
Abstract
Background:
Depression is considered as one of the most common neuropsychiatric symptoms (NPS) in Alzheimer’s disease (AD) patients. Prescription of antidepressants is a current clinical practice well-established as the first-line treatment for such patients. Our study was aimed at systematically examining the evidence on the efficacy of antidepressants in the treatment of depression in AD patients.
Methods:
We conducted a network meta-analysis of randomized controlled trials retrieved by systematic search of the Cochrane Central Register of Controlled Trials, PubMed, Embase, and CNKI databases. Primary outcomes included mean depression score and safety. Secondary outcomes were cognition. The surface under the cumulative ranking curve was performed to estimate a ranking probability for different treatments.
Results:
A total of 25 studies including 14 medications met the inclusion criteria. Compared with placebo, only mirtazapine (standard mean deviation [SMD], −1.94; 95% confidence interval [CI], −3.53 to −0.36; p < 0.05) and sertraline (SMD, −1.16; 95% CI, −2.17 to −0.15; p < 0.05) showed a slightly better effect in treating symptoms of depression. Clomipramine increased risk of adverse events than placebo (odds ratio, 3.01; 95% CI, 1.45 to 4.57; p < 0.05). In terms of cognitive function, there was no statistically significant difference between antidepressants and placebo.
Conclusion:
Overall, in the short-term treatment, these data suggest that commonly used antidepressants sertraline and mirtazapine should be considered as an alternative treatment for depression in AD patients. However, more high-quality trials with large samples and longer following-up are proposed.
Introduction
Depressive disorder is widely recognized as one of the most common neuropsychiatric symptoms (NPS) in Alzheimer’s disease (AD) with approximately 4.8% to 50% of patients with AD meeting the diagnostic criteria for major depressive disorder (Modrego, 2010). Depression in AD currently affects more than 7 million Chinese people and this figure is expected to triple by 2050 (Jia et al., 2018). The presence of depression among AD patients has been associated with poor quality of life, a higher rate of disability, a faster decline in cognitive function, relatively excess mortality, and an increase in caregiver burden (Brzezinska et al., 2020; Cannon-Spoor et al., 2005; Kaup et al., 2007; Scazufca et al., 2002).
Various classes of antidepressants are widely used for this condition, including tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and monoamine oxidase inhibitors, etc. (Lozupone et al., 2018). Multiple clinical trials have been conducted to investigate their therapeutic effect on depression in AD. Nevertheless, a growing body of evidence reveals that antidepressant use is also associated with an increased risk of adverse effects and events in older people, such as nausea, diarrhea, falls, hip fractures, cardiovascular events, all-cause mortality, and orthostatic hypotension (Coupland et al., 2011; Maslej et al., 2017; Taipale et al., 2017; Torvinen-Kiiskinen et al., 2017). Research has indicated that patients with dementia receiving TCAs may suffer severe cognitive impairment due to anti-cholinergic side effects (Nishtala et al., 2009). Although SSRIs are currently the gold standard treatment for elderly patients with depression, they have been found to be ineffective in treating depression symptoms in patients with AD (Banerjee et al., 2011; Rosenberg et al., 2010). Four prior systematic reviews and meta-analyses have examined effectiveness in people with depression and dementia, but all are not conclusive (Modrego, 2010; Nelson and Devanand, 2011; Orgeta et al., 2017; Thompson et al., 2007). In this study, we aimed to conduct a systematic review and network meta-analysis to make comparisons among different antidepressants for the treatment of patients with AD.
Methods
Search strategy and selection criteria
A systematic search of The Cochrane Central Register of Controlled Trials, PubMed, Embase, and China National Knowledge Infrastructure (CNKI) was performed from database inception through to May 8, 2020. We used the search keywords depression or depressive disorder and Alzheimer’s or AD and antidepressants or antidepressive drugs. In addition, the reference lists of the included studies and relevant reviews were screened for additional studies.
Trials were considered eligible if they met the following criteria: (1) they were double-blind, randomized controlled trials (RCTs) comparing antidepressants with placebo or another active antidepressant; (2) they enrolled subjects with clinical diagnosis of AD (irrespective of pathologic confirmation); (3) subjects had a diagnostic of depression according to a validated rating scale: Cornell scale for depression in dementia (CSDD), Hamilton depression rating scale (HDRS), Montgomery-Asberg depression rating scale (MADRS), geriatric depression scale (GDS) or diagnostic and statistical manual (DSM); (4) the original research article provides sufficient data for further analysis. Two reviewers (Yanhong He and Hao Li) independently screened the full text of potentially relevant publications using a structured manual. Disagreements were resolved by consensus.
Outcomes
The primary outcome was efficacy (mean change in depression score from baseline to the endpoint) and safety (number of adverse events). The preferred depression score scale to measure the outcome was CSDD and then any other scale, such as HDRS, MADRS, GDS, DSM. The secondary outcomes were a measure of the cognition mini-mental status examination (MMSE). Results from intention-to-treat analysis were preferred over results from per-protocol or completer analysis. For cross-over trials, only data from the first stage are used.
