
Abstract
Background:
Sarcosine (N-methylglycine), a type 1 glycine transporter inhibitor (GlyT1), has shown therapeutic potential for treating schizophrenia; however, studies have reported conflicting results. This meta-analysis aimed to explore the efficacy and cognitive effect of sarcosine for schizophrenia.
Methods:
In this study, PubMed, Cochrane Systematic Reviews, and Cochrane Collaboration Central Register of Controlled Clinical Trials were searched electronically for double-blinded randomised controlled trials that used sarcosine for treating schizophrenia. We used the published trials up to November 2019 to investigate the efficacy of sarcosine in schizophrenia. We pooled studies by using a random-effect model for comparing sarcosine treatment effects. Patients who were diagnosed with schizophrenia according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition were recruited. Clinical improvement and cognitive function scores between baseline and after sarcosine use were compared using the standardised mean difference (SMD) with 95% confidence intervals (CIs). The heterogeneity of the included trials was evaluated through visual inspection of funnel plots and through the I2 statistic.
Results:
We identified seven trials with 326 participants with schizophrenia meeting the inclusion criteria. All these studies evaluated the overall clinical symptoms, and four of them evaluated overall cognitive functions. Sarcosine use achieved more significant effects than the use of its comparators in relieving overall clinical symptoms (SMD = 0.51, CI = 0.26–0.76, p < 0.01). Moreover, studies with the low Positive and Negative Syndrome Scale range of 70–79 showed significant effect size (ES)s of 0.67 (95% CI: 0.03–1.31, p = 0.04). In addition, trials enrolling patients with stable clinical symptoms had significant ESs: 0.53 (95% CI: 0.21–0.85, p < 0.01). Add-on sarcosine combined with first- and second-generation antipsychotics, except clozapine, had a positive effect. For overall cognitive functions, sarcosine showed a positive but insignificant effect compared with its comparators (SMD = 0.27, CI = −0.06 to 0.60, p = 0.10). The effects were correlated with increased female proportions and decreased illness duration, albeit nonsignificantly.
Conclusions:
The meta-analysis suggests that sarcosine may be associated with treatment effect on overall clinical symptoms in patients with schizophrenia but not cognitive functions.
Introduction
Schizophrenia is a chronic and complicated psychotic disorder characterised by cognitive deficits that places a great burden on patients, their families, and society (Freedman, 2003). Studies have shown that the hypofunction of the N-methyl-D-aspartate (NMDA) glutamate receptor may be a critical mechanism in schizophrenia (Coyle, 1996; Olney and Farber, 1995). NMDA receptors are composed of one or two GluN1 subunits and two or three GluN2 subunits (Beesley et al., 2019; Hollmann and Heinemann, 1994). After binding of agonists such as L-glycine or D-serine to GluN1 or GluN3 subunits and glutamate to GluN2 subunits, NMDA receptors activate ligand-gated cationic channels. NMDA receptors mediate glutamatergic excitatory neurotransmission and induce synaptic plasticity related to learning and memory (Nakazawa et al., 2004). This hypothesis of the hypofunction of NMDA receptors in schizophrenia is supported by studies on noncompetitive NMDA receptor antagonists such as ketamine and phencyclidine. In animal and human studies, ketamine has shown an ability to induce positive, negative, and cognitive symptoms (Krystal et al., 1994; Lieberman et al., 2008; Malhotra et al., 1996). Moreover, ketamine causes psychotic symptoms in patients with schizophrenia (Malhotra et al., 1997). In addition, in anti-NMDA receptor encephalitis, antibodies cross-react with NMDA receptors, which may cause psychotic symptoms such as first-episode psychosis in schizophrenia (Dalmau et al., 2008). Moreover, the abnormality of NMDA glutamate receptors has been noted in brains post mortem (Ibrahim et al., 2000; Meador-Woodruff and Healy, 2000). NMDA glutamate receptor expression was lower in the thalamus of patients with schizophrenia than in controls (Ibrahim et al., 2000). These findings imply that the hypofunction of NMDA neurotransmission may cause psychotic symptoms and cognitive deficits in schizophrenia (Javitt et al., 1999). Therefore, improving the hypofunction of NMDA neurotransmission may benefit both psychotic symptoms and cognitive functions in schizophrenia.
