
Abstract
Background:
Recent studies have demonstrated that alcohol consumption can modulate the immune system by directly activating natural immunity and triggering inflammatory processes in the central nervous system and in peripheral organs, such as the liver and pancreas. Patients with alcohol use disorders have an elevated frequency of comorbid mental disorders and gut diseases (i.e. fatty liver and pancreatitis) that complicate diagnosis, treatment and prognosis.
Aims:
The present study aims to explore possible associations in circulating plasma cytokine concentrations in abstinent patients diagnosed with alcohol use disorders.
Methods:
To this end, 85 abstinent subjects with alcohol use disorders from an outpatient setting and 55 healthy subjects were evaluated for both substance and mental disorders. The plasma levels of cytokines interleukin 1 beta, interleukin 4, interleukin 6, interleukin 17A, interferon gamma and tumour necrosis alpha were determined and their association with (a) history of alcohol consumption, (b) psychiatric comorbidity and (c) liver/pancreas comorbidities was explored.
Results:
We found that plasma concentrations of interleukin 1 beta, interleukin 6 and tumour necrosis alpha were increased, whereas plasma concentrations of interleukin 4, interleukin 17A and interferon gamma were decreased in abstinent alcohol use disorder patients as compared with control subjects. Moreover, we found that changes in interleukin 6 and interleukin 17A plasma concentrations in alcohol use disorder patients were associated with the presence of liver and pancreatic diseases.
Conclusion:
The present results suggest alcohol use disorder is associated with alterations of plasma cytokines, being interleukin 6 and interleukin 17A potential biomarkers of the presence of comorbidities of digestive organs. The clinical relevance of these findings is discussed in the context of alcohol-induced inflammatory processes.
Introduction
Alcohol is the most used psychoactive substance, with a high prevalence of consumption in the general population in the world (Organization for Economic Co-operation and Development (OECD), 2017). Chronic alcohol consumption is frequently associated with health problems, including liver diseases, pancreatitis, cancer, other substance use disorders (SUD) and psychiatric comorbidity (García Marchena et al., 2016; Goldsmith et al., 2016; Kleeff et al., 2017; Scoccianti et al., 2016). Alcohol use disorder (AUD) is a chronic relapsing brain disease characterised by compulsive alcohol use, loss of control over alcohol intake and a negative emotional state when not using (Koob, 2013).
It has been described that the immune system regulates the behaviours through actions related to inflammatory signals in the central nervous system (CNS) and several studies indicate the pharmacodynamic actions of alcohol and the abuse of other substances implicate the central modulation of immunological signalling pathways (Coller and Hutchinson, 2012; Gan et al., 1999). Among these signals, cytokines play a central role in the communication and activation of cellular processes. These mediators interact in different tissues regulating inflammatory processes, migration and cell proliferation (Dinarello, 2007). Cytokines can reach the brain through the blood brain barrier (Banks, 2015) or be locally produced by non-neuronal cells, such as astrocytes and microglia.
Substantial evidence suggests that alcohol is a direct modulator of the immune system and induces neuroinflammation by modifying the expression of inflammatory mediators at both central and peripheral levels (Pascual et al., 2015). It is known that the microglia-neuron interaction mediated by cytokines is affected by alcohol consumption (Crews et al., 2017); however, this view has recently challenged by in vivo neuroimaging studies in humans (Hillmer et al., 2017; Kim et al., 2018), although further work is needed to clarify this fact in adult AUD patients (Tyler et al., 2019). Because the expression profile of inflammatory cytokines is altered during the development of AUD and is normalised after cessation, it is feasible to think this normalisation might play a decisive role in the improvement of AUD (Yen et al., 2017).
Concerning SUD, a growing number of studies indicate the association between alcohol, other drugs of abuse and immunological mediators. We reported a decrease in the plasma levels of cytokines and chemokines (family of small cytokines) (tumour necrosis factor-alpha (TNF-α), chemokine (C-C motif) ligand 2/monocyte chemotactic protein-1 (CCL2/MCP-1) and chemokine (C-X-C motif) ligand 12 (CXCL12)/stromal cell-derived factor-1 (CXCL12/SDF-1)) in outpatients diagnosed with cocaine use disorders (Araos et al., 2015). Another study from our group on patients with AUD in abstinence reported that CXCL12/SDF-1 and chemokine (C-X3-C motif) ligand 1 (CX3CL1/fractalkine) were lower compared to controls (García-Marchena et al., 2017).
Additionally, changes in circulating cytokines have been associated with psychiatric disorders. A meta-analysis study confirmed elevated levels of circulating inflammatory cytokines (IL-6 and TNF-α) in depressed patients (Goldsmith et al., 2016). Furthermore, the serum levels of cytokines have revealed positive associations of anxiety (panic disorders) with IL-6, IL-1β and IL-5 (Quagliato and Nardi, 2018). We recently described that AUD patients diagnosed with mood disorders and/or anxiety disorders displayed lower concentrations of CCL11/eotaxin 1 than non-comorbid patients (García-Marchena et al., 2017). A recent study in AUD patients described a positive association between IL-6 and depression and a negative association between IL-10 and anxiety (Martinez et al., 2018). These results suggest that cytokines and chemokines could be potential biomarkers of psychiatric diseases.
However, it is unknown whether these immuno-inflammatory signals could have a significant impact on the development of other comorbidities associated with AUD. One group of these comorbid diseases is constituted by the induction of alcohol liver disease and/or pancreatitis. Alcohol-induced fatty liver (steatosis) is regarded as a significant risk factor for advanced liver pathology (Donohue, 2007). It is known that alcohol is the main factor that contributes to alcoholic cirrhosis and daily alcohol consumption is associated with an increased risk of alcoholic cirrhosis (Askgaard et al., 2017). Thus, the relationship between alcohol consumption and the development of liver cancer is becoming more evident every day (Akinyemiju et al., 2017). Moreover, heavy drinking is associated with a high rate of pancreatic diseases (Setiawan et al., 2017). Patients with liver cirrhosis and chronic pancreatitis have the most important etiological factor in alcohol abuse (Veena et al., 2012).
A growing body of evidence suggests the relationship between cytokines and liver and/or pancreatic diseases is becoming more relevant. Increased levels of IL-6 are associated with mortality in patients with liver diseases (Remmler et al., 2017). Other studies have mentioned that there are significantly higher levels of IL-6, IL-8 and TNF-α in patients with liver diseases compared to controls (Akberova et al., 2017). In contrast, excessive alcohol consumption contributes to the development of pancreatitis (Maléth et al., 2015). It has been established that IL-1, IL-6 and TNF-α are produced in greater amounts, promoting the progression of pancreatitis (Gukovskaya et al., 2017).
These findings confirm the existence of a close interaction between the inflammatory mediators of the peripheral tissues (e.g. the liver) and neuroinflammation through the bloodstream and the blood-brain barrier. After all these observations, we could hypothesise that the chronic use of alcohol leads to progressive changes in neurobiology and behaviour that could be mediated, not only by the innate immune system, but also by the coordinated actions of plasma cytokines. This research is the continuation of a previous study in patients with AUD (García-Marchena et al., 2017). The selected molecules in these two studies were chosen according to an exhaustive bibliographic search.