Data extraction
The data extracted from each report included baseline participant characteristics, study drug, concomitant medications, and depression score. For the effect size calculation, we extracted sample sizes, means, and standard deviations (SDs) for each treatment group. If these values were missing, other statistical data that could be converted into means and SDs were extracted. If change scores were not reported, they were imputed using the difference between baseline and endpoint. The SD of the change score was imputed using the technique as reported (Higgins et al., 2020). Studies were excluded if the missing outcome data could not be calculated, imputed, or obtained from the authors. For the calculation of odds ratio (OR) as an indicator of treatment safety, we extracted the number of adverse events.
Assessment of the risk of bias (RoB) of the included studies was conducted by two authors in duplicate (Yanhong He and Jinbo Huang) using the Cochrane RoB assessment tool (sequence generation, allocation concealment, blinding, selective reporting bias, and attrition bias) (Cumpston et al., 2019). We evaluated the potential for publication bias by visual inspection of funnel plots to identify asymmetry.
Data analysis
Network meta-analysis was performed to evaluate the direct and indirect evidence in a network of trials that compare multiple interventions. The standard mean deviation (SMD) and corresponding 95% confidence interval (CI) were calculated for depression scores and MMSE scores. Additionally, for safety monitoring, ORs and 95% CI were calculated. We assumed a two-sided p < 0.05 to indicate statistical significance.