Sarcosine (also known as N-methylglycine) is a competitive inhibitor of the type 1 glycine transporter (GlyT1) (Lopez-Corcuera et al., 1998) and an NMDA receptor glycine site coagonist (Zhang et al., 2009). Studies have investigated the use of sarcosine with respect to its treatment effect in patients with schizophrenia. However, the results of these trials are conflicting. Five studies (Amiaz et al., 2015; Lane et al., 2005, 2010; Strzelecki et al., 2018b; Tsai et al., 2004) found significant improvement in clinical symptoms, whereas three trials (Lane et al., 2006, 2008; Lin et al., 2017) did not. Singh and colleagues evaluated the efficacy of adjunctive NMDA receptor modulators in chronic schizophrenia (Singh and Singh, 2011). They examined four sarcosine trials (Lane et al., 2005, 2006, 2008; Tsai et al., 2004) and found that the overall effect of sarcosine was significant for total symptoms in Positive and Negative Syndrome Scale (PANSS) total scores (standardised mean difference [SMD] = −0.41, confidence interval [CI] = −0.76 to −0.06, p = 0.02). However, modulators such as disease severity and treatment duration, which may affect the treatment response, remain unclear. Moreover, trials published after 2011 were not included in these reviews. Furthermore, several animal and human studies have shown that sarcosine may improve cognition (Kumar et al., 2016; Manahan-Vaughan et al., 2008; Peyrovian et al., 2019). A rat model of psychosis demonstrated that sarcosine can mitigate hippocampal long-term potentiation (LTP) and learning deficits (Manahan-Vaughan et al., 2008). Co-administration of sarcosine and risperidone can improve cognition and learning in MK-801-induced learning- and memory-impaired rats (Kumar et al., 2016). A study of 38 patients with schizophrenia showed a 13% improvement in the scores on the PANSS cognitive subscale of the sarcosine (Tsai et al., 2004).
Therefore, in this meta-analysis, we aimed to evaluate the effects of sarcosine on overall clinical symptoms and cognitive functions in patients with schizophrenia.
Methods
Search strategy and study selection
In this study, two well-trained authors (C.H. Chang and S.J. Chen) independently performed a systematic literature search from the study’s inception until 2 November 2019. The search keywords were (sarcosine OR N-methylglycine OR glycine transporter-1 inhibitor) AND (schizophrenia OR schizoaffective disorder). We searched PubMed, the Cochrane Collaboration Central Register of Controlled Clinical Trials, and Cochrane Systematic Reviews for studies on sarcosine for schizophrenia. The included trials and related review articles were reviewed manually to identify pertinent references. The guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) were followed (Moher et al., 2009) (Figure 1).
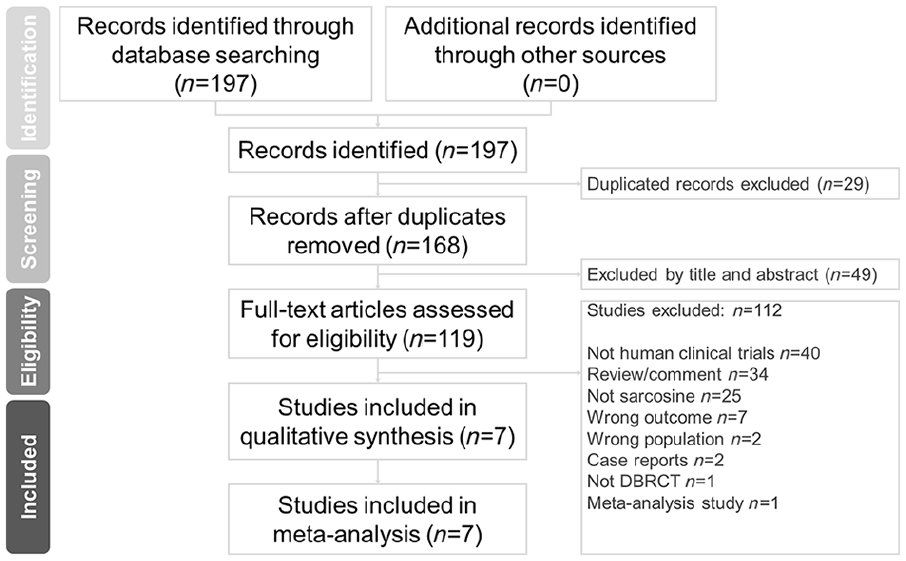
PRISMA flow diagram for searching and identifying included studies.
Eligibility criteria
Inclusion criteria were (a) studies with participants with a diagnosis of schizophrenia according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition, (b) double-blind randomised placebo-controlled trials (DBRCTs), and (c) the use of sarcosine as a monotherapy or adjunctive treatment to concomitant antipsychotics. The exclusion criteria were as follows: (a) nonhuman trials, (b) review/comment papers, (c) trials that did not include sarcosine, (d) trials that did not evaluate clinical symptoms after sarcosine treatment, (e) trials that enrolled patients without schizophrenia or schizoaffective disorder, (f) case reports, (g) studies that were not DBRCTs, and (h) meta-analysis studies. We followed the criteria of previous meta-analytic studies on sarcosine or NMDA receptor modulators to obtain the maximum number of trials.
Data extraction
The two authors independently extracted data of interest following the PRISMA guidelines. Chang and Chen examined the retrieved articles and recorded information, including the first author, published year, number of participants, sex ratio, mean age, duration, sarcosine dosage, a clinical symptom tests, and neurocognitive tests (Table 1).
Summary of study characteristics in the current meta-analysis.