In the present study, we examined the plasma concentration of IL-1β, IL-4, IL-6, IL-17A, interferon gamma (IFN-γ) and TNF-α in a cohort of abstinent AUD patients from outpatient treatment programmes. We explored the relationship between these circulating cytokines and AUD-related variables (i.e. duration of problematic alcohol use, abstinence length, addiction severity, alcohol-induced liver and pancreatic diseases and psychiatric comorbidities).
Materials and methods
Study design and recruitment
The present cross-sectional study was performed in 140 Caucasian subjects who were divided into alcohol and control groups. In total, 85 abstinent subjects diagnosed with AUD (alcohol abuse or dependence) were recruited from outpatient programmes for AUD at Hospital Universitario 12 de Octubre in Madrid (Spain) for a period of 18 months (November 2013–May 2015). Overall, 55 healthy individuals with no history of substance use disorders or pathological use of substances were matched with the alcohol group for age, sex ratio and body mass index (BMI). The average participant was male (65%), 46.6 years old, with a BMI of 25.5 kg/m2.
The participants in the alcohol group had to meet eligibility criteria based on (a) inclusion criteria: 18–60 years of age, lifetime AUD and at least 4 weeks of abstinence before testing; (b) exclusion criteria: presence of infectious diseases, incapacitating cognitive alterations to complete psychiatric interviews and pregnancy for female participants. A breathalyser was used daily to estimate blood alcohol content from a breath sample. Because of the high incidence of alcohol-induced diseases (liver and pancreas), we included these individuals in the alcohol group.
AUD patients were being treated with pharmacological approaches and psychosocial therapies. In total, 61 subjects were treated with disulfiram during the last year. Regarding psychiatric medication, 60 patients were treated with medication during the last year: antidepressants (N = 35), benzodiazepines (N = 26), anticonvulsants (N = 29) and antipsychotics (N = 7).
Ethics statement
Written informed consent was obtained from each participant after a complete description of the study and discussing any questions or issues. The study and protocols for recruitment were approved by the Ethics Committee of the CEI Provincial de Málaga and Hospital Universitario 12 de Octubre in accordance with the Ethical Principles for Medical Research Involving Human Subjects adopted in the Declaration of Helsinki by the World Medical Association (64th WMA General Assembly, Fortaleza, Brazil, October 2013), Recommendation No. R (97) 5 of the Committee of Ministers to Member States on the Protection of Medical Data (1997) and Spanish Data Protection Act (Ley Orgánica 15/1999 de Protección de Datos).
Clinical assessments
Patients from outpatient programmes for AUD were evaluated according to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) criteria, using the Spanish version of the Psychiatric Research Interview for Substance and Mental Diseases (PRISM) (Torrens et al., 2004). Diagnoses were made using two timeframes: current (criteria were met within the past year) and past (criteria were met before the previous 12 months). Lifetime prevalence, considering both current and past diagnoses, was used to present the frequency of substance use disorders and other mental disorders. DSM-IV-TR criteria for substance dependence and abuse were used to diagnose substance use disorders and determine the severity of substance use disorders (Pavón et al., 2013). Control subjects were initially evaluated by PRISM (for substance screening and abuse and dependence) and subsequently by the Spanish version of the Dual Diagnosis Screening Instrument (DDSI) to detect psychiatric disorders (DSM-IV-TR) (Mestre-Pintó et al., 2014). All the interviews were performed by experienced psychologists who had received both PRISM and DDSI training.
Collection of plasma samples
Blood samples were obtained in the morning (9:00–11:00 a.m.) after fasting for 8–12 h (prior to the psychiatric interviews). Venous blood was extracted into 10 mL K2-EDTA tubes (BD, Franklin Lakes, NJ, USA) and was immediately processed to obtain plasma. Blood samples were centrifuged at 2200 × g for 15 min (4°C) and individually assayed for infectious diseases using three rapid tests for HIV (HIVTOP®), hepatitis B (HBVTOP®) and hepatitis C (HCVTOP®), which were purchased from ALL DIAG (Strasbourg Cedex, France). Samples displaying infection were discarded following safety protocols. Plasma samples were individually characterised, registered and stored at −80°C until further analyses.
Multiplex immunoassay analysis
Cytokines were chosen based on previous studies about inflammatory mediators and psychiatric disorders and addiction (Araos et al., 2015). A Bio-Plex Suspension Array System 200 (Bio-Rad Laboratories, Hercules, CA, USA) and ProcartaPlex Immunoassay Kit, with magnetic beads and an appropriate Plasma Standard Diluent Kit (eBioscience, Affymetrix, Santa Clara, CA, USA), were used to quantify protein levels in the plasma. This method of analysis is based on the Luminex technology and a human cytokine 6-plex panel (Mix&Match Panel) was used to simultaneously detect the following analytes: IL-1β, IL-4, IL-6, IL-17A, IFN-γ and TNF-α. Raw data (mean fluorescence intensity) were analysed using the Bio-Plex Manager Software 4.1 (Bio-Rad Laboratories). Data were expressed as pg of protein per mL of plasma.
Determination of biochemical parameters related to liver and pancreatic functions
In addition to immunoassays, plasma samples from the participants were assessed for markers of liver and pancreatic functions in a clinical analysis laboratory (Analysis Clinics Rodriguez Vergara S.L., Malaga, Spain). We examined the following parameters: aspartate transaminase (AST/GOT), alanine transaminase (ALT/GPT), gamma-glutamyltransferase (GGT), pancreatic α-amylase and pancreatic lipase. The reference ranges from the laboratory were established as follows: 0–40, 0–40, 0–45, 5–100 and 0–67 IU/L, respectively.
Statistical analyses
All clinical data are expressed as the number and percentage of subjects (N (%)) or the mean and standard deviation (mean (SD)). Significant differences between the categorical variables were determined using Fisher’s exact test (Chi-square test). We applied a Monte Carlo simulation of p values for the Chi-square test in necessary situations. Significant differences between normal continuous variables or non-normal continuous variables were determined using the Student’s t-test and the Mann-Whitney U test, respectively. Statistical analysis of protein levels was performed using multiple analysis of covariance (ANCOVA) to indicate the relative effect of explanatory variables and their interactions on the protein expression in the plasma, controlling for additional covariates. Log10 transformation was used to ensure statistical assumptions for positively skewed distributions. Estimated marginal means (95% confidence intervals (95% CI)) of protein levels were expressed after back-transformation. In this study, we used the Kolmogorov-Smirnov test with Lilliefors correction to analyse normality of the data. We used Levene’s test to analyse homoscedasticity of the data. As Log10 transformation was used to assure parametric statistical, correlation analyses were performed using Pearson’s coefficient (r) to explore the relation between plasma concentrations.
Binary logistic regression models (backward stepwise approach) were used to identify the subset of proteins that best distinguished between abstinent alcohol-dependent and control subjects. All models satisfied the Hosmer-Lemeshow test. We use the Akaike Information Criterion to assess the quality of each model by comparing related models.
The Receiver Operating Characteristics (ROC) analysis evaluated the discriminative power of the logistic regression models through the area under the curve (AUC), including the closest top left estimation of sensitivity and specificity as the descriptive cut-off. Overall, statistic values and degrees of freedom were indicated in the results when appropriate. Accordingly, a p value < 0.05 was considered statistically significant. The specific statistical analysis and values used are indicated in the text and in each figure caption.
