom clusters significantly predicts symptomatic or functional remission at week 8 in patients with depression receiving desvenlafaxine (50 or 100 mg) or placebo. Importantly, patients without early improvement were less likely to remit.
Keywords
Introduction
Depressive disorders are the leading cause of disability worldwide and a major contributor to suicide deaths (World Health Organization, 2017). Numerous drugs have demonstrated efficacy for treating the symptoms of major depressive disorder (MDD; Arroll et al., 2005; Carrasco et al., 2016; Girardi et al., 2009; Maneeton et al., 2013; Thase et al., 2017), but overall rates of remission for MDD patients treated with drugs for depression remain below 50% in clinical trials (Machado et al., 2006), and even those patients who achieve symptomatic remission may fail to return to pre-illness functioning (McIntyre et al., 2015). Because efficacy differences between medications for depression are modest at the population level (Cipriani et al., 2018; Kennedy et al., 2016), MDD treatment guidelines recommend considering patient factors such as response to prior medication and risk for nonadherence, clinical features, and co-occurring conditions when planning pharmacological treatment (Gelenberg et al., 2010; Kennedy et al., 2016; Pompili et al., 2013). Identifying and characterizing between-patient differences associated with positive patient outcomes with specific drugs is now a critical focus of depression research (National Institute of Mental Health, 2015). Recognizing which individuals will benefit from a particular drug will allow clinicians to personalize treatment for patients with MDD.
MDD is characterized by the presence of five or more defined symptoms that cause significant impairment of functioning (American Psychiatric Association, 2013). Dysregulation in specific neurocircuits has been hypothesized to underlie related groups or clusters of symptoms in MDD, such as those related to mood or sleep (Stahl, 2003; Stahl et al., 2003). Different clusters of symptoms may be more or less responsive to drugs for depression, with differences between agents based on their hypothesized mechanisms of action (Chekroud et al., 2017; Cooper et al., 2014; Mallinckrodt et al., 2007; Stahl, 2003). Symptom clusters may also differ in their time course for improvement during treatment for depression, with both symptom cluster and severity of depression potentially impacting the timing of improvement (Cooper et al., 2014; Shelton et al., 2007). The assessment of MDD symptom cluster severity at baseline, with follow-up evaluations over the course of treatment of depression, can be a key element of measurement-based care for individuals with MDD (Chekroud et al., 2017; McIntyre, 2013; Oluboka et al., 2018). It is therefore of interest to explore early symptom response to treatment and the association with treatment outcomes, with the goal of identifying individuals who will benefit from a particular drug over another.
Symptom clusters in MDD patients are based on related groupings of depression scale items. For example, Cleary and Guy used a factor analysis of the 21-item Hamilton Rating Scale for Depression (HAM-D; Hamilton, 1960) with data from 32 clinical trials to identify related groupings of symptoms or factors (Cleary and Guy, 1977). They reported a five-factor solution for patients with heterogeneous diagnoses (neurotic depression, major affective disorders, and schizophrenia) and a six-factor solution for patients with neurotic depression only, which included: factor I, anxiety/somatization symptoms; factor II, weight; factor III, cognitive disturbance (e.g. guilt, agitation, paranoid symptoms); factor IV, diurnal variation; factor V, retardation; and factor VI, sleep disturbance (Cleary and Guy, 1977). Two other HAM-D subscales, the Maier scale and HAM-D6, provide measures of severity of depressive symptoms (Bech et al., 1975; Maier and Philipp, 1985). Similarly, a principal component analysis of responses on the Montgomery–Åsberg Depression Rating Scale (MADRS; Montgomery and Åsberg, 1979) yielded dysphoria, retardation, and vegetative symptom clusters (Suzuki et al., 2005). Additional MADRS clusters have also been defined, including symptoms related to anhedonia (McIntyre et al., 2016), and the MADRS6, a unidimensional depression scale generally comparable to the HAM-D6 (Bech et al., 2002, 2004). Symptom subscales such as these can be used to explore the differential effects of individual drugs for depression on symptom clusters (Chekroud et al., 2017; McIntyre et al., 2016), whether the presence of symptom clusters at baseline are predictive of treatment outcomes (Shelton et al., 2007), or whether improvement in specific symptom clusters predicts later overall treatment outcome (Katz et al., 2009).
Numerous previous analyses have demonstrated that early improvement in depression or function scale scores strongly predicts symptomatic and functional outcomes in patients treated for MDD (reviewed by Habert et al., 2016). The most commonly used definition of early improvement was a ⩾20% change from baseline in depression scale score after two weeks of treatment for depression (Habert et al., 2016). The current pooled post hoc analysis was conducted both to examine the treatment effect of desvenlafaxine (50 or 100 mg) versus placebo on specific clusters of symptoms derived from the 17-item Hamilton Rating Scale for Depression (HAM-D17; Hamilton, 1960) or MADRS, and to examine the association between improvement in symptom cluster scores at week 2 and symptomatic and/or functional remission at week 8. Based on its known efficacy for treating symptoms of depression (Carrasco et al., 2016), we hypothesized that the serotonin-norepinephrine reuptake inhibitor desvenlafaxine may improve scores for multiple symptom clusters in patients with MDD. Further, we hypothesized that early improvement in symptom clusters may predict treatment outcomes, as reported for overall symptom improvement.
Methods
Data were pooled from nine multicenter, randomized, double-blind, placebo-controlled studies of desvenlafaxine for the treatment of MDD (Supplemental Table S1; Boyer et al., 2008; Clayton et al., 2013, 2015; DeMartinis et al., 2007; Dunlop et al., 2011; Iwata et al., 2013; Liebowitz et al., 2008, 2013; Tourian et al., 2009). Studies that met criteria for inclusion in the analysis were all Phase II, III, or IV, fixed-dose, placebo-controlled MDD studies conducted by the sponsor (Pfizer, Inc.) that included, at a minimum, desvenlafaxine 50 and/or 100 mg dose arms and placebo. Several studies had additional treatment arms (desvenlafaxine 200 and 400 mg, DeMartinis et al., 2007; duloxetine 60 mg, Tourian et al., 2009; desvenlafaxine 25 mg, Iwata et al., 2013; desvenlafaxine 10 mg, Liebowitz et al., 2013). Any treatment arm other than desvenlafaxine 50 or 100 mg or placebo were excluded from the analysis. Each study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki, and all study protocols were consistent with Principles of Good Clinical Practice and applicable regulatory requirements in each participating country.
Patient demographics and baseline characteristics: intent-to-treat population. a .