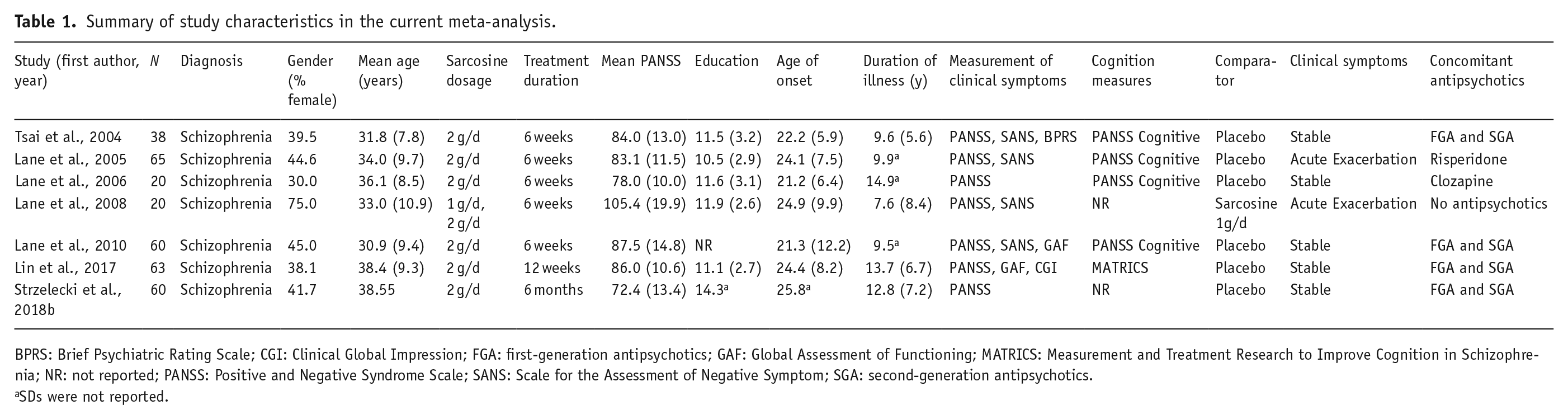
BPRS: Brief Psychiatric Rating Scale; CGI: Clinical Global Impression; FGA: first-generation antipsychotics; GAF: Global Assessment of Functioning; MATRICS: Measurement and Treatment Research to Improve Cognition in Schizophrenia; NR: not reported; PANSS: Positive and Negative Syndrome Scale; SANS: Scale for the Assessment of Negative Symptom; SGA: second-generation antipsychotics.
SDs were not reported.
Methodological quality appraisal
We used Jadad scoring (Jadad et al., 1996) to evaluate the methodological quality of selected studies for the randomised controlled trials (RCTs). The Jadad score is used to evaluate RCT methodology according to the following three aspects: (a) randomisation (2 points), (b) blinding (2 points), and (c) an account of all patients (1 point). The potential Jadad scores range from 0 to 5; a higher score indicates better methodological quality (Palys and Berger, 2013). Between-reviewer discrepancies were resolved through discussions under the supervision of the corresponding author.
Outcome measures
We aimed to evaluate the efficacy and cognitive effect of sarcosine in participants with schizophrenia. In this study, effects on overall clinical symptoms and cognitive functions were compared between add-on sarcosine and a comparator (mainly a placebo).
Data synthesis and analysis
We compared clinical improvement and cognitive function scores between baseline and after sarcosine use using the SMD with 95% CIs. Positive values indicated that the total clinical symptoms or cognitive functions improved after sarcosine therapy. We used a random-effects model to pool individual SMDs. We used I2 tests to evaluate between-trial heterogeneity. Values >50% were regarded as exhibiting considerable heterogeneity. Two-tailed p-values <0.05 were considered statistically significant. We used a sensitivity test with a ‘one study removal’ test to evaluate the effect of removing each individual study and reanalysed the overall effect on the remaining studies. We evaluated potential publication bias by using funnel plots and Egger’s test. The meta-analysis was performed using Comprehensive Meta-Analysis software, version 3 (Biostat, Englewood, NJ, USA).
Results
Characteristics of included studies
The seven included studies consisted of a total of 326 patients with schizophrenia (mean age = 34.91 ± 3.07 years, male proportion = 56.74%). The average number of subjects was 46.57 ± 20.23 (range: 20–65), and the treatment duration of these trials was 10.47 ± 6.83 weeks (range: 6–24 weeks). The mean baseline PANSS total score was 83.39 ± 8.06. The mean age at onset was 23.61 ± 1.64 years, and the mean illness duration was 11.22 ± 2.11 years. Six trials used add-on sarcosine treatment (Lane et al., 2005, 2006, 2010; Lin et al., 2017; Tsai et al., 2004), while one trial used sarcosine monotherapy (Lane et al., 2008). Eight trials (Strzelecki et al., 2015a, 2015b, 2015c, 2015d, 2016a, 2016b, 2018a, 2018b) used the PULSAR sample, and we included the latest PULSAR study (Strzelecki et al., 2018b). We followed the PRISMA guidelines and have presented the search process in Figure 1. Table 1 shows the summary of the study characteristics.
