
Abstract
Background:
Classical psychedelics are a group of drugs which act as agonists on the serotonin-2A (5-HT2A) receptor. Evidence suggests they may have a uniquely rapid and enduring positive effect on mood. However, marked heterogeneity between methodological designs in this emerging field remains a significant concern.
Aims:
To determine how differences in the type of psychedelic agent used and the number of dosing sessions administered affect subjects’ depression and anxiety outcomes and adverse drug reactions (ADR).
Methods:
This review collected and screened 1591 records from the MEDLINE and Web of Science databases for clinical trials reporting objective data on mood for subjects with a known anxiety or depression.
Results:
After screening, nine clinical trials met inclusion criteria. Meta-analysis of these studies showed significant, large positive effect sizes for measures of anxiety (Cohen’s d = 1.26) and depression (Cohen’s d = 1.38) overall. These positive effects were also significant at acute (⩽1 week) and extended (>1 week) time points. No significant differences were observed between trials using different psychedelic agents (psilocybin, ayahuasca or lysergic acid diethylamide (LSD)), however, a significant difference was observed in favour of trials with multiple dosing sessions. No serious ADR were reported.
Conclusion:
Psilocybin, ayahuasca and LSD all appear to be effective and relatively safe agents capable of producing rapid and sustained improvements in anxiety and depression. Moreover, the findings of the present analysis suggest that they may show a greater efficacy when given to patients over multiple sessions as compared to the more common single session used in many of the existing trials.
Keywords
Introduction
Classical psychedelics are a class of drugs that have garnered substantial recent attention for their potential applications in a different mental health conditions from anxiety and depression (Barrett et al., 2020; Griffiths et al., 2016; Grob et al., 2011; Luoma et al., 2020) to substance use (Bogenschutz et al., 2015; DiVito and Leger, 2020; Garcia-Romeu et al., 2019; Johnson et al., 2014; Krebs and Johansen, 2012; Noorani et al., 2018). Many of these psychedelics—such as ayahuasca, psilocybin and peyote—have been used in ritual practices for thousands of years (Aixalà et al., 2018; Daniel and Haberman, 2017; Garcia-Romeu and Richards, 2018) and are still used today by some spiritual and religious groups (Garcia-Romeu and Richards, 2018). However, modern Western interest in psychedelics largely arose as a result of Swiss chemist Albert Hofmann’s discovery of lysergic acid diethylamide (LSD) in 1943 (Hofmann and Ott, 1980). Initial research showed potential for LSD as a possible therapy for depression, anxiety and alcohol use; however, cultural forces shortly thereafter lead to an association between psychedelics and anti-Vietnam war counter-culture in the United States (Nutt and Carhart-Harris, 2021). Subsequently, research into the potential applications of psychedelics in the domain of clinical psychiatry was largely halted following the reclassification of psychedelics as schedule I controlled substances in 1970 within the United States (Bonson, 2018; Controlled Substances Act, 1970) and internationally in a subsequent resolution adopted by the United Nations (UN General Assembly, 1971). The initial research preformed in the 20th century investigating psychedelics largely does not conform to modern standards of academic rigour—lacking proper controls, blinding, follow-up or validated measures of assessment (Garcia-Romeu and Richards, 2018). These earlier studies did inspire more recent investigations, which over the past two decades have reignited interest (Bogenschutz et al., 2015; Griffiths et al., 2011, 2016; Grob et al., 2011). One of the most promising new avenues in which psychedelics may play a future role is in the treatment of depression and anxiety.
Depression and anxiety constitute a tremendous and serious burden on patients throughout the world. Globally, depressive disorders constitute one of the three leading causes of years lived with disability worldwide (James et al., 2018). In 2017, the global prevalence of depressive and anxiety disorders was found to be over 260,000,000 and 280,000,000, respectively (James et al., 2018). Overall, the projected cost of mental health disorders is over $8.5 trillion and expected to double by 2030 (Trautmann et al., 2016). In the United States alone the cost of depressive and anxiety disorders in 2013 totalled at $71,100,000,000 and $29,700,000,000 each (Dieleman et al., 2016). Furthermore, the personal impact of mood disorders on patients is substantial, with some estimates reporting the risk of dying from a depressive disorder being as high as 15 per 1000 in the general population (Trautmann et al., 2016). As per the Centers for Disease Control and Prevention (CDC, 2020) report, the number of deaths attributable to suicide in 2018 was 48,344 in the United States alone—the 10th leading cause of death in the country. Thus, the need for meaningful improvement in the current treatments for anxiety and depression is clear.
Current standard therapies for depression and anxiety—antidepressants and psychotherapy—are generally found to have small-moderate effect sizes, with neither considered superior to the other (Kamenov et al., 2017). Of the standardly used medications in the treatment of major depressive disorder (MDD) and anxiety, most share a common primary pharmacological target, the monoamine transporters (Richelson, 2001; Stahl, 2013). They function as reuptake inhibitors, thus elevating synaptic levels of monoamines (i.e. serotonin, norepinephrine and dopamine) or, in the case of older antidepressants, by inhibiting monoamine breakdown via the enzyme monoamine oxidase (Richelson, 2001; Stahl, 2013). Despite their well-characterized primary target, the mechanism by which conventional monoaminergic drugs relieve depression and anxiety symptomology remains debated. Their therapeutic effects have been attributed to direct or indirect actions on other non-monoamine targets including glutamate transmission, mTOR signalling, mitochondrial function, neurotrophic factors (e.g. BDNF) and neurogenesis, to name a few (Deyama and Duman, 2019; Duman, 2004; Karabatsiakis and Schönfeldt-Lecuona, 2020; Olescowicz et al., 2020; Witkin et al., 2020). Likewise, the mechanism of action of classical psychedelics are complex and poorly understood. It is established that these drugs function as serotonin-2A (5-hydroxytryptamine-2A, 5-HT2A) receptor agonists (Garcia-Romeu and Richards, 2018), and activation of 5-HT2A receptors in cortical areas result in elevated glutamate release and activation of AMPA glutamate receptors (Dos Santos and Hallak, 2020; Dos Santos et al., 2018; Martin and Nichols, 2018; Sampedro et al., 2017). They also have direct or indirect interactions with dopamine transmission (Nichols et al., 2017; Vollenweider et al., 1999; Watts et al., 1995). These drugs display some activity at other serotonergic receptors, 5-HT2C in particular (Canal and Murnane, 2017), as well as the dopamine D1 and D2 receptors in the case of LSD (Nichols et al., 2017). Further, the classic psychedelics can promote neuroplasticity through increasing neurotrophins including BDNF, regulating mTOR signalling and enhancing neurogenesis (de Almeida et al., 2019; Dos Santos and Hallak, 2020; Ly et al., 2018). Thus, while their primary molecular targets differ, monoaminergic antidepressants and psychedelics may share common downstream effectors that may contribute to their antidepressant and anxiolytic actions.