We used a random-effects model to represent overall effect estimate comparisons. Statistical evaluation of inconsistency and generation of network graphs and result figures were performed using the network and network graphs packages in Stata software version 15 (Stata Corp. LP, College Station, TX, USA). The surface under the cumulative ranking curve (SUCRA) value and the mean ranks were calculated to rank the therapeutic effect of the various outcomes. The larger the SUCRA value, the better the rank.
Inconsistency was also tested formally using an overall chi-squared test of inconsistency. In addition, a loop-specific approach will be applied to assess the inconsistency between direct and indirect evidence.
Results
Study characteristics
A total of 599 records were identified during the search and 72 articles were considered potentially relevant after the initial screening of titles and abstracts (Figure 1). Overall, 25 published RCTs comparing 14 antidepressants or placebo were included in our analysis (Table 1). 14 studies were placebo-controlled trials (An et al., 2017; Banerjee et al., 2011; Chen, 2014; de Vasconcelos et al., 2007; Fuchs et al., 1993; Lyketsos et al., 2003; Magai et al., 2000; Nyth and Gottfries, 1990; Passeri et al., 1985; Petracca et al., 1996, 2001; Rosenberg et al., 2010; Teri et al., 1991; Zhao et al., 2015), and 11 antidepressants comparison trials did not include a placebo (Fei et al., 2010; Katona et al., 1998; Liu et al., 2011; Mokhber et al., 2014; Ren et al., 2004; Su et al., 2007; Taragano et al., 1997; Wang et al., 2005; Wu and Zhang, 2007; Zhou and Chi, 2012; Zhu et al., 2006). Three of the 25 included trails had three arms, and ten were head-to-head trial. Nine studies explicitly report a diagnosis of probable AD according to the Chinese Classification of Mental Disorders criteria, whereas others used National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association criteria and Diagnostic and DSM criteria. Most studies (N = 21) met the criteria for probable or possible AD.
