
Abstract
Background:
Classic psychedelics show promise in the treatment of mental health conditions; however, more scalable intervention protocols are needed to maximize access to these novel therapeutics. In this proof-of-concept study, perceptions of safety, subjective effects, and beliefs about the clinical utility of lysergic acid diethylamide (LSD) were evaluated among healthy participants (N = 31) administered 50 to 100 µg LSD in a treatment paradigm conceptualized as more scalable than traditional approaches to administering classic psychedelics.
Methods:
Semi-structured interviews assessed participants’ expectations, experience, and thoughts on the safety and efficacy of the study design. These interviews were transcribed for thematic analysis relating to perceptions of safety, subjective effects, and beliefs about the clinical utility of LSD.
Results:
Most participants felt safe throughout the study, with a minority reporting concerns related to having a challenging experience that diminished over time. Participants attributed their feelings of safety to the study structure and support of their attendants, which allowed them to “let go” and immerse themselves in the experience without pre-occupation. Furthermore, participants reported transcendent, mystical-type experiences characteristic of classic psychedelics, with almost half highlighting the prominent role played by music during the acute period of drug action. Finally, participants endorsed support for the clinical utility of LSD in controlled environments, expressing the belief that LSD is safe and has the potential to help others.
Conclusion:
Findings provide preliminary support for the feasibility of this scalable interventional paradigm and set the stage for future critical research with clinical populations.
Introduction
The discovery of the 5HT2aR agonist (i.e. classic psychedelic) lysergic acid diethylamide (LSD) in 1943 sparked notable scientific interest, with thousands of manuscripts, dozens of books, and a number of international conferences focused on LSD-assisted psychotherapy (Grinspoon and Bakalar, 1979; Masters, 1973; Nutt et al., 2013; Passie et al., 2008). Due to a lack of modern methodological rigor, most of the early clinical studies of LSD are best understood as inconclusive, yielding only pilot data suggesting safety and efficacy (Bonson, 2018). Nevertheless, among the most promising findings was LSD’s potential to treat alcohol dependence (Krebs and Johansen, 2012) and other substance use disorders (Savage and McCabe, 1973), as well as end-of-life distress (Gasser et al., 2014). Despite a clear medical and scientific rationale, legal proscriptions were enacted and funding was withdrawn, leading to a protracted moratorium on human research with LSD and other classic psychedelics.
Human research with classic psychedelics re-emerged in the 1990s (Hasler et al., 1997; Strassman, 1994); however, in 2014, results of the first modern clinical trial of LSD-assisted psychotherapy were published (Gasser et al., 2014). Contemporary research suggests LSD has a favorable safety profile at doses ranging from 5 to 200 µg (Family et al., 2020; Liechti, 2017; Schmid et al., 2015), and several clinical trials of LSD are currently underway (NCT03153579, n.d.; NCT03781128, n.d.; NCT03866252, n.d.).
As is characteristic of classic psychedelics, LSD can occasion transcendent, mystical-type experiences characterized by feelings of oneness or unity, profound insight, sacredness, deeply felt positive emotion, transcendence of time and space, and ineffability (Hendricks, 2018; Johnson et al., 2019; Liechti, 2017). LSD is not physiologically toxic, but like all classic psychedelics, LSD can engender challenging experiences, colloquially known as “bad trips,” characterized by feelings of acute anxiety/fear/panic, paranoia, and depersonalization/derealization (Gasser et al., 2014; Holze et al., 2021; Johnson et al., 2019; Passie et al., 2008; Schmid et al., 2015). For this reason, modern research emphasizes the importance of several practices in the administration of classic psychedelics to both minimize the likelihood and impact of challenging experiences and maximize transcendent, mystical-type effects during clinical trials. These practices, articulated by Johnson et al. (2008), typically involve intensive preparation prior to drug administration, oversight of two attendants or “guides” during the acute period of drug action, and multiple follow-up psychotherapy “integration” sessions in the days or weeks following drug administration. For example, in a study of psilocybin in the treatment of demoralization, Anderson et al. (2020) administered one dose of psilocybin over a 7-week intervention period that involved approximately 3 h of individual psychotherapy and up to 15 h of group psychotherapy. In a study comparing psilocybin to escitalopram for depression, Carhart-Harris et al. (2021) administered two doses of psilocybin over an approximately 6-week intervention period that included one 3-h in-person preparatory session, two in-person integration sessions, and six “debriefing” or integration sessions via telephone or mobile technology. Moreover, in a study of psilocybin in the treatment of major depressive disorder, Davis et al. (2020) administered two doses of psilocybin over an 8-week intervention period that involved at least 18 in-person visits, 8 h of preparation, and up to 6 h of integration. Finally, in the only contemporary clinical trial of LSD published to date, Gasser et al. (2014) administered two doses of LSD to patients with life-threatening illnesses over a month-long intervention period that included two preparatory sessions and six integration sessions lasting 60 to 90 min. Unfortunately, the intensive nature of these practices raises concerns about their implementation in the real world, where affordability is vital (Cairns, 2016). Indeed, just as esketamine has faced barriers to adoption secondary to its resource intensiveness (Wilkinson et al., 2019), it has been noted that the intensive nature of classic psychedelic therapies will almost surely render them expensive and difficult to access, especially for those living with economic disadvantage (Thrul and Garcia-Romeu, 2021). More scalable approaches are essential to allow for broad accessibility to LSD-assisted psychotherapy as an affordable treatment modality.
