
Abstract
Introduction:
In two previous meta-analyses of randomized controlled trials (RCTs) examining antipsychotic switching strategies in patients with schizophrenia, we showed no significant differences in any clinical outcomes between immediate versus gradual and gradual versus wait-and-gradual discontinuation of the pre-switch antipsychotic. In this report, we compared immediate versus wait-and-gradual antipsychotic discontinuation.
Methods:
We identified five RCTs examining immediate versus wait-and-gradual discontinuation of the pre-switch antipsychotic in antipsychotic switching involving patients with schizophrenia. However, no data were available from one RCT. The following clinical outcome data were extracted and meta-analyzed: study discontinuation, psychopathology, extrapyramidal symptoms, and treatment-emergent adverse events that were reported in two or more of the studies.
Results:
The meta-analysis included four RCTs involving 351 patients (n=175 for immediate and n=176 for wait-and-gradual antipsychotic discontinuation). A significant difference was found in study discontinuation due to all causes (n=4, n=351, risk ratio=1.58, 95% confidence interval 1.15–2.17, p=0.005, I2=0%) between the immediate and wait-and-gradual antipsychotic discontinuation groups, while there was no significant difference in any other clinical outcomes. The group difference in study discontinuation due to all causes remained significant for the studies adopting immediate antipsychotic initiation but not for the studies switching to ziprasidone.
Conclusion:
Findings suggest that wait-and-gradual antipsychotic discontinuation may be preferable when a more cautious antipsychotic switch is needed. However, further long-term, double-blind RCTs are needed to confirm the present findings.
Introduction
When switching antipsychotics in patients with schizophrenia, there are three discontinuation options available with respect to the pre-switch antipsychotic: (a) immediate discontinuation (i.e., abrupt stopping); (b) gradual discontinuation (i.e., tapering over more than one day); and (c) wait-and-gradual discontinuation (i.e. waiting more than one day after the introduction of the post-switch antipsychotic before tapering the pre-switch antipsychotic over more than one day). We previously published two meta-analyses of randomized controlled trials (RCTs) examining antipsychotic switching strategies in patients with schizophrenia (Takeuchi et al., 2017a, 2017b), where no significant differences were observed in any clinical outcomes between immediate versus gradual and gradual versus wait-and-gradual discontinuation of the pre-switch antipsychotic. In this report, we compared immediate versus wait-and-gradual antipsychotic discontinuation in antipsychotic switching.
Methods
The detailed methods of the systematic literature search are described elsewhere (Takeuchi et al., 2017a, 2017b). A total of five RCTs involving patients with schizophrenia were identified that examined immediate versus wait-and-gradual discontinuation of the pre-switch antipsychotic in antipsychotic switching: three were rater blind, while two were open label. No data were available from one RCT (Alptekin et al., 2012) because the study was only reported in a conference abstract, and no further relevant RCTs have been published since the previous meta-analyses.
The following clinical outcome data were extracted: (a) number of patients who discontinued the study due to all causes, inefficacy, or intolerability; (b) changes (mean±standard deviation) from baseline to endpoint in the Positive and Negative Syndrome Scale (PANSS) total, positive, and negative subscale scores (Kay et al., 1987) in addition to Clinical Global Impression—Severity Scale score (Guy, 1976) as psychopathology measures, and the Simpson–Angus Scale (Simpson and Angus, 1970) total score, Barnes Akathisia Rating Scale (Barnes, 1989) total or global score, and Abnormal Involuntary Movement Scale (Guy, 1976) total or Item 8 score as extrapyramidal symptom measures; and (c) number of patients who experienced treatment-emergent adverse events that were reported in two or more studies.
Meta-analyses were conducted using Review Manager v5.3. Pooled estimates of risk ratios (RRs) for dichotomous outcomes and standardized mean differences (SMDs) for continuous outcomes were calculated with two-sided 95% confidence intervals (CIs) using a random-effects model. As reported (Takeuchi et al., 2017a, 2017b), one study (Weiden et al., 2003) was treated as three separate studies because this is a pooled analysis, and individual data for all three RCTs were obtained from Pfizer. Accordingly, six comparisons of immediate versus wait-and-gradual antipsychotic discontinuation were yielded. All effect sizes with a p-value of <0.05 were considered significant.