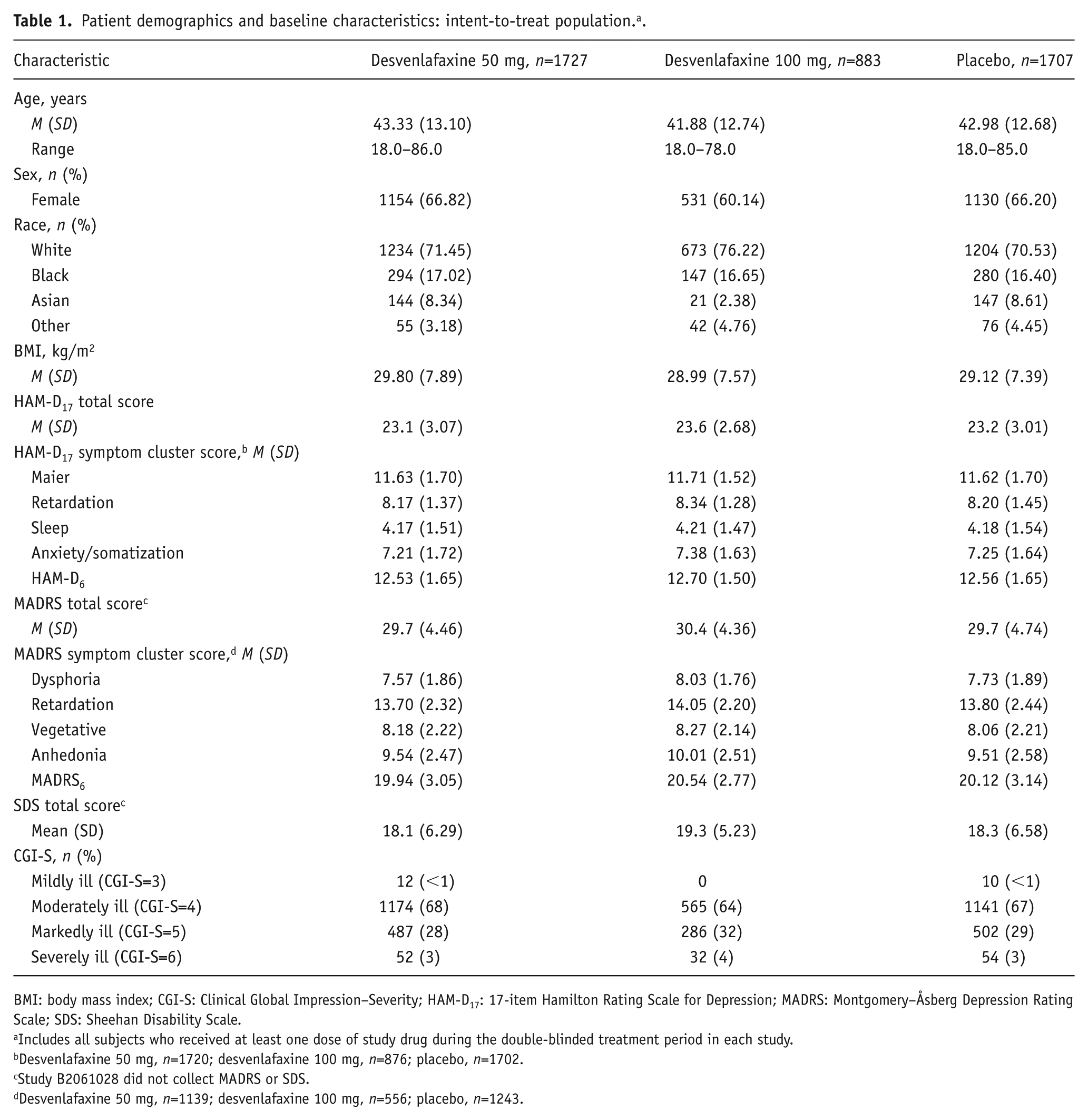
BMI: body mass index; CGI-S: Clinical Global Impression–Severity; HAM-D17: 17-item Hamilton Rating Scale for Depression; MADRS: Montgomery–Åsberg Depression Rating Scale; SDS: Sheehan Disability Scale.
Includes all subjects who received at least one dose of study drug during the double-blinded treatment period in each study.
Desvenlafaxine 50 mg, n=1720; desvenlafaxine 100 mg, n=876; placebo, n=1702.
Study B2061028 did not collect MADRS or SDS.
Desvenlafaxine 50 mg, n=1139; desvenlafaxine 100 mg, n=556; placebo, n=1243.
Patients
All included studies enrolled adult outpatients, aged 18 years or older or 20 years or older for patients in Japan; one enrolled perimenopausal and postmenopausal women aged 40–70 years (Clayton et al., 2013). Patients in each study had a diagnosis of MDD based on the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (American Psychiatric Association, 1994) or fourth edition, text revision (American Psychiatric Association, 2000) depressive symptoms for at least 30 days before screening, and a minimum baseline HAM-D17 total score of 20 (seven studies) or baseline MADRS score of 25 (two studies). One study required participants to be gainfully employed and to have a Sheehan Disability Scale (SDS; Sheehan, 2000) score of at least 10 at screening and baseline (Dunlop et al., 2011). Each study excluded patients who had a lifetime diagnosis of bipolar or psychotic disorder, or other comorbid psychiatric disorders (except generalized anxiety disorder, panic disorder, or social anxiety disorder, not considered primary), clinically important abnormalities on screening physical examinations (including vital signs and electrocardiograms), a significant risk of suicide, or current psychoactive substance abuse or dependence. Inclusion and exclusion criteria for the pooled studies are detailed in the Supplemental Appendix.
Study design
Patients were randomly assigned to receive short-term treatment with placebo or a fixed dose of desvenlafaxine (10, 25, 50, 100, 200, or 400 mg) in each study (or duloxetine in one study). Seven studies were eight weeks in duration, one study (Clayton et al., 2013) was 10 weeks in duration with week 8 as the primary endpoint, and one study (Dunlop et al., 2011) was 12 weeks in duration. Patients assigned to the desvenlafaxine 50 mg dose received their assigned dose on study day 1. Patients assigned to the desvenlafaxine 100 mg dose received their first assigned dose on day 1 (one study: DeMartinis et al., 2007) or on day 8 after a one-week titration with desvenlafaxine 50 mg (four studies: Boyer et al., 2008; Clayton et al., 2015; Liebowitz et al., 2008; Tourian et al., 2009). The primary efficacy outcome in each trial was change from baseline in HAM-D17 total score at week 8, except for the 12-week study, which had a week 12 primary endpoint. MADRS and SDS were administered in all but one study (Clayton et al., 2015); data from that study were included for HAM-D17 analyses only.
Outcome measures
Symptom clusters in this analysis, selected to encompass a range of MDD symptoms, were based on HAM-D17 and MADRS factors and subscales previously defined in the literature. The HAM-D17 clusters included Maier (items 1, 2, 7, 8, 9, and 10; Maier and Philipp, 1985), retardation (items 1, 7, 8, and 14; Cleary and Guy, 1977), sleep (items 4, 5, and 6; Cleary and Guy, 1977), anxiety/somatization (items 10, 11, 12, 13, 15, and 17; Cleary and Guy, 1977), and HAM-D6 (items 1, 2, 7, 8, 10, and 13; Bech et al., 1975). The MADRS clusters included dysphoria (items 2, 9, and 10; Suzuki et al., 2005), retardation (items 1, 6, 7, and 8; Suzuki et al., 2005), vegetative (items 3, 4, and 5; Suzuki et al., 2005), anhedonia (items 5, 7, 8, and 10; McIntyre et al., 2016), and MADRS6 (items 1, 2, 3, 7, 8, and 9; Bech et al., 2002). For each symptom cluster, early improvement was defined as 20% or greater improvement from baseline in that symptom cluster score at week 2, based on previously published analyses of early improvement (Habert et al., 2016).