The current proof-of-concept study was developed to evaluate the safety, tolerability, pharmacokinetics, and subjective effects of 50 to 100 µg LSD base among healthy participants in an intervention paradigm conceptualized as more scalable than traditional approaches to administering classic psychedelics. This paradigm involved abbreviated preparation and integration, and a single attendant to assist each participant. As described in a companion article reporting quantitative outcomes (Family et al., 2022), participants spent full days at the research site and their participation was framed around exploring creative problem solving regarding a work-related issue, results of which will be reported elsewhere. This framing allowed for the development of an operational protocol for an interventional trial and differentiates the current protocol from previous studies that have administered classic psychedelics to healthy participants (Carhart-Harris et al., 2015, 2016; Dolder et al., 2017; Preller et al., 2019; Schmid et al., 2015) that have evaluated only safety, pharmacokinetics, and/or neurobiological outcomes. Although caution should be exercised in generalizing to clinical populations, healthy participants were deemed appropriate for this preliminary examination insofar that healthy adults can and do have challenging experiences as well as transcendent, mystical-type experiences associated with improvements in psychological functioning with classic psychedelics (e.g. Galvão-Coelho et al., 2021; Griffiths et al., 2008; Nicholas et al., 2018).
The objectives of the present report were to assess perceptions of safety, subjective effects, and beliefs about the clinical utility of LSD using data from semi-structured interviews among those who completed the current protocol. The qualitative approach described here allowed participants to describe their experience without having their experience imposed upon them and provide information not otherwise captured by existing quantitative measures. From this perspective, the current study was conceptualized as a valuable first step in refining the novel intervention paradigm and generating hypotheses for future clinical trials. Indeed, qualitative approaches can provide a wealth of information for understudied areas of research (Lewin et al., 2009), and considering that only one other contemporary qualitative study of LSD administered in a clinical setting has been conducted (Gasser et al., 2015), qualitative methods were considered especially well suited for the present report.
Methods
This was a phase 1 proof-of-concept, single-center, dose-escalation study that used both open-label and double-blind placebo-controlled designs. The study protocol and informed consent form were reviewed and approved by the independent ethics committee for the investigational site. The study was conducted in accordance with International Conference on Harmonisation harmonized tripartite guideline on Good Clinical Practice and UK law. Each participant provided written informed consent after adequate explanation of the aims, methods, anticipated benefits, and potential hazards of the study.
Study design
Two sub-studies in different populations of healthy participants were carried out as follows: part 1 was an open-label dose-escalation study in psychedelic non-naïve participants, and part 2 was a double-blind, placebo-controlled, randomized study in psychedelic naïve participants. Psychedelic non-naïve participants were defined as those who used LSD or any other classic psychedelic on more than three occasions in their lifetime. Psychedelic non-naïve participants were chosen for part 1 as they were assumed to be less likely to have psychologically adverse reactions to blood draws at multiple points during the acute effects of LSD. Psychedelic naïve participants were defined as those who had not used LSD or any other classic psychedelic in the past 7 years. In practice, only one of the participants in part 2 of the study reported previously ingesting a classic psychedelic: one instance of psilocybin-containing mushrooms at age 14. Naïve participants were recruited to measure safety and tolerability in a population closer to the target population (i.e. individuals with no prior experience with psychedelics).
In part 1, 13 participants were randomly assigned to one of five cohorts (maximum three participants per cohort) and received a single dose of 50, 75, or 100 µg LSD. In part 2, participants were assigned to one of eight cohorts (maximum three participants per cohort), and then randomly assigned to the experimental treatment group (n = 9) or the placebo-controlled group (n = 10). They received their assigned study treatment on two separate occasions, as follows: participants either received 50 µg LSD followed by 75 µg LSD (experimental group), or placebo followed by 75 µg LSD (placebo-controlled group), with dosing separated by 7 days. All participants received their assigned study doses in an inpatient setting and follow-up visits were conducted approximately 1 week and 1 month after the last dose. A depiction of the trial design is displayed in Figure 1.
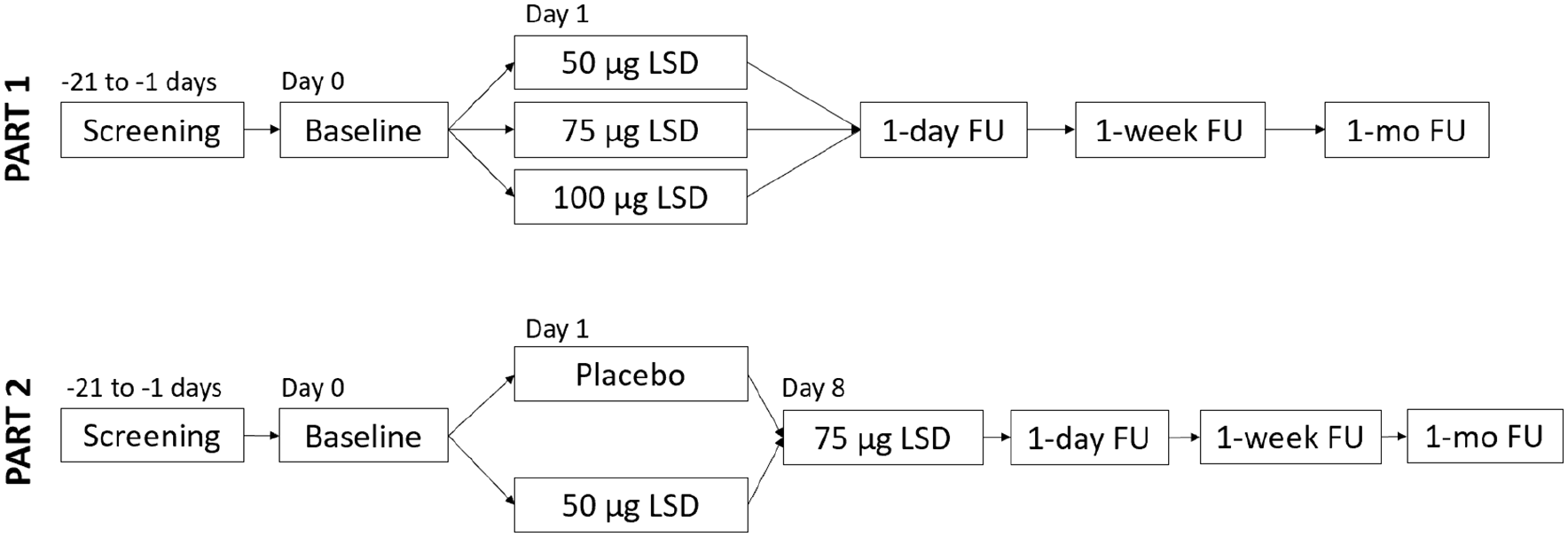
Schematic representation of study design.