Study heterogeneities were quantified using I2 statistics, with I2 of ⩾50% indicating significant heterogeneity. Publication bias was assessed using visual inspection of funnel plots for each outcome. A lack of obvious asymmetry indicates a low possibility of significant publication bias.
As sensitivity analyses, the following two sets of studies were analyzed separately: (a) switching to ziprasidone (N=2), and (b) adopting immediate introduction of the post-switch antipsychotic (n=3). All effect sizes with a p-value of <0.05 were considered significant.
Results
The meta-analysis included four RCTs (Ganguli et al., 2008; Pae et al., 2009; Stip et al., 2010; Weiden et al., 2003), involving 351 patients (n=175 for immediate and n=176 for wait-and-gradual antipsychotic discontinuation). Table 1 summarizes the study characteristics. The duration of the studies ranged from 6 to 12 weeks, while the follow-up period after completion of a switch spanned 5–6 weeks (Table 1). A significant difference between the immediate and wait-and-gradual antipsychotic discontinuation groups was found for study discontinuation due to all causes, while there was no significant difference in study discontinuation due to inefficacy or intolerability (Figure 1).
Randomized controlled trials examining immediate versus wait-and-gradual antipsychotic discontinuation in antipsychotic switching in patients with schizophrenia.
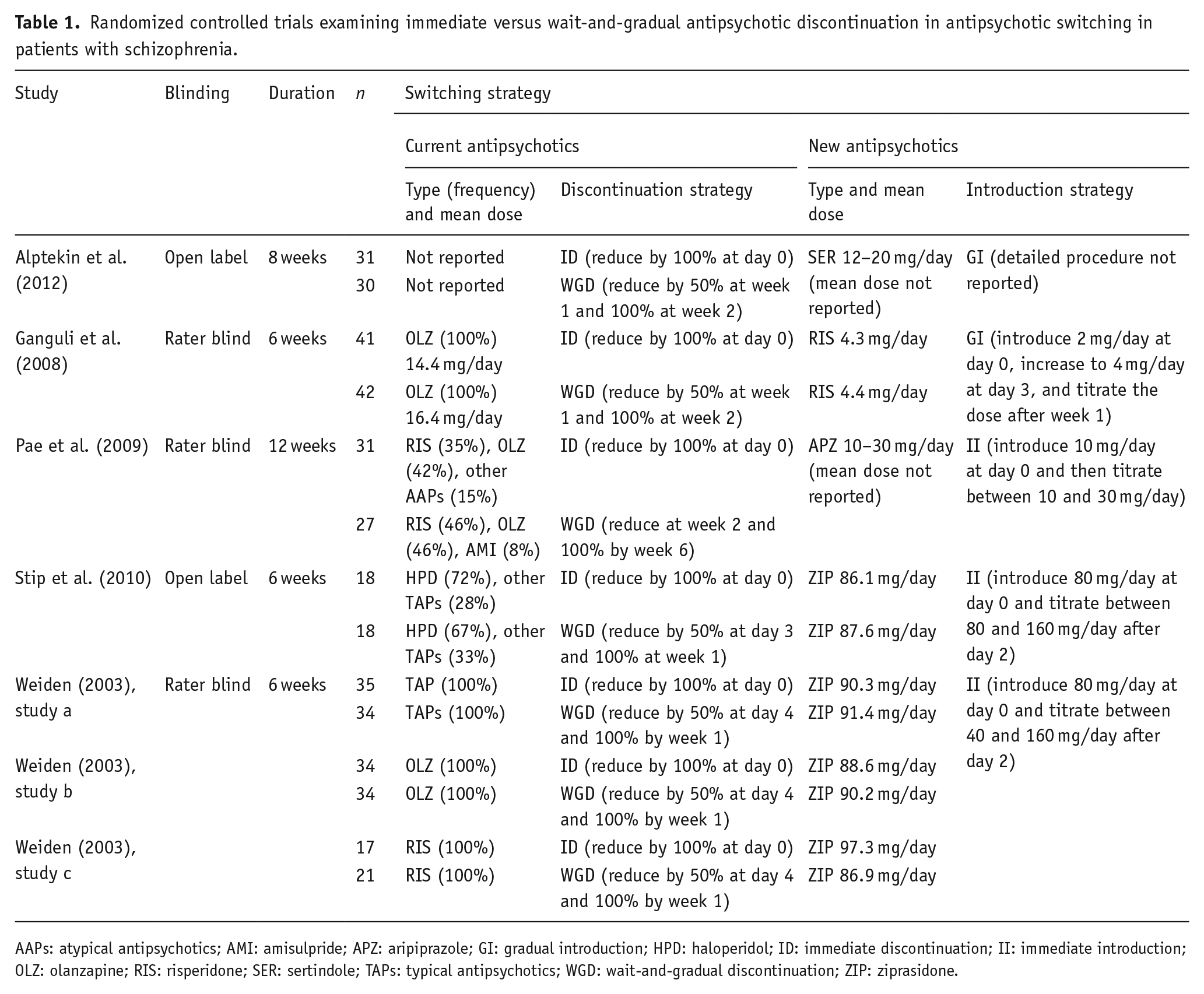
AAPs: atypical antipsychotics; AMI: amisulpride; APZ: aripiprazole; GI: gradual introduction; HPD: haloperidol; ID: immediate discontinuation; II: immediate introduction; OLZ: olanzapine; RIS: risperidone; SER: sertindole; TAPs: typical antipsychotics; WGD: wait-and-gradual discontinuation; ZIP: ziprasidone.