Several definitions of remission have been used in published research relating to the goals of MDD treatment. Remission from symptoms and functional recovery (or functional remission) differ in their time course and are measured using separate tools (Frank et al., 1991; Hirschfeld et al., 2002; Sheehan et al., 2011; Zimmerman, 2004). To be inclusive, multiple definitions of remission were used in the current analysis. Symptomatic remission at week 8 was defined as (a) a HAM-D17 total score of ⩽7 (Frank et al., 1991) at week 8 and (b) a MADRS total score of ⩽10 (Zimmerman et al., 2004) at week 8. Functional remission was defined as a SDS total score of <7 at week 8 (Soares et al., 2014a). Symptomatic/functional remission was defined as (a) a HAM-D17 total score of ⩽7 and a SDS total score of <7 at week 8 and (b) a MADRS total score of ⩽10 and a SDS total score of <7 at week 8. The HAM-D17 remission definitions were used for HAM-D symptom cluster analyses, and the MADRS remission definitions were used for MADRS symptom cluster analyses. MADRS symptom cluster analyses were repeated using an alternate definition of MADRS remission (MADRS total score ⩽12; Zimmerman et al., 2004).
Statistical analysis
The full analysis set included all patients who received at least one dose of study drug during the double-blinded treatment period. No imputation was done for missing item scores in symptom clusters; if any HAM-D17 or MADRS item scores included in a cluster were missing, the cluster score was set to missing. A 20% imputation rule was applied for missing items in HAM-D17 and MADRS total scores calculation. If ⩽20% of items in the scale were missing, the total score was imputed with the average of the available items multiplied by the total number of the items in the scale. Otherwise, the total score was set to missing. If any SDS item score (work/school, social life, and family life/home responsibilities) was missing, the SDS total score was set to missing. The last observation carried forward (LOCF) approach was used for missing cluster score or total score at week 8 for HAM-D17, MADRS, and SDS, but no imputation was applied to week 2 scores. Patients were excluded from the analysis of early improvement for a particular symptom cluster if they were missing week 2 data for that symptom cluster.
Change from baseline in each of the five HAM-D17 clusters’ scores at week 8/LOCF was analyzed using analysis of covariance (ANCOVA) models with terms for treatment, baseline HAM-D17 total score, and study. Similarly, change from baseline in each of the 5 MADRS clusters’ scores at week 8/LOCF was analyzed using ANCOVA with terms for treatment, baseline MADRS total score, and study. The association between early improvement in symptom cluster score at week 2 and depression and/or functional remission at week 8 was examined using logistic regression models. For each definition of remission, the proportion of patients achieving remission among those with versus without early improvement was presented for each symptom cluster by treatment group. Odds ratios (ORs) and 95% confidence intervals for each definition of remission for patients with versus without early improvement were estimated using logistic regression models for each cluster of HAM-D17 symptoms and each cluster of MADRS symptoms. The model for each definition of remission included terms for study, treatment, early improvement in the symptom cluster (yes or no), and the interaction of treatment and early improvement.
Results
Patients
The full analysis set for the nine pooled studies included 4317 patients (desvenlafaxine 50 mg, n=1727; desvenlafaxine 100 mg, n=883; placebo, n=1707). Analyses based on MADRS and SDS endpoints (i.e. without study 1028) included 3408 patients (desvenlafaxine 50 mg, n=1427; desvenlafaxine 100 mg, n=574; placebo, n=1407). Demographic and baseline characteristics were generally similar across treatment groups (Table 1). In the full analysis set, 65% of patients were women, and 72% of patients were white. More than 95% of patients in each treatment group were moderately ill (Clinical Global Impression–Severity=4) or markedly ill (Clinical Global Impression–Severity=5) at baseline.
Improvement in symptom clusters, week 8/LOCF
Patients receiving 50 or 100 mg desvenlafaxine had significantly greater improvement from baseline at week 8/LOCF in all HAM-D17 symptom clusters compared to patients receiving placebo (p<0.001), with the exception of the HAM-D17 sleep cluster. For that cluster, the desvenlafaxine 50 mg group separated statistically from placebo (p=0.0004), but the desvenlafaxine 100 mg group did not reach statistical significance (p=0.0681). Desvenlafaxine doses of 50 and 100 mg were both associated with significantly greater improvement from baseline at week 8/LOCF in all MADRS symptom clusters compared to placebo (p<0.001). Change from baseline HAM-D17 and MADRS symptom cluster scores at week 8/LOCF are presented by treatment group in Table 2.
Effect of desvenlafaxine (50 or 100 mg) versus placebo on HAM-D17 and MADRS symptom clusters at week 8 (LOCF). a
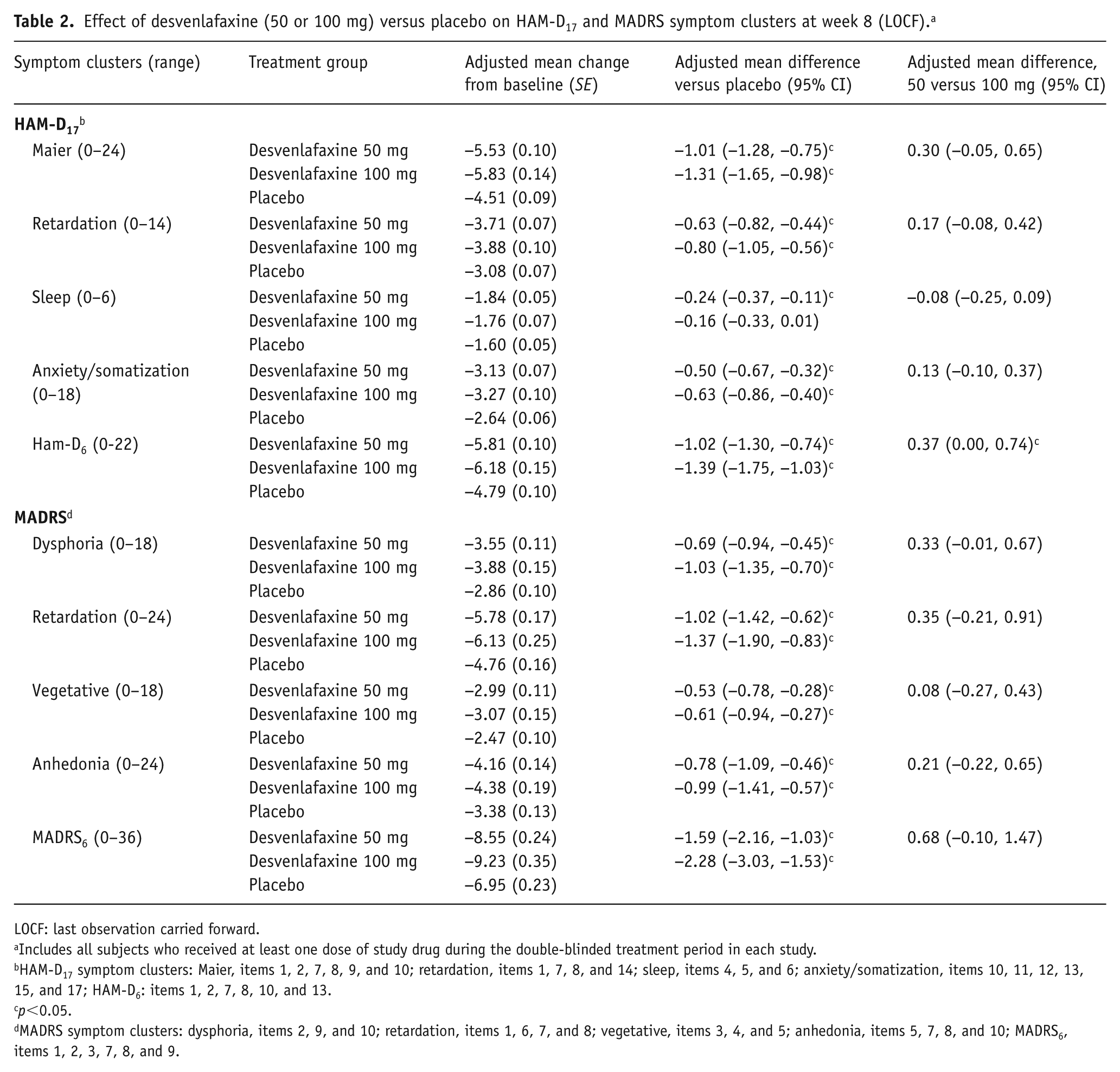
LOCF: last observation carried forward.