The temporal effects of these drugs appears to also be distinct from those of traditional antidepressants, as past meta-analyses have found positive results on patients’ mood in as little as 1 day after psychedelic administration and persisting for up to 6 months (Romeo et al., 2020). This is a striking difference from current and conventional treatments, which can require weeks to months to become effective (Machado-Vieira et al., 2010). Interest surrounding the potential for psychedelics is likely to only increase in the near future, as the US Food and Drug Administration recently designated psilocybin as a breakthrough therapy for the management of treatment-resistant depression (TRD) and MDD with ongoing phase II clinical trials at this time by COMPASS Pathways and Usona, respectively (ClinicalTrials.gov, 2021a, 2021b). This status will facilitate research into psilocybin, potentially paving the way for the near future applications in mental health conditions (Yaden et al., 2020). However, before this can happen, the need for a deeper understanding of how methodological variables affect treatment outcomes is required in order to optimize further use of these compounds for the treatment of depression and anxiety (Yaden et al., 2020). Most recent studies typically provide the drug in a warm and naturalistic-like setting with music (Kaelen et al., 2018; Nutt and Carhart-Harris, 2021). They usually consist of preparatory sessions, where patients are educated about the trial usually by one or often two facilitators (Nutt and Carhart-Harris, 2021). A post-drug integration session and often a limited number of psychotherapy sessions are also common (Nutt and Carhart-Harris, 2021). Although the outline of a ‘standard approach’ to psychedelic-assisted psychotherapy is beginning to take shape, there still remain many factors which are largely inconsistent between trials.
Amidst the enthusiasm in this burgeoning field, there remains many outstanding differences between investigations with studies using different psychedelic agents and various numbers of doses being administered to subjects. There is marked heterogeneity between research methods employed by different investigators looking at the use of psychedelic as therapeutic adjuncts with little clear understanding of how these factors contribute to potential differences in patient outcomes. This concern is especially important as more large-scale investigations are intended for the near future. The aim of this systematic review and meta-analysis is to determine the impact of methodological differences on the effects of psychedelic-assisted therapy for anxiety and depressive disorders. Specifically, differences in the selected psychedelic agent (psilocybin, LSD or ayahuasca), the number of doses administered to subjects and the outcomes at different time points. To our knowledge this is the first meta-analysis to compare the effects of these methodological differences in the context of anxiety and depression at multiple time points for classical psychedelics.
Materials and methods
A systematic review of relevant literature was performed in accordance with the guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement (Moher et al., 2009). An a priori protocol for this meta-analysis and systematic review was registered with the PROSPERO international prospective register of systematic reviews (Registration ID: CRD42020216782).
A search of the electronic databases MEDLINE and Web of Science was conducted employing the following search terms and Boolean variables: (psychedelic* OR hallucinogen* OR LSD OR lysergic acid diethylamide* OR psilocybin) AND (depress* OR anxiety OR posttraumatic* OR mood). Search parameters were restricted to include only studies published in English and consisting of human subjects. Reference lists from screened articles were assessed for additional potential studies meriting inclusion, which did not appear during initial electronic searches within the aforementioned databases. Initial database searches between these two sources were performed on 5 Oct 2020; however, additional records were found using an automated alert system for new records meeting criteria for saved searches in the Web of Science database, which were returned after the initial search was performed, with instances of studies questionably meriting inclusion being independently assessed by both authors. In all cases, authors independently reached agreeing determinations regarding inclusion of these questionable studies.
The investigated population was to be samples of human subjects with confirmed depressive and anxiety disorders at baseline, exposed to a classical psychedelic and for whom data on outcomes and methodology were reported and amenable to effect size determination. Only studies in which participants received doses large enough to yield psychoactive responses (i.e. those capable of producing alterations in perception) were included in this analysis, as it has been suggested that this is required to precipitate the drugs’ therapeutic effects (Yaden and Griffiths, 2021), though notably there has been some controversy regarding this necessity (Olson, 2021). Investigations without baseline or control comparators or objective measurement scales were excluded. Additionally, as the objective of this review and meta-analysis is to improve the understanding of the effects of methodological differences on outcomes, study designs that failed to employ consistent methodology between subjects within the investigation were also excluded. As such, observational studies and case series were not included in this analysis. Clinical trials—open-label, single-blinded, double-blinded and placebo-controlled investigations of human subjects—were all considered. Of the full text articles assessed for eligibility, those that reported data from samples of subjects published elsewhere were only reported using the publication providing the most detailed description of methodology and outcomes.
In cases in which outcome data were not directly reported in otherwise inclusion-worthy studies, corresponding authors for the given studies were contacted for the purposes of obtaining additional information. Failing this, relevant data were extracted graphically from published figures using ImageJ (Version 1.53) (Schneider et al., 2012). A schematic representation of the selection and exclusion process is presented in Figure 1.
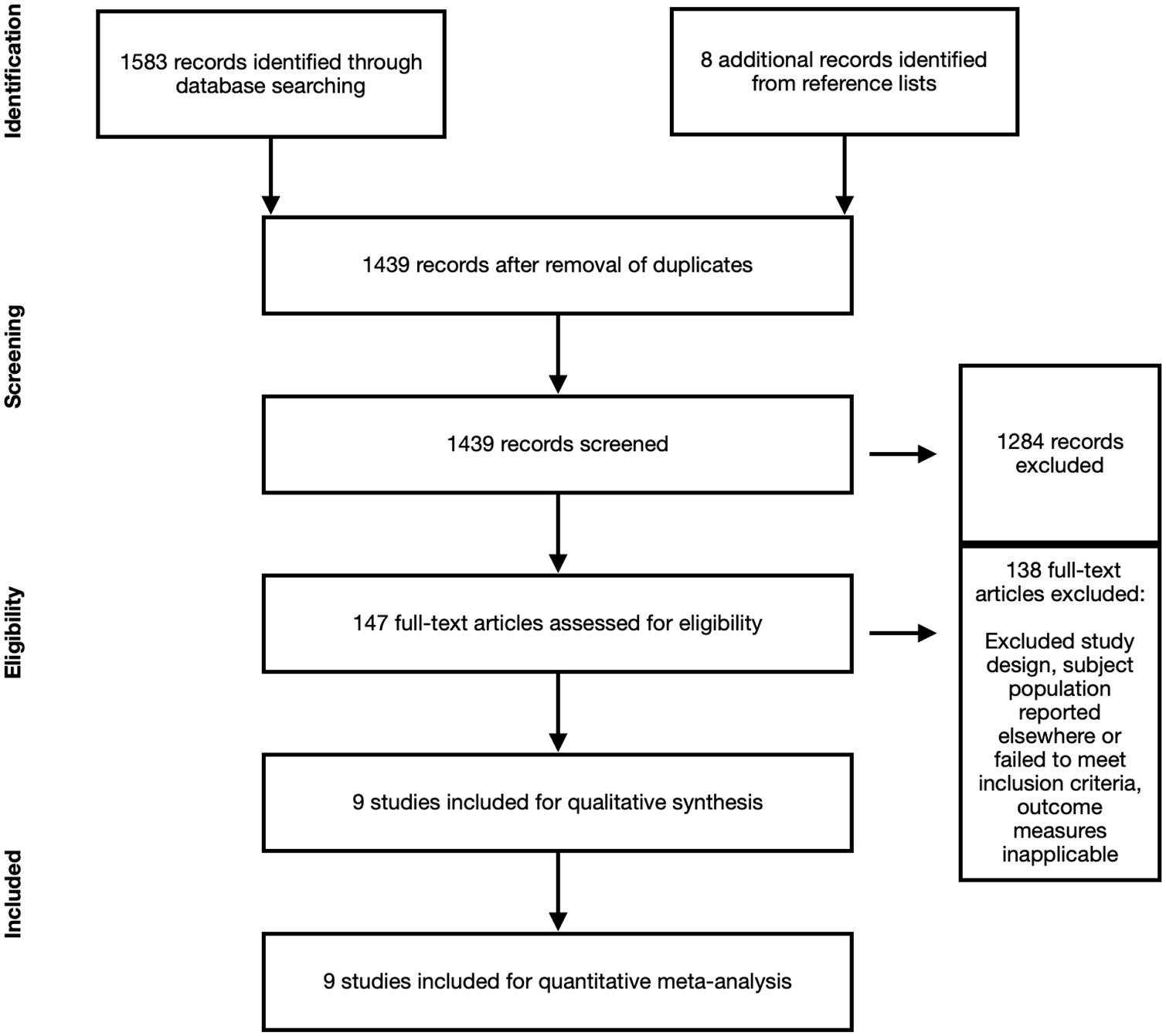
Study selection process flow diagram.