All statistical analyses were performed using R, version 3.3.2, free software (with RStudio as IDE) and GraphPad Prism version 5.04 software (GraphPad Software, San Diego, CA, USA).
Results
Socio-demographic characteristics
The description of the socio-demographic variables of the participants is presented in Table 1. A total of 140 subjects of both sexes met the eligibility criteria for this study and were divided into the alcohol (N = 85) and control (N = 55) groups.
Baseline sociodemographic variables in abstinent AUD patients and controls.
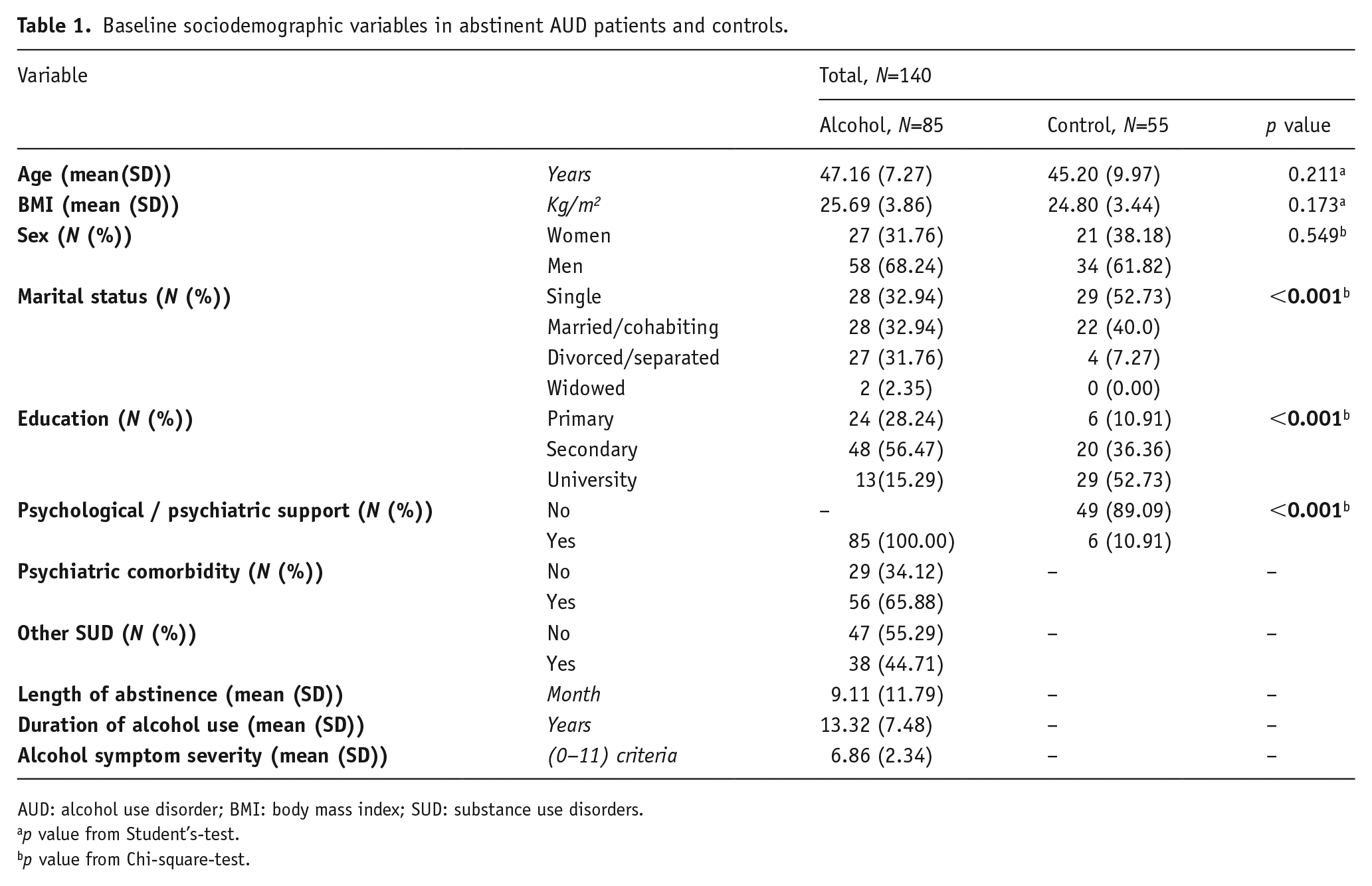
AUD: alcohol use disorder; BMI: body mass index; SUD: substance use disorders.
p value from Student’s-test.
p value from Chi-square-test.
The average participant in the alcohol group was a 47-year-old male with a BMI of 26.
We found significant differences in the marital status between patients with AUD and controls (p < 0.001). Alcohol patients had a significantly lower educational level and a higher percentage of psychological/psychiatric support compared with the control group (p < 0.001).
A total of 66% of alcohol patients were diagnosed with psychiatric comorbidity, which included at least one psychiatric disorder throughout life (i.e. mood, anxiety and/or personality disorders (antisocial and borderline)). In addition, 45% of alcohol patients were diagnosed with other comorbid SUD (i.e. cocaine, cannabis, heroin, sedative, hallucinogens, stimulants and/or opioids).
Plasma levels concentrations of cytokines in AUD patients and controls
First, we evaluated the differences in the plasma concentration of IL-1β, IL-4, IL-6, IL-17A, IFN-γ and TNF-α using a one-way ANCOVA according to the ‘history of alcohol use’ and ‘age’, ‘BMI’ and ‘sex’ as covariates. To ensure that statistical assumptions were met, a logarithmic transformation (base-10 logarithm) of the concentration of these cytokines was performed. The estimated marginal means after back-transformation are shown in Figure 1.