Includes all subjects who received at least one dose of study drug during the double-blinded treatment period in each study.
HAM-D17 symptom clusters: Maier, items 1, 2, 7, 8, 9, and 10; retardation, items 1, 7, 8, and 14; sleep, items 4, 5, and 6; anxiety/somatization, items 10, 11, 12, 13, 15, and 17; HAM-D6: items 1, 2, 7, 8, 10, and 13.
p<0.05.
MADRS symptom clusters: dysphoria, items 2, 9, and 10; retardation, items 1, 6, 7, and 8; vegetative, items 3, 4, and 5; anhedonia, items 5, 7, 8, and 10; MADRS6, items 1, 2, 3, 7, 8, and 9.
Comparison between desvenlafaxine 50 and 100 mg groups was statistically significantly different for HAM-D6 cluster (adjusted mean (SE) change from baseline: desvenlafaxine 50 mg, −5.81 (0.10); desvenlafaxine 100 mg, −6.18 (0.15); p=0.0495). No other significant differences between desvenlafaxine dose groups were observed for HAM-D17 or MADRS symptoms clusters.
Association between early improvement and week 8/LOCF remission
Proportions of patients who achieved early improvement (week 2) in HAM-D17 symptom cluster scores were in the range 52–58% in the desvenlafaxine groups compared to 45–49% in the placebo group. Similarly, the proportions of patients who achieved early improvement (week 2) in MADRS symptom cluster scores were in the range 47–61% in the desvenlafaxine groups compared to 40–49% in the placebo group. Proportions of patients who achieved symptomatic, functional, and symptomatic/functional remission at week 8/LOCF are shown by treatment in Figure 1. As expected, greater proportions of patients achieved MADRS remission using the less stringent MADRS definition (MADRS total score ⩽12 vs. MADRS total score ⩽10).
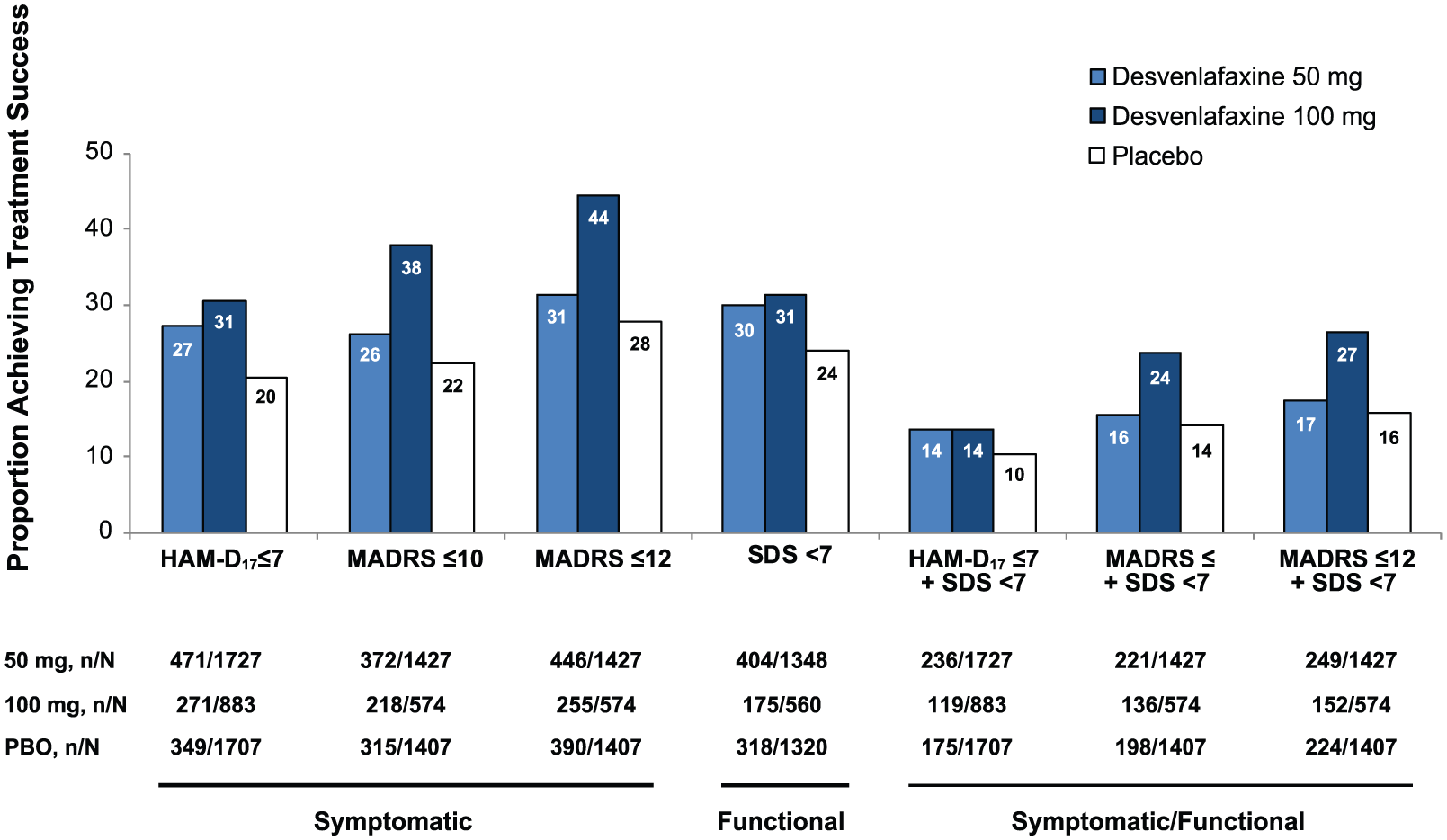
Proportions of patients who achieved remission for each definition, by treatment.