Participants arrived at the inpatient clinical trial unit late in the evening on the day prior to their pre-drug baseline assessment and preparation day and stayed overnight (part 2 participants arrived the night before their second dose on their second visit). The following day, participants completed pre-drug baseline assessment and preparation, which included (1) a brief introduction to their attendant after a 1-h breakfast in a communal area with other participants; (2) the completion of computer-based assessments in their room until lunch; (3) a 1-h communal lunch with study administrators, other participants, and attendants, with one of the study administrators presenting an overview of LSD effects, guidance with regard to navigating these effects including challenging experiences per Johnson et al. (2008), and instruction to remain lying down while wearing eyeshades and listening to a predetermined music playlist with headphones for the first 4 h of acute drug action prior to initiating problem solving; (4) an individual session with their attendant after lunch that included 30 min discussing their work-related problem, 60 min of breathing exercises, and 30 min of rapport-building in their room; (5) the completion of computer-based assessments in their room; and (6) a 1-h dinner with study administrators, other participants, and attendants. Participants stayed overnight once more and could read, work, and use their phones. The following day, after a light 1-h breakfast in a communal area with other participants, the study drug was administered at 9:00 a.m. Each attendant remained in the room with his or her assigned participant until 6:30 p.m., with brief breaks for food or bathroom use. A remote monitor was responsible for keeping watch of all three rooms via video and audio streaming and stepped into the rooms in the event attendants needed a break or assistance with challenging experiences. At 6:30 p.m., participants were allotted 1 h for dinner in a communal area with the study administrators, other participants, and attendants, after which their attendants left, and the participants completed final computer-based assessments for the day in their rooms. Participants remained in the clinical trial unit overnight one final time and could use their phones and work on their problems. The following day, they completed computer-based assessments and a semi-structured interview conducted by an external interviewer or study administrator prior to departing before lunchtime. Part 2 participants completed the semi-structured interview after their second drug dose only. Follow-up assessment-only visits were conducted approximately 1 week and 1 month after the last dose at the clinical trial unit, during which no study personnel were present. During these visits, medical assessments were carried out, and participants completed computer-based assessments that focused on secondary exploratory aims (these data not presented here).
D-lysergic acid diethylamide base (d-LSD, high-performance liquid chromatography (HPLC) purity >99%, Onyx Scientific Limited, United Kingdom) was dissolved in ethanol at 25 mg/mL and prepared as a solution 50 or 4 µg d-LSD/mL in distilled water and completed to a final volume of 25 mL with the addition of distilled water for oral administration. A shelf life of 78 h was allocated to the doses, when stored in the defined container closure at a temperature of 2°C to 8°C, with the start of the expiry period being defined as the time of combining the d-LSD with ethanol. Placebo was distilled water only and presumed to be indistinguishable from the LSD solution.
Study participants
Participants were recruited via flyers posted on university campuses that framed the study around exploring the effects of LSD on creative problem solving. Healthy men and women aged 21 to 65 years old were screened within 28 days of randomization. Participants who met all inclusion and no exclusion criteria and provided written informed consent were assigned to a cohort based on availability. For both part 1 and part 2, eligibility was based on a participant meeting the study inclusion criteria and none of the exclusion criteria. Eligibility was also dependent on the outcome of an interview with a physician that was performed as part of the screening process. Key inclusion criterion for part 1 was lifetime use of LSD or any other classic psychedelic drug, including psilocybin, mescaline, and ayahuasca, on more than three occasions. Key inclusion criterion for part 2 was no use of LSD or any other classic psychedelic drug, including psilocybin, mescaline, and ayahuasca, during the past 7 years. Exclusion criteria for both parts included presence or clinically relevant history of any psychiatric, respiratory, gastrointestinal, renal, hepatic, hematological, lymphatic, neurological, cardiovascular, musculoskeletal, genitourinary, immunological, dermatological, or connective tissue diseases or disorders, as judged by the investigator, and blood pressure exceeding 140 mm Hg (systolic) and 90 mm Hg (diastolic). Key psychiatric exclusion criteria included a clinically relevant history of psychiatric disorder as judged by the investigator, first- or second-degree relative with schizophrenia, any manic or hypomanic episode, lifetime presence of any major depressive disorder, dependence on any substance in the past 5 years (part 2 only), current diagnosis of schizophrenia, obsessive-compulsive disorder, dysthymic disorder, panic disorder, anorexia or bulimia, or current symptoms of drug abuse. Current smokers were excluded as per phase 1 guidelines, to avoid drug–drug interactions for pharmacokinetic and other measurements. Also excluded were participants receiving chronic or acute administration of tricyclic antidepressants or lithium, administration of selective serotonin reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, monoamine oxidase inhibitors, or other prescription drugs that may interact with the pharmacokinetics of LSD within 14 days of first dosing. In practice, none of the participants received concomitant central nervous system medications during the trial period. Participants were administered the Columbia–Suicide Severity Rating Scale (C-SSRS) and the structured clinical interview clinical trials version (SCID-CT: First et al., 2002) as a screening tool, modified based on guidelines described by Johnson et al. (2008).
Thirty-two participants were determined eligible for this study. In part 1, 13 participants were enrolled and received 50 µg (n = 3, no women, mean age = 28), 75 µg (n = 7, 1 woman, mean age = 28), or 100 µg (n = 3, no women, mean age = 32) LSD on a single occasion. In part 2, the experimental group (n = 9, 2 women, mean age = 27) received two sequential single doses of LSD (50 µg followed by 75 µg), with dosing separated by 7 drug-free days. The placebo-controlled group (n = 10, 1 woman, mean age = 31) received placebo followed, after 7 drug-free days, by a single dose of LSD 75 µg. The demographic and baseline characteristics for each dose group are summarized in Table 1.