Overall clinical symptom analyses
Meta-analyses of overall clinical symptoms
All seven trials (Lane et al., 2005, 2006, 2008, 2010; Lin et al., 2017; Strzelecki et al., 2018b; Tsai et al., 2004) used PANSS scores to report raw data of overall clinical symptoms (Kay et al., 1987). Positive SMD results indicate the improvement of clinical symptoms after treatment with add-on sarcosine. In addition to PANSS, four studies (Lane et al., 2005, 2008, 2010; Tsai et al., 2004) used the Scale for the Assessment of Negative Symptom (Andreasen, 1982) to evaluate clinical symptoms, while two trials (Lane et al., 2010; Lin et al., 2017) used the Global Assessment of Functioning (Hall, 1995). Sarcosine achieved a more significant effect than the comparator on relieving overall clinical symptoms in participants with schizophrenia (SMD = 0.51, CI = 0.26–0.76, p < 0.01; Figure 2(a)).

Meta-analyses of (a) overall SMD, (b) group by mean PANSS score range, (c) group by clinical symptoms, (d) group by comparator, (e) group by treatment duration, and (f) group by concomitant antipsychotics.
Subgroup analyses of modulators in overall clinical symptoms
Furthermore, we performed a subgroup meta-analysis of modulators, including the mean PANSS score range, clinical symptoms, comparator, treatment duration, and concomitant antipsychotics (Table 2). The two studies (Lane et al., 2006; Strzelecki et al., 2018b) with the lowest range of 70–79 showed the largest significant effect sizes (ESs): 0.67 (95% CI: 0.03–1.31, p = 0.04), while four studies (Lane et al., 2005, 2010; Lin et al., 2017; Tsai et al., 2004) with a range of 80–89 showed significant ESs: 0.41 (95% CI: 0.10–0.72, p = 0.01; Figure 2(b)). Five trials (Lane et al., 2006, 2010; Lin et al., 2017; Strzelecki et al., 2018b; Tsai et al., 2004) enrolled patients with stable clinical symptoms and had significant ESs (0.53; 95% CI: 0.21–0.85, p < 0.01), whereas two trials (Lane et al., 2005, 2008) enrolled patients with acute exacerbation; in these, a positive but nonsignificant effect was found (ESs: 0.44; 95% CI: −0.06 to 0.93, p = 0.09; Figure 2(c)). Six trials (Lane et al., 2005, 2006, 2010, Lin et al., 2017; Strzelecki et al., 2018b; Tsai et al., 2004) that used a placebo as a comparator had significant ESs: 0.51 (95% CI: 