Data were extracted from included studies assessing: (1) a primary outcome of improvement in mood and (2) a secondary outcome of risk of adverse drug reactions (ADRs). The Cohen’s d measure of standardized mean difference was used as an estimate of effect size. Measures of effect size for anxiety and depressive outcomes were averaged for different comparisons within trials when provided or calculated from given means and standard deviations, with values for each trial’s sampling variance being calculated in line with prior guidelines for meta-analysis of this nature assessing studies comparing both independent groups and repeated measures (Morris and DeShon, 2002). When available, separate effect sizes for immediate changes in mood and effect sizes measured at extended time points were calculated separately in order to assess differences between acute and prolonged alterations in mood. Time points occurring ⩽1 week following psychedelic administration were pooled together and considered to constitute an early improvement of symptoms in line with prior reviews (Machado-Vieira et al., 2010). Subgroup analysis was performed to assess for differences between primary and secondary outcome measures based on psychedelic agents used and the dosage(s). Statistical analysis for the primary meta-analysis was performed with a random-effects model using the Metafor (Viechtbauer, 2010) meta-analysis package for R statistical software (R Core Team, 2020), with a mixed-effects model used for secondary subgroup analysis. Random-effects model was chosen due to the significant methodological variability between studies, with mixed-effects model used for subgroup analysis. I2 values were employed to assess between trial heterogeneity, using Higgins et al.’s (2003) value cut-offs of 25%, 50% and 75% as representing low, moderate and high quantities of heterogeneity, respectively.
An assessment of the risk of bias in the assessed studies was made using the Cochrane risk of bias (RoB) tool for randomized controlled trials and the Risk Of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool for non-randomized clinical trials. The six domains of bias assessed were random sequence generation, allocation concealment, blinding, incomplete outcome data and selective outcome reporting. Calculation of a fail-safe-N value was performed to assess for potential publication bias amongst the selected studies (Orwin, 1983).
Results
Search methods yielded a total of 1591 total records prior to manual screening by investigators. One hundred and fifty-two of these records were removed after they had been determined to be duplicates, leaving a remainder of 1439 records. Titles and abstracts of these records were assessed for relevance, with the full texts of 147 records being evaluated for inclusion into the final analysis. Of these 147 articles, nine were ultimately considered to meet full criteria.
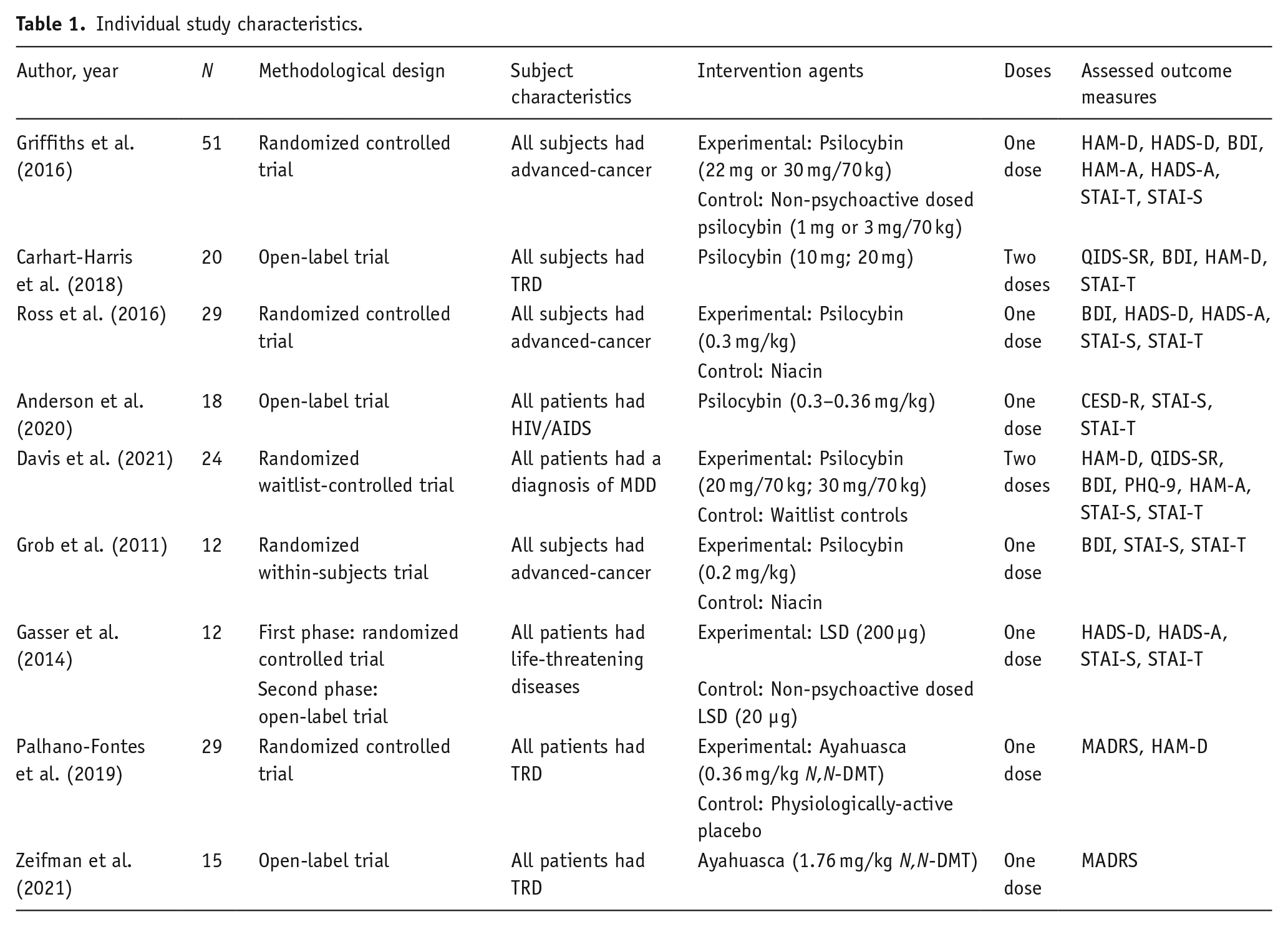
Amongst the studies selected, psilocybin was by far the most commonly investigated psychedelic agent, with six trials using this compound (Anderson et al., 2020; Carhart-Harris et al., 2018; Davis et al., 2021; Griffiths et al., 2016; Grob et al., 2011; Ross et al., 2016). Of the remaining studies, two used ayahuasca (Palhano-Fontes et al., 2019; Zeifman et al., 2021) and one used LSD (Gasser et al., 2014). All trials used psychoactive doses of psychedelics. For trials using ayahuasca which is comprised of both a classical psychedelic N,N-dimethyltryptamine (N,N-DMT) and multiple reversible monoamine oxidase inhibitors (MAOi): harmine, harmaline and tetrahydroharmine, concentrations of these constituents were determined using mass spectroscopy (Palhano-Fontes et al., 2019; Zeifman et al., 2021). The combined number of experimental subjects from these trials was 201. Between subgroups, 154 subjects received psilocybin, 35 were given ayahuasca, and 12 took LSD. Three of the studies used an open-label design; three were randomized controlled trials; one study consisted of a first phase that was a randomized controlled trial with a second phase that was open-label. Grob et al. (2011) used a within-subjects design in which subjects received either psilocybin or a physiological placebo (i.e. niacin) in two separate trial arms, with a randomized order. In five of the nine studies, subjects had co-morbid severe medical conditions. For three of these samples, the diagnosis was advanced-cancer (Griffiths et al., 2016; Grob et al., 2011; Ross et al., 2016) and one was long-standing HIV/AIDS (Anderson et al., 2020). In Gasser et al. (2014), patients had life-threatening diseases ranging from cancer (75%) to Parkinson Disease (12.5%) or Bechterew Disease (12.5%). The objective mood scales used by different studies were highly varied and are shown in Table 1.