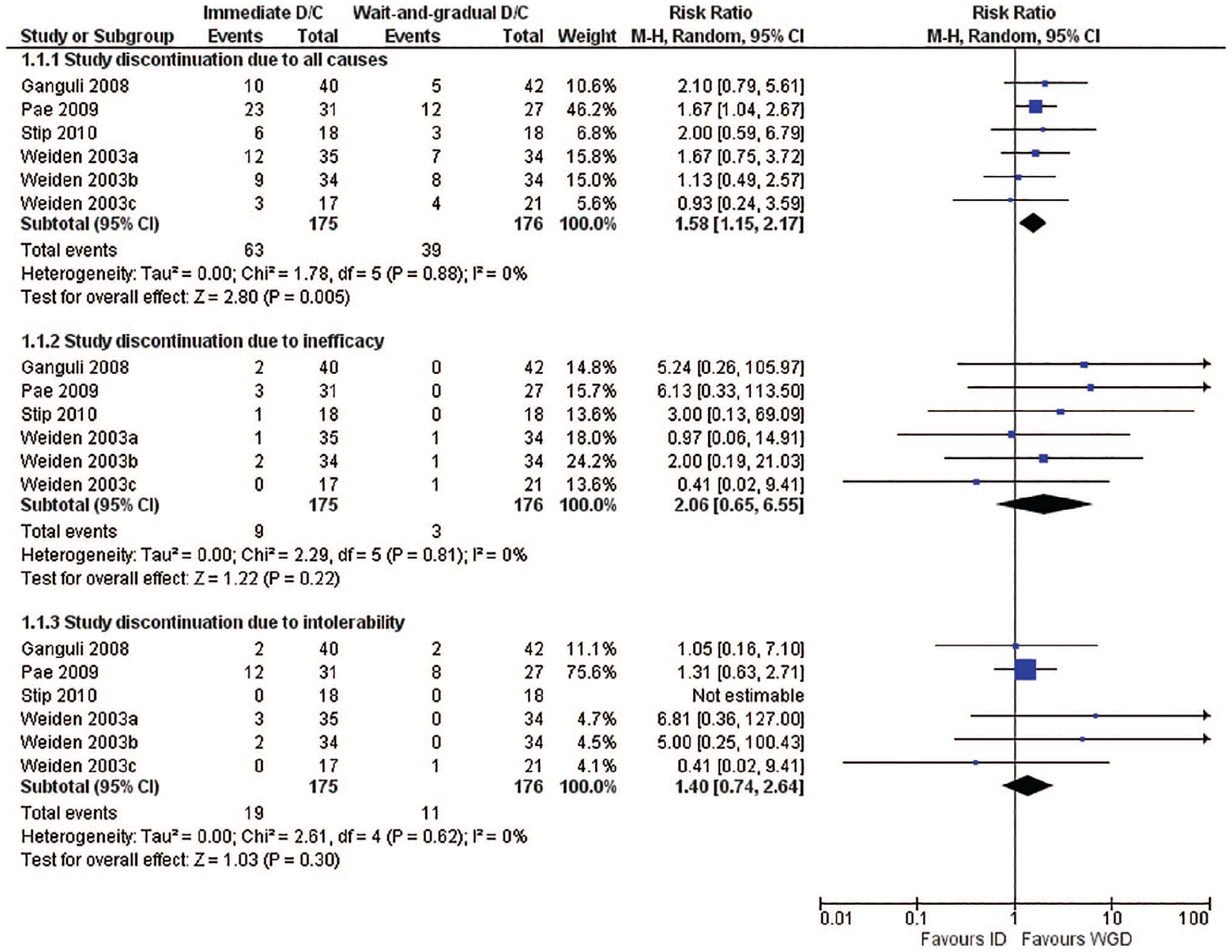
Study discontinuation.
Regarding psychopathology, no significant difference between the two groups was observed for PANSS total, positive, or negative subscale scores or Clinical Global Impression—Severity scores (Figure 2).
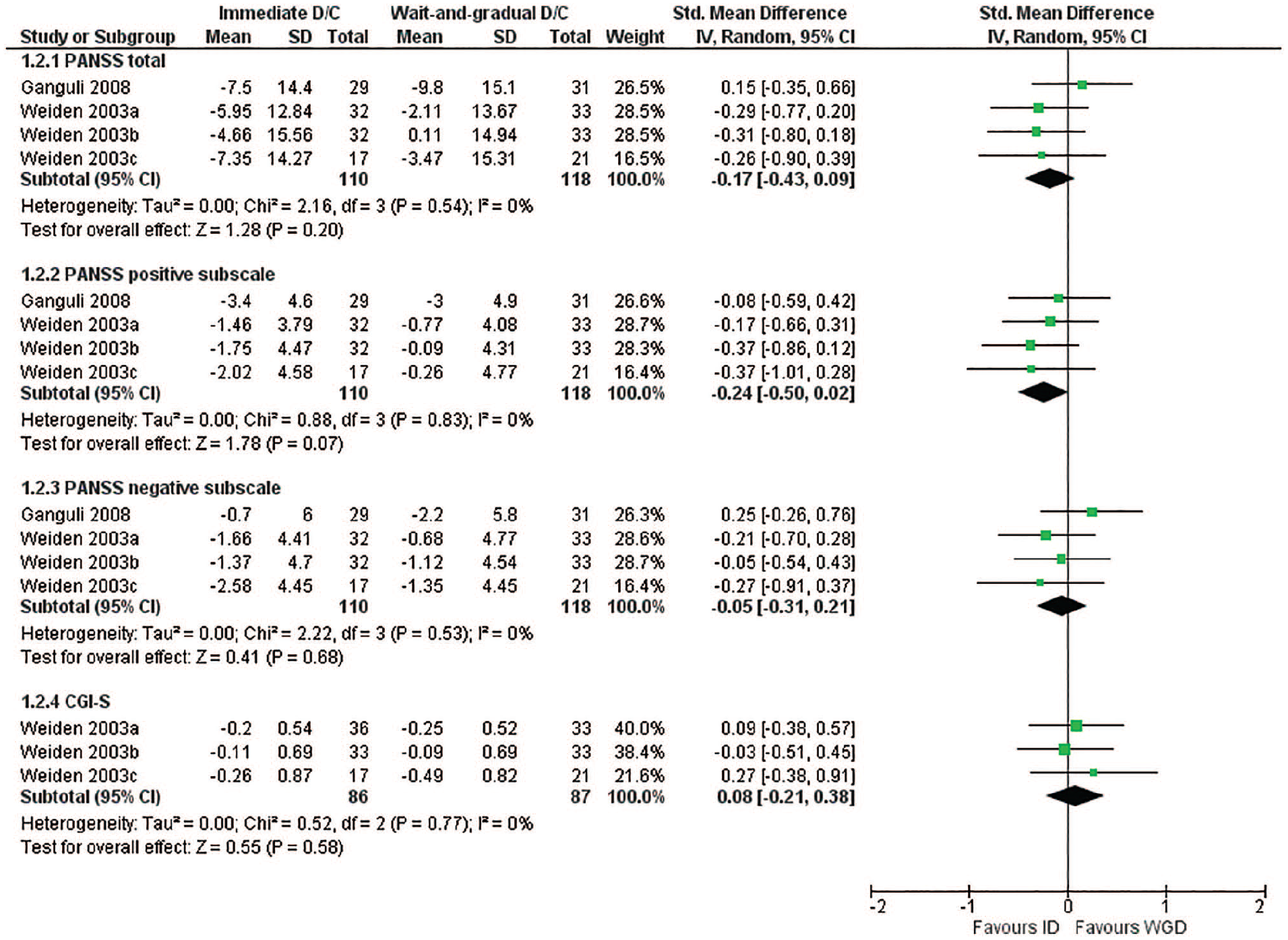
Psychopathology.
In terms of extrapyramidal symptoms, there was no significant difference between the two groups for Simpson–Angus Scale, Barnes Akathisia Rating Scale, or Abnormal Involuntary Movement Scale scores (Figure 3).
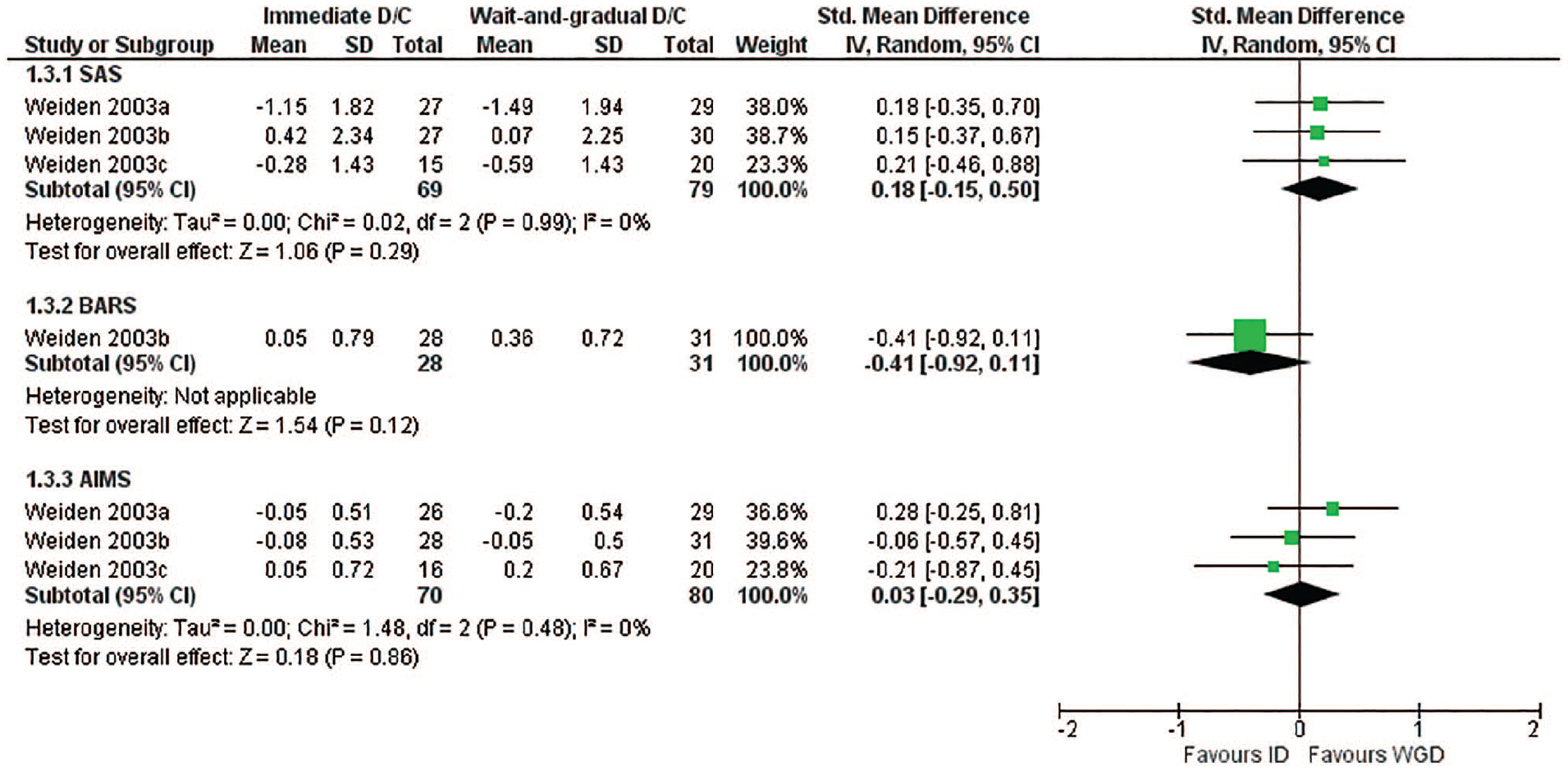
Extrapyramidal symptoms.
Regarding treatment-emergent adverse events, no significant difference was found between the two groups in terms of number of patients who experienced anxiety, headache, insomnia, or somnolence (Figure 4).
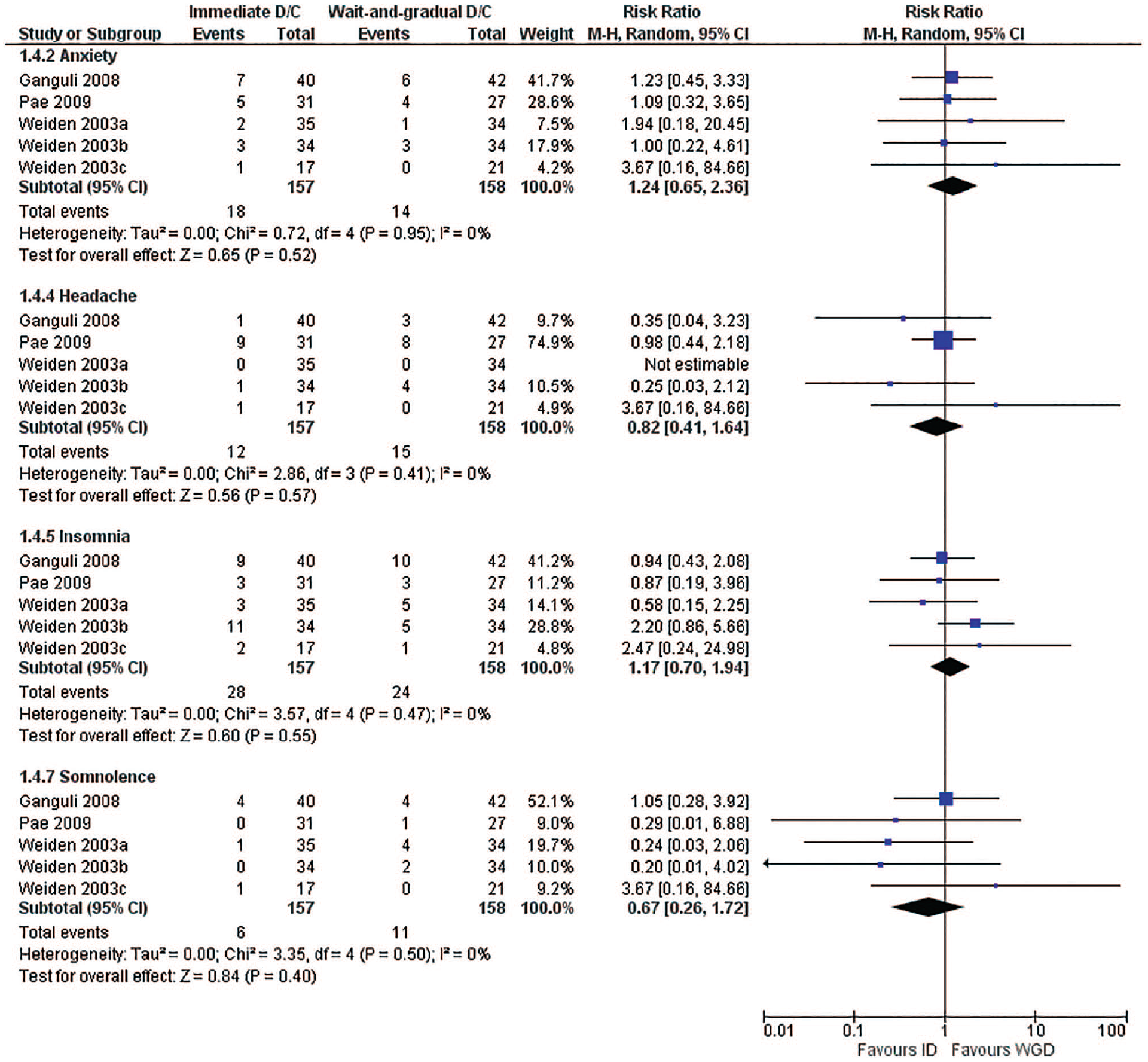