0.25–0.77, p < 0.01; Figure 2(d)). Five studies (Lane et al., 2005, 2006, 2008, 2010; Tsai et al., 2004) with a 6-week treatment duration showed significant ESs: 0.49 (95% CI: 0.18–0.81, p < 0.01; Figure 2(e)). Four studies (Lane et al., 2010; Lin et al., 2017; Strzelecki et al., 2018b; Tsai et al., 2004) that used first-generation antipsychotics (FGA) and second-generation antipsychotics (SGA) showed significant ESs: 0.56 (95% CI: 0.19–0.93, p < 0.01; Figure 2(f)).
Subgroup analysis of pooled standardised mean differences for overall clinical symptoms.
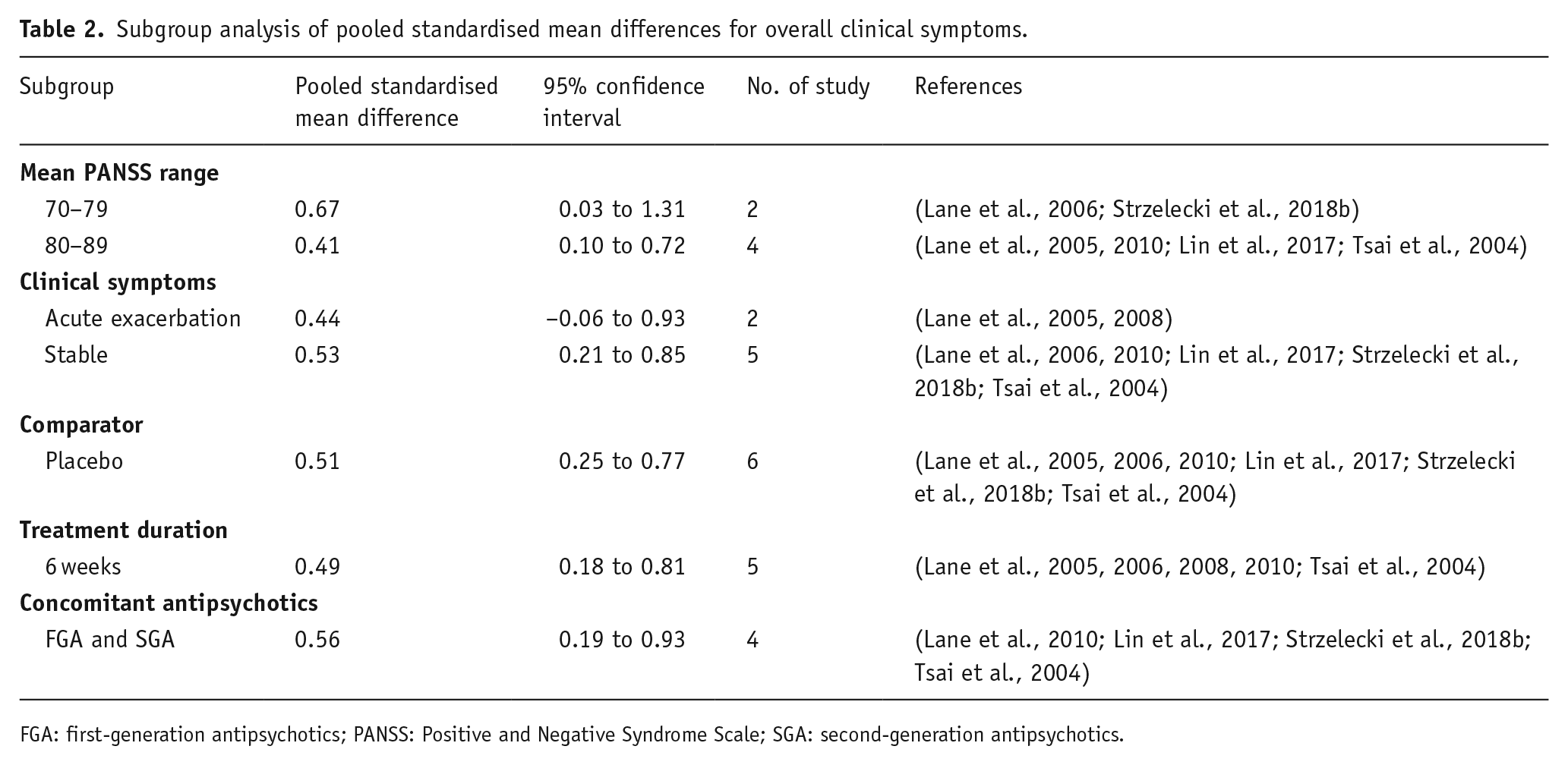
FGA: first-generation antipsychotics; PANSS: Positive and Negative Syndrome Scale; SGA: second-generation antipsychotics.
Meta-regression analyses of overall clinical symptoms
We noted that the increased effect of sarcosine on overall clinical symptoms was correlated with the sex ratio, age of onset, and years of education, whereas a decreased effect of sarcosine on overall clinical symptoms was correlated with illness duration and mean age (Supplement Figure 1). However, these findings did not exhibit significance.
Heterogeneity and publication bias
No significant heterogeneity was observed among the seven studies (Q = 5.13, df = 6, I2 = 0.00%, p = 0.53). Egger’s test revealed no significant publication bias regarding the overall SMD (p = 0.45). The funnel plots for the SMD of overall clinical symptoms are shown in Supplementary Figure 2(a).
Sensitivity analysis
In the meta-analysis of the effect of sarcosine on overall clinical symptoms, the conclusion remained significant with the removal of any single study.
Overall cognitive functions analyses
Meta-analyses of overall cognitive functions
Among the seven trials, four studies (Lane et al., 2005, 2006, Lin et al., 2017; Tsai et al., 2004) reported raw data on overall cognitive functions. Three studies (Lane et al., 2005, 2006; Tsai et al., 2004) used the PANSS cognitive subscale, while one study (Lin et al., 2017) used the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) (Green et al., 2004) battery of tests. Compared with a placebo, sarcosine showed a positive but nonsignificant effect on the overall cognitive function of participants with schizophrenia (SMD = 0.27, CI = −0.06 to 0.60, p = 0.10) (Figure 3(a)).