Demographic and baseline characteristics of healthy participants (safety population).
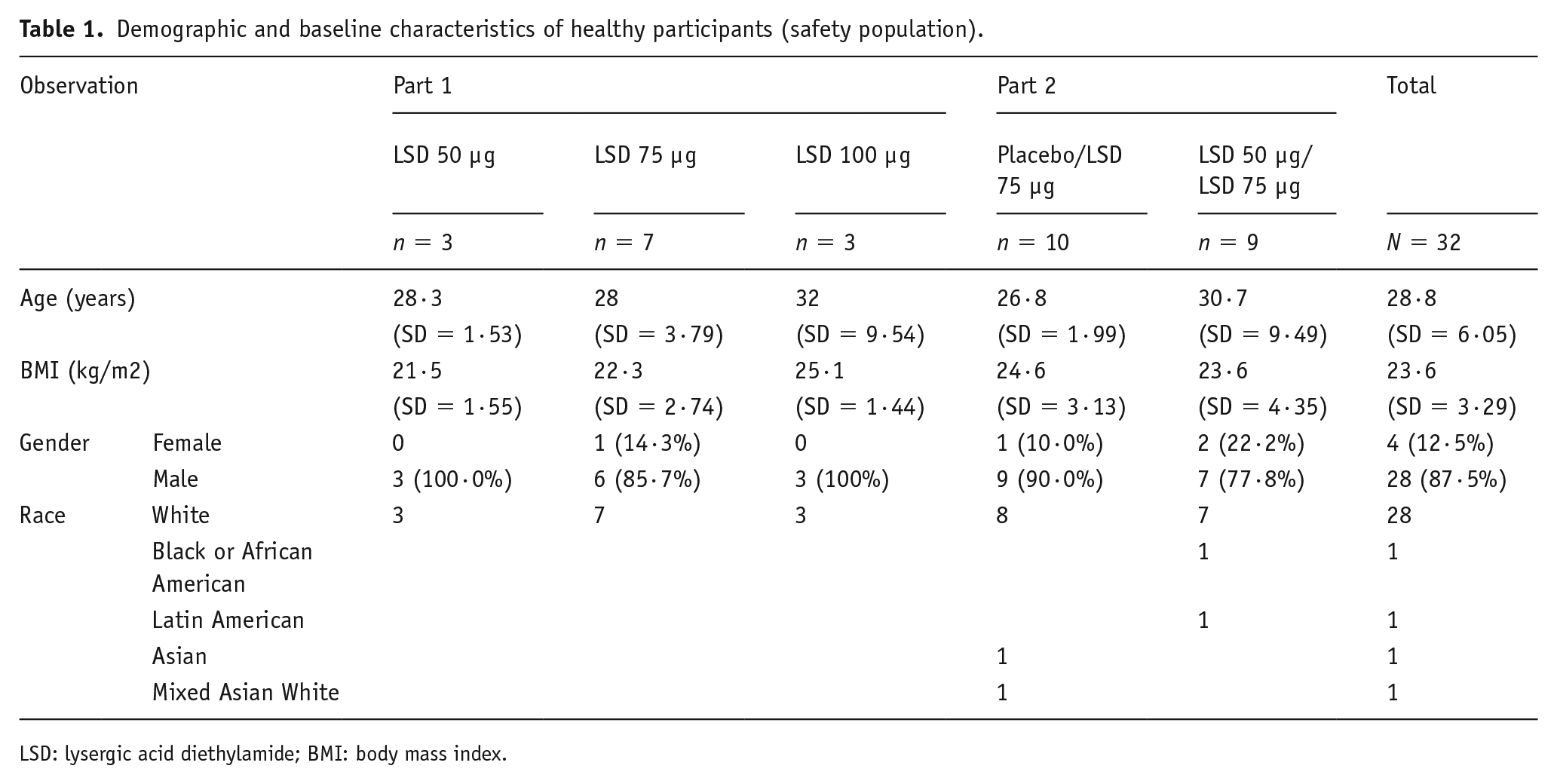
LSD: lysergic acid diethylamide; BMI: body mass index.
The day after participants completed the final drug dose, they were interviewed by either an independent interviewer they had not previously met or by a study administrator who was not in the room with the participant during the LSD experience. The interviews took place in an office space in the same clinical trial unit. One participant was not interviewed because he was withdrawn from the study due to nicotine intake after his first dose, which was a placebo dose, leaving us with a sample of 31 participants.
In semi-structured interviews (see Supplemental File for semi-structured interview script), the participants were asked about their expectations and the outcome of their project-related work, their experience overall, and their thoughts on the safety and efficacy of the study. These interviews were used as a general guide for questions, but questions were not asked in the same order or in the same way for each participant. At times, participants would talk about issues related to questions that had not yet been asked, and in these cases, participants were not asked questions they had already answered. Semi-structured interviews were video-recorded and later transcribed and uploaded into NVivo 12 for thematic analysis. Two members of the research team coded the transcripts relating to perceptions of safety, subjective effects, and beliefs about the clinical utility of LSD. These two team members began by engaging in initial coding of the first five interviews independently and then coming together to compare codes. Any discrepancies in coding were discussed until agreement on coding was met. They then coded the next five transcripts independently and compared them. At this stage, the coders had a high degree of consistency in coding. They continued this process until they had coded all transcripts and compared them. Once all transcripts were coded for themes relating to perceptions of safety, subjective effects, and beliefs about the clinical utility of LSD, the lead coders developed axial codes that were reflected in the results. Such a style of coding is consistent with general standards of qualitative research analysis (Kvale and Brinkmann, 2009).
Results: Perceptions of safety
When assessing the safety of a protocol, it is important to examine objective or quantifiable measures of harm (e.g. adverse events or abnormal values in physiological measures). However, to get a richer understanding of safety, it is important to understand the subjective perceptions of safety among the participants. The objective measures of safety for the current protocol are reported elsewhere (Family et al., 2022). Accordingly, the focus of this article is to investigate participants’ perceptions of safety using qualitative data from a semi-structured interview conducted after their participation in the inpatient segment of the study, which included treatment with LSD.
To assess general perceptions of safety, participants were asked how safe they felt during the protocol. Twenty-three of the 31 participants expressed that they felt safe throughout the entire process. Participant 01 responded to the question about safety by saying, “Completely safe. I think the safest experience ever in the sense I couldn’t harm myself in no way.” Similarly, Participant 06 responded, “I think I felt incredibly safe, you know, especially as I was cannulated and people were taking blood from me and I knew I was under constant observation. I think I felt remarkably comfortable and at ease.” The eight who expressed some anxiety about the study said that these feelings emerged at the beginning but dissipated as the study went along. They were initially concerned about the effects of LSD, believing that they may have “an anxiety attack in the middle of the trip and, you know, freak out in some way” (Participant 04). However, even those with initial concerns said they felt safe by the end of the study.
LSD may cause users to feel a loss of control, which may engender anxiety. Accordingly, participants were asked whether they thought they had lost control at any point during the experiment. Twenty-six of the participants responded in ways similar to Participant 31 who said, “I don’t think I felt I lost control at any point.” Those five who did say they lost control made a point of explaining that losing control was the point of the experiment and that it was an intentional and planned loss of control. Participant 16 said, “I think that’s part of the point [laughs].” He then went on to question what was meant by losing control saying: What do we mean by lose control? I mean it’s kind of weird, I thought I was fully involved in the experience and I was enjoying it and to a larger extent I was directing the experience I would say, so in that respect I didn’t lose control but the whole experience is a loss of control.
Others believed that losing control was expected, but this loss of control was not associated with feeling at risk or in danger. As Participant 21 said, I never felt like I was in danger. For most of the time during the highest intensity trips I couldn’t move, so that kind of keeps you safe in a way [laughs] and I had no desire to move and I was having a lovely time. And, even when I did have maybe a distressing idea, I’d been told that these ideas are very fluid and if you don’t like something you can just . . . leave it and it will turn into something else or don’t worry too much.
The last sentence of this statement supports the importance of adequately preparing participants for their experiences, which was done in the current study.
Overall, the participants expressed that they felt safe and at limited risk of danger due to the protocol. The feelings of safety they expressed were largely generated by two primary aspects of the protocol: (1) the overall structure and (2) the presence of attendants.
Structure of the protocol
The study took place in a phase I clinical unit in London (UK), and participants were compensated for travel expenses and for participating in the study in accordance with ethical approval. The days’ events were structured, and staff guided participants as to where to go and what was to come. This defined structure was partly designed to enhance participant safety and foster feelings of trust so that participants could feel comfortable and “let go.” To assess the success of this structure for facilitating feelings of safety, participants were asked if the structure of the protocol reduced or mitigated possible negative experiences. All participants said something positive about the structure of the protocol, though some were ambivalent. The aspects of the structure that the participants found effective at minimizing their concerns of negative experiences were (1) the presence of staff throughout the process, (2) the clearly defined schedule, and (3) legally sanctioned use of medical grade LSD.
Participants’ days were structured so that they knew when each event of the day took place. For 23 participants, this meant that they did not have to worry about keeping up with where to be or how to get there. Participant 24 described what the protocol was like: The setup was quite helpful in the way that it was quite clear what to do: lay down, close the eyeshades, listen to the music. . . . You didn’t need to take any decisions. . . . You don’t have to think about what is to come.
For the majority of participants, being in a structured setting aided in enhancing their experiences and contributing to feelings of security during the process. However, eight participants were ambivalent about the tight structure and schedule. These participants suggested that the structure felt safe, but it may have inhibited their experiences. Namely, they said that the constraints associated with being administered LSD in a formal setting prevented them from being able to fully explore the world around them during the acute period of drug action. Participant 22 said, “I wanted a bit of fresh air. . . . If anything I felt too safe. So, yeah, I just wanted to feel that breeze. . . . But, yeah, it was more than safe.” Participant 26 also expressed the ambivalence of the setting: It’s a bit awkward being in a hospital, but it’s also kind of comforting because it is in the back of your head that you know there’s lots of people here who know what they’re doing and you can think, “Well, what if I’m like this for days?” But you kind of think, “Well, I’m in the best environment really because there’s medics.” . . . I wouldn’t say [its] the best place to be ’cause I guess the best place to be is somewhere in a forest or something like that, but as far as, you know, if somebody’s anxious about their health or something like that, I would say this was an optimal environment.
Others expressed that they would have preferred to be with close friends rather than with strangers. Participant 22 said, “I remember saying, I just wanna be with a couple of my mates and just talk through this like strange situation that is going on.” In short, these eight participants believed that they felt safe throughout the protocol, but that the safety protocols diminished their autonomy and ability to experience the effects of LSD in ways they would have preferred.
Perceptions of attendants
The protocol for the study included having an attendant be available at all times during the acute period of action of LSD. The current protocol had attendants from a variety of backgrounds. Ten attendants (six women and four men) were hired to sit with participants. These attendants had backgrounds in psychotherapy (n = 2), breath work (n = 4), cognitive science (n = 3), and literature (n = 1). Their role was to attend the baseline session and the drug treatment session to provide support by practicing some of the basic components of the competencies of a psychedelic therapist (Phelps, 2017): namely, being knowledgeable and able to answer questions about the drug experience, supporting the session by building trust with the participant, practicing mindfulness, and empathetic listening. They also were responsible for any logistical issues, like providing the participant with any immediate requirements of pen/paper, food, water, or being escorted to the restroom.
When asked what they thought about having an attendant with them during the trial, the participants were in near-universal agreement that having an attendant was beneficial to their experience. All participants expressed very positive reactions to the attendants, believing that they very much facilitated a good experience. Echoing this, Participant 17 said, “I think it’s the whole idea that you’re being looked after gives you freedom to actually let go.” Participant 28 said, “I couldn’t have done it without the assistant.” The reasons for the beneficial experiences fell in two broad categories: emotional security and practical benefits.
Emotional security included statements relating to how the attendants helped ease any emotional uncertainty or anxiety. Eighteen participants mentioned such ideas. Those who mentioned the emotional security said that they felt a bond with their attendants, which they believed might have been due to the effects of LSD. Participant 01 said of his attendant: “I love my assistant. It’s my dad now I have two fathers. [smiles] And, so it’s really important to have an assistant because it can help you during the task.” Similarly, Participant 29 said of his attendant: I cannot imagine doing this without a person. And the other part is a little bit like it gives confidence. So you feel like because there’s someone there that can help you any time then you feel more like relaxed and you can just enjoy the experience. So very useful, yeah.
Practical benefits included statements relating to how the attendants were able to satisfy any needs they had. Many of these needs included having access to writing equipment, directions to restrooms, help in case of medical emergencies, and access to food and drinks. Twenty-three participants mentioned practical benefits. Some appreciated having someone to help with simple needs. As Participant 05 said, “Yeah, [the attendant] asked like all the time, ‘Is everything okay?’ And he was really attentive. . . . Can I have some water please? And can we switch on the heating?” Participant 06 said, “It was very nice having somebody to take me to the bathroom.” Participant 07 said of the attendant: He completely looked after me for since I’ve been here. So, you know, where I need to go, food I need to eat, what I need to be doing, my experiences, if I have any problems. He’s like the go-to person for comfort: so comfort in the room, changing light levels, simple things like opening the window, which I couldn’t even see so [laughs].
Participant 03 succinctly summed up why attendants helped: “Worries were contracted out. I didn’t have to think about being too hot or too cold or where my food was going to come from.”
We should note that seven of the participants said that they understood why attendants were present, but that they did not know if the attendant was needed. Participant 22 said that he “didn’t have the independence because they do so much for you.” He recognized the need for the attendant but also thought having one stifled his independence. Participant 23 said, I didn’t feel like I needed them there but I understand that that’s almost the definition of their success is that I didn’t feel imposed upon or imposing upon them. So, if they weren’t there I don’t see that I would have had a significantly different time. . . . I think they helped with physical things, like I might have found it hard to carry my tray over to my table or something, so that was great.
Participant 14 said, Well it was very comforting knowing that someone was there in case I needed anything. At the same time though sometimes I really thought I would like to be alone here because I’m accessing myself and I really need to focus on my own and I feel a bit shy about being in the room with someone else, just exploring inside me. But I really couldn’t distract myself and just say it out loud so I just lived with it.
In general, these ambivalent participants expressed a concern that the attendant would at times get in the way of their experiences. The attending behaviors of checking in on participants to ensure they were doing well were seen as bringing them out of the pleasurable moment. Nevertheless, each of these participants did say that they understood why the attendant was there and that having them helped for many situations.
Results: Subjective effects
Use of LSD has been shown to occasion transcendent, mystical-type experiences where users feel awe, wonder, amazement, and deep connections with others. These experiences are relevant to the clinical application of the current protocol insofar that such experiences are thought to underlie the therapeutic efficacy of classic psychedelics (Hendricks, 2018; Johnson et al., 2019). Accordingly, it was important to determine what type of experiences participants had after being administered LSD. Participants were asked to describe their experiences during the protocol, including what they perceived as the most enjoyable aspect of it. Participants described experiencing deeply felt positive mood/euphoria, pseudohallucinations/visual effects, and a connection with others (and their work), which they said were the most enjoyable parts of the study. In fact, every participant referenced the acute effects of LSD when asked what was most enjoyable about the study.
For some participants, the euphoria brought on by LSD was the most enjoyable aspect of the study. Participant 06 replied, Now I felt euphoria before with other drugs, but this one was, I think the best word to describe it was a very deep, rich euphoria. . . . And with that came a very intense sensation of well-being, happiness with myself, happiness with my surroundings, and just a contentment with the way my thoughts and mind processes were going.
For some, these feelings lasted throughout the day. Participant 09 said, “It was quite euphoric in terms of it allows you to, I was smiling the entire day. There was no feelings of fear, no feelings of worry.” Finally, Participant 20 said, I feel the most enjoyable moment was when I met happiness in my trip. I really met happiness and I met love. I really met the feelings. I could see them and I could feel them, and it was very enjoyable. It was great because it was not connected—it was not happiness for something that has happened or happiness for something that I saw or whatever. And it was not love for someone, love for something. They were just there, pure emotions that I could embrace and really see, feel, and probably taste as well.
Participants also discussed experiencing pseudohallucinations (audio and visual), which they found pleasant and contributed to their euphoric feelings. Participant 29 said, The most enjoyable part was the visuals that I got when the effect of the drug started. It was the diamond sparkling-like colors and they were so, so enjoyable. I was just looking at them and they were making so many different patterns. And the feeling of joy inside, the feeling of peace inside. And the feeling of awe and wonder that I’ve never seen this before.
Similarly, Participant 15 described the visuals in a favorable manner: I mean yeah for that particularly that was just a very vivid moment where just everything was sort of white and this kaleidoscope tunnel around me. Yeah, kaleidoscope tunnel vision everywhere. In terms of other visualizations, I mean there was hundreds throughout the day. Yeah, and every moment, like say, everything would be sort of segmented. So for one minute I could be I don’t know in my mind’s eye just like riding down the Euphrates in like a boat at the start of civilization, and then at the next, however much time had passed later, I’d be yeah, staring at a mark on—well I didn’t realize it was a mark I was just staring into sort of some kind of space and there was um, with my eyes open or maybe closed I couldn’t tell, and there was just sort of um, sort of visions going on around me and one particular very strong vision which looked like a black hole swallowing things and that happened to be a mark on the ceiling for example, yeah. But yeah, it was quite powerful, some of the visions, and really interesting.
When describing their experiences after being administered LSD, the participants highlighted how they felt connected with others and the world. For example, Participant 06 said, “I felt a very deep sense of connection with my environment and the people around me after I took it and a greater sense of well-being and comfort with myself.” The current protocol was framed around the effect of LSD on creativity for problems the participants were working on for their jobs or in school. They said that these feelings of connectedness gave them additional motivation to work on their problems because they saw how their work related to the world more broadly.
Fourteen participants said their perception of the music was among the most enjoyable aspects of the study. During the protocol when participants were experiencing the effects of LSD, a pre-arranged playlist was played, which included a mix of ambient, classical, and neoclassical music, although some participants chose to play their own music instead. Participant 24 stated, “I was feeling music very, very emotionally. There were different bits of music that were playing, and they would completely, totally change the emotions I would have.” Participant 17 said, The best thing was listening to music and have synesthesia effect where I could see the music and taste it. So, this violin classical music would like freeze in the air and just being crunchy and taste like coconut, so it was quite new, enjoyable.
Participant 27 said, “Listening to the music under the influence was just amazing.” Finally, Participant 20 reported, So, I was following the music. And the music was very vivid, was very dynamic, and it was very visual. I could really follow it as if I was following some strings that were growing in some directions. I could feel that it was directing me toward different feelings. And I realized that at some point I arrived, say, in Happiness Island or whatever, and that’s how I found it, and the same for love. . . . It was very, very different because listening under LSD I was giving to it some meaning. I think that the music was kind of the sea in which I was traveling through with my vessel, say, but I could still decide where to go. So, I could decide whether I wanted to explore that side of the music or something else and that’s how I reached happiness and really, I was so happy. I can hardly describe it.
All except one of the remaining participants expressed neutral or no preference for music. The one negative case said the “music was a bit annoying.” Findings suggest that music was either a benefit or neutral for enhancing the experience during the protocols. However, the one negative case suggests that it is important to provide participants with options regarding music.
Of note, three participants referenced their bonding with the study team as among the most enjoyable aspects of the study. Participant 27, for instance, stated, It was a really nice setting and the people were really nice. You know, I just enjoyed dinner with the people, and they treated us so well, giving us great food and rooms and things, so that was definitely the best part or one of the best parts.
Results: Beliefs about the clinical utility of LSD
Participants were asked what they might tell others, including regulators, about their experience in the study. The assumption was that if they believed they benefited from their participation, they would endorse the clinical utility of LSD. Twenty-six of the 29 participants who were asked what they would say to regulators if asked about LSD said that they would encourage them to either make LSD legal or at the least allow scientists to study it more. These respondents said they would speak favorably about LSD to regulators for two reasons. First, they believed that LSD was a relatively safe drug that has the potential to help people. Participant 11 reflected this positive perception of the benefits of LSD in general. When asked what he would say to regulators, Participant 11 said, That this drug has a lot of potential to help people in a great number of ways, and also teach us a lot about human consciousness and that it’s a great shame that more research can’t be undertaken on this substance. Both in terms of the people who are not able to benefit from this and also in terms of our not expanding our understanding of who we are and how we operate.
The other reason was more about the need for better science on the topic and that regulators should at least provide more opportunities to clinically test the benefits of the drug. Participant 30’s comment reflected this argument: With all regulations that they’re to protect people. If there’s any kind of change to these kind of regulations it should be conducted in a very, very, very controlled way. There should be a lot of checks and sanctions on who has access to these kind of substances and how people are introduced to them and the context in which they are given them? I think the regulators should consider lowering all of the sanctions but responsibly.
Four participants expressed enthusiasm for the utility of the LSD for clinical help when administered in controlled environments. Participant 18 said, There should be special pharmacies where depressed physicists can come and just ask for a dose and just lie down for the night in a single bedroom and come very, very happy and with a smile on their face the other day and everything changes, yeah. Because as I noticed it has no side effects, so why not? Of course, it shouldn’t be open to the public but under restricted conditions I would be very up for it.
Participant 31 said, With the screening process, making sure people are completely mentally capable and safe to take it, it’s boundlessly useful and beneficial and I think it has so many legs for like real-world therapies and um, just helping. It’s like no other drug that I’ve observed. Like there’s seemingly no negatives, but I guess we’re still investigating that just to make sure.
Finally, Participant 29 expressed the belief that LSD administered in controlled and supportive settings could be a useful treatment for alcohol misuse: Yeah [laughs] that’s a little bit embarrassing. But anyway, I really like and enjoy drinking, I just don’t go and do it like every day of my life. But I can handle quite a lot of alcohol and all that. So, I enjoy it a lot. And the first time I tried the dose I was thinking oh I should have a drink on Sunday with my friends. I didn’t want to see or smell any alcohol during the whole week, and I feel the same way now. So, I don’t know if there’s an inhibition for that after the LSD, and I think I asked you about that. So, experiencing that myself I can tell that that could be a way to solve that.
Such statements suggest that the participants believed they benefited from the participation in the protocol.
Discussion
The objectives of the present study were to assess perceptions of safety, subjective effects, and beliefs about the clinical utility of LSD among healthy participants in an intervention paradigm conceptualized as more scalable than traditional approaches to administering classic psychedelics. In contrast to these more intensive approaches (e.g. Anderson et al., 2020; Carhart-Harris et al., 2021; Davis et al., 2020; Gasser et al., 2014), the current paradigm involved abbreviated preparation and integration, and a single attendant to assist each participant. Most of the participants (23 of 31) felt safe for the duration of their participation in this paradigm, with a minority (8 of 31) reporting concerns about having a challenging experience with LSD. These eight who reported initial concerns said that the presence of attendants and a clear structure aided in relieving their initial anxieties to a point that they no longer had them by the end of the study. Addressing the potential of challenging experiences during the pre-drug preparation period and resolving them during the acute period of drug action is a focal point in the administration of classic psychedelics to humans (Johnson et al., 2008). Consistent with this focus, those participants reporting concerns of a challenging experience reported that these concerns dissipated with time. Importantly, participants attributed their feelings of safety to the structure of the current paradigm and the emotional and practical support provided by the attendants. Consistent with analyses indicating that a mental state of surrender predicts positive experience whereas pre-occupation predicts adverse experience with classic psychedelics (e.g. Aday et al., 2021; Russ et al., 2019), participants indicated that the study structure and attendant support allowed them to “let go” during their experience with LSD. Although some participants expressed that the study structure (8 of 31 participants) and attendant presence (7 of 31 participants) may have stifled their independence, they nevertheless acknowledged the benefit of a controlled and supportive environment in ensuring safety. These findings highlight the importance of structure and interpersonal support in the administration of classic psychedelics, and show that they can be established in a more condensed and practical timeline.
With regard to subjective effects, participants reported transcendent, mystical-type experiences characteristic of classic psychedelics like LSD. Although this finding was not unanticipated, it is nonetheless critical to note because mystical experiences are believed to be a key mechanism through which classic psychedelics exert their beneficial effects. Indeed, mystical experiences might be considered a proxy for therapeutic response (Hendricks, 2018; Johnson et al., 2019). These findings therefore suggest that the current intervention paradigm may hold promise of efficacy in clinical populations. Almost half of the participants (14 of 31) reported that their perception of music was among the most enjoyable aspects of the protocol. Although music has long been used in classic psychedelic-assisted psychotherapy, it remains an understudied topic. Nevertheless, emerging evidence supports the central role of music in clinical settings (Barrett et al., 2018; Kaelen et al., 2018). The current findings are consistent with this growing body of evidence and support the important contribution of music to classic psychedelic-assisted therapy. However, because some participants did not enjoy the music, study personnel should consider offering the option of changing or turning off the music.
Finally, participants endorsed near-universal support for the clinical utility of LSD. They reported the belief that LSD is a relatively safe drug with the potential to help others and expressed support for additional scientific study on its clinical application. Although participants were supportive of the clinical utility of LSD, a number emphasized caution, urging for appropriate screening of participants and administration in controlled environments similar to the current protocol. Interestingly, one participant stated that LSD-assisted treatment could be effective in treatment of alcohol misuse. This is consistent with a major line of research in the older body of LSD literature (Krebs and Johansen, 2012). In sum, these findings suggest that participants believed they benefited from their participation, further supporting the potential efficacy of the current paradigm in clinical populations.
Results of the current research should be interpreted in light of some important limitations. Most notably, participants were healthy and did not meet criteria for any mental health conditions. This is significant because neuroticism, which is robustly associated with a number of mental health conditions (Lahey, 2009), is also associated with the intensity of challenging experiences with psilocybin mushrooms (Barrett et al., 2017). It is possible, therefore, that individuals suffering from anxiety, mood, substance use, or other disorders might require more intensive pre-drug preparation, support during the acute period of drug action, and post-drug integration so as to mitigate these outcomes. It also stands to reason that the current novel intervention paradigm would need to be augmented with components designed to address the targeted mental health condition with a focus on the post-acute “afterglow” period, which may represent an ideal window of opportunity for behavior modification (Garcia-Romeu et al., 2020). Relatedly, future research would need to account for psychotherapy process constructs, including therapist empathy, therapeutic alliance, and feelings of connectedness and acceptance (Elliott et al., 2018; Martin et al., 2000; Watts et al., 2017). As noted in the “Introduction” section, healthy participants were deemed appropriate for this initial proof-of-concept study as these individuals can and do have both challenging experiences and transcendent, mystical-type experiences associated with improvements in psychological functioning with classic psychedelics. However, how and whether the current findings generalize to clinical populations is a key question for future research. Similarly, the generalizability of the current findings to less affluent Western cultural contexts, samples with larger proportions of women, and studies using larger doses of LSD requires further interrogation. Furthermore, though gender differences would not be expected in the accounts reported here, it is notable that most participants in this study were men and future studies should investigate any possible differences not accounted for in this sample. Finally, though interviewers were either unknown to the participants or not in the room with them during the acute period of drug action, as in any study, demand effects may have influenced participant responses.
These limitations notwithstanding, the current study evaluates a novel LSD intervention paradigm designed for enhanced scalability, with qualitative data providing preliminary support for its safety as well as its potential therapeutic efficacy and clinical utility. As the intensive nature of the predominant classic psychedelic-assisted treatment approach may limit its real-world implementation, the current findings provide a foundation for future clinical research with the ultimate goal of promoting broad accessibility to LSD-assisted psychotherapy.
Supplemental Material
sj-docx-1-jop-10.1177_02698811211055855 – Supplemental material for Perceptions of safety, subjective effects, and beliefs about the clinical utility of lysergic acid diethylamide in healthy participants within a novel intervention paradigm: Qualitative results from a proof-of-concept study
Supplemental material, sj-docx-1-jop-10.1177_02698811211055855 for Perceptions of safety, subjective effects, and beliefs about the clinical utility of lysergic acid diethylamide in healthy participants within a novel intervention paradigm: Qualitative results from a proof-of-concept study by Peter S Hendricks, Heith Copes, Neiloufar Family, Luke TJ Williams, David Luke and Shlomi Raz in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NF, LTJW, DL, and SR were paid consultants of Eleusis Companies. PSH is on the scientific advisory board of Eleusis Benefit Corporation, Bright Minds Biosciences Ltd., and Reset Pharmaceuticals Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Eleusis Health Solutions Ltd.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.