Individual study characteristics.
Within study assessments of bias were made for the primary mood outcome data. A detailed breakdown of the sources of bias across the different domains of bias within trials are shown for the randomized clinical trials or trials with a randomized phase (Gasser et al., 2014), in Supplemental Table 1, with non-randomized trials displayed in Supplemental Table 2. As a whole, the risk for bias for all trials included in this meta-analysis was high, largely due to issues surrounding failure to blind patients successfully as to whether they are receiving a psychedelic versus a placebo (Gasser et al., 2014; Griffiths et al., 2016; Ross et al., 2016) or failed to assess blinding success in investigators (Palhano-Fontes et al., 2019). Other trials introduced bias in the selection of the reported result domain via inclusion of multiple scales measuring the same outcome in most included trials (Carhart-Harris et al., 2018; Davis et al., 2021; Gasser et al., 2014; Griffiths et al., 2016; Grob et al., 2011; Palhano-Fontes et al., 2019; Ross et al., 2016), however, the impact of this bias would likely be small, as results from all scales for most of these trials attained statistical significance; the anxiety outcome results measured using the Hospital Anxiety and Depression Scale-Anxiety (HADS-A) did not attain statistical significance for any time point in Griffiths et al. (2016). Of note, although many of these outcome measures were clinician rated, others such as the Beck Depression Inventory (BDI), Quick Inventory of Depressive Symptomatology (QIDS), State Trait Anxiety Inventory (STAI) and HADS are based on subjects’ self-report, and therefore introduce additional bias. These results are similar to bias assessments made in past systematic reviews investigating trials with psychedelics (Fuentes et al., 2019; Goldberg et al., 2020) and may represent an inherent systemic difficulty in conducting research with psychedelic compounds. Furthermore, like most systematic reviews, the present analysis is subject to selection bias, largely associated with a publication bias in favour of studies with significant results. This was addressed by use of fail-safe N in the present analysis.
Meta-analysis of trials reporting outcome data for dedicated measures of depression (k = 9) using a random-effects model yielded a large, estimated effect size of 1.38 (CI: 0.93–1.82) that was highly significant (p < 0.0001). Moderate variability was present between trials (I2 = 68.53%). The potential for publication bias effecting this result was extremely unlikely; using fail-safe-N (file drawer analysis) it was determined that 374 unpublished studies of null results would have to be present in order for the true effect size not to be significant. Similarly, in line with prior investigations, acute effects of psychedelics were also significant for periods ⩽1 week, with an estimated effect size of 1.68 (CI: 0.98–2.39; k = 6; p < 0.0001) and high heterogeneity (I2 = 80.99%). The effect of psychedelics on depression remained highly significant and large at extended time points beyond 1 week, 1.30 (CI: 0.82–1.79; k = 8; p < 0.0001) with high between trial variability (I2 = 71.34%). Subgroup analysis using psychedelic agent as a moderator did not yield significant differences between groups at any time points. Overall, the estimate for ayahuasca’s effect (1.82, CI: 0.81–2.83) did not significantly vary from that of psilocybin (1.34, CI: 0.18–2.49; p = 0.41) or LSD (0.80, CI: −0.9799–2.58; p = 0.26), nor did psilocybin and LSD differ from one another (p = 0.53). Heterogeneity was high (I2 = 81.25%). Forest plots of meta-analyses with subgroups ordered by type of psychedelic agent administered are shown below in Figure 2. However, comparison between subgroups using the number of doses instead as a moderator did produce significant results using a mixed-effects model. The effect of two psychoactive doses of psychedelics produced an effect size that was 1.31 (CI: 0.41–2.21) larger than that of a single dose (p = 0.0043). Moderate variability was present between trials (I2 = 37.29%). Forest plots of meta-analyses with subgroups ordered by the number of doses administered within trials are shown below in Figure 3.