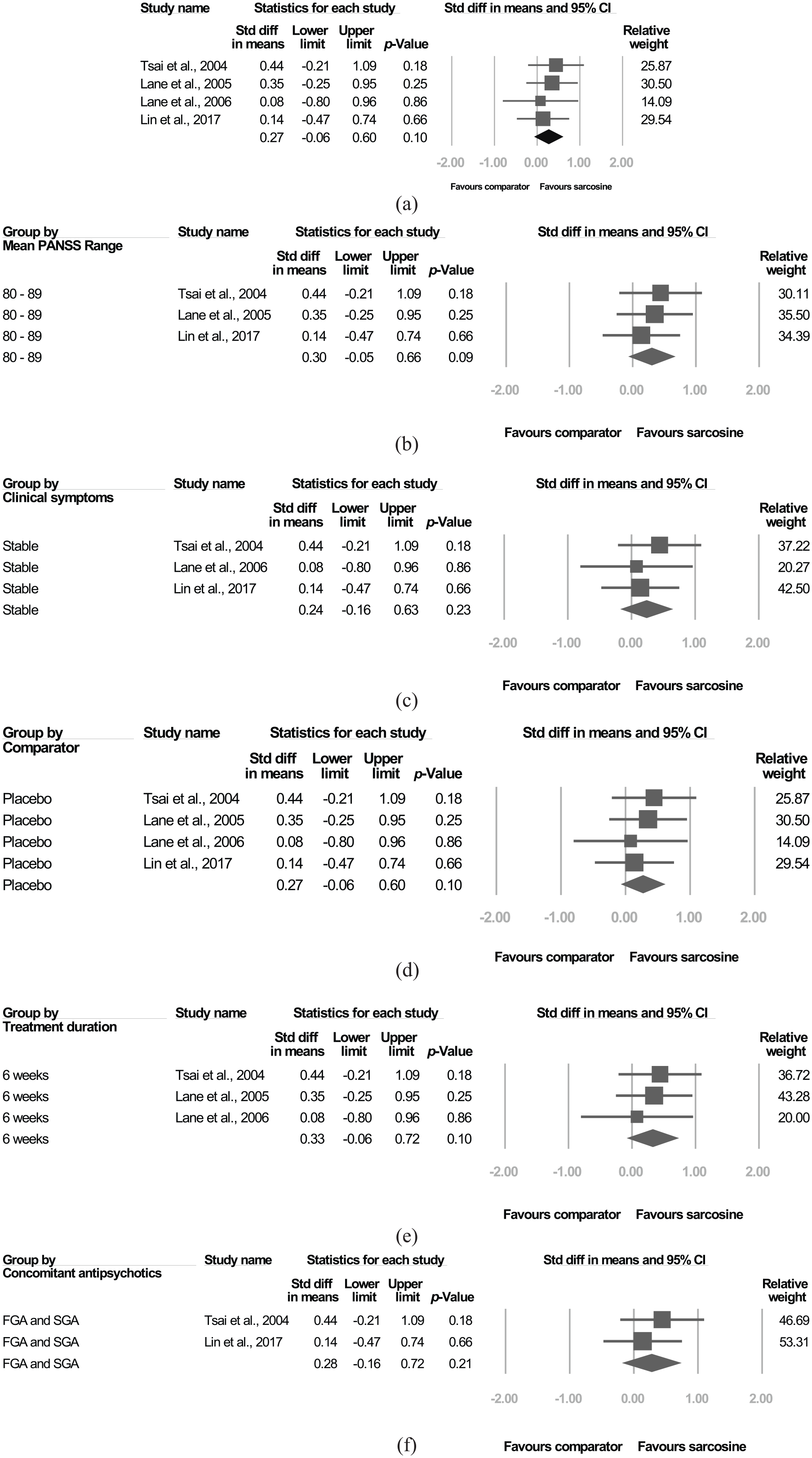
Meta-analyses of (a) overall cognitive function, (b) group by mean PANSS score range, (c) group by clinical symptoms, (d) group by comparator, (e) group by treatment duration, and (f) group by concomitant antipsychotics.
Subgroup analyses of modulators in overall cognitive function
Further, we performed a subgroup meta-analysis of modulators, including the mean PANSS score range, clinical symptoms, comparator, treatment duration, and concomitant antipsychotics. All these subgroup meta-analyses of modulators exhibited a positive but nonsignificant effect on the overall cognitive function of participants with schizophrenia (Figure 3(b–f)).
Meta-regression analyses of overall cognitive function
We noted that a high proportion of women was correlated with a high effect of sarcosine on overall cognitive function (slope = 2.05, 95% CI: −5.10 to 9.20, p = 0.58), while a long illness duration was correlated with a low effect of sarcosine on overall cognitive function (slope = −0.06, 95% CI: −0.22 to 0.09, p = 0.41; Supplement Figure 3).
Heterogeneity and publication bias
No significant heterogeneity was observed among these studies (Q = 0.70, df = 3, I2 = 0.00%, p = 0.87). Egger’s test revealed no significant publication bias regarding the overall SMD (p = 0.56). The funnel plots for the SMD of overall cognitive function are shown in Supplementary Figure 2(b).
Sensitivity analysis
In the meta-analysis of the effect of sarcosine on overall cognitive function, the conclusion remained nonsignificant when any single study was removed.
Discussion
To the best of our knowledge, this is the first meta-analytic study to focus on the efficacy and cognitive effect of sarcosine in patients with schizophrenia. The main results of this analysis found that (a) sarcosine was associated with a significant positive effect, compared with its comparator, on overall clinical symptoms in participants with schizophrenia (SMD = 0.51, CI = 0.26–0.76, p < 0.01); (b) studies with a low baseline mean PANSS score range and stable clinical symptoms showed significant positive effects; (c) add-on sarcosine combined with FGA and SGA was associated with a better effect; and (d) sarcosine was associated with a more positive effect than its comparator on overall cognitive functions. The ESs increased with the proportion of females, whereas they decreased with illness duration; however, the difference was nonsignificant.