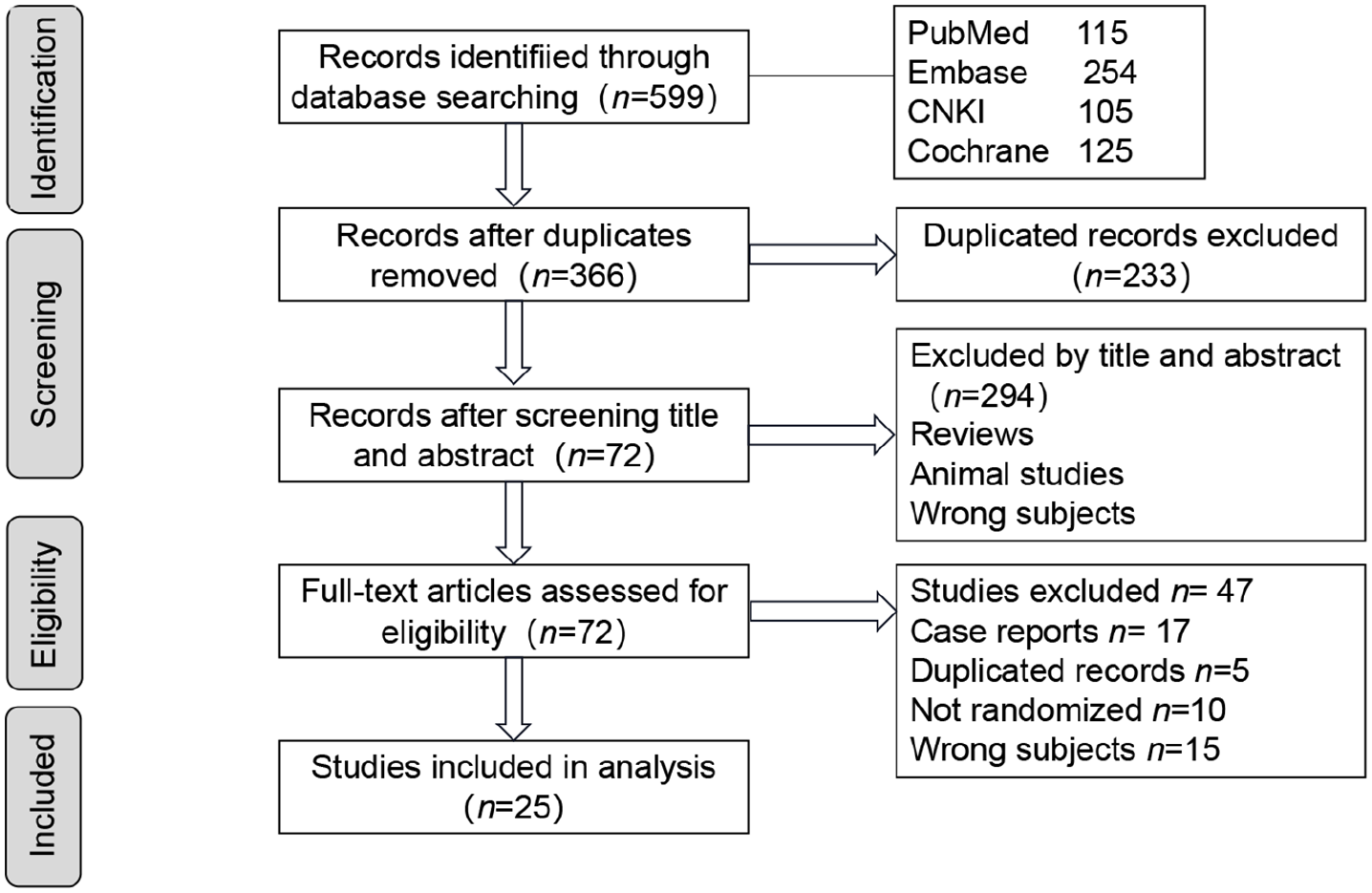
Study selection process.
Characteristics of included studies.
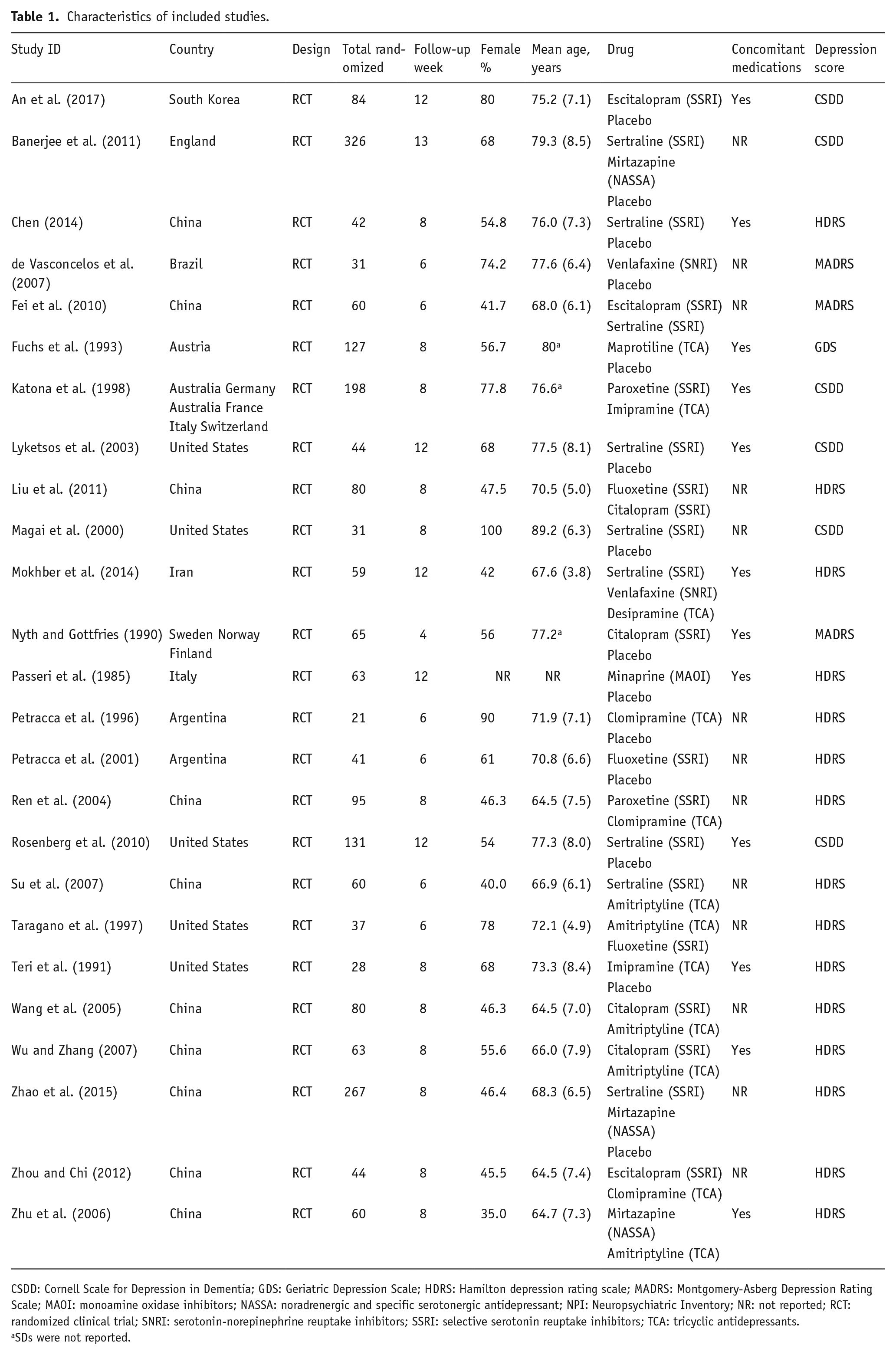
CSDD: Cornell Scale for Depression in Dementia; GDS: Geriatric Depression Scale; HDRS: Hamilton depression rating scale; MADRS: Montgomery-Asberg Depression Rating Scale; MAOI: monoamine oxidase inhibitors; NASSA: noradrenergic and specific serotonergic antidepressant; NPI: Neuropsychiatric Inventory; NR: not reported; RCT: randomized clinical trial; SNRI: serotonin-norepinephrine reuptake inhibitors; SSRI: selective serotonin reuptake inhibitors; TCA: tricyclic antidepressants.
SDs were not reported.
Sertraline was the most commonly prescribed SSRI antidepressants (N = 9 studies), other SSRIs included escitalopram, fluoxetine, paroxetine, and citalopram, which are selective in their inhibition of serotonin reuptake and have little effect on other neurotransmitters. TCAs included amitriptyline, clomipramine, desipramine, imipramine, and maprotiline, which are potent inhibitors of serotonin and norepinephrine reuptake. Venlafaxine is an SNRI, exerting its effects primarily by blocking the transporters involved in the reuptake of the neurotransmitters serotonin and norepinephrine. Mirtazapine is an antagonist of serotonin receptors and peripheral adrenergic receptors. Minaprine not only acts as a reversible inhibitor of MAO-A but also an antagonist of serotonin and dopamine receptors.
The characteristics of the included articles are presented in Table 1. In total, 2137 participants were randomly assigned to an active drug or placebo, 1581 treated with an antidepressant, 556 received placebo. The mean age was 73.1 years for both men and women; 1213 (58.5%) of the sample population were women.
Primary outcomes