Treatment-emergent adverse events.
There were no study heterogeneities for any of the clinical outcomes (i.e., all I2=0%). Also, no overt publication biases were observed for any of the clinical outcomes.
The group difference in study discontinuation due to all causes remained significant for the studies adopting immediate antipsychotic initiation but not for the studies switching to ziprasidone.
Discussion
With regard to antipsychotic switching in patients with schizophrenia, the current meta-analysis demonstrated the superiority of wait-and-gradual discontinuation of the pre-switch antipsychotic versus immediate discontinuation in terms of study discontinuation due to all causes. The present results suggest that wait-and-gradual antipsychotic discontinuation may be preferable when a more cautious antipsychotic switch is needed. On the other hand, no significant differences were found for any other clinical outcomes. Study discontinuation due to all causes includes a variety of reasons other than inefficacy and intolerability, such as withdrawal of consent and loss to follow-up. On this point, though, there was no significant difference in study discontinuation due to causes other than inefficacy or intolerability (data not shown).
This finding differs from our previous two meta-analyses, which demonstrated no significant differences in any clinical outcomes between immediate versus gradual and gradual versus wait-and-gradual antipsychotic discontinuation (Takeuchi et al., 2017a, 2017b). That said, the present report poses a different question, examining immediate versus wait-and-gradual antipsychotic discontinuation.
We highlight that the current findings cannot be applied to first-episode schizophrenia or clozapine, since studies included here focused on patients with chronic schizophrenia. Moreover, only four open-label or rater-blind RCTs with a relatively short duration were included in the current meta-analysis. Antipsychotic switching represents a critical component of routine clinical care, underscoring the need for additional long-term, double-blind RCTs specific to this topic.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Takeuchi received speaker’s fees from Kyowa, Janssen, Meiji Seika Pharma, Mochida, Otsuka, Sumitomo Dainippon Pharma, and Yoshitomiyakuhin, and manuscript fees from Sumitomo Dainippon Pharma. Dr. Remington received conference support from Neurocrine Biosciences for data presentation, and research and advisory board support from HLS Therapeutics and Mitsubishi Tanabe Pharma.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.