Early improvement on each HAM-D17 and MADRS symptom cluster score was significantly associated with achievement of remission at week 8/LOCF (overall, p<0.0001). In each treatment group, symptomatic (HAM-D17 or MADRS), functional (SDS), and symptomatic (HAM-D17 or MADRS) combined with functional remission (SDS) were all significantly predicted by week 2 improvement in symptom cluster scores (p⩽0.0254). The ORs of symptomatic remission for early symptom cluster improvement versus non-early improvement ranged from 1.40 to 6.94 (HAM-D17 symptom clusters, Figure 2; MADRS symptom clusters, Figure 3). The ORs with versus without early symptom improvement were generally higher for symptomatic remission versus functional remission for both HAM-D17 and MADRS symptom clusters. The ORs were smallest for the HAM-D17 sleep symptom cluster for each definition of remission. No notable differences in the magnitude of ORs were observed based on the less stringent definition of MADRS remission (MADRS total score ⩽12; MADRS Supplemental Figure 1); early improvement in all symptom clusters was significantly associated with MADRS remission and MADRS and functional remission (p<0.0001).
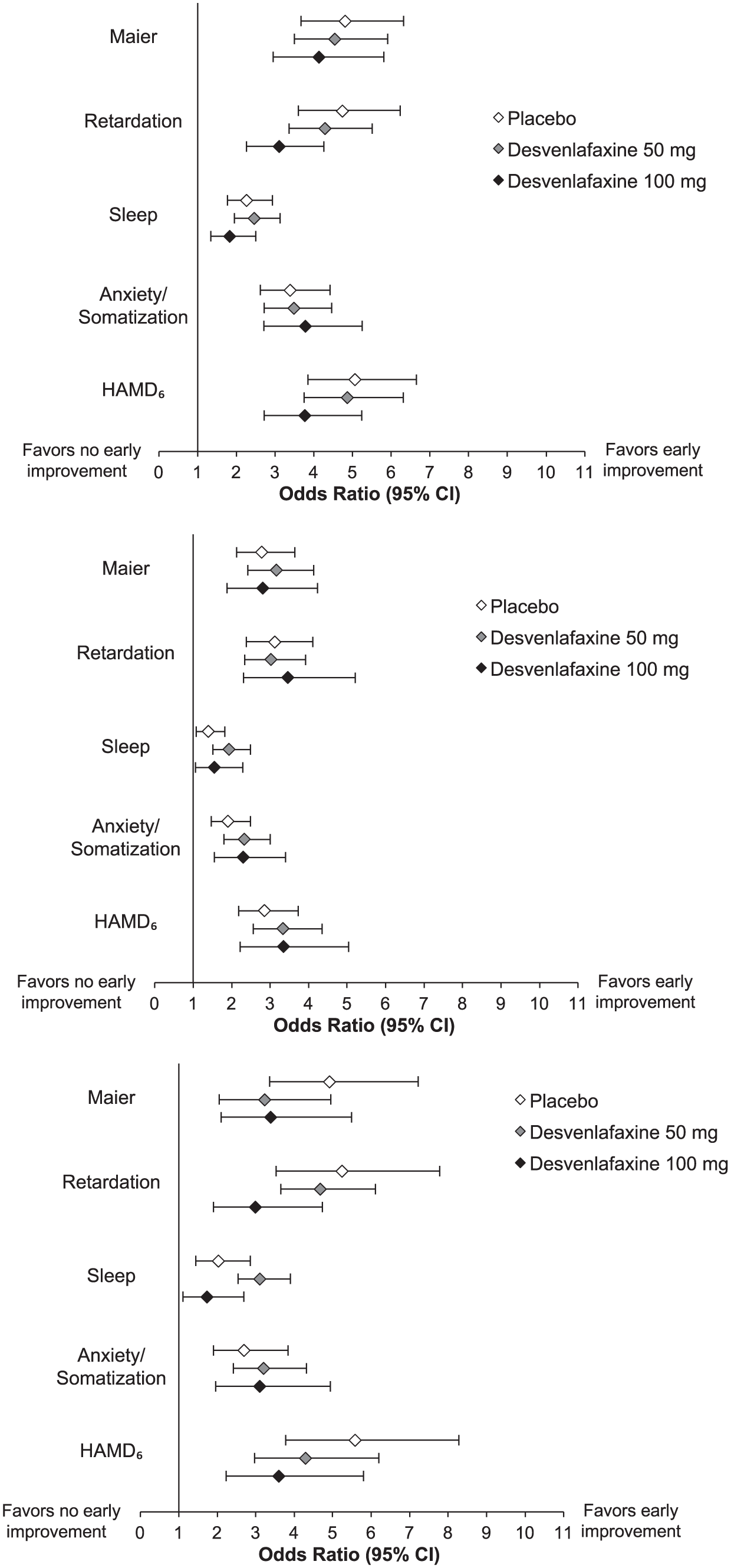
Forest plots of odds ratios (95% CI) for probability of remission at week 8/LOCF in those with early improvement versus those without early improvement in HAM-D17 symptom cluster scores, based on logistic regression analysis.