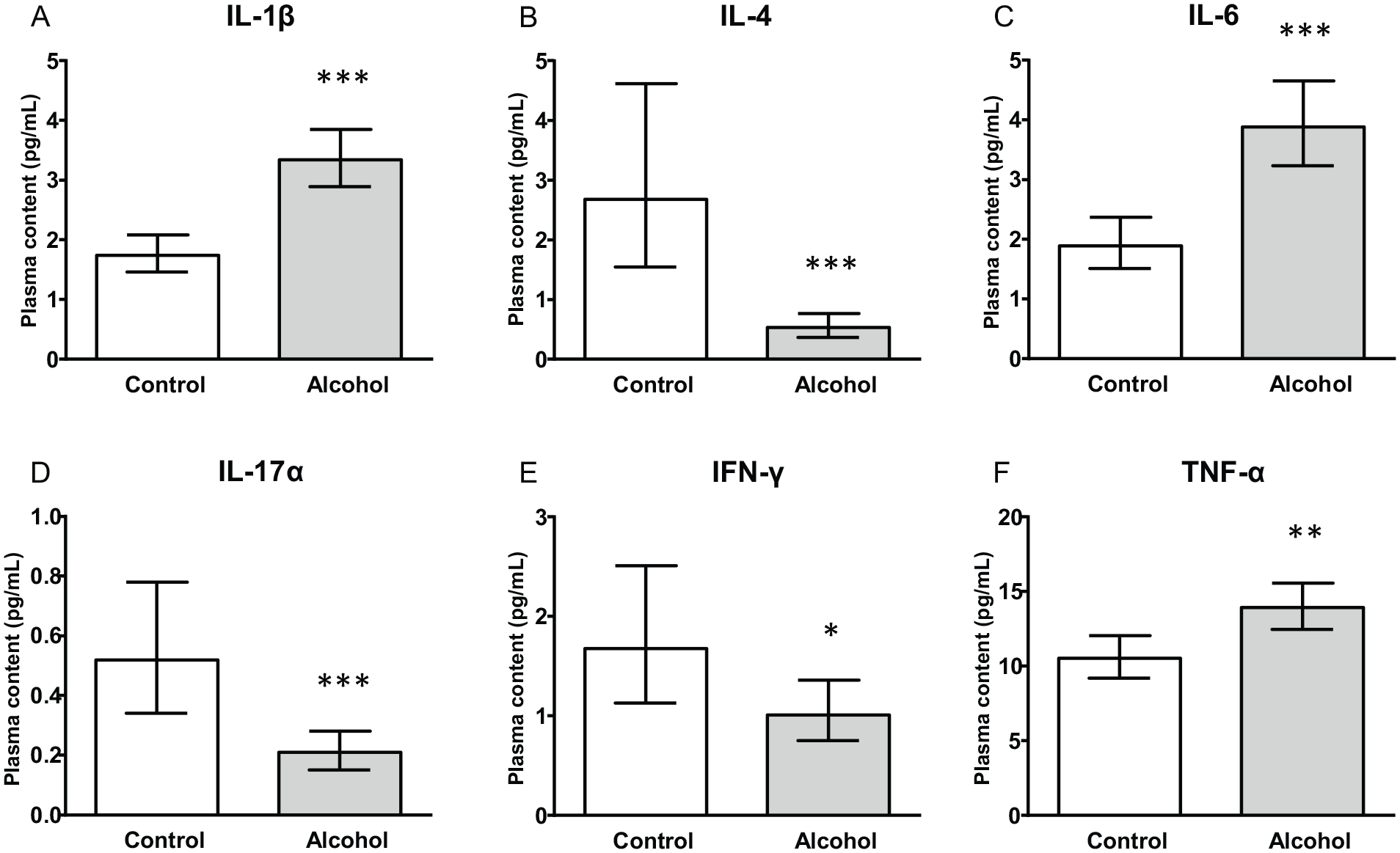
Plasma chemokine concentrations in AUD patients and control subjects. (A) IL-1β, (B) IL-4, (C) IL-6, (D) IL-17A (E) IFN-γ and (F) TNF-α concentrations according to “history of AUD”. Bars are estimated marginal means and 95% confidence intervals (95% CI) (pg/mL). Data were analyzed by one-way analysis of covariance (ANCOVA) and *p < 0.05, **p < 0.01 and ***p < 0.001 denote a significant main effect of “history of AUD”.
All cytokines were significantly affected by ‘history of alcohol use’: IL-1β (F1,133 = 32.72, p < 0.001), IL-4 (F1,115 = 24.36, p < 0.001), IL-6 (F1,133 = 25.10, p < 0.001), IL-17A (F1,123 = 13.35, p < 0.001), IFN-γ (F1,125 = 4.27, p < 0.041) and TNF-α (F1,133 = 10.34, p = 0.002). Thus, a significant increase in plasma concentrations of IL-1β, IL-6 and TNF-α was found in the alcohol group compared with the control group. By contrast, the concentrations of IL-4, IL-17A and IFN-γ were lower in the alcohol group than in controls.
In addition, the concentrations of IL-1β (F1, 133 = 0.41, p < 0.05), IFN-γ (F1, 125 = 1.37, p < 0.05) and IL-17A (F1, 123 = 2.41, p < 0.01) were significantly affected by the covariate ‘age’. We also found a significant effect by the covariate ‘BMI’ on IFN-γ (F1, 125 = 5.66, p < 0.05).
Because all cytokine concentrations were significantly affected by the ‘history of alcohol use’ factor, a logistic regression model was generated to evaluate the potential of cytokines as explanatory variables to discriminate abstinent alcohol-dependent patients and controls. We included ‘age’ and ‘sex’ as variables in the initial model at step 1. As shown in Table 2, the backward stepwise approach was used to generate the final model, which was restricted to four explanatory variables in the equation: the cytokines IL-1β, IL-4, IL-6 and IL-17A. The final model showed the calibration (χ28 = 4.82; p = 0.776).
Stepwise logistic regression model based on plasma cytokine concentrations for abstinent alcohol use disorders and controls.
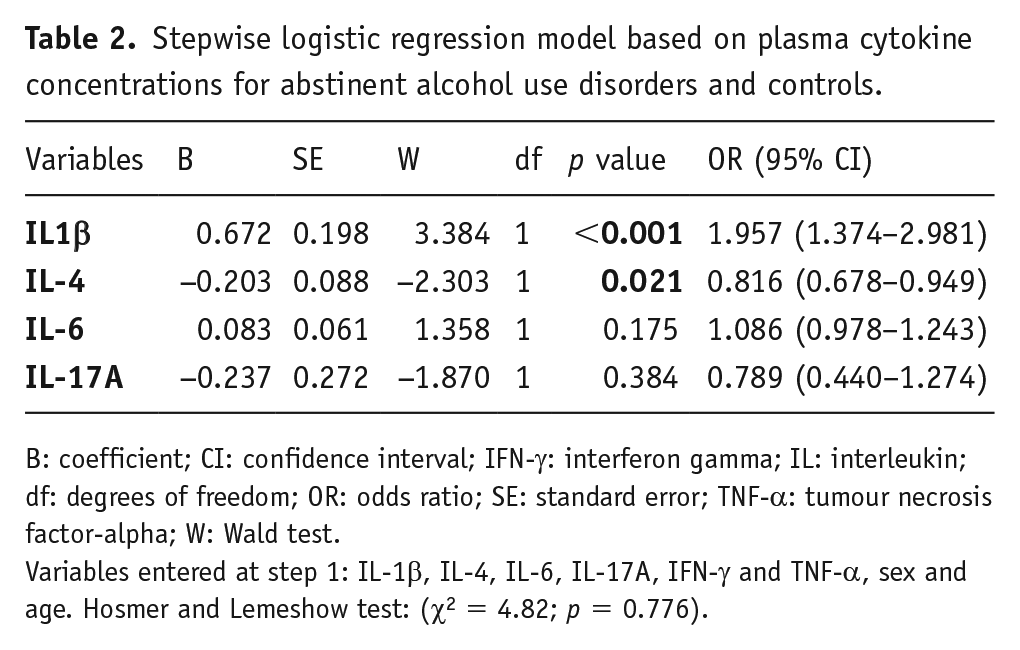
B: coefficient; CI: confidence interval; IFN-γ: interferon gamma; IL: interleukin; df: degrees of freedom; OR: odds ratio; SE: standard error; TNF-α: tumour necrosis factor-alpha; W: Wald test.
Variables entered at step 1: IL-1β, IL-4, IL-6, IL-17A, IFN-γ and TNF-α, sex and age. Hosmer and Lemeshow test: (χ2 = 4.82; p = 0.776).