The network of eligible comparisons for efficacy and safety is shown in Figure 2. All antidepressant drugs, except paroxetine and desipramine, had at least one placebo-controlled trial. Six of the placebo-controlled trials employed sertraline with a maximum dosage of 150 mg/d, two used mirtazapine with a maximum dosage of 45 mg/d.
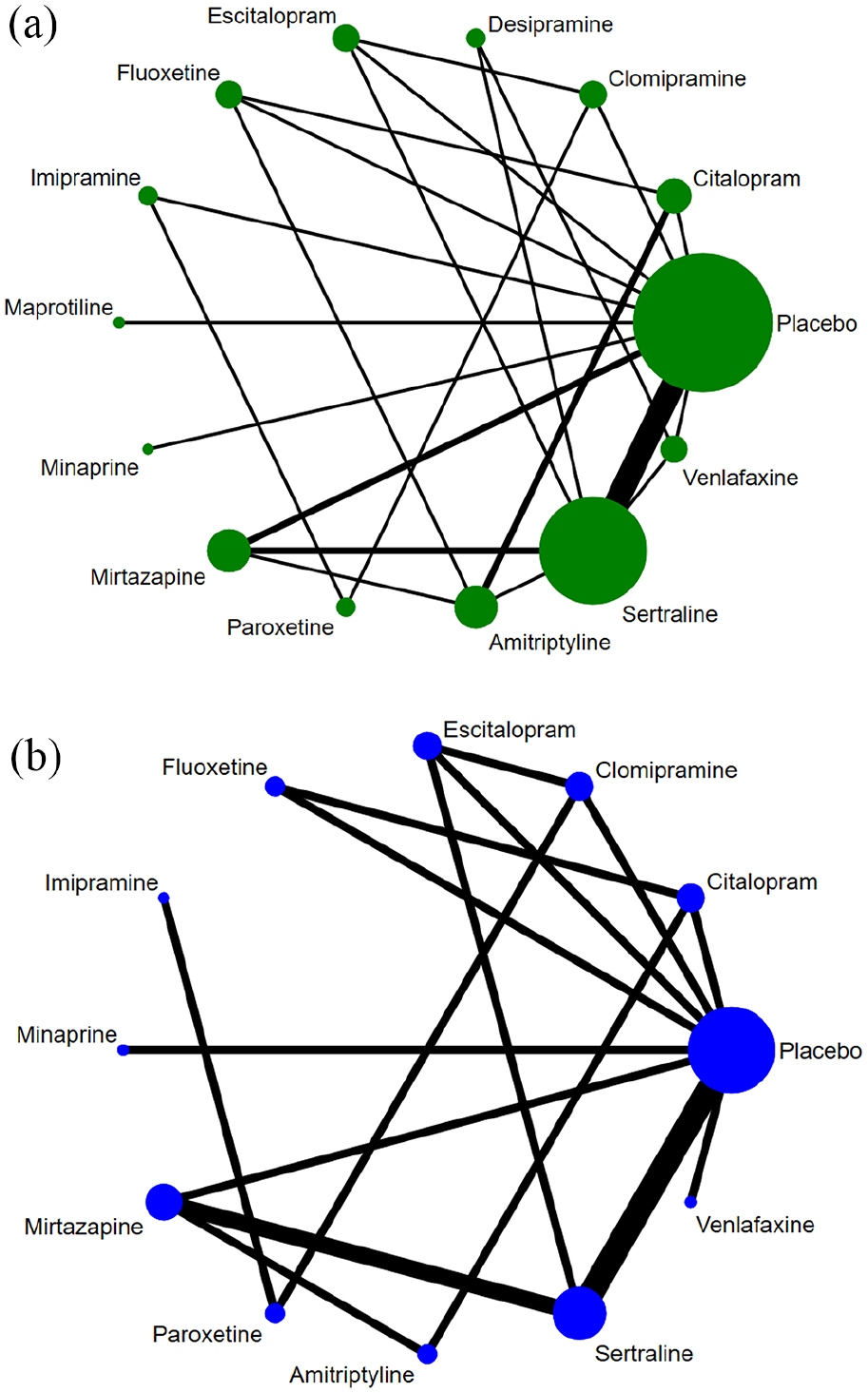
Network meta-analysis of included comparisons for efficacy (a) and safety (b). Size of every circle is proportional to the number of patients at that node. Width of the lines is proportional to the number of trials comparing every pair of treatments.
The network meta-analysis results for the primary outcomes are shown in Figure 3. Decreases in depression scores were considered indicative of efficacy. The HDRS and CSDD were the most frequently administered depression scales, utilized in 15 and six studies, respectively. At first glance one can conclude that mirtazapine (SMD, −1.94; 95% CI, −3.53 to −0.36; p < 0.05) and sertraline (SMD, −1.16; 95% CI, −2.17 to −0.15; p < 0.05) were more effective than placebo on the basis of these 25 trials.
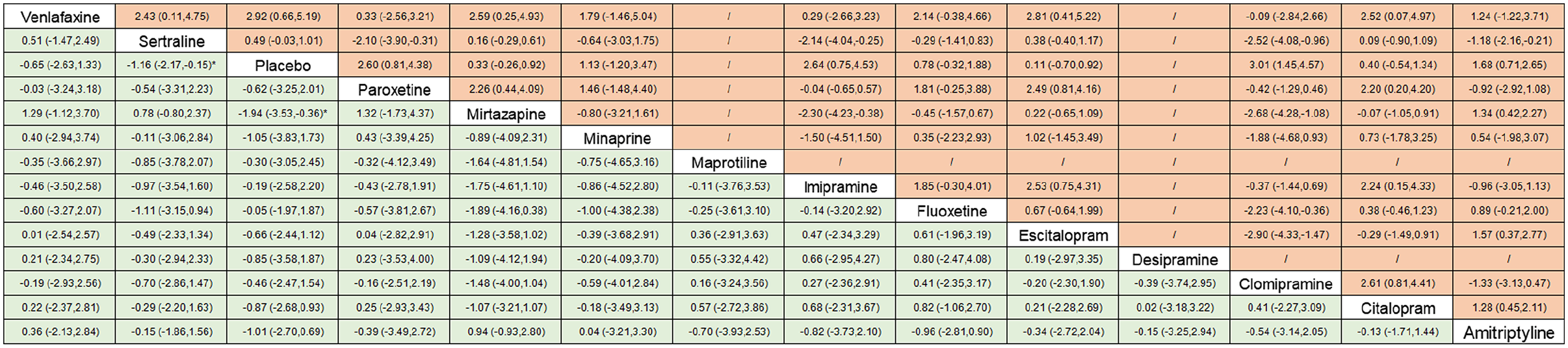
The comparisons for primary outcomes. Results on the comparative efficacy (green) and safety (orange) from network meta-analysis. Standardized mean differences less than 0 and ORs less than 1 favor the former drug in table. “/” indicates not applicable.
Discontinuation rates for adverse events were reported in 14 trials, while this outcome was not explicitly reported in the studies employed desipramine or maprotiline. In addition, an overview of the adverse events for the included studies, clomipramine increased risk of adverse events than placebo (OR, 3.01; 95% CI, 1.45 to 4.57; p < 0.05). The other antidepressants showed comparable safety with placebo (Figure 3 and Supplementary Figure S3).