Our findings accord with those of a previous study. Singh and colleagues performed a meta-analysis to evaluate the efficacy of adjunctive NMDA receptor modulators in chronic schizophrenia (Singh and Singh, 2011). They included 29 DBRCTs, and four of 29 trials had used sarcosine. They found that the ES of sarcosine was significant for total symptoms of chronic schizophrenia (SMD = −0.41, CI = −0.76 to −0.06, p = 0.02). In our study, we included seven trials and found that sarcosine was associated with a more significant positive effect than its comparator on overall clinical symptoms in participants with schizophrenia (SMD = 0.51, CI = 0.26 to 0.76, p < 0.01).
Moreover, studies with a lower baseline mean PANSS score range and patients with stable clinical symptoms showed significant positive effects. Two studies with a low baseline mean PANSS score range of 70–79 showed significantly large ESs compared with four studies with PANSS scores in the range of 80–89 (0.67 vs. 0.41), whereas one study with a high range of 100–110 did not show significant ESs (Figure 2(b)). Five trials enrolled patients with stable clinical symptoms and had significant ESs (0.53; 95% CI: 0.21–0.85, p < 0.01), whereas two trials enrolled patients with acute exacerbation of clinical symptoms and showed nonsignificant ESs (0.44; 95% CI: −0.06 to 0.93, p = 0.09; Figure 2(c)). Nevertheless, it should be noted that one of the two trials that enrolled patients with acute exacerbation clinical symptoms used sarcosine 1 g/day as a comparator instead of a placebo (Lane et al., 2008). Thus, patients with mild and stable clinical symptoms appear to benefit more than those with severe or acutely exacerbated symptoms. Why do patients during the acute stage benefit less from the effect of sarcosine? A previous study identified the hyperactivity of glutamatergic neurotransmission in first-episode schizophrenia as the reason (Theberge et al., 2007). Moreover, sarcosine can enhance glutamatergic neurotransmission (Peyrovian et al., 2019). Therefore, sarcosine may improve the hypoactivity of glutamatergic neurotransmission at the chronic stage instead of the hyperactivity of glutamatergic neurotransmission at the acute stage.
Moreover, patients receiving prolonged treatment (6 months) had larger ESs than those receiving a 6-week treatment: (0.92 vs. 0.49). However, it should be noted that only one trial had a treatment duration of 6 months (Strzelecki et al., 2018b). Furthermore, add-on sarcosine combined with FGA and SGA had a significant positive effect, whereas add-on sarcosine combined with only risperidone or clozapine did not. Nevertheless, add-on sarcosine combined with only risperidone was used to treat patients at the acute stage instead of at the chronic stage (Lane et al., 2005). Moreover, sarcosine did not show a significant effect at the acute stage. Furthermore, the subgroup analysis showed that patients receiving sarcosine combined with clozapine had the lowest and a nonsignificant effect compared with those receiving other concomitant antipsychotics (Figure 2(f)). A possible reason for this is that clozapine may enhance NMDA receptor-mediated neurotransmission (Arvanov et al., 1997; Fukuyama et al., 2019). Previous studies have shown that clozapine can augment NMDA response (Arvanov and Wang, 1999; Javitt et al., 2005; Kubota et al., 2000; Schwieler et al., 2004). Sarcosine also enhances NMDA receptor-mediated neurotransmission (Peyrovian et al., 2019); thus, patients receiving clozapine may already have achieved the ‘ceiling benefit’ from the enhancement of NMDA function. Moreover, patients treated with clozapine were treatment-resistant to other antipsychotics (Kane, 1992). Therefore, adding sarcosine did not show a significant effect when patients had already received clozapine.
We further evaluated the effect of sarcosine on overall cognitive function. In our study, sarcosine showed a nonsignificant but more positive effect than the placebo on overall cognitive function in participants with schizophrenia (SMD = 0.27, CI = −0.06 to 0.60, p = 0.10; Figure 3(a)). Our findings accord with those of previous studies. Four meta-analyses have investigated the effect of NMDA receptor-enhancing agents on cognition in patients (Chang et al., 2019; Choi et al., 2013; Iwata et al., 2015; Tsai and Lin, 2010). However, only two of them conducted trials with sarcosine and reported the ESs. Tsai and his colleagues performed three trials (Lane et al., 2005, 2006; Tsai et al., 2004) and found the ES of studies including sarcosine with PANSS cognitive scores (SMD = 0.29, CI = −0.10 to 0.69, p = 0.14), whereas Chang and his colleagues studied one trial (Lin et al., 2017) and found that the ES of studies of sarcosine on MATRICS test scores was (SMD = −0.05, CI = −0.65 to 0.56, p = 0.87). Sarcosine showed a nonsignificantly more positive effect than a placebo on overall cognitive function in participants with schizophrenia due to two possible reasons. First, the small sample may be the cause, because only four trials with 186 patients evaluating the overall cognitive function were included. Second, three studies (Lane et al., 2005, 2006; Tsai et al., 2004) used the PANSS cognitive subscale, while one study (Lin et al., 2017) used MATRICS tests (Green et al., 2004). The PANSS cognitive subscale is not used for standard cognitive tests like that of MATRICS. Therefore, further studies with large sample sizes and standard cognitive tests are warranted. Nevertheless, the treatment effect of sarcosine on clinical cognitive function was positive with a small ES (SMD = 0.27, 95% CI: −0.06 to 0.60, p = 0.10).