As shown in Figure 2, the ROC curve analysis for this model showed an AUC = 0.855 (p < 0.001), which indicated a high discriminative power. A representative cut-off value was 0.73 (sensitivity: 0.76 (95% CI = 0.51–0.89); specificity: 0.81 (95% CI = 0.64–0.94)).
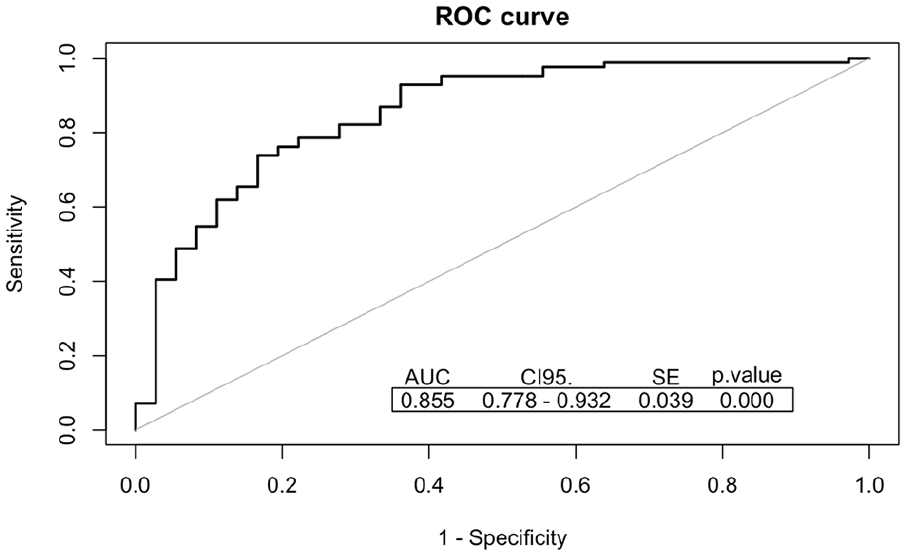
ROC analyses for predictive logistic models of AUD patients. Backward stepwise approach determined the final multivariable model using four predictors: IL-1β, IL-4, IL-6 and IL-17A.
Impact of other SUD and psychiatric comorbidities on plasma concentrations of cytokines in AUD patients
Because the alcohol group displayed a high incidence of SUD and/or others psychiatric comorbidities, we evaluated the effects of these comorbidities on cytokine concentrations in plasma. Therefore, alcohol patients were divided into subgroups according to these diagnoses: (a) diagnosis of other SUD and (b) diagnosis of psychiatric comorbidity (Table 3).
Substance use disorders and psychiatric comorbidity in AUD patients.
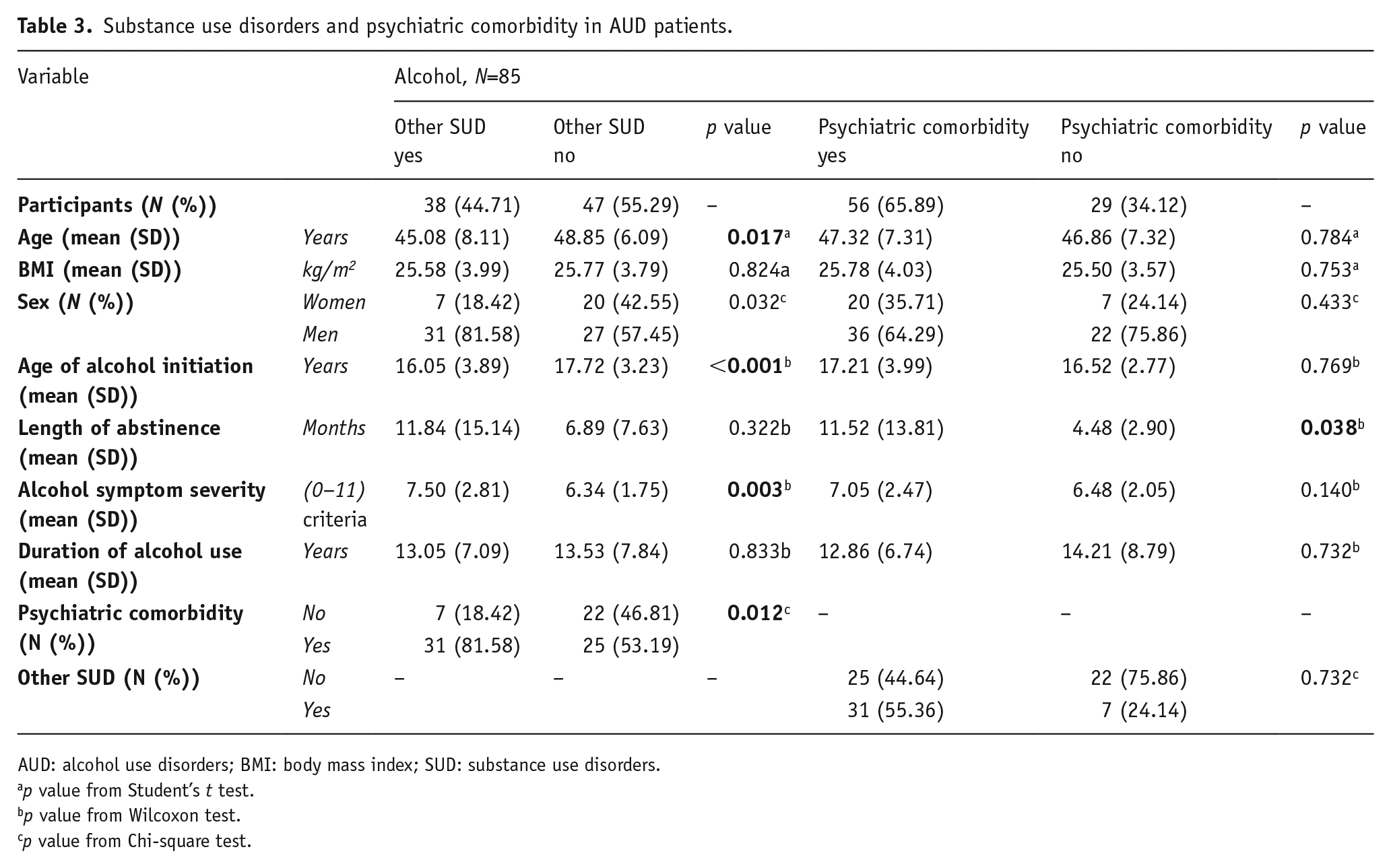
AUD: alcohol use disorders; BMI: body mass index; SUD: substance use disorders.
p value from Student’s t test.
p value from Wilcoxon test.
p value from Chi-square test.
The first classification of the alcohol group was performed according to the diagnosis of other SUD (yes (N = 38); no (N = 47)). The comparison between both subgroups showed there were significant differences in socio-demographic variables, including age (p = 0.017) and sex (p = 0.032). We also observed differences relative to age of alcohol initiation (p < 0.001). Specifically, the average age of initiation of consumption in patients with other SUD was about 16 years old, whereas the age of initiation of consumption was about 18 years old in the subgroup with no other SUD. Moreover, patients with other SUD had a higher alcohol symptom severity (p < 0.01) than the group with no other SUD (7.5 versus 6.3 criteria) and higher prevalence of psychiatric comorbidity than patients with no other SUD (82% and 53%, respectively). We evaluated the plasma levels of cytokines in both subgroups, but we did not find any significant differences between these subgroups (data shown in supplementary material).