Network meta-analysis summary plots have been shown in supplementary Figure S2 and Figure S3). On SUCRA analysis of efficacy, mirtazapine had the largest SUCRA score (84.5%) and ranked first (supplementary Figure S4). Clomipramine performed worst in safety (SUCRA score of 9.8 %, supplementary Figure S5).
Joint rankings of efficacy and safety
In addition, a clustered ranking plot based on SUCRA values was also generated to visually illustrate the primary outcomes as shown in Figure 4. Four distinct clusters of treatments were identified with respect to efficacy and safety. Citalopram, escitalopram, minaprine, mirtazapine, and sertraline formed one cluster, characterized by high efficacy and safety. Fluoxetine showed a comparable efficacy and incidence of adverse events (AE) with the placebo. Amitriptyline formed its group, characterized by high efficacy but moderate safety. Clomipramine, imipramine, paroxetine, and venlafaxine formed another cluster, characterized by moderate efficacy with poorer safety. Included articles did not present data on the incidence of any AE of desipramine or maprotiline.
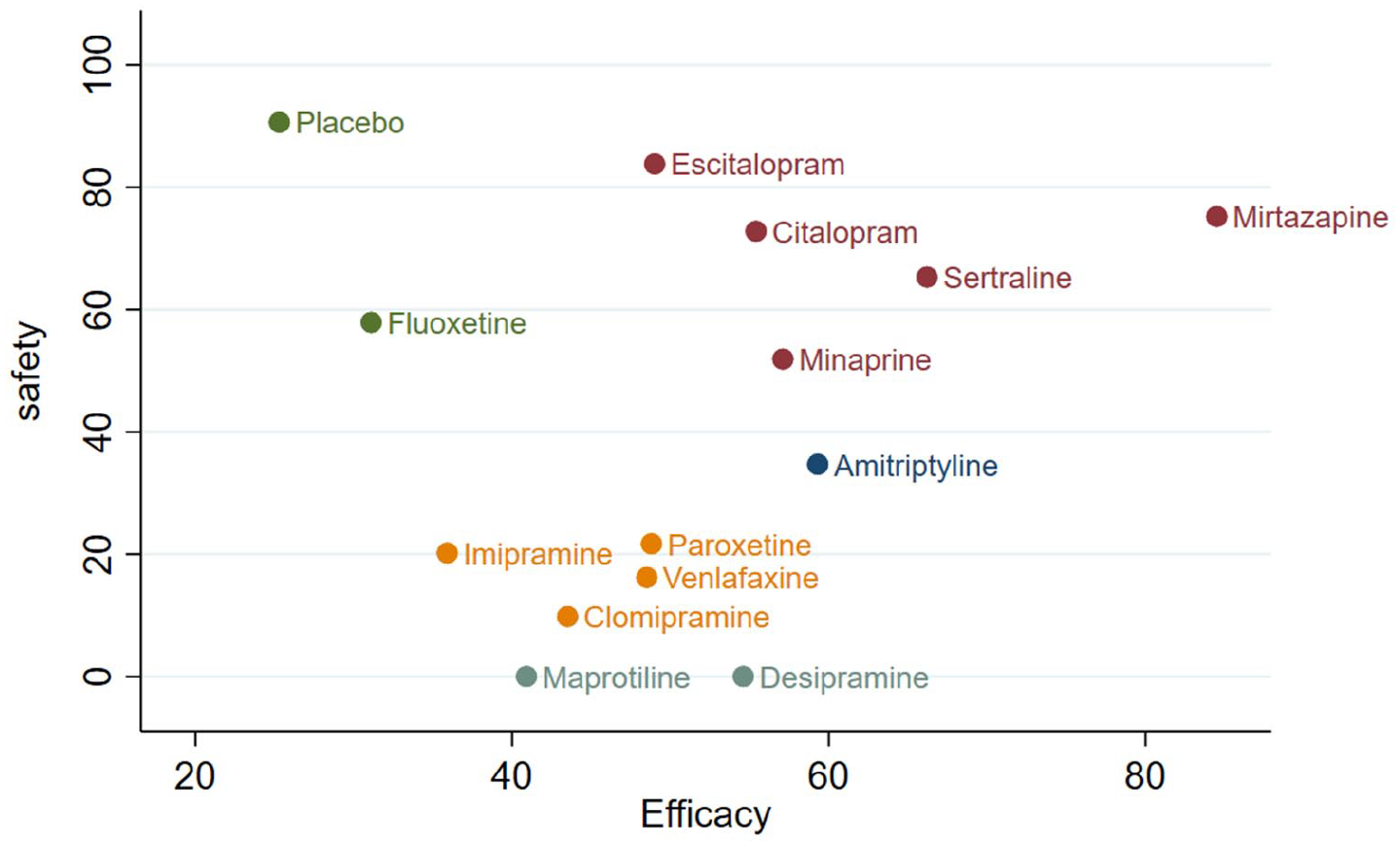
Clustered ranking plot based on cluster analysis of surface under the cumulative ranking curves (SUCRA) values of the efficacy and safety. Each color represents a group of treatments that belong to the same cluster. Treatments lying in the upper right corner are more effective and less adverse events than the other treatments.