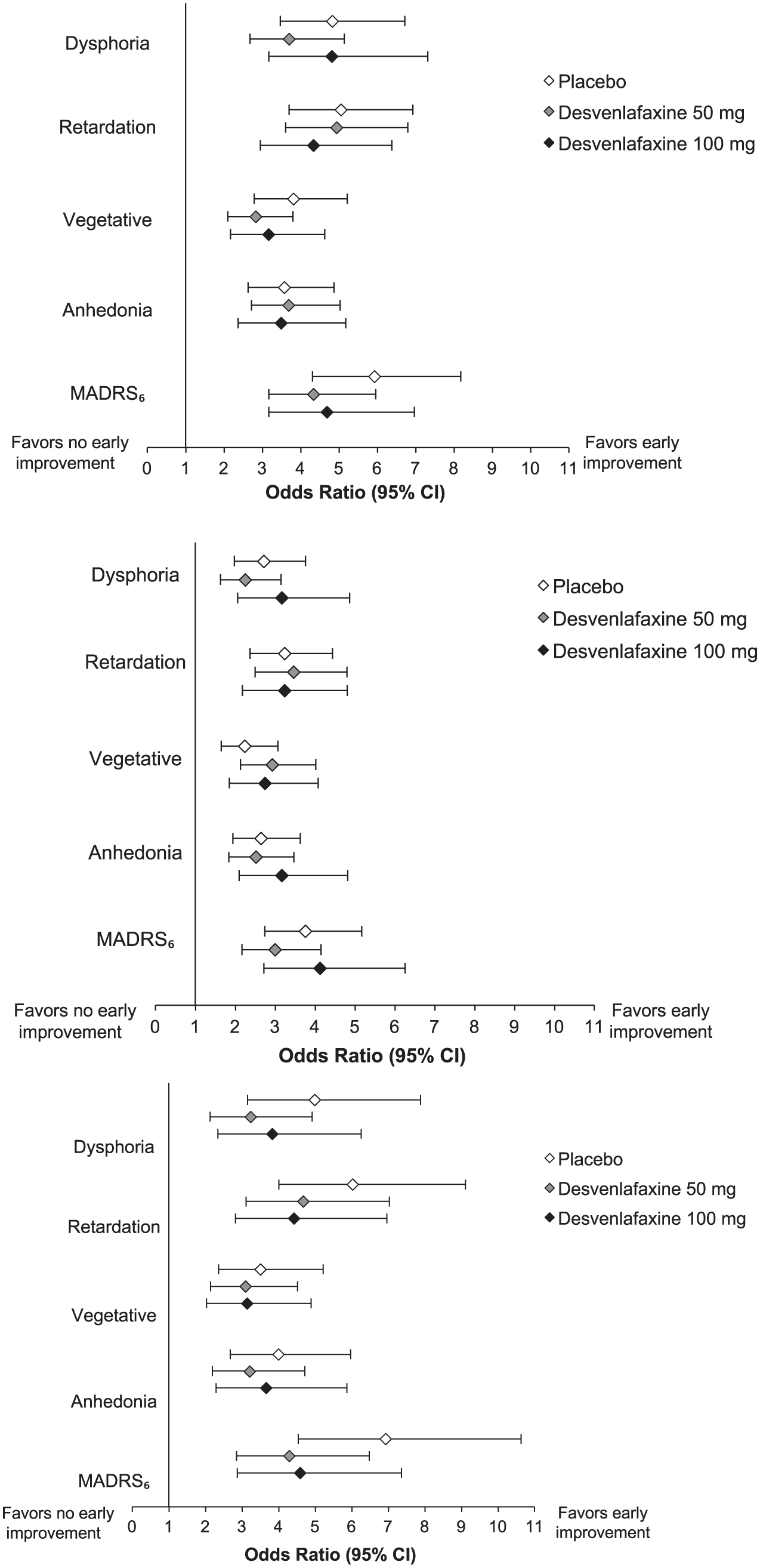
Forest plots of odds ratios (95% CI) for probability of remission at week 8/LOCF in those with early improvement versus those without early improvement in MADRS symptom cluster scores, based on logistic regression analysis.
There were no significant effects of the interaction between treatment and early improvement. Although early improvement was associated with an increased likelihood of achieving symptomatic and/or functional remission at week 8/LOCF for each treatment group, there were significant differences between desvenlafaxine and placebo in week 8/LOCF remission rates in both early improvers and patients without early improvement (Table 3). Among patients with early improvement in all HAM-D17 symptom clusters, treatment with desvenlafaxine 50 or 100 mg was associated with significantly higher rates of HAM-D17 remission compared to placebo at week 8/LOCF (p⩽0.0384). Similar MADRS remission rates were observed on early improvement in MADRS symptom clusters for the desvenlafaxine 100 mg dose (p⩽0.0085 vs. placebo). However, significantly higher MADRS remission rates were observed for desvenlafaxine 50 mg versus placebo only among patients who had early improvement in the anhedonia symptom cluster (p=0.0098).
Proportion of patients who achieved symptomatic remission, functional remission, or symptomatic/functional remission at week 8/LOCF for patients with versus without early improvement in symptom clusters.
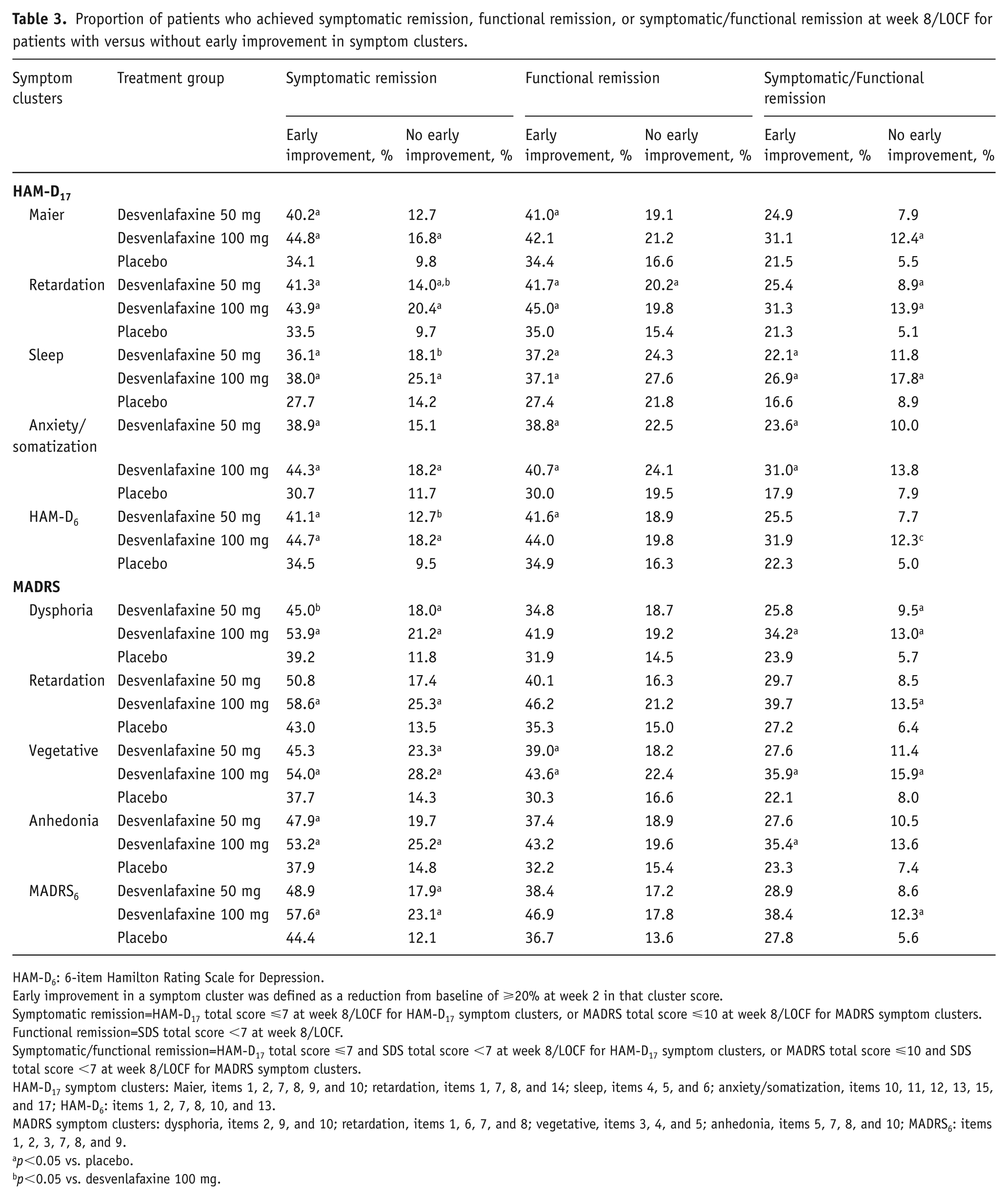
HAM-D6: 6-item Hamilton Rating Scale for Depression.
Early improvement in a symptom cluster was defined as a reduction from baseline of ⩾20% at week 2 in that cluster score.
