
Abstract
Background:
Suicide is one of the leading causes of death worldwide and rates within the United States have risen over the past two decades. Hence, there is a critical need for novel tools to treat suicidal ideation and related mental health conditions. 3,4-Methylenedioxymethamphetamine (MDMA)/ecstasy and classic psychedelics may be two such tools.
Aims:
The aim of this study was to assess non-causal associations between MDMA/ecstasy and classic psychedelic use and psychological distress and suicide risk.
Methods:
In this study, we examined the aforementioned associations among 484,732 adult participants in the National Survey on Drug Use and Health (2008–2019).
Results:
Lifetime MDMA/ecstasy use was associated with reduced odds of past year suicidal thinking (10% reduced odds; odds ratio (OR) = 0.90; 95% confidence interval, CI = (0.84–0.97); p < 0.01) and past year suicidal planning (OR = 0.88; 95% CI = (0.78–0.99); p < 0.05). Furthermore, lifetime psilocybin use was associated with reduced odds of past month psychological distress (OR = 0.78; 95% CI = (0.73–0.84); p < 0.001) and past year suicidal thinking (OR = 0.90; 95% CI = (0.83–0.96); p < 0.01). Finally, lysergic acid diethylamide (LSD) was associated with increased odds of past year suicidal thinking (OR = 1.07; 95% CI = (1.00–1.15); p < 0.05).
Conclusion:
MDMA/ecstasy and psilocybin use are associated with reduced odds of suicidal thinking and related outcomes—though experimental studies are needed to determine whether these associations are causal. These findings call for more research into the efficacy of MDMA/ecstasy and classic psychedelics for treating psychological distress and suicidal thoughts and behaviors, and for updated drug legislation that allows for further investigation into these substances.
Suicide is among the leading causes of death worldwide (World Health Organization, 2019) and despite decades of research, suicide rates in the United States have continued to climb in recent years (Hedegaard et al., 2018a, 2018b, 2020), even as the percentage of suicidal people who receive treatment has dramatically increased (Kessler et al., 2005). Moreover, meta-analyses of existing treatments suggest that they have small effects at best (Inagaki et al., 2015; Kothgassner et al., 2020; Tarrier et al., 2008). Thus, there is an urgent need for novel treatments to assist in the alleviation of suicidal thoughts and behaviors (STBs), as well as the mental health conditions that give rise to STBs.
3,4-methylenedioxymethamphetamine (MDMA) and classic psychedelics (i.e. lysergic acid diethylamide (LSD), peyote, psilocybin, mescaline) offer two potential avenues for novel treatments for STBs and related mental health conditions. MDMA was first synthesized in 1912 by Merck; the compound increases feelings of empathy and social connectedness, as well as the ease of processing and discussing difficult memories. Classic psychedelics, on the other hand, are found in nature or are synthesized from natural compounds and elicit mystical-type experiences that can have lasting personal and spiritual significance (Griffiths et al., 2006). Four of the main compounds included in this class of substances are LSD (synthesized from the ergot fungus), psilocybin (the active component within “magic mushrooms”), peyote (a cactus with psychoactive properties), and mescaline (the active compound within peyote). In the 1950s–1970s, MDMA and classic psychedelics were in clinical use, and evidence from the time suggested these compounds held significant therapeutic potential (Dyck, 2015; Greer and Tolbert, 1986, 1998; Holland, 2001; Sessa et al., 2019). However, following recreational use of MDMA (a.k.a. “Ecstasy”) and classic psychedelics and sensationalized media coverage on their risks, these substances were classified as Schedule 1 substances by the Drug Enforcement Administration (DEA) in the 1970s (no accepted medical uses and a high risk for abuse). Over the subsequent decades, virtually no research was conducted on MDMA or classic psychedelics (Nutt et al., 2013).
However, in recent years, researchers have begun to explore MDMA and classic psychedelics as treatments for a host of psychiatric disorders that confer risk for STBs (Müller et al., 2020). Starting in 2011, researchers reported that MDMA showed promise as a treatment for people with chronic and treatment-resistant post-traumatic stress disorder (PTSD), many of whom were experiencing STBs (Mitchell et al., 2021; Mithoefer et al., 2019, 2011, 2013; Oehen et al., 2013; Ot’alora et al., 2018). Anxiety disorders are a key risk factor for suicide (Cougle et al., 2009; Nepon et al., 2010) and PTSD is among the strongest anxiety-related predictors of suicidal ideation and behavior (Bentley et al., 2016), indicating MDMA may effectively treat key risk factors for suicide. MDMA also has demonstrated efficacy at treating social anxiety (Danforth et al., 2018) and may successfully treat anxiety associated with life-threatening illnesses (Multidisciplinary Association for Psychedelic Studies, 2020), suggesting yet more pathways through which MDMA may reduce the risk for suicide.
Trials of classic psychedelics similarly demonstrate promise. A 2011 pilot trial consisting of individuals with late stage cancer found that a single session of psilocybin-assisted psychotherapy elicited significant and sustained reductions in anxiety and depression (Grob et al., 2011), another well-known risk factor for suicide (Gaynes et al., 2004; Kessler and Bromet, 2013). A 2016 trial replicated these findings (Griffiths et al., 2016). In addition, a 2014 trial found that LSD promoted significant reductions in state and trait anxiety related to life-threatening illnesses as well (Gasser et al., 2014). In addition to treating anxiety and depression, classic psychedelics also have demonstrated efficacy at treating substance use disorders, another key antecedent of STBs (Bogenschutz et al., 2015; Bohnert et al., 2017; Harris and Barraclough, 1997; Johnson et al., 2014; Wilcox et al., 2004). Overall, extant clinical evidence suggests MDMA and classic psychedelics may hold promise for treating STBs.
Despite the strong evidence suggesting the therapeutic potential of both MDMA and classic psychedelics, these substances retain their Schedule 1 designations, leaving many gaps in our understanding. While conducting trials of these substance remains difficult, population-based survey studies provide one fortuitous way to examine the link between these compounds, mental health, and STBs. Although one cannot use population-based surveys to draw causal inferences, the robust samples and the strong external validity offered by large surveys allow one to make solid population-level inferences about the relationship of MDMA/ecstasy and classic psychedelics to mental health and STBs (Jones et al., 2013).
To our knowledge, only four prior population-based studies have investigated the associations between classic psychedelic use and mental health, and none have looked specifically at the associations between MDMA/ecstasy use and these outcomes. First, Krebs and Johansen (2013) analyzed data from the 2001–2004 samples of the National Survey on Drug Use and Health (NSDUH) and found that lifetime classic psychedelic use was largely unrelated with past month psychological distress, past year mental health treatment use, and past year DSM-IV diagnoses (American Psychiatric Association, 1994). Second, Hendricks et al. (2015b) analyzed data from nearly 190,000 American adult respondents from the NSDUH (2008–2012) and found that classic psychedelic use was associated with lowered odds of past month psychological distress, suicidal ideation, suicidal planning, and suicidal attempting. Third, Hendricks et al. (2015a) found that the findings of Hendricks et al. (2015b) extend to psilocybin use specifically. Finally, Sexton et al. (2020) compared the outcomes of classic versus novel psychedelic drug use and found that classic tryptamines (i.e. psilocybin and dimethyltryptamine (DMT)) were associated with decreased odds of psychological distress and STBs.
The current study seeks to expand on this earlier work and investigate non-causal associations of MDMA/ecstasy and classic psychedelic use with psychological distress and STBs. More specifically, we expanded on the work of Hendricks et al. (2015b) and Sexton et al. (2020) by incorporating more recent survey data and testing whether those who report lifetime use of MDMA/ecstasy or classic psychedelics report significantly lower odds of past month psychological distress and past year suicidal ideation, suicidal planning, and suicide attempting.
Methods
Sample
Data are from the NSDUH, an annual survey that aims to provide the latest information on substance use, mental health, and overall health in the United States. NSDUH employs a complex, multistage probability sample design and is conducted in all 50 states and the District of Columbia on citizens aged 12 years and older. NSDUH uses a computer-assisted self-interviewing paradigm in which interviewers administer the survey in participants’ homes; individuals listen to pre-recorded questions and submit answers on the computer. For our analyses, we used all 12 years of available data on our outcomes of interest within the NSDUH database (2008–2019) (United States Department of Health and Human Services, 2008, 2009, 2010, 2011, 2012, 2013, 2014, 2015, 2016, 2017, 2018, 2019). The overall sample size for these years was 484,732. All NSDUH data is publicly available and can be found at: https://www.datafiles.samhsa.gov.
We included lifetime use of the following substances as independent variables in our analyses: MDMA/ecstasy, classic psychedelics (psilocybin, LSD, peyote, mescaline), other illegal substances (cocaine, heroin, phencyclidine (PCP)), and commonly misused legal substances (inhalants, pain relievers, tranquilizers, stimulants, sedatives, and marijuana).
We included in our analyses the four outcome variables measuring psychological distress and STBs that were included in the NSDUH survey: past month serious psychological distress, past year suicidal ideation (At any time in the past 12 months . . . did you seriously think about trying to kill yourself?), past year suicidal planning (During the past 12 months, did you make any plans to kill yourself?), and past year suicide attempt (During the past 12 months, did you try to kill yourself?). Past month serious psychological distress is a composite variable included in the NSDUH survey based on the following six domains: feeling nervous, feeling hopeless, feeling restless or fidgety, feeling so sad or depressed that nothing could cheer you up, feeling that everything was an effort, and feeling down on yourself, no good, or worthless. Participants provided a score of 0 (“none of the time”) to 4 (“all of the time”) for each domain, and participants with a total score of 13 or greater (out of 24) were coded positively for past month serious psychological distress.
Data analysis
For our analyses, we drew from the approach of Hendricks et al. (2015b) and conducted four multivariable logistic regressions to test the non-causal associations between use of all aforementioned substances and our four dependent variables assessing psychological distress and STBs. In line with Hendricks et al. (2015b) and Hendricks et al. (2018), we controlled for the following covariates: sex (male or female), age (25, 26–34, 35–49, 50–64, or 65 or older), race (Non-Hispanic White, Non-Hispanic Black, Non-Hispanic Native American/Alaska Native, Non-Hispanic Native Hawaiian/Pacific Islander, Non-Hispanic Asian, Non-Hispanic more than one race, or Hispanic), educational attainment (5th grade or less, 6th grade, 7th grade, 8th grade, 9th grade, 10th grade, 11th grade, 11th or 12th grade, high school diploma, some college (no degree), Associate’s degree, college degree or higher), self-reported engagement in risky behavior (never, seldom, sometimes, or always), annual household income (less than $20,000, $20,000–$49,999, $50,000–$74,999, or $75,000 or more), marital status (married, divorced/separated, widowed, or never married), and survey year (2008–2019). All analyses were conducted in R version 3.5.3 using the “Survey” package (Lumley, 2020) and incorporated the sampling weights and complex study design provided by the NSDUH survey.
Results
Rates for past month psychological distress and past year suicidal ideation, planning, and attempt were 5.3%, 4.1%, 1.2%, and 0.5%, respectively. 9.4% of participants reported lifetime use of psilocybin, whereas 7.1% reported lifetime use of MDMA/ecstasy.
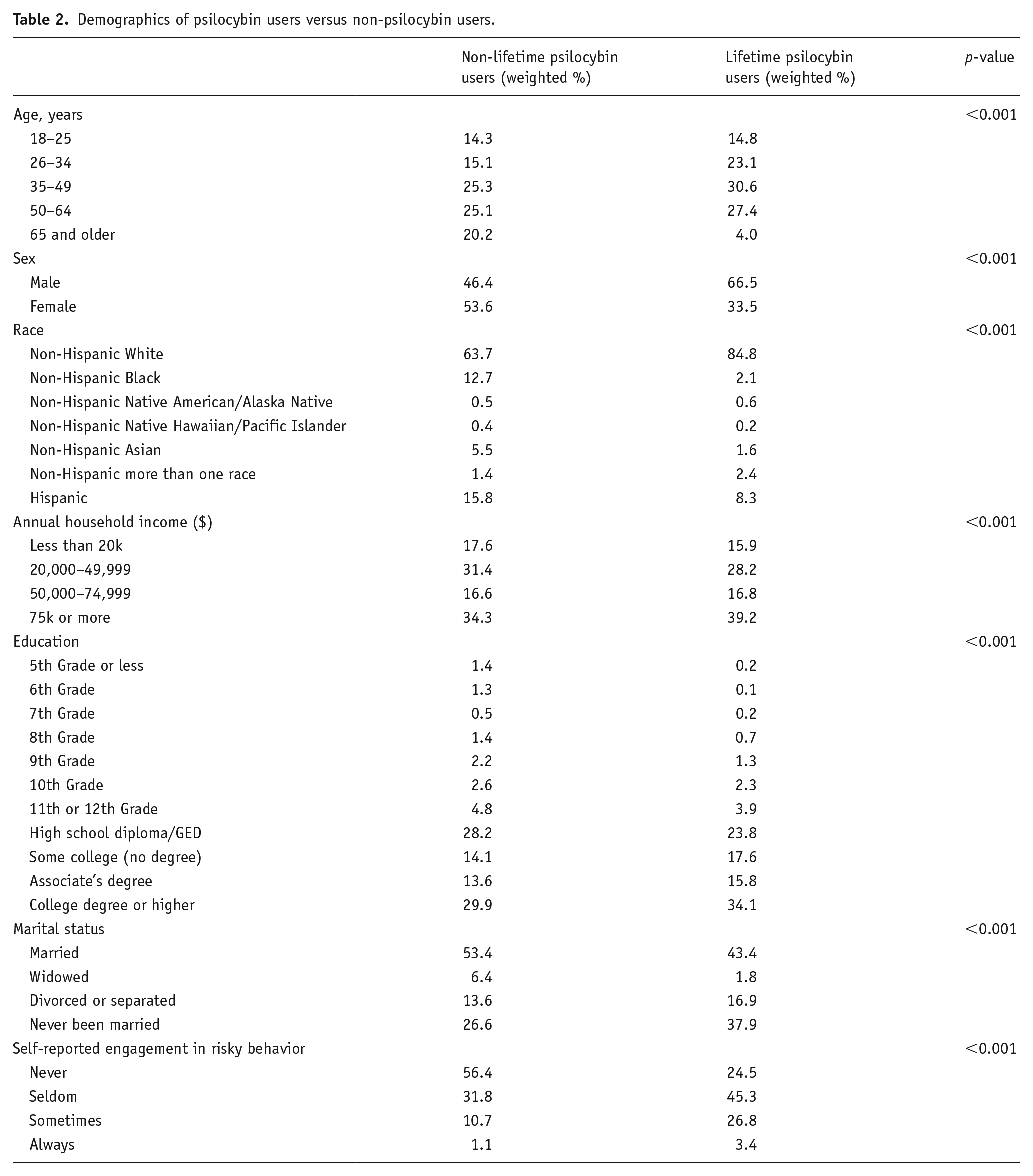
Table 1 provides information regarding those who have versus have not used MDMA/ecstasy in their lives. Lifetime MDMA/ecstasy use was distributed relatively evenly among individuals aged 18–49 years, with lower rates of lifetime use among those aged 50 years and older. Most individuals who have used MDMA/ecstasy are male, Non-Hispanic White, higher income ($75k or more), formally educated (High School Diploma or College Educated), and report seldom engagement with risky behaviors. Table 2 provides demographic information for those who have versus have not used psilocybin. Although lifetime psilocybin use skews slightly older than MDMA/ecstasy use, the demographics for psilocybin use roughly mirrored those of MDMA/ecstasy use (White, higher income, educated, and reporting seldom engagement with risky behavior).
Demographics of MDMA/ecstasy users versus non-MDMA/ecstasy users.
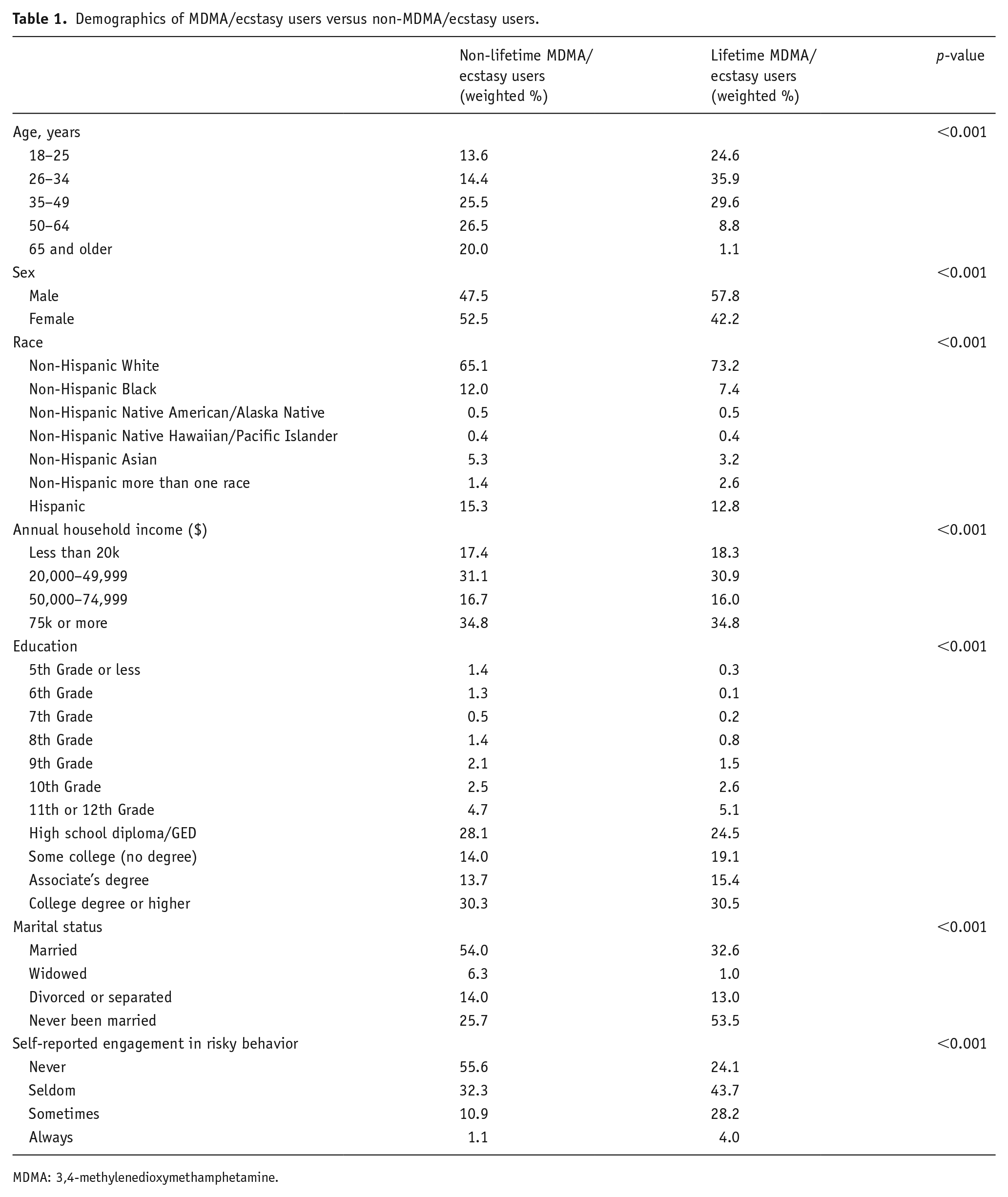
MDMA: 3,4-methylenedioxymethamphetamine.
Demographics of psilocybin users versus non-psilocybin users.
Figures 1 to 4 present the results of four multivariable logistic regression models predicting past month psychological distress, past year suicidal ideation, past year suicidal planning, and a past year suicide attempt. Lifetime MDMA/ecstasy use was associated with significantly reduced odds of past year suicidal thinking (10% reduced odds; odds ratio (OR) = 0.90; 95% confidence interval (CI) = (0.84–0.97); p < 0.01) and was additionally associated with reduced odds of past year suicidal planning (12% reduced odds; OR = 0.88; 95% CI = (0.78–0.99); p < 0.05).
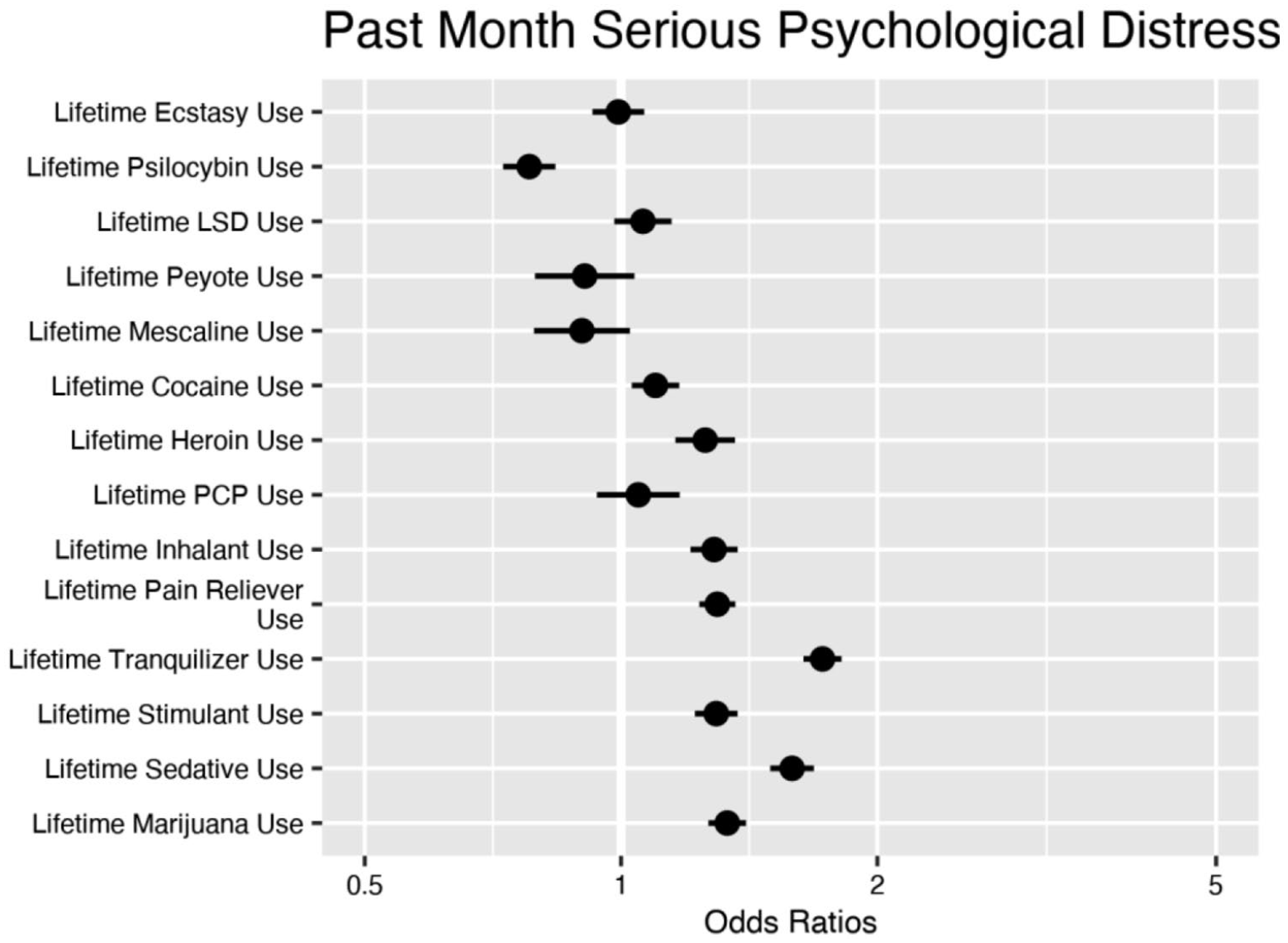
Result of multiple logistic regression model predicting past month serious psychological distress. Circles are point estimates and the bars are 95% confidence intervals.
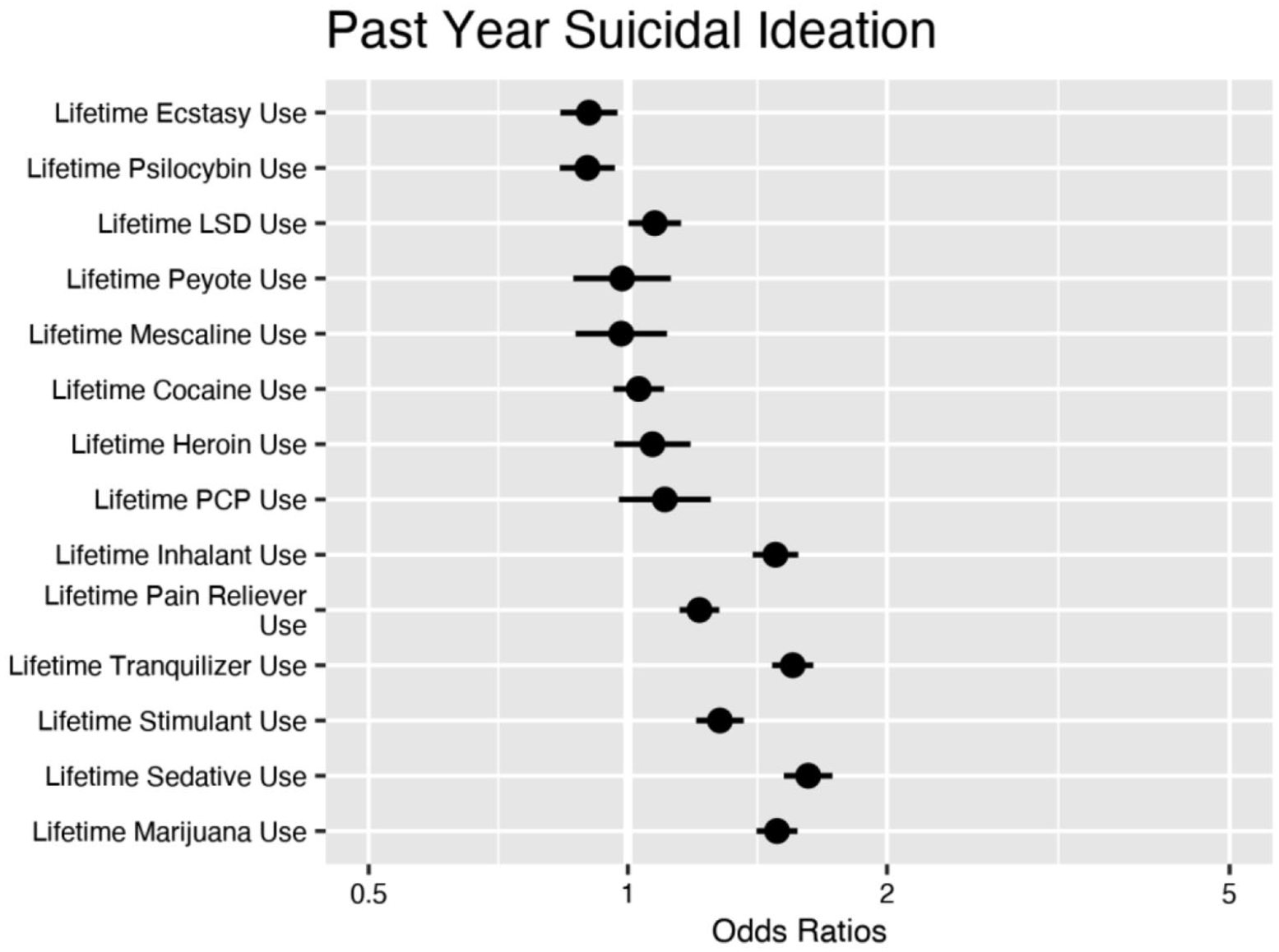
Result of multiple logistic regression model predicting past year suicidal ideation. Circles are point estimates and the bars are 95% confidence intervals.
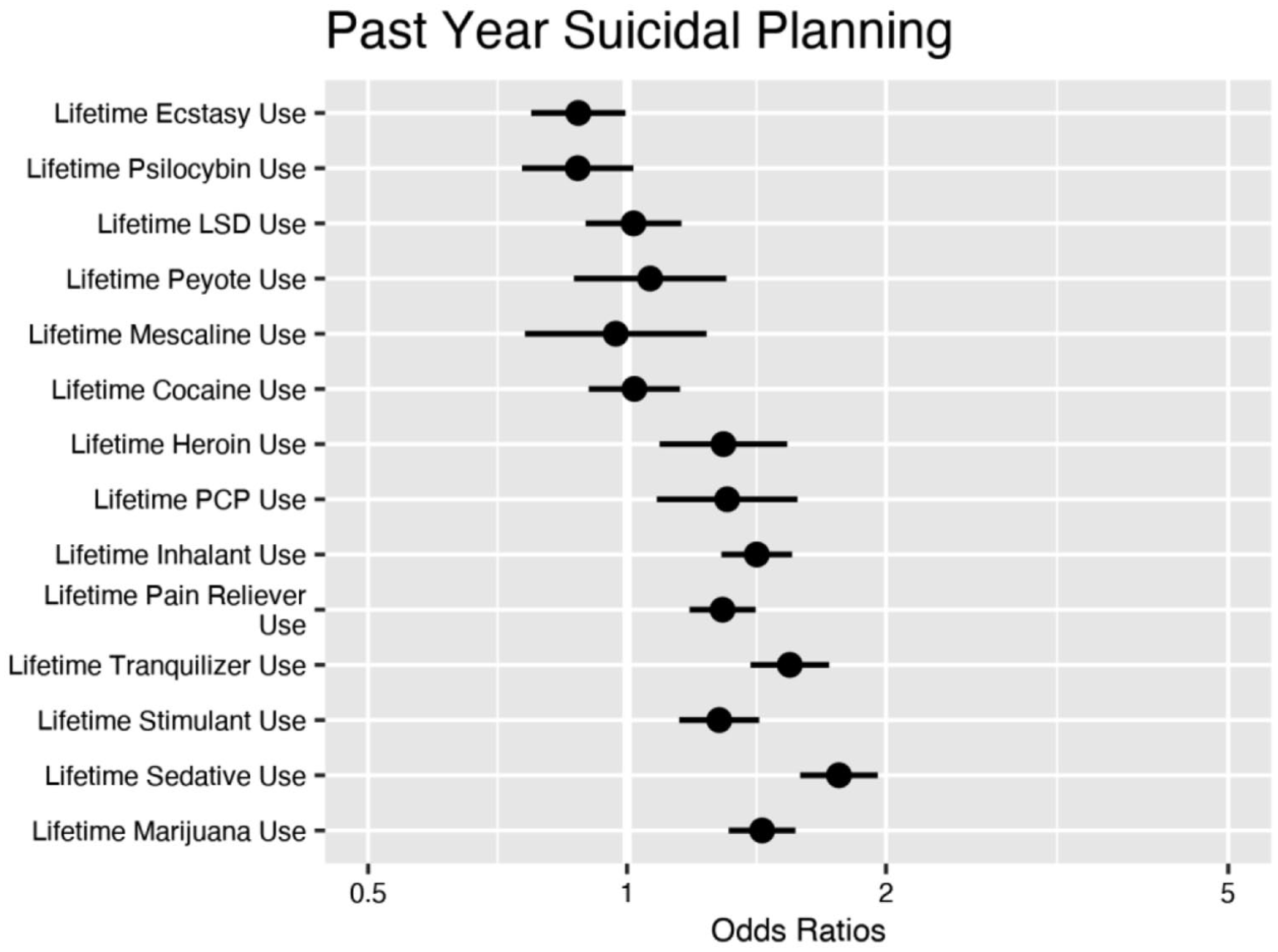
Result of multiple logistic regression model predicting past year suicidal planning. Circles are point estimates and the bars are 95% confidence intervals.
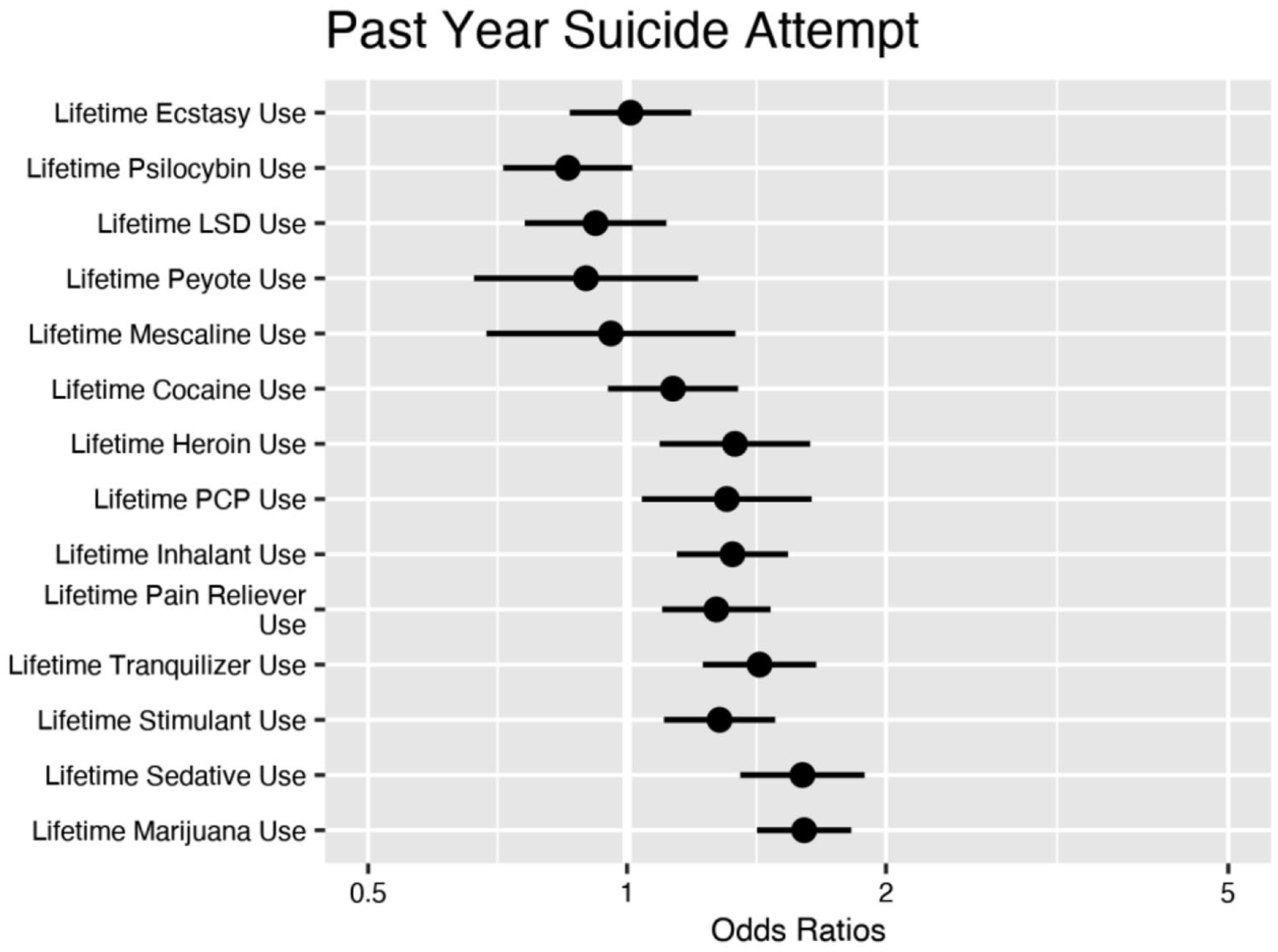
Result of multiple logistic regression model predicting past suicide attempt. Circles are point estimates and the bars are 95% confidence intervals.
Lifetime psilocybin use was associated with significantly reduced odds of past month psychological distress (22% reduced odds; OR = 0.78; 95% CI = (0.73–0.84); p < 0.001) and past year suicidal thinking (10% reduced odds; OR = 0.90; 95% CI = (0.83–0.96); p < 0.01) and was marginally associated with decreased odds of past year suicidal planning (OR = 0.88; 95% CI = (0.76–1.01); p = 0.08) and a past year suicide attempt (OR = 0.85; 95% CI = (0.72–1.01); p = 0.07). Lifetime use of other classic psychedelics (LSD, peyote, mescaline) largely shared no relationship with any of our outcomes of interest; LSD, however, was associated with increased odds of past year suicidal thinking (7% increased odds; OR = 1.07; 95% CI = (1.00–1.15); p < 0.05).
In addition, lifetime use of all other substances (cocaine, heroin, PCP inhalants, pain relievers, tranquilizers, stimulants, sedatives, and marijuana) either shared no associations with our outcomes of interest or conferred increased odds of distress or STBs.
Discussion
The aim of this study was to assess non-causal associations of lifetime MDMA/ecstasy and classic psychedelic use with psychological distress and risk of STBs in a large representative sample of the U.S. adult population. In line with our hypotheses, lifetime MDMA/ecstasy use was associated with decreased odds of past year suicidal thinking and planning. In addition, lifetime psilocybin use was associated with decreased odds of past month psychological distress and past year suicidal thinking and was marginally associated with decreased odds of past year suicidal planning and a past year suicide attempt. Lifetime use of all other substances either shared no associations with our outcomes or conferred increased odds of psychological distress and suicide risk.
Our findings on MDMA/ecstasy support the growing evidence linking MDMA to the alleviation of STBs and related mental health conditions. Although we cannot infer causality from this observational study, our findings warrant further investigation into the causal links between MDMA and reduced psychological distress and STBs. Hill’s (1965) criteria for causality provide a framework with which to assess the causal power of this study. Of Hill’s nine criteria, this study demonstrates strength of association between MDMA/ecstasy use and decreased risk of psychological distress and STBs, consistency with prior findings, specificity of effect, temporality (with some caveats discussed below), plausibility, and coherence and analogy with prior findings. The two criteria not yet met are experiment and biological gradient (i.e. dose–response effect), both of which require conducting a randomized controlled trial and suggest this step should be next in this line of research.
There are several potential pharmacological pathways through which MDMA may plausibly decrease STBs. First, MDMA may do so by promoting the release of serotonin and inhibiting its reuptake (Farré et al., 2007; Kamilar-Britt and Bedi, 2015; Liechti et al., 2001; Yazar, Klosinski, and Mithoefer, 2017). Second, MDMA may decrease STBs by increasing neuroplasticity via the increased availability of brain-derived neurotropic factor (BDNF)) (Baumeister et al., 2014; Dwivedi, 2010; Dwivedi et al., 2003; Hendricks et al., 2015b; Vollenweider and Kometer, 2010). Finally, MDMA may reduce STBs through the release of oxytocin, a hormone that increases feelings of social connectedness; the hormone may also lessen fear activity within the amygdala, reducing stress, anxiety, and ultimately STBs (Hysek et al., 2014; Sessa et al., 2019; Thompson et al., 2007).
Overall, the positive findings within our study indicate a need for more clinical trials testing the impact of MDMA on mental health conditions related to STBs, as well as the mechanisms of action underlying MDMA/ecstasy for related outcomes. In addition, these findings add to the growing literature suggesting that the Schedule 1 designation of MDMA/ecstasy should be reviewed and updated. In addition to these positive findings, there have been no significant adverse events within monitored clinical research on MDMA within the past 15 years (Doblin et al., 2014). Updated drug legislation can facilitate further investigations into MDMA/ecstasy and related compounds.
Although the potential harm of MDMA is likely lower than suggested by its Schedule 1 designation, research is still needed to ensure safe engagement with this substance. For instance, Sessa et al. (2019) noted that in clinical trials of MDMA for PTSD, participants can experience an uptick in symptoms immediately following a session due to the intense emotional experiences yielded by the substance; without proper supervision, the researchers note that participants could be at increased risk for STBs or symptom exacerbation. In addition, mild adverse experiences may occur within ~25% of recreational users, who report paranoia, fear, thoughts of death, and panic (Davison and Parrott, 1997). Thus, further research is needed to ensure safety when using MDMA/ecstasy as a therapeutic agent.
Within all currently available NSDUH data, psilocybin was the sole classic psychedelic compound that shared an association with decreased odds of psychological distress and STBs. This finding accords with the broader literature on classic psychedelics, which has largely demonstrated psilocybin to be an effective treatment for a host of mental health conditions that confer risk for STBs (Hendricks et al., 2015b; Johnson and Griffiths, 2017; Sexton et al., 2020). Psilocybin may decrease STBs by increasing neuroplasticity via the transmission of glutamate (Ly et al., 2018; Nichols, 2004, 2016), downregulating serotonin 2A (5HT2A) receptors (the site through which antidepressants and antipsychotics potentiate their effects) (Mahapatra and Gupta, 2017; Van Oekelen et al., 2003; Vollenweider and Kometer, 2010), and reducing markers of inflammation that are linked to STBs and related mental health disorders (Flanagan and Nichols, 2018). To the extent that our current findings do reflect a causal link between use of psilocybin and decreases in psychological distress and STBs, the aforementioned biological mechanisms may be implicated.
In light of our findings on other classic psychedelics (LSD, mescaline, peyote), future research should investigate both the therapeutic potential and the risks of classic psychedelics on outcomes related to psychological distress and STBs. Within this study, LSD was associated with increased odds of past year suicidal thinking. On the contrary, existing evidence has demonstrated LSD, as well as a range of other classic psychedelics (i.e. ayahuasca), to effectively treat mental health disorders that confer risk for STBs (i.e. anxiety, treatment-resistant depression, substance use disorder) (Bogenschutz and Johnson, 2016; Gasser et al., 2014; Palhano-Fontes et al., 2019; Zeifman et al., 2019). Studies that further investigate both the risks and benefits of classic psychedelic substances may assist with the development of safe and effective treatment protocols for a host of disorders.
Limitations
There are a few limitations of note within this study. First, the study design cannot control for important confounds that may exist for the link between MDMA/ecstasy and psilocybin use and decreased odds of STBs. Due to this design, we cannot infer causal relationships from our data. There may be pre-drug differences between those who have versus have not used MDMA/ecstasy and psilocybin that underlie our findings. For instance, ter Bogt et al. (2006) found personality differences between those who have versus have not used MDMA in a naturalistic setting; hence, pre-drug differences such as these may give rise to differences found in our sample. Randomized controlled trials that assess and control for such confounds will be critical for advancing our understanding of MDMA/ecstasy and psilocybin.
Second, this study does not assess moderators or mediators of the observed effects. There remains much that we do not know about the mechanisms through which these compounds may confer their potentially salutary effects. Furthermore, the NSDUH data, given its cross-sectional design, is limited in what it can tell us about mechanisms. Longitudinal research designed to assess moderators or mediators can additionally advance our understanding.
Third, pharmacological interpretations of our study are limited due to the impurity of naturalistic MDMA/ecstasy samples. Whereas some studies have reported naturalistic MDMA/ecstasy to contain MDMA in 100% of samples (Cole et al., 2002), others have found estimates as low as ~60% (Saleemi et al., 2017), weakening pharmacological interpretations of the observed association between MDMA/ecstasy and lowered odds of STBs. However, this limitation may paradoxically strengthen our claims as well. Virtually all common adulterants for MDMA/ecstasy increase risk for neurotoxicity (Clemens et al., 2007; Gorska et al., 2018; Vanattou-Saïfoudine et al., 2012)—amid impure naturalistic samples, it is thus remarkable to find an association between MDMA/ecstasy use and lowered odds of STBs. Randomized controlled trials using pure MDMA may find even stronger associations between MDMA and decreased risk of STBs.
Fourth, as mentioned in our discussion of Hill’s criteria, these data do not allow for the clear establishment of a temporal precedent between MDMA/ecstasy and psilocybin use and our outcomes of interests. As MDMA/ecstasy and psilocybin use were assessed on a significantly longer time horizon (lifetime) than the outcome variables of interest (past month/year), this time gap increases the likelihood that our observed associations are due to third variable factors. However, given the years-long time horizon over which MDMA and psilocybin can potentiate their salutary effects (Agin-Liebes et al., 2020; Mithoefer et al., 2013), our large sample size, and established analytical practice within seminal psychedelics research (Hendricks et al., 2015b, 2018; Pisano et al., 2017; Sexton et al., 2020), we do not believe this limitation substantially hinders the strength of our observed associations. However, future studies that can clearly establish a temporal precedent between MDMA and psilocybin use and outcome variables of interest would strengthen the possible causal inference of similar analyses.
Conclusion
MDMA and classic psychedelics are gaining attention for their therapeutic and clinical potential. The current findings add yet more evidence suggesting that MDMA/ecstasy and psilocybin may hold therapeutic potential for treating psychological distress and suicide and call for further research on these compounds. Overall, this study represents one step toward bettering our understanding of MDMA and classic psychedelics and maximizing their potentially salubrious psychological effects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.