Secondary outcomes
To investigate whether antidepressants had an impact on cognitive performance, we performed a network meta-analysis of MMSE scores (supplementary Figure S6 and Figure S7). Ten studies provided data for this outcome and showed no statistically significant difference between antidepressants and placebo (Supplementary Figure S8).
RoB and overall quality of the evidence
The RoB varied between individual studies, ranging from low to high (Supplementary Table S10). Although all studies were randomized trials, only six studies provided information on the method of sequence generation. A total of 17 of 25 studies did not outline their allocation concealment method. Blinding was judged to be adequate in 13 trails. A total of 19 of 25 studies had a low risk of reporting bias. 17 studies had stated the details of attrition bias. A funnel plot was used to assess the publication bias and there was no obvious asymmetry for all the outcomes (supplementary Figure S11, Figure S12, and Figure S13).
Network consistency analysis
Overall tests of consistency did not identify statistically significant inconsistency for mean change in depression scores [χ2(9) = 1.16, p = 0.999], or number of adverse events [χ2(6) = 3.68, p = 0.382] (supplementary Figure S1). Additionally, there was no overall statistically significant loop inconsistency for the outcomes of efficacy and safety (supplementary Figure S14). These generally suggested consistency between direct and indirect results.
Discussion
A total of 2137 subjects from 25 studies were included in the analysis, and the therapeutic efficacy of commonly used antidepressant drugs in the treatment of depression in AD patients was investigated. The effectiveness of antidepressants for depression in AD has been evaluated by systematic reviews. A review included data from five studies of 165 participants found antidepressant treatment is efficacious, with rates of discontinuation that are equivalent to placebo (Thompson et al., 2007). Likewise, another systematic review concluded that antidepressants were superior to placebo in terms of response or remission (Modrego, 2010). Nevertheless, Drs. Nelson and Devanand found there is a lack of efficacy in antidepressants for bringing about a greater reduction in depressive symptoms than placebo (Nelson and Devanand, 2011). Finally, the 2017 study (Orgeta et al., 2017) indicated that antidepressants appear to display relatively poor efficacy in people with AD. The reviews and meta-analyses taken together are inconclusive due to variable trial methods and different type of antidepressants tested. One important finding of our network meta-analysis is it can yield more precise estimates than a single direct or indirect estimate for comparing different classes of antidepressants across a network of studies. It also allows estimation of superiority of efficacy between classes of antidepressants and finds out the optimal treatment option.
The high efficacy in improving depression was observed in SSRIs in our study, which is consistent with many treatment guidelines. The 2019 practice guidelines issued by the Academy of Cognitive Disorder of China recommend SSRIs as the first pharmacological treatment for the management of behavioral and psychological symptoms of dementia in patients with AD (Cao et al., 2020). SSRIs tend to be a better option than other antidepressants because they are often associated with a reduced risk of an adverse event. It should also consider the effects on the liver Cytochrome P450 (CYP450) family when using SSRIs. Numerous genomic and pharmacogenetic factors have been proved to influence the metabolism of psychotropic drugs, which might subsequently affect the efficacy and side effects. Some studies confirmed that CYP2D6, 2C19, 2B6, and 2C9-mediated metabolism is responsible for the metabolism of sertraline and the metabolism mediated by these CYPs rescued the cytotoxicity of sertraline (Chen et al., 2020). It has been reported that the genetic polymorphisms in CYP2C19 may influence metabolism of the escitalopram and treatment response (Tsai et al., 2010). Genetic polymorphisms of ApoEε4 were associated with greater efficacy of antidepressants (Murphy et al., 2003). Aging and comorbidity-associated changes in pharmacokinetics and pharmacodynamics often result in therapeutic failure to psychoactive drugs of the elderly. As recommended in guidelines, sertraline, escitalopram, and citalopram had a better safety profile treating depression in AD (Yu et al., 2020).
As mentioned above, the selection of a particular antidepressant should take potential adverse effects into account. SSRIs target the serotonin receptor transporters, preventing serotonin reuptake from the synapse. Potential adverse effects of these agents are usually relatively mild, such as gastrointestinal reactions, nausea, vomiting, abdominal pain, diarrhea, headaches, anxiety, dry mouth, loss of appetite, and dizziness (Burke et al., 2019). Furthermore, SSRIs have less pronounced anticholinergic and antiadrenergic properties, and hence, less likely to cause confusion or falling.