An additional classification of the alcohol group was performed according to the diagnosis of psychiatric comorbidity (yes (N = 56), no (N = 29)). We only found differences in length of abstinence (p < 0.05). Specifically, patients with psychiatric comorbidity displayed higher duration of abstinence than the group with no psychiatric comorbidity (11.52 versus 4.48 months).
Regarding the circulating cytokines, there were no significant differences in their levels between patients with psychiatric comorbidity and patients with no psychiatric comorbidity (data not shown).
Impact of liver and/or pancreas diseases on plasma levels concentrations of cytokines in AUD patients
Next, we evaluated the effects of another variable associated with AUD, such as liver and pancreatic diseases, on cytokine concentrations in the alcohol group. An additional classification of the alcohol group was performed according to the diagnosis of liver and/or pancreatic disease comorbidities (yes (N = 20 (n: 9 fatty liver; n: 6 cirrhosis; n: 5 pancreatic)), no (N = 65)).
First, we evaluated the differences in the plasma concentrations of IL-1β, IL-4, IL-6, IL-17A, IFN-γ and TNF-α using a one-way ANCOVA according to the ‘alcohol-induced liver and pancreatic diseases’ and ‘age’, ‘BMI’ and ‘sex’ as covariates. To ensure that statistical assumptions were met, a logarithmic transformation (base-10 logarithm) of the concentration of these cytokines was performed. The estimated marginal means after back-transformation are shown in Figure 3.
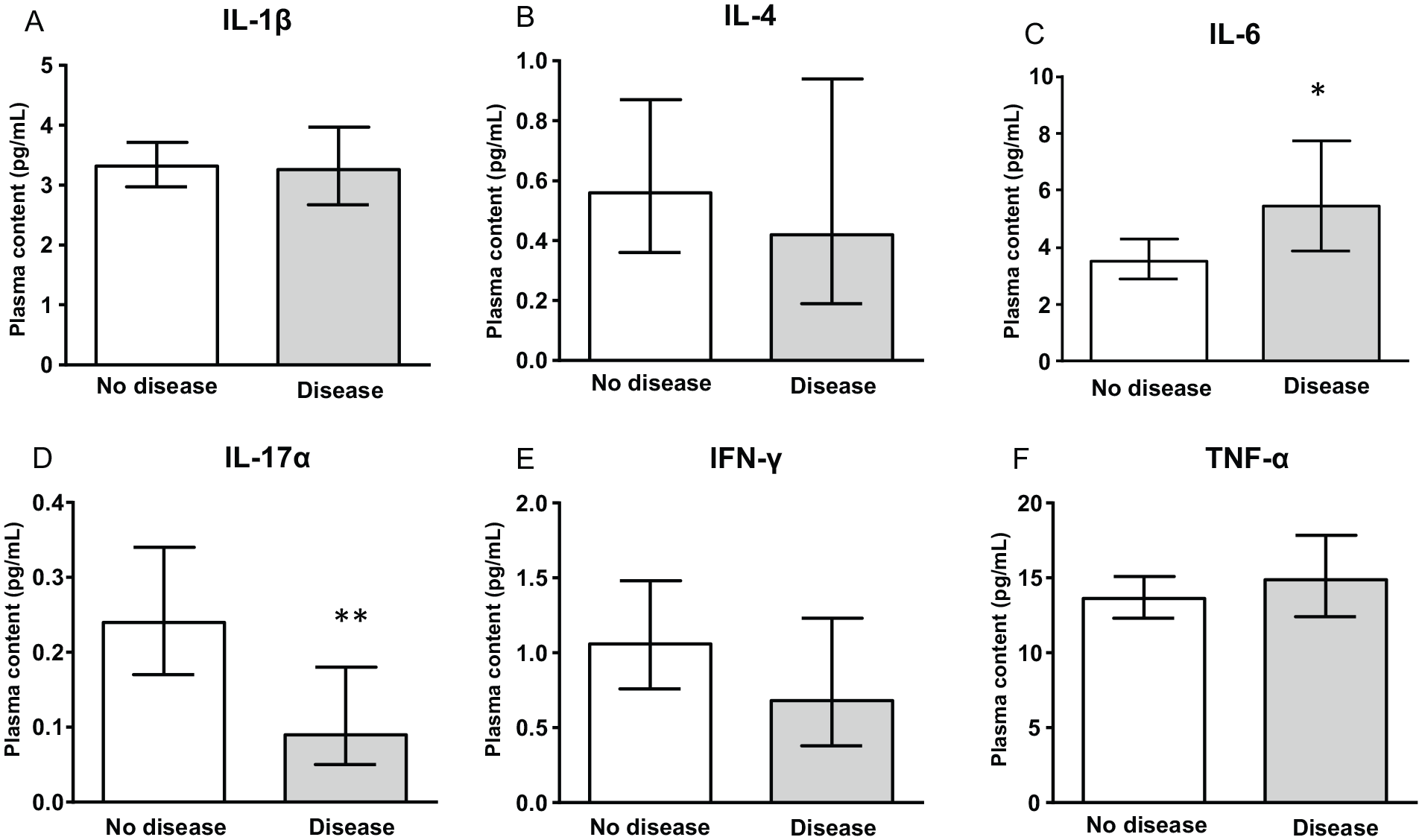
Plasma chemokine concentrations in AUD patients with and without alcohol-induced liver and pancreas diseases. (A) IL-1β, (B) IL-4, (C) IL-6, (D) IL-17A (E) IFN-γ and (F) TNF-γ concentrations according to “alcohol-induced liver and pancreas diseases”. Bars are estimated marginal means and 95% confidence intervals (95% CI) (pg/mL). Data were analyzed by one-way analysis of covariance (ANCOVA), *p < 0.05 and **p < 0.01 denote a significant main effect of “alcohol-induced liver and pancreas diseases”.
Two cytokines were significantly affected by ‘alcohol-induced liver and pancreatic diseases’: IL-6 (F1, 79 = 4.99, p < 0.05), which was influenced by age (p < 0.05) and IL-17A (F1,79 = 6.99, p < 0.01), which was influenced by the BMI (p < 0.05). In fact, we found higher levels of IL-6 and lower levels of IL-17A in AUD patients diagnosed with liver and/or pancreatic diseases than patients with no disease.
Correlation analysis between cytokine concentrations and biochemical parameters associated with liver and/or pancreatic diseases in AUD patients
As shown in Table 4, we performed correlation analyses between the different cytokines evaluated and several biochemical markers of liver and/or pancreatic diseases (pancreatic α-amylase, pancreatic lipase, GGT, AST/GOT and ALT/GPT).
Correlation between cytokine concentrations and biochemical parameters associated to liver and/or pancreas diseases in AUD patients.

AUD: alcohol use disorder; IFN-γ: interferon gamma; IL: interleukin; TNF-α: tumour necrosis factor-alpha; AST/GOT: aspartate transaminase; ALT/GPT: alanine transaminase; GGT: gamma-glutamyltransferase.
Bold indicates statistically significant p value.
denotes significant p value after Benjamini-Hochberg correction.
We observed a positive correlation between GGT and IL-6 concentrations (r = 0.315, p < 0.01). In contrast, there was a negative correlation between pancreatic amylase and TNF-α (r = −0.290, p < 0.01).