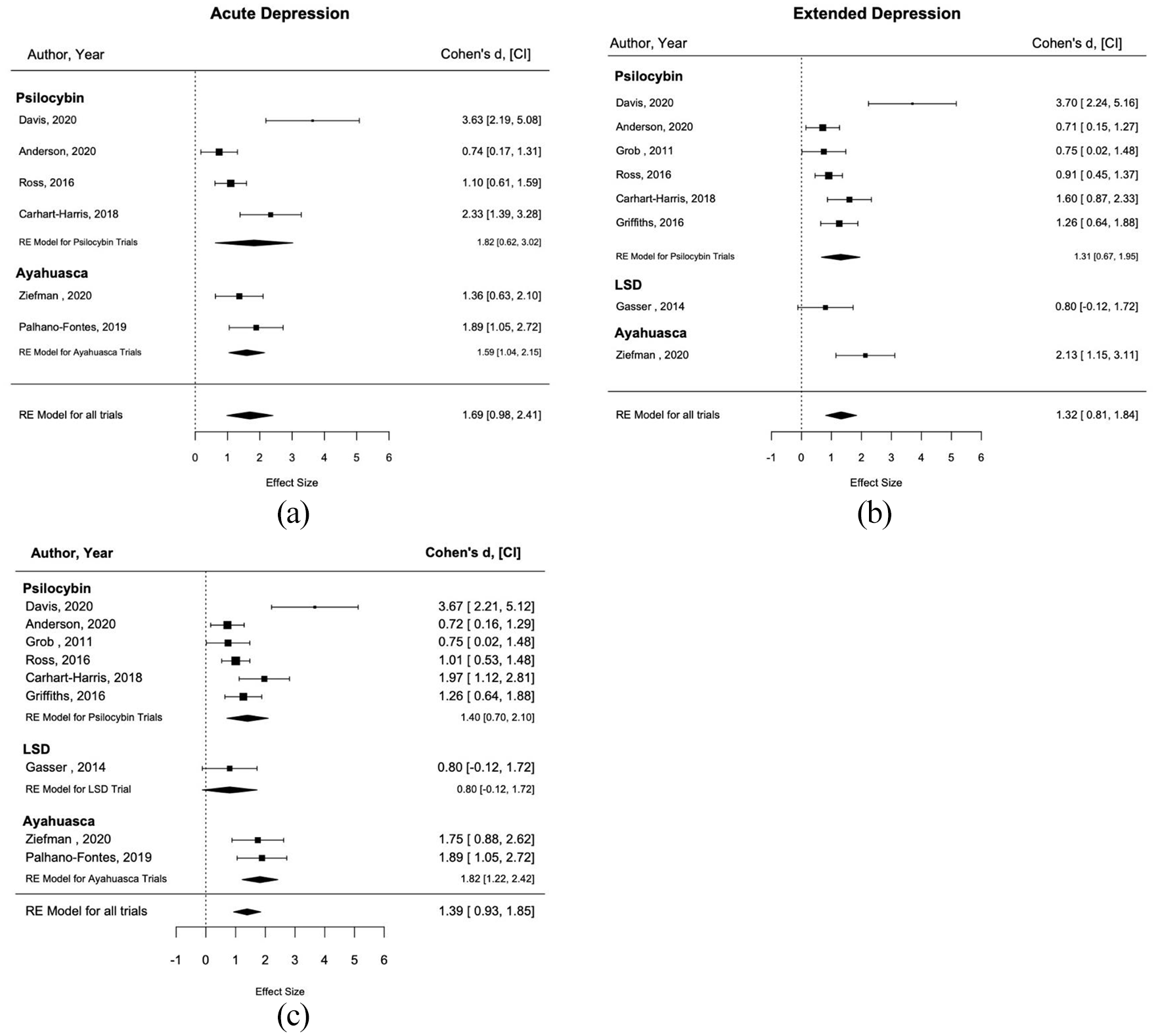
Forrest plots of depression with choice of psychedelic agent as a moderator: (a) shows effect sizes for studies reporting data for depression outcomes at ⩽1 week post administration (k = 6) and a random-effects model for the estimate of effect size, (b) shows effect sizes for studies reporting data for depression outcomes at >1 week post administration (k = 8) along with a random-effects model for the estimate of effect size and (c) displays the overall outcomes averaged over all reported time points for studies reporting measures of depression (k = 9) and a random-effects estimate of the effect size.
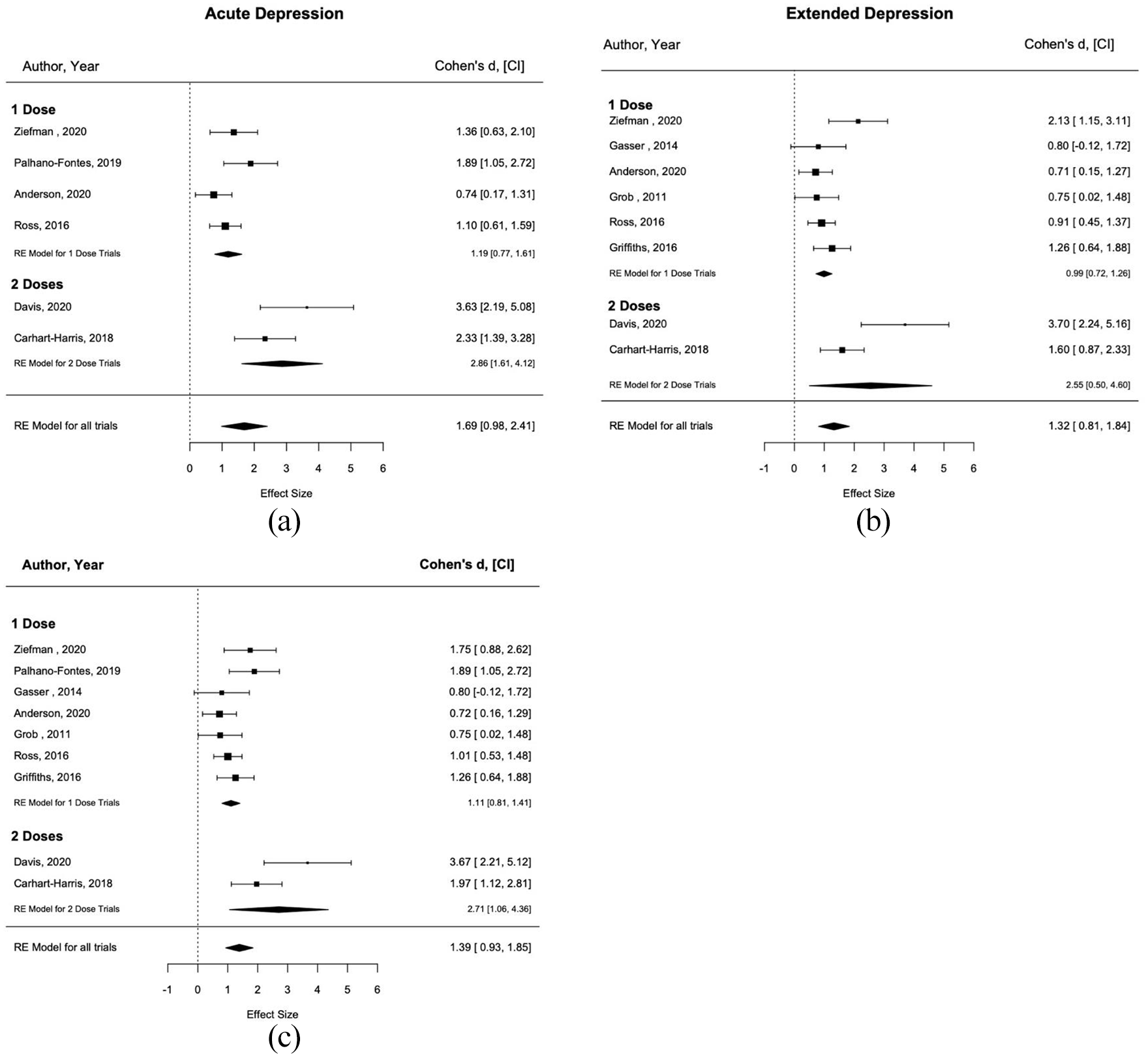
Forrest plots of depression with number of administered doses as a moderator: (a) shows effect sizes for studies reporting data for depression outcomes at ⩽1 week post administration (k = 6) and a random-effects model for the estimate of effect size, (b) shows effect sizes for studies reporting data for depression outcomes at >1 week post administration (k = 8) along with a random-effects model for the estimate of effect size and (c) displays the overall outcomes averaged over all reported time points for studies reporting measures of depression (k = 9) and a random-effects estimate of the effect size.