It has also been well reported that treatment with SSRIs in combination with acetylcholinesterase inhibitors has protective effects on cognition in AD patients (Lavretsky et al., 2020; Rozzini et al., 2010). A longitudinal study including 755 nondepressed participants has confirmed that long-term SSRI treatment may delay progression from mild cognitive impairment (MCI) to Alzheimer’s dementia (Bartels et al., 2018). However, this study found that treatment with these agents did not have any significant effect on AD patients in terms of improvement or deterioration of any of the cognitive outcomes. Our results are in accordance with the previous study (Jones et al., 2016). Notably, a large registry study found administrating antidepressants during prodromal stages is associated with a reduced mortality rate, specifically in patients with AD (Enache et al., 2016).
The evidence regarding the efficacy of SSRIs, however, remains conflicting. Two of SSRIs, fluoxetine, and paroxetine apparently were not superior to placebo in this study. It is possible that variations in the quality of the evidence may have influenced the results. Only one study used a randomized, placebo-controlled design (Petracca et al., 2001), whereas others compared fluoxetine or paroxetine to another antidepressants (Katona et al., 1998; Liu et al., 2011; Ren et al., 2004; Taragano et al., 1997). The very influential Banerjee study showed there’s no statistically significant difference between mirtazapine or sertraline versus placebo group in treating depression in AD, which, however, is not seemingly consistent with our results in this meta-analysis. Limitations of methodological bias in these studies bring out diverse outcomes. Conducting a systematic review and meta-analysis to integrate the current studies’ results will allow us to draw a robust conclusion on the effects in which the interventions work.
There are a number of earlier and generally smaller trials included in the analysis, which investigated TCAs and MOIs. They revealed that minaprine was more effective than placebo and adverse events are most frequently found in clomipramine groups. However, this class of antidepressants now is rarely used because of side effects. They are associated with potentially problematic adverse effects in elderly patients. Especially their anticholinergic properties are relevant to negative effects on cognition.
There is an international consensus that psychiatry services are identified as first-line interventions prior to any pharmacological treatment for depressed patients with AD (Kales et al., 2019). However, due to insufficient resources, antidepressants are used more frequently than psychological interventions (Kitching, 2015). These findings do not imply that people with severe depression and AD should not be treated with antidepressants. We may need to predict individual response to treatment and provide personalized optimal dosage strategies. Given that this study is limited by a paucity of trials, small studies overall, and variation in patients recruited, further RCTs are needed in order to confirm the effects of antidepressants in AD.
Most of the attention has appropriately, been focused on evaluating the most frequently prescribed drugs. More recently, a new multimodal antidepressant, namely vortioxetine, appeared to be promising. Vortioxetine is a new “multimodal” antidepressant with a complex and not entirely known mechanism of action. One RCT provides evidence that vortioxetine had a beneficial effect on cognition and mood in older individuals with AD and was safe and well-tolerated (Cumbo et al., 2019). Perhaps we can identify new approaches in the therapy of AD-associated depression.
Limitation
There is no gold standard outcome measure for depression in AD. In this meta-analysis, continuous score of the scale was adopted as an outcome measure, the majority of studies used the HDRS, which has not been validated for use in patients with AD, while the remaining studies used the CSDD and fewer MADRS discontinuation studies were conducted. Due to a lack of head-to-head trials, the majority of our comparisons relied on results from network meta-analyses to estimate the comparative efficacy of the interventions of interest for the treatment of AD patients with depression. Network meta-analyses are an important analytic tool in the absence of direct head-to-head evidence, but they also have limitations. The number of patients included in the eligible studies could not have been large enough to detect significant statistical differences in the efficacy between the intervention and control groups.
Despite these limitations, we believe that our study can help clinicians and patients make more evidence-based and impartial decisions when selecting an optimal treatment strategy for depression in AD.
Conclusion
Overall, in the short-term treatment, our results suggest that sertraline and mirtazapine should be an alternative treatment for depression in AD patients. However, the available evidence does not indicate greater benefits or less harm for other commonly used antidepressants compared with placebo. We believe that the results of this study may assist in clinical decision-making and future practice. More high-quality trials with large samples and longer following-up are proposed.
Supplemental Material
sj-docx-1-jop-10.1177_02698811211030181 – Supplemental material for Efficacy of antidepressant drugs in the treatment of depression in Alzheimer disease patients: A systematic review and network meta-analysis
Supplemental material, sj-docx-1-jop-10.1177_02698811211030181 for Efficacy of antidepressant drugs in the treatment of depression in Alzheimer disease patients: A systematic review and network meta-analysis by Yanhong He, Hao Li, Jinbo Huang, Sumei Huang, Yunpeng Bai, Yingbang Li and Wendong Huang in Journal of Psychopharmacology
Footnotes
Author contributions
Yanhong He, Hao Li, and Wendong Huang were responsible for the initial plan, study design, conducting the study, and data interpretation. Yanhong He, Jinbo Huang, and Wendong Huang were responsible for data collection, data extraction, statistical analysis, and manuscript drafting. Sumei Huang, Yunpeng Bai, Yingbang Li and Wendong Huang were responsible for analysis and interpretation of the data and critically revised the paper. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by High-level Hospital Construction Research Project of Maoming People’s Hospital (zx2020027), and the Medical Research Fund of Guangdong Province (A2020196, B2018061, A2017490).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.