Discussion
There are numerous scientific reports describing the contribution of immune system-derived signals to the pathogenesis of psychiatric disorders. However, this contribution is poorly understood in the case of addictive disorders, especially when there are comorbid diseases associated with the primary addiction diagnosis. In the case of AUD, we still do not know in depth how certain immune signals participate in neuronal adaptations after repeated alcohol exposure. Additionally, the contribution of the altered, alcohol-induced immune system to AUD-related harm to the liver and the pancreas is not totally described. In the present study, we evaluated the IL-1β, IL-4, IL-6, IL-17A, IFN-γ and TNF-α concentrations in a sample of patients with AUD in abstinence, recruited from an outpatient treatment programme and analysed the relationship between these cytokine concentrations and comorbid diseases, including psychiatric and liver/pancreatic diseases. This cohort of patients was characterised by a high prevalence of both SUD and psychiatric comorbidities, highlighting the significant effect of length of abstinence in AUD patients with psychiatric comorbidity. The main results are: (a) plasma concentrations of IL-1β, IL-6 and TNF-α were significantly elevated in the alcohol group compared with the control group; (b) plasma concentrations of IL-4, IL-17A and IFN-γ were significantly lower in the alcohol group compared with the control group; (c) AUD patients with alcohol-induced liver and/or pancreatic diseases showed elevated concentrations of IL-6 and lower concentrations IL-17A compared with other AUD patients without liver and/or pancreatic diseases; and (d) IL-1β, IL-6, TNF-α, IL-4, IL-17A and IFN-γ concentrations were not statistically affected by other AUD-related variables, such as abstinence, problematic alcohol use, alcohol symptom severity or psychiatric comorbidity.
Plasma concentrations of cytokines are altered in AUD patients in abstinence
Patients with a history of AUD displayed elevated (IL-1β, IL-6 and TNF-α) and lower (IL-4, IL-17A and IFN-γ) plasma concentrations compared with control subjects. A growing body of evidence suggests a relationship between cytokines and AUD. In this regard, a previous study from our group described the association between immune mediators and psychiatric comorbidity in AUD patients (García-Marchena et al., 2017). The IL-1 system plays a relevant role in alcohol consumption and the development of AUD (Crews and Vetreno, 2011).
Moreover, in clinical models, an increase in IL-6 has been detected in adolescent subjects with intermittent alcohol abuse compared to their controls (Ward et al., 2014). In addition to this, another study that associated types of alcohol consumption and cytokines has shown that moderate alcohol consumption is associated with low levels of IL-6 compared with chronic consumers (Marques-Vidal et al., 2012). Additionally, the concentration of IL-6 is elevated in AUD patients compared with controls, but the concentration decreases during abstinence (González-Quintela et al., 2000). Thus, IL-6 is involved in the pathophysiology of AUD and could be a candidate marker of AUD (Zago et al., 2016).
Furthermore, a significant increase in TNF-α has been observed in adolescent alcohol drinkers compared to controls (Zago et al., 2016).
Few studies have linked the addition of alcohol to the mediator IL-4, as it has been reported that acute ethanol abuse increases IL-4 levels in the liver (Yan et al., 2017). However, in animal models, it has been described that ethanol could inhibit the effect of IL-4 (Aldo-Benson et al., 1992). Additionally, another study from our group did not find statistically significant changes in the plasma levels of IL-4 in patients with cocaine use disorders compared to controls, but we observed significantly lower plasma levels of IL-17A (Maza-Quiroga et al., 2017).
However, there are a few studies that show IL-17A is involved in the effects of alcohol or other abused drugs. As discussed in the next section, IL-17A is a molecule related to liver disorders. For example, a relevant role for IL-17A in alcoholic liver diseases in mice has been described (Blackmore et al., 2015), but in patients with AUD without liver disease, the role of IL-17A has not been studied in depth.
Regarding IFN-γ, a study in healthy young subjects evaluated after a hangover showed high levels of this inflammatory mediator during the hangover and these values decreased after the hangover (Kim et al., 2003). Previous studies and the present results support that alcohol consumption induces changes in the immune system. In addition, it has been detected that the chronic use of alcohol is related to a greater activation of cytokines (Hagström, 2017). Although we found that AUD is linked to significant changes in the balance of the cytokines evaluated, we did not observe changes in their levels associated with AUD severity, other SUD and psychiatric comorbidity.
Plasma concentrations of cytokines are altered in AUD patients with liver and/or pancreatic diseases
In our cohort, about 24% of AUD patients were diagnosed with cirrhosis, hepatitis or pancreatitis. Our results show that IL-6 and IL-17A plasma concentrations in abstinent AUD patients are related to possible liver and/or pancreatic pathologies. The present results showed a significant relationship between plasma cytokine concentrations and these diseases in accessory organs. In this regard, a previous study from our group reported that alcohol-induced diseases in accessory organs affect the plasma concentration of IL-8 (García-Marchena et al., 2017). Consistent with these findings, previous studies have reported that AUD is the leading cause of liver and/or pancreatic diseases worldwide (Gür et al., 2017; Tsujimoto et al., 2008). It is important to clarify that our outpatients enrolled in AUD programmes come mostly from psychiatric/primary care facilities, being less frequent those with severe alcohol liver/pancreatic disease (ALD/APD). Thus, the design of the present study was not oriented to analyse specifically those ALD/APD patients. As such, these data have to be confirmed using specific cohorts of patients with ALD/APD. In these patients, the use of standard blood chemistry panels for fibrosis associated with alcohol liver disease might help to define the stages of the disease, regarding the concentrations of these cytokines.
Changes in IL-6 concentrations may be responsible for hepatic manifestations of AUD. In particular, the increase in IL-6 concentrations correlates with the severity of alcohol-induced liver diseases related to alcohol consumption (Daniluk et al., 2001). An increase in IL-6 concentrations has been found in patients with compensated liver cirrhosis and an increase in IL-6 and TNF-α has been found in patients with decompensate liver cirrhosis, compared to the control population in both cases (Daniluk et al., 2001). Further, IL-6 is related to pancreatic diseases, which include acute pancreatitis, chronic pancreatitis and pancreatic cancer (Lesina et al., 2014).
Regarding IL-17A, several studies have suggested that this cytokine might play a primary role in several liver diseases (Hammerich et al., 2011; Liu et al., 2014). Here we have observed a decrease in the concentration of IL-17A in AUD patients diagnosed with liver and/or pancreatic diseases. By contrast, another study reported elevated concentrations of this cytokine in patients with alcoholic liver disease (Lemmers et al., 2009). These contradictory results may be due to the fact that the patients of the previous study were in active consumption (Lemmers et al., 2009), whereas our AUD patients were in abstinence. Several studies have identified that alcohol consumption alters cytokine concentrations. In addition, some potential candidates for biomarkers have been described (TNF-α, IL-1β, IL-6, IL-8 and IL-12) (Achur et al., 2010). According to our results, chronic exposure to alcohol alters the plasma concentration of IL-1β, IL-4, IL-6, IL-17A, IFN-γ and TNF-α in abstinent AUD patients. In addition, changes in the plasma concentration of IL-6 and IL-17A were associated with the presence of comorbidities of liver and/or pancreatic diseases. These results suggest both cytokines may be candidates for potential biomarkers of alcohol-induced liver and pancreatic diseases, contributing to better prognosis and treatment.
Potential biomarkers could be useful and reliable tools in patients with AUD to confirm the diagnosis, define the current stage of the AUD and diagnose these patients early.
Limitations and future perspectives
We are aware this exploratory study has some limitations that future research should address. First, the small number of female patients in our cohort is a limitation of this study. A higher effort on recruiting female participants is required, as well as better clinical characterisation (stage of menstrual cycle, levels of luteinising hormone, follicle-stimulating hormone and oestrogen, among others) because the average age of the women seeking treatment for alcohol problems usually falls within the menopause transition years. Although our statistical analysis did not reveal that sex had any significant effect, we cannot exclude the influence of this factor on the circulating concentrations of cytokines. Second, it would be necessary to include patients with active alcohol consumption to characterise the effects of the presence of alcohol on the concentration of cytokines. Third, the validity of the results presented here needs to be assessed in a larger sample of patients and include psychiatric patients with no history of substance use disorders. Finally, a specific study in alcohol liver/pancreatic disease patient’s cohort is necessary to identify the stages at which both IL-6 and IL-17A serve as specific biomarkers.
As a future perspective, we need to integrate all the information related to this multiplicity of inflammatory signals in a single model of alcohol addiction. Although certain factors such as IL-6 and IL-17A may contribute to important aspects of alcohol addiction and associated liver and pancreatic diseases, the complexity of the interactions of these inflammatory signalling proteins goes beyond our current knowledge. Further clinical research is necessary to elucidate the role of cytokines in the etiology of AUD and associated comorbidities.
Supplemental Material
Table_5_OH_supplementary – Supplemental material for Abstinent patients with alcohol use disorders show an altered plasma cytokine profile: Identification of both interleukin 6 and interleukin 17A as potential biomarkers of consumption and comorbid liver and pancreatic diseases
Supplemental material, Table_5_OH_supplementary for Abstinent patients with alcohol use disorders show an altered plasma cytokine profile: Identification of both interleukin 6 and interleukin 17A as potential biomarkers of consumption and comorbid liver and pancreatic diseases by Nuria García-Marchena, Rosa Maza-Quiroga, Antonia Serrano, Vicente Barrios, Nerea Requena-Ocaña, Juan Suárez, Julie Ann Chowen, Jesús Argente, Gabriel Rubio, Marta Torrens, Meritxell López-Gallardo, Eva María Marco, Estela Castilla-Ortega, Luis Javier Santín, Fernando Rodríguez de Fonseca, Francisco Javier Pavón and Pedro Araos in Journal of Psychopharmacology
Supplemental Material
z_Figure_1_supplementary_OH – Supplemental material for Abstinent patients with alcohol use disorders show an altered plasma cytokine profile: Identification of both interleukin 6 and interleukin 17A as potential biomarkers of consumption and comorbid liver and pancreatic diseases
Supplemental material, z_Figure_1_supplementary_OH for Abstinent patients with alcohol use disorders show an altered plasma cytokine profile: Identification of both interleukin 6 and interleukin 17A as potential biomarkers of consumption and comorbid liver and pancreatic diseases by Nuria García-Marchena, Rosa Maza-Quiroga, Antonia Serrano, Vicente Barrios, Nerea Requena-Ocaña, Juan Suárez, Julie Ann Chowen, Jesús Argente, Gabriel Rubio, Marta Torrens, Meritxell López-Gallardo, Eva María Marco, Estela Castilla-Ortega, Luis Javier Santín, Fernando Rodríguez de Fonseca, Francisco Javier Pavón and Pedro Araos in Journal of Psychopharmacology
Supplemental Material
z_Table_1_supplemenraty_OH – Supplemental material for Abstinent patients with alcohol use disorders show an altered plasma cytokine profile: Identification of both interleukin 6 and interleukin 17A as potential biomarkers of consumption and comorbid liver and pancreatic diseases
Supplemental material, z_Table_1_supplemenraty_OH for Abstinent patients with alcohol use disorders show an altered plasma cytokine profile: Identification of both interleukin 6 and interleukin 17A as potential biomarkers of consumption and comorbid liver and pancreatic diseases by Nuria García-Marchena, Rosa Maza-Quiroga, Antonia Serrano, Vicente Barrios, Nerea Requena-Ocaña, Juan Suárez, Julie Ann Chowen, Jesús Argente, Gabriel Rubio, Marta Torrens, Meritxell López-Gallardo, Eva María Marco, Estela Castilla-Ortega, Luis Javier Santín, Fernando Rodríguez de Fonseca, Francisco Javier Pavón and Pedro Araos in Journal of Psychopharmacology
Footnotes
Acknowledgements
Author contributions
NG-M, RM-Q and AS contributed equally to this article. Conceived and designed the experiments: PA, FRF and FJP. Performed the experiments: NG-M, PA, AS, FJP, VB and JS. Analysed the data: RM-Q, LJS and NR-O. Contributed reagents/materials/analysis tools: MT, EC-O, LJS and GR. Wrote the paper: PA, FJP and NG-M. Responsible for the study concept and design: PA, FRF and FJP. Coordinated and recruited participants: NG-M, PA and GR. Contributed to the acquisition of psychiatric data through interviews: NG-M, PA and GR. Obtained and processed blood samples: AS, JS, EC-O, FJP and ML-G. Supervised and performed the quantification of cytokines from human plasma: VB, JAC, JA and EMM. Assisted with data analysis and interpretation of findings: LJS, FRF, FJP, MT and PA. Drafted the manuscript: PA, FRF and FJP. Provided critical revision of the manuscript for important intellectual content: MT, LJS, EC-O, VB, GR, AS, JS, JA and EMM. Critically reviewed content and approved final version for publication: all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study has been supported by the following programs and research projects: Subprograma Redes Temáticas RETICS (Red de Trastornos Adictivos, RD16/0017/0001 and RD16/0017/0021) funded by Instituto de Salud Carlos III (ISCIII), Ministerio de Economía y Competitividad (MINECO) and the European Regional Development Fund/European Social Fund (ERDF/ESF); Proyectos de Investigación en Salud (PI16/01953, PI16/01689, PI17/02026 and PI19/00886) funded by ISCIII and ERDF/ESF; Proyectos de Investigación en Drogodependencias (PND2017/043, PND2018/033, PND2018/044 and PND2019/040) funded by Delegación del Gobierno para el Plan Nacional sobre Drogas, Ministerio de Sanidad, Servicios Sociales e Igualdad and ERDF/ESF; Proyecto de Investigación en Salud (PI-0140-2018) funded by Consejería de Salud y Bienestar Social, Junta de Andalucía and ERDF/ESF. NGM holds a ‘Sara Borrell’ research contract (CD19/00019) funded by ISCIII and ERDF-EU. AS, JS and FJP hold a ‘Miguel Servet’ research contract (CPII19/00031, CPII17/00024 and CPII19/00022 respectively) funded by ISCIII and ERDF-EU. ECO holds a ‘Young Researchers’ grant (PSI2015-73156-JIN) funded by Agencia Estatal de Investigación, MINECO and ERDF-EU. PA holds a research project (CI-17-415) funded by the University of Malaga Incorporation to Doctors, Plan Propio.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.