Symptomatic remission=HAM-D17 total score ⩽7 at week 8/LOCF for HAM-D17 symptom clusters, or MADRS total score ⩽10 at week 8/LOCF for MADRS symptom clusters.
Functional remission=SDS total score <7 at week 8/LOCF.
Symptomatic/functional remission=HAM-D17 total score ⩽7 and SDS total score <7 at week 8/LOCF for HAM-D17 symptom clusters, or MADRS total score ⩽10 and SDS total score <7 at week 8/LOCF for MADRS symptom clusters.
HAM-D17 symptom clusters: Maier, items 1, 2, 7, 8, 9, and 10; retardation, items 1, 7, 8, and 14; sleep, items 4, 5, and 6; anxiety/somatization, items 10, 11, 12, 13, 15, and 17; HAM-D6: items 1, 2, 7, 8, 10, and 13.
MADRS symptom clusters: dysphoria, items 2, 9, and 10; retardation, items 1, 6, 7, and 8; vegetative, items 3, 4, and 5; anhedonia, items 5, 7, 8, and 10; MADRS6: items 1, 2, 3, 7, 8, and 9.
p<0.05 vs. placebo.
p<0.05 vs. desvenlafaxine 100 mg.
Functional remission results for early improvers based on the HAM-D17 symptom clusters were generally consistent with the symptomatic remission findings. For patients with early improvement in any HAM-D17 symptom cluster, rates of functional remission at week 8/LOCF were significantly higher for desvenlafaxine 50 mg versus placebo groups (p⩽0.0089). Desvenlafaxine 100 mg was associated with higher functional remission rates versus placebo in patients with early improvement in retardation, sleep, and anxiety/somatization symptom clusters (p⩽0.0303). For MADRS symptom clusters, however, significant differences in functional remission rates between desvenlafaxine versus placebo were observed only in patients with early improvement in vegetative symptoms (desvenlafaxine 50 mg vs placebo, p=0.0121; desvenlafaxine 100 mg vs placebo, p=0.0175).
In the analysis of symptomatic/functional remission, few differences between desvenlafaxine and placebo groups were observed in patients who had early symptom cluster score improvement. Both dose groups had significantly higher rates of symptomatic/functional remission at week 8/LOCF compared to placebo in patients with early improvement in HAM-D17 sleep or anxiety/somatization symptoms (p⩽0.0274), and desvenlafaxine 100 mg separated from placebo in patients with early improvement in MADRS dysphoria, vegetative, or anhedonia symptoms (p⩽0.0478).
Among patients who did not have early improvement in symptom cluster scores at week 2, the pattern of significant effects of desvenlafaxine versus placebo were generally similar to those for patients who did have early improvement. However, there were fewer statistically significant differences between treatment groups in non-early improvers overall, mainly because there was only a single observed difference between groups for rates of functional remission (Table 3).
In the analyses based on the less stringent MADRS definition of remission (MADRS total ⩽12), statistically significant separation between desvenlafaxine and placebo groups was observed for all clusters among both early improvers and non-early improvers, with only two exceptions: desvenlafaxine 50 mg did not separate from placebo in early improvers for MADRS6 or in non-early improvers for the retardation symptom cluster (Supplemental Table 2), For symptomatic/functional remission using the less stringent MADRS definition, the pattern of differences between groups was similar to the results for MADRS total ⩽10.
Few significant differences between desvenlafaxine 50 and 100 mg groups were observed in remission rates, either in patients who had early improvement in symptom clusters or in those who did not. Significantly higher rates of symptomatic remission were observed in patients taking desvenlafaxine 100 mg versus those taking 50 mg among those without early improvement in HAM-D17 retardation, sleep, or HAM-D6 symptom cluster scores (p⩽0.0482). A single significant dose-group comparison was observed for MADRS symptom clusters (significantly higher MADRS total ⩽10 remission rates with desvenlafaxine 100 mg versus 50 mg in patients with early improvement in dysphoria symptom cluster score; p=0.0189). No significant dose-group differences in functional or symptomatic/functional remission rates were observed. In analyses based on the less stringent MADRS definition of remission (MADRS total ⩽12), no significant dose-group differences were observed for any comparison (Supplemental Table 2).
Discussion
Several meta-analyses have previously assessed the efficacy of desvenlafaxine at the population level based on HAM-D17 total score or remission rates (Carrasco et al., 2016; Laoutidis and Kioulos, 2015; Thase et al., 2009). Overall, desvenlafaxine is associated with significant improvement on efficacy measures. However, the observed remission rates are <50% for desvenlafaxine-treated patients, indicating that there are individual differences among MDD patients in responsiveness to this drug (Carrasco et al., 2016; Laoutidis and Kioulos, 2015; Thase et al., 2009). The question of whether differences in symptom profile or early symptom improvement could potentially identify those patients likely to benefit from a given drug was explored in this pooled analysis. In this post hoc analysis of pooled data from nine placebo-controlled clinical trials, eight-week treatment with desvenlafaxine significantly improved symptom cluster scores compared to placebo. All symptom clusters scores improved significantly versus placebo in both the desvenlafaxine 50 and 100 mg groups, with one exception: the sleep cluster score did not separate from placebo at the higher desvenlafaxine dose (p=0.0681). The only significant difference between dose groups in symptom cluster scores at week 8/LOCF was a greater mean improvement in HAM-D6 for patients treated with desvenlafaxine 100 mg versus 50 mg. The prescribing information for desvenlafaxine indicates that no additional benefit has been observed in clinical trials for doses >50 mg (Pristiq package insert, 2018). However, in the clinical setting (Redrobe et al., 1998), some patients may benefit from an increased dose.
Numerically greater proportions of patients in the desvenlafaxine groups showed early improvement in symptom cluster scores at week 2 compared to patients in the placebo group, and early symptom improvement was significantly associated with higher rates of remission at week 8/LOCF. Multiple mechanisms have been hypothesized to explain the time course of symptom improvement in MDD, including changes to neural circuits at the receptor level through desensitization of presynaptic receptors, downregulation of neurotransmitter transporters or postsynaptic autoreceptor signaling, or remodeling via neurogenesis and neuroplasticity (Celada et al., 2004; Frazer and Benmansour, 2002; Lam, 2012; Machado-Vieira et al., 2010; MacQueen and Frodl, 2011; Wainwright and Galea, 2013). However, further research would be needed to relate such mechanisms to the predictive association between early improvement and later treatment outcomes. In fact, previous analyses have demonstrated that whether patients achieved early improvement while taking active drug or placebo, their odds of treatment success with continued therapy are increased compared to patients without early improvement (Soares et al., 2014a, 2014b). Early improvement in symptom cluster scores in the current analysis also predicted later remission regardless of treatment group, with no significant interaction between improvement (yes or no) and treatment. However, differences in rates of remission favoring desvenlafaxine over placebo were observed. For most symptom clusters, desvenlafaxine doses of 50 and 100 mg were associated with significantly higher rates of symptomatic remission compared to placebo in patients with early symptom improvement. Rates of functional remission were generally higher for desvenlafaxine- versus placebo-treated patients who had early improvement in HAM-D17 symptom clusters, but fewer effects of treatment were noted in the MADRS symptom cluster analysis.