Similar to the observed results for depression outcomes, anxiety was also significantly attenuated by psychedelics in reporting studies (k=7), with an estimated large effect size of 1.26 (CI: 0.75–1.78; p < 0.0001). Moderate variability was present between trials (I2 = 70.69%). Using fail-safe-N it was determined that 189 unpublished studies with null results would be necessary for the true effect size not to be significant. Estimates of acute effects on anxiety—those observed at ⩽1 week—were also large and significant at 1.28 (CI: 0.40–2.17; p = 0.0044), however, meta-analysis for the acute setting was limited, as only three studies in this analysis reported data for anxiety measures taken at ⩽1 week from psychedelic administration. The effects of psychedelics at extended time points on anxiety remained large at 1.17 (CI: 0.65–1.69; k = 7; p < 0.0001). A subgroup analysis of trials using the type of psychedelic agent administered as a moderator using a mixed-effects model showed no significant difference between the effect size for trials with LSD, 1.72 (CI: −0.19–3.64), and that for psilocybin, 1.23 (CI: −2.49–1.50; k = 7; p = 0.6275). Between study variance was high (I2 = 75.40%). Forest plots of meta-analyses with subgroups divided by type of psychedelic agent administered are shown below in Figure 4. As such, meta-analysis on secondary outcomes of ADRs was not preformed. However, much like in the depression outcomes, a significant effect was observed between subgroups when comparing the number of doses as a moderator. Trials in which subjects received two psychoactive doses of psychedelics had an estimated effect size that was 1.09 (CI: 0.13–2.06) greater than that of trials with a single dose administered (p = 0.0256). Heterogeneity was moderate (I2 = 52.38%). Forest plots of meta-analyses with subgroups divided by the number of doses administered are shown below in Figure 5 for anxiety outcomes.
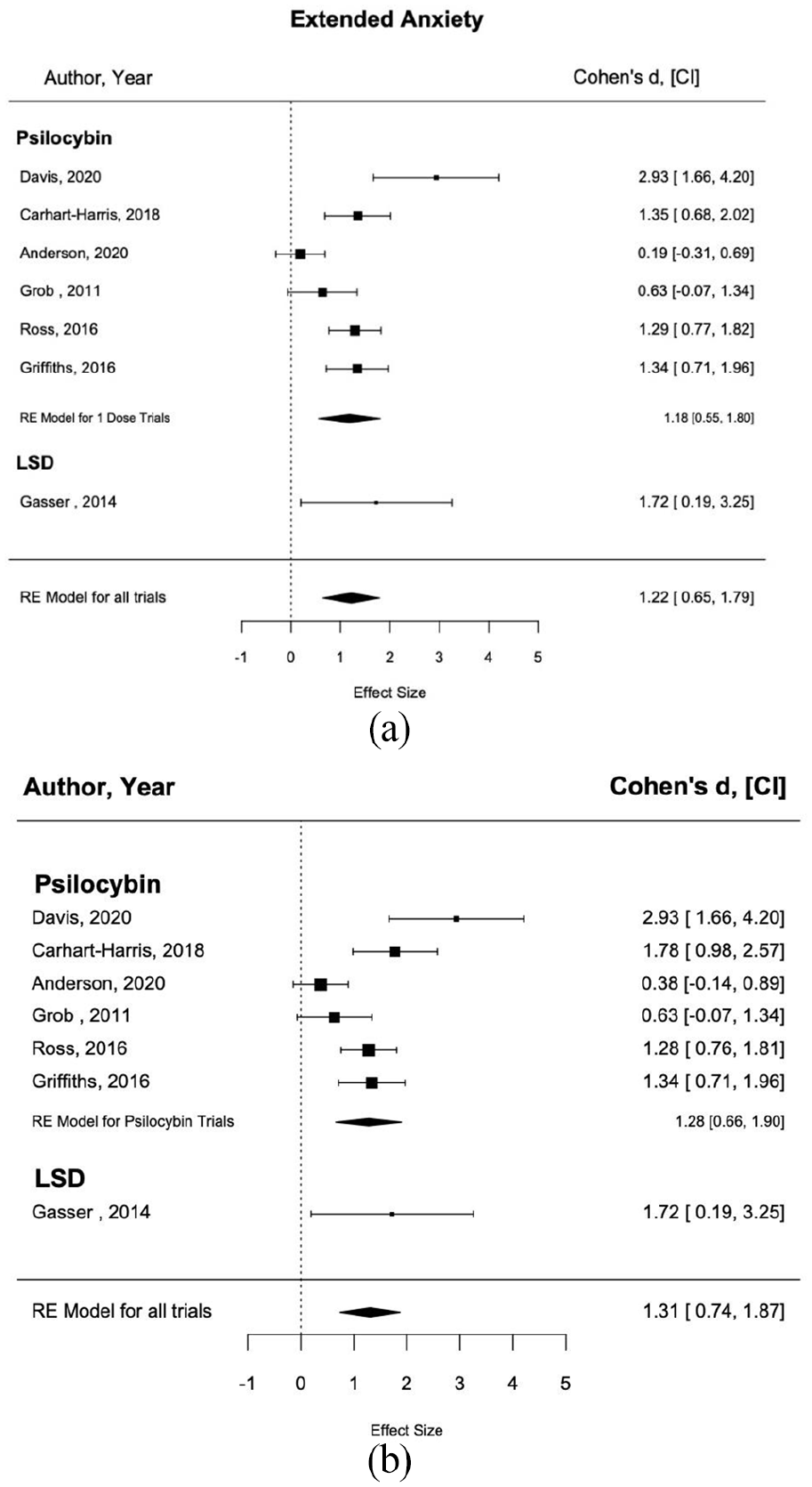
Forrest plots of anxiety with choice of psychedelic agent as a moderator: (a) shows effect sizes for studies reporting data for depression outcomes at >1 week post administration (k = 7) and a random-effects model for the estimate of effect size. Note, no studies using agents other than psilocybin reported data for ⩽1 week; please refer to Figure 5 for plot of acute anxiety outcomes and (b) displays the overall outcomes averaged over all reported time points for studies reporting measures of depression (k = 7) and a random-effects estimate of the effect size.