Furthermore, a high proportion of females was correlated with a high effect of sarcosine on overall cognitive function (slope = 2.05, 95% CI: −5.10 to 9.20, p = 0.58), whereas long illness duration was correlated with a low effect of sarcosine on overall cognitive function (slope −0.06, 95% CI: −0.22 to 0.09, p = 0.41; Supplementary Figure 3). Nevertheless, these findings did not achieve significance. A previous meta-analysis of glutamate-positive modulators on cognition in schizophrenia found that a high proportion of female patients was significantly correlated with high SMDs (Iwata et al., 2015). Why female patients with schizophrenia may benefit more than male patients and exhibit better improvements in overall cognitive function from sarcosine treatment could be due to the following. Previous studies have reported that women perform better than men in neuropsychological tests (Krysta et al., 2013). Female patients with schizophrenia had better cognition than male patients in terms of social cognition, processing speed, verbal learning, and visual learning (Zhang et al., 2017). Because cognition reserve influences schizophrenia prognosis, better cognition may be associated with better response in women (Herrero et al., 2019). In addition, animal studies have found that oestradiol enhances NMDA receptor transmission in the female rat dentate gyrus (Nebieridze et al., 2012). The association between cognitive function and gender warrants further investigation.
Strengths
Our study has several merits compared with the three previous meta-analytic studies. First, this is the first meta-analytic study that focused on the treatment and cognitive effects of sarcosine in schizophrenia. Second, seven sarcosine trials were included, whereas earlier works have included four trials (Singh and Singh, 2011), three trials (Tsai and Lin, 2010), and one trial (Chang et al., 2019). Third, we performed subgroup analysis and meta-regression to evaluate modulators, including the mean PANSS score, clinical symptoms, comparator, treatment duration, and concomitant antipsychotics.
Implications
Cognitive impairment is a critical issue both in schizophrenia and Alzheimer disease (AD) (Cummings and Cole, 2002; Freedman, 2003; Guo et al., 2019). The dysfunction of NMDA receptor-mediated neurotransmission plays a crucial role in both schizophrenia and AD (Li and Tsien, 2009; Snyder and Gao, 2019). Animal studies have shown that sarcosine can rescue hippocampal LTP and learning deficits (Manahan-Vaughan et al., 2008). The co-administration of sarcosine and risperidone improves cognition and learning in MK-801-induced learning- and memory-impaired rats (Kumar et al., 2016). Thus, further trials of sarcosine with standard cognitive tests on schizophrenia and AD are warranted.
Limitations
Our study has some limitations. First, the numbers of included trials and patients were small. Second, the duration of most trials was less than 36 weeks, and the long-term cognitive effect of NMDA-enhancing agents remains uncertain. Third, not all trials used the same standard cognitive tests or evaluated all cognitive domains. Fourth, we did not consider trials without a double-blind design or unpublished studies. Five, comprehensive genetic (Nimgaonkar et al., 2017) or psychosocial factors (Lange et al., 2017) such as suicide, which are potential confounders associated with the treatment outcome, were not evaluated in this study. Another review suggested that emotional turmoil in suicide survivors may last a long time and affect the treatment outcome (Pompili et al., 2013). Further trials with large sample sizes and the inclusion of comprehensive variables and adverse events may be warranted for future analysis.
Conclusions
This meta-analytic study showed that sarcosine has a significantly positive treatment effect in patients with schizophrenia. Sarcosine had a positive effect on overall cognitive functions, and the effect was correlated with an increased proportion of females and reduced illness duration, although the difference was nonsignificant. Further trials with large sample sizes are suggested to evaluate these findings and explore the role of sarcosine in the specific cognitive domains of patients with schizophrenia.
Supplemental Material
Supplementary_Figures – Supplemental material for Efficacy and cognitive effect of sarcosine (N-methylglycine) in patients with schizophrenia: A systematic review and meta-analysis of double-blind randomised controlled trials
Supplemental material, Supplementary_Figures for Efficacy and cognitive effect of sarcosine (N-methylglycine) in patients with schizophrenia: A systematic review and meta-analysis of double-blind randomised controlled trials by Chun-Hung Chang, Chieh-Hsin Lin, Chieh-Yu Liu, Shaw-Ji Chen and Hsien-Yuan Lane in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from An Nan Hospital, China Medical University Hospital (ANHRF108-01 and ANHRF108-15), China Medical University Hospital (DMR109103), the National Health Research Institutes (NHRI-EX109-10731NI) and the Ministry of Science and Technology (MOST 108-2314-B-039-002).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.