Early symptom improvement based on HAM-D17 factor subscales was investigated previously as a predictor of successful treatment outcome in an analysis that compared two drugs for depression (duloxetine and escitalopram; Katz et al., 2009). In that study, the investigators hypothesized that the two drugs would be associated with different sets of symptoms for which improvement predicted treatment success. Indeed, while early improvement in most subscale scores predicted sustained remission for either drug, improvement in HAM-D17 sleep scores predicted treatment success in patients treated with escitalopram but not in those treated with duloxetine. In the current analysis, the predictive effect of early symptom improvement was observed for each HAM-D17 and MADRS symptom cluster. The odds of remission with versus without early symptom improvement were generally greater for symptomatic remission than for functional remission, but results based on the different definitions of remission point to the same conclusions: for all symptom clusters, early improvement was predictive of each definition of remission (symptomatic, functional, or symptomatic/functional, and based on either HAM-D17 or MADRS).
Although improvement in each symptom cluster had predictive value in this analysis, some notable differences were observed for the HAM-D17 sleep symptom cluster. The predictive effect of early improvement was weakest for the sleep cluster in this analysis. The percentages of patients who achieved early improvement were similar or higher for this cluster compared to other HAM-D17 clusters, suggesting that the difference in predictive value of sleep symptoms was not due to a lag in their improvement. The HAM-D17 sleep cluster was also the only symptom cluster (HAM-D17 or MADRS) for which the difference between desvenlafaxine and placebo at week 8/LOCF was not significant. It may be that although they may begin to improve with treatment, sleep symptoms require longer than eight weeks to be fully addressed or are more resistant to treatment compared to other symptoms. Symptoms such as insomnia and fatigue are among the most commonly reported residual symptoms in patients treated for depression (Shelton et al., 2007). Further, treatment with drugs for depression may itself contribute to sleep symptoms in some patients, as the majority of drugs for depression are associated with either insomnia or somnolence as adverse events (Alberti et al., 2015); drugs with serotonergic and noradrenergic activity may disrupt sleep behavior (Mitchell and Weinshenker, 2010; Stahl, 1998). Indeed, both insomnia and somnolence are among the most common adverse events reported in patients treated with desvenlafaxine in clinical trials (Kornstein et al., 2014). It should also be noted, however, that among the five HAM-D clusters, the sleep cluster had the narrowest range of possible scores (0–6 vs. 0–14 to 0–24 for other clusters), and that narrow range could reduce the likelihood of observing statistically significant differences between treatment groups.
The predictive value of symptom cluster improvement is clinically important for the use of measurement-based care in managing patients with MDD. In patients whose symptoms are assessed at baseline and monitored over the course of treatment, early improvement in symptoms, or the lack thereof, can inform treatment decisions (Habert et al., 2016). Previous predictor analyses that examined operating characteristics of early improvement for predicting remission have shown that negative predictive value generally exceeds positive predictive value, meaning that failure to meet threshold improvement is a more accurate predictor of a negative treatment outcome than meeting the improvement threshold is for predicting treatment success (Gorwood et al., 2013; Habert et al., 2016; Soares et al., 2014a, 2014b). A patient’s failure to show symptom improvement after the first few weeks of treatment might prompt the clinician to consider changes to the treatment plan (Habert et al., 2016; Soares et al., 2014a). In the current analysis, generally <20% of patients without early symptom improvement achieved remission with continued treatment to week 8. However, patients who do show early improvement in symptoms should be followed closely nonetheless: >50% of early improvers in this analysis did not ultimately achieve remission at week 8.
Several important limitations of this analysis should be considered. This was a post hoc analysis of data from studies that were not specifically designed to examine the effect of early improvement on later outcomes. In addition, although the full HAM-D17 and MADRS scales were included as efficacy outcomes in the pooled studies, none of the studies were designed to assess subscales or factors. The results of this analysis are also limited by differences between studies in their design, which may have contributed to variability in the data. The exclusion of study 1028 from analyses based on MADRS and SDS data may underlie some of the differences in findings for HAM-D17 versus MADRS clusters. Although a dose comparison was included in the analysis, no conclusions regarding the effect of dose were drawn, as the pooled studies were not designed to allow optimal dose treatment or to test for differences between dose groups. Patients included in the analysis were those who met the eligibility criteria for enrollment in the pooled studies. Thus, findings may or may not generalize to a broader patient population. Finally, it should be noted that in this analysis, symptom clusters were defined by grouping items on the depression scales and were not based on sets of patients grouped based on similarities in their baseline symptom scores (Schacht et al., 2014).
Conclusion
Desvenlafaxine doses of 50 and 100 mg were associated with significant improvement compared to placebo in HAM-D17 and MADRS symptom clusters at week 8/LOCF. Early improvement on each symptom cluster score was a significant predictor of achievement for all definitions of remission at week 8/LOCF for each treatment group. The proportion of patients who achieved each definition of remission at week 8/LOCF overall was significantly greater for desvenlafaxine (50 or 100 mg) versus placebo, and both desvenlafaxine dose groups separated from placebo among early improvers for most symptom clusters, and among non-early improvers for some symptom clusters. Previous analyses have shown the benefit of measurement-based care approach to managing MDD by administering depression and function scales at baseline and during therapy. These results expand on those findings to demonstrate that monitoring improvement in symptom clusters can similarly help guide treatment decisions for individual patients. We know that with any given drug for depression, less than half of MDD patients treated will achieve remission (Machado et al., 2006). Identifying key features that will indicate at baseline or early in treatment which subsets of patients are likely to respond to a particular drug is therefore a critical research goal. If clinicians can understand what differentiates early responders from nonresponders, they can increase their chances of prescribing effective medications early in treatment, with the prospect of meaningfully improving patient outcomes. Our analysis contributes to an understanding of how MDD patients’ symptom profiles may both inform treatment selection and aid in monitoring progress toward a goal of full functional recovery.
Supplemental Material
Supplemental_Table,_Figure_files,_appendix_for_submission – Supplemental material for Effects of desvenlafaxine versus placebo on MDD symptom clusters: A pooled analysis
Supplemental material, Supplemental_Table,_Figure_files,_appendix_for_submission for Effects of desvenlafaxine versus placebo on MDD symptom clusters: A pooled analysis by Martin A Katzman, Xuemei Wang, Dalia B Wajsbrot and Matthieu Boucher in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.B. was an employee of Pfizer Canada, Inc., at the time of the study and owns Pfizer stock. D.W. is a full-time employee of Pfizer and owns stocks and options from Pfizer. M.A.K.’s financial interests/affiliations in the past two years include: START Clinic, 1 Datapoint, Talking Touch, Canopy, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Forrest/Actavis/Allergan, Janssen, Lundbeck, Merck, Otsuka, Pfizer, Purdue, Shire, Sunovion, AstraZeneca, Biotics, Genuine Health, Takeda, Canadian Foundation for Innovation, and Lotte & John Hecht Memorial Foundation. X.W. is a full-time employee of Syneos Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medical writing support was provided by Kathleen M. Dorries, PhD, at Peloton Advantage, an OPEN Health company, and was funded by Pfizer, Inc.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.