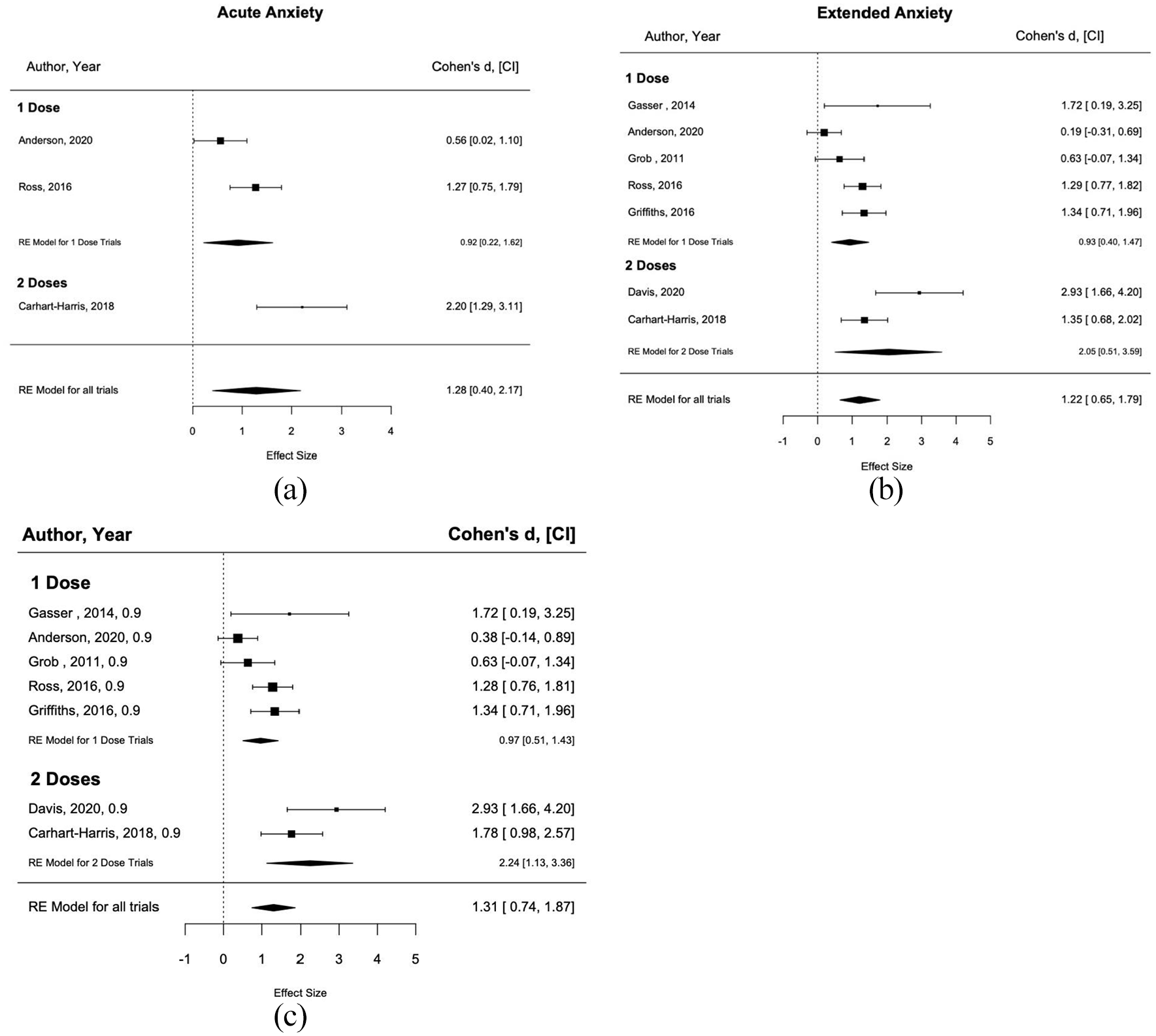
Forrest plots of anxiety with number of administered doses as a moderator: (a) shows effect sizes for studies reporting data for depression outcomes at ⩽1 week post administration (k = 3) and a random-effects model for the estimate of effect size, (b) shows effect sizes for studies reporting data for depression outcomes at >1 week post administration (k = 7) along with a random-effects model for the estimate of effect size and (c) displays the overall outcomes averaged over all reported time points for studies reporting measures of depression (k = 7) and a random-effects estimate of the effect size.
Between all nine trials included, zero serious ADR were reported. There were also no ADR resulting in withdrawal from the study. All reported adverse reactions were mild-moderate, with the level of detail of descriptions varying between studies. As such, meta-analysis on secondary outcomes of ADRs was not preformed. See Supplemental Table 3 for details of reported adverse reactions within studies.
Discussion
The results of this meta-analysis strongly support prior work suggesting the potent effects of psychedelics as therapeutic adjuncts in the treatment of mood and anxiety disorders. Moreover, these effects appear to be large even in the acute setting, a trait that differentiates psychedelics from more conventional antidepressants and anxiolytic therapies, which typically require weeks of drug therapy to become effective (Machado-Vieira et al., 2010) and which is in line with past results (Romeo et al., 2020; Ross et al., 2016). The results of the subgroup analyses, additionally, implicate a preference for regimens with two versus single dose of psychedelic being administered. Although there are only two such studies using two psychoactive doses of psychedelics; the other trials either used one dose or an additional dose given at dosages insufficient to precipitate psychoactive effects (Gasser et al., 2014; Griffiths et al., 2016). These data remain promising, especially in the case of depression, in which the results displayed a very high effect size and level of statistical significance.
Prior randomized controlled trials of healthy subjects with psilocybin (Griffiths et al., 2011) and LSD (Holze et al., 2020) have shown that these agents display a dose-dependent relationship with subjective effects within patients for drug administration occurring on a single occasion. Correspondingly, the results of the present subgroup analysis would suggest that this dose-response relationship can be applied to multiple time points. Of note, in both of these prior studies (Gasser et al., 2014; Griffiths et al., 2016) higher doses of psychedelics were unsurprisingly associated with greater incidences of ADRs. Because psychedelic-associated ADRs are also typically transient (Dos Santos et al., 2018) administering larger quantities of drug by dividing it over the course of multiple sessions may represent a safer and more efficacious dosing regimen for future investigations. Of note, in trials using non-psychoactive doses of psychedelics as controls (Gasser et al., 2014; Griffiths et al., 2016), effect sizes may be larger than they appear, as this approach may not have served as a true control. Although researchers have proposed psychedelic-induced subjective changes to be necessary to facilitate change (Griffiths et al., 2011), sceptics have pointed out that the supporting evidence is largely correlational and may not be required to induce plastic changes (Olson, 2021).
