
Abstract
Background:
A large number of studies indicate that subanesthetic doses of ketamine induce a fast antidepressant effect. Limited studies have investigated the subcutaneous (SC) route, and it remains unclear for whom this treatment is most suitable.
Aims:
The aim of this study was to examine the effect on depressive symptoms of repeated subanesthetic doses of SC esketamine in unipolar and bipolar treatment-resistant depression (TRD) and clinical predictors of response.
Methods:
A retrospective analysis of 70 patients who received six SC esketamine doses weekly as an adjunctive treatment was carried out. Doses started at 0.5 mg/kg and it could be titrated up to 1 mg/kg, according to response. The primary outcome was reduction in depressive symptoms. Statistical analysis to investigate clinical predictors of effectiveness included logistic regression analysis using a dependent variable of a 50% reduction in rating scale scores at the end of treatment. Comparisons between groups were made through analysis of variance and treatment effects.
Results:
At baseline, our sample presented with severe treatment resistance in 65.7%, as assessed by the Maudsley Staging Method (MSM), and 47.1% had anxiety disorder comorbidity. The response rate was 50%. A better outcome was predicted by mild and moderate MSM scores (OR = 3.162, p = 0.041) and anxiety disorder comorbidity (OR = 3.149, p = 0.028).
Conclusions:
Our results suggest that higher levels of treatment resistance may be associated with a poor response to SC esketamine. Unlike traditional pharmacotherapies, it might benefit those with poor prognosis such as patients with depression and comorbid anxiety. Therefore, future research could investigate whether esketamine should receive a more prominent place in the treatment algorithm for TRD.
Introduction
Depression is the most common mental health problem in the medical setting, and it is associated with disability and suicide worldwide (World Health Organization (WHO), 2020). The Sequenced Treatment Alternatives to Relieve Depression (STAR*D), a large effectiveness study, showed that about 30% of patients respond to a first pharmacological intervention, and the majority of individuals required more treatment steps in order to achieve remission (Rush et al., 2006). Greater illness severity and chronicity and psychiatric or general medical comorbidities are associated with lower remission rates (Trivedi et al., 2006). Treatment failures and longer duration of symptoms are related to worse prognosis and progression of treatment-resistant depression (TRD), a severe and relatively frequent clinical condition (Fekadu et al., 2018).
Psychiatric and clinical comorbidity is the rule rather than the exception in patients of mood disorders (Kessler et al., 2007; Kroenke et al., 2007), and anxiety symptoms are risk factors to poor outcomes. Depression with anxious features is more difficult to treat, has lower improvement rates and patients are significantly less likely to respond to medication and achieve remission (Fava et al., 2008; Ionescu et al., 2014; Thase, 2018). Therefore, effective treatments for depression with comorbid anxiety are required.
Several studies suggest that subanesthetic doses of ketamine induce a fast antidepressant effect compared to current pharmacotherapies (Papadimitropoulou et al., 2017). Ketamine is a racemic mixture of two enantiomers, S (+) and R (−). The S isomer, esketamine, appears to be a more potent NMDA receptor antagonist than its enantiomer R-ketamine (Andrade, 2017a; Muller et al., 2016; Yang et al., 2015). Compared to its racemic mixture, esketamine has a similar cardiovascular safety profile (Del Sant et al., 2020) and non-inferior antidepressant effect (Correia-Melo et al., 2020). Ketamine has been tested in several routes of administration; moreover, intravenous (IV) infusions are the most extensively researched (Berman et al., 2000; Coyle and Laws, 2015; Murrough et al., 2013). The subcutaneous (SC) route appears to be more viable than IV infusions in terms of cost, safety, tolerability and effectiveness, even in geriatric populations (George et al., 2017). SC ketamine had comparable concentrations to intramuscular (IM) ketamine, and both injections lead to plasma ketamine concentrations that are comparable to the 40-minute IV infusion method (Loo et al., 2016). The bioavailability of IM injections is approximately 93%, whereas the bioavailability of nasal spray is 45% (Quibell et al., 2015). These characteristics enable and encourage its use in outpatient settings.
In March 2019, the United States Food and Drug Administration (FDA) had approved intranasal (IN) esketamine in conjunction with an oral antidepressant for TRD after a large number of phase 2 and 3 studies were published (Canuso et al., 2018; Daly et al., 2018, 2019; Doherty et al., 2020; Popova et al., 2019). Esketamine was also studied in IV route administration (Correia-Melo et al., 2018; Singh et al., 2016) and showed similar response rates in small samples.
Although esketamine has a rapid antidepressant effect, it remains unclear for whom this treatment is most suitable. As supported by evidence, features associated with better response include a positive family history of alcohol abuse disorder in first-degree relatives (Pennybaker et al., 2017), no personal history of suicide attempts, higher body mass index (Niciu et al., 2014), lower baseline speed of processing (Murrough et al., 2015) and anxious depression (Ionescu et al., 2014). Research of clinical characteristics that may indicate improvement of depression with esketamine trials is critical due to the current scarcity of predictors of response.
This study aims to investigate the effect on depressive symptoms of repeated subanesthetic doses of SC esketamine in a retrospective naturalistic cohort of unipolar and bipolar TRD patients and to identify clinical predictors of treatment response.
Methods
Participants
The data included in this report is selected from the medical records of 70 sequential patients treated in an academic clinical program (the esketamine clinic) of the Psychiatry Department of the Federal University of Sao Paulo (UNIFESP) from April 2017 to December 2018. We performed a retrospective analysis in a large case series of 70 TRD outpatients to examine the impact of adjunctive SC esketamine on depressive symptoms. All patients were referred to the esketamine clinic by their treating psychiatrist due to lack of improvement of symptoms of their depressive episode. SC bolus esketamine injections were administered once a week as part of their clinical care. Only patients who completed the full 6-week adjunctive esketamine treatment protocol were included in this study. Patients who decided to interrupt the treatment were not considered for the purposes of this study.
An electronic database created at REDCap - Research Electronic Data Capture (Harris et al., 2009) stored patients' clinical and demographic information. Ethical approval and a waiver of consent was provided by the Ethics Board of the Federal University of Sao Paulo. All patients signed a written informed consent describing esketamine's risks and limitations, and they consented to their data being used in future research.
Pretreatment assessment
At baseline, a certified psychiatrist confirmed the DSM-IV depressive episode and psychiatric diagnoses of either major depressive disorder or bipolar disorder applying the MINI International Neuropsychiatric Interview - MINI Plus 5.0 (Lecrubier et al.,1997). Requirement of enrollment was a moderate or severe depressive episode, assessed by the Montgomery-Åsberg Depression Rating Scale – MADRS, i.e., baseline MADRS score ⩾ 20 (Montgomery et al., 1985) and without response to two or more adequate antidepressant treatments during the current episode.
History of psychotic symptoms, suicide ideation or psychiatric comorbidities were not exclusionary, except from substance abuse disorder. Anxiety disorder comorbidity was defined as having at least one of the following diagnoses assessed by MINI Plus 5.0: generalized anxiety disorder, panic disorder, post-traumatic stress disorder, phobias-related disorder or obsessive compulsive disorder.
Level of treatment resistance
The Maudsley Staging Method (MSM) (Fekadu et al., 2009) was used to assess the level of treatment resistance. Composite scores of the MSM are based on duration, severity and treatment history of the current episode and were determined retrospectively. Such severity gradation would be useful to describe TRD populations. Total score ranges from 0 to 15 and is categorized into three levels: mild (3 to 6 points), moderate (7 to 11 points) and severe (11 to 15 points).
Treatment protocol and longitudinal assessments
This was a multiple dose treatment that followed an ascending dose protocol. Patients were advised to remain on their usual medications and received one SC bolus injection of esketamine once a week during a 6-week period. Doses were administered by a psychiatrist, certified with Basic Life Support, with the assistance of a nurse. At the first treatment session, all patients received a 0.5 mg/kg SC bolus injection of esketamine. We assessed symptom response every 7 days after each esketamine dose, which was defined as a ⩾50% improvement in MADRS score compared with the baseline score rated in the first interview (Zimmerman et al., 2004). If the patient did not meet the criterion for response in symptoms 7 days after treatment, and the dose was well tolerated, the esketamine dose was titrated to 0.75 mg/kg. On the following assessment, if response was still not met, the dose was titrated to 1.0 mg/kg in the following injections.
Given that this treatment is relatively novel in the field, it still does not have a well-established protocol. However, a review presented that the 0.5 mg/kg dose may remain the default and that higher doses may benefit patients who do not respond in 0.5 mg/kg sessions (Andrade, 2017b). In addition, an analysis (Loo et al., 2016) has shown, based on an individual dose-titration study, that 0.2–0.3 mg/kg is a threshold dose for reducing severity of depression in patients with TRD, and that higher doses (up to 0.5 mg/kg) appear to have more robust antidepressant effects. Finally, doses were titrated up to 1 mg/kg because it was reported that the 1 mg/kg dose had the greatest durability of response in patients with TRD (Glue et al., 2017).
Patients were monitored for at least 2 hours after each esketamine dose to manage possible side-effects, taking into account the risk of sedation and dissociation, as well as to carefully assess heart rate, blood pressure and digital pulse oximetry every 15 minutes (cf. Del Sant et al., 2020).
Statistical analysis
Our primary outcome of interest was decreasing depressive symptoms, i.e., the reduction in MADRS scores over time. We first calculated the percentage change in MADRS score from baseline to the end of follow-up (scheduled 7 days after the sixth dose, i.e., on day 42), creating two subsets of patients afterward. The first were defined as
The chi-squared test, Fisher's exact test or independent sample t-test were duly applied to compare baseline demographic and clinical features between them, whenever appropriate. We investigated clinical predictors of treatment response using multiple logistic regression including ‘level of treatment resistance’ and ‘anxiety disorder comorbidity’ and all variables that attained a statistical significance of up to 20% in the univariate analyses. Our regression model included the examination of the interaction between variables 'level of treatment resistance’ and ‘anxiety disorder comorbidity' to determine if the effects were independent and whether anxiety would influence treatment resistance.
Repeated measures analysis of variance addressed changes in MADRS score at anchor moments to investigate differences among these groups (anxiety comorbidity and/or severe MSM, using response as the dependent variable). Repeated measure analysis (ANOVA) relies on normality distribution as an assumption, which was accomplished with the Kolmogorov–Smirnov test. Bonferroni correction was applied to correct for multiple comparisons. The effect size was calculated using Cohen’s index. Missing data were included with the Last Observation Carried Forward (LOCF) methodology.
All statistics were conducted using SPSS version 23 and Stata version 12. Significance was considered at p < 0.05, two-tailed.
Results
Our sample had 70 patients: 64 completed the 6-week SC esketamine treatment and six patients did not. Three patients requested to interrupt treatment after the 3rd dose and three patients after the 4th dose, and they were considered in our analysis using the LOCF method.
At the end of follow-up, 50% (n=35) of the sample were considered responders (⩾50 % improvement in MADRS final score, compared with baseline one). In this group, MADRS final score mean was 9.9 (SD=3.9), ranging from 1 to 18; and 25.7% (n=18) of patients achieved full remission, i.e., MADRS final score ⩽10 (Zimmerman et al., 2004). In the remainder of patients, 50% (n=35) were considered non-responders (
The MADRS baseline score mean was 33.6 (SD=6.4), ranging from 22 to 50. No statistically significant differences were found (t=-0.560, p=0.577) on MADRS baseline score comparing responders and non-responders. Diagnosis, age, gender, education or the absence of previous suicide attempts were not associated with response. Table 1 presents baseline and clinical features by response status. For most patients (72.9%, n=51), the esketamine dose was titrated to 1 mg/kg, the maximum protocol dose. This was a flexible-dose study and dose–response relationships were not evaluated.
Demographic and clinical characteristics of patients broken down by total, responders and non-responders.
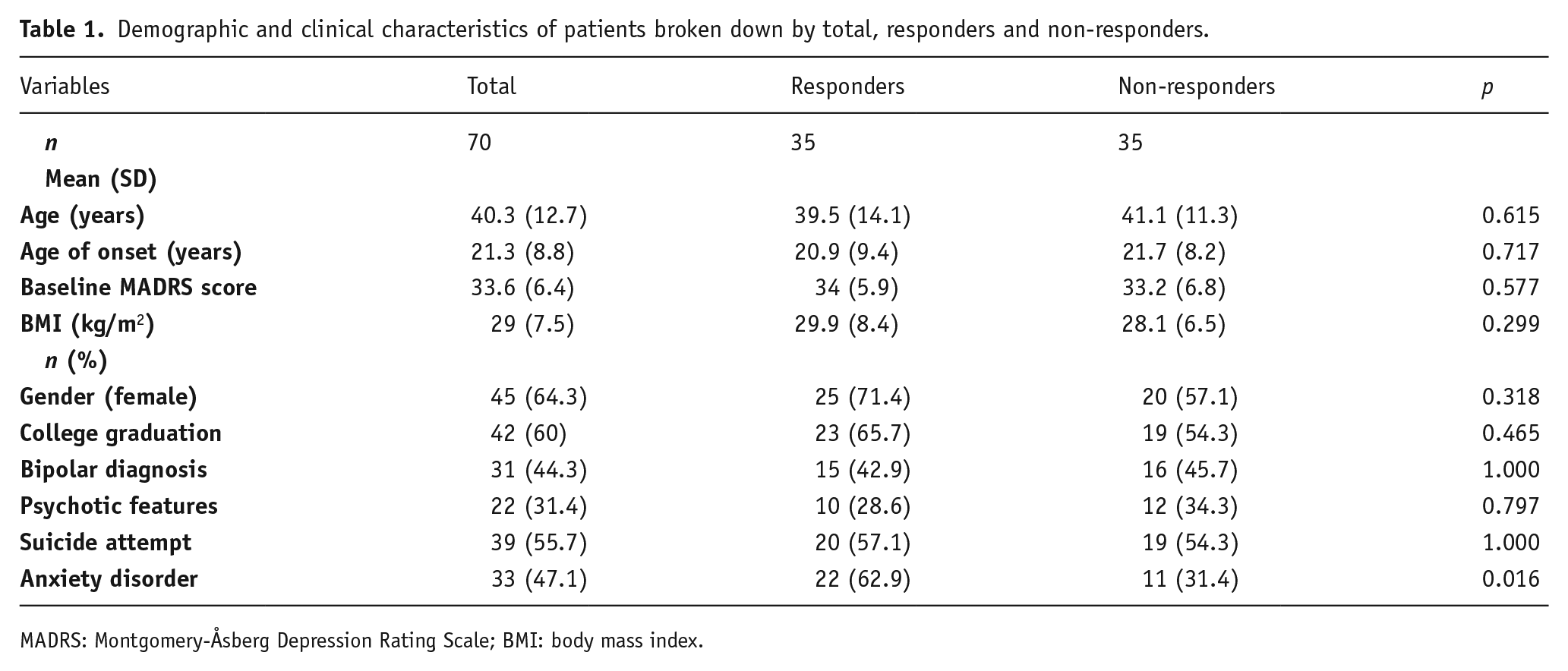
MADRS: Montgomery-Åsberg Depression Rating Scale; BMI: body mass index.
According to MSM, baseline features demonstrated a severe level of resistance in this population. Frequencies of MSM are displayed in Table 2, stratified by treatment response. For further investigation, patients were broken down into two groups according to MSM total score, severe versus non-severe (which included mild and moderate scores).
Maudsley Staging Method: frequencies and scores broken down by total, responders and non-responders.
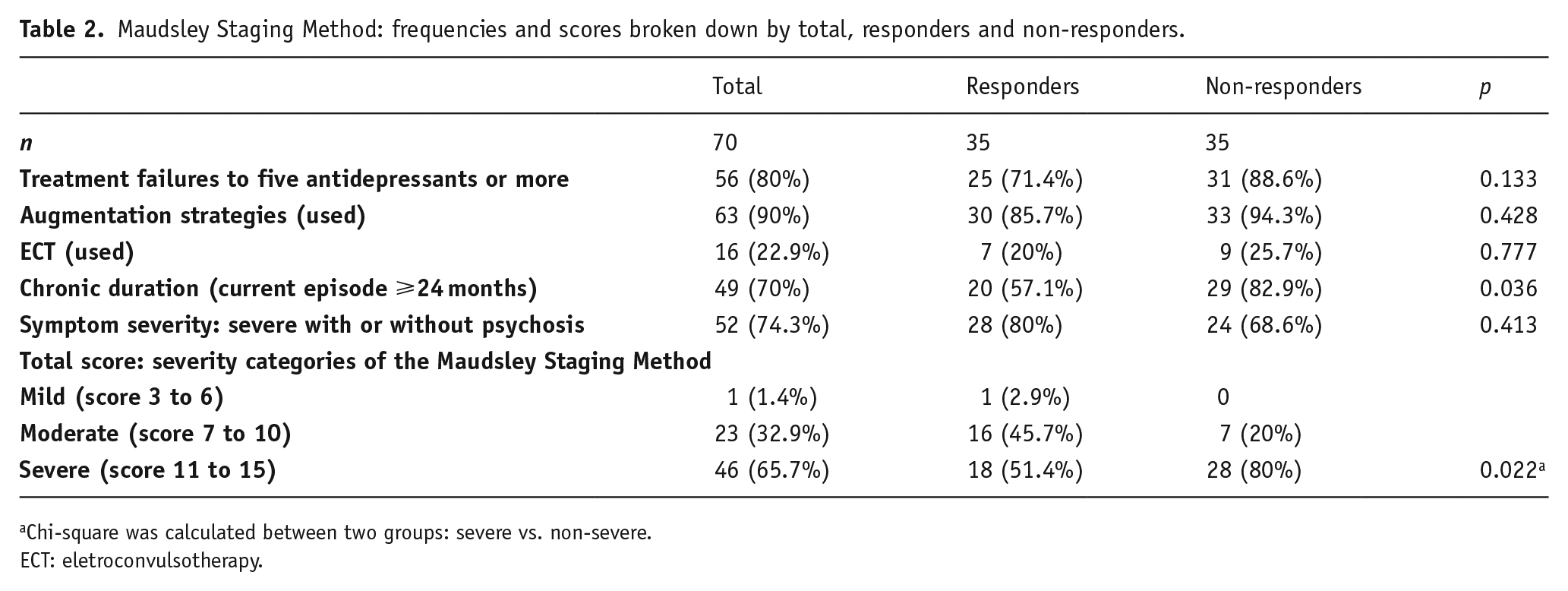
Chi-square was calculated between two groups: severe vs. non-severe.
ECT: eletroconvulsotherapy.
Predictors of treatment response
Multiple logistic regression was applied to investigate predictors of outcome, using response as the dependent variable.
Anxiety disorder comorbidity (AD) and non-severe MSM score, and their interaction were used as the independent variables. Patients with non-severe MSM scores were three times more likely to respond to SC esketamine (OR=3.162, p=0.041), as well as patients with anxiety disorder comorbidity (OR=3.149, p=0.028). Interaction between these factors did not reach statistical significance (p=0.273). Considering non-severe MSM score and AD comorbidity as response predictors, the area under the receiver operating characteristic (ROC) curve was 0.72 (95% confidence interval (CI) 0.60–0.84), 80% sensitivity and 60% specificity.
Level of treatment resistance and anxiety disorder comorbidity
We separated our sample into four groups to examine the antidepressant effect variance of esketamine: non-severe MSM scores with and without AD, and severe MSM score with and without AD. A repeated measure ANOVA was used to examine variance in MADRS raw score at the baseline and 7 days subsequent to each session. In terms of significant effects over time, there was an overall main effect of dose with reduced depressive symptoms across all groups (all p<0.01); furthermore, groups had different trajectories (Time X Groups F18,391=2.43, p=0.001). Patients with severe MSM scores without AD had a poor outcome compared to the other groups: there was a reduction in MADRS baseline score after the first dose, leveling off afterward, in contrast to what was observed in the other groups.
Bonferroni correction demonstrated a marginal difference in two groups: non-severe MSM score with AD and severe MSM score without AD (p=0.067); without Bonferroni correction this difference reached statistical significance (p=0.011). The standardized mean difference measure of effect was −1.01 (95% CI: −1.65 to −0.34). Differences in groups are displayed in Figure 1.
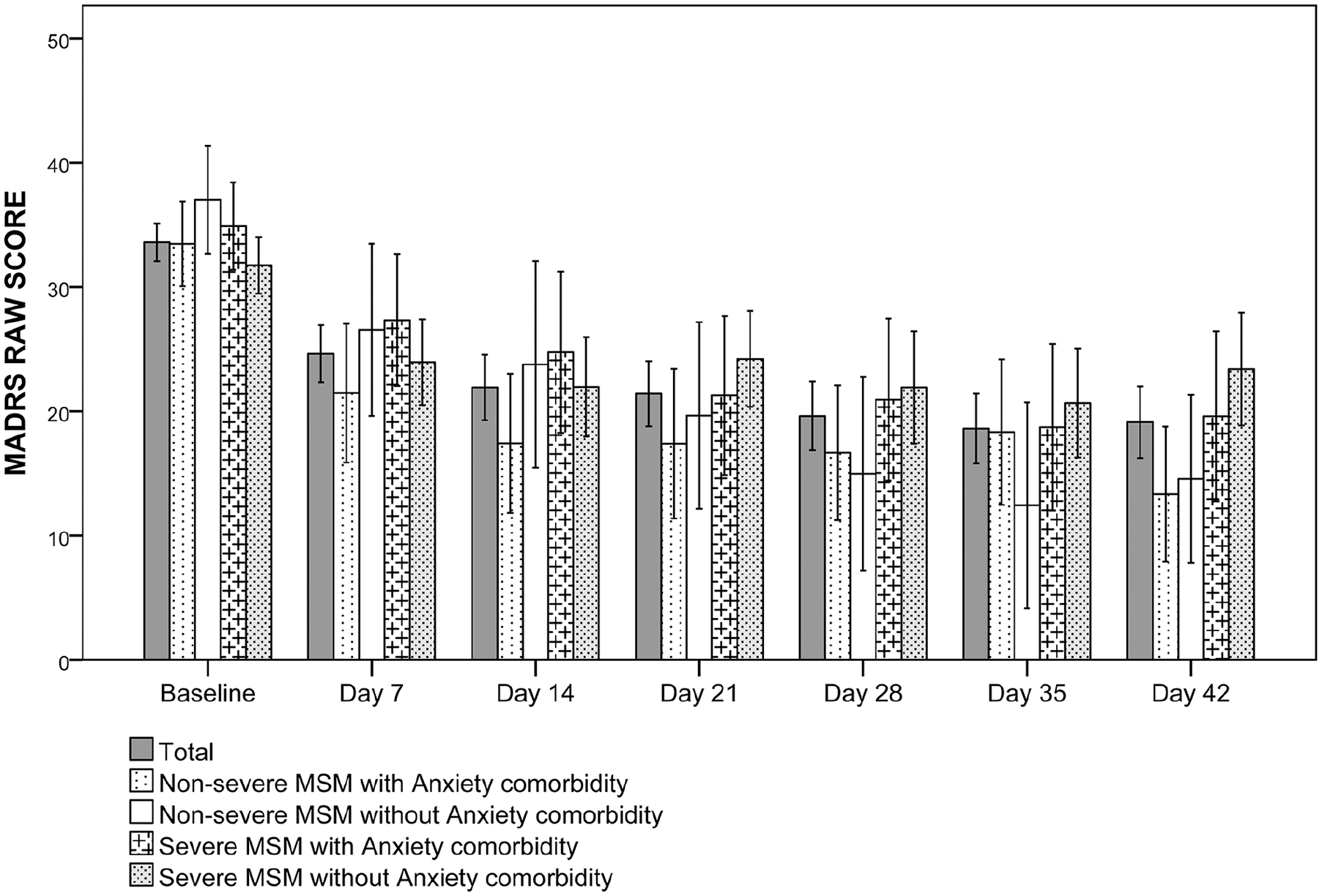
Change in MADRS score means comparing groups.
Discussion
This study presents data suggesting that repeated SC esketamine may have an impact on depressive symptoms of unipolar or bipolar TRD patients. Comorbid anxiety disorders are usually mentioned as a risk factor for treatment resistance (Fava et al., 2008); however, in our sample, it was not associated with worse outcomes. Higher levels of treatment resistance were the main factor related to poor response. Our population had a high level of treatment resistance: 80% of patients had experienced failed treatment with five antidepressants and the current episode lasted for more than 2 years for 70%.
Prior studies have shown that SC esketamine may be safe, feasible and effective along with standard antidepressant therapies under real-world conditions (George et al., 2017; Glue et al., 2017; Iglewicz et al., 2015; Loo et al., 2016). Long-term safety concerns with ketamine for treating depression stem from preclinical studies and from adverse effects observed in long-term recreational users of ketamine. The TRANSFORM-3 Study reported that treatment-emergent adverse events were transient and ultimately safe in several assessments, such as hematology and serum chemistry, urinalysis, physical examination, electrocardiogram, suicidal ideation, dissociation symptoms and cognition (Ochs-Ross et al., 2020). We have described the cardiovascular safety of repeated SC esketamine elsewhere (Del Sant et al., 2020).
The SC esketamine route decreases costs dramatically compared to the IV route. In compliance with local regulations, an anesthesiologist was not required to administer the doses. Doses were administered by a psychiatrist with the assistance of a nurse. Moreover, it was performed in outpatient facilities with SC bolus injections, and also dismisses the need for venous access and infusion pumps. In addition, esketamine is a relatively inexpensive medication: in Brazil, one esketamine ampoule (50 mg/mL, 2 mL) costs BRL R$15.00 (approximately US$2.70) and amounts to approximately two doses.
Our sample received six SC esketamine doses with response rates comparable to open-label studies that administered six IV ketamine infusions. The Thomas et al. study described response rates of 44% with remission rates of 16%. In addition, in the Zhou et al. study, the response rate was 54.8% and remission 31%. Both studies also included unipolar and bipolar patients, and anxiety comorbidity was not excluded (Thomas et al., 2018; Zhou et al., 2018).
Although differences in study design limit direct comparisons, esketamine has been investigated in routes other than SC in double-blind and randomized studies for TRD, mostly with administrations twice a week (Daly et al., 2018, 2019; Popova et al., 2019; Singh et al., 2016). Moreover, these authors’ samples are quite different from ours: including only unipolar patients while excluding bipolar depression, suicidal ideation, depression with psychotic features and obsessive compulsive disorder, among others.
Singh and colleagues studied IV esketamine in a small sample (n = 30) presenting a response rate of 67% at day 35 after four infusions (Singh et al., 2016). Another study with a small sample also investigated IN esketamine administered twice a week, and the response rates at day 15 ranged from 36% to 50% depending on the dosage, and the group that received placebo had a 10% response rate (Daly et al., 2018). In phase 3, a double-blind multicenter study (Popova et al., 2019) assessed 223 patients thus comparing responses to IN esketamine versus placebo, both adjunctive to a newly initiated oral antidepressive. Esketamine was administered twice a week for 28 days with a response rate of 69.3%. They also presented a high response rate to the oral antidepressant plus placebo, amounting to 52%. During phase 3, a double-blind randomized study to assess effectiveness and relapse time with the administration of IN esketamine was investigated among a larger sample (n=297), and it was observed that continued treatment with IN esketamine could sustain antidepressant effects during a greater time span and delay relapse time compared to placebo (Daly et al., 2019). Canuso and colleagues also investigated IN esketamine, and this was the only study that did not exclude suicidal ideation. Patients were diagnosed with MDD without psychotic features at imminent risk of suicide; however, bipolar depression was also a criterion of exclusion. IN esketamine was administered twice a week for 4 weeks, and compared and contrasted with placebo. They revealed a rapid reduction of depressive symptoms 4 hours after the first dosing; however, this reduction did not reach statistical significance against the placebo’s results on day 25 (Canuso et al., 2018). In a recent meta-analysis (McIntyre et al., 2020), the short-term efficacy of IV and IN ketamine/esketamine for adults with TRD was established.
In a review (Rong et al., 2018), predictors of response to ketamine identified the following: body mass index, history of suicide attempts and family alcohol use disorder; however, these findings were not replicated in our sample. In our population treated with esketamine, characteristics of severe mental illness, such as bipolar depression, psychotic features, MADRS baseline score, and history of suicide attempts were not predictors of response.
Anxiety comorbidity is usually associated with poor outcomes (Fava et al., 2008; Hung et al., 2020), and it is a replicated risk factor for TRD itself (Kautzky et al., 2019). In our sample, patients with anxiety disorders were more responsive to esketamine: anxiety disorder at baseline presented a three-fold increase in likelihood of responding at the end of the protocol. The utility of ketamine for treating anxiety has been investigated in several studies (Sartori and Singewald, 2019). Researchers have demonstrated the critical role of glutamate in neuroplasticity relating it to antidepressant and anxiolytic effect (Duman et al., 2016). Patients with anxious depression relapsed significantly later than those with non-anxious depression after a single IV ketamine infusion (Ionescu et al., 2014).
Several studies (Glue et al., 2017, 2018, 2020; Taylor et al., 2018) that investigated ketamine's anxiolytic effects excluded severely depressed patients to ensure that changes in anxiety ratings were not confounded by comorbid depression. SC route of administration was investigated in a small sample (n=12) of refractory generalized anxiety disorder and, after three SC ketamine doses, patients presented an 83% response rate in anxiety rating scales (Fear Questionnaire and Hamilton-Anxiety) (Glue et al., 2017); those who responded received a maintenance treatment over 3 months and most patients reported marked improvement in work and social functioning (Glue et al., 2018). Another replication of this study with a more robust design (including a double-blind and control) also reported ketamine's anxiolytic effects (Glue et al., 2020). Taylor and colleagues compared a single IV ketamine dose with placebo and also presented evidence that ketamine may be effective in reducing anxiety (Taylor et al., 2018).
Studies (Trivedi et al., 2006) have consistently demonstrated that the duration of depression is associated with worse response to treatment, and it is a risk factor for the development of chronic illness (Hölzel et al., 2011), as well as a higher burden of disease. As we expected, the main factor in predicting poor response in our sample was a higher level of treatment resistance.
Improving the management of patients who did not experience remission is a key challenge for clinical practice. It may be inappropriate to wait until a patient has a two-year long illness to bring non-standard interventions into consideration, since the proposed treatment algorithm for multiple-therapy resistant depression needs to be preemptive (McAllister-Williams et al., 2018). Our findings suggest that many topics need to be addressed, for instance whether TRD patients have a better prognosis if esketamine treatment is used early on or if esketamine should have a more prominent role in the treatment algorithm for TRD. Double-blind, randomized and controlled studies are needed to confirm esketamine’s long-term safety and efficacy prior to considering its administration as routine pharmacotherapy.
Limitations
The current study had several limitations. First, we assessed a small sample with characteristics inherent to real-world analyses, such as lack of randomization and the absence of a control group. The last follow-up evaluation happened 1 week after the last dose; thus, no conclusions can be drawn on relevant aspects of esketamine treatment such as time to relapse or beneficial effects of repeated administrations. Furthermore, our subjects are patients from a single academic site and may not be truly representative of TRD patients.
Additionally, all participants continued to receive prior prescribed medications. They took a high variability of oral psychotropic medications that were not possible to control, which may have influenced outcomes.
Finally, this study was a flexible-dose study and dose–response relationships were not evaluated. Our protocol had an ascending dose depending on treatment response, rather than a randomized or fixed-dose design.
Conclusion
Our results suggest that a higher stage of treatment resistance may be associated with a poor response to SC esketamine regarding a short-term effect. Otherwise, patients with anxiety disorder comorbidity were more responsive to esketamine, as opposed to traditional pharmacotherapies. A critical issue is improving the management of those difficult-to-treat groups of anxious and chronic TRD patients. Replications of these findings are needed to establish the ideal schedule of esketamine to extend its antidepressant properties; hence, reaffirming the SC use of esketamine for TRD and an effective maintenance protocol.
Non-standard interventions are only brought into consideration much later, which might ultimately compromise the patient’s well-being. TRD is a widespread burdensome condition with long-standing untoward consequences, reduced quality and years of life, and impaired social and work functionality. There is a need for novel non-standard interventions that are not only effective but also able to change the progression of depressive disorders when used in proper time spans.
Further research and clinical trials are key in order to effectively and safely investigate whether esketamine could be an intervention to lower the risk of chronicity and treatment resistance in TRD and, therefore, whether esketamine should receive a more prominent place in the treatment algorithm. Once these studies are in place and long-term safety of administering esketamine is confirmed, it will most likely be used earlier in the treatment algorithm and change the very course of the illness as we know it.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Lucchese has nothing to disclose; Dr. Sarin reports personal fees from Daiichi Sankyo Brasil, personal fees from Lundbeck Brasil, personal fees from Pfizer, personal fees from Janssen, non-financial support from Takeda Brasil, non-financial support from Moksha Brasil, non-financial support from Torrent Pharma, outside the submitted work; Dr. Muniz Magalhães reports non-financial support from Torrent Pharma, non-financial support from Hypera Pharma, outside the submitted work; Dr. Del Sant has nothing to disclose; Dr. Puertas has nothing to disclosure; Dr. Oliveira reports personal fees from Janssen, outside the submitted work; Dr. Nakahira reports non-financial support from Eurofarma, non-financial support from Cristália, non-financial support from Sanofi, outside the submitted work; Dr. Nakahira reports non-financial support from Eurofarma, non-financial support from Cristália, non-financial support from Sanofi, outside the submitted work; Dr. Fava has nothing to disclose; Dr. Delfino has nothing to disclose; Dr. Surjan has nothing to disclose; Dr. Steiglich has nothing to disclose; Dr. Barbosa has nothing to disclose; Dr. Abdo has nothing to disclose; Dr. Molina Cohrs has nothing to disclose; Dr. Del Porto has nothing to disclose; Dr. Lacerda has received consulting fees from Janssen Pharmaceutical, Daiichi Sankyo Brasil, Cristália Produtos Químicos e Farmacêuticos, Pfizer, Mantecorp Indústria Química e Farmacêutica, Libbs Farmacêutica and Sanofi-Aventis over the last 24 months and has received research fees from Janssen Pharmaceutical, Eli Lilly, H. Lundbeck A/S, Servier Laboratories, Hoffman-La Roche and Forum Pharmaceuticals, not related to the submitted manuscript; Dr. Sergio Baxter Andreoli has nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Coordination of Improvement of Higher Education Personnel – Brazil (CAPES) – Financing Code 001.