The present findings also suggest that there may not be a significant difference between the selection of different psychedelic agents, ayahuasca, LSD or psilocybin; no significant differences were observed between any of the three agents for analyses of either depression or anxiety outcomes. Some scepticism of this result is required, however, as the samples of trials utilizing either ayahuasca or LSD are far more limited than those using psilocybin. This is especially true given that there were no reported results for any dedicated measures of anxiety in trials using ayahuasca, highlighting an important future area of scrutiny.
One of the most important findings of this meta-analysis was the extremely large effect that all psychedelic dosing regimens displayed on early improvements of both depression and anxiety in the acute time period. The ability of a potential antidepressant to take effect almost immediately has previously been described as a characteristic of an ‘ideal drug’ (Richelson, 1994). Currently the only other agent known to produce such immediate antidepressant effects in <24 h following administration is ketamine (Berman et al., 2000; Feifel, 2016). However, unlike ketamine where the duration of effect is typically 3–14 days (Feifel, 2016), psychedelics’ antidepressant and anxiolytic effects appear to be more enduring (Romeo et al., 2020). Although there is a degree of uncertainty regarding the magnitude of this effect at different extended time points, as our present analysis averaged all values for time points >1 week, the results for all studies were significant at all extended periods for anxiety and all but one (Gasser et al., 2014) had averages for their depressive scores that were significant. More longitudinal studies are needed to understand how the therapeutic effects change over prolonged periods of time.
Apart from their rapid effect, the large effect sizes observed in these trials also distinguishes psychedelics from traditional medications, which have remission rates of roughly 36% for any single first line agent (Rush et al., 2006). For psychedelics to show the responses that they did within these trials—many of which included patients who were experiencing TRD (Carhart-Harris et al., 2018; Palhano-Fontes et al., 2019; Zeifman et al., 2021)—is distinguishing from current treatment modalities. However, the hopefulness of these findings must be tempered with caution and an abundance of academic rigor, testing with larger sample sizes and more effective blinding measures. It is important to consider the opinions of some of the field’s experts who have cautioned against overly optimistic thinking regarding the tendency of some to look at psychedelics as a new panacea for mental health (Berman et al., 2000; Yaden et al., 2020). This is especially true given the significant deficiency of all included trials to show susceptibility to different domains of bias, though this may represent an inherent quality of conducting research with drugs possessing such readily identifiable psychoactive properties. In the construction of future trials, the use of non-antidepressant comparators, such as midazolam, with psychoactive properties meant to better mask the subjects’ treatment arm, would be of great value in order to better ascertain the contribution of the placebo effect to observed results. Currently, the failure of blinding significantly introduces bias into any interpretation of all current studies, as they are effectively all unblinded. This is similar to the prevalent failure in successfully blinding patients in trials using selective serotonin reuptake inhibitors (SSRIs), in which subjects consistently correctly assess whether they have received an active drug (Kirsch, 2019). However, whereas the effect sizes of SSRIs in the treatment of depression and anxiety are typically considered around d = 0.3 (Hengartner and Plöderl, 2018; Kirsch, 2019), not much larger than those observed in placebo arms, the effect sizes observed in trials reported here are substantially larger. Regardless, future refinement of current techniques is needed to elucidate the extent that this is due to intrinsic effects of the drugs and to limit bias. If psychedelics are ever to become useful parts of mainstream psychiatric treatment, remaining cognizant of their limitations now, as their uses and side effects are still being uncovered, is of the utmost importance.
Conclusion
The potential for psychedelic drugs to become licensed medicines for the treatment of anxiety and depression has gone from a pipe dream to an ever more likely reality, as new trials are registered with accelerating frequency. It is imperative that before this new wave begins to crest, a solid foundational groundwork is present to underpin these future investigations. The conclusions to be drawn from this present work suggest strongly that psychedelics are able to opportune significant changes in patients’ experiences of depression and anxiety in a uniquely early and enduring way. Moreover, based on extant investigations, though still limited to a relatively small but growing number of studies, there do not appear to be substantive differences between individual psychedelic agents with regard to impact on depression and anxiety. However, the present analysis does suggest a significantly greater effect dependent on repeated versus single psychedelic dosing. Further investigations are needed to better elucidate these benefits and determine the optimal number of psychedelic administrations for patient outcomes.
Supplemental Material
sj-docx-1-jop-10.1177_02698811211044688 – Supplemental material for Assessing the effects of methodological differences on outcomes in the use of psychedelics in the treatment of anxiety and depressive disorders: A systematic review and meta-analysis
Supplemental material, sj-docx-1-jop-10.1177_02698811211044688 for Assessing the effects of methodological differences on outcomes in the use of psychedelics in the treatment of anxiety and depressive disorders: A systematic review and meta-analysis by Robert F Leger and Ellen M Unterwald in Journal of Psychopharmacology
Supplemental Material
sj-docx-2-jop-10.1177_02698811211044688 – Supplemental material for Assessing the effects of methodological differences on outcomes in the use of psychedelics in the treatment of anxiety and depressive disorders: A systematic review and meta-analysis
Supplemental material, sj-docx-2-jop-10.1177_02698811211044688 for Assessing the effects of methodological differences on outcomes in the use of psychedelics in the treatment of anxiety and depressive disorders: A systematic review and meta-analysis by Robert F Leger and Ellen M Unterwald in Journal of Psychopharmacology
Supplemental Material
sj-docx-3-jop-10.1177_02698811211044688 – Supplemental material for Assessing the effects of methodological differences on outcomes in the use of psychedelics in the treatment of anxiety and depressive disorders: A systematic review and meta-analysis
Supplemental material, sj-docx-3-jop-10.1177_02698811211044688 for Assessing the effects of methodological differences on outcomes in the use of psychedelics in the treatment of anxiety and depressive disorders: A systematic review and meta-analysis by Robert F Leger and Ellen M Unterwald in Journal of Psychopharmacology
Footnotes
Acknowledgements
We would like to acknowledge Dr. Rafael Guimarães dos Santos & Dr. Jaime EC Hallak of the Department of Neuroscience and Behavior at Ribeirão Preto Medical School for assistance in providing subject data for this analysis.
Author contributions
RFL contributed to the design of the investigation’s research questions and methodological protocols, performed screening, evaluation and data extraction, as well as statistical analysis and drafting of the manuscript. EMU contributed to the design of the investigation’s research questions and methodological protocols, evaluation of screened studies and